The clinical value of transcranial doppler ultrasonography in patients ...
Upload
durhane-wong-riegerCategory
view
395download
0
TREATING PATIENTS AS
VALUED PARTICIPANTS
Durhane Wong-Rieger, PhD
Chair, Consumer Advocare Network
President, Canadian Organization for Rare Disorders
President & CEO, Institute for Optimizing Health Outcomes
VALUE OF BIOTECHNOLOGY TO PATIENT
1990: height of awareness that 1/3 of hemophilia patients had been infected with HIV through tainted blood products. 7-year old Alex had never received clotting factor because of parental fears. Great hope was recombinant clotting factor. Canada denied access because it was considered “too expensive”
Ap
ril 15
, 20
23
2
VALUE OF BIOTECHNOLOGY TO PATIENT
2002: 32-year-old Mary has been diagnosed with rheumatoid arthritis for 10 years and has already had more than a dozen joint-replacement surgeries. Was in hospital at least half dozen times a year; soon to be wheelchair dependent. Received Enbrel on extended clinical trial and was able to resume normal activities. Public drug plan denied access because of lack of long-term data and cost.
Ap
ril 15
, 20
23
3

VALUE OF BIOTECHNOLOGY TO PATIENT
2004: 44-year old Ken, retired engineer because of Fabry disease; kidney transplant and enlarged heart. Received enzyme-replacement therapy through clinical trial and responded with immediate reduction in symptoms. Assumed would be funded similar to ERT for Gaucher’s. Public drug plan initially denied because of cost and lack of long-term data. Subsequent 3-year funding agreement, but only for patients with severe symptomology.
Ap
ril 15
, 20
23
4

VALUE OF BIOTECHNOLOGY TO PATIENT
2008: 12-year-old Justin with MPS II was excluded from clinical trail because lack of symptoms at time. Now, progressively deteriorating with permanent loss of hearing and mobility reduced in walking, raising arms, and uncurling fists. 10-year-old Nick with MPS II was excluded from clinical trial because of cognitive involvement. Public drug plan has just approved ERT but only to children with symptoms and has denied coverage to patients because they were not represented in clinical trials. New evidence suggests ERT may improve cognitive functioning.
Ap
ril 15
, 20
23
5

VALUE TO WHOM?
Value to individual patient: treatment with most health benefits
Value to healthcare system: treatment with best health benefits relative to costs
Value to payer: treatment with lowest cost Value to society: treatments with health and
social benefits relative to other uses for public funds
Ap
ril 15
, 20
23
6
Ap
ril 15
, 20
23
7
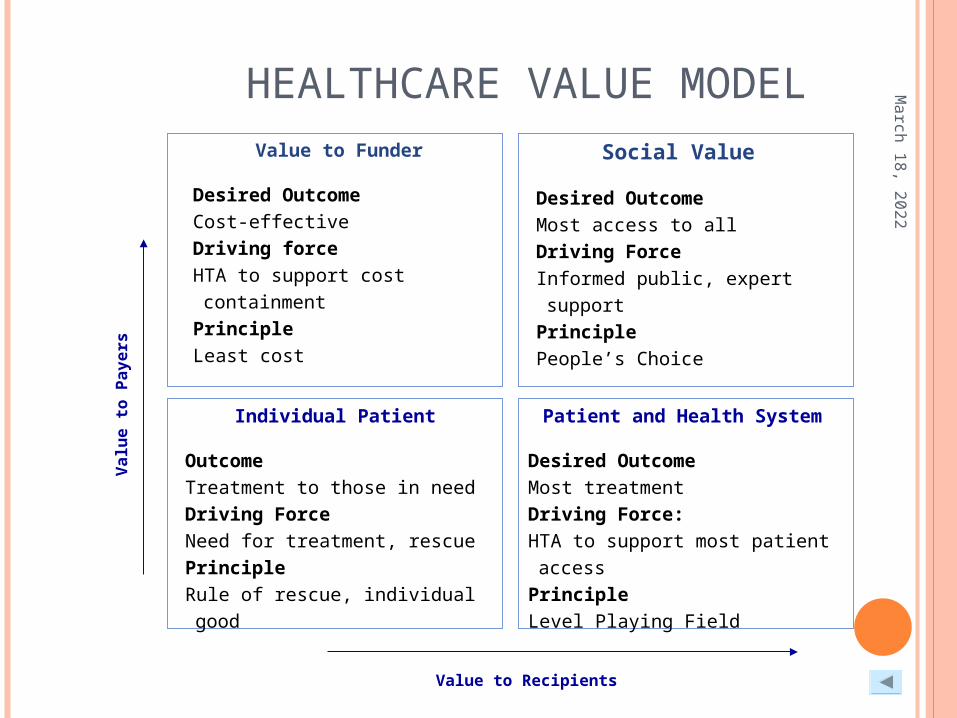
HEALTHCARE VALUE MODEL
Value to Recipients
Valu
e t
o P
ayers
Value to Funder
Desired OutcomeCost-effectiveDriving forceHTA to support cost containment
PrincipleLeast cost
Social Value
Desired OutcomeMost access to allDriving ForceInformed public, expert support
PrinciplePeople’s Choice
Individual Patient
Outcome Treatment to those in needDriving ForceNeed for treatment, rescuePrincipleRule of rescue, individual good
Patient and Health System
Desired OutcomeMost treatmentDriving Force:HTA to support most patient access
PrincipleLevel Playing Field

