
USAID Nurturepdf.usaid.gov/pdf_docs/PA00MJZ9.pdf · USAID Nurture A Literature Review: Maternal,...
41
USAID Nurture A Literature Review: Maternal, Infant and Young Child Nutrition and WASH Practices in Lao PDR September, 2016
Transcript of USAID Nurturepdf.usaid.gov/pdf_docs/PA00MJZ9.pdf · USAID Nurture A Literature Review: Maternal,...

USAID Nurture A Literature Review: Maternal, Infant and Young Child Nutrition and WASH Practices in Lao PDR September, 2016

Acknowledgements & Forward With support from the United States Agency for international Development (USAID) Cooperative Agreement Number: No. AID-486-A-16-00001, this literature review was drafted by Joy Del Rosso, Alice Atkins and Margaret Kajeckas of Save the Children United States (SCUS). It is intended to inform the design of USAID Nurture’s formative research, and ultimately the project’s social and behavior change communication (SBCC) strategy. The review includes information from both published and grey literature from Lao PDR covering maternal nutrition, child nutrition, dietary diversity of households, select health service utilization, water, sanitation and hygiene (WASH), and gender.
This literature review report is made possible by the generous support of the American people through
the United States Agency for International Development (USAID). The contents are the responsibility of
Save the Children and do not necessarily reflect the views of USAID or the United States Government.

iii
Contents Acknowledgements & Forward ..................................................................................................................... ii
Acronyms...................................................................................................................................................... iv
Introduction .................................................................................................................................................. 1
Purpose and Methodology ............................................................................................................................ 2
Overview of Findings ..................................................................................................................................... 1
Maternal Nutrition Findings .......................................................................................................................... 4
Maternal Nutrition Overview .................................................................................................................... 6
Infant and Young Child Feeding Findings .................................................................................................... 13
Infant and Child Feeding Overview ......................................................................................................... 14
Water, Sanitation and Hygiene Findings ..................................................................................................... 22
WASH Behaviors Overview ..................................................................................................................... 22
Annotated Reference List ............................................................................................................................ 27
List of Tables Table 1. Key National and Project Province Nutrition and WASH Indicators (%) ......................................... 2
Table 2. Comparison of National and Provincial Level Data on Maternal Health and Nutrition .................. 5
Table 3. Summary Matrix of Information on Maternal Nutrition Behaviors ................................................ 8
Table 4. Comparison of National and Provincial Level Data on Infant and Young Child Feeding ............... 13
Table 5. Summary Matrix of Information on Infant and Child Nutrition Behaviors ................................... 17
Table 6. Comparison of National and Provincial Level Data on WASH ....................................................... 22
Table 7. Summary Matrix of Information on WASH Behaviors .................................................................. 24
iv
Acronyms
ANC Antenatal Care
CF Complementary Food CLTS Community Led Total Sanitation
EBF Exclusive Breastfeeding
EIBF Early Initiation of Breastfeeding
IYCF Infant and Young Child Feeding
IYCN Infant and Young Child Nutrition
IUGR Intrauterine Growth Retardation
LBW Low Birth Weight
LSIS Lao Social Indicator Survey MIYCN Maternal, Infant and Young Child Nutrition
OD Open Defecation PDR Lao People’s Democratic Republic PNC Postnatal Care SBCC Social and Behavior Change Communications
SCI Save the Children International
TBA Traditional Birth Attendant
USAID U.S. Agency for International Development
WASH Water, Sanitation, and Hygiene

1
Introduction
Despite significant economic growth, Lao PDR children remain some of the most undernourished in the region, with national prevalence of stunting at 35.6%, underweight at 25.5%, and wasting at 9.6%.1 According to the Laos Social Indicator Survey 2011-2012, factors driving stunting in Laos are complex and multi-faceted. Stunting and poverty are related, with 61% of children in the poorest compared to only 20% in the richest wealth quintile stunted.2
Anemia among children is also a significant issue, with more than half of provinces showing rates up to 55% of children under 5 years affected.3 Fifteen percent (15%) of women are underweight and one-third anemic, key contributing factors to the 15% of infants with a low birth weight.4 Low access, utilization and quality of health care services are also persistent problems in Laos and contribute to stunting; rural populations without road access have the highest rates of stunting, and only 25.4% of rural women in areas without roads access antenatal care (ANC).5 Other factors that influence stunting include suboptimal behaviors practiced after birth and related to child feeding and care, access to and use of improved sanitation, and limited practice of healthy WASH behaviors. All practices vary by province and district. The U.S. Agency for International Development “Nurture” (USAID Nurture) project, led by Save the Children International (SCI) is aimed at contributing to a reduction in young child stunting. Over a three-year period, USAID Nurture will be implemented in all villages of six districts of two provinces — Savannakhet and Khammouane — in the central region of Lao PDR. The approach supported by this project focuses on: improving maternal, infant and young child nutrition (MIYCN) and water, sanitation and hygiene (WASH) behaviors in households with pregnant women and children under two years; increasing access and use of quality nutrition and health services and WASH facilities and products; and strengthening the enabling environment, through human resource capacity building and strengthening multi-sectoral coordination and planning, particularly at provincial and district levels. Project efforts are underpinned by social and behavior change communication (SBCC), including addressing gender issues, and monitoring, learning and evaluation. The project works to build capacity of government at national, provincial, and district levels and non-governmental partners to ensure the ground is set for scale up within and beyond operational provinces.
1 2015 Lao Child Anthropometry Assessment Survey (LCAAS). 2 Ministry of Health and Lao Statistics Bureau (2012) Laos Social Indicator Survey 2011-12, Vientiane, Lao PDR. 3 United Nations and Government of Lao PDR (2013) MDG Progress Report for Lao PDR 2013: United Nations Development Program, p 47; 4 Ministry of Health and Lao Statistics Bureau (2012) Laos Social Indicator Survey 2011-12, Vientiane, Lao PDR. 5 World Bank (2013) Lao People’s Democratic Republic, Maternal Health, Child Health and Nutrition in Lao PDR: Evidence from a Household Survey in Six Central and Southern Provinces, World Bank, Washington DC.

2
The project provides interpersonal communications and house-to-house and peer group support, linkages with health services, and a community mobilization approach for integrated nutrition and WASH that incorporates a modified form of community-led total sanitation (CLTS). Communities will be mobilized to appraise and analyze their own nutrition, water, sanitation and hygiene environment. This process is intended to spur actions to address nutrition-related issues resulting from poor infant and young child feeding (IYCF) practices, inadequate water, sanitation and hygiene, including environmental enteropathy, diarrhea and other conditions that limit nutrient absorption, a major cause of stunting. The project will leverage private sector relationships to facilitate supply of products needed for improved uptake of WASH practices. This integrated delivery model supports the Lao government in its implementation of the National Nutrition Strategy to 2025, and the National Plan of Action 2016-2020. Using data from 2011-2012, compared to national averages, USAID Nurture’s two targeted provinces have slightly lower prevalence of stunting, but rates are still high at 40%, and few nutrition projects operate in these areas. (The 2015 LCAAS found stunting rates in Savannakhet have declined to 30.8%, and in Khammouane to 33.9%). Rates of exclusive breastfeeding are extremely low, much lower than the national average, and similarly, WASH practices are very poor (see Table 1). Table 1. Key National and Project Province Nutrition and WASH Indicators (%)
Data National Savannakhet Khammouane
Population size 6.77million 825,879 337,314
Proportion of children under 5 who are stunted 44.2 40.8 40
Exclusive breastfeeding rate 40.4 16.5 13.4
Households using improved sanitation facilities 56.9 39 42
Households disposed of children’s last stool safely 18.6 9.8 3.7 Source: Lao PDR Social Indicator Survey (LSIS), 2012.
Purpose and Methodology A review of the nutrition literature from Lao PDR was conducted to inform the design of USAID Nurture project’s formative research, and social and behavior change communications (SBCC) strategy. The review included both peer-reviewed and grey literature. Two search engines, PubMed and Google Scholar were used to identify relevant articles. Primary search terms were “Laos” and “nutrition;” secondary terms included “water,” “hygiene,” “sanitation,” “health,” and “gender.” Additional articles were found in the reference sections of the initial review articles, and existing literature reviews produced by Save the Children and other stakeholders. To identify reports and other grey literature for inclusion, Google searches were conducted for program names mentioned in key articles.

3
Documents included in this review had study designs containing quantitative and qualitative methods, or both, and included data from Laos, although articles could also include neighboring countries (Vietnam and Thailand). Excluded articles were those that did not include data from Lao PDR, and articles published prior to 2000. This was intended to focus findings on the current context. Comments, editorials, and conference presentations were also excluded. A total of 40 documents were included for review. Five main dimensions were used to extract and summarize the information in the literature: (a) theme; (b) target population; (c) geographic coverage; (d) key results/findings; and (e) knowledge/belief/behavior. Where reported, any data on nutritional status of women and children and on the ethnicity of the target population were extracted.
Overview of Findings This document summarizes what is known about MIYCN, WASH, and related practices that
influence nutrition outcomes in Lao PDR. Overall, the findings indicate that many gaps exist in
our knowledge and understanding of nutrition practices, particularly in the USAID Nurture
project implementing areas. The formative research to be conducted under USAID Nurture and
stakeholder discussions will further contribute to building the knowledge base, filling gaps in
the understanding of nutrition practices during the first 1,000 days period, and developing
effective strategies to address suboptimal practices. The main findings for Lao PDR from the
review are:
Health Service Utilization
Mothers and households have limited interaction with the health system during
pregnancy and the post-partum period. These interactions (or lack thereof) can have an
impact on MIYCN behaviors, which highlights the need to strengthen the quality and use
of health services during these 1,000 day stages.
Maternal Nutrition
Post-partum confinement or lying periods with accompanying food restrictions are
widespread, and relatively well-documented in the literature.
Women’s time to breastfeed and prepare food for children may be a significant barrier
to good nutrition—both ensuring women’s nutrition during pregnancy and post-partum,
and among children.

