Use of plasma DNA in detection of loss of heterozygosity in patients with multiple myeloma
5
Use of plasma DNA in detection of loss of heterozygosity in patients with multiple myeloma Multiple myeloma (MM) is a malignant tumor of somatically mutated plasma cells (PCs). MM pro- gresses within the bone marrow (BM), frequently in patchy fashion and then to an extramedullary stage (1). Important prognostic factors in MM are stage of disease, beta-2 microglobulin (b2-M), C-reactive protein serum levels (1), proliferative activity of PCs (labeling index or proportion of S-phase PCs) (2, 3), and cytogenetics (4). Deletion of the long arm of chromosomes 13 and 11, and monosomy of these chromosomes are commonly described in MM PCs by conventional metaphase analysis (5), comparative genomic hybridization (6), and meta- phase fluorescence in situ hybridization (FISH) (7). Most recently, chromosomal abnormalities emerged as a major independent parameter pre- dicting the outcome of patients with MM. Specif- ically, poor responses to chemotherapy and short survival have been demonstrated in patients with MM, and deletions of 13q and 11q (8, 9). Being a hypoproliferative malignancy, MM yields inform- ative metaphase karyotyping in no more than 30% of newly diagnosed cases (5, 10). The patchy distribution of PCs and the poor yield in cyto- genetic examination may lead to underestimation of the cytogenetic abnormalities. Ahmed M, Giles F, Joe Y, Weber DM, Jilani I, Manshouri T, Giralt S, De Lima M, Keating M, Albitar M. Use of plasma DNA in detection of loss of heterozygosity in patients with multiple myeloma. Eur J Haematol 2003: 71: 174–178. Ó Blackwell Munksgaard 2003. Abstract: Background: Deletions or structural abnormalities in chro- mosomes 11 and 13 have been shown to be important in predicting clinical behavior in patients with multiple myeloma (MM). However, cytogenetic analysis in MM is frequently difficult because of poor yield of informative metaphases and the disease is frequently patchy, which complicates fluorescent in situ hybridization studies. Objectives: The purpose of this study was to explore the potential of using peripheral plasma DNA for the detection of loss of heterozygosity (LOH) in chromosomes 11 and 13 in patients with MM. Methods: Peripheral blood (PB) plasma of 81 patients with MM, was used as a source of DNA for the detection of LOH at chromosomes 13q14 (D13S319 and D13AFMaw301wb5), and 11q21 (D11S2179) using polymerase chain reaction. Results: Only 62 of the studied patients were informative for the two 13q microsatellite markers and 16 (26%) of these patients showed LOH. Only seven (11%) of 61 patients with informative D11S2179 microsatellite maker showed LOH. Purified plasma cells (PCs) from six bone marrow (BM) samples using anti-CD138-coated magnetic beads showed identical results to those detected in DNA iso- lated from PB plasma. Three patients with LOH underwent autologous BM transplantation, and two of three reverted to a normal state (no LOH) after transplantation. Seven of the patients with 13q LOH in PB plasma had <10% PCs (PCs) in their BM at the time of testing. Con- clusion: PB plasma appears to be enriched by tumor-specific DNA and can be used to detect chromosomal abnormalities in patients with MM. Further studies are needed to establish the clinical relevance of this approach in comparison with other techniques. Maha Ahmed 1 , Francis Giles 2 , Youngson Joe 1 , Donna M. Weber 3 , Iman Jilani 1 , Taghi Manshouri 1 , Sergio Giralt 4 , Marcos De Lima 4 , Michael Keating 2 , Maher Albitar 1 Departments of 1 Hematopathology, 2 Leukemia, 3 Myeloma, and 4 Blood and Marrow Transplantation, M.D. Anderson Cancer Center, The University of Texas, Houston, TX, USA Key words: polymerase chain reaction; microsatellite markers; plasma; myeloma; 13q; 11q; loss of heterozygosity Correspondence: Maher Albitar MD, Department of Hematopathology, M.D. Anderson Cancer Center, The University of Texas, 1515 Holcombe Boulevard, Box 72 Houston, TX 77030-4095, USA Tel: (713) 794-1292 Fax: (713) 794-1800 e-mail: [email protected] Accepted for publication 19 June 2003 Eur J Haematol 2003: 71: 174–178 Printed in UK. All rights reserved Copyright Ó Blackwell Munksgaard 2003 EUROPEAN JOURNAL OF HAEMATOLOGY ISSN 0902-4441 174
