
Validation of a low-cost HPV genotyping assay based on...
31
1 Validation of a low-cost HPV genotyping assay based on PGMY- 1 PCR and reverse blotting hybridization with reusable membranes 2 Estrade, C. 1 , Menoud, P.-A. 2+ , Nardelli-Haefliger, D. 1 and R. Sahli 1* 3 1: WHO HPV LabNet Regional Reference Laboratory for Europe, Institute of Microbiology, 4 Centre Hospitalier Universitaire Vaudois (CHUV) and University of Lausanne, 1011 Lausanne, 5 Switzerland 6 2: MCL Medical Laboratories, 3172 Niederwangen, Switzerland 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 * Corresponding author. Institute of Microbiology, Bugnon 48, 1011 Lausanne, Switzerland. 23 Phone: +41 21 3144082. Fax: +41 21 3144060. E-mail: [email protected] 24 + Present address: Unilabs, Molecular Diagnostics unit, 1003 Lausanne, Switzerland 25 Running Title: Low-cost HPV genotyping 26 Keywords: HPV genotyping, PCR, Reverse Blotting Hybridization 27 Copyright © 2011, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights Reserved. J. Clin. Microbiol. doi:10.1128/JCM.05039-11 JCM Accepts, published online ahead of print on 10 August 2011 on May 16, 2018 by guest http://jcm.asm.org/ Downloaded from
Transcript of Validation of a low-cost HPV genotyping assay based on...

1
Validation of a low-cost HPV genotyping assay based on PGMY-1
PCR and reverse blotting hybridization with reusable membranes 2
Estrade, C.1, Menoud, P.-A.2+, Nardelli-Haefliger, D.1 and R. Sahli1* 3
1: WHO HPV LabNet Regional Reference Laboratory for Europe, Institute of Microbiology, 4
Centre Hospitalier Universitaire Vaudois (CHUV) and University of Lausanne, 1011 Lausanne, 5
Switzerland 6
2: MCL Medical Laboratories, 3172 Niederwangen, Switzerland 7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
* Corresponding author. Institute of Microbiology, Bugnon 48, 1011 Lausanne, Switzerland. 23
Phone: +41 21 3144082. Fax: +41 21 3144060. E-mail: [email protected] 24
+ Present address: Unilabs, Molecular Diagnostics unit, 1003 Lausanne, Switzerland 25
Running Title: Low-cost HPV genotyping 26
Keywords: HPV genotyping, PCR, Reverse Blotting Hybridization 27
Copyright © 2011, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights Reserved.J. Clin. Microbiol. doi:10.1128/JCM.05039-11 JCM Accepts, published online ahead of print on 10 August 2011
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

2
ABSTRACT 28
Genotyping of human papillomaviruses (HPV) is essential for surveillance of HPV vaccines. 29
Here we describe and validate a low-cost PGMY-based PCR assay (PGMY-CHUV) for genotyping 30
of 31 HPV by reverse blotting hybridization (RBH). Genotype-specific detection limits were 50-500 31
genome equivalents per reaction. RBH was 100% specific and 98.61% sensitive using DNA 32
sequencing as gold standard (n=1024 samples). 33
PGMY-CHUV was compared with the validated and commercially-available Linear Array 34
(Roche) on 200 samples. Both assays identified the same positive (n=182) and negative samples 35
(n=18). Seventy-six percent of the positives were fully concordant after restricting the comparison to 36
the 28 genotypes shared by both assays. At the genotypic level agreement was 83% (285/344 37
genotype-sample combinations; kappa=0.987 for single and 0.853 for multiple infections). Fifty-38
seven of the 59 discordant cases were associated with multiple infections and significantly with the 39
weakest genotypes within each sample (P < 0.0001). PGMY-CHUV was significantly more 40
sensitive for HPV56 (P = 0.0026) and could unambiguously identify HPV52 in mixed infections. 41
PGMY-CHUV was reproducible on repeat testing (n=275 samples, 392 genotype-sample 42
combinations; kappa=0.933) involving different reagents lots and different technicians. Discordants 43
(n=47) were also significantly associated with the weakest genotypes in samples with multiple 44
infections (P < 0.0001). Successful participation in proficiency testing also supported the robustness 45
of this assay. 46
The PGMY-CHUV reagents costs were estimated at 2.4 US Dollars per sample using the least 47
expensive, yet proficient genotyping algorithm including quality control. This assay may therefore 48
be used in low-resource laboratories having sufficient manpower and PCR expertise. 49
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

3
INTRODUCTION 50
High risk genital human papillomaviruses (HPV) are etiologically linked to cervical cancer and 51
other anogenital malignancies. HPV16 and HPV18 account together for 70% of the cases worldwide 52
(25). The infectious nature of cervical cancer raises hopes that vaccines against high risk HPV will 53
effectively reduce the incidence of this disease. The positive effect of the two vaccine formulations 54
available now, Gardasil (quadrivalent HPV6/11/16/18, Merck & Co.) and Cervarix (bivalent 55
HPV16/18, GlaxoSmithKline), has been demonstrated with phase III efficacy trials to yield 56
significant reduction in the frequency of precursor lesions associated with these viruses (21, 27). 57
Some degree of cross protection against infections by HPV31, 33, 45, 52 and 58 have also been 58
reported with Gardasil (37) and for HPV31, 33 and 45 with Cervarix (27). Long term epidemiologic 59
surveillance is therefore required to monitor vaccine efficacy and to monitor HPV genotype-specific 60
disease incidence rates in the vaccination context (14, 30). Continued gynecological and 61
pathological examinations as well as HPV diagnosis will also be required for decades prior to 62
modification of patient’s care approach taking into account the effect of the vaccines since cervical 63
cancer is the rare outcome of long term persistent infections (9). 64
There are several methods to identify HPV infections. While the hybrid capture assay (HCII) has 65
proven its clinical reliability for colposcopic triage of women based on the high risk profile of their 66
HPV infection (6, 12, 32), more sensitive PCR-based assays with typing capacity are necessary for 67
epidemiological purposes and vaccine surveillance. Typing may also be desirable clinically to 68
identify persistent genotypes as an adjunct to clinically validated tests, as it has been shown that 69
persistent infections confer increased risk of high grade disease in an HPV genotype-specific 70
manner, with HPV16, 18, 31 and 33 being most carcinogenic (2, 26). 71
Two widely used HPV genotyping assays that rely on reverse blotting hybridization (RBH) 72
against a panel of HPV genotype-specific probes immobilized on membrane strips are available 73
commercially: Inno-Lipa (Innogenetics) based on the SPF primers (22) and Linear Array (LA, 74
Roche) based on the PGMY primers (17). Both probe panels address the most frequent high risk and 75
several low or undetermined risk genotypes that are frequently observed. These probe arrays cannot 76
be reused as detection reagents leave a precipitate on the membrane that cannot be removed. The 77
performance of both assays is comparable for cervical smears in liquid transport medium in terms of 78
sensitivity, specificity and predictive values (5, 28, 32, 35). Other commercial assays based on probe 79
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

4
hybridization following broad range PCR are also available (CLART, Genomica; DNA chip, 80
Biocare; Papillocheck, Greiner bio-one; PCR Luminex, Multimetrix; HPV genotyping LQ, Qiagen 81
to name a few). Unlike the RBH platforms, these assays require additional potentially expensive 82
instruments. The reagent costs and availability of all commercial assays, regardless of platform, 83
may restrict their use, especially in low-resource settings. 84
We validate the in-house assay based on the PGMY primers and a reusable probe array (PGMY-85
CHUV) described in chapter 5 of the WHO HPV Laboratory Manual (33). We have used this assay 86
in our laboratory as an adjunct to cytology as well as for the follow-up of treated patients and for 87
epidemiological purposes over 10 years. The assay allows genotyping of 40 to 80 samples per day. 88
It was developed under a quality assurance program to ensure its reproducibility and accuracy, and 89
was optimized in terms of costs (2.4 dollars per sample). It has been evaluated within the WHO 90
HPV Laboratory Network after technology transfer to member laboratories, and was found suitable 91
for HPV genotyping with successful participation in proficiency panels established in this network 92
(13, 15). 93
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

5
MATERIALS AND METHODS 94
Samples 95
Nine thousand four hundred and eight ThinPrep® samples were submitted to our laboratory for 96
HPV testing from March 1999 to April 2010. They were from 5904 patients (median age 35 years; 97
IQR, 27-47 years) who visited the outpatient clinics of the Gynecology and Obstetrics Department 98
of our Hospital Center and affiliated family planning centers. HPV testing was performed as an 99
adjunct to cytology. Cytology results were atypical squamous cells of undetermined significance 100
(n=5017 samples; 53.3%), low (n=3683; 39.1%), high (n=112; 1.2%), normal (n=512; 5.4%) or 101
unspecified cytology grades (n=84; 1.0%). 102
Two hundred additional samples were obtained from an external laboratory (MCL diagnostics) 103
for comparison with the Linear Array (LA). 104
Use of clinical samples for assay development and comparative analyses was approved by our 105
local ethics committee. 106
Quality controls 107
WHO HPV proficiency panel DNAs were kindly provided by Carina Eklund and Joakim Dillner 108
(WHO HPV LabNet Global Reference Laboratory, Malmö, Sweden) (15, 16). HPV16 and HPV18 109
plasmid DNA international standards were obtained from NIBSC (38). 110
Positive controls 111
Non biotinylated HPV genotype-specific amplicons were cloned with the pGEM-T (Promega, 112
Dübendorf, Switzerland) or pCR-TOPO (Invitrogen, Basel, Switzerland) cloning kits according to 113
the manufacturer’s instructions. Each positive control was verified by DNA sequencing and kept as 114
a bacterial stab in glycerol at -80°C. 115
SiHa (2 copies HPV16 per cell), CasKi (600 copies HPV16 per cell), HeLa (50 copies HPV18 116
per cell) and HEK293 (HPV negative) cells were used for evaluation of the PGMY PCR sensitivity. 117
Their HPV genome content per cell was confirmed by quantitative real time PCR against HPV16 118
and HPV18 DNA international standards (NIBSC). Cells were grown in DMEM supplemented with 119
10% fetal calf serum in an atmosphere of 5% CO2 at 37°C according to standard procedures. Cells 120
were counted and mixed at appropriate ratios of infected to uninfected cells prior to DNA extraction 121
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

