Utility of Frameless Stereotaxy
10
Essam Alshail, M.B., B.S., James T. Rutka, M.D., Ph.D., James M. Drake, M.B., B.C.H., Harold J. Hoffman, M.D., Robin Humphreys, M.D., John Phillips, M.D., Michael Cusimano, M.D., Vito Forte, M.D., Blake Papsin, M.D., and Stephanie Holowka Utility of Frameless Stereotaxy in the Resection of Skull Base and Basal Cerebral Lesions in Children 29 Skull Base Surgery, Volume 8, Number 1, 1998. Divisions of Neurosurgery, Craniofacial Surgery (J.P.), Otolaryngology (V.F., B.P.), The Hos- pital For Sick Children, and St. Michael's Hospital (M.C.), The University of Toronto, Toronto, Ontario, Canada Reprint requests: Dr. Rutka, the Division of Neurosurgery, Suite 1504, The Hospital for Sick Children, 555 University Avenue, Toronto, Ontario M5G I X8, Canada. Copyright C 1998 by Thieme Medical Publishers, 333 Seventh Avenue, New York, NY 10001. All rights reserved.
Transcript of Utility of Frameless Stereotaxy

Essam Alshail, M.B., B.S., James T. Rutka, M.D., Ph.D.,James M. Drake, M.B., B.C.H.,
Harold J. Hoffman, M.D., Robin Humphreys, M.D.,John Phillips, M.D., Michael Cusimano, M.D.,
Vito Forte, M.D., Blake Papsin, M.D., andStephanie Holowka
Utility of Frameless Stereotaxy
in the Resection of Skull Base and
Basal Cerebral Lesions in Children
29
Skull Base Surgery, Volume 8, Number 1, 1998. Divisions of Neurosurgery, Craniofacial Surgery (J.P.), Otolaryngology (V.F., B.P.), The Hos-pital For Sick Children, and St. Michael's Hospital (M.C.), The University of Toronto, Toronto, Ontario, Canada Reprint requests:Dr. Rutka, the Division of Neurosurgery, Suite 1504, The Hospital for Sick Children, 555 University Avenue, Toronto, Ontario M5G IX8,Canada. Copyright C 1998 by Thieme Medical Publishers, 333 Seventh Avenue, New York, NY 10001. All rights reserved.

SKULL BASE SURGERY/VOLUME 8, NUMBER 1 1998
The ISG Viewing Wand (ISG Technologies, Mis-sasauga, ON) has been gaining in popularity amongneurosurgeons since its introduction at the beginning ofthis decade. In pediatric neurosurgery, the ISG Wand isused for tumor removal, vascular malformations,epilepsy surgery, treatment of hydrocephalus in combi-nation with endoscopy, aspiration of brain abscess, andbrain biopsy. Several reports have confirmed the accu-racy of this system in providing continuous stereotacticguidance throughout an intracranial procedure.'-6 Thissystem has also proved to be quite versatile.
A major concern with any frameless stereotaxy de-vice is the drift which occurs secondary to manipulationof a lesion which can lead to improper image guidance.In addition, rigid skull fixation is usually necessary toachieve accurate stereotactic guidance, and this may beproblematic in young children and infants.
Since 1991 we have utilized the ISG Wand at TheHospital for Sick Children in over 300 pediatric patientsfor different lesions. In this report, we review the utilityof the ISG Wand in the resection of skull base and basalcerebral lesions in order to evaluate the applicability ofthis frameless stereotactic system among this group ofpediatric patients.
CLINICAL MATERIAL AND METHODS
Patients
We identified 34 children with deep cerebral (n =21 ) or skull base lesions (n = 13) from 300 patients whounderwent nearly 325 ISG Wand directed surgical pro-cedures between 1991-1996 at The Hospital for SickChildren in Toronto. A total of 38 procedures were per-formed in this subgroup using ISG viewing Wand guid-ance.
Viewing Wand System Components
As the details of this system have been previouslyreported,2 only the essentials are provided here. TheViewing Wand consists of a mechanical articulated armwhich acts as the three-dimensional (3D digitizer), in-terfaced to a computer graphics workstation which dis-plays reformatted computed tomography (CT) and mag-netic resonance imaging (MRI) images in a variety ofconfigurations.