-
Upload
maha-ahmed -
Category
Documents
-
view
212 -
download
0
Transcript of Use of plasma DNA in detection of loss of heterozygosity in patients with multiple myeloma

Use of plasma DNA in detection of loss ofheterozygosity in patients with multiplemyeloma
Multiple myeloma (MM) is a malignant tumor ofsomatically mutated plasma cells (PCs). MM pro-gresses within the bone marrow (BM), frequently inpatchy fashion and then to an extramedullary stage(1). Important prognostic factors in MM are stageof disease, beta-2 microglobulin (b2-M), C-reactiveprotein serum levels (1), proliferative activity ofPCs (labeling index or proportion of S-phase PCs)(2, 3), and cytogenetics (4). Deletion of the longarm of chromosomes 13 and 11, and monosomy ofthese chromosomes are commonly described inMM PCs by conventional metaphase analysis (5),comparative genomic hybridization (6), and meta-
phase fluorescence in situ hybridization (FISH)(7). Most recently, chromosomal abnormalitiesemerged as a major independent parameter pre-dicting the outcome of patients with MM. Specif-ically, poor responses to chemotherapy and shortsurvival have been demonstrated in patients withMM, and deletions of 13q and 11q (8, 9). Being ahypoproliferative malignancy, MM yields inform-ative metaphase karyotyping in no more than 30%of newly diagnosed cases (5, 10). The patchydistribution of PCs and the poor yield in cyto-genetic examination may lead to underestimationof the cytogenetic abnormalities.
Ahmed M, Giles F, Joe Y, Weber DM, Jilani I, Manshouri T, Giralt S,De Lima M, Keating M, Albitar M. Use of plasma DNA in detection ofloss of heterozygosity in patients with multiple myeloma.Eur J Haematol 2003: 71: 174–178. � Blackwell Munksgaard 2003.
Abstract: Background: Deletions or structural abnormalities in chro-mosomes 11 and 13 have been shown to be important in predictingclinical behavior in patients with multiple myeloma (MM). However,cytogenetic analysis in MM is frequently difficult because of poor yieldof informative metaphases and the disease is frequently patchy, whichcomplicates fluorescent in situ hybridization studies. Objectives: Thepurpose of this study was to explore the potential of using peripheralplasma DNA for the detection of loss of heterozygosity (LOH) inchromosomes 11 and 13 in patients with MM. Methods: Peripheralblood (PB) plasma of 81 patients with MM, was used as a source ofDNA for the detection of LOH at chromosomes 13q14 (D13S319 andD13AFMaw301wb5), and 11q21 (D11S2179) using polymerase chainreaction. Results: Only 62 of the studied patients were informative forthe two 13q microsatellite markers and 16 (26%) of these patientsshowed LOH. Only seven (11%) of 61 patients with informativeD11S2179 microsatellite maker showed LOH. Purified plasma cells(PCs) from six bone marrow (BM) samples using anti-CD138-coatedmagnetic beads showed identical results to those detected in DNA iso-lated from PB plasma. Three patients with LOH underwent autologousBM transplantation, and two of three reverted to a normal state (noLOH) after transplantation. Seven of the patients with 13q LOH in PBplasma had <10% PCs (PCs) in their BM at the time of testing. Con-clusion: PB plasma appears to be enriched by tumor-specific DNA andcan be used to detect chromosomal abnormalities in patients with MM.Further studies are needed to establish the clinical relevance of thisapproach in comparison with other techniques.