6
with the QIAGEN blood DNA kit according to the manufacturer’s instructions (QIAGEN, 122
Hombrechtikon, Switzerland). 123
Clinical sample DNA extraction 124
Residual ThinPrep® cell suspensions were transferred into 15 ml conical polystyrene tubes and 125
sedimented by low speed centrifugation (1000 x g) for 10 min at room temperature. Cells were 126
suspended in 10 pellet volumes or 200 μl, whichever was larger, of ThinPrep® supernatant prior to 127
DNA extraction. 128
DNA for PGMY-CHUV was purified with the Magna Pure DNA isolation kit I on the Magna LC 129
robot (Roche, Rotkreuz, Switzerland) and eluted in 100 μl elution buffer according to the 130
manufacturer’s instructions. 131
DNA for LA was purified with the Nuclisens DNA extraction kit on the EasyMAG robot 132
(bioMérieux, Geneva, Switzerland) and eluted in 110 μl according to the manufacturer’s 133
instructions. 134
PBS negative controls accompanied systematically each set of clinical samples during the DNA 135
extraction procedure and throughout all PCR and gel electrophoresis steps to assess contaminations. 136
PGMY-CHUV assay 137
The PGMY-CHUV assay was performed as described in chapter 5 of the WHO HPV Laboratory 138
Manual (33). It is based on PCR amplification of HPV DNA with biotinylated PGMY primers (17) 139
and determination of HPV genotypes by RBH against a panel of HPV genotype-specific probes. 140
This panel allows genotyping of 31 HPV (6, 11, 16, 18, 26, 31, 33, 34, 35, 39, 40, 42, 44, 45, 51, 52, 141
53, 54 (AE9 subtype), 55, 56, 57, 58, 59, 66, 68 (ME180 subtype), 69, 70, 73, 82 (AE2 subtype), 83, 142
and 84). Key points for data interpretation are provided below. 143
PCR 144
Five μl sample DNA was PCR amplified in 50 μl replicate (up to 3) reactions with buffer A 145
containing 1.5 mM MgCl2 for the first 8348 samples (33). The most recent 1060 samples were PCR 146
amplified in 50 μl duplicate reactions, one with buffer A and the other with buffer B containing 147
3 mM MgCl2 (33). Buffer B was found necessary to achieve adequate sensitivity for 148
epidemiological purposes, and was introduced for routine genotyping only recently. The analytical 149
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