VALUE OF HEALTHCARE
Value of Healthcare is Degree of Benefit Experienced Like Value of Education, Arts, Sport, or Entertainment Based solely on the benefits to the recipient No further justification of contribution in other ways
necessary Value should not be confused with cost
Cost is what it takes to bring the good to recipient Something may be valuable and not very costly;
something may be costly and not much value Cost refers to what payer is able or willing to pay to make
“good” available
Ap
ril 15
, 20
23
8

SOCIAL VALUES IN HEALTHCARE
Social values are principles, morals, ethics sometimes used by society to decide which “goods” to make available
Anomaly of Canadian Healthcare: Based on Strong Social Values Universal: Achieve sufficiency for all Comprehensive: Essential core needs Portable: Similar service everywhere Medically Necessary: Needed to sustain life Accessible: Available When Needed Sustainable: Funded, Affordable
Drugs are Excluded from Canada Health Act and not subject to social values
Ap
ril 15
, 20
23
9

DRUGS NOT IN CANADA HEALTH ACT
Drug Access is: Not Universal but based on ability to pay or social welfare Essential medicines provided only in hospital or to
seniors, disabled Drug coverage varies considerably across provinces Even “life-saving” medically necessary drugs denied Access may be delayed for long time Sustainability (cost control) driving factor
Drug Access Controlled by Formulary Listing
Ap
ril 15
, 20
23
10

MOST COUNTRIES: RATIONING OF DRUGS
Phenomenon is evident to varying degrees in almost every country, with rules for drug access and rationing that are not applied to most other medical services
“Who gets what, when, and how much of it” not determined as personal decision by your doctor but is based on a “group decision” made by a “disinterested” panel of experts and/or bureaucrats
Ap
ril 15
, 20
23
11

WHOSE VALUES? DEPENDS ON WHO’S PAYING
Value of Regulators: Balance harms and benefits to maximize public good (not individual patients)
Value of Payers: Allocate scarce healthcare$ to maximize benefit to patient roster (not individual patients)
Value of Industry: ROI high enough to justify marketing and low enough to get reimbursement
Value of HC Associations/Academics: Guidelines or “standard of care” (evidence-based for most patients)
Value of Clinicians: Easy access (formulary for most patients) versus “Individual Patient Request” (requires justification)
Value of Patients: Individualized protocol (Right product for right patient at right time)
Ap
ril 15
, 20
23
12

UNCERTAINTY OF BIOTECHNOLOGICAL THERAPIES
Risks very high To industry from discovery to market To regulators where safety issues may take a long time to
be known To patients because of individual variable in response To funders because cost of product is high
Benefits may not be well established Costs often very high
Ap
ril 15
, 20
23
13