4
Facilitating factors identified in the literature related to maternal nutrition are families’
beliefs in the importance of reducing a women’s work load during pregnancy, and
postpartum rituals that include support for rest following childbirth.
Infant and Young Child Nutrition
Feeding practices during the first six months, especially in project target areas, need
attention. Exclusive breastfeeding rates are very low, likely do in part, at least, to pre-
lacteal feeding practices. Lack of access to health services, women’s time constraints
and reliance on family members for breastfeeding support (and decision-making) may
contribute to these practices.
Major gaps in information exist on feeding behaviors across the crucial 6 to 23-month
period, when good practices are needed for the rapid growth occurring in this period.
The poor quality of young child diets and inadequate quantity of food appears linked in
part to issues of access to quality foods and social norms. Little evidence exists on the
ability or methods to affect change, particularly in project areas.
Family members remain the most trusted source of information for health, childbirth
and nutrition. This suggests that reaching a wide range of community members will be
critical for influencing MIYCN practices.
WASH
WASH practices are limited by access to water and sanitation facilities. The practice of
open defecation is still common in many areas. Water supply is a major limiting factor
for good WASH practices. A number of motivating factors for better WASH practices in
households and communities exist, such as convenience, and awareness of the health
risks associated with open defecation.
Maternal Nutrition Findings Maternal nutrition refers to the nutritional needs of women during the antenatal and postnatal
period (i.e., when they are pregnant and breastfeeding) and also may refer to the pre-
conception period (i.e., adolescence). Maternal under-nutrition affects the health of both
mothers and children and, as a result, negatively affects economic and social development.
Undernourished pregnant women have higher reproductive risks, including death during or
following child birth. Globally, many women suffer from a combination of chronic energy
deficiency, inadequate weight gain in pregnancy, anemia, and other micronutrient deficiencies,
as well as infections like HIV and malaria. These, along with inadequate obstetric care,
contribute to high rates of maternal mortality and poor birth outcomes. Under-nutrition in

5
pregnant women is directly linked to intrauterine growth retardation (IUGR), which results in
low birth weight (LBW), prematurity, and low nutrient stores in infants. Maternal under-
nutrition also diminishes a woman’s productivity, causing repercussions for herself, her family,
her community, and the broader society.
According to the Lao Social Indicator Survey (LSIS) 2011/2012, health service use during pregnancy, delivery and postpartum period is low (Table 2). While over half of women receive some antenatal care (ANC), many do not receive the recommended four visits or more: less than a third of women in both Khammouane (28%) and Savannakhet (31%) attended at least four ANC visits. Iron supplementation during pregnancy is low; nationally one in four women consume more than 90 iron tablets during pregnancy compared to 16% of women in Khammouane and 19% in Savanakhet. Nationally 40% of women delivered in a health facility compared to 39% of women in Savannakhet and 30% of women in Khammouane. Postnatal care (PNC) is poor; just over a third of women nationally (40%) and in the two project provinces (35-37%) received any PNC check from any health provider within two days of the last pregnancy. Nationally, 15% of children in Laos PDR are born with low birth weight (LBW). In the project areas, LBW rates range from 14% in Savannakhet to 22% in Khammouane. Table 2. Comparison of National and Provincial Level Data on Maternal Health and Nutrition
Maternal Nutrition and Health National Khammouane Savannakhet
ANC─% of women who had a live birth who received ANC from any health professional
54% 48% 52%
% of women who had a live birth during the 2 years preceding who had 4+ ANC visits by any provider
37% 28% 31%
Iron during pregnancy─% of women age 15-49 who took the recommended 90+ iron pills during the last pregnancy
25% 16% 19%
% of women age 15-49 who had a live birth in the past 2 years assisted at delivery by any health professional
42% 35% 42%
% of women age 15-49 who had a live birth in the past 2 years who delivered in a health facility
38% 30% 39%
PNC─% of newborns born who received any health check following delivery or post-natal care visit from any health provider within 2 days of delivery
41% 39% 36%
PNC─% of women age 15-49 years who received health checks and PNC visits from any health provider within 2 days of delivery
40% 37% 35%
Low birth weight─% of last-born children in the past 2 years estimated to have weighed <2500 grams at birth
15% 22% 14%
Source: Lao PDR Social Indicator Survey (LSIS), 2011/2012.

6
Maternal Nutrition Overview
There were 16 articles included in this review with information on maternal nutrition practices. The literature shows that practices vary across regions and ethnic groups. The details of these studies are presented in Table 3 organized by the recommended practices for maternal nutrition. Information on dietary practices during pregnancy is limited. The practice of ‘eating-down’ was shown to be prevalent in at least one study area in Luang Prabang.6 Food taboos and restrictions appear to be less common in the pregnancy period than post-partum, although in Khammouane, egg and meat were noted as restricted foods during pregnancy.7 The qualitative literature lacks information on women’s use of iron or other micronutrient supplementation during pregnancy.8 Likewise very little is documented specifically on calorie consumption during pregnancy and lactation, or on women’s dietary diversity. Little also is known of the barriers and facilitators to good practices, with limited information on practices in USAID Nurture Provinces. More qualitative information has been collected on postpartum practices; food taboos and restrictions accompanied by lying in practices are the norm in Laos. These are believed to aid a woman’s recovery and ensure the quantity and quality of breastmilk, with quality perceived to protect the child from illness. The specific food restrictions differ by village and ethnic group. Steam sauna and bathing, and ‘hotbed’ (also called mother roasting, is the practice of mothers sitting or lying on a bed placed over hot embers or coals) practices vary by the birth and location, although these general practices are widespread among most ethnic groups. The hotbed is particularly common, and considered an essential part of postpartum recovery.9,10 In Vientiane the practice usually lasts about 14 days, although it has been reported to last as long as 4 weeks in other areas.11
6 Identifying priorities to improve maternal and child nutrition among the Khmu ethnic group, Laos: a formative study (2012) de Sa J, Bouttasing N, Sampson L, Perks C, Osrin D, Prost A. Maternal & Child Nutrition 9(4): 452-466. 7 Women, Food and Land: Understanding the impact of gender on nutrition, food security and community resilience in Lao PDR. Food Security Risk and Vulnerability Survey – Summary Report (2013) Stoeber S, Sisomphone E, Han C. Care International and National University of Laos. Vientiane, Lao PDR. 8 Influences on maternal and child nutrition in the highlands of the northern Lao PDR (2007). Holmes W, Hoy D, Lockley A, Thammavongxay K, Bounnaphol S, Xeuatvongsa A, Toole M. Asia Pac J Nutr 16(3): 537-545. 9 Influences on maternal and child nutrition in the highlands of the northern Lao PDR (2007). Holmes W, Hoy D, Lockley A, Thammavongxay K, Bounnaphol S, Xeuatvongsa A, Toole M. Asia Pac J Nutr 16(3): 537-545. 10 Steam sauna and mother roasting in Lao PDR: practices and chemical constituents of essential oils of plant species used in postpartum recovery (2011) de Boer H. J, Lamxay V, Bjork L. BMC Complementary and Alternative Medicine, 11:128. 11 Steam sauna and mother roasting in Lao PDR: practices and chemical constituents of essential oils of plant species used in postpartum recovery (2011) de Boer H. J, Lamxay V, Bjork L. BMC Complementary and Alternative Medicine, 11:128.

7
Postpartum food restrictions in USAID Nurture provinces include avoiding rotten, fermented, oily, sour, raw or spicy foods, and some meats (particularly from white animals). In Khammouane, women in the post-partum period have a staple of rice, salt, ginger, and boiled root water, and among some ethnic groups, women consume only salt water for a few days after birth.
The literature indicates that women reduce rigorous physical activities during pregnancy. Research from Mahaxay and Thakek districts of Khammouane identified lifting heavy objects, such as carrying water; gardening; working in the rice fields, and carrying charcoal as restricted activities. Rigorous activities are seen as harmful to a pregnant woman and thought to lead to miscarriage or abortion. Women continue with light housework during pregnancy, and are expected to resume restricted activities after giving birth and finishing their confinement period. These beliefs were found to be shared across women, including mothers-in-law, and among husbands. In some provinces, men take on extra domestic work during pregnancy.12 A number of articles addressed health seeking and health service utilization practices in Lao, particularly as they relate to nutrition outcomes. Health seeking-practices during pregnancy show, as confirmed by quantitative surveys, low health facility delivery rates, with families often preferring to deliver at home. This practice influences early child feeding; avoidance of pre-lacteal feeds is more common among women who had skilled birth attendants. Understanding the barriers and motivations for family decisions around birth location will be useful in addressing sub-optimal nutrition practices.
12 Cultural Beliefs And Traditional Rituals About Childbirth Practices in Lao PDR (2009) Sychareun V, Phengsavanh A, Hansana V, Somphet V, Sysouvanh, Menorath S. Kuala Lumpar, Malaysia: The Asian-Pacific Resource & Research Centre for Women (ARROW).

8
Table 3. Summary Matrix of Information on Maternal Nutrition Behaviors
Recommended Behavior Current Practices, Motivations and Barriers to Improved Practice Gaps in Information (what do we need to know)
Dietary Quantity Eat at least one extra serving of staple food (285kcal) a day while pregnant (Reference 23, 20, 38) Consume enough extra calories to gain 11-16 kg if normal weight pre-pregnancy and 13-18kg if underweight before pregnancy (Reference 23, 5)
General understanding in different areas (Huaphan, Phongsaly, Luang Prabang) that women need to eat well during pregnancy (Huaphan and Phongsaly).
Luang Prabang reported that increasing the amount of food is considered ‘good’, such as meat and fruit, to improve quality, no mention of amount consumed.
Some practice “eating down” during pregnancy (Luang Prabang).
In Vientiane, maternal age (below 18 years of age); strenuous physical labor; lack of adequate knowledge about the details of a healthy pregnancy; mothers in poor health; low-income mothers (<1 million Kips) increased the risk of a LBW baby.
No information found regarding specific diet and caloric consumption during pregnancy by ethnic group No information regarding USAID Nurture implementation areas: What are families willing to adjust/change and how?
Dietary Quality and Micronutrients Increase daily consumption of fruits and vegetables, animal products and fortified foods (Reference 20, 27, 23, 22, 38)
Women reported a desire to improve their nutrition for the baby during pregnancy.
Food taboos exist─less common during pregnancy than lactation. Taboo foods during pregnancy include coconut, pork, alcohol, fermented fish betel nut (Luang Prabang), eggs and meat (Ethnic minorities in Khammouane).
Understanding of availability and seasonality needed and gender norms related to food consumption Additional information on food restrictions in pregnancy in Savannakhet and Khammouane
Take daily supplements of 60 mg iron and folic acid or multiple
No indication of widespread use of iron-folate, multi-micronutrients, or Vitamin A and B1 during pregnancy.
Information on micronutrient intake and facilitators to increase