7
sensitivity of the PCR reaction was determined to be 50 genome equivalents (GE) for genotypes 6, 150
11, 16, 18, 33, 35, 39, 45, 51, 52, 58, 59, 66, 68(ME180 subtype) and 500 GE for HPV31 and 56 151
with proficiency panel DNAs, DNAs from HPV16 and 18 cell lines (CasKi, SiHa and HeLa) and 152
HPV16 and 18 international standards (Supplemental Material 1). 153
Samples were non informative if the HPV and the HLA internal control were negative (33). 154
RBH 155
After gel electrophoretic analysis, amplicons from doubtful or positive reactions were subjected 156
to RBH in a miniblotter allowing up to 45 samples and controls to be processed in parallel. 157
The arrays were produced by covalent binding of the probes to a negatively-charged nylon 158
membrane. This allowed washing the membrane at high temperature in a low salt solution with 159
minimal loss of sensitivity on repeat reprobing. Enhanced chemiluminescence (ECL®) was used to 160
reveal biotinylated hybrids with streptavidin peroxidase after exposure to an autoradiography film. 161
This detection method did not leave an imprint on the membrane and therefore allowed reprobing 162
the arrays. Washing the miniblotter with hydrogen peroxide prevented strong, non-specific 163
background at further membrane usage (Supplemental Material 2). 164
Genotype identification 165
RBH-positives were identified by visual inspection of films (Supplemental Material 2). A 166
positive was defined by signal strength superior to local background, square shape and position 167
within a corresponding grid array. Evaluation was done by two of us independently (CE, RS) to 168
avoid errors due to misreading. Errors were very rare (less than 0.5%). They were associated mainly 169
with lack of genotype recording in multiple infections. 170
For objective evaluation, the film was scanned and stored as a tiff file with 256 grey levels at 200 171
dots per inch. Image analysis software was then used to measure the grey level of each spot 172
(AlphaEaseFC®, v.4.01; Cell Biosciences, Santa Clara, USA). It was expressed as percentage of 173
255, with 100% corresponding to saturating black pixels and 0% as white. On screen display was 174
with gamma value set at 0.90. Image enhancement was not allowed. A blank lane parallel to the 175
probes was used as a negative control to calculate the average background grey value and its 176
standard error. Threshold of positivity was set as grey level > mean background + 5 standard errors, 177
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
8
corresponding visually to very faint signals. The specificity of such low signals was confirmed by 178
DNA sequencing. 179
DNA sequencing 180
Amplicons were purified with the Qiaquick PCR purification kit (QIAGEN) and sequenced with 181
4 μl of the Big Dye Terminator chemistry (BDT v.1.1, Applied Biosystems) in 10 μl reactions 182
containing up to 3 μl purified DNA (10-50 ng) and 3 pmoles of each PGMY11 primer. Labeled 183
DNA from sequencing reactions was purified either by ethanol precipitation or by the Montage 184
SEQ96 purification kit (Millipore, Zug, Switzerland) according to the manufacturer’s instructions, 185
and resolved by capillary electrophoresis on ABI instruments (Applied Biosystems, Rotkreuz, 186
Switzerland). 187
Sequencing chromatograms were evaluated with Chromas (Technelysium, Tewantin, Australia) 188
or Geneious [Drummond AJ, Ashton B, Buxton S, Cheung M, Cooper A, Heled J, Kearse M, Moir 189
R, Stones-Havas S, Sturrock S, Thierer T, Wilson A (2010) Geneious v5.4, available from 190
http://www.geneious.com (accessed June 21, 2011); Biomatters LTD, New Zealand]. Sequence 191
comparison to the non redundant nucleic acid Genbank database was performed with BLAST (1) 192
available at http://blast.ncbi.nlm.nih.gov/Blast.cgi (accessed June 21, 2011) and probe mismatches 193
within sequenced amplicons identified with the find motif tool of Geneious. 194
Reagents and equipment 195
Primers and probes were obtained from 3 different manufacturers (Microsynth, Balgach, 196
Switzerland; Eurogentec, Seraing, Belgium; Eurofins MWG Operon, Ebersberg, Germany). All 197
other reagents and equipment were from the manufacturers indicated in chapter 5 of the WHO HPV 198
Laboratory Manual (33). 199
Linear Array (LA) 200
LA was performed as recommended by the manufacturer (Roche, Basel, Switzerland) except for 201
the input DNA. Five μl DNA in 50 μl PCR reaction was used as larger relative volumes of DNA 202
purified with the EasyMAG system frequently inhibited the PCR. This assay detects 9 additional 203
genotypes compared with PGMY-CHUV: 61, 62, 64, 67, 71, 72, 81, 82 (IS39 subtype) and 89 204
(CP6108). 205
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
9
Validation studies 206
PGMY-CHUV PCR buffer comparison (Supplemental Material 3) 207
Of the 9408 samples submitted to our laboratory for HPV testing, 827 were prospectively 208
collected to compare the performance of PGMY-CHUV realized with PCR buffer A or with PCR 209
buffer B. 210
Probe sensitivity and specificity (Supplemental Material 4) 211
PGMY-CHUV genotyping was completed by DNA sequencing of PCR-positive or doubtful 212
samples if they were also negative or weakly positive by RBH (n=1024 out of 9408 samples). 213
Sequencing was performed for quality control purposes and included also randomly-selected RBH-214
positive samples. 215
Comparison with LA 216
Two hundred samples were collected prospectively at the MCL diagnostic laboratory over 217
several weeks to obtain at least 180 positives covering as much as possible the entire spectrum of 218
high risk genotypes and equilibrated in single vs. multiple infections. This set was supplemented 219
with negative samples selected randomly over this period. Original DNA stored at -20°C was used 220
for PGMY-CHUV testing. Genotypes determined with PGMY-CHUV were recorded before 221
disclosure of LA results. The number of genotypes per sample was determined after combining 222
PGMY-CHUV and LA results assuming 100% probe specificity for each assay. 223
PGMY-CHUV reproducibility 224
Two hundred seventy-nine samples from all women known to have persistent HPV among the 225
5904 patients whose samples were submitted to our laboratory were selected for repeat testing. A 226
single sample was evaluated from each patient to increase genotype/subtype diversity. This mode of 227
selection did not exclude negative samples due to the known fluctuation in HPV DNA detection rate 228
among the same patient over time (36). DNA was stored at -20°C until PGMY-CHUV retesting. 229
Samples were renamed prior to repeat analysis. Repeat HPV typing results were recorded before 230
sample decoding, and then compared with the original data. 231
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
10
Determination of the occurrence of HPV genotypes in routine HPV testing 232
All samples (n=9408) submitted for HPV testing in our laboratory were considered for 233
occurrence data (Supplemental Material 5). Occurrence did not necessarily reflect that of the normal 234
patient’s population since it was determined in a population previously screened by cytology with a 235
high proportion of patients presenting with abnormal cytology (see Samples above). Risk attribution 236
of HPV genotypes was according to Munoz et al. (24, 25). Risk category based on phylogeny is 237
controversial for HPV26 and HPV53 (8, 19, 29). The former was considered as undetermined and 238
the latter as low risk due to its high prevalence in low grade disease and low prevalence, similar to 239
HPV6, in cervical cancer cases (18, 29). 240
Reagent cost evaluation 241
Reagent cost per sample was evaluated using a typical analysis setup in 96 well PCR plates (33). 242
This setup consisted of analyzing each sample together with 5 positive controls (1 with 1000, 2 with 243
100 and 2 with 10 copies of HPV16 DNA) and 2 negative controls (1 DNA extraction control and 1 244
no template PCR control) either with buffer B or with both buffer A and buffer B. One 1000 copy 245
HPV16 control was placed in each additional row of the plate at increasing column number to serve 246
as a unique row identifier when more than 5 samples were analyzed. Systematic gel electrophoretic 247
analysis in 96 well formats was considered together with PCR plate and plastic sealing foil as fixed 248
PCR costs (21 Swiss francs). PCR reagents, polymerase and primers were considered as variable 249
PCR costs (0.81 Swiss francs per reaction). The calculation for RBH took into consideration 250
membrane, probes, probe cross-linking reagent, production of quality control amplicons and the 251
array quality control as fixed costs (103 Swiss francs), hybridization solutions, film, ECL® detection 252
reagents, foam pads and streptavidin peroxidase as variable costs (27 Swiss francs). Filter tips and 253
common labware shared with commercial assays have not been taken into consideration for this 254
calculation except for gel electrophoresis which was specific to PGMY-CHUV. DNA sequencing 255
was not included in cost estimates as it was used only as quality control for assay design purposes 256
and it is not necessary for routine use of PGMY-CHUV. Cost did not include personnel time for 257
preparation and quality control of reagents. DNA extraction was not evaluated in this study. It was 258
therefore not included in the calculations which were for genotyping per se. DNA extraction with 259
the Qiagen kit mentioned above would cost 4 Swiss francs (2.2 US Dollars, US list price) per 260
sample, and should be added to the genotyping cost in order to estimate the total analysis cost. 261
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
11
Data analysis and statistics 262
Tables for statistics were generated with Microsoft Access® or Excel®, and statistics performed 263
with GraphPad Prism [http://www.graphpad.com/quickcalcs/ (accessed June 21, 2011); GraphPad 264
Software, La Jolla, USA]. Agreement of HPV typing results between paired cases was evaluated 265
with the Cohen’s kappa (κ) statistics and their uneven distribution evaluated with the McNemar’s 266
test. Agreement was interpreted as weak (0.200 < κ < 0.401), moderate (0.400 < κ < 0.601), strong 267
(0.600 < κ < 0.801), near perfect (0.800 < κ < 1.000) and perfect (κ = 1.000). Statistics for unpaired 268
cases was performed with the two-sided Fisher’s exact test using 2x2 contingency tables. 269
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
12
RESULTS 270
Comparison with LA 271
To compare PGMY-CHUV with a similar, commercially-available and thoroughly evaluated 272
assay, we examined 200 samples that were genotyped by LA. Of these 200 samples, 182 were 273
positive and 18 negative. Attribution of positive and negative results was identical with PGMY-274
CHUV PCR, independent of the RBH results. Both methods agreed therefore on all samples at this 275
level of evaluation (positive vs. negative). 276
The array-specific genotypes observed during this study were excluded from subsequent analysis 277
as they accounted for only 10% of the observed genotype-sample combinations (HPV34, 44, 57 278
with PGMY-CHUV or HPV61, 62, 64, 67, 71, 72, 81, IS39 and CP6108 with LA, n=38 among 279
382). One HPV61 single infection determined by LA was confirmed by DNA sequencing of 280
PGMY-CHUV amplicon and one IS39 single infection by LA was reported unknown (mixed 281
profile) after PGMY-CHUV DNA sequencing. Both samples were excluded from comparison. 282
Thus 180 of the 182 positive samples contained genotypes represented by both arrays (HPV6, 11, 283
16, 18, 26, 31, 33, 35, 39, 40, 42, 45, 51-56, 58, 59, 66, 68, 69, 70, 73, 82-84). Of 83 single 284
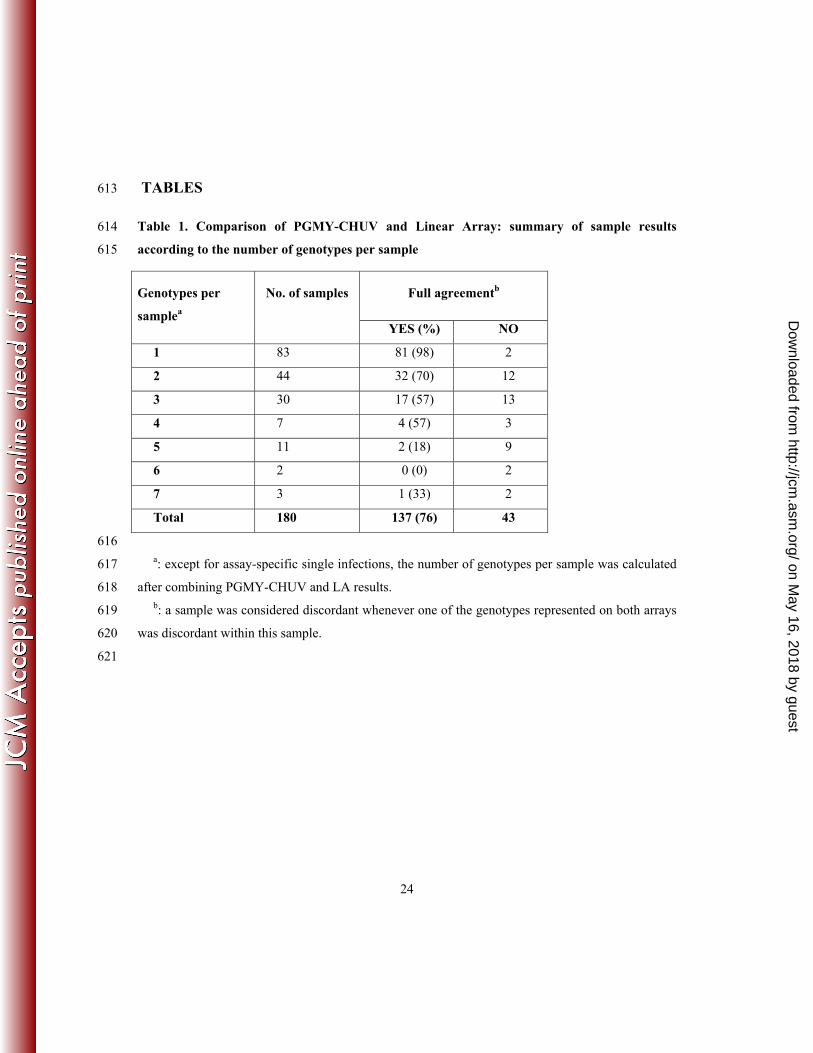
infections reported by LA, 81 (98%) were each attributed the same genotype with PGMY-CHUV 285
(Table 1). The two discordant cases were RBH-negative with PGMY-CHUV and HPV59 and 286
HPV84 with LA. DNA sequencing was used with the corresponding PGMY-CHUV amplicons to 287
evaluate discordance. Both samples were HPV-positive for a genotype not represented on the array 288
as expected: HPV107 and HPV114, respectively. 289
In contrast to samples with single infection, full agreement on samples with double infections or 290
other multiple infections was significantly lower (< 71%, P < 0.0001, two-tailed Fisher’s exact test). 291
On average, full agreement was 76 percent (137/180). Agreement at the genotype level was slightly 292
higher in comparison. Out of 344 genotype-sample combinations, 285 (83%) were concordant 293
(Table 2). Agreement was lower in multiple infections (< 86%, P < 0.0001, two-tailed Fisher’s 294
exact test) compared with single infections (98%) and its level was not associated with the number 295
of genotypes per sample (P > 0.05, two-tailed Fisher’s exact test). 296
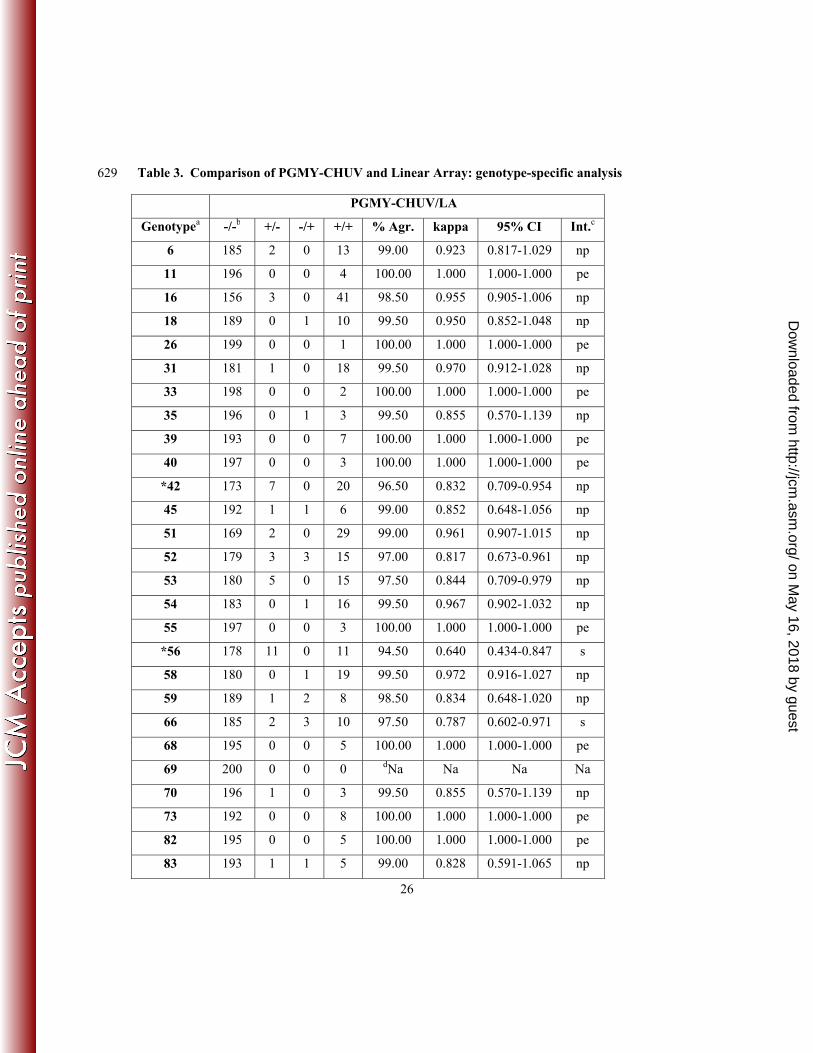
Except for HPV69 which could not be evaluated (n=0), all genotypes were identified by both 297
assays with genotype-specific kappa values superior to 0.639 (strong agreement, Table 3). The 298
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

