UTI_2013 - Final
61
Urinary Tract Infections
description
uti
Transcript of UTI_2013 - Final

Urinary Tract Infections


Overview of UTI UTIs: “presence of micro organisms within the urinary tract”
May be difficult to distinguish between contamination, colonisation or infection !!
Rare in men and in children, common in females
About 2/3rds of patients are women; 40% to 50% of women have UTI at some point during their lives
Important complications of pregnancy, diabetes mellitus, polycystic disease, renal transplantation, conditions that impede urine flow (structural and neurologic)
If left untreated, simple cystitis may progress to renal scarring ie/pyelonephritis which may develop renal failure

UTI by age and sex



Classification
Based on anatomyUpper UTI (pyelonephritis)
Lower UTI ( cystitis, urethritis)Based on clinical symptoms
Asymptomatic UTISymptomatic UTI
Based on complicationUncomplicated UTI: infection involving a structurally and functionally normal urinary tract.Complicated UTI : UTI with any underlying neurologic,structural or medical problems (include UTI in male)

Definition or TermsUrinary Tract Infection :
A microbial colonization of the urine and infection of the structure of urinary tract.
Bacteriuria : the presence of the bacteria in the urineSignificant bacteriuria→ ≥ 100.000 cfu/mlFrequent recurrent→ > 4 events every year
Relaps → same organism, after eradicationRe-infection→ different organism, after eradication
Persistent is the continued infection of the same microorganism despite therapy

Definition or Terms
“Upper UTI”: infection above the level of the bladder “Lower UTI”: infection at or below the level of the
bladder “Urethral syndrome”: clinical manifestations of lower
UTI (dysuria, frequency, urgency) without significant bacteriuria
Pyuria: the presence of leukocytes]in urine, which may or may not be caused by UTI.

Frequency of significant bacteriuria
After one bladder catheterization: 2%After one bladder catheterization: 2%Medical outpatients: 5%Medical outpatients: 5%Pregnancy at term: 10%Pregnancy at term: 10%Hypertensive patients: 14%Hypertensive patients: 14%Diabetes mellitus: 20%Diabetes mellitus: 20%Women with cystocoele: 23%Women with cystocoele: 23%

Frequency of significant bacteriuria (2)
Congenital urologic disease: 57%Hydronephrosis; nephrolithiasis: 85%Indwelling catheter, open drainage >
48 hours: 98%
Jackson et al, Arch Intern Med 1962; 110: 663)

Etiology of UTI

community-acquired UTI
Aerobic gram-negative rods most oftenE. coli accounts for about 90%Staphylococcus saprophyticus has
been increasingly appreciated in recent years
Rare: anaerobes; pyogenic cocci; viruses

nosocomial UTI
E. coli is the most common pathogenHowever, also common are other
Enterobacteriacae (Proteus, Klebsiella, Enterobacter, Serratia, Providencia species) and Pseudomonadaceae (notably, Pseudomonas aeruginosa)
Enterococci: often in obstructive uropathyYeasts: Candida albicans, others

Urease-producing microorganisms
Urease splits urea into ammonia, which has a direct toxic effect on the kidney; inactivates C4, and alkalinizes the urine with production of struvite crystals (MgNH4P04.6H20) crystals
Proteus mirabilis most often; also Providencia, Morganella, S. saprophyticus, Klebsiella, Corynebacterium D2; mycoplasma

UTI in children
Newborns: overall rate is about 1% (higher in males than in females)
Preschool children: UTI is 10 to 20 times more common in girls
School-aged children: about 1.2% of schoolgirls have bacteriuria on any given day

UTI in adults
Women: bacteriuria increases with age and sexual activity
Men: bacteriuria is rare before age 50. Subsequently, bacteriuria increases with onset of prostatism

Role of bacterial virulence in UTI
Bacterial adherence to uroepithelial cells involves specific binding of bacterial surface receptors (adhesins) to complementary components on the epithelial cells (receptors).
The ability of E. coli to adhere to uroepithelial cells is associated with the presence of pili or fimbriae.
Virulence of E. coli strains multiple factors, including adhesins, hemolysin, capsular polysaccharide, aerobactin).