9
Recommended Behavior Current Practices, Motivations and Barriers to Improved Practice Gaps in Information (what do we need to know)
vitamin/mineral supplements and use iodized salt (Reference 23)
access and use during pregnancy needed Information on iodized salt access and use needed, in addition to family perceptions of iodized salt
Decrease consumption of iron-inhibiting foods/fluids such as tea with meals
No information available. Need information
Workload and Care During Pregnancy Avoid heavy labor or lifting during pregnancy and rest more during pregnancy (Reference 37)
Restricted activities include lifting heavy objects such as carrying water, gardening, working in the rice fields, carrying charcoal; though women continue with cooking and cleaning their houses.
Prohibitions on sleeping during day time due to belief that they would experience difficulty in labor, in retaining the placenta and the baby would contract jaundice. (Champasak and Khammouane)
Husbands take on additional domestic work during pregnancy (Huaphan and Phongsaly)
Information gaps in understanding factor of seasonality, gender roles, assistance from extended family members, regional differences
Workload and Care Postpartum Avoid heavy labor or lifting and rest more during lactation. Seek postnatal care (Reference 27, 23, 6, 4)
Use of ‘hotbeds’, steam saunas, and baths are common (Khammouane, Vientiane Huaphan, Sekong, Phongsaly).
Hotbed considered to have medicinal qualities: aids physical recovery, protects against puerperal fever, alleviates symptoms of postpartum anemia (dizziness and headaches), stimulates expulsion of the lochia, and ceases postpartum bleeding, perineal healing. It is also helpful because it enforces a time of rest and avoidance of household duties, and strengthens social relations (Khammouane, Vientiane, Champasak and Sekong).
Mothers eat, nurse and sleep on the hotbeds (Khammouane, Vientiane)
Need additional information on work load concerns and also how traditional practices can be motivations for protecting women postpartum and/or if there are barriers

10
Recommended Behavior Current Practices, Motivations and Barriers to Improved Practice Gaps in Information (what do we need to know)
Confinement may be less strict due to food shortages and increased workload (Khammouane).
Use of medicinal plants during child birth and for postpartum recovery, recovery after miscarriage; postpartum hemorrhage, lactagogue, and normal postpartum recovery.
Husbands prepare for childbirth: save money, buy nappies, baby clothes, rope, ginger, herbal medicine, boiled water, wood, and bamboo bed.
Dietary Quantity and Quality During Lactation Increase consumption of fresh or dried fruits and vegetables; iron-rich foods, animal source foods, and foods that enhance absorption (meat, fish, poultry, and vitamin C-rich foods) Eat equivalent of an extra meal (500 extra kcal) when lactating (Reference 21, 23, 27, 22, 20, 29, 24, 40)
Food taboos and dietary restrictions post-partum are widespread; similar across the Mekong Corridor and Northern Uplands but less widespread in the Southern Highlands.
Food restrictions are intended to ensure the health of the new mother and production of an adequate quality and quantity of breastmilk.
Animal source proteins may be restricted on the color of the animal. Restricted animal source foods include beef, water buffalo, pork, and some local fish such as catfish, snake-head fish, nile tilapia, and fish with no scales (Muang Feng district of Vientiane); white buffalo, chicken with white feathers, cattle, and all kinds of wildlife are avoided (Khammouane).
Fruit and vegetable restrictions are common.
Consumption of only traditional unsweetened herb tea in the first 15 days postpartum─considered to be beneficial for lactation; healing of injuries caused by delivery; and for prevention of cardiac failure (Vientiane).
Breastfeeding mothers should not eat "rotten, fermented, oily, sour, raw or spicy food", some meats, bamboo, jack fruits or pumpkin because "baby might get stomach ache" or “digestive problems” (Savannakhet and Champasak). Avoid consumption of foods such as raw or fermented vegetables, fruits, meat (lap-mou, sommou, pad-dek), white skinned mammals, liquid meals and sauces, sugar and spices (Vientiane).
Some groups consume a limited diet in the first days after delivery; sticky rice with salt and galangal; salt water; hot water, combined with boiled rice and
Further information on the specifics of restrictions in project areas is needed. Are women required to restrict foods during all breastfeeding or just the first 6-month period, by ethnic group? What is the effect of restrictions on dietary diversity and caloric intake? How does this impact intake of highly nutritious foods by ethnic group? Do socioeconomic factors, seasonality also affect post-partum rituals? What post-partum practices are families willing to adjust/change and how?

11
Recommended Behavior Current Practices, Motivations and Barriers to Improved Practice Gaps in Information (what do we need to know)
boiled vegetables, boiled unripe banana flowers, boiled rattan shoots and salt, chicken or fish soup; boiled rice, vegetables fish and salt.
Un-boiled water and cold drinks are universally prohibited (Savannakhet).
Home production influences diet; market access is highly variable.
Barriers to optimal maternal nutrition include maternal education, time since delivery, lack of medical care and household income.
No large survey data on maternal dietary diversity or caloric intake. Seasonal/regional differences, urban/rural. Socioeconomic and gender/decision making factors on maternal/women’s diet.
Health Care Seeking and Delivery Practices Have at least four antenatal care visits during pregnancy (References: 36, 40)
Distance from health facility plays a role in whether women are more likely to disregard food taboos (Luang Prabang).
Use of ANC services variable by region: near Vientiane, 91% of mothers use ANC, across 6 provinces 40% access at least one ANC visit. Ethnic minority groups access less ANC. Lowland and midland mothers had higher use of ANC than highland mothers.
Barriers to antenatal care include: financial factors; not wanting to go alone; physical access–distance; lack of transport; cultural norms; and language/communication concerns.
Need more in-depth information on facilitators and motivations to access to health services in project areas by ethnic group and region
Deliver in a health facility or have a health care provider-assisted delivery (References: 32, 37, 38)
Many women give birth at home even those who attend ANC at public hospitals (Khammouane and Savannakhet).
Family members, including fathers and TBAs assist with home births or those in simple birthing shelters or in the forest.
TBAs and health care providers influence mother’s choice of delivery location (Champasak and Khammouane).
Home birth viewed as easy, convenient, and preferred since family support is there; husbands cannot enter the delivery room in some hospitals and home births align better with traditional practices and rituals.
Distance of homes from health facilities plays a role in whether women are likely to disregard food taboos.
What is the perception of the health facilities and health system in project communities, by ethnic group? Are health service providers able to communicate with mothers in local languages and respect local belief systems?

12
Recommended Behavior Current Practices, Motivations and Barriers to Improved Practice Gaps in Information (what do we need to know)
Women consult husbands and grandmothers on where to give birth (Khammouane and Champasak).
What are families willing to change and how?

13
Infant and Young Child Feeding Findings Infant and young child feeding (IYCF) is context specific. Optimal breastfeeding and
complementary feeding behaviors have been defined (Table 4), however to what extent (and
how) the range of behaviors is practiced—from initiation of breastfeeding, continuation of
breastfeeding and introduction of complementary food to introducing family foods, among
others—varies tremendously according to culture, geography, social, economic and other
family and community factors.
As previously noted, stunting is high in Lao PDR. In USAID Nurture provinces Khammouane and
Savannakhet 33.9% and 30.8% of children are stunted respectively.13 IYCF affects nutritional
status, including stunting. According to the LSIS study, IYCF practices are sub-optimal in both
USAID Nurture provinces. Early initiation of breastfeeding (EIBF) is low in both Khammouane
(30%) and Savannakhet (22%). Seventy percent (70%) of children in Khammouane are given
pre-lacteal feeds, defined as any food except mother's milk provided to a newborn before
initiating breastfeeding, limiting early initiation and exclusive breastfeeding. According to LSIS
2011/2012, very few children are exclusively breastfed in Laos—only 40% of children nationally
are given breastmilk exclusively for the first 6 months of life compared to 13% in Khammouane
and 17% in Savannakhet. Despite the low rates of EBF, EIBF and pre-lacteal feeding, children are
breastfed for an average of 20 months. The proportion of children receiving foods the minimum
number of times in a day varies greatly between the provinces. The national average is 43%, but
in Savannakhet only one-third of children receive the minimum meal frequency. Feeding
practices during illness are particularly poor across Laos and in the targeted provinces. Only one
in ten children in Savannakhet are fed according to recommended practices when they are ill.
Table 4. Comparison of National and Provincial Level Data on Infant and Young Child Feeding
IYCF Practices National Khammouane Savannakhet
Pre-lacteal feeds--% of last born children in last 2 years who received a pre-lacteal feed
34% 70% 57%
Early initiation--% of last born children in last 2 years who were breastfed within one hour of birth
39% 30% 22%
Exclusive BF--% of last born children in last 2 years who were exclusively breastfed for the first six months
40% 13% 17%
Duration of BF--Median duration of any breastfeeding among children age 0-35 months (in months)
20 21 20
Introduction of complementary foods--% of infants aged 6-8 months who received solid, semi-solid or soft foods during the previous day
52% N/A N/A
13 2015 Lao Child Anthropometry Assessment Survey (LCAAS).

14
IYCF Practices National Khammouane Savannakhet
Minimum meal frequency--% of children 6-23 months who received solid, semi-solid or soft foods (and milk feeds for non-BF children) the minimum number of times or more during the previous day
43% 62% 33%
Feeding during diarrhea--% of children 0-5 years with diarrhea in the last 2 weeks given more to eat during episode of diarrhea
19%
32%
11%
Feeding during diarrhea--% of children 0-5 years with diarrhea in the last 2 weeks given more to drink during episode of diarrhea
27% 32% 11%
Treatment of diarrhea with ORS--% of children 0-59 months with diarrhea in last 2 weeks and treatment with ORS and recommended homemade fluids
48% 31% 35%
Source: Lao PDR Social Indicator Survey (LSIS), 2011/2012.
Infant and Child Feeding Overview
IYCF practices in Laos are sub-optimal. The literature review revealed contextual information
that limits optimal breastfeeding and complementary feeding practices (Table 5).
One of the most significant impediments to exclusive breastfeeding is pre-lacteal feeding. Many
children receive water (Savannakhet, Champasak and Khammouane), and pre-masticated
glutinous rice (Luang Prabang, Savannakhet and Champasak).14 The full complement of reasons
why mothers give pre-lacteal feeds are unclear, but in some districts, it is believed that the
baby should drink water immediately after birth, and failing do to so will lead to jaundice and
conjunctivitis. Pre-lacteal feeding is more common when births are attended by traditional birth
attendants (TBAs), and least common among ethnic Hmong and Mon-Khmer infants.15
EIBF is more common among educated mothers, and those who received ANC and delivered at
a health facility. However, evidence on provision of colostrum was inconsistent in the literature.
It appeared relatively common in some areas (Luang Prabang, Vientiane) and less common in
14 Consulting with Caregivers – Using Formative Research to Improve Maternal and Newborn Care and Infant and Young Child Feeding in the Lao People’s Democratic Republic. (2004) Gillespie A, Creed-Kanashiro H, Deuanesay S, Sayakoummane, Galloway R. The World Bank Health Nutrition and Population Discussion Paper. The World Bank: Washington DC. 15 Key Determinants of Optimal Breastfeeding Practices in Laos (2013) S. Kounnavong S, Pak-Gorstein K, Akkhavong U, Palaniappan V, Berdaga J, Conkle J, Gorstein J. Food and Nutrition Sciences, 4: 61-70.