13
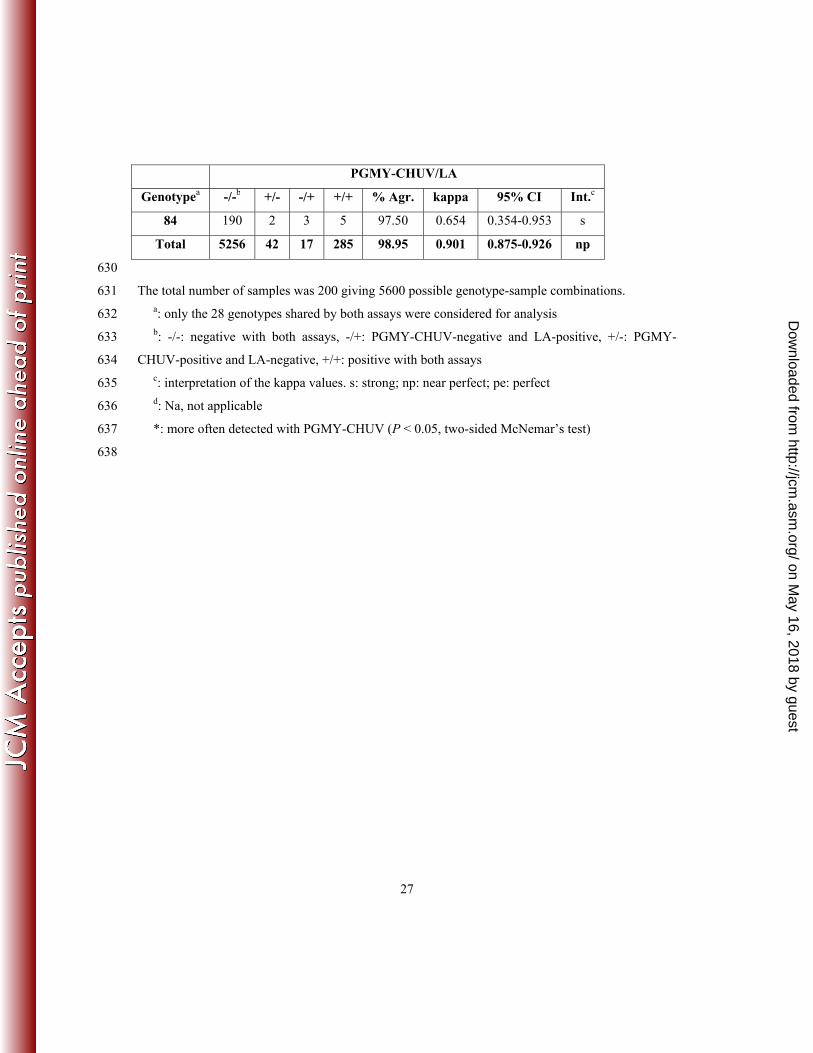
overall agreement was 98.95% (kappa=0.901; 95% CI, 0.875-0.926, near perfect). Average kappa 299
values of 0.987 were observed for single infections and of 0.853 for multiple infections (data not 300
shown). HPV42 (P = 0.0233, two-sided McNemar’s test) and HPV56 (P = 0.0026, two-sided 301
McNemar’s test) were significantly more often detected with PGMY-CHUV conferring together 302
with HPV53 (P = 0.0736, two-sided McNemar’s test) a slightly higher relative sensitivity of 303
PGMY-CHUV over LA (8%; P = 0.0018, two-sided McNemar’s test) when the combined results 304
obtained with both tests served as reference. 305
To assess whether discordant results in multiple infections were associated with genotypes 306
representing a minor fraction in each sample, they were re-evaluated taking into account RBH signal 307
strength. A genotype was considered weak when it had the weakest relative RBH signal strength in 308
comparison with that of all other genotypes within a sample. Of the 59 discordant genotype-sample 309
combinations, 49 (83%) were recorded as weak. In contrast, only 41 (14%) out of 285 concordant 310
combinations were recorded as such. Discordant results in multiple infections were therefore 311
significantly associated with weakly-positive genotypes (P < 0.0001, two-sided Fisher’s exact test), 312
consistent with inter-genotypic competition in the PCR reactions. 313
Reproducibility 314
To verify the robustness of PGMY-CHUV, one sample per patient from a set of 279 independent 315
patients were re-analyzed with different reagent lots and probe arrays. Laboratory work involved 4 316
different technicians over a period of 2 years. The original data were then compared to the newly 317
acquired ones with kappa statistics. 318
Three samples were non informative on repeat testing and one was missing. Of the resulting 275 319
informative samples (98.6%), 13 were reproducibly negative (4.7%), 10 became negative on 320
retesting (3.6%) and 252 were reproducibly positive (91.6%). Most samples (84.0%) showed 321
complete concordance for all genotypes even with multiple infections containing up to 8 (not 322
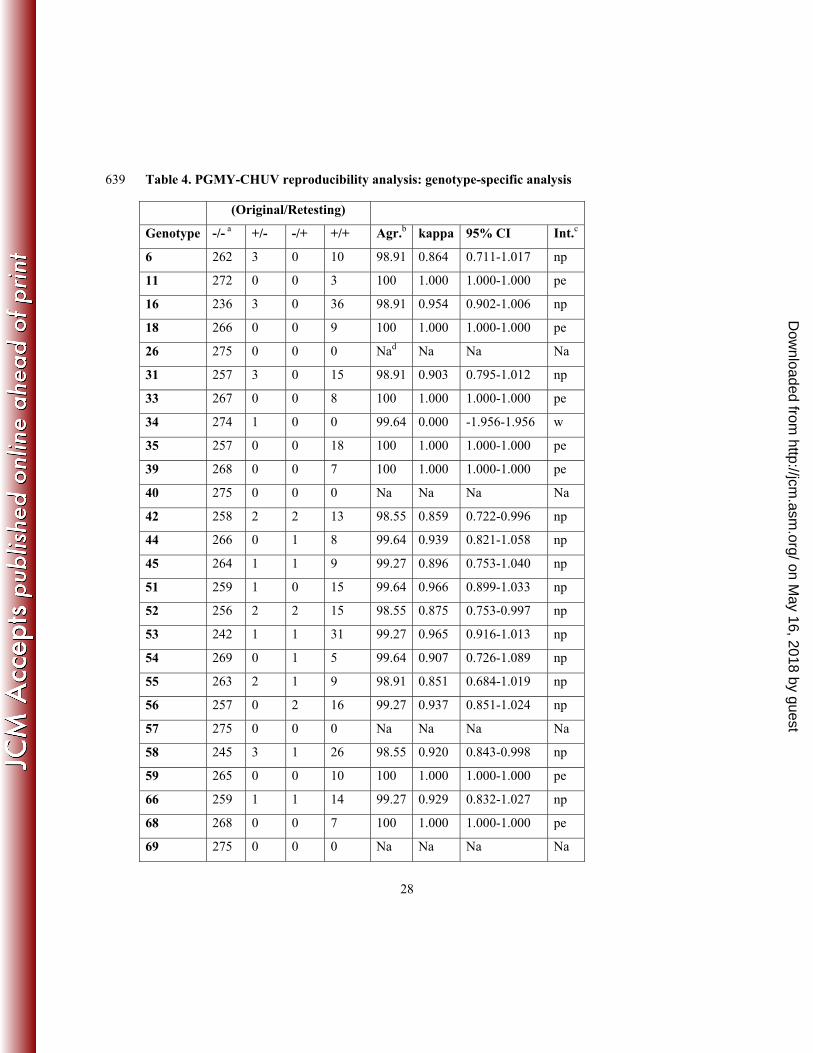
shown). Results from single and multiple infections were combined for genotype-specific analysis 323
(Table 4). Original testing identified 375 genotype-sample combinations and retesting identified 362 324
(95.3%). The global level of genotype-specific agreement reached 99.47% with a kappa value of 325
0.933 (95% CI, 0.914-0.952) interpreted as near perfect. The number of discordant cases of each 326
category was not statistically different (30 +/- vs. 17 -/+, P = 0.08, two-sided McNemar’s test). 327
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
14
Genotype-wise, kappa values were interpreted as near perfect for most genotypes but HPV82 328
(strong). The number of HPV26, 34, 40, 57 and 69 cases was insufficient for statistical analysis. 329
To assess whether discordant results were associated with genotypes representing a minor 330
fraction within each sample, they were re-evaluated taking into consideration RBH signal strength 331
as above with LA for multiple infections. For single infections, samples were considered weak by 332
the stochastic nature of PCR or by their RBH signal strength being less than the average grey value of 333
the negative control plus 8 times the standard deviation. Of the 47 discordants, 27 (57%) were 334
recorded as weak. In contrast, only 38 (11%) out of 345 concordant results were recorded as such. 335
Discordant results were therefore significantly associated with weakly-positive genotypes 336
(P < 0.0001, two-sided Fisher’s exact test), consistent with the comparison of PGMY-CHUV with 337
LA. 338
Cost evaluation 339
Cost evaluation was determined after distinguishing fixed and variable costs, and taking into 340
consideration the systematic use of at least 5 positive controls and 2 negative controls per set of 341
samples. 342
Fixed costs for PCR were estimated at 21 Swiss francs and variable costs at 0.81 Swiss francs per 343
reaction (see Materials and Methods). For PCR, a sharp cost decrease was seen as soon as several 344
samples were PCR amplified in parallel, with a plateau starting at around 16 samples (Figure 1, 345
Panel PCR costs). Sixteen samples corresponded to 24 wells of a 96 well PCR plate (16 samples 346
plus 5 positive and 2 negative controls and 1 positive control in the second row). Typical sets of 347
PCR performed in 96 well plates with either 1 (dotted line) or 2 (solid line) PCR buffers and up to a 348
maximum of 82 or 37 samples, respectively, resulted in a cost per sample of 1.21 to 2.63 Swiss 349
francs. 350
Fixed costs for RBH were estimated at 103 Swiss francs and variable costs at 27 Swiss francs per 351
hybridization run (see Materials and Methods). Filling the miniblotter was necessary to optimize 352
costs. Thus 40 lanes per hybridization were considered for the calculations presented in Figure 1 353
(Panel RBH costs). Under this condition, the cost per sample of RBH diminished strongly as soon 354
as the membrane was used more than 4 times, with a plateau starting at around 9 times. The median 355
number of membrane usage was 11 (Supplemental Material 2), well into the plateau. Therefore, the 356
median cost per sample of RBH was 0.97 to 1.94 Swiss francs depending on whether amplicons 357
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