Host defenses

Antibacterial properties of urine
Osmolality (extremes of high or low osmolalities inhibit bacterial growth)
High urea concentrationHigh organic acid concentrationpH

Anti-adherence mechanisms
Bacterial interference (naturally endogenous bacteria in the urethra, vagina, and periurethral region)
Urinary oligosaccharides (have the potential to detach epithelial-bound E. coli
Tamm-Horsfall protein (uromucoid): coating of E. coli by this protein might prevent attachment

MiscellaneousMucopolysaccharide lining of the
bladderUrinary immunoglobulinsSpontaneous exfoliation of uroepithelial
cells with bacterial detachmentMechanical flushing of micturition

Mechanisms of UTI

Pathway Of Renal InfectionPathway Of Renal Infection
ASCENDING INFECTION
Common agents :• E.coli• Proteus• Enterobacter
ASCENDING INFECTION
Common agents :• E.coli• Proteus• Enterobacter
Bacterial colonizationBacterial colonization
Bacteria enter bladderBacteria enter bladder
Deranged vesicoureteral junctionDeranged vesicoureteral junction
Vesicoureteral refluxVesicoureteral reflux
Intrarenal refluxIntrarenal reflux
AORTAAORTABacteremiaBacteremia
HEMATOGENOUS INFECTION
Common agents :• Staphylococcus• E.coli
HEMATOGENOUS INFECTION
Common agents :• Staphylococcus• E.coli

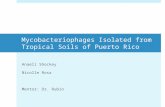
PATHOGENESIS
Gut floraGut flora
UropathogensUropathogens
Colonization Colonization
Barrier normal mucosaBarrier normal mucosa
CystitisCystitisBACTERIA VIRULENCEBACTERIA VIRULENCE HOST’S IMMUNE DEFENCE HOST’S IMMUNE DEFENCE
1. VUR1. VUR
2. Intrarenal Reflux2. Intrarenal Reflux 33. Urinary tract . Urinary tract obstructionobstruction 4. Foreign bodies (cateter )4. Foreign bodies (cateter )
Acute PyelonephritisAcute Pyelonephritis
scarringscarring UrosepsisUrosepsis
AscendingAscending
1. P-fimbrie2. O & K serotype3. Haemolicine4. Colistine V5. Aerobactin6. Bactericidal action resistant

Mechanisms of lower UTI
Experimentally, 99.9% of a bladder inoculum of bacteria is promptly excreted by voiding.
Deficient antibodies in vaginal secretions; and biochemical differences in receptors on uroepithelial cells.

Mechanisms of upper UTI
Ascent of bacteria from the bladder to the kidneys is promoted by obstruction and by reflux.
In addition, motile bacteria can ascend against the flow of a column of urine. Gram-negative bacteria (or endotoxin derived from them) can inhibit ureteral peristalsis.

Localization: upper vs. lower
Indirect: pattern of recurrence (i.e., same organism?); maximum urinary concentration; water loading test; serum antibodies; cellular excretion; urinary proteins
Direct: renal biopsy; ureteral catheterization; antibody-coated bacteria test

Localization: upper vs. lower (in practice)
Frequency, dysuria, and urgency lower UTI symptoms.. sometime can occur with upper UTI as well.
Fever and flank pain acute upper urinary tract infection.
Scarring of the kidney by imaging procedures suggests chronic UTI.
The distinction is sometimes difficult.

Acute cystitis
Characterized by sudden onset, multiple urinary symptoms, pyuria, and sometimes hematuria (uncommon)
Acute dysuria in young women usually indicates: acute bacterial cystitis; the urethral syndrome; or vaginitis
Causes: E. coli (80%), S. saprophyticus (10% to 15%), and occasionally Klebsiella, Proteus mirabilis, and other microorganisms

Acute uncomplicated pyelonephritis
Largely a clinical diagnosis Pyuria is usually present; about 20% have
positive blood cultures; causative organisms the same as with cystitis
Predisposing factors: structural abnormalities; strains of E. coli with unique markers; genetically-determined carbohydrate receptors on uroepithelial cells

Recurrent UTIs in women
Between 20% and 25% of young women with acute uncomplicated cystitis have 2 or more infections per year,
Usually due to reinfection with a different E. coli strain
Predisposing factors: genetically-determined receptors on uroepithelial cells.

