

Cardiology Surgical & Interventional Cardiology Devices Market
Upload
silas-evansCategory
view
220download
0
Valvular Hemodynamics
Morton J. Kern, MDProfessor of Medicine
Chief of CardiologyAssociate Chief CardiologyUniversity California Irvine
Orange, California

Hemodynamic Problems for the Cath Lab
• Valvular heart disease:• Aortic stenosis/insufficiency• Mitral stenosis/insufficiency
• Intraventricular gradients• Pericardial effusion/tamponade• Constrictive/restrictive physiology• Coronary Hemodynamics• Intracardiac Shunts

Tri/MV valves open
Pa/Ao valves are closed
Pa/Ao valves open
Tri/MV valves close
Pa/Ao valves close
Tri/MV valves opensystole
=Valve action

BAMC Case #3117: Patient: 61 yo maleDx: 3V CAD filter: 50 Hz/ sample 250 Hz
Pre ContrastNormal LV and Aortic Pressure Fluid-filled system micromanometer transducers Fluid filled, FA sheath

Normal aortic valve Congenital bicuspid aortic stenosis
Aortic Stenosis

Mechanism of AS: LV-Ao Gradient
Consequences of LV-Ao Gradient:
1. late peaking Systolic murmur
2. Single A23. Slow pulse upstroke

LV
Fusmann and Feldman T, Cath and CV Int 53:553;2001
Hemodynamics of ASPeak to peak pressure gradients differ between ECHO and CATH
Peak instantaneous P-P
Unshifted=larger Grad



Parham and Kern, Cath and CV Int 53:553;2001
Retrograde hemodynamic Assessment of Prosthetic Valves with a Pressure Wire

Low Gradient AS. EF 25%, no CAD. Valve replacement?
P-P gradient 30mmHgCO = 3.2l/m FickAVA = 0.7cm2

Base 10 Dob+Pace 80 20 Dob + Pace 95
Dobutamine challenge for LG AS
P-P = 50mmHgCO = 4.2l/m
AVA = 0.6cm2

Grayburn, P. A. Circulation 2006;113:604-606
What should you do with Symptomatic AS patient, low gradient, low flow? The Dobutamine Challenge
AVA = 0.7cm2
AVA = 1.0cm2
AVA = 1.5cm2
Fixed area

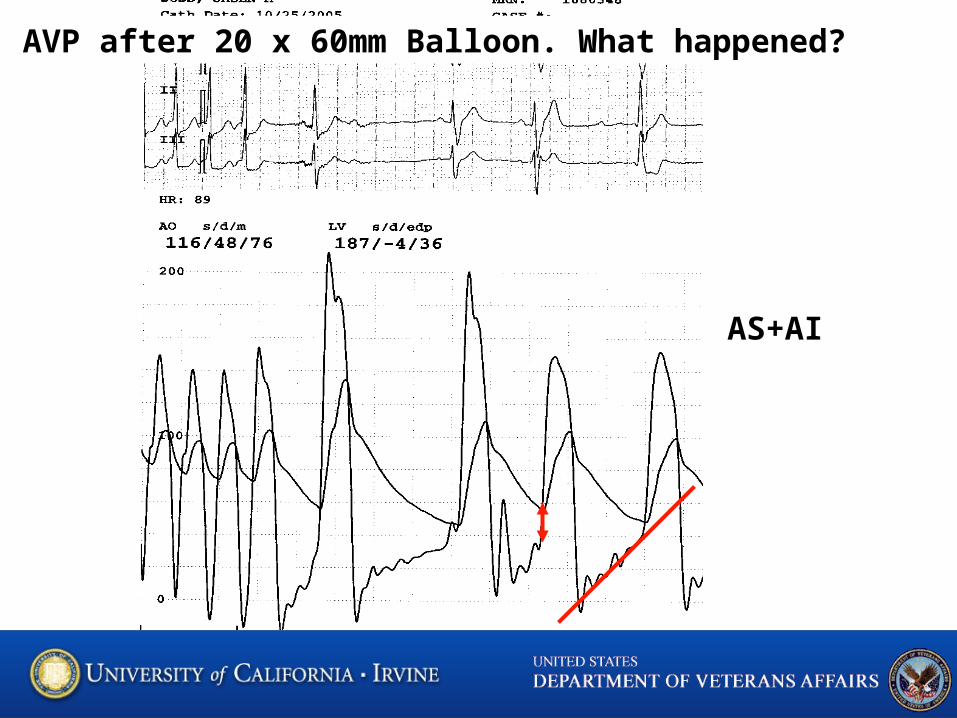
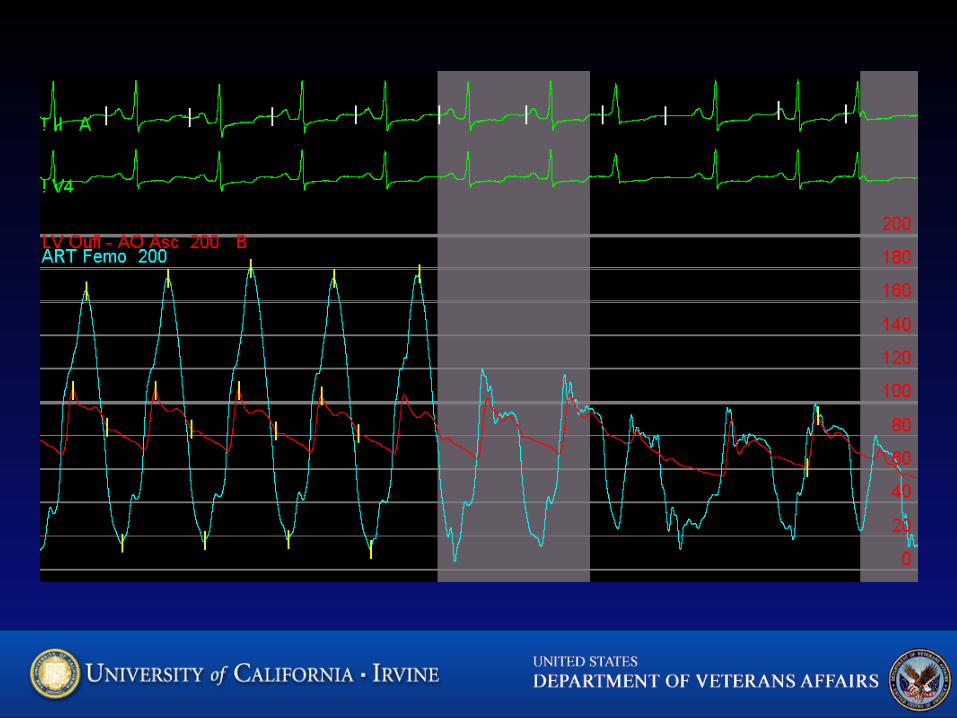
AVP after 20 x 60mm Balloon. What happened?
AS+AI

Hemodynamics of Aortic Insufficiency• Greatest Diastolic Gradient early • Volume filling LV is rapid• LVEDP will be high unless
compensated



Normal LA and LV diastolic pressures LA-LV Diastolic Gradient





Pressure Waves are related Chamber compliance (p/v)

Hemodynamics for the Cath Lab
Low Gradient ASComplications of AVP – AIAS vs. HOCMMitral Regurgitation after MVP for MSDiastolic CHF – constrictive v RestrictiveTamponadeIntracardiac Shunts


















