Improving nutrition through local agricultural biodiversity in kenya
Upload
nguyennhanCategory
view
237download
5
USAID KENYA NUTRITION AND
HEALTH PROGRAM PLUS
QUARTERLY PROGRESS REPORT
JULY 2016
This publication was produced for review by the United States Agency for International Development. It was prepared by Kenya Nutrition and Health Program plus

USAID KENYA NUTRITION AND
HEALTH PROGRAM plus
FY 2016 Q3 PROGRESS REPORT
APRIL 1–JUNE 30, 2016
Award No: AID-615-H-15-00001
Prepared for Ruth Tiampati
United States Agency for International Development/Kenya
C/O American Embassy
United Nations Avenue, Gigiri
P.O. Box 629, Village Market 00621 Nairobi, Kenya
Prepared by
Nutrition and Health Program plus
2nd Floor Chancery Building, Valley Road
P.O Box 38835 00623
Nairobi, Kenya
DISCLAIMER The authors’ views expressed in this report do not necessarily reflect the views of the United States Agency for
International Development or the United States Government.

i
USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
I. NUTRITION AND HEALTH PROGRAM PLUS
EXECUTIVE SUMMARY ................................................ iv
I. Background ......................................................... 1
II. KEY ACHIEVEMENTS (Qualitative Impact) ............ 1
III. ACTIVITY PROGRESS (Quantitative Impact) ...... 10
IV. CONSTRAINTS AND OPPORTUNITIES ............. 18
V. PERFORMANCE MONITORING ............................ 18
VI. PROGRESS ON ENVIRONMENTAL
MITIGATION AND MONITORING ............................ 20
VII. PROGRESS ON LINKS TO OTHER USAID
PROGRAMS .................................................................... 20
VIII. PROGRESS ON LINKS WITH GOK
AGENCIES ...................................................................... 20
1X. SUBSEQUENT QUARTER’S WORK PLAN ........ 21
X. FINANCIAL INFORMATION .................................. 24
XI: ANNEXES & ATTACHMENTS: ............................. 25

USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
ACRONYMS AND ABBREVIATIONS AIDS Acquired Immune Deficiency Syndrome
AMPATH Academic Model for Providing Access to Healthcare
APHIAplus AIDS, Population and Health Integrated Project
ART Antiretroviral Therapy
CBO Community-Based Organization
CCC Comprehensive Care Centers
CDC Centers for Disease Control
CHANIS Child Health and Nutrition Information System
CHEW Community Health Extension Worker
CHV Community Health Volunteer
CLTS Community-Led Total Sanitation
CNTF County Nutrition Technical Fora
CO Country Office
COP Chief of Party
CRISP Central Regional Integrated Program
CU Community Health Unit
DCOP Deputy Chief of Party
DHIS District Health Information System
EDL Economic Development and Livelihoods
EmOC Emergency Obstetric Care
EMR Electronic Medical Records
EMMP Environmental Mitigation and Monitoring Plan
ENA Essential Nutrition Actions
EPZ Export Processing Zone
FAFSA Food Aid and Food Security Assessment
FANTA Food and Nutrition Technical Assistance Project
FAO Food and Agriculture Organization
FBF Fortified Blended Food
FBP Food by Prescription
FFP Food for Peace
FHI Family Health International
FtF Feed the Future
GAIN Global Alliance for Improved Nutrition
GIS Geographic Information System
GMP Good Manufacturing Practice
GOK Government of Kenya
HACCP Hazard Analysis and Critical Control Points
HEA Household Economic Assessment
HFP Household Food Production
HiNi High impact Nutrition interventions
HIV Human Immunodeficiency Virus
HNDU Human Nutrition and Dietetics Unit
HTC HIV Testing and Counseling
IMAM Integrated Management of Acute Malnutrition
IP Implementing Partner
IR Intermediate Result

USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
IYCF Infant and Young Child Feeding
IYCN Infant and Young Child Nutrition
KARI Kenya Agriculture Research Institute
KEBS Kenya Bureau of Standards
KDHS Kenya Demographic and Health Survey
KEMSA Kenya Medial Supplies Authority
KFDA Kenya Food and Drug Administration
KHCP Kenya Horticultural Competitiveness
KNDI Kenya Nutritionists and Dieticians Institute
KPPB Kenya Pharmacy and Poisons Board
LMIS Logistics Management Information System
M&E Monitoring and Evaluation
MEDS Mission for Essential Drugs and Supplies
MIYCN Maternal and Child Health Integrated Program
MNCH Maternal Newborn and Child Health
MOH Ministry of Health
MT Metric Ton
NACS Nutritional Assessment, Counseling and Support
NASCOP National AIDS and STI Control Program
NFSNSC National Food and Nutrition Security Secretariat
NHP Nutrition and HIV Program
NHPplus Nutrition and Health Program Plus
NICC Nutrition Interagency Coordinating Committee
NNAP National Nutrition Action Plan
NSR Nutrition Service Register
OR Operations Research
ORT Oral Rehydration Therapy
OVC Orphans and Vulnerable Children
PEPFAR President’s Emergency Program for AIDS Relief
PLHIV People Living with HIV
PAC Project Advisory Committee
PMEP Performance Monitoring and Evaluation Plan
PMTCT Prevention of Mother-To-Child Transmission of HIV
QA/QI Quality Assurance / Quality Improvement
RUTF Ready-to-use Therapeutic Food
SBC Social Behavior Change
SCNTF Sub-County Nutrition Technical Fora
SMT Senior Management Team
SUN Scaling Up Nutrition
TA Technical Assistance
TWG Technical Working Group
USAID United States Agency for International Development
WASH Water, Sanitation and Hygiene WFP World Food Program

USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
I. NUTRITION AND HEALTH PROGRAM PLUS EXECUTIVE SUMMARY
Nutrition and Health Program plus is a five-year program running from January 1, 2015 to December
31, 2019. The program purpose is to increase access and demand for nutrition services, and improve
food and nutrition security as well as commodity management support. The program funding is from
three different streams: PEPFAR for commodity management support, Feed the Future (FtF) for
improving food and nutrition security, and MNCH/Nutrition for implementing MNCH interventions
that ensures greater effect for women and children under two years with regard to nutrition. Feed
the Future (FtF) activities are implemented in the Counties of Busia, Tharaka Nithi, Kitui, Samburu and
Marsabit, while MNCH activities are implemented in the counties of Busia, Tharaka Nithi, Kitui, and
Marsabit. Commodity management support is provided across all the 47 counties in Kenya. During
the period of April 1 through June 30, 2016, the program made progress towards achieving its
objectives. Details the project’s accomplishments, successes and challenges faced are summarized below.
Towards improving access and demand for quality nutrition interventions at community and facility
levels, a concept note has been developed to conduct Kenya PROFILES on nutrition. PROFILES uses
models and country-specific data to project the economic and health consequences of not adequately
addressing a country’s nutrition problems, illustrating what the negative consequences would be with
no improvement and no change in nutrition problems over a defined time period. It simultaneously
estimates the benefits of improved nutrition over the same time period, including lives improved and saved and economic productivity losses averted.
In the counties of Kitui, Samburu, Marsabit and Busia, 56 health facilities were assessed using the
National HiNi Gap assessment tool. This tool is used to assess health facilities capacity to manage
acute malnutrition. Based on the total scores achieved during assessment 4 health facilities were found
to have limited capacity (0-25%), 28 health facilities with moderate capacity (26-50%); 23 health
facilities with good capacity (51-75%) and 1 health facilities excellent capacity (76-100%) to manage acute malnutrition. This is an achievement of 103.7% against the set annual target of 54 health facilities.
As part of the support towards improving vitamin A supplementation coverage, the program
participated in the Malezi Bora activities held in May 2016. The program supported Vitamin A
supplementation for a total of 57,638 children (Tharaka Nithi-6,110, Marsabit-8,747, Kitui-25,099,
Busia-9,826, and Samburu-7,856). An achievement of 87.8% against the FY16 set target of 72,387. It is expected that this target will be surpassed by the end of the FY16.
The program supported a one-day consultative meeting organized by Nutrition and Dietetics Unit and
Scaling up Nutrition (SUN) Academia and Research Network (ARN) for 42 participants drawn from
universities, research institutions and other stakeholders from the donor community. During the
meeting national nutrition research priorities were determined. The program is working towards determining key operational research priorities that can be supported by the program.
To strengthen the technical capacity of the USG funded programs to support quality implementation
of NACS approach beyond HIV services; horizontal scale up across service points, integration of
NACS within routine care and treatment, provide better commodity management and nutrition
reporting including routine mentorship and OJT activities at health facility and community level, the
program conducted a two-day NACS training for 29 Nutrition officers and monitoring and evaluation
officers from local Implementing Partners.
To support provision of commodity interventions to malnourished clients, 29,667 cartons of Fortified
Blended Flours were procured from Equatorial Nut Processors comprising of 17,800 cartons (60%)
of FBF for Adolescents and Adults; 8,900 cartons (30%) of FBF for Children less than 9 years and 2,967
cartons (10%) of FBF for Pregnant and post-partum mothers. The procured FBF quantities exceeded
quarterly procurement targets by 15.5% and can serve approximately 15,000 patients. During the same

USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
period 23,000 (77.5%) of FBF procured were distributed to 378 health facilities. During the same
period, the number of health facilities directly receiving FBF was increased from 350 to 378, an 8%
increase from previous quarter. The program supported a total of 857 health facilities with data
management and reporting representing an overall reporting rate of 85.7% of target facilities representing an increased facility reporting of 29.0% from the preceding quarter (857 vs 609).
Towards improving food and nutrition security, cooking demonstrations were conducted in the key
focus counties of Busia, Tharaka Nithi, Kitui, Samburu and Marsabit where a total of 404 community
members were provided with information on how to improve the quality of the food prepared and
learning how to modify food recipes to provide better nutrition value. Additionally, to improve
physical access and consumption of nutritious foods, two demonstration gardens were setup in
Mayenje and Burumba Primary ECDE centres in Mayenje and Burumba wards. The demonstration
gardens will be used to promote production and utilization of Vitamin A rich foods within the
community.
Towards improving resilience of vulnerable households and communities, the program in collaboration
with National Disaster Management Authority (NDMA) trained 61 NDMA Early Warning System Field
Monitors on correct screening of undernourished persons using MUAC within the communities. The
monitors will use the skills acquired to identify malnourished cases during their monthly assessments and refer them to health facilities for malnutrition management.
During the same period, a SMART survey was initiated in Samburu County. The population based
surveys are necessary for providing baseline data on the prevailing nutrition related indicators with a
view to setting targets. The overall objective is to determine the prevalence of malnutrition among the children aged 6- 59 months old and women of reproductive age of 15 to 49 years.
Towards achievement of the Monitoring and Evaluation Plans targets, the program is on track with
most of targets. During the quarter, the program completed assessment of 56 facilities within the focus
counties with capacity to manage acute malnutrition against an annual target of 54 heath facilities, an
achievement of 103.7%. To increase the number of people trained in child health and nutrition through
USG-supported programs, a total of 354 HCWs have been trained from the beginning of FY16, an
achievement of 164.7%. against the set target of 215.
To increase the number of children under five years reached by USG supported nutrition programs,
a total of 92,931 of under five children from the five focus counties, were reached,100.5% achievement
against the FY16 target of 92,484. A total of 63,557 of under five children have been provided with
Vitamin A supplementation through the programs, an achievement of 87.8% against the set target of
72,387.
By the end of FY16 Quarter 3, cumulatively 292,945 clients were nutritionally assessed using
anthropometric measurement, an achievement of 209% against the set target of 140,122 clients. During
the quarter, a total of 67,641 against a target of 62,285 clients were provided with Nutrition
Assessment, Counselling and Support. A total of 64,690 clinically malnourished PLHIV were provided
with therapeutic or supplementary food through the program, a 64.8% achievement against the set target of 99,885 for the FY16.
Although the program is on track, challenges in reaching children under five who are wasted and
children under five who are underweight still remains. The program is analyzing different sets of data
to understand whether the targets provided are reachable or not. Other indicators that are not on
track includes specifically process based targets that will take longer to achieve. These includes
creation of mechanisms to facilitate coordination, number of people trained/ Mentored, provided TA
at National Level and the number of tools/templates/models provided by target institutions in order to facilitate devolution at the local level as a result of USG assistance.
Challenges continue to be encountered in receiving commodity and service data from the facilities,
mainly attributed to staff turnover at facility level due and inadequate number of HCWs trained to
support nutrition. Due to intensive programming that is required in the key focus counties, the
program has also found the need to increase the number of staff in the key focus counties, specifically

USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
to include staff with knowledge of home economics to provide the necessary skills required in food and nutrition security.
During the subsequent quarter, the program will upscale NACS, IMAM, MYCN and agri-nutrition
sensitive training, complete the SMART surveys in the focus counties, expand use of EMR to improve facility reporting and conduct PROFILES for the nutrition in the country.

USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
I. BACKGROUND
The Kenya Nutrition and Health Program plus, a five-year program running from January 1, 2015 to
December 31, 2019 is a national program with county level mandates. The overall goal of the program
is to improve nutrition status of Kenyans. At the national level, the mandate of the program is to
increase access and demand for nutrition services and strengthen nutrition commodity management.
In addition to cascading these at county levels, the program works with Feed the Future partners in
the