The Viewing Wand, manufactured by ISG Tech-nologies (Mississauga, Ontario) is comprised of the fol-lowing parts:
1. an articulated passive robotic arm (the SURGICOMmanufactured by FARO (Orlando, FL) with inter-changeable probe tips;
30 2. a Hewlett-Packard Apollo Series 710 computer;
3. a Hewlett-Packard CRX Graphics Color 19" moni-tor;
4. an uninterruptible power supply;5. input pre-processor for the arm;6. a keyboard and a mouse;7. a mounting device to the operating table or head
fixation frame;8. multiple tape drives; and9. specialized software that operate under the UNIX
System.
The system is assembled onto a mobile cabinet,which facilitates the movement of the equipment to anylocation.
Image Acquisition
CT or MRI slices are taken in an axial plane con-tiguously at 3-mm intervals. The gantry angle is slightlyreduced in order to include the nose and eyes for use aslandmarks during registration. MRI images are taken asa volume acquisition making sure that the nose and eyesare included. CT/MRI images are then transferred to themain computer where the data can be reformatted anddisplayed in three orthogonal planes. In addition to thetriorthogonal image display, an image outlying the tra-jectory of the probe tip to the lesion is routinely em-ployed prior to lesion removal. This mode is particu-larly valuable for surgical planning and intraoperativelocalization of deep seated lesions.
Stereotactic Registration
At The Hospital for Sick Children a fully dedicatedISG Wand technician attends every frameless stereotac-tic guided procedure to reduce the chances for registra-tion error and to reduce the time spent in registration. Inthe operating room the head is fixed to the operatingtable with the Sugita head frame. The articulated arm isthen rigidly attached to the head frame and to the surgi-cal table. The arm is then calibrated. The registration ofthe mechanical arm with the patient's head is initiatedusing surface landmarks such as the medial and lateralcanthal margins and the anterior tip of the tragus oneach side. These surface landmarks are then correlatedwith the same points on the three-dimensional CT/MRIsurface reconstructions of the skin. After this, over 80random surface points on the face and scalp are regis-tered with the probe allowing the computer to generate abest fit analysis of these points to the previously cap-tured CT/MRI data set. Each point is assigned an errorbased on this fit, and a root mean square error is calcu-lated.
The registration is accepted if the root mean squareerror is less than 2.5 mm. Points with a large error are

FRAMELESS STEREOTAXY IN PEDIATRIC SKULL BASE LESIONS-ALSHAIL, ET AL.
deleted to improve the overall fit. During the neurosur-gical procedure, prior to turning the bone flap, precau-tionary re-registration is carried out using four pointsaround the periphery of the craniotomy. In the event thatthe head moves with the craniotomy, these four pointscan be used to rapidly re-register the patient to theCT/MRI data. Following the craniotomy, and duralopening, the ISG wand probe is passed along the surfaceof the cerebral cortex or along the skull base until MRIimages are obtained which identify both the probe tipand the mass lesion of interest. If dissection is carriedout in the depth of the brain or skull base, correlation ofthe Wand tip with rigid anatomical structures such as theclinoid process, sella turcica, or circle of Willis, will aidthe neurosurgeon in recognizing if brain shifts have oc-curred.
ILLUSTRATIVE CASES
Case 1
A 14-year-old boy had a 2 year history of progres-sive facial asymmetry. On examination, there was leftsupraorbital prominence. The lesion was biopsied in an-other institution which confirmed the diagnosis of fi-brous dysplasia involving the frontal orbital bone. Thepatient was referred to the Hospital for Sick Childrenand CT and MRI scans were performed (Figs. IA andB). Due to ophthalmologic evidence of early visual de-terioration, the patient underwent surgical excision ofthis monostotic fibrous dysplasia. Decompression of thesuperior orbital fissure and the optic canal was per-formed using a totally extradural approach using theISG Wand. The ISG Wand was helpful in identifying theoptic nerve without the need for an intraorbital or in-tradural dissection (Fig. IC). Both the orbital roof andthe frontal bone defects were reconstructed using autol-ogous split calvarial bone grafts. His postoperativecourse was uneventful, and he has had no further deteri-oration in his vision with an excellent cosmetic result(Fig. 1D).