CHALLENGE: PUBLIC FUNDING TO VALUE “INCREMENTAL” BENEFIT OF BIOTECHNOLOGY
Biologics are enhanced therapies to replace traditional Biologics are therapies often targeted to smaller
patient populations Recombinant Factor product for hemophiliacs replacing
plasma-based Biologics for arthritis: more advanced degree; where
traditional therapies no longer effective Cancer therapies as 2nd and 3rd line, for those with more
advanced disease For rare diseases
Ap
ril 15
, 20
23
14

WELL BALANCED SOCIETY BARACK OBAMA PLAYING BASKETBALL
Ibbitson (Globe &Mail, Canada): “Don’t underestimate power of Obama’s hoop skills” Well-balanced society is like a pyramid with a detachable
top being spun around an internal gyroscope The three sides = faith, tradition, and reason Top never spins too close to one side where it could fall
down and the whole thing would be in danger of toppling Obama, held in suspicion by the American public for his
intellectual elitism (reason) and affiliation with “religious fringe” (faith) is saved by his ability to make a “3-pointer” (tradition)
Ap
ril 15
, 20
23
15

WELL-BALANCED DRUG VALUATION
Drug Valuation: A Pyramid Balanced by 3 sides: ration, values, and real-life impact Ration = evidence-based rules, including cost-effectiveness
calculations Social values are principles of serving public good Real-life impact = personal benefits, patient reported outcomes,
consumer impact One-sided Drug Plan => No wonder patients experience the
system as “not working” Values are set aside because no one can agree on which values to
apply Real-life impact, or personal appropriateness, has precedence
only when other considerations are negligible, that is, when drugs are abundantly available (very cheap)
Ration claims dominance because it is supposedly objective
Ap
ril 15
, 20
23
16

HEALTH TECHNOLOGY ASSESSMENT: RATIONAL APPROACH Drug Plans Prefer Rational Market Approach
Cost-Benefits Analysis (Buying a Car) Cost-Effectiveness Analysis (Shopping at Walmart) Cost-Utility Analysis (Lifeboat Decision)
“Quasi-scientific” approaches that can be defended Analyses based on “benefits” and “costs” that are often
nonconsensual, controversial and even capricious Process can arrive at “objective” answers, even though different
committees using same process and inputs could arrive at very different conclusions
Provide rational basis for committees to “work through” differences in opinion
Provides rationale why exceptional cases can be rejected
Ap
ril 15
, 20
23
17

HTA INHERENTLY BIASED AGAINST BIOLOGICAL PRODUCTS First recombinant (non-blood derived) clotting factor for
hemophiliacs: more expensive, same efficacy, but no evidence of greater safety
Newer therapies (biologics for rheumatoid arthritis, HIV, cancer) replacing pharmaceuticals but without long-term clinical or survival outcomes or long-term safety data (skews risks-benefits analysis)
First therapies for life-threatening disorders (ERT) may use surrogate measures without evidence of impact on clinical outcomes or long-term survival (makes cost-effectiveness comparisons challenging); lack of natural history of disease for comparison
Early positive results of RCTs for “life-extending” kidney cancer drug compelled company to allow patients to “cross-over”; regulators agreed and approved. Reimbursement committee rejected based on “lack of significant difference” with remaining patient data.
First approved drug for age-related macular degeneration: reimbursement committee initially rejected based partly on comparison with “much cheaper” similar drug being used “off-label”
Ap
ril 15
, 20
23
18

USE OF SOCIAL VALUES INSTEAD OF (IN ADDITION TO) HTA
Leveling Playing Field: Help everyone achieve “basic” well-being
Rule of Rescue: Saving an individual in imminent danger (at all costs)
Most in Need: Saving worst off (regardless of cost and potential benefit)
Fair Innings: Help the young (lives not yet lived) Longevity Reward: Help those who will gain most
(regardless of age) People’s Choice: Numerous small benefits versus few
large benefits (orphan drugs vs. PPIs)
Ap
ril 15
, 20
23
19