Complicated UTIs
Definition: UTI in patients with predisposing anatomic, functional, or metabolic abnormalities
Spectrum of organisms is skewed toward difficult-to-treat pathogens (e.g., Pseudomonas sp., yeasts, enterococci, Enterobacteriaceae other than E. coli)

Catheter-associated UTI
Risk factors: female sex; duration of catheterization; disconnecting the junction between the catheter and the collecting tube


Long-term bladder catheterization
Incidence of significant bacteriuria in patients who are not receiving antibiotics is 8% to 10% per day
More than 85% of patients have at least two strains of bacteria and 10% have more than five strains
Some species (notably, enterococci, Pseudomonas, and Proteus) notoriously tend to persist

Prostatitis
Relapsing acute urinary tract infection in men caused by the same bacterial species often suggests chronic prostatitis with periodic spill-over into the bladder
Symptoms: pelvic “heaviness,” rectal or perineal pain, urinary hesitancy, dribbling, and burning
A risk of catheterization

DIAGNOSIS

Diagnosis of UTI
History Physical exam (PE) Lab
UrinalysisUrine cultureSensitivity
Imaging study

Clinical Presentation
Suprapubic pain, pain or burning during urination
↑ frequency and urgency of urination Dysuria Nocturia Hematuria Cloudy urine Foul or strong urine odor Upper: fever, chills, malaise, N/V, weight loss,
flank or back pain

Costovertebral angle (CVA) tenderness Abdominal tenderness or mass Palpable bladder Dribbling, poor stream, or straining to void Examine the pelvic & vaginal area in women for
signs of irritation, vaginitis, trauma, or sexual abuse.
Men require a digital rectal examination to determine if prostate enlargement is present
History and Physical Examination

UrinalysisBacteriuria : bacteria identified on culture
Significant bacteriuria :
bacteria > 100.000 colony /ml fresh urine
↓
Gold standard diagnostic UTI
Urine collection
Diagnosis of UTI

Diagnosis of UTI
• Determination of the number and type of bacteria important diagnostic procedure.
• Symptomatic– ≥ 105 CFU bacteria/ml
• Asymptomatic– ≥ 105 CFU bacteria/ml on 2 consecutive specimens
• Catheterized patients– ≥ 102 CFU bacteria/ml
• antibiotic, high urea concentration, high osmolarity, low pH inhibits bacterial multiplication low bacterial colony counts

Urinalysis Valuable clues for an accurate diagnosis:
- Color and cloudiness of urine - Acidity - White blood cells (leukocytes).
Treatment can be started without the need for further tests if the following urinalysis results are present in patients with symptoms and signs of UTIs: - A high white cell count - Cloudy urine

UrinalysisParameter Normal values UTI
Appearance Yellow Cloudy
pH 4.5-8.5 Alkaline
Protein Negative Positive
Nitrite test Negative Positive
RBC Negative Positive
WBC 0-5 / hpf > 5 / hpf
Cast Negative Positive
Bacteria Absent Many present

White blood cell casts
Highly
significant!
Presence
suggests
pyelonephritis

Treatment

General Principles of treatment
1. Except in acute uncomplicated cystitis in women, a urine culture, a Gram stain, or an alternative rapid diagnostic test should be performed to confirm infection before treatment is begun.
2. Factors predisposing should be identified and corrected.
3. Relief of clinical symptoms ≠ bacteriologic cure.
4. Each course of treatment failure or cure.
5. In general, lower tract short courses, upper tract longer.
6. community-acquired infections antibiotic-sensitive strains.
7. In patients with repeated infections, instrumentation, or recent hospitalization antibiotic-resistant strains should be suspected.