Case 2
This 13-year-old boy presented with an 18 monthhistory of mouth breathing. His neurological examina-tion was normal. Preoperative radiological investiga-tions showed a retropharyngeal tumor eroding theclivus which coursed posteriorly to occupy the epiduralspace compressing the high cervical spinal cord (Figs.2A-C). A transoral approach was performed to exposethis lesion. The ISG Wand was utilized to guide the ex-tent of tumor removal (Figs. 2D and E). A gross total ex-cision was achieved as confirmed by a postoperativestudy (Fig. 2F). The diagnosis was chordoma. His post-
operative course was uneventful, without neurologicaldeficit. He underwent posterior cervical fusion 10 dayspost-tumor removal using a titanium rectangle, wires,and bone graft. He received a curative dose of radiationtherapy including a stereotactic boost to the region ofthe clivus.
Case 3
This 9-year-old boy presented with a brief historyof headaches, visual loss, and progressive obtundation.On examination he had marked papilledema with abitemporal field cut. Preoperative radiological studiesshowed a large suprasellar tumor obstructing his thirdventricle causing hydrocephalus (Figs. 3A and B). Thepatient required urgent VP (venriculo peritoneal) shuntinsertion. Three days later, a subfrontal approach to thesuprasellar lesion was performed. The tumor took originfrom the undersurface of the optic chiasm. The ISGWand was utilized to identify the surrounding criticalstructures and to guide tumor removal (Fig. 3C). Asmall portion of the tumor which invaded the chiasmwas not removed (Fig. 3D). The final pathology reportwas low-grade astrocytoma. His postoperative coursewas unremarkable with no evidence of endocrinopathy.His visual acuity has gradually improved in both eyesover the past 12 months. He has received no furthertreatments and his residual tumor has been stable.
RESULT
Clinical Features of Study Population
Over 300 ISG Wand-guided procedures have beenperformed at the Hospital for Sick Children for differentcranial lesions in patients less than 22 years of age. Ofthese, 40 procedures were performed on 34 patients forskull base and basal cerebral lesions. There were 18 fe-males and 16 males with a mean age of 9.45 years and arange of 3.5 months to 22 years. There were 21 patientswith basal cerebral lesions. These lesions were distrib-uted in the thalamus (10), basal ganglia (2), third ventri-cle (2), and hypothalamus (7). The clinical features ofthese patients varied according to the site of the lesion(Table 1). The common clinical findings were headache(13), hemiparesis (10) ataxia (4) tremor (3), and preco-cious puberty (3). There were 13 patients with skullbase lesions. These lesions were found in the anteriorcranial base (3), the sella turcica (4), middle cranialbase (2), foramen magnum (2), clivus, or high cra-niocervical region (2). The most common clinical fea-tures were visual loss (14), mass (4), headache (3),panhypopituitarism (3), and breathing difficulties (2)(Table 2). 31

SKULL BASE SURGERY/VOLUME 8, NUMBER 1 1998
A J1-B
W~ ~ ~~ ~ ~ ~~~ ~ ~ ~ ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~. ..__ X._.*._
C D
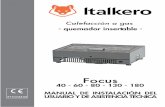
Figure 1. Fourteen-year-old boy with left orbital fibrous dysplasia. (A) Axial CT, bone windows,through the orbits showing marked fibrous dysplasia of the sphenoid wing narrowing the right opticcanal. (B) Axial Ti-weighted MRI scan through the orbits showing loss of orbital fat signal in the apicalregion of the orbit posteriorly. (C) Intra-operative ISG Wand screen save showing the approach to the de-compression of the optic can. The optic canal was unroofed in its entirety from a completely extraduralapproach. The point where the cross hairs intersect represents the tip of the ISG Wand in space, and it ispointing on the surface of the optic nerve after it was successfully decompressed. (D) Postoperative 3DCT reconstruction showing resection of fibrous dysplastic bone and reconstruction of the frontal-orbitalregion using autogenous, split-thickness bone grafts taken from the right posterior parietal region.
32

FRAMELESS STEREOTAXY IN PEDIATRIC SKULL BASE LESIONS-ALSHAIL, ET AL.
