Utah’s Pre-paid, Capitated Behavioral Health Medicaid Plan NACBHDD Legislative Conference,...
12
Utah’s Pre-paid, Capitated Behavioral Health Medicaid Plan NACBHDD Legislative Conference, Washington, D.C. March 4, 2013 Kyle Snow, ED, Northeastern Counseling Center, [email protected] Mike Deal, ED, Southwest Behavioral Health, [email protected] Pat Fleming, DD, SLCo Div. Behavioral Health Services, [email protected]
-
Upload
christine-talton -
Category
Documents
-
view
212 -
download
0
Transcript of Utah’s Pre-paid, Capitated Behavioral Health Medicaid Plan NACBHDD Legislative Conference,...

Utah’s Pre-paid, Capitated Behavioral Health Medicaid Plan
NACBHDD Legislative Conference, Washington, D.C.
March 4, 2013
Kyle Snow, ED, Northeastern Counseling Center, [email protected] Deal, ED, Southwest Behavioral Health, [email protected] Fleming, DD, SLCo Div. Behavioral Health Services, [email protected]

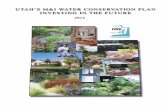
1980’s-90
State Level Reorganizati
on“Genesis”
Community Mental Health
Movement Took Firm
Hold
Followed by the Expansion of Grant
Funding for Community SUD Svc’s and Svc’s
For Older Americans
Counties
Human Service
sAging
Services
MH & SUD
Services
Child WelfareDisability ServicesJuvenile Justice Services
Child Welfare
DisabilityServices
Juvenile JusticeServicesSTATE
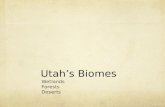
Utah began adding optional services to it’s Medicaid plan, including MH Svc’s to the disabled populations…inpatient psychiatric services were covered…
Overbuild of psychiatric facilities -
costs skyrocket
Counties given
responsibility to manage optional Medicaid
Program & inpatient
costs
Cost savings to be used to expand MH Svcs (Medicaid & Unfunded/uninsured)
1993
Utah’s Capitated MH Plan was born - with almost full coverage across 13 Co
MH Authorities by
1996
1996 – 2004 Worked exactly as designed, inpatient costs under control, allowed counties to expand while
decreasing demand on State funds. It worked too well. 2006 – CMS changes, savings to be used for Medicaid only.

Three Common Financing Methods1. Cost reimbursement model2. Fee-for-service model3. Capitated model

Capitation Model – What is it?
• Under this model, payer or providers, receive a fee for each enrollee to cover a specified level of behavioral health care and offer a defined package of services, for a specified period of time. The enrollees are usually residents of a specific area. Enrollee may be identified from a specific list. Payer or provider assumes risk (all risk, shares risk, limit risk share, etc.), associated with delivering services to enrollees.

When to use Capitation Model
• When behavioral health expenditures growing faster than available funding.
• When acute behavioral costs (inpatient care) growing more rapidly than the outpatient or traditional behavioral health expenditures.
• When available funding is being reduced or no growth in funding is being projected within the near future.
• When coordination of benefits of patient between different providers is not being done or very limited.
• When provider network is providing unnecessary services or keeping patients in higher levels of care longer than needed.

How Do You Determine Enrollee Rates
• Need to know total units of service provided by service code.
• Need to know Medicaid units of service provided by service code.
• Need to know cost by service code.• Need to know Medicaid units of service by service code
and by rate cell.• Need to know Third Party Liability or insurance collection
by Medicaid rate cell.• Need to know the number of eligibles by rate cell or
category.

How Many Eligible or Rate Cells to Use?
State of Utah’s 10 Eligibility Categories
1. AFDC 0 to Age 5 Years2. AFDC 6 to 18 Years3. AFDC 19 to 64 Years4. Aged (65 Years and Older)5. Disabled Male (All Ages)6. Disabled Female (All Ages)7. Pregnant Woman (All Ages)8. Medically Needy Child (0 to 18
Years)9. Medically Need Adults (19 to 64
Years)10.Foster Care
State of Utah has over 130 eligibility categories. Each based up a set of criteria submitted to CMS (Centers for Medicare and Medicaid Services). Too many to use!!!!! Utah has chosen to collapse all these into 10 categories.

