Valvular Heart Disease/Myopathy/Aneurysm By Nancy Jenkins.
50
Valvular Heart Disease/Myopathy/Aneur ysm By Nancy Jenkins
-
Upload
richard-burdett -
Category
Documents
-
view
222 -
download
1
Transcript of Valvular Heart Disease/Myopathy/Aneurysm By Nancy Jenkins.

Valvular Heart Disease/Myopathy/Aneurysm
By Nancy Jenkins

Definition
• Abnormal dilation of a blood vessel at a site of weakness or a tear in the vessel wall.
• Usually secondary to atherosclerosis.
• Most commonly affect the aorta

Bing Video: Abdominal Aortic Aneurysm Surgery

Aortic Aneurysms• Atherosclerotic plaques deposit beneath the intima
– Plaque formation is thought to cause degenerative changes in the media
– Leading to loss of elasticity, weakening, and aortic dilation• Dilated aortic wall can become lined with thrombi than can
embolize– Leads to acute ischemic symptoms in distal branches
– Important to assess peripheral pulses

Aorta
• Largest artery• Responsible for supplying oxygenated
blood to essentially all vital organs
• **Aneurysm can occur in any artery but the aorta is most common
• Growth rate unpredictable– **Larger the aneurysm greater risk of rupture

May also involve the aortic arch or the thoracic aorta,
Most (3/4) are found in abdominal aorta below renal arteries
¼ are found in the thoracic area

Aortic Aneurysms
– Studies suggest strong genetic predisposition
• *Male gender and smoking stronger risk factors than hypertension and diabetes
• Abdominal aortic aneurysms (AAA)– Occur in 4.1% to 14.2% of men– 0.35% to 6.2% of women over 60– Cause of 16,000 deaths per year

Risk Factors- Atherosclerosis


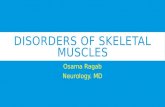
Fusiform
Most AAA are fusiform and 98% are below the renal artery

Aortic AneurysmsClassification
• False aneurysm– Also called pseudoaneurysm– Not an aneurysm– Disruption of all layers of arterial wall
• Results in bleeding contained by surrounding structures• Pseudoaneurysm: an outpouching of a blood vessel,
involving a defect in the two innermost layers (the tunica intima and media) with continuity of the outermost layer, the adventitia. Alternatively, all three layers are damaged and bleeding outside of the vessel is contained by a clot or by surrounding tissue.

False Aneurysms
• May result from– Trauma– Infection– After peripheral artery bypass graft surgery at
site of anastomosis– Arterial leakage after cannulae removal

Aortic AneurysmDiagnostic Studies
• X-rays- Most are diagnosed without symptoms on routine X-ray– Chest - Demonstrate mediastinal silhouette and any
abnormal widening of thoracic aorta
– Abdomen -May show calcification within wall of AAA
• ECG -to rule out MI

Aortic AneurysmDiagnostic Studies
• Echocardiography– Assists in diagnosis of aortic valve
insufficiency• Related to ascending aortic dilation
• Ultrasonography– Useful in screening for aneurysms– Monitor aneurysm size

Aortic AneurysmDiagnostic Studies
• CT scan– Most accurate test to determine
• Anterior to posterior length
• Cross-sectional diameter
• Presence of thrombus in aneurysm
• MRI– Diagnose and assess the location and severity

Aortic AneurysmDiagnostic Studies
• Angiography– Anatomic mapping of aortic system using
contrast– Not reliable method of determining diameter or
length– Can provide accurate info about involvement of
intestinal, renal or distal vessels

Clinical Manifestations By Location-
Thoracic Aortic Aneurysm• Frequently asymptomatic• May have substernal, neck or back pain• Coughing, due to pressure placed on
the windpipe (trachea) • Hoarseness • Difficulty swallowing • Swelling (edema) in the neck or arms • Myocardial infarction, or stroke due to
dissection or rupture involving the branches of the aorta


Ascending Aortic AneurysmAortic Arch
Clinical Manifestations
ASH– Angina – Hoarseness– If presses on superior vena cava
• Decreased venous return can cause– Distended neck veins
– Edema of head and arms

Abdominal Aortic AneurysmClinical Manifestations
• Abdominal aortic aneurysms (AAA)– Often asymptomatic– Frequently detected
• On physical exam– Pulsatile mass in periumbilical area (Grey’s Anatomy)
– Bruit may be auscultated
• When patient examined for unrelated problem (i.e., CT scan, abdominal x-ray)

Aortic AneurysmClinical Manifestations
• AAA, con’t– May mimic pain associated with abdominal or back
disorders– Pain correlates to the size- can be excrutiating– May spontaneously embolize plaque
• Causing “blue toe syndrome” patchy mottling of feet/toes with presence of palpable pedal pulses
• It can rupture, causing shock and death in 50% of rupture cases
–