A - -;i B
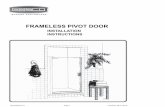
Figure 2. Thirteen-year-old boywith clival chordoma. (A) Sagittal MRI
=_ _ * QL)* showing large retropharyngeal mass le-Sion destroying the clivus and com-pressing the upper cervical spinal cord.(B) Axial MRI scan through the uppercervical region depicting the indenta-tion of the dural sac by the lesion. (C)Three-dimensional CT reconstruction of
W AAPR ~~~~~~~~~~chordoma. Left: Sagittal image clearlydemarcating bony erosion by tumor.Right: Trans-basal skull view showingrelationship of tumor to posteriorly dis-placed vertebral and basilar arteries.Figure continues on page 34.
33

SKULL BASE SURGERY/VOLUME 8, NUMBER 1
Figure 2 (Continued). (D) Dem-onstration of the intra-operative usage ofISG Wand in patient undergoing trans-oral approach to clival chordoma. Thesoft palate has been split. The ISC Wandprobe is resting on the surface of the tu-mor. (E) Intra-operative ISC Wandscreen save showing approach to clivalchordoma. The tip of the probe at thispoint in the operation is resting on thetumor to the right side of the odontoidprocess. As tumor removal proceeded,the ISC Wand was valuable in determin-ing the rostral-caudal extent of the tu-mor. (F) Postoperative MRI showing sur-gical changes in the pharyngeal tissues.The upper cervical spinal cord is nownicely decompressed. Posterior fusionwas performed using a titanium rectan-gle supplemented with bone graft 1week after the patient's chordoma was
F ~~~~~~~~~~~~~~~removed.
34
1 998

FRAMELESS STEREOTAXY IN PEDIATRIC SKULL BASE LESIONS-ALSHAIL, ET AL.
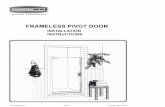
A D!JI | ' I ~~~~~~~~~~~~~11111 SiiiM M~~~~~~~~~~~~~~~~~~~~~~~~~~~._...........t|1 RFigure 3. Nine-year-old male with large optic chiasmatic glioma. (A) Axial gadolinium-enhanced MRI
showing large suprasellar tumor enveloping right middle cerebral artery. (B) Sagittal MRI showing tumor in-vaginating into third ventricle causing obstructive hydrocephalus. (C) Intra-operative ISG Wand screen saveshowing tip of probe resting on the right oculumotor nerve at the level of the cerebral peduncle, an obser-vation which was correlated directly and visually at surgery. (D) Postoperative axial MRI scan showing tu-mor resected from the suprasellar region. Tumor has been removed from around the middle cerebral arteryon the right. A small amount of residual tumor is seen in front of the brainstem.
35

SKULL BASE SURGERY/VOLUME 8, NUMBER 1 1998
Table 1. Clinical Findings Among Patients with BasalCerebral Lesions
HeadacheHemiparesisPapi loedemaAtaxiaPrecocious pubertyTremorPast historySeizureNausea/vomitingDysarthriaDiplopiaVisual lossPrecocious pubertySecondary amenorrheaAsymptomaticDecreased memoryOptic atrophySixth nerve palsyNeurofibromatosis 1
1 31094333222111111
11
Table 2. Clinical Finding Among Patients withSkull Base Lesions
Visual loss 15Mass 7Headache 3Panhypopituitarism 3Hemiparesis 2Weakness 1Precocious puberty 1Secondary amenorrhea 1Proptosis 1Nasal mass 1Hypertelorism 1
Operative Procedures
The patients with basal cerebral lesions underwenta total of 24 ISG-guided procedure (Table 3). The mostcommon neurosurgical approaches included transcal-losal (11), temporal (5), and pterional (3). Two proce-dures were performed on two patients with thalamic le-sions and one patient with a third ventricular lesion.Fourteen ISG Wand-guided procedures were performedon patients with skull base lesion (Table 4). The mostcommon approaches were transsphenoidal (3), pterional
Table 3. Surgical Approaches for Basal Cerebral LesionsTranscallosal 1 1Temporal 5Pterional 3Parietal occipital 2Frontal 1Shunt insertion 1Burr hole drainage 1Total 24
Table 4. Surgical Approaches for Basal Skull LesionsTranssphenoidal 3Pterional 2Frontal 2Transoral 2Subtemporal 1Bifrontal 1Bifrontal mid facial 1Transnasal 1Parietal temporal 1Total 14
(2), frontal (2), and transoral (2). One patient with a sel-lar tumor underwent two neurosurgical procedures: thefirst to drain a tumor cyst and the second for tumor re-moval.