15
from 1 (dotted line) or 2 PCR reactions (solid line), respectively, were subjected to RBH. The 358
contribution of RBH to costs was a conservative evaluation. Membrane usage more than 11 times 359
was feasible, reducing costs further. For instance, with a membrane used 29 times (Supplemental 360
Material 2, panel B), RBH cost per sample would be 0.79 to 1.57 Swiss francs depending on 361
whether amplicons from one or both PCR reactions are subjected to RBH. 362
The most expensive algorithm (duplicate PCR, two RBH per sample, median RBH usage) was 363
calculated to be 4.6 Swiss francs (5.5 US Dollars) per sample. It was used only during the 364
prospective evaluation of the effect of PCR buffer composition on genotyping (Supplemental 365
Material 3). Median cost for routine use with duplicate PCR and one RBH per sample was 366
estimated to be 3.6 Swiss francs (4.3 US Dollars). This median cost could be reduced to 2.2 Swiss 367
francs (2.6 US Dollars) with a single PCR (buffer B containing 3 mM MgCl2) and a single RBH per 368
sample. Using the membranes beyond the median usage number allowed further price reduction 369
down to a plateau close to 2 Swiss francs (2.4 US Dollars), for instance with the membrane shown 370
in Supplemental Material 2, panel B, as mentioned above. 371
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

16
DISCUSSION 372
Our data show that we were able to design an in house HPV genotyping method that compares 373
favorably with the research-grade, commercially available Linear Array assay (LA). It is 374
reproducible and cost-effective even taking into account quality control procedures. Like LA and 375
other HPV genotyping assays, PGMY-CHUV has not been validated for primary cervical cancer 376
screening according to published guidelines (23). It should therefore be used in its present format as 377
adjunct to a clinically validated screening test which identifies risk of progression to high grade 378
cervical intraepithelial neoplasia, as a follow up test to monitor patients after treatment or as an 379
epidemiological or research tool. In comparison to a similar assay based on the GP5+/6+ primers 380
(GP5+/6+-PCR EIA) (34), PGMY-CHUV relies on gel electrophoresis rather than enzyme 381
immunoassay for sorting positive samples for RBH, hence it is simpler and less expensive. 382
To confirm its adequacy for genotyping, PGMY-CHUV was compared with LA because both 383
share the same PGMY primers (17) and LA had already been thoroughly evaluated against the 384
original PGMY reverse line blot array (3, 11) and against other commercial assays with reported 385
good performance (4, 32). PGMY-CHUV agreed with LA for 81 out of 83 assay-specific single 386
infections (98%). Samples were not available for sequencing of the corresponding discordant LA 387
amplicons. It is therefore impossible to assess the specificity of LA in these 2 instances. The other 388
discordants were found in multiple infections indicating a slightly superior global sensitivity of 389
PGMY-CHUV if the combined results of both assays were used as reference. At the genotypic level, 390
higher sensitivity was significant only for HPV42 and 56 however. 391
Discordants were significantly associated with weakly-positive genotypes. This may be related 392
not only to the use of duplicate PCR reactions with PGMY-CHUV, vs. a single reaction with LA, 393
but also to a potentially limiting primer concentration established to minimize competition by 394
dominant targets. Genotyping of high risk HPVs with both assays is therefore expected to be highly 395
comparable, with discordants having only a limited impact on epidemiological studies except 396
possibly for HPV56. 397
An advantage of PGMY-CHUV over LA is the unambiguous detection of HPV52 regardless of 398
coexisting genotypes in multiple infections. The 3 samples that were HPV52 positive by PGMY-399
CHUV and negative by LA corresponded indeed to multiple infections containing HPV58 (n=2) or 400
HPV35 (n=1). The simultaneous presence of one of these two genotypes is known to interfere with 401
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

17
HPV52 detection by LA (10). Being able to detect HPV52 is important as its prevalence is high in 402
our patients population (ranks 3rd among the high risk genotypes and 5th overall, Supplemental 403
Material 5) and also in squamous cell carcinoma in Asia compared to other regions of the world (7, 404
20). PGMY-CHUV avoids the use of alternative methods like genotype-specific PCR to identify 405
HPV52 in such multiple infections. Another advantage of PGMY-CHUV is the lower number of 406
cases subjected to RBH since the procedure can be stopped after PCR for PCR-negative samples, 407
hence reducing costs further especially for studies dealing with low HPV-prevalence populations. 408
Intra-laboratory reproducibility of PGMY-CHUV was a prerequisite for its technology transfer to 409
members of the WHO HPV laboratory network. Our comparison of genotyping data performed at 410
two different time points showed a very high degree of genotype-specific reproducibility 411
(kappa=0.933) and sample full concordance (84 percent). These values are similar to those obtained 412
by Steinau and colleagues with LA (31). Discordant cases were significantly associated with weak 413
positives as seen in the comparison with LA. This is a common observation underscoring the 414
stochastic nature of PCR amplification of low starting copy number targets in the context of 415
primer/polymerase competition. 416
Five laboratories using PGMY-CHUV participated in the 2009 proficiency panel study within the 417
WHO HPV LabNet after technology transfer from our laboratory. Two were non proficient because 418
of contaminations, one was proficient at 88 percent (sensitivity issues), but used only one PCR 419
reaction with buffer A (containing 1.5 mM MgCl2) known to be less sensitive analytically than 420
buffer B (containing 3 mM MgCl2), and two were fully proficient (15). These results were not 421
different from those obtained with LA where 2 laboratories out of 4 were proficient (15). Recent 422
results of the 2010 proficiency panel showed that 4 laboratories out of 6 using PGMY-CHUV were 423
fully proficient this time, one was proficient at more than 90 percent and another was not proficient, 424
suffering from lack of sensitivity overall (13). Again, these results were not different from those 425
obtained with LA where 8 laboratories out of 17 were fully proficient (13). Successful participation 426
of several laboratories in proficiency testing confirmed therefore that PGMY-CHUV is suitable for 427
epidemiological studies with adequate sensitivity and specificity, and that it can be transferred to 428
other laboratories. We feel that these proficiency testing results reflect the ease of PGMY-CHUV 429
implementation by laboratories provided they are using PCR on a regular basis, in research as well 430
as in routine clinical testing. In comparison to commercial assays, PGMY-CHUV requires however 431
strict, additional quality control as expected for an in house assay. 432
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