Maha Ahmed1, Francis Giles2,Youngson Joe1, Donna M. Weber3,Iman Jilani1, Taghi Manshouri1,Sergio Giralt4, Marcos De Lima4,Michael Keating2, Maher Albitar1
Departments of 1Hematopathology, 2Leukemia,3Myeloma, and 4Blood and Marrow Transplantation,M.D. Anderson Cancer Center, The University of Texas,Houston, TX, USA
Key words: polymerase chain reaction; microsatellitemarkers; plasma; myeloma; 13q; 11q; loss ofheterozygosity
Correspondence: Maher Albitar MD, Department ofHematopathology, M.D. Anderson Cancer Center, TheUniversity of Texas, 1515 Holcombe Boulevard, Box 72Houston, TX 77030-4095, USATel: (713) 794-1292Fax: (713) 794-1800e-mail: [email protected]
Accepted for publication 19 June 2003
Eur J Haematol 2003: 71: 174–178Printed in UK. All rights reserved
Copyright � Blackwell Munksgaard 2003
EUROPEANJOURNAL OF HAEMATOLOGY
ISSN 0902-4441
174

Using circulating plasma tumor-derived DNAfor detection of molecular changes like loss ofheterozygosity (LOH), microsatellite instability andtumor suppressor gene promotor methylation havebeen reported in patients with various malignanciesincluding lung (11), head and neck (12), breast (13),esophageal (14), pancreatic (15), renal (16), andbladder cancer (17).Our study was conducted to evaluate the utility
of plasma DNA in patients with MM for detectingmicrosatellite alterations and LOH at chromo-somes 13q (D13S319 and D13AFMaw301wb5)and 11q (D11S2179) using polymerase chain reac-tion (PCR)-based microsatellite marker analysis.Chromosomes 11 and 13 were selected because oftheir prognostic importance in MM patients. Thespecific microsatellite markers were chosen basedon our previous work showing highest frequency ofdetecting deletions on chromosomes 11 and 13 inchronic lymphocytic leukemia using these markers(18, 19). The microsatellite marker on chromosome11 corresponds to an intron in the ATM gene. TheATM gene is most likely the target for the 11q21deletion in most lymphoid tumors (18).
Materials and methods
Patients and samples
We obtained peripheral blood (PB) samples from81 patients. All patients were evaluated in themyeloma clinic at the M.D. Anderson CancerCenter (University of Texas) from July 1999 toOctober 2003. For all the patients, the diagnosis ofMM was confirmed by BM aspiration and biopsy(PCs), flow cytometry (clonality), and immuno-globulin serum analysis (clonal peak). All PBsamples were collected at points of the course oftherapy with significant variation between patients.The aim of this study was to prove the conceptrather than to correlate with clinical behavior. Wealso collected BM aspirates from 17 of thesepatients. In six of these patients, we sorted thePCs using CD138-coated magnetic beads and
the AutoMACS columns as recommended by themanufacturer (Miltenyi Biotec, Auburn, CA,USA). The specimens were acquired underapproved protocols with informed consent. PBmononuclear cells from each patient were used as acontrol for allele pattern after confirming lack ofcirculating PCs. Being important prognostic fac-tors, the following information was also collected:age, sex, BM PC count, plasma levels of b2-M,levels of abnormal immunoglobulin, and lactatedehydrogenase (LDH) (Table 1). Seventeen PBsamples from normal individuals, younger than30 yr, were analyzed for LOH using the samemicrosatellite markers.
DNA extraction
We separated mononuclear cell fractions by usingFicoll–Hypaque gradient centrifugation (Sigma,St Louis, MO, USA) and washed the cells twicein phosphate-buffered saline. Plasma was obtainedby spinning whole blood, anti-coagulated withethylenediaminetetraacetic acid, at room tempera-ture for 10 min at 3000 · g. For isolation of normal(control) genomic DNA, lymphocytes were diges-ted with proteinase K followed by phenol–chloro-form extraction and ethanol precipitation. Wemeasured the DNA concentrations with aDu-7000 spectrophotometer (Beckman InstrumentInc., Fullerton, CA, USA) at an optical density of260 nm. Plasma DNA was extracted using QIAmpDNA blood mini Kit (QIAGEN Inc., Valencia,CA, USA) as recommended by the manufacturer.