WHY SOCIAL VALUES ARE OFTEN IGNORED Reimbursement committees fail to engage in “values-based”
discussions Membership usually includes health economists Members usually receive expert “economic” assessment as well as
medical assessment Members receive training in health economics and
pharmacoeconomic assessments Members have background in scientific methodology
Reimbursement committees not skilled in values deliberations Committees do not include ethicists, social scientists or those who
can speak to values Members receive no training in concepts of justice, ethics, or values Members not trained in dialectic process or deliberative dialogue to
work through competing values or ethical dilemmas NICE: Values considered “after the fact” and application not
systematic
Ap
ril 15
, 20
23
20

WHY PATIENT REAL-LIFE IMPACT NOT REPRESENTED Committees may include patients or public members but there is
no framework for deliberating on “patient impact” or values “I don’t know what I’m expected to contribute. Most of the time,
I’m not an expert in the disease or drug being discussed.” “Sometimes, when I put forth an opinion, others listen politely but
it doesn’t change anything.” “Rules and criteria are such that it really doesn’t matter who is at
the table; decision would be the same.” Affected Patients and patient impact are excluded from the
discussions Testimony from patients or clinicians not allowed at committee “I can’t talk to you about this because it would put me in a conflict
of interest and I would have to excuse myself from decision.” Patients have been forced to take their stories to the media to
reintroduce the “real-life” impact
Ap
ril 15
, 20
23
21

KEY PROBLEM: LACK OF TRANSPARENCY
Committee meetings are closed No record or minutes of discussions Record of decision tends to be sparse Criteria and decision making process are not known No process for patients and clinicians to challenge the
decisions
Ap
ril 15
, 20
23
22

REIMBURSEMENT COMMITTEES: RATIONAL COST CONTROL Canada’s Common Drug Review provides “centralized” HTA-based
recommendation for reimbursement of drugs by public drug plans In 4 years, almost all “me-too” submissions have been recommended for
reimbursemen Less than 25% of “first-in-line” or “novel” therapies have been
recommended (too expensive, lack of evidence, lack of added value) Almost no drugs for rare disorders (orphan drugs) have been recommended
for funding Provincial/territorial/federal drug plans follow similar cost-based
decision making In Ontario, drugs that can demonstrate significant cost savings can receive
“priority reviews” Priority reviews for drugs that are “life-saving” or treat conditions for which
there are no other therapies have generally resulted in negative decisions
Ap
ril 15
, 20
23
23
PATIENT “SUFFRAGE” = TURN OF 20TH CENTURY
Manitoba gave women right to vote in 1916; Canada in 1919; USA in 1920; and Quebec in 1940
In Quebec, at least one hospital has a patient on P&T Committees (there may be more)
In 2006, 2 “public” members were appointed to Canadian Expert Drug Advisory Committee, which recommends drugs for reimbursement on public drug plans
In 2007, 2 “patients” were appointed to Ontario Committee to Evaluate Drugs, which recommends drugs for Ontario Public Drug Plan
Australia, UK, France, EMEA, Netherlands have patients on drug advisory committees for evaluation and/or reimbursement
Ap
ril 15
, 20
23
24

TOUGH CHALLENGES FOR PATIENTS ON REIMBURSEMENT COMMITTEES
“2 are better than 1” but “2 divided are worse than 1” Expertise in being a patient is not the same as being a
patient expert You gotta be able to handle the math No matter how many initials you have after your name,
the minute you’re identified as a patient, you lose 50 IQ points
If you are paid less, you are valued less
Ap
ril 15
, 20
23
25

HOW TO INCORPORATE PATIENT VALUE
Continue to challenge the “cost-effectiveness” and “cost-utility” analyses against “real-life” impact and long-term outcomes
Train patients and public to better engage in health economic and evidence-based deliberations
Develop a values-based decision making framework and train members and public to engage in values deliberations
Bring into the committees the patients and clinicians who represent the “real-life” perspective
Hold meetings in public and make the process publicly accountable
Ap
ril 15
, 20
23
26

CHICKEN AND PIG WHO DECIDE TO OPEN A BREAFAST RESTAURANT
5/2
/08
27
ISP
OR
Chicken was motivated
Pig was totally committed