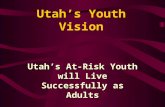
Example of Monthly Payment Capitation
• Utah uses a prepaid full capitation prepaid model. Under this model, the govt. agency, MCO, Providers and etc. receives a fixed amount of money for providing services to a patient for a particular period of time, including all the cost associated with behavioral health. (Inpatient hospital, outpatient, supported living, and other services - pharmacy is not included.) Prepayment allows agency a chance to contract for all services, staff for services and etc., without having to acquire large loans, or restrict prior years earning, to cover cost of providing the service.
ROW TITLES Pay BIRTH 6 THROUGH NON- DISABLED DISABLED TOTALS Date THROUGH 18 YEARS TRADITIONAL MALE FEMALE 5 YEARS ADULTS (ALL AGES) (ALL AGES)
Current Month Eligibles First October 1, 2012 325 700 490 82 95 1,692Rates for Year $ 12.83 $ 13.04 $ 25.22 $ 193.37 $ 190.85 Amount of First Check $ 4,169.56 $ 9,129.19 $ 12,359.07 $ 15,856.64 $ 18,131.20 $ 59,645.68 New Eligibles for Month October 8, 2012 40 80 30 16 16 182Rates for Year $ 12.83 $ 13.04 $ 25.22 $ 193.37 $ 190.85 Amount of Second Check $ 513.18 $ 1,043.34 $ 756.68 $ 3,093.98 $ 3,053.68 $ 8,460.85 New Eligibles for Month October 15, 2012 22 10 15 14 15 76Rates for Year $ 12.83 $ 13.04 $ 25.22 $ 193.37 $ 190.85 Amount of Third Check $ 282.25 $ 130.42 $ 378.34 $ 2,707.23 $ 2,862.82 $ 6,361.06 New Eligibles for Month October 22, 2012 10 6 11 11 15 53Rates for Year $ 12.83 $ 13.04 $ 25.22 $ 193.37 $ 190.85 Amount of Fourth Check $ 128.29 $ 78.25 $ 277.45 $ 2,127.11 $ 2,862.82 $ 5,473.93 New Eligibles for Month October 22, 2012 3 4 4 10 5 26
Rates for Year $ 12.83 $ 13.04 $ 25.22 $ 193.37 $ 190.85
Amount of Fifth Check $ 38.49 $ 52.17 $ 100.89 $ 1,933.74 $ 954.27 $ 3,079.56
Total for Month $ 5,131.77 $ 10,433.36 $ 13,872.43 $ 25,718.70 $ 27,864.80 $ 83,021.06

Advantages of Capitation• Strong incentives to minimize financial costs.• Strong incentive to intervene earlier in patient’s
treatment rather that waiting until clients admit at inpatient hospital.
• Strong incentive to coordinate patient’s care between programs and providers.
• Patient is likely to receive only those services and interventions that are necessary.
• Limits the chances of exceeding the budget that has been approved.
• Encourages the use of new programs that limit the exposure to the more intensive services such as inpatient.

Disadvantages of Capitation • Agencies, providers, MCOs, and etc., (providers) have an
incentive to limit the quantity of services provided to the patient.
• Patients may potentially receive less than optimal care since both quality and quantity may increase costs.
• In capitation-based settings, it is not as easy and straightforward for the patient to change her therapist.
• Providers may limit the days in intensive care to less than optimal before releasing back to the community to reduce cost, thus placing family, the new provider and the patient at greater risk.
• Agency overseeing capitation contract may incur additional costs for monitoring to ensure appropriate levels and quality of care are provided to the patients.

So which of the three methods is the best, cost reimbursement, fee-for-service, or capitation?
• At Salt Lake County we use all three methods. Each has as mentioned advantages and disadvantages.
• We use the cost reimbursement for new programs and programs looking for a particular usually non traditional service. (24 Crisis line)
• We use fee-for-service with our substance abuse providers with a ceiling on the max dollars allowed per year. The monthly amount is limited to allow for services throughout the year.
• On our mental health services both inpatient and outpatient we have placed our MCO contractor at full risk with reimbursement based upon the enrollment of eligibles in the 10 categories mentioned. But we added an additional aspect with our MCO any unspent funding will be deposit into an account maintained by our MCO, but belonging to Salt Lake County. These funds have been used to open new programs and cover shortfall in the falling year.