Microsatellite marker analysis
The primer sequences for the amplification ofmicrosatellite repeats in D13S319, D13AF-Maw301wb5, and D11S2179 were identified bysearching the Gene Bank Database. The PCRprimers were made by Genosys (The Woodlands,TX, USA). One primer in each pair was labeledwith a fluorescent dye (Carboxyfluorescein (FAM),carboxytetramethylrhodamine (TAMRA), carboxy-
Table 1. Clinical characteristics of patients
CharacteristicAll patients (n ¼ 81)
median (range)Informative patients
for D11S2179 (n ¼ 61) 11q21 (n ¼ 7)1Informative D13S319 and D13AFMaw301wb5 (n ¼ 62) 13q14 (n ¼ 16)1
Age 59 (34–92) 59 (34–92) 59 (44–92) 60 (34–79) 61 (42–72)Plasma cells in BM (%) 10 (0–90) 10 (0–90) 5 (1–75) 10 (0–90) 7 (1–43)b2-M (mg/dL) 3.6 (1.4–52.6) 3.6 (1.4–17.5) 3.1 (1.6–11.2) 3.6 (1.4–52.6) 3.3 (1.8–12)LDH 475 (190–1317) 475 (272–1317) 45.9 (310–1317) 461 (190–791) 32.4 (344–791)Serum M-peak 1.8 (0.1–9.4) 1.7 (0.1–7.1) 1.5 (0.1–5.1) 2.2 (0.1–9.4) 2.7 (0.1–5.1)Male (%) 62 62 74 59 65
BM, bone marrow; LDH, lactate dehydrogenase; b2-M, beta-2 microglobulin;1 Of the 81 patients, only 61 and 62 were heterozygous (informative) for 11q21 and 13q14, respectively.
LOH in MM using plasma
175

hexam (HEX)). Paired plasma and lymphocyteDNA (control) samples from each patient wereamplified in a 9700 Perkin-Elmer thermal cycler(Perkin-Elmer Cetus, Norwalk, CT, USA) in a totalvolume of 15 lL. Several experiments were per-formed to establish the optimal concentrations forDNA and optimal amplification conditions (MgCl2concentration and annealing temperature) forreproducible results. One hundred nanograms ofcellular DNA or 2–5 lL of plasma DNA solutionfrom each subject was amplified in a typical PCR.The reaction mixture contained 1· PCR buffer(ABI, Foster City, CA, USA), MgCl2 (2.5 mm forD11S2179, 3.3 mm for D13AFMa301wb5, and4.16 mm for D13S319), 250 lm each deoxynucleo-side triphosphate, 0.33 lm each primer pair, and1 unit of AmpliTaq DNA polymerase (ABI). Thereaction mixture was first denatured at 95�C for12 min. This was followed by 15 cycles of annealingand extension for 30 s (at 56�C for D13AF-Ma301wb5 and 60�C for the other two markers),each with a denaturation at 94�C for 15 s, andcompleted with another 20 cycles of annealing/extension under the same conditions (each cyclestarted with a denaturation step at 89�C for 15 s. Afinal extension step was carried out at 72�C for30 min.
Electrophoresis and data analysis
Aliquots of PCR reaction were then mixed withROXTM-500 size standard (ABI) and formamideand subjected to electrophoresis on an ABI PRISM3100 Genetic Analyzer (ABI). The automaticallycollected data were analyzed with GENESCANsoftware (ABI) as described in the manufacturer’smanual. The sizes (in bp) of the microsatellitealleles were calculated automatically with ROX-500internal size marker. Automatic analysis of peakareas allowed relative quantification of PCR prod-ucts and determination of allelic ratios. An indi-vidual was considered to have LOH if the allelicratio of the plasma PCR products and correspond-ing lymphocyte PCR products was 0.6 or ‡1.4.