18
PGMY-CHUV PCR was never associated with defects that had an impact on routine use of the 433
assay over more than 10 years in our laboratory. In contrast, PGMY-CHUV RBH was affected twice 434
by probes being cross-contaminated during synthesis. Contamination appeared more recently with 435
high automation levels and utilization of reusable devices. For this reason, we now order desalted 436
probes rather than HPLC-purified ones, and split the probe order time-wise or among different 437
manufacturers' production sites. Cross-contaminated probes were detected at delivery by our 438
membrane array quality control, underscoring its value and necessity. The quality assurance 439
program used with PGMY-CHUV is described in chapter 5 of the WHO HPV Laboratory Manual 440
(33). Additional aspects of quality assurance are also covered in chapters 3 and 6 of this manual. 441
Excluding DNA extraction (on the order of 2.2 US Dollars per sample with a commercial kit), the 442
estimated cost of performing a single genotyping under the most sensitive algorithm consisting of 443
duplicate PCR and a single RBH per sample was 4.3 US Dollars per sample. The least expensive, 444
but slightly less sensitive, yet proficient genotyping algorithm was estimated at 2.4 US Dollars per 445
sample. It consisted in processing 82 samples in parallel with a single PCR condition (buffer B 446
containing 3 mM MgCl2) and one RBH per sample. This algorithm appears well adapted to 447
epidemiological studies. DNA sequencing was not included in the cost estimates because it is not 448
essential for routine use of PGMY-CHUV owing to the high sensitivity of RBH (98.61%, 449
Supplemental Material 4, Table 2). Knowing that there were only 32 RBH-negative cases without 450
mismatches among 6703 genotype-sample combinations (Supplemental Material 4, Table 3), probe 451
sensitivity could be improved even further at more than 99.5% with updated probes currently being 452
prospectively evaluated. They target HPV subtypes affected by mismatches within probes of the 453
present version of the array (HPV45, 51, 54, 56, 58, 68 and 82 in particular). Their sequences are 454
available upon request. 455
In conclusion, we present an in-house HPV genotyping assay which is proficient for HPV 456
vaccine monitoring. With its proven transferability to other laboratories, its low cost and robustness, 457
PGMY-CHUV is a valuable method for HPV genotyping, especially in low-resource settings. 458
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
19
ACKNOWLEDGMENTS 459
Development of the assay was supported by the Institute of Microbiology of the Centre 460
Hospitalier Universitaire Vaudois, University of Lausanne, and by a grant of the Ligue Vaudoise 461
Contre le Cancer to RS. 462
The authors are especially indebted to Patty Gravitt and Janet Kornegay who provided sequences 463
of PGMY primers prior to publication in 1999. 464
We gratefully acknowledge the expert technical help of the staff of the diagnostic virology and 465
molecular diagnostic laboratories at our Institute. 466
Technology transfer within the WHO HPV LabNet was supported by WHO via a project funded 467
by the Bill and Melinda Gates Foundation that was coordinated by Tiequn Zhou (WHO). 468
Elizabeth Unger and Joakim Dillner provided helpful advice during the course of this evaluation 469
and together with the other members of the WHO HPV LabNet critically reviewed the standard 470
operating procedures provided in Chapter 5 of the WHO HPV Laboratory Manual. 471
Stefan Gerber, Phillip Shaw and Elizabeth Unger critically reviewed the manuscript. 472
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

20
REFERENCES 473
1. Altschul, S. F., W. Gish, W. M. Miller, E. W. Myers, and D. J. Lipman. 1990. Basic local 474 alignment search tool. J Mol Biol. 215:403-10. 475
2. Berkhof, J., N. W. Bulkmans, M. C. Bleeker, S. Bulk, P. J. Snijders, F. J. Voorhorst, 476 and C. J. Meijer. 2006. Human papillomavirus type-specific 18-month risk of high-grade 477 cervical intraepithelial neoplasia in women with a normal or borderline/mildly dyskaryotic 478 smear. Cancer Epidemiol Biomarkers Prev 15:1268-73. 479
3. Castle, P. E., P. E. Gravitt, D. Solomon, C. M. Wheeler, and M. Schiffman. 2008. A 480 Comparison of Linear Array and Line Blot Assay for Detection of HPV and Cervical 481 Precancer and Cancer in the ASCUS LSIL Triage Study. J Clin Microbiol 46:109-117. 482
4. Castle, P. E., C. Porras, W. G. Quint, A. C. Rodriguez, M. Schiffman, P. E. Gravitt, P. 483 Gonzalez, H. A. Katki, S. Silva, E. Freer, L. J. Van Doorn, S. Jimenez, R. Herrero, and 484 A. Hildesheim. 2008. A Comparison of Two PCR-Based Human Papillomavirus 485 Genotyping Methods. J Clin Microbiol 46:3437-3445. 486
5. Castle, P. E., M. Sadorra, F. Garcia, E. B. Holladay, and J. Kornegay. 2006. A Pilot 487 Study of a Commercialized Human Papillomavirus (HPV) Genotyping Assay: Comparison 488 of HPV Risk Group to Cytology and Histology. J Clin Microbiol 44:3915-3917. 489
6. Clavel, C., M. Masure, J. P. Bory, I. Putaud, C. Mangeonjean, M. Lorenzato, P. 490 Nazeyrollas, R. Gabriel, C. Quereux, and P. Birembaut. 2001. Human papillomavirus 491 testing in primary screening for the detection of high-grade cervical lesions: a study of 7932 492 women. Br J Cancer 84:1616-23. 493
7. Clifford, G. M., J. S. Smith, M. Plummer, N. Munoz, and S. Franceschi. 2003. Human 494 papillomavirus types in invasive cervical cancer worldwide: a meta-analysis. Br J Cancer 495 88:63-73. 496
8. Cogliano, V., R. Baan, K. Straif, Y. Grosse, B. Secretan, and F. El Ghissassi. 2005. 497 Carcinogenicity of human papillomaviruses. Lancet Oncol 6:204. 498
9. Coupe, V. M., J. van Ginkel, H. E. de Melker, P. J. Snijders, C. J. Meijer, and J. 499 Berkhof. 2009. HPV16/18 vaccination to prevent cervical cancer in The Netherlands: 500 model-based cost-effectiveness. Int J Cancer 124:970-8. 501
10. Coutlee, F., D. Rouleau, G. Ghattas, C. Hankins, S. Vezina, P. Cote, J. Macleod, A. de 502 Pokomandy, D. Money, S. Walmsley, H. Voyer, P. Brassard, and E. Franco. 2007. 503 Confirmatory Real-time PCR assay for HPV-52 infection in anogenital specimens screened 504 for HPV infection with the LINEAR ARRAY HPV Genotyping Test. J Clin Microbiol 505 45:3821-3823. 506
11. Coutlee, F., D. Rouleau, P. Petignat, G. Ghattas, J. R. Kornegay, P. Schlag, S. Boyle, C. 507 Hankins, S. Vezina, P. Cote, J. Macleod, H. Voyer, P. Forest, S. Walmsley, and E. 508 Franco. 2006. Enhanced Detection and Typing of Human Papillomavirus (HPV) DNA in 509 Anogenital Samples with PGMY Primers and the Linear Array HPV Genotyping Test. J Clin 510 Microbiol 44:1998-2006. 511
12. Cuzick, J., E. Beverley, L. Ho, G. Terry, H. Sapper, I. Mielzynska, A. Lorincz, W. K. 512 Chan, T. Krausz, and P. Soutter. 1999. HPV testing in primary screening of older women. 513 Br J Cancer 81:554-8. 514
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
21
13. Dillner, J. 2011. Technical Report of the 2010 WHO HPV LabNet Proficiency Study on 515 HPV testing and typing, available from Dr. J. Dillner, WHO HPV LabNet Global Reference 516 Laboratory, Malmö, Sweden. 517
14. Dillner, J., M. Arbyn, and L. Dillner. 2007. Translational mini-review series on vaccines: 518 Monitoring of human papillomavirus vaccination. Clin Exp Immunol 148:199-207. 519
15. Eklund, C., T. Zhou, and J. Dillner. 2010. A global proficiency study of Human 520 Papillomavirus genotyping. J Clin Microbiol 48:4147-55. 521
16. Ferguson, M., D. E. Wilkinson, and T. Zhou. 2009. WHO meeting on the standardization 522 of HPV assays and the role of the WHO HPV Laboratory Network in supporting vaccine 523 introduction held on 24-25 January 2008, Geneva, Switzerland. Vaccine 27:337-47. 524
17. Gravitt, P. E., C. L. Peyton, T. Q. Alessi, C. M. Wheeler, F. Coutlee, A. Hildesheim, M. 525 H. Schiffman, D. R. Scott, and R. J. Apple. 2000. Improved amplification of genital 526 human papillomaviruses. J Clin Microbiol 38:357-61. 527
18. Herrero, R., P. E. Castle, M. Schiffman, M. C. Bratti, A. Hildesheim, J. Morales, M. 528 Alfaro, M. E. Sherman, S. Wacholder, S. Chen, A. C. Rodriguez, and R. D. Burk. 2005. 529 Epidemiologic profile of type-specific human papillomavirus infection and cervical 530 neoplasia in guanacaste, costa rica. J Infect Dis 191:1796-807. 531
19. Hiller, T., S. Poppelreuther, F. Stubenrauch, and T. Iftner. 2006. Comparative analysis 532 of 19 genital human papillomavirus types with regard to p53 degradation, immortalization, 533 phylogeny, and epidemiologic risk classification. Cancer Epidemiol Biomarkers Prev 534 15:1262-7. 535
20. Hwang, H. S., M. Park, S. Y. Lee, K. H. Kwon, and M. G. Pang. 2004. Distribution and 536 prevalence of human papillomavirus genotypes in routine pap smear of 2,470 korean women 537 determined by DNA chip. Cancer Epidemiol Biomarkers Prev 13:2153-6. 538
21. Kjaer, S. K., K. Sigurdsson, O. E. Iversen, M. Hernandez-Avila, C. M. Wheeler, G. 539 Perez, D. R. Brown, L. A. Koutsky, E. H. Tay, P. Garcia, K. A. Ault, S. M. Garland, S. 540 Leodolter, S. E. Olsson, G. W. Tang, D. G. Ferris, J. Paavonen, M. Lehtinen, M. 541 Steben, F. X. Bosch, J. Dillner, E. A. Joura, S. Majewski, N. Munoz, E. R. Myers, L. L. 542 Villa, F. J. Taddeo, C. Roberts, A. Tadesse, J. Bryan, R. Maansson, S. Lu, S. Vuocolo, 543 T. M. Hesley, A. Saah, E. Barr, and R. M. Haupt. 2009. A pooled analysis of continued 544 prophylactic efficacy of quadrivalent human papillomavirus (Types 6/11/16/18) vaccine 545 against high-grade cervical and external genital lesions. Cancer Prev Res 2:868-78. 546
22. Kleter, B., L. J. van Doorn, L. Schrauwen, A. Molijn, S. Sastrowijoto, J. ter Schegget, J. 547 Lindeman, B. ter Harmsel, M. Burger, and W. Quint. 1999. Development and clinical 548 evaluation of a highly sensitive PCR-reverse hybridization line probe assay for detection and 549 identification of anogenital human papillomavirus. J Clin Microbiol 37:2508-17. 550
23. Meijer, C. J., J. Berkhof, P. E. Castle, A. T. Hesselink, E. L. Franco, G. Ronco, M. 551 Arbyn, F. X. Bosch, J. Cuzick, J. Dillner, D. A. Heideman, and P. J. Snijders. 2009. 552 Guidelines for human papillomavirus DNA test requirements for primary cervical cancer 553 screening in women 30 years and older. Int J Cancer 124:516-520. 554
24. Munoz, N., F. X. Bosch, S. de Sanjose, R. Herrero, X. Castellsague, K. V. Shah, P. J. 555 Snijders, and C. J. Meijer. 2003. Epidemiologic classification of human papillomavirus 556 types associated with cervical cancer. N Engl J Med 348:518-27. 557
25. Munoz, N., X. Castellsague, A. B. de Gonzalez, and L. Gissmann. 2006. Chapter 1: HPV 558 in the etiology of human cancer. Vaccine 24S3:S1-S10. 559
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

