
Vaccination of Adolescents Andrew Kroger National Center for Immunization and Respiratory Diseases...
59
Vaccination of Adolescents Andrew Kroger National Center for Immunization and Respiratory Diseases National Assembly on School-based Health Care (NASBHC)
Transcript of Vaccination of Adolescents Andrew Kroger National Center for Immunization and Respiratory Diseases...

Vaccination of Adolescents
Andrew KrogerNational Center for Immunization and
Respiratory Diseases
National Assembly on School-based Health Care (NASBHC)

Disclosure
The speaker is a U.S. government employee and has no conflict or interest with any manufacturer of products
The speaker will discuss the use of Tdap in a manner that varies from the package insert

Adolescent Vaccination

The 11-12 Year Old Visit
•The recommended age for certain vaccines
•An opportunity to catch-up on lapsed vaccinations

Adolescent VaccinesRecommended1. Tdap or Td2. Meningococcal Conjugate3. Human Papillomavirus
Catch-up1. Hepatitis B2. MMR3. Varicella4. Polio
Risk Groups1. Pneumococcal Polysaccharide2. Influenza 3. Hepatitis A 4. Meningococcal Polysaccharide

Tetanus,reduced-diphtheria, acellular pertussis vaccine

Tetanus,reduced-diphtheria, acellular pertussis vaccine

Pertussis

Pertussis Clinical Features
Stages– Incubation period – 5-10 days (21 days
rare)
– Catarrhal Stage – 1-2 weeks
– Paroxysmal Stage – 1-6 weeks (10 days rare)
– Convalescent stage – 2-3 weeks

Pertussis Clinical Features
Complications – Secondary bacterial infection pneumonia
• More often in infants < 6 months
– Seizures, otitis media, anorexia, dehydration
– Complications from actual coughing: choking, epistaxis, subdural hematoma, hernia, rib fractures, rectal prolapse

Adolescent Pertussis Vaccination Objectives
Primary– Protect vaccinated adolescents
Secondary– Reduce B. pertussis reservoir– Potentially reduce incidence of pertussis in
other age groups

Tdap Vaccines
AdacelTM (sanofi pasteur)– Licensed June, 2005– Approved for persons 11-64 years of age
Boostrix® (GlaxoSmithKline)– Licensed May, 2005– Approved for persons 10-18 years of age

General Principles for Use ofTdap and Td Among Adolescents
• Tdap products are interchangeable
• Tdap preferred to Td to provide protection against pertussis
• Licensed only for a single dose at this time
• Tdap not approved or recommended for children 7-9 years of age

ACIP Recommendations for Tdap Vaccines
• Adolescents 11-12 years of age should receive a single dose of Tdap instead of Td*
• Adolescents 13-18 years who have not received Tdap should receive a single dose of Tdap as their catch-up booster instead of Td*
*if the person has completed the recommended childhood DTaP vaccination series, and has not yet received a Td booster
*if the person has completed the recommended childhood DTaP vaccination series, and has not yet received a Td booster

• ACIP encourages adolescents who received a Td booster to receive a single dose of Tdap to provide protection against pertussis*
• A 5-year interval between the Td and Tdap is encouraged to reduce the chance of a local reaction
ACIP Recommendations for Tdap VaccinesACIP Recommendations for Tdap Vaccines
*if the person has completed the recommended childhood DTaP vaccination series*if the person has completed the recommended childhood DTaP vaccination series

Minimum Interval Between Td and Tdap
• ACIP did not define an absolute minimum interval between Td and Tdap
• Provider will need to decide based on whether the benefit of pertussis immunity outweighs the risk of a local adverse reaction

Tdap For Persons Without AHistory of DTaP
• All adolescents should have documentation of having received a series of DTAP, DTP, DT, or Td
• Persons without documentation should receive a series of 3 vaccinations
• Preferred schedule:– Single dose of Tdap*– Td at least 4 weeks after the Tdap dose– Second dose of Td at least 6 months after the Td dose
**off-label recommendationoff-label recommendation**off-label recommendationoff-label recommendation
Tdap Contraindications
• Severe allergic reaction to a vaccine component or following a prior dose
• Encephalopathy within 7 days of administration of a pertussis vaccine that is not attributable to another identifiable cause

Tdap Precautions
• History of an Arthus-type reaction following a previous dose of tetanus- or diphtheria-containing vaccine
• Progressive neurological disorder, uncontrolled epilepsy, or progressive encephalopathy
• History of Guillain-Barré syndrome (GBS) within 6 weeks after a previous dose of tetanus toxoid-containing vaccine
• Moderate or severe acute illness