Nursing Diagnoses
• Risk for Ineffective Tissue Perfusion
• Risk for Injury
• Anxiety
• Pain
• Knowledge Deficit

Medical Treatment of Aneurysms- if less than 5cm
• Anti-hypertensives– Beta blockers, – Vasodilators– Calcium channel blockers– Nipride
• Sedatives• Niacin, mevocor, statins
Post-op anti-coagulants

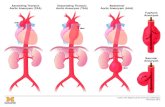
ComplicationAortic Dissection
• Blood invades or dissects the layers of the vessel wall- most often thoracic
Aortic dissection - Wikipedia, the free encyclopedia

Dissecting aneurysms are unique and life threatening. A break or tear in the tunica intima and media allows blood to invade or dissect the layers of the vessel wall. The blood is usually contained by the adventitia, forming a saccular or longitudinal aneurysm.

Aortic Dissection• Affects men more often
than women
• Occurs most frequently between fourth and seventh decades of life
• Acute and life threatening
• Mortality rate 90% if not medically or surgically treated

Aortic DissectionEtiology and Pathophysiology
• As heart contracts, each systolic pulsation ↑ pressure on damaged area– Further ↑ dissection – May occlude major branches of aorta
• Cutting off blood supply to brain, abdominal organs, kidneys, spinal cord, and extremities
• People with Marfan’s at risk

Manifestations of Aortic D issection Aneurysm
Abrupt, severe, ripping or tearing pain in area of aneurysm
Mild or marked hypertens ion early
Weak or absent pulses and blood pressure in upper extremities
S yncopeC omplications: hemorrhage,
ischemic kidneys (renal failure), MI, heart failure, cardiac tamponade, seps is , weakness or paralys is of lower extremities .

Aortic DissectionCollaborative Care
• Initial goal – ↓ BP and myocardial contractility to diminish pulsatile
forces within aorta
• Drug therapy– IV β-adrenergic blocker
• Esmolol (Brevibloc)
– Other hypertensive agents • Calcium channel blockers• Sodium Nitroprusside• Angiotensin-converting enzyme

Aortic Dissection
• Surgical therapy– When drug therapy is ineffective
or
– When complications of aortic dissection are present• Heart failure, leaking dissection, occlusion of an artery
– Surgery may be delayed to allow edema to decrease and permit clotting of blood.
– Even with prompt surgical intervention• 30-day mortality of acute aortic dissections remains high
(10%-28%)

AAA-Medical Treatment - Surgery or Stent
• Usually repaired if >5cm• Open procedure- abd incision, cross clamp
aorta,aneuysm opened and plaque removed, then graft sutured in place. Care much like after CABG (Not done as much anymore unless a rupture)– Pre-op assess all peripheral pulses– Post-op-check urine output and peripheral pulses
hourly for 24 hours- (when to call Dr.)
• Endovascular stents- placed through femoral artery

http://www.youtube.com/watch?v=oQazyeFRNaM
Stent Graft Repair

Aortic Aneurysm
• Endovascular graft procedure, con’t– Approach is percutaneous femoral access
• Advantages– Shorter operative time
– Shorter anesthesia time
– Reduction in use of general anesthesia
– Reduced groin complications within first 6 months

Open Repair of AAA• Post-Op- Similar to CABG
• ICU monitoring– Arterial line
– Central venous pressure (CVP) or pulmonary artery (PA) catheter
– Mechanical ventilation
– Urinary catheter
– Nasogastric tube
– ECG
– Pulse oximetry
– Pain medication

Nursing ManagementNursing Implementation
• Acute Intervention– Postop, continued
• Cardiovascular status– Continuous ECG monitoring
– Electrolyte monitoring
– Arterial blood gas monitoring
– Oxygen administration
– Antidysrhythmic/pain medications

Nursing ManagementNursing Implementation
• Acute Intervention– Postop, continued
• Infection– Antibiotic administration
– Assessment of body temperature
– Monitoring of WBC
– Adequate nutrition
– Observe surgical incision for signs of infection

Nursing ManagementNursing Implementation
• Acute Intervention– Postop, continued
• Gastrointestinal status– Nasogastric tube
– Abdominal assessment
– Passing of flatus is key sign of returning bowel function
– Watch for manifestations of bowel ischemia

Nursing ManagementNursing Implementation
• Acute Intervention– Postop, continued
• Neurologic status– Level of consciousness
– Pupil size and response to light
– Facial symmetry
– Speech
– Ability to move upper extremities
– Quality of hand grasps