15
others.16,17,18 In Savannakhet, it was reported that some mothers think colostrum is “is not real
milk”, “is hot, dirty, sour or bad tasting” and “it is tradition not to give it.”19
The highest EBF rates are among ethnic Hmong (69%), Mon-Khmer (57%) and Lao-Thai (33%).
The Hmong-Yao ethnic groups have high rates of EBF, and are one of the only groups whose
norm is to not introduce foods until 5 months.
Breastfeeding is widely practiced in Lao; data from Savannakhet show that most infants are
breastfed until 2 years. Mothers stop EBF and/or any breastfeeding because of the need to
return to work, the belief that breastmilk is not enough, or becoming pregnant again. Factors
associated with EBF are ethnicity, encouragement of father and family support, inter-spousal
communication about breastfeeding and location. Mothers in rural areas are more likely to
practice EBF than mothers in urban areas.20
Six studies in Vientiane, Attapeu, Saravane and Sekong examined practices related to the
introduction of semi-solid, solid and soft foods. Over half of children are introduced to
complementary foods (CFs) at 6-7 months of age. Complementary foods provided to children
after 6 months varied across the regions and according to traditional beliefs that vary among
ethnic groups. In Luang Prabang, Phongsaly, and Khammouane children often start consuming a
rice porridge and are gradually introduced to other foods, such as small pieces of barbecued
fish or meat.21,22 In Khammouane, some communities feel that vegetables are not suitable
complementary foods. Food scarcity, lack of understanding on preparing food for children and
time constraints were cited in different studies as reasons why children did or did not receive
16 Identifying priorities to improve maternal and child nutrition among the Khmu ethnic group, Laos: a formative study (2012) de Sa J, Bouttasing N, Sampson L, Perks C, Osrin D, Prost A. Maternal & Child Nutrition 9(4): 452-466. 17 Influences on maternal and child nutrition in the highlands of the northern Lao PDR (2007). Holmes W, Hoy D, Lockley A, Thammavongxay K, Bounnaphol S, Xeuatvongsa A, Toole M. Asia Pac J Nutr 16(3): 537-545. 18 A qualitative study on the breastfeeding experiences of first-time mothers in Vientiane, Lao PDR (2013) Mei Hong Lee H, Durham J, Booth J, Sychareun V. BMC Pregnancy and Childbirth 13:223. 19 Consulting with Caregivers – Using Formative Research to Improve Maternal and Newborn Care and Infant and Young Child Feeding in the Lao People’s Democratic Republic. (2004) Gillespie A, Creed-Kanashiro H, Deuanesay S, Sayakoummane, Galloway R. The World Bank Health Nutrition and Population Discussion Paper. The World Bank: Washington DC. 20 Key Determinants of Optimal Breastfeeding Practices in Laos (2013) S. Kounnavong S, Pak-Gorstein K, Akkhavong U, Palaniappan V, Berdaga J, Conkle J, Gorstein J. Food and Nutrition Sciences, 4: 61-70. 21 Nutritional status of children in rural Lao PDR: who are the most vulnerable? (2005) Miyoshi M, Phommasack B, Nakamura S and Kuroiwa C. European Journal of Clinical Nutrition (2005) 59, 887–890. 22 Women, Food and Land: Understanding the impact of gender on nutrition, food security and community resilience in Lao PDR. Food Security Risk and Vulnerability Survey – Summary Report (2013) Stoeber S, Sisomphone E, Han C. Care International and National University of Laos. Vientiane, Lao PDR.

16
diverse foods. Minimum dietary diversity was highest among children from urban areas, those
with wealthy parents, and educated mothers in Attapeu, Saravane, Sekong.23
Information is extremely limited on child feeding practices during illness across Lao PDR, and
especially in USAID Nurture project areas. Some data suggest that mothers continue to
breastfeed during periods of illness and limit sour and spicy foods, and sometimes encourage
consumption of “good foods.” No information is available on whether children consume more,
less or the same during periods of illness. 24,25
23 Report of the Baseline Survey for the Maternal and Young Child Security Initiative (EU-UNICEF MYCNSIA) in Lao PDR, 2012 (2012) National Institute of Public Health, Department of Hygiene & Health Promotion, Ministry of Health UNICEF/Laos, European Union, with Technical Assistance from the Global Center for Integrated Health of Women, Adolescents, and Children/University of Washington. 24 Influences on maternal and child nutrition in the highlands of the northern Lao PDR (2007). Holmes W, Hoy D, Lockley A, Thammavongxay K, Bounnaphol S, Xeuatvongsa A, Toole M. Asia Pac J Nutr 16(3): 537-545. 25 Identifying priorities to improve maternal and child nutrition among the Khmu ethnic group, Laos: a formative study (2012) de Sa J, Bouttasing N, Sampson L, Perks C, Osrin D, Prost A. Maternal & Child Nutrition 9(4): 452-466.

17
Table 5. Summary Matrix of Information on Infant and Child Nutrition Behaviors
Recommended Behavior Current Practices, Motivations and Barriers to Improved Practice Gaps in Information (what do we need to know)
Place the newborn on the breast within 1 hour of the delivery; Give colostrum (Reference 10, 23, 20, 11, 24, 11)
Early initiation of BF most prevalent among mothers with higher education, those who receive ANC and those who deliver at a health facility; Hmong (45%) and Mon-Khmer (34%) had slightly lower rates than Lao-Thai (43%) in Attapeu, Saravane and Sekong.
Widespread belief that colostrum is harmful and that it is normal for white milk not to appear for 2-3 days after birth (Huaphan and Phongsaly).
Distance of homes from the health facility influences giving colostrum to newborns.
Mothers do not feed colostrum because: “is not real milk”, “is hot, dirty, sour or bad tasting” and “is tradition not to give it” (Champasak, Luang Prabang, and Savannakhet).
Practices to “get breasts ready for breastfeeding include: showering both mother and baby so that they were both ‘clean’ and massaging the breasts to encourage creation of a hole in the nipple for the milk to drain through (Luang Prabang).
High rates of giving colostrum in Vientiane and Luang Prabang but the practice is less common in Savannakhet and Champasak.
Lack of proximity to a community hospital was a barrier to giving colostrum to newborns.
Further information on perceptions and understanding of importance of colostrum in project areas. What factors are associated with providing colostrum in project areas? Need more data on practice of giving colostrum, and beliefs relating to colostrum and what will motivate families to practice immediate breastfeeding in project areas
No pre-lacteal feeds (Reference 24, 10, 33, 10, 20, 37)
Prelacteal feeding more common when traditional birth attendant present at birth compared to a professional skilled attendant, or even when assisted by an untrained family or friend. Hmong and Mon-Khmer infants are less likely to receive pre-lacteal feeds, as are children born in public health facilities (compared to out of facility births).
Information on what alternatives families are willing to try in relation to prelacteal feeds (including reducing the amounts/frequency)
18
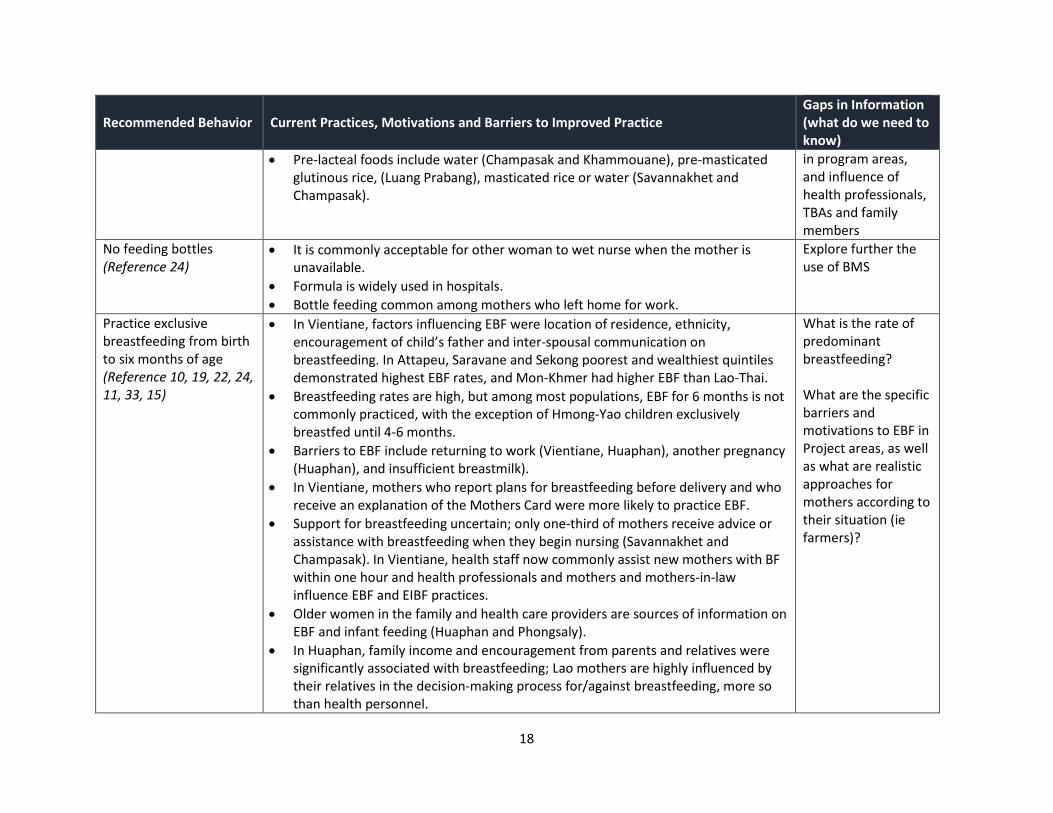
Recommended Behavior Current Practices, Motivations and Barriers to Improved Practice Gaps in Information (what do we need to know)
Pre-lacteal foods include water (Champasak and Khammouane), pre-masticated glutinous rice, (Luang Prabang), masticated rice or water (Savannakhet and Champasak).
in program areas, and influence of health professionals, TBAs and family members
No feeding bottles (Reference 24)
It is commonly acceptable for other woman to wet nurse when the mother is unavailable.
Formula is widely used in hospitals.
Bottle feeding common among mothers who left home for work.
Explore further the use of BMS
Practice exclusive breastfeeding from birth to six months of age (Reference 10, 19, 22, 24, 11, 33, 15)
In Vientiane, factors influencing EBF were location of residence, ethnicity, encouragement of child’s father and inter-spousal communication on breastfeeding. In Attapeu, Saravane and Sekong poorest and wealthiest quintiles demonstrated highest EBF rates, and Mon-Khmer had higher EBF than Lao-Thai.
Breastfeeding rates are high, but among most populations, EBF for 6 months is not commonly practiced, with the exception of Hmong-Yao children exclusively breastfed until 4-6 months.
Barriers to EBF include returning to work (Vientiane, Huaphan), another pregnancy (Huaphan), and insufficient breastmilk).
In Vientiane, mothers who report plans for breastfeeding before delivery and who receive an explanation of the Mothers Card were more likely to practice EBF.
Support for breastfeeding uncertain; only one-third of mothers receive advice or assistance with breastfeeding when they begin nursing (Savannakhet and Champasak). In Vientiane, health staff now commonly assist new mothers with BF within one hour and health professionals and mothers and mothers-in-law influence EBF and EIBF practices.
Older women in the family and health care providers are sources of information on EBF and infant feeding (Huaphan and Phongsaly).
In Huaphan, family income and encouragement from parents and relatives were significantly associated with breastfeeding; Lao mothers are highly influenced by their relatives in the decision-making process for/against breastfeeding, more so than health personnel.
What is the rate of predominant breastfeeding? What are the specific barriers and motivations to EBF in Project areas, as well as what are realistic approaches for mothers according to their situation (ie farmers)?