Conditions NOT Precautionsfor Tdap
Following a dose of DTaP/DTP:– Temperature 105o F (40.5o C) or higher– Collapse or shock-like state– Persistent crying lasting 3 hours or longer– Convulsions with or without fever– History of an extensive limb swelling reaction

DTaP and Tdap Administration Errors
ErrorDTaP given to person >7 years
Tdap given to child <7 years as DTaP #1, 2, or 3
Tdap given to child <7 years as DTaP #4 or 5
ErrorDTaP given to person >7 years
Tdap given to child <7 years as DTaP #1, 2, or 3
Tdap given to child <7 years as DTaP #4 or 5
Action
Count dose as valid
Do not count dose; give DTaP now
Count dose as valid
Action
Count dose as valid
Do not count dose; give DTaP now
Count dose as valid

Meningococcal Conjugate Vaccine

Meningococcal Conjugate Vaccine


Meningococcal Vaccine
Recommended for:– all persons at the preadolescent visit (ages 11-
12 years)– persons about to enter high school (age 15
years)– college freshmen living in a dormitory– other adolescents who wish to reduce their risk
for meningococcal disease
MMWR 2005;54(RR-7)MMWR 2005;54(RR-7)

18-23 years old 1.4 / 100,000
18-23 years old not college student 1.4 / 100,000
Freshmen 1.9 / 100,000
Freshmen in dorm 5.1 / 100,000
Meningococcal Disease Meningococcal Disease Among Young Adults, United Among Young Adults, United
States, 1998-1999States, 1998-1999
Bruce et al, JAMA 2001;286;688-93

Meningococcal Vaccine
Recommended for certain high-risk persons:
– military recruits– certain research and laboratory personnel– travelers to and U.S. citizens residing in
countries in which N. meningitidis is hyperendemic or epidemic

Meningococcal Belt

Meningococcal Vaccine
Recommended for certain high-risk persons:
– complement component deficiency– functional or anatomic asplenia– HIV infection (“should be considered”)

Conjugate Conjugate vaccine - MCVvaccine - MCV

Meningococcal Vaccines
Menomune – ‘old’
4 types – A,C,Y,W-135
Approved for >2 yrs of age
1 dose, selective revaccination
Subcutaneous injection
Menactra – new
4 types– A,C,Y,W-135
Approved for 11-55 years of age
1 dose, (currently) no revaccination
Intramuscular injection
Meningococcal Conjugate VaccineContraindications and Precautions
Contraindications
Severe allergic reaction to vaccine component or following prior dose
Precautions
Moderate or severe acute illnessMenactra: prior history of Guillain-Barré if not extremely high risk for
meningococcal disease

MCV: Extremely High Risk
•Microbiologists routinely exposed to isolates of Neisseria meningitidis

Human Papillomavirus

Human Papillomavirus (HPV) Vaccine
A vaccine to prevent cervical cancer
Licensed for 9-26 year olds as:
Gardasil™– Merck- Quadrivalent HPV (Types 6, 11, 16, 18) L1 VLP Vaccine
Cervarix™- GlaxoSmithKline (GSK) pending licensure (Types 16 and 18)

Human Papillomavirus Vaccine

Human Papillomavirus Vaccine

HPV Prevalence: Population Estimates, U.S.
20 million people are infected 6.2 million new infections each year> 50% of sexually active men & women acquire
genital HPV infection74% of new infections occur in persons 15 – 24
years of age
W. Cates, STD April 1999, Weinstock, Perspectives on Sexual and Reproductive Health 2004, Koutsky Am J Med 1997

Human PapillomavirusHuman Papillomavirus>100 types>100 types
CutaneousCutaneous(~60 types)(~60 types)
““CommonCommon””wartswarts
((hands/hands/feet)feet)
MucosalMucosal(~(~4040 types)types)
““high-risk”high-risk”typestypes
(16,18)(16,18)
““low-risk”low-risk”typestypes (6,11)(6,11)
• low grade cervical low grade cervical abnormalitiesabnormalities
• high grade abnormalities/high grade abnormalities/ cancer precursors cancer precursors • anogenital cancersanogenital cancers
• low grade cervical low grade cervical abnormalitiesabnormalities
• genital wartsgenital warts• respiratory papillomasrespiratory papillomas