Nursing ManagementNursing Implementation
• Acute Intervention– Postop, continued
• Peripheral perfusion status– Pulse assessment
• Mark pulse locations with felt-tip pen
– Extremity assessment
• (5P’s) Temperature, color, capillary refill time, sensation and movement of extremities

Nursing ManagementNursing Implementation
• Acute Intervention– Postop, continued
• Renal perfusion status– Urinary output
– Fluid intake
– Daily weight
– CVP/PA pressure
– Blood urea nitrogen/Creatinine

Nursing Management
• Ambulatory and Home Care• Encourage patient to express concerns
• Patient instructed to gradually increase activities
• No heavy lifting
• Educate on signs and symptoms of complications• Infection
• Neurovascular changes

Prevention• 1.Ultrasound is extremely effective at
detecting AAAs.The U.S. Preventive Services Task Force (USPSTF) recommends that anyone aged 65 to 75 who has ever smoked undergo a one-time ultrasound screening for AAA
• 2.Prevent atherosclerosis• 3.Treat and control hypertension• 4.Diet- low cholesterol, low sodium and no
stimulants• 5.Careful follow-up if less than 5cm. It can
grow .5cm /year

Other Complications
• Rupture- signs of ecchymosis (triad)– Back pain– Hypotension– Pulsating mass
• Thrombi
• Renal Failure

Rupture Triad
Back pain
HypotensionPulsating hematoma

Rupture• Rupture- serious complication related to untreated
aneurysm– Posterior rupture
• Bleeding may be tamponaded by surrounding structures, thus preventing exsanguination and death
• Severe pain
• May/may not have back/flank ecchymosis
Anterior rupture• Massive hemorrhage
• Most do not survive long enough to get to the hospital WHY??

Rupture
False Aortic Aneurysm with Rupture of the Aorta : Medical Animation
http://www.austincc.edu/adnlev4/rnsg2331online/module05/aneurysm_case_study.htm

Patient History27 year old male F ull C ode African AmericanL ives alone in apartmentF amily hx DMMorbid obesity (314.6 lbs )Height: 5’11Ambulates with walker
Medical His tory:E T OH abuseS mokerHypertens ionDO E
S leep apneaT rach (8/30)E jection F raction 50%Hemodialys is (M-W-F )Mitral insufficiency, Mild regurgitation(mitrial, tricuspid)P ressure ulcer on coccyxR espiratory failure with trach , pneumonia, delirium
Student Case Study

(8/13) P t appeared in E R w c/o flank and abd pain
B /P 270/159 (C ardene drip which decreased pressure to 185/73)
Na 138 K 4.4 C h108 B UN 24 C reat 3.0 G lucose 147 C a 8.5 Hgb 12.5
Admiss ion diagnos is : Malignant hypertens ionT ype B Aortic D issectionR enal insufficiencyMorbid obes ity
P t teaching:S moking cessationC ontrol HTNL ifestyle changesDiet controlUse of s tool softeners (increase fluid and fiber in diet)
• E X T R A DX DE VE L O P E D DUR ING HO S P IT AL S T AY :
• Myopathy• Acute respiratory failure• C hronic kidney disease• P neumonia due to S taph
and Hemophilus Influenze
• HT N encephalopathy acute renal dis eas e with les ion of tubular necros is
• Delirium• Uns pec d/o of kidney and
ureter

S urgery
• S urgery is done when an aneurysm is 6 cm in diameter, expanding fast or symptomatic. T ype B diss ections are surgically repaired depending on extent of involvement and risk for rupture.
• Aneurysm excised and replaced with s ynthetic fabric graft.
Nsg Dx:• R isk for Ineffective tissue
perfus ion.• Anxiety

Med i ca ti on s Al lergy:PCN
T reated with long term beta blocker therapy and antihypertens ive drugs as needed to control heart rate and blood pressure. Initially treated with I.V beta blockers such as propranolol (Inderal),metoprolol (L opressor), Normodyne or B revibloc to reduce heart rate to 60 bpm. Niprideinfus ion to reduce systolic to 120mmHg. C alcium channel blockers may also be used. Direct vasodilators are avoided because they may worsen the dissection. After surgery anticoagulants may be initiated; used indefinitely and maybe even lifelong.
P t meds: Albuterol 2.5mg IH q8hHeparin 5000u S Q q8hF lonase nas al spray 2 sprays each nose q12hAmphojel 1020mg q8hC atapress 0.2mg q4hMinoxidil 10mg P O q12hE ns ure supp 240ml P O T IDP rotonix 40mg po dMultivitamin 1 tab P O dL exapro 20mg P O d R enal D ietP rocrit 10000u S Q MWF R P ermacath, R AC , S L