Pathology and Extent of Resection
As defined in Tables 5 and 6, generally thehistopathology of the lesions in both groups of patientswas predominantly low grade. Only one patient with ahigh grade glioma was identified.
All patients underwent postoperative contrast-enhanced radiological studies to assess the degree ofsurgical resection. The ISG Wand helped the neurosur-geons to achieve a gross total resection in 10 patientswith basal cerebral and 6 patients with skull base le-sions. The degree of resection achieved in the variousprocedures is outlined in Table 7.
Table 5. Histopathological Finding Among Patients withBasal Cerebral Lesions
Astrocytoma low grade 1 0Ol igoastrocytoma 4Astrocytoma high grade 1Ependymoma 1Subependymoma 1Ganglioglioma 1Cavernous hemangioma 1Hamartoma 1Fungal abscess 1Total 21
Table 6. Histopathological Finding Among Patients withSkull Base Lesions
Astrocytoma low grade 3Craniopharyngioma 2Pituitary adenoma 2Fibrous dysplasia 2Chordoid meningioma 1Hemangioma 1Encephalocele 1Chordoma 1Total 1 3
36

FRAMELESS STEREOTAXY IN PEDIATRIC SKULL BASE LESIONS-ALSHAIL, ET AL.
25 T-
20+ inSKULL BASE
* BASAL CEREBRAL
15+
10+
Figure 4. Four patients with basalcerebral lesion had transient postopera-tive neurological complication, and sixpatients with lesions in thalamic hypo-thalamic regions had permanent motordeficit of variable degrees.
0 a
NONEUROLOGICAL
CHANGE
TRANSIENTNEUROLOGICAL
DEFICIT
PERMANENTNEUROLOGICAL
DEFICIT
Table 7. Extent of surgical resectionBasal Cerebral Skull Base
Drainage 2 1Biopsy 1 2Subtotal 11 4Gross total 10 6Decompression 1Total 24 14
Surgical Morbidity and Outcome
There was no permanent postoperative deficit inpatients with base of skull lesions. However, four pa-tients with basal cerebral lesion had transient postopera-tive neurological complication, and six patients with le-sions in thalamic hypothalamic regions had permanentmotor deficit of variable degrees (Fig. 4).
DISCUSSION
In the past decade several frameless stereotacticsystems have been introduced into neurosurgical prac-tice. These systems have revolutionized the practice ofneurosurgery and have definite advantages over frame-based stereotactic systems. Frameless stereotaxy en-ables intraoperative navigation with an accuracy of 1-2mm, but also provides continuous radiological data thatare linked to the patient." The main disadvantage of allstereotactic systems is loss of accuracy following brainshift.7 We have been using ISG Wand for 5 years in over300 cases. As such, we have eliminated most of the in-trinsic technical problems, that were identified in theearly phases of development of the ISG Wand.
The ISG Wand requires rigid fixation of the pa-tient's head to the operating table. With the Sugita headframe, we have been able to use the ISG Wand in infantsas young as 4 months of age. This has been achieved byusing six short infant pins that are gently tightened to
the scalp. Other methods to keep the head relatively im-mobile in young children or infants is to use tape or a fa-cial stocking that wraps around the Mayfield headrestwhile-the scalp and skull flaps are being raised. We havegenerally found that these procedures will provide ade-quate head stability to perform the procedure withoutencountering significant ISG Wand drift.
Several recent reports have confirmed the accuracyof the ISG Wand as an intraoperative navigational de-vice.3-9,1l Most of these reports described the use of fu-dicial marks as a method for registration rather than sur-face fit registration. However, we have utilized asurface fit registration which we have also confirmed tobe accurate.2
In pediatric neurosurgery, the ISG Wand can beused to guide the neurosurgical excision of an intra-axial brain lesion or skull base lesion,3,4,6,9 for epilepsysurgery,8 for vascular lesions such as cavernous malfor-mation,3 in combination with endoscopy for the treat-ment of a loculated ventricular system, for brain biopsy,and for aspiration of brain abscess.)0
A unique feature of skull base lesions in childrenare their benign nature and frequent attachment to boneor dural.3 These features make them ideal lesions for theapplication of frameless stereotaxy since they are at-tached to relatively immobile structures. As such, theaccuracy of targeting lesions at the skull base can re-main fixed in the 1-2 mm range, whereas with theparenchymal lesions postcraniotomy with CSF venting,brain shifts of up to 1-2 cm can occur.6 Even basal cere-bral lesions as defined here are relatively immobilecompared to more superficial cerebral lesions.