Results
The characteristics of the patients at the time ofobtaining the PB samples are presented in Table 1.All patients were previously treated and wererandomly selected. Heterozygosity using theD11S2179 on chromosome 11 was seen in only 61patients of the total 81 patients studied and thesepatients are considered informative for this marker.Sixty-two patients were informative using D13S319and D13AFMaw301wb5 microsatellite markers onchromosome 13. DNA extracted from PB plasma
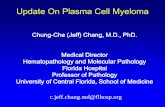
showed LOH in 16 of 62 (26%) informativepatients on chromosome 13 and in seven of 61(11%) of the informative cases at the ATM gene onchromosome 11 (Fig. 1A, B, Tables 1 and 2). Therewas no significant difference between the cases withand without LOH in the percentage of PCs, b2-M,or serum M-peak (Wilcoxon rank test) (Table 1).This suggests that the detection of the abnormal-ities on chromosomes 11 and 13 using PB plasmawas possible even when the level of disease in thesepatients was low. These patients were tested atdifferent stages of their disease. All patients werepreviously treated and no attempt was made tocorrelate our findings with other clinical features.Cells from BM samples of 11 patients who testednegative for LOH in plasma were analyzed forLOH on chromosomes 11 and 13 using the threemarkers, and all were negative. PCs from sixpatients were isolated using CD138-coated beadsand magnetic sorting, and analyzed for LOH
240 280
120
900750600450300150
0
18001350900450
0
2700225018001350900450
05280462039603300264019801320660
0
160
A
PB Cells
Plasma
PB Cells
Plasma
B
Fig. 1. Example of an electropherogram showing loss ofheterozygosity (LOH) at 13q14 (D13AFMaw301wb5) (A)and at 11q21 (D11S2179) (B) in the plasma DNA from twopatients with multiple myeloma (MM). Both patients had<10% plasma cells in their BM and neither had circulatingplasma cells (PCs).
Table 2. Cytogenetic results in patients with LOH and concurrent cytogeneticstudies
Cytogenetics
LOH
11q21 (n ¼ 15) 13q14 (n ¼ 14)
Diploid 8 1011q21 abnormalities 4 213q14 abnormalities 31 22
LOH, loss of heterozygosity.1 One of the patients tested negative for the 13 LOH analysis.2 One patient had both 13 and 11 abnormalities.
Ahmed et al.
176

alongside DNA extracted from plasma from thesame patients. Of the six patients three showedLOH on chromosome 13 and two of these threepatients had LOH on chromosome 11 as well. Twoof these six patients tested negative for chromo-some 11 and one patient for chromosome 13. Theplasma from the same patients showed identicalresults. Follow-up samples after autologous BMtransplantation were available from three patientswho had LOH before the transplant. Two of thesepatients had LOH on chromosome 11 and one hadLOH on chromosome 13. Two of these patientsreverted to a normal state (no LOH) after BMtransplantation and the one who had LOH onchromosome 13 showed detectable LOH in a 1-wkpost-transplantation sample. Detection of LOH inplasma was not dependent on the number of PCs inBM. Seven of the 13 patients with LOH onchromosome 13 had <10% BM PCs and 10 had<20% BM PCs at the time of detection of LOH inPB plasma. All five patients with LOH onchromosome 11 had <20% BM PCs.
Discussion
These results support the hypothesis that PBplasma is a reliable source of DNA for studyingmolecular abnormalities in patients with MM.Plasma DNA has been used to monitor many solidtumors (11–17). Plasma can be an ideal tool formonitoring hematologic disorders as cellular DNAis continually shed into the plasma. Our resultsrevealed that 26% of informative MM patientsshow 13q14 LOH. Metaphase studies revealedfewer deletions of 13 or 13q in patients with MM(20). The detection of LOH in patients was notdependent on the levels of PCs in BM and we wereable to detect LOH in patients with very fewpercentage of PCs in BM. The presence of morethan one subclone of myeloma cells with differentmolecular abnormalities may call for more thanone technique for the detection of these abnormal-ities. Earlier studies in solid tumors suggested thatdespite the high turnover of DNA in tumor, tumor-specific DNA is more abundant in plasma (12–16).It remains to be seen if DNA from more aggressivemyeloma subclones are abundant in the plasma orthey are below the detectable level of our approach.FISH techniques have shown deletion of 13q in11.5–86% of MM patients (20). The underestima-tion of 13q deletions by metaphase studies may berelated to the difficulty in capturing PCs in mitosis.Further prospective studies comparing FISH stud-ies with LOH using PB plasma may provide a newstrategy in evaluating and treating MM patients.PB plasma is an easily accessible source of DNAthat can be used for diagnosing and monitoring
patients. Clearly, further studies with large num-bers of patients and correlation with clinicalbehavior and response to therapy will allow us toevaluate this approach better.Taken together, our findings show that plasma
DNA reflects the molecular abnormalities of PCs inMM. The use of PB plasma could potentiallyreplace painful and costly BM aspiration for eval-uating molecular abnormalities in MM. Moreover,PB plasma analysis may be useful for monitoringpatients, especially after BM transplantation.