Skin Warts and Tags

Background: HPV-associated Conditions HPV types 16,
18, 6, 11
Clifford GM, BJ Ca 2003, Munoz Int J Cancer 2004; Brown J Clin Micro 1993; Carter Cancer Res 2001;Clifford Cancer Epi Biomarkers Prev 2005; Gissman Proc Natl Acad Science 1983;Kreimer Cancer Epidemiol Biomarkers Prev. 2005* All oncogenic types
HPV types 16, 18
Cervical cancer 70%
High/low grade cervical abnormalities 40%
Anal, vulvar, vaginal, penile 70%*
Head and neck cancers 10%
HPV 6, 11
Low grade cervical abnormalities 10%
Genital warts 90%
RRP 90%

Cervical Cancer Mortality Rates U.S., 1946-1984
0
2
4
6
8
10
1246 48 50 52 54 56 58 60 62 64 66 68 70 72 74 76 78 80 82 84
Year
Mo
rtal
ity
Rat
e (p
er 1
00,0
00)
Source: Program for Improving Clinical Pap Smear Programs and Management, Office of Population Affairs, DHHS, 1987.
Source: Program for Improving Clinical Pap Smear Programs and Management, Office of Population Affairs, DHHS, 1987.

Efficacy for Prevention of Clinical HPV Disease Due to HPV
6/11/16/18*
EndpointVaccine
N CasesPlacebo
N Cases Efficacy (95% CI)
HPV 16/18related CIN2/3 or AIS
8487 0 8460 53 100 (93,100)
HPV 6/11/16/18related CIN
7858 4 7861 83 95 (87, 99)
HPV 6/11/16/18related Genital warts
7897 1 7899 91 99 (94,100)
*Integrated dataset; results in the Per-Protocol Populations

Immunogenicity Bridge
Antibody Titers by Age at Enrollment Anti-HPV 6 GMTs (Quadrivalent HPV vaccine)
9 10 11 12 13 14 15 16 17 18 19 20 21 22 23Age at Enrollment (Years)
500
700
900
1100
1300
15001600
Ser
um
GM
T w
ith
95%
CI,
mM
U/m
L
Efficacy Program
Merck, unpublished data, ACIP presentation by Eliav Barr, February 2006

Potential Unintended Consequences of HPV
Vaccine– Research shows generally low levels of HPV knowledge
– Multiple influences on adolescent sexual behavior
– Fear of STD not apparent major motivation for abstinence
Increase in sexual risk unlikely

Pediatricians’ Intention to Recommend HPV Vaccine for Female and Male Patients, by
Age
0
10
20
30
40
50
60
70
80
90
100
11 year olds 14 year olds 17 year olds
% s
om
ew
hat
or
extr
em
ely
lik
ely
female
male
Kahn J et al. Journal of Adolescent Health 2005

Quadrivalent HPV Vaccine
Summary
High efficacy in 16 to 26 year-old females who are naïve to the HPV vaccine type– HPV 16,18 related CIN 2/3 – HPV 6,11,16,18 related CIN – HPV 6,11,16,18 related external genital lesions
No evidence of efficacy against disease in persons already infected with relevant type
Efficacy data available through 5; duration of protection and need for booster unknown
Safe; side effects mainly local reactions

Recommendations
Routine vaccination Catch-up vaccination Special situations Precautions and contraindications

Routine Vaccination Recommendation
ACIP recommends routine vaccination of females 11-12 years of age with three doses of quadrivalent HPV vaccine
The vaccination series can be started as young as 9 years of age

Rationale: Routine Vaccination Females at 11-12 Years
Routine– Prevalent infection, targeting ‘high risk’ groups not possible
– Modeling shows greater impact
11-12 years– Vaccination prior to sexual debut
– Implementation advantages; consistent with young adolescent health care visit
– High antibody titers after vaccination at this age
– Data through 5 years show no evidence of waning immunity; ongoing studies will monitor duration of protection

Females 13-26 Years Recommendation
Vaccination is recommended for females 13-26 years of age who have not been previously vaccinated
Ideally vaccine should be administered before onset of sexual activity, but females who are sexually active should still be vaccinated
Rationale: Vaccination of Females 13-26 Years
Females not yet sexually active can be expected to have the full benefit of vaccination
Sexually active females may not have full benefit of vaccine because they may have been infected with vaccine HPV types,
however:
– Only a small percentage are likely to have been infected with all four vaccine HPV types
– For those already infected with >1 vaccine HPV types, vaccine would provide protection against disease caused by the other vaccine HPV types
– Therefore, although overall vaccine effectiveness would be lower, most females will still derive benefit from
vaccination