22
26. Naucler, P., W. Ryd, S. Tornberg, A. Strand, G. Wadell, B. G. Hansson, E. Rylander, 560 and J. Dillner. 2007. HPV type-specific risks of high-grade CIN during 4 years of follow-561 up: A population-based prospective study. Br J Cancer 97:129-132. 562
27. Paavonen, J., P. Naud, J. Salmeron, C. Wheeler, S. N. Chow, D. Apter, H. Kitchener, X. 563 Castellsague, J. Teixeira, S. Skinner, J. Hedrick, U. Jaisamrarn, G. Limson, S. 564 Garland, A. Szarewski, B. Romanowski, F. Aoki, T. Schwarz, W. Poppe, F. Bosch, D. 565 Jenkins, K. Hardt, T. Zahaf, D. Descamps, F. Struyf, M. Lehtinen, and G. Dubin. 2009. 566 Efficacy of human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine against cervical 567 infection and precancer caused by oncogenic HPV types (PATRICIA): final analysis of a 568 double-blind, randomised study in young women. Lancet 374:301-314. 569
28. Safaeian, M., R. Herrero, A. Hildesheim, W. Quint, E. Freer, L. J. Van Doorn, C. 570 Porras, S. Silva, P. Gonzalez, M. C. Bratti, A. C. Rodriguez, and P. Castle. 2007. 571 Comparison of the SPF10/LiPA System to the HC2 Assay for Detection of Carcinogenic 572 HPV Genotypes among 5683 Young Women in Guanacaste, Costa Rica. J Clin Microbiol 573 45:1447-54. 574
29. Schiffman, M., M. J. Khan, D. Solomon, R. Herrero, S. Wacholder, A. Hildesheim, A. 575 C. Rodriguez, M. C. Bratti, C. M. Wheeler, and R. D. Burk. 2005. A study of the impact 576 of adding HPV types to cervical cancer screening and triage tests. J Natl Cancer Inst 97:147-577 50. 578
30. Stanley, M., and L. L. Villa. 2008. Monitoring HPV vaccination. Vaccine 26 Suppl 1:A24-579 7. 580
31. Steinau, M., D. C. Swan, and E. R. Unger. 2008. Type-specific reproducibility of the 581 Roche linear array HPV genotyping test. J Clin Virol 42:412–414. 582
32. Szarewski, A., L. Ambroisine, L. Cadman, J. Austin, L. Ho, G. Terry, S. Liddle, R. 583 Dina, J. McCarthy, H. Buckley, C. Bergeron, P. Soutter, D. Lyons, and J. Cuzick. 2008. 584 Comparison of predictors for high-grade cervical intraepithelial neoplasia in women with 585 abnormal smears. Cancer Epidemiol Biomarkers Prev 17:3033-42. 586
33. Unger, E. R., J. Dillner, and T. Zhou (ed.). 2009. HUMAN PAPILLOMAVIRUS 587 LABORATORY MANUAL, 1 ed. WHO. 588
34. van Den Brule, A. J., R. Pol, N. Fransen-Daalmeijer, L. M. Schouls, C. J. Meijer, and P. 589 J. Snijders. 2002. GP5+/6+ PCR followed by Reverse Line Blot Analysis Enables Rapid 590 and High-Throughput Identification of Human Papillomavirus Genotypes. J Clin Microbiol 591 40:779-87. 592
35. van Hamont, D., M. A. van Ham, J. M. Bakkers, L. F. Massuger, and W. J. Melchers. 593 2006. Evaluation of the SPF10-INNO LiPA human papillomavirus (HPV) genotyping test 594 and the roche linear array HPV genotyping test. J Clin Microbiol 44:3122-9. 595
36. Wheeler, C. M., C. E. Greer, T. M. Becker, W. C. Hunt, S. M. Anderson, and M. M. 596 Manos. 1996. Short-term fluctuations in the detection of cervical human papillomavirus 597 DNA. Obstet Gynecol 88:261-8. 598
37. Wheeler, C. M., S. K. Kjaer, K. Sigurdsson, O. E. Iversen, M. Hernandez-Avila, G. 599 Perez, D. R. Brown, L. A. Koutsky, E. H. Tay, P. Garcia, K. A. Ault, S. M. Garland, S. 600 Leodolter, S. E. Olsson, G. W. Tang, D. G. Ferris, J. Paavonen, M. Steben, F. X. Bosch, 601 J. Dillner, E. A. Joura, R. J. Kurman, S. Majewski, N. Munoz, E. R. Myers, L. L. Villa, 602 F. J. Taddeo, C. Roberts, A. Tadesse, J. Bryan, L. C. Lupinacci, K. E. Giacoletti, M. 603 James, S. Vuocolo, T. M. Hesley, and E. Barr. 2009. The Impact of Quadrivalent Human 604 Papillomavirus (HPV; Types 6, 11, 16, and 18) L1 Virus-Like Particle Vaccine on Infection 605
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

23
and Disease Due to Oncogenic Nonvaccine HPV Types in Sexually Active Women Aged 606 16-26 Years. J Infect Dis 199:936-944. 607
38. Wilkinson, D. E., S. A. Baylis, D. Padley, A. B. Heath, M. Ferguson, S. R. Pagliusi, W. 608 G. Quint, and C. M. Wheeler. 2009. Establishment of the 1(st) world health organization 609 international standards for human papillomavirus type 16 DNA and type 18 DNA. Int J 610 Cancer 126:2969-2983. 611
612
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
24
TABLES 613
Table 1. Comparison of PGMY-CHUV and Linear Array: summary of sample results 614
according to the number of genotypes per sample 615
Genotypes per
samplea
No. of samples Full agreementb
YES (%) NO
1 83 81 (98) 2
2 44 32 (70) 12
3 30 17 (57) 13
4 7 4 (57) 3
5 11 2 (18) 9
6 2 0 (0) 2
7 3 1 (33) 2
Total 180 137 (76) 43
616 a: except for assay-specific single infections, the number of genotypes per sample was calculated 617
after combining PGMY-CHUV and LA results. 618 b: a sample was considered discordant whenever one of the genotypes represented on both arrays 619
was discordant within this sample. 620
621
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