References
1. Kyle RA. Prognostic factors in multiple myeloma. StemCells 1995;13:56–56.
2. San Miguel JF, Garcia-Sanz R, Gonzalez M, et al. Anew staging system for multiple myeloma based on thenumber of S-phase plasma cells. Blood 1995;85:448–455.
3. San Miguel JF, Blade Creixenti J, Garcia-Sanz R.
Treatment of multiple myeloma. Haematologica 1999;84:36–58.
4. Bergsagel PL, Kuehl WM. Chromosome translocationsin multiple myeloma. Oncogene 2001;20:5611–5622.
5. Greipp PR, Katzmann JA, O’Fallon WM, Kyle RA.
Value of beta 2-microglobulin level and plasma cell labelingindices as prognostic factors in patients with newly diag-nosed myeloma. Blood 1998;72:219–223.
6. Cigudosa, JCH, Rao PH, Calasanz MJ, et al. Charac-terization of nonrandom chromosomal gains and losses inmultiple myeloma by comparative genomic hybridization.Blood 1998;91:3007–3010.
7. Sawyer JR, Lukacs JL, Munshi N, et al. Identification ofnew nonrandom translocations in multiple myeloma withmulticolor spectral karyotyping. Blood 1998;92:4269–4278.
8. Tricot G, Barlogie B, Jagannath S, et al. Poor prog-nosis in multiple myeloma is associated only with partial orcomplete deletions of chromosome 13 or abnormalitiesinvolving 11q and not with other karyotype abnormalities.Blood 1995;86:4250–4256.
9. Desikan R, Barlogie B, Sawyer J, Ayers D. Results ofhigh-dose therapy for 1000 patients with multiple myeloma:durable complete remissions and superior survival in theabsence of chromosome 13 abnormalities. Blood 2000;95:4008–4010.
10. Shaughnessy J, Tian E, Sawyer J, et al. High incidenceof chromosome 13 deletions in multiple myeloma detec-ted by multiprobe interphase FISH. Blood 2000;96:1505–1511.
11. Sozzi G, Conte D, Mariani L, et al. Analysis of circu-lating tumor DNA in plasma at diagnosis and duringfollow-up of lung cancer patients. Cancer Res 2001;61:4675–4678.
12. Nunes DN, Kowalski LP, Simpson AJ. Circulating tumor-derived DNA may permit the early diagnosis of head andneck squamous cell carcinomas. Int J Cancer 2001;92:214–219.
13. Shaw JA, Smith BM, Walsh T, et al. Microsatellitealterations plasma DNA of primary breast cancer patients.Clin Cancer Res 2001;6:1119–1124.
14. Kawakami K, Brabender J, Lord RV, et al. Hyper-methylated APC DNA in plasma and prognosis of patientswith esophageal adenocarcinoma. J Natl Cancer Inst2000;92:1805–1811.
15. Yamada T, Nakamori S, Ohzato H, et al. Detection ofK-ras gene mutations in plasma DNA of patients with
LOH in MM using plasma
177

pancreatic adenocarcinoma: correlation with clinicopatho-logical features. Clin Cancer Res 1998;4:1527–1532.
16. Goessl C, Heicappell R, Munker R, et al. Microsatelliteanalysis of plasma DNA from patients with clear cell renalcarcinoma. Cancer Res 1998;58:4728–4732.
17. Utting M, Werner W, Muller G, Schubert J, Junker
K. A possible noninvasive method for the detection ofbladder cancer in patients: microsatellite analysis of freeDNA in urine and blood. Ann N Y Acad Sci 2001;945:931–935.
18. Starostik P, Manshouri T, O’Brien S, et al. Deficiency ofthe ATM protein expression defines an aggressive of B-cellchronic lymphocytic leukemia. Cancer Res 1998;58:4552–4557.
19. Starostik P, O’Brien S, Chung CY, et al. The prognosticsignificance of 13q14 deletions in chronic lymphocytic le-ukemia. Leuk Res 1999;23:795–801.
20. Smadja NV, Louvet C, Isnard F, et al. Cytogenetic studyin multiple myeloma at diagnosis: comparison of twotechniques. Br J Haematol 1995;90:619–624.
Ahmed et al.
178