19
Recommended Behavior Current Practices, Motivations and Barriers to Improved Practice Gaps in Information (what do we need to know)
Continue frequent, on-demand breastfeeding until two years of age or beyond. (Reference 24, 15, 33, 11, 20)
Rural women continue breastfeeding longer than urban women. Women state economic reasons for breastfeeding and that it is the best they could do for their baby (Vientiane).
Continued breastfeeding is affected by the need for mothers to return to work (Luang Prabang).
In the absence of the mother, caregivers provide masticated rice and water, and in some cases canned or powdered milk (Savannakhet and Champasak).
Further information on barriers and motivations to continued breastfeeding and how it is possible to do, by region and socioeconomic group.
Start at six months of age with small amounts of food and increase the quantity as the child gets older, 200 kcal/day at 6-8 months; (Reference 21, 23, 27, 20, 24)
Studies in Vientiane, Attapeu, Saravane and Sekong indicate the over half of children are introduced to complementary foods at 6-7 months of age.
Children with educated mothers are more likely than children of non-educated mothers to be introduced to CF at the appropriate age.
Commonly introduced foods are rice and sugar (Huaphan and Phongsaly) and pre-masticated/mashed sticky rice (Phongsaly, Sekong, Khammouane). Mothers report introducing foods early due to having to return to work (Huaphan and Phongsaly).
Some parents use developmental milestones to decide when to initiate extra feeding.
What is the age of introduction in project communities, how do parents decide when the child is ready? What foods can be introduced and how? What changes related to mastication are mothers willing to try and how? Who can influence them?
Gradually increase food consistency as the infant gets older, adapting to the infant’s requirements and abilities. Infants can eat pureed or mashed foods starting at 6
CF starts with consuming a rice porridge and then parents gradually introduce other foods, such as small pieces of barbecued fish or meat (Luang Prabang).
Consume mainly rice with some vegetable and small fish (Luang Namtha and Sekong).
Mothers provide meat with rice soup, and steamed mash bananas (Phongsaly and Khammouane).
Consume meat, but more likely to consume fish (Savannakhet and Champasak).
Further detail on introduction of foods for children in project areas as well as what mothers are willing to try and how.

20
Recommended Behavior Current Practices, Motivations and Barriers to Improved Practice Gaps in Information (what do we need to know)
months; by 8 months semi-solids (Reference 18, 23, 27, 1, 20)
Feed 3-4 times/day (Reference 20)
Children are fed more often than adults, although it is often up to them to demand food. If they did not want to eat, parents described trying to coax them, threatening them or giving up and buying candy (Luang Prabang).
Feeding frequency, dependent on mother’s workload, particularly when mothers are working in the field away from the house.
Frequency of feeding information needed, as well as what families are willing and able to do, and how.
Feed a variety of foods: meat, poultry, fish or eggs daily; vitamin A-rich fruits and vegetables daily; diets with adequate fat content; avoid giving drinks/foods with low nutritive value (Reference 20, 18, 23, 27, 1, 33)
Children consume mainly rice with some vegetable and small fish (Luang Namtha and Sekong).
Mothers provide meat with rice soup, and steamed mash bananas as a food for children Phongsaly and Khammouane.
When food is scarce children may only consume rice (Huaphan and Phongsaly).
Few children in Attapeu, Saravane and Sekong found to be consuming adequately diverse diets.
Children from urban areas, with wealthy parents and educated mothers had the highest proportion of children meeting minimum dietary diversity (Attapeu, Saravane and Sekong).
Further detail on child dietary diversity and feeding practices (including what and how much food is fed by age of child, according to season) in project areas is needed, as well as what families are willing to change and how by age of child. Gender considerations?
By 12 months of age most young children should eat family foods (Reference 23, 27)
Some parents report waiting until 1 year of age to introduce more diverse foods, such as fruit due to lack of knowledge on how to prepare them for younger children, (Luang Prabang)
Lack of knowledge and awareness of foods to prepare for special meals for children affects food choices (Phongsaly, Khammouane and Sekong).
Identification of other barriers and motivations to introduce family foods by 12 months. Explore what families are willing to try and

21
Recommended Behavior Current Practices, Motivations and Barriers to Improved Practice Gaps in Information (what do we need to know)
how, and who can influence them on this practice.
Feeding During and After Illness and Health Care Seeking Practices
Increase fluid intake during illness, including more frequent breastfeeding, and encourage the child to eat more (Reference 23, 20)
Common for mothers to continue to breastfeed and for children to avoid certain foods during illness (Huaphan and Phongsaly).
Children may only be given rice and water, and children (and mothers) avoid spicy and sour foods.
Illness prevalence by type, season, age of child? More information on feeding (both breastfeeding and foods) during illness needed for project areas, in addition to what families are willing to change and how, by ethnic group.
Seek routine and sick child care at health facilities (Reference 30)
Strong preference to initially seek care from local providers. Mothers seek multiple sources for care and information, which results in patients leaving the health facilities before recovery and ending the recommended treatment prematurely. (Sekong and Savannakhet).
More information on care seeking and access and availability of health services in project areas, by ethnic group What are families willing to change and how? Whom do families trust /believe to encourage the changes?

22
Water, Sanitation and Hygiene Findings According to LSIS 2011/2012, WASH indicators vary across Lao PDR. Nationally, 70% of
households use improved sources of drinking water, however only 48% of households in
Savannakhet and 57% in Khammouane have access to improved sources. Of those who have
access to an unimproved source of drinking water, half (53%) of people nationally treat
drinking water compared to 39% in Khammouane and 25% in Savannakhet. Access to
improved, not shared, sanitation facilities in Khammouane and Savannakhet is 40%, also
lower than the national average of 57%. Access is a proxy for use, however having a latrine
does not necessarily mean that households and individuals use them, and open defecation
(OD) remains a common problem in USAID Nurture provinces. Furthermore, few households
dispose of child stools safely (by definition in an improved, not shared, latrine) (7% in
Khammouane and 10% in Savannakhet) compared to 19% nationally.
Table 6. Comparison of National and Provincial Level Data on WASH
Source: Lao PDR Social Indicator Survey (LSIS), 2011/2012.
WASH Behaviors Overview
The literature review included seven papers that addressed WASH practices related to
nutrition outcomes (Table 7). The information shows that behaviors vary across the country,
and no consistent patterns emerge. Water scarcity associated with low rates of
handwashing, arises as a problem for 59% of households in Northern provinces, 28% of
Central households and 12% in Southern provinces.26 Access to and use of latrines is
inconsistent; some reports indicate that even when households have latrines, open
defecation is still commonly practiced (Sekong, Champasak, Phongsaly,
26 Consumer research to inform rural sanitation behaviour change and marketing communications (2014) Emerging Markets Consulting for Lao PDR, WSP World Bank and MoH.
WASH National Khammouane Savannakhet
% of household population using improved drinking water sources
70 57 48
% of household members in households using unimproved drinking water sources and using an appropriate water treatment method
53 39 25
% of household population who have improved sanitation facilities that are not shared facilities
57 40 39
% of children age 0-2 years whose stools were disposed of safely the last time the child passed stools
19 7 10

23
Khammouane),27,28,29 while others indicate that households with latrines, used them
regularly. Convenience, durability, cleanliness and privacy all appear to be factors that
contribute to latrine use or desirability of ownership.30,31 Open defecation does not seem to
carry stigma in all regions. Overall, information on hygiene and handwashing practices
suggests some positive practices; one study from 7 provinces found that respondents
reported washing their hands before (97%) and after (82%) meals, however almost all of
them (97%) wash hands using water only; 55% of rural households in the North and 43% in
the Central regions use soap to wash their hands compared to only 9% in the South.32
27 Report of the Baseline Survey for the Maternal and Young Child Security Initiative (EU-UNICEF MYCNSIA) in Lao PDR, 2012 (2012) National Institute of Public Health, Department of Hygiene & Health Promotion, Ministry of Health UNICEF/Laos, European Union, with TA from the Global Center for Integrated Health of Women, Adolescents and Children/University of Washington. 28 Women, Food and Land: Understanding the impact of gender on nutrition, food security and community resilience in Lao PDR. Food Security Risk and Vulnerability Survey – Summary Report (2013) Stoeber S, Sisomphone E, Han C. Care International and National University of Laos. Vientiane, Lao PDR. 29 Development and Marketing of Affordable Technology Options for Sanitation in Lao PDR – Field Report. (2012). Pedi, D, Hahn, M, Nanthavong, K, Bounnaphol, S. World Bank’s Water and Sanitation Program and iDE. 30 Water, sanitation and hygiene: a situation analysis paper for Lao PDR Lahiri S and Chanthaphone S. (2003). International Journal of Environmental Health Research 13, S107-S114. 31 Consumer research to inform rural sanitation behaviour change and marketing communications (2014) Emerging Markets Consulting for Lao PDR, WSP World Bank and MoH. 32 Consumer research to inform rural sanitation behaviour change and marketing communications (2014) Emerging Markets Consulting for Lao PDR, WSP World Bank and MoH.