Goals of Therapy
Prevent or treat systemic consequences
Relieve symptoms
Eradicate invading organism
Eliminate uropathogenic bacterial strains from fecal & vaginal reservoirs
Prevent reoccurrence of infection
Prevent long-term sequelae

Antimicrobial Selection
Empiric Therapy - based on most probable pathogens - local rates of resistance - acute infection vs chronic - reinfection or relapse - indwelling catheter etc
Good urine concentration Minimal effects on fecal and vaginal flora Acceptable safety profile Cost-effective

Antimicrobial Therapy
Cystitis - usually responds to 3 days of treatment
- effective concentrations into the urine > serum
uncomplicated pyelonephritis - 2 weeks treatment
- effective concentrations into the urine = serum
complicated infections / prostatitis - 6 weeks
IV antibiotics may be required in seriously ill
patients, but oral drugs usually effective

Antimicrobial Therapy
Acute Uncomplicated cystitis– Trimethoprim/sulfamethoxazole (TMP/SMX)
1 DS (160/800 mg) BID x 3 days– Fluoroquinolones:
Ciprofloxacin 250 mg BID x 3 daysLevofloxacin 250mg QD x 3 daysGatifloxacin 200 mg QD x 3 days
– Nitrofurantoin: 100 mg QD x 3 days– Cephalosporins, doxycycline, amoxicillin/clavulanate

Acute pyelonephritis– Duration on therapy= 7-14 days– TMP/SMX
1 DS (160/800 mg) BID x 14 days– Fluoroquinolone
Ciprofloxacin 500 mg BID x 14 daysLevofloxacin 250mg QD x 14 daysGatifloxacin 250 mg QDx 14 days
– Cephalosporins, doxycycline, amoxicillin/clavulanate– For more seriously ill patients → IV therapy
Antimicrobial Therapy

UTI in Pregnancy should be screened for UTIs high risk for UTIs and
their complications. Asymptomatic bacteriuria have a 30% risk for acute
PN short course of antibiotics (3 to 5 days). Uncomplicated UTI need longer-term antibiotics (7
to 10 days). Sulfonamides, nitrofurantoin, ampicillin, cephalexin
safe in early pregnancy Avoid: sulfonamides (near term kern icterus ), TMP
(toxic effects in the fetus at high doses), fluoroquinolone (fetal cartilage development),


UTI in Men Uncommon in younger than 50 years Older than 50 years assumed from prostate or kidney Recurrent infection sustained focus within the prostate Difficulty of eradication of prostatic foci
- failure antimicrobial diffuse into the prostatic gland
- prostate may harbor calculi block drainage or act as a foreign bodies
- enlarged & inflamed bladder outlet obstruction Intensive therapy: at least 4-6 weeks with TMP/SMX, fluoroquinolones Failure treatment:
- Anatomic factors
- Infection due to E. faecalis or P. aeruginosa Treatment relapse Long term antimicrobial suppression, repeated
treatment courses for each relapse and surgical removal of infected prostate gland

Adults
The prognosis for most women with cystitis and pyelonephritis is good; about 25% of women with cystitis will experience a recurrence.
The prognosis for emphysematous pyelonephritis is not as good and is discussed in Special Concerns.
Infected cysts in polycystic kidney disease respond to treatment slowly.
Prognosis

ChildrenChildren In industrialized countries, kidney damage with long-In industrialized countries, kidney damage with long-
term complications as a consequence of urinary tract term complications as a consequence of urinary tract infection per se is currently less common than in the infection per se is currently less common than in the early 20th century, when pyelonephritis was a early 20th century, when pyelonephritis was a frequent cause of hypertension and ESRD in young frequent cause of hypertension and ESRD in young womenwomen
This change is probably a result of improved overall This change is probably a result of improved overall healthcare and close follow-up of children after an healthcare and close follow-up of children after an episode of pyelonephritis. episode of pyelonephritis.
Prognosis