The ISG Wand is a surgical tool for framelessstereotaxy which, in our opinion, improves the confi-dence of the surgeon by providing detailed informationregarding the surgical location and the relationship tothe important neurovascular scructures. It is our impres-sion that possession of such detailed anatomical infor-mation may ultimately reduce patient morbidity.46 Ad-mittedly it is impossible to prove that the use of the
37
..M II-I

SKULL BASE SURGERY/VOLUME 8, NUMBER 1 1998
device improves surgical outcome compared to tradi-tional surgical technique, but it is difficult to conceiveof the design of a prospective controlled study in whichthe use of ISG Wand can be subjected to more rigorousanalysis. However, as a surgical tool, the ISG Wand andall frameless stereotactic devices must be judged firstand foremost by the neurosurgeon conducting the proce-dure.2 As this paper has demonstrated, we have foundthe ISG Wand to be of particular benefit for childrenwith skull base and basal cerebral lesions.
REFERENCES
1. Black P, Tarbell N, III, E, Rockoff M, and Zhan, M-S: Stereotac-tic techniques in managing pediatric brain tumors. Child NervSyst 9:343-347, 1993
2. Drake J, Prudencio J, Holowka S, Rutka J, Hoffman H, andHumphreys R: Frameless Stereotaxy in Children. Pediatr Neu-rosurg 20:125-159, 1994
3. Golfinos J, Fitzpatrick B, Smith L, and Spetzler R: Clinical useof a frameless stereotactic arm results of 325 cases. J Neuro-surg 83:197-205, 1995
4. McDermott M and Gutin P: Image-guided surgery for skull baseneoplasms using the ISG viewing wand: anatomic and techni-cal considerations. Neurosurgery Clin North Am 7:285-295,1996
5. Pollack I, Albright A, Adelson P, and Fitz C: The role of frame-less stereotactic techniques in the treatment of pediatric CNSlesions. Pediatric Neurol 13:209-216, 1995
6. Robinson J, Golfinos J, and Spetzler R: Skull base tumors: Acritical appraisal and clinical series employing image guid-ance. Neurosurg Clin North Am 297-311, 1996
7. Sipos E, Iebo S, Zinreich S, Long D, and Brem H: In vivo accu-racy testing and clinical experience with the ISG ViewingWand. Neurosurgery 39:164-204, 1996
8. Stapleton S, Kiriakopoulos E, Mikulis D, et al. Combined utilityof functional MRI, cortical mapping, and frameless stereotaxyin the resection of lesions in eloquent areas of brain in chil-dren. Pediatric Neurosurg 2:68-82, 1997
9. Kilmek L, Mbsges R, Laborde G, and Korves B: Computer-assisted image-guided surgery in pediatric skull-base proce-dures. J Pediatric Surg 30:1673-1676, 1995
10. Bucholz R, and Creco D: Image-guided surgical techniques forinfections and trauma of the central nervous system. Neuro-surg Clin North Am 7:187-200, 1996
11. Drake J, Rutka J, and Hoffman H: ISG Viewing Wand system.Neurosurgery 34:1094-1097, 1994
REVIEWER'S COMMENTS
Based on a large experience in the pioneer work and thedevelopment of frameless stereotaxy, this article focuseson skull base tumors and basal cerebral lesions in thepediatric population and describes the authors' experi-ence in such lesions. They favorably review their expe-rience and express the benefit of this technique in skullbase lesions. They highlight the distinguished advan-tages of skull base lesions in regard to frameless stereo-taxy and these are the stable bony landmark and theminimal shift of the deep basal cerebral lesion. Our ex-perience with frameless stereotaxy is identical to theirsin terms of the reliability of the intraoperative feedbackbecause of the immobile bone or dural landmark on theskull base. I think with the increasing use of this tech-nology more assertive and radical skull base tumors canbe achieved.
The authors have indicated six permanent deficitswith lesions at the basal cerebral location suggestingthat although the use of frameless stereotaxy might fa-cilitate the exposure and precise localization it mightnot change the morbidity in handling such tumors.
Ossama Al-Mefty, M.D.
38