24
Table 7. Summary Matrix of Information on WASH Behaviors
Recommended Behavior Current Practices, Motivations and Barriers to Improved Practice Gaps in Information (what do we need to know)
Hygiene Practices
Wash caregivers’ and children’s hands before food preparation and eating (Reference 26)
Most report washing hands before and after meals—water only. One-third use soap. Use of soap varies by region, with the lowest use in the South. Most families have handwashing stations.
“Good hygiene was apparent in all four villages as participants emphasized the importance of hand washing before preparing meals and feeding children. This was facilitated by relatively easy access to water in three villages.” (Luang Prabang)
No in-depth information on handwashing at critical points or use of soap or ash for handwashing
Water and Sanitation Practices
Provide only safe drinking water (Reference 26, 33)
Water scarcity an issue in many households in Northern provinces; less so in central and southern regions. Most of the Northern and Southern households surveyed in mountainous regions get water from gravity-fed water supplies, while Central households fetch water from pumped wells.
Quality of water is an issue; common unimproved sources of drinking water are from surface water (river, stream, dam, lake, pond, canal, irrigation channel, unprotected wells, and unprotected springs).
Lao-Tai have access to improved drinking water and sanitation at about 2 times as often as other ethnic groups.
Further information about water access and availability and drinking water treatment in project provinces, districts and communities. Need an understanding about how families are willing to treat drinking water on a regular basis, by season, especially for children
25
Recommended Behavior Current Practices, Motivations and Barriers to Improved Practice Gaps in Information (what do we need to know)
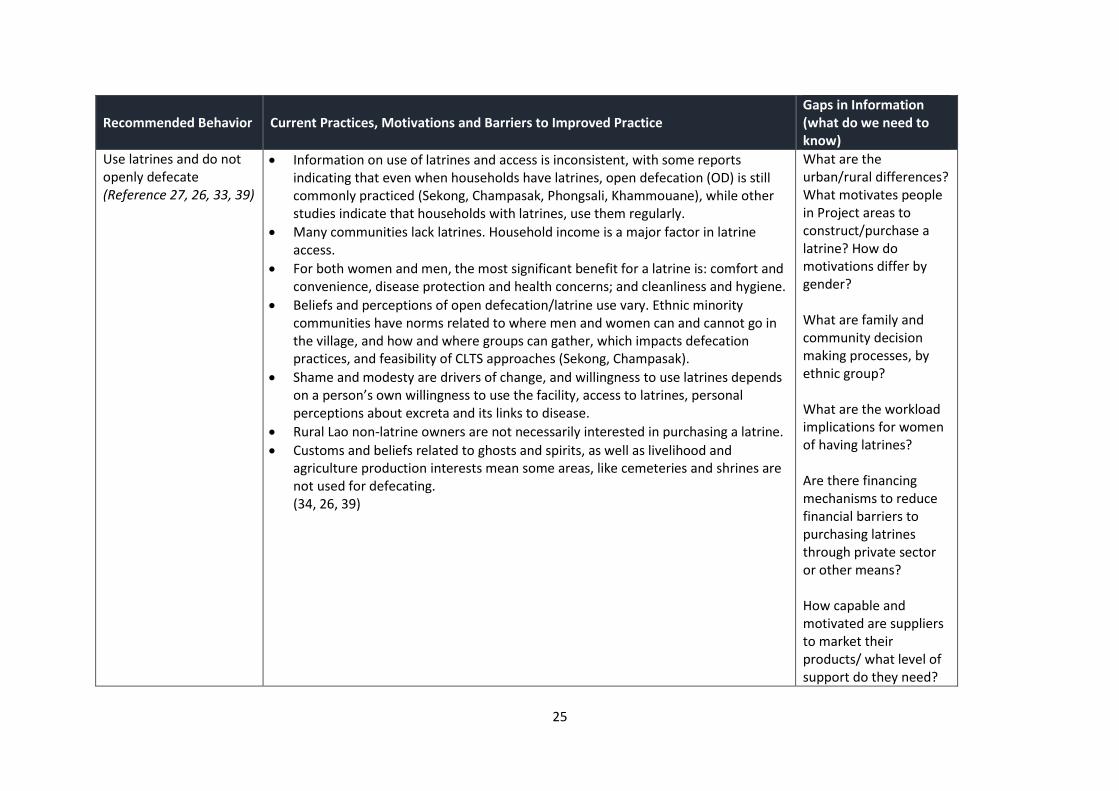
Use latrines and do not openly defecate (Reference 27, 26, 33, 39)
Information on use of latrines and access is inconsistent, with some reports indicating that even when households have latrines, open defecation (OD) is still commonly practiced (Sekong, Champasak, Phongsali, Khammouane), while other studies indicate that households with latrines, use them regularly.
Many communities lack latrines. Household income is a major factor in latrine access.
For both women and men, the most significant benefit for a latrine is: comfort and convenience, disease protection and health concerns; and cleanliness and hygiene.
Beliefs and perceptions of open defecation/latrine use vary. Ethnic minority communities have norms related to where men and women can and cannot go in the village, and how and where groups can gather, which impacts defecation practices, and feasibility of CLTS approaches (Sekong, Champasak).
Shame and modesty are drivers of change, and willingness to use latrines depends on a person’s own willingness to use the facility, access to latrines, personal perceptions about excreta and its links to disease.
Rural Lao non-latrine owners are not necessarily interested in purchasing a latrine.
Customs and beliefs related to ghosts and spirits, as well as livelihood and agriculture production interests mean some areas, like cemeteries and shrines are not used for defecating. (34, 26, 39)
What are the urban/rural differences? What motivates people in Project areas to construct/purchase a latrine? How do motivations differ by gender? What are family and community decision making processes, by ethnic group? What are the workload implications for women of having latrines? Are there financing mechanisms to reduce financial barriers to purchasing latrines through private sector or other means? How capable and motivated are suppliers to market their products/ what level of support do they need?

26
Recommended Behavior Current Practices, Motivations and Barriers to Improved Practice Gaps in Information (what do we need to know)
What Socioeconomic factors are associated with OD/latrine ownership?

27
Annotated Reference List
Maternal Nutrition
1. Beriberi (Thiamine Deficiency) and High Infant Mortality in Northern Laos (2015) Barennes H, Sengkhamyong K René J.P., Phimmasane M. Plos Negl Trop Dis 9(3): 1-16.
Cross-sectional study conducted between 2007 and 2010 with mothers of thiamine deficient infants in 22 villages in Luang Namtha Province. Mothers in villages with confirmed cases of beriberi had combinations of all risk factors described for thiamine
deficiency─farmers, predominantly illiterate, low family income, poor dietary diversity and almost all respected food avoidances during the postpartum period.
2. Insect Consumption to Address Undernutrition, a National Survey on the Prevalence of
Insect Consumption among Adults and Vendors in Laos (2015) Barennes H, Phimmasane M, Rajaonarivo C. PloS ONE 10(8): e0136458.
Survey in 1303 households and insect vendors (3 per village) in 96 villages in 16 Lao provinces. Survey found that for the majority of households consumption of insects was infrequent. Respondents would have eaten more insects if they had been available. Consumption of insects started in childhood. Hmong and Leu ethnic groups had significantly lower consumption levels than the general population.
3. Progressive growth deterioration in a context of nutritional transition: A case study from Vientiane (Lao PDR) (2012) Benefice E, Levi P, Banouvong P Annals of Human Biology 39(3): 239-246.
Food frequency questionnaire and 24-hour dietary recall with mothers (either pregnant or who had just given birth) and anthropometric measurements of infants in Vientiane. Dietary energy content was low and the main energy source was rice. But there was great diversity of foods and recipes. Level of urbanization contributed to differences in energy intake and food diversity. Stunting was 14% in infants. Stunting was related to age, the sex of the child, the mother’s physique and level of urbanization.
4. Steam sauna and mother roasting in Lao PDR: practices and chemical constituents of essential oils of plant species used in postpartum recovery (2011) de Boer H. J, Lamxay V, Bjork L. BMC Complementary and Alternative Medicine, 11:128.
Semi-structured interviews conducted with 67 women of 4 different ethnic groups (Alo, Saek, Brou, Kry, Phong) between 2005 and 2010 in 15 rural villages in Khammouane Province and Vientiane prefecture. All informants reported postpartum recovery customs and rituals. Describes in detail confinement rituals, hotbed, steam sauna and mother roasting.
5. Factors Affecting Low Birth Weight at Four Central Hospitals in Vientiane, Lao PDR (2010) Louangpradith V, Yoshida, Yoshitoku Y, Harun-Or-Rashid MD, Sakamoto J. Nagoya Journal of Medical Science. 72: 51058.

28
Case-control study in 2008 with 235 mothers of low birth weight babies and 265 mothers of normal birth weight babies from 4 central hospitals in Vientiane province. Significant associations with low birth weight were found for delivery at age less than 18 years, low family income, physical labor during, and first child birth. Mothers with an inadequate level of knowledge regarding healthy pregnancy and those lacking adequate nutrition practices were at higher risk of developing low birth weight babies.
6. Plants used during pregnancy, childbirth and postpartum healthcare in Lao PDR: A comparative study of the Brou, Saek and Kry ethnic groups (2009) de Boer H, Lamxay V Journal of Ethnobiology and Ethnomedicine 5(25): 1-10.
Individual and group interviews conducted between 2005 and 2007 with 38 women in Saek, Brou and Kry ethnic groups in 10 villages in Khammouane province. Found that medicinal plant use is common among the Brou, Saek and Kry to facilitate childbirth, alleviate menstruation problems, assist recovery after miscarriage, mitigate postpartum hemorrhage, aid postpartum recovery, and for use in infant care.
7. Dietary and socio-economic factors associated with beriberi in breastfed Lao infants (2003) Soukalouna D, Kounnavongb S, Pengdya B, Bouphab B, Durondejc S, Olnessd K, Paul N. Newtone P.N, White N.J. Annals of Tropical Paediatrics 23, 181–186.
Prospective case-control study in 1993 with 43 breastfeeding infants with beriberi with 43 matched controls in 3 public hospitals in Vientiane. Clinically significant thiamine deficiency in breastfed infants in Lao relates to methods of preparing rice, the food selected by lactating mothers and the family's socio-economic status.
Infant and Young Child Feeding (IYCF)
8. Implementation of International Code of Marketing of Breastmilk Substitutes in Lao PDR (2015) Phongluxa K, Philavong K, Lathsavong K, Phasavath B, Choummaly C, Mikhasith V, Phomsouvanh P, Sampson L. Presented as oral presentation at the 9th National Health Research Forum, 2015. Funded by Save the Children Australia.
Cross-sectional descriptive study in 2014 that included interviews with hospital directors, health staff, mothers of children under six months at 13 hospitals at the provincial, district and central levels, together shop observations and interviews with shop owners. Eight of the 13 hospitals were classified as ‘baby friendly hospitals’ but 50% of these hospitals introduced formula in the child’s first six months. Bottle feeding common among mothers who left home for working and a variety of milk products were available at the shops.
9. Cross-border Formula Milk Promotion in Lao People’s Democratic Republic and Its
Effect on Maternal Attitudes Towards Breastfeeding (2014) Phoutthkaeo, P, Otsuka K, Ito C, Sayamounghoun P, Kounnavong S, Jimba M. J Paediatr Child Health 50(1):51-6.
Cross-sectional survey in 2011 that included face-to-face structured questionnaire and focus group discussions of 1241 mothers who had children under 2 years of age in 42