Special Situations
Equivocal or abnormal Pap test
Positive HPV testGenital warts

Cervical Cancer Screening
Cervical cancer screening – no change
– 30% of cervical cancers caused by HPV types not in the quadrivalent HPV vaccine
– Vaccinated females could subsequently be infected with non-vaccine HPV types
– Sexually active females could have been infected prior to vaccination
Decision to vaccinate should not be based on Pap testing, HPV DNA testing or HPV serologic testing
Providers should education women about the importance of cervical cancer screening
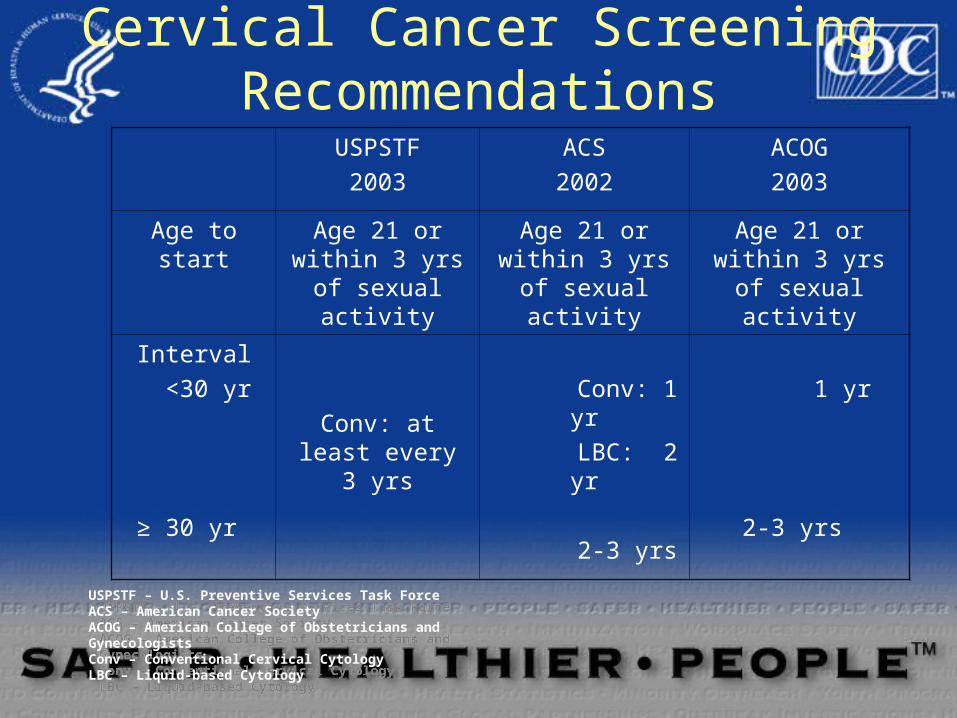
Cervical Cancer Screening Recommendations
USPSTF2003
ACS2002
ACOG2003
Age to start Age 21 or within 3 yrs of sexual activity
Age 21 or within 3 yrs of sexual activity
Age 21 or within 3 yrs of sexual
activity
Interval <30 yr
≥ 30 yr
Conv: at least every 3 yrs
Conv: 1 yr LBC: 2 yr
2-3 yrs
1 yr
2-3 yrs
USPSTF – U.S. Preventive Services Task ForceACS – American Cancer SocietyACOG – American College of Obstetricians and GynecologistsConv – Conventional Cervical CytologyLBC – Liquid-based Cytology
USPSTF – U.S. Preventive Services Task ForceACS – American Cancer SocietyACOG – American College of Obstetricians and GynecologistsConv – Conventional Cervical CytologyLBC – Liquid-based Cytology

Precautions and Contraindications
Contraindication: History of immediate hypersensitivity or severe allergic reaction to yeast or to any vaccine component
Precaution: Moderate or severe acute illnesses: should be deferred until after the illness improves

Vaccination during Pregnancy:Recommendation
Initiation of the vaccine series should be delayed until after completion of the pregnancy
If a woman is found to be pregnant after initiating the vaccination series, completion should be
delayed until after the pregnancy
If a vaccine dose has been administered during pregnancy, there is no indication for intervention


Questions?


