25
Table 2. Comparison of PGMY-CHUV and Linear Array: summary of genotype-sample 622
combination results according to the number of genotypes per sample 623
Genotypes per
samplea
No. of genotype-sample
combinations b
Agreement
YES (%) NO
1 83 81 (98) 2
2 81 69 (85) 12
3 75 57 (76) 18
4 27 23 (85) 4
5 51 35 (67) 16
6 12 7 (58) 5
7 15 13 (87) 2
Total 344 285 (83) 59
624 a: except for assay-specific single infections, the number of genotypes per sample was calculated 625
after combining PGMY-CHUV and LA results. 626 b: the genotypes were restricted to those represented on both arrays. 627
628
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
26
Table 3. Comparison of PGMY-CHUV and Linear Array: genotype-specific analysis 629
PGMY-CHUV/LA
Genotypea -/-b +/- -/+ +/+ % Agr. kappa 95% CI Int.c
6 185 2 0 13 99.00 0.923 0.817-1.029 np
11 196 0 0 4 100.00 1.000 1.000-1.000 pe
16 156 3 0 41 98.50 0.955 0.905-1.006 np
18 189 0 1 10 99.50 0.950 0.852-1.048 np
26 199 0 0 1 100.00 1.000 1.000-1.000 pe
31 181 1 0 18 99.50 0.970 0.912-1.028 np
33 198 0 0 2 100.00 1.000 1.000-1.000 pe
35 196 0 1 3 99.50 0.855 0.570-1.139 np
39 193 0 0 7 100.00 1.000 1.000-1.000 pe
40 197 0 0 3 100.00 1.000 1.000-1.000 pe
*42 173 7 0 20 96.50 0.832 0.709-0.954 np
45 192 1 1 6 99.00 0.852 0.648-1.056 np
51 169 2 0 29 99.00 0.961 0.907-1.015 np
52 179 3 3 15 97.00 0.817 0.673-0.961 np
53 180 5 0 15 97.50 0.844 0.709-0.979 np
54 183 0 1 16 99.50 0.967 0.902-1.032 np
55 197 0 0 3 100.00 1.000 1.000-1.000 pe
*56 178 11 0 11 94.50 0.640 0.434-0.847 s
58 180 0 1 19 99.50 0.972 0.916-1.027 np
59 189 1 2 8 98.50 0.834 0.648-1.020 np
66 185 2 3 10 97.50 0.787 0.602-0.971 s
68 195 0 0 5 100.00 1.000 1.000-1.000 pe
69 200 0 0 0 dNa Na Na Na
70 196 1 0 3 99.50 0.855 0.570-1.139 np
73 192 0 0 8 100.00 1.000 1.000-1.000 pe
82 195 0 0 5 100.00 1.000 1.000-1.000 pe
83 193 1 1 5 99.00 0.828 0.591-1.065 np
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
27
PGMY-CHUV/LA
Genotypea -/-b +/- -/+ +/+ % Agr. kappa 95% CI Int.c
84 190 2 3 5 97.50 0.654 0.354-0.953 s
Total 5256 42 17 285 98.95 0.901 0.875-0.926 np
630
The total number of samples was 200 giving 5600 possible genotype-sample combinations. 631 a: only the 28 genotypes shared by both assays were considered for analysis 632 b: -/-: negative with both assays, -/+: PGMY-CHUV-negative and LA-positive, +/-: PGMY-633
CHUV-positive and LA-negative, +/+: positive with both assays 634 c: interpretation of the kappa values. s: strong; np: near perfect; pe: perfect 635 d: Na, not applicable 636
*: more often detected with PGMY-CHUV (P < 0.05, two-sided McNemar’s test) 637
638
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
28
Table 4. PGMY-CHUV reproducibility analysis: genotype-specific analysis 639
(Original/Retesting)
Genotype -/- a +/- -/+ +/+ Agr.b kappa 95% CI Int.c
6 262 3 0 10 98.91 0.864 0.711-1.017 np
11 272 0 0 3 100 1.000 1.000-1.000 pe
16 236 3 0 36 98.91 0.954 0.902-1.006 np
18 266 0 0 9 100 1.000 1.000-1.000 pe
26 275 0 0 0 Nad Na Na Na
31 257 3 0 15 98.91 0.903 0.795-1.012 np
33 267 0 0 8 100 1.000 1.000-1.000 pe
34 274 1 0 0 99.64 0.000 -1.956-1.956 w
35 257 0 0 18 100 1.000 1.000-1.000 pe
39 268 0 0 7 100 1.000 1.000-1.000 pe
40 275 0 0 0 Na Na Na Na
42 258 2 2 13 98.55 0.859 0.722-0.996 np
44 266 0 1 8 99.64 0.939 0.821-1.058 np
45 264 1 1 9 99.27 0.896 0.753-1.040 np
51 259 1 0 15 99.64 0.966 0.899-1.033 np
52 256 2 2 15 98.55 0.875 0.753-0.997 np
53 242 1 1 31 99.27 0.965 0.916-1.013 np
54 269 0 1 5 99.64 0.907 0.726-1.089 np
55 263 2 1 9 98.91 0.851 0.684-1.019 np
56 257 0 2 16 99.27 0.937 0.851-1.024 np
57 275 0 0 0 Na Na Na Na
58 245 3 1 26 98.55 0.920 0.843-0.998 np
59 265 0 0 10 100 1.000 1.000-1.000 pe
66 259 1 1 14 99.27 0.929 0.832-1.027 np
68 268 0 0 7 100 1.000 1.000-1.000 pe
69 275 0 0 0 Na Na Na Na
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

29
(Original/Retesting)
Genotype -/- a +/- -/+ +/+ Agr.b kappa 95% CI Int.c
70 263 1 0 11 99.64 0.955 0.866-1.043 np
73 266 1 1 7 99.27 0.871 0.693-1.049 np
82 270 0 2 3 99.27 0.747 0.397-1.097 s
83 268 2 0 5 99.27 0.830 0.595-1.065 np
84 269 0 1 5 99.64 0.907 0.726-1.089 np
Othere 242 3 0 30 98.91 0.946 0.886-1.007 np
All 8408 30 17 345 99.47 0.933 0.914-0.952 np
640
The total number of samples was 275 giving 8800 possible genotype-sample combinations. 641 a: -/-: negative on original as well as on retesting, -/+: original-negative and retesting-positive, 642
+/-: original-positive and retesting-negative, +/+: positive on original as well as on retesting 643 b: Agr., level of agreement in percent 644 c: Int: interpretation of the kappa values; pe: perfect, np: near perfect; s: strong; w: weak 645 d: Na, not applicable 646 e: other, HPV genotypes not on the probe array and considered as a single group (61, 62, 71, 647
72, 74, 81, 89, 114, HLT7474S, unknown) 648
649
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
30
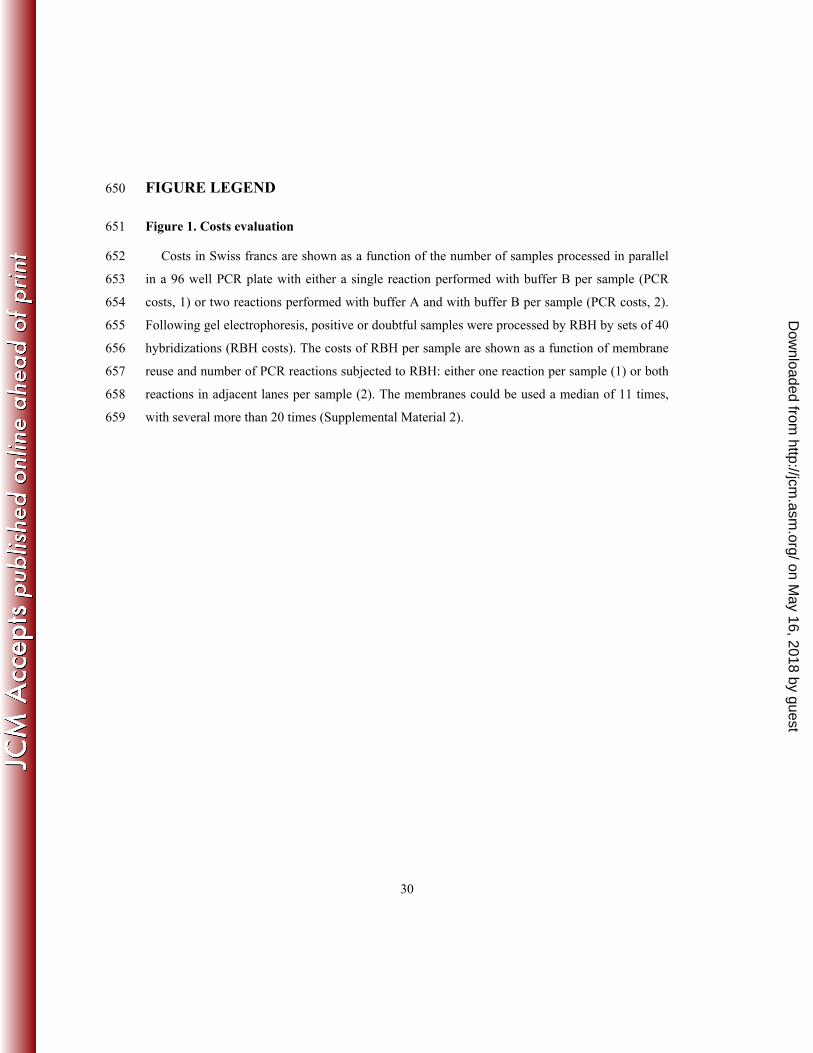
FIGURE LEGEND 650
Figure 1. Costs evaluation 651
Costs in Swiss francs are shown as a function of the number of samples processed in parallel 652
in a 96 well PCR plate with either a single reaction performed with buffer B per sample (PCR 653
costs, 1) or two reactions performed with buffer A and with buffer B per sample (PCR costs, 2). 654
Following gel electrophoresis, positive or doubtful samples were processed by RBH by sets of 40 655
hybridizations (RBH costs). The costs of RBH per sample are shown as a function of membrane 656
reuse and number of PCR reactions subjected to RBH: either one reaction per sample (1) or both 657
reactions in adjacent lanes per sample (2). The membranes could be used a median of 11 times, 658
with several more than 20 times (Supplemental Material 2). 659
on May 16, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

Figure 1
0.00
1.00
2.00
3.00
4.00
5.00
6.00
7.00
8.00
1 6 11 16 21 26 31
Cos
t per
sam
ple
in S
wiss
fra
ncs
Number of times membrane was used
RBH costs
0.002.004.006.008.00
10.0012.0014.0016.0018.0020.0022.0024.0026.0028.0030.0032.0034.00
1 13 25 37 49 61 73
Cos
t per
sam
ple i
n Sw
iss fr
ancs
Number of samples per PCR run
PCR costs
21
21 on M
ay 16, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from


