29
villages in Vientiane. Found prevalence of exclusive breastfeeding for 6 months was 16% and complementary feeding at one year was 60%. 90% of respondents reported frequent exposure to promotion of formula milk through TV commercials and 79% identified TV commercials as influential for them to develop a positive attitude towards the use of formula milk. Mothers who showed a positive response to the commercial on formula use were approximately 75% less likely to practice exclusive breastfeeding for 6 months than those who reported a negative attitude.
10. Key Determinants of Optimal Breastfeeding Practices in Laos (2013) S. Kounnavong S,
Pak-Gorstein K, Akkhavong U, Palaniappan V, Berdaga J, Conkle J, Gorstein J. Food and Nutrition Sciences, 4: 61-70.
Statistical analysis of LSIS and MYCNSIA survey data conducted in 2011/12 with 4322 children aged 6-23 months in Attapeu, Saravane and Sekong. This study looked at early initiation of breastfeeding and avoidance of pre-lacteal feeds by demographics – age, level of education, ethnicity (Khmer, Hmong, Lao-Tai), religion, household wealth index, residence and region.
11. A qualitative study on the breastfeeding experiences of first-time mothers in
Vientiane, Lao PDR (2013) Mei Hong Lee H, Durham J, Booth J, Sychareun V. BMC Pregnancy and Childbirth 13:223.
Qualitative research that included focus group discussions with Lao Loum first-time mothers and in-depth interviews with key informants in 2 districts in Vientiane. This study explored the reasons and influences behind first-time mothers' breastfeeding practices, as well as the role of attitudes, beliefs and experiences in influencing those practices. Participants demonstrated positive attitudes towards breastfeeding and recognized its importance. Despite this, breastfeeding practices were suboptimal.
12. Factors Influencing Nutritional Status of Minority Ethnic Groups in Southern Laos
Peoples Democratic Republic - What to Promote? Presentation at 13th World Congress on Public Health, April 26, 2012 by Kym D. Blechynden University of Tasmania, Australia
18 focus groups, 6 community interviews and 3 market audits in villages where the Feeding the Future project is being carried out (a community nutrition program promoting culturally appropriate and locally available foods to prevent malnutrition) in 10 villages in 3 provinces in Southern Laos. Food taboos, dietary practices and perceptions of malnutrition were identified for nine different ethnic groups.
13. Breast-Milk Substitutes: A New Old-Threat for Breastfeeding Policy in Developing
Countries. A Case Study in a Traditionally High Breastfeeding Country (2012) Barennes H, Empis G, Quang T.D, Sengkhamyong K, Phasavath P, Harimanana A, Sambany E.M, Koffi P.N. PLoS ONE 7(2): e30634.
A randomized, multi-stage sampling survey in 2009 with 1057 mothers with infants under 24 months of age 90 villages in 12 provinces in Laos (not including Khammouane or Savannakhet). Found 73% of children were currently breastfed and 25% had been

30
given BMS. Thai television was the main source of information on BMS for mothers. Found Lao mothers were highly influenced by their relatives in the decision making process for/against breastfeeding.
14. Anemia and Related Factors in Preschool Children in the Southern Rural Lao People’s
Democratic Republic (2011) Kounnaving S, Sunahara T, Hashizume M, Okumura J, Moji K, Boupha B, Yamamoto T. Tropical Medicine and Health. 39(4): 95-103.
Population-based cross-sectional survey in 2009 of 331 pre-school children in 6 villages in Savannakhet (Songkhone district – 6 villages: Muangkhai, Kouthi, Lahakhok, Lahanam, Thakhamlian, Bengkhamlai). 40% children stunted, 7% wasted, 27% underweight and 49% anemic. 74% never breastfed. 27% deworming and 64% diarrhea or cough. Rates also disaggregated by village. For anemia there was no protective effect of BF. Prevalence was higher in children: aged 6-23 months; with large families (6 or more members); and in remote villages with difficult access to markets.
15. Factors influencing breastfeeding in children less than 2 years of age in Lao PDR (2009)
Putthakeo P, Ali M, Vilayhong P, Kuroiwa C, Journal of Paediatrics and Child Health 45: 487–492.
Cross-sectional survey in 2007 with 400 mothers in 40 villages in Vientiane capital and Vientiane province. The prevalence of exclusive breastfeeding at 6 months was 19%. Some of the factors influencing exclusive breastfeeding at 6 months included: location of residence, ethnicity, encouragement of the child’s father and inter-spousal communication. A majority of the mothers (75%) had watched television advertisements for infant formula from Thailand and 48% said they wanted to buy formula after watching them.
16. Misperceptions and misuse of Bear Brand coffee creamer as infant food: national cross
sectional survey of consumers and paediatricians in Laos; (2008) Barennes H, Andriatahina T, Latthaphasavang V, Anderson M, Srour L.M. BMJ 337: 1-4.
Questionnaires with 1098 households and 26 interviews with pediatricians in 84 villages in South, Central, and northern Laos. The Nestle Bear Brand coffee creamer is used as a breastmilk substitute in Laos. The cartoon logo influences people’s perception of the product that belies the written warning “this product is not to be used as a breastmilk substitute”. Most adults believe the product contains milk and almost half believe it is formulated for infant feeding.
17. Risk factors for protein–energy malnutrition in children under 5 years: Study from
Luangprabang province, Laos (2007) Phengxay M, Ali M, Yagyu F, Soulivanh P, Kuroiwa C, Ushijima H. Pediatrics International 49(2): 260-265.
Cross-sectional study conducted in 2004 with 798 children under 5 and their mothers Luang Prabang province. High prevalence of stunting, underweight and wasting (55%, 35%, 6%). Children aged 12–23 months and Khmu and Hmong ethnic children had a higher prevalence of stunting (65% and 66%) and underweight (45% and 40%),

31
respectively. It was also found that boys were more prone to be stunted and underweight. Restricted intake of meats and vegetables during illness and low maternal education affect children’s stunting and underweight.
18. Nutritional status of children in rural Lao PDR: who are the most vulnerable? (2005)
Miyoshi M, Phommasack B, Nakamura S and Kuroiwa C. European Journal of Clinical Nutrition (2005) 59, 887–890.
Cross-sectional study in 2001 with 1075 children aged 3-15 years old in remote villages Luangnamtha and Sekong provinces. Prevalence of stunting was 74% in Luangnamtha and 63% in Sekong province, with school-age children worse-off than under-fives. Children's diets were inadequate in quality as well as in quantity, with very limited availability of rice and other food items throughout the year.
19. Psychosocial Factors Related to Practicing Exclusive Breastfeeding among Mothers of
Infants 4-12 Months Old in Huamuang District, Huaphanh province, Laos (2003) Chanthalangsay S, Isaranurug S, Nanthamongkolchai S, Swongsawass S. Journal of Public Health and Development 1(2): 32-39.
Cross-sectional study in 2003 with 265 mothers of infants 4-12 months of age in Huamuang District, Huaphan Province. This study identified psychosocial factors related to practicing exclusive breastfeeding. Family income and encouragement from parents and relatives were significantly associated with breastfeeding. Husbands were the main support for household chores during the postpartum period. Health providers were the main resource for providing information about exclusive breastfeeding. Returning to work and getting pregnant again were the main reasons for mothers to quit exclusive breastfeeding.
Maternal and IYCF
20. Identifying priorities to improve maternal and child nutrition among the Khmu ethnic
group, Laos: a formative study (2012) de Sa J, Bouttasing N, Sampson L, Perks C, Osrin
D, Prost A. Maternal & Child Nutrition 9(4): 452-466.
MICS 2006 data and focus group discussions and semi-structured interviews in 2010
with villagers and health care workers in 2 villages with majority Khmu ethnicity in 2
rural districts of Luang Prabang (one with the Primary Health Care (PHC) project). Found
a higher prevalence of stunting in the Khmu and Hmong than the ethnic minority groups
when MICs data was disaggregated. Nutrition behaviors were associated with ethnicity.
Villagers described a strong adherence to post-partum food restrictions while little
change was described during intake during pregnancy. Most children were breastfed,
although early introduction of pre-lacteal foods was noted in the non-PHC district.
Widespread variation in introduction to and diversity of complementary foods.
21. Postpartum traditions and nutrition practices among urban Lao women and their
infants in Vientiane, Lao PDR (2009) Barennes, C Simmala C, Odermatt P, Thaybouavone

32
T, Vallee J, Martinez-Ussel B, Newton P N, Strobel M. European Journal of Clinical
Nutrition 63: 323–331.
A cross-sectional study in 2005 with 300 pairs of infants under 6 months of age and their
mothers from 41 randomly selected villages on outskirts of Vientiane. Found 10% of
children were stunted, 9% underweight and 10% wasted. Information was collected
about pregnancy, delivery and traditional practices. Found high ANC attendance and
delivery under health professional supervision. But also found a high prevalence of
traditional postpartum restricted diets and practices and inadequate maternal nutrition
and IYCF practices.
22. Maternal Eating Practices and Infant Feedings in a Laos People’s Democratic Republic
Rural Area. (2009) Bouphavanh K, Vongkhily S, Xayyalath B, Ongroongruang S.
Thammasat Medical Journal. 9(2): 130-139.
Cross-sectional, descriptive study in 2008/9 with 112 mother-infant pairs (postpartum
mothers and mothers of 0-1 year-old infants) in Muang-Fueng district, 136 kilometers
from Vientiane. All mothers underwent hot bed exposure and during this period diet
was restricted. Two factors, religion of spirit and incomplete ANC, were found associated
with longer duration of hot bed exposure. Almost all infants were breastfed within one
hour of birth, given colostrum and exclusive breastfeeding until 4 months of age. At 6-7
months, 61% of children were given complementary foods.
23. Influences on maternal and child nutrition in the highlands of the northern Lao PDR
(2007). Holmes W, Hoy D, Lockley A, Thammavongxay K, Bounnaphol S, Xeuatvongsa A,
Toole M. Asia Pac J Nutr 16(3): 537-545.
Focus group discussions, key informant interviews and structured observations in 2002 with village leaders, health volunteers, traditional birth attendants and healers, and leaders of the Women’s Union, and male and female villagers in 8 villages in Huaphan and Phongsaly provinces. Ethnic groups were Hmong, Khmu, Phuthai and Yao in Huaphan province and Akha, Khmu, Lue and Phunoi in Phongsaly province. Influences on maternal and child nutrition were found to be food availability, beliefs and practices about eating during pregnancy, beliefs and practices about eating post-partum, and infant feeding practices. Found that often people did not know the reason for a taboo.
24. Consulting with Caregivers – Using Formative Research to Improve Maternal and
Newborn Care and Infant and Young Child Feeding in the Lao People’s Democratic
Republic. (2004) Gillespie A, Creed-Kanashiro H, Deuanesay S, Sayakoummane, Galloway
R. The World Bank Health Nutrition and Population Discussion Paper. The World Bank:
Washington DC.
Knowledge, Attitudes Practices (KAP) survey, qualitative interviews and a diet re-call
with mothers and family members from three ethno-linguistic groups (Hmong-Yao,
Austro-Asiatic, Tai-Kadai) in 4 villages in Savannakhet and Champasak. Found that all
groups have prescribed and proscribed foods for new mothers. Newborns are given pre-
lacteal foods and liquids, usually masticated rice or water instead of colostrum. All

33
infants are breastfed on average for two years but few exclusively breastfeed. All but the
Hmong-Yao group introduce complementary foods before the infants fifth month of life.
Multiple Themes—Maternal, IYCF, WASH, Health Services, Gender
25. Lack of community-level improved sanitation causes stunting in rural villages of Lao
PDR and Vietnam. (2014) Quattri M, Smets S. Conference Paper. 37th WEDC
International Conference, Hanoi, Vietnam.
Regression analysis of MICS and LSIS data to look at the relationship between height and sanitation in children under five from rural villages in Lao PDR and Vietnam. Unimproved sanitation in rural villages leads to shorter children in those villages. Neighbor’s poor sanitation negatively affects a child’s height even when the child’s family uses improved facilities. Local poor sanitation causes children to be shorter than average at every age.
26. Consumer research to inform rural sanitation behaviour change and marketing
communications (2014) Emerging Markets Consulting for Lao PDR, WSP World Bank and
MoH.
Mixed-methods approach with qualitative and quantitative aspects (household surveys, focus groups discussions, in-depth interviews) in 2014 with 1,281 households in 84 villages in 7 provinces, including Savannakhet (Atsaphone, Pin & Xonbouri districts). Among rural, poor households: 63% openly defecate; 89% of latrine owners clean latrines at least once per week; 22% dispose of infant feces in the latrine; 35% wash hands using soap. Describes opportunity, ability and motivation determinants for sanitation behaviors.
27. Women, Food and Land: Understanding the impact of gender on nutrition, food
security and community resilience in Lao PDR. Food Security Risk and Vulnerability
Survey – Summary Report (2013) Stoeber S, Sisomphone E, Han C. Care International
and National University of Laos. Vientiane, Lao PDR.
Fieldwork and focus group discussions or interviews with 214 participants in 2012. Men and women in 9 villages in 3 provinces - Phongsaly, Sekong, Khammouane (Nyommalath district in Phanesaed, Nafamimai and Natherd villages). Detailed description and analysis of qualitative data around food availability, dietary diversity, complementary feeding practices, maternal nutrition, gender dynamics.
28. Provider perspectives on constraints in providing maternal, neonatal and child health
services in the Lao People’s democratic republic: a qualitative study (2013) Sychareun
V, Phommachanh S, Soysouvanh S, Lee C, Kang, M, Oh J, Durham J. BMC Pregnancy and
Childbirth 13:243.
Interviews with 27 hospital providers, 8 health center staff and 10 village health
volunteers in 2012 in Xiengkuang, Huaphan and Salavane provinces. Supply-side
constraints related to inadequate human resources, poor remuneration, weak technical
guidance, minimal supervision and limited equipment. Demand-side constraints related
mainly to cost, limited access to transport, cultural practices and languages. Contextual

34
constraints included low levels of limited education, women’s position in society and
poor transport and communications networks.
29. Lao People’s Democratic Republic Maternal Health, Child Health and Nutrition in Lao
PDR – Evidence from a Household Survey in Six Central and Southern Provinces. (2013)
Boudreaux C, Tandon A, Yap, W A. World Bank: Washington DC.
Household survey in 2010 with 2741 households with a child under two in 193 villages across 21 high-priority and/or poor districts in the Bolikhamxay, Khammouane, Savannakhet, Saravane, Champasak, and Attapeu provinces. 51% of the sample was Lao-Tai, 44% Mon-Khmer, and 3% Hmong-Mien. 36% children were stunted and 14% were wasted. 29% of Lao-tai, 43% Mon-Khmer, 40% Mon-Hmong were stunted and 11%, 17% and 13% were wasted, respectively. The survey also captured: dietary diversity; service utilization for ANC; PNC and delivery; care for mothers; and breastfeeding practices.
30. Coping with uncertainty during healthcare-seeking in Lao PDR (2013) Alvesson H M,
Lindelow M, Khanthaphat B, Laflamme L, International Health and Human Rights 13:28.
Interviews and focus groups discussions with mothers and fathers of children under 5, caregivers of sick children, traditional healers, drug vendors, CHWs, nurses and doctors in 6 villages in Sekong and Savannakhet provinces. Care-seekers expressed a strong preference for initially seeking local providers. Subsequently, multiple providers were consulted to increase chances of recovery. There was a strong desire to be responsible caregiver and of show respect for household norms. In general, healthcare-seeking was shrouded in uncertainty.
31. The Gender and Equity Implications of Land-Related Investments on Land Access and
Labour and Income-Generating Opportunities – A Case Study of Selected Agriculture
Investments in Lao PDR (2013) Daly E, Osorio, M, Mi Youg Park C. Food and Agriculture
Organization of the United Nations: Rome.
Focus group discussions with local farmers and agriculture works in 10 villages in
Bolikhamxay province, Vientiane province and Vientiane Capital and a literature review.
Women in rural Laos are traditionally responsible for family finances and for the
household food security and nutrition. Women traditionally do most of the farm work
and also spend long hours performing off-farm household chores. Some ethnic
minorities are widely considered more open in terms of gender relations, particularly
among Lao Loum, but some are more repressive for women. Domestic violence is a
serious issue throughout the country.
32. Reasons rural Laotians chose home delivery over delivery at health facilities: a
qualitative study (2012) Sychareun V, Hansana V, Somphet V, Xayavong S, Phengsavanh
A, Popenoe R. BMC Pregnancy and Childbirth 12:86.
Qualitative study with interviews and focus group discussions in 2008/9 with 71
mothers, husbands and grandmothers in Khammouane and Champasack provinces.
Obstacles to giving birth at health facilities included: (1) distances to health facilities and

35
difficulties and costs of getting there; (2) attitudes, quality of care, and care practices at
health facilities; (3) the wish to have family members nearby; (4) the wish to follow
traditional birth practices.
33. Report of the Baseline Survey for the Maternal and Young Child Security Initiative (EU-
UNICEF MYCNSIA) in Lao PDR, 2012 (2012) National Institute of Public Health,
Department of Hygiene & Health Promotion, Ministry of Health UNICEF/Laos, European
Union, with TA from the Global Center for Integrated Health of Women, Adolescents
and Children/University of Washington.
EU-UNICEF MYCNSIA baseline combined data from the National Lao Social Indicator
Survey (LSIS) and a supplementary EU-UNICEF MYCNSIA ‘add-on’ survey, both
conducted between October 2011 and February 2012 in Attapeu, Saravane and Sekong.
Describes behaviors around BF, complementary feeding, dietary diversity and WASH
disaggregated by geography, urban/rural, religion, wealth and mother education.
34. Development and Marketing of Affordable Technology Options for Sanitation in Lao
PDR – Field Report. (2012). Pedi, D, Hahn, M, Nanthavong, K, Bounnaphol, S. World
Bank’s Water and Sanitation Program and iDE.
Field Report that includes a Demand Assessment with 28 in-depth consumer interviews
of female and male latrine owners and non-owners in Tatheng District in Sekong
Province and Bachieng District in Champasak Province. Open defecation (OD) was the
social norm and a very common practice, the overwhelming practice in some villages.
There did not appear to be a social stigma around OD. But OD is also considered an
unpleasant experience and households are motivated to build a toilet to avoid OD.
35. Socioeconomic Determinants of Nutritional Status of Children in Lao PDR: Effects of
Household and Community Factors (2011) Kamiya Y. Journal of Health Population and
Nutrition 29(4): 339-348.
Paper investigated the effects of socioeconomic factors at both household and
community levels on the nutritional status of Lao children under 5 using MICS 3 dataset.
Children from the ethnic Lao group were better nourished than the other ethnic groups
(Khmu, Hmong, others). Children from households in Southern Laos were less-
nourished. Level of education of parents, attitudes of mothers towards domestic
violence, assets of household, local health services, and the condition of sanitation and
water were considered to be important determinants of nutritional status of children.
36. Antenatal care among ethnic populations in Louang Namtha Province, Lao PDR (2010)
Phathammavong O, Ali M, Souksavat S, Chounramany K, Kuroiwa C Southeast Asian J
Trop Med Public Health 41(3): 705-716.
Cross-sectional survey in 2008 with 620 mothers of children under five years of age in
the Viengphukha district, Louang Namtha province. 23% of mothers had at least one
ANC visit but only 5% had four or more ANC visits for their last pregnancy. ANC visit

36
rates were lower in highland mothers and less educated mothers. ANC visits enhanced
hospital deliveries and child immunizations.
37. Cultural Beliefs and Traditional Rituals About Childbirth Practices in Lao PDR (2009)
Sychareun V, Phengsavanh A, Hansana V, Somphet V, Sysouvanh, Menorath S. Kuala
Lumpar, Malaysia: The Asian-Pacific Resource & Research Centre for Women (ARROW).
Qualitative research methods in 2008/9 with focus group discussions and in-depth
interviews of women who delivered at home, family members, traditional birth
attendants, head villagers, and Lao women’s union representatives in 2 districts in
Champasack province and Khammouane province (Thakek and Mahaxay districts).
Outlines socio-cultural beliefs and practices on child births, particularly home births and
gender aspects of birth practices. Describes ‘mother roasting’ (or “Yum Kam” or “Yu
Fai”), the belief the baby should drink water immediately after birth, and the influence
of husbands and grandmothers on a women’s child birth practices.
38. Maternity waiting homes in Southern Lao PDR: The unique ‘silk home’ (2008)
Eckermann E, Deodato D J Obstet Gynaecol Res 35(5): 767-775.
Focus group discussions and individual interviews with villagers, traditional birth
attendants, midwives and village health committee members in 18 villages in Thateng
district, Sekong province. Most births took place in the village with only 10% of mothers
giving birth in hospitals. Women desire to give birth in the traditional squatting position,
have their own foods post-partum, and have fire or source of heat after birth.
Geographic and economic barriers prevent women using the health system.
39. Water, sanitation and hygiene: a situation analysis paper for Lao PDR Lahiri S and
Chanthaphone S. (2003). International Journal of Environmental Health Research 13,
S107-S114.
Participatory assessment in 2002 with men and women in 37 villages in 8 provinces that
received hygiene sanitation and wash supply support from various NGOs. The findings
confirmed some beliefs and dismissed others. Key findings were that household
behavior change in the use of latrines depend upon: a person’s own willingness to use
the facility; access to latrines; and personal perceptions about excreta and its links to
disease.
40. Advantages of trained TBA and the perception of females and their experiences with
reproductive health in two districts of the Luangprabang province, Lao PDR (2003)
Sirivong A, Silphong B, Simphaly N, Phayasane T, Bonouvong V, Schelp F Southeast Asian
J Trop Med Public Health 34(4): 919-928.
Closed questionnaire in 2000 with 298 women who had children under 2 in 30 villages in
Xieng Ngeun and Pakou districts in Lunag Prabang province. Most women belonged to
Lao Sung or Lao Lum ethnic groups with less than 8% belonging to Lao Theung. Over 80%
of women gave birth at home. The distance of homes from the community hospital

37
played a major role in whether women were more likely to participate in ANC, give
colostrum to their newborns and disregard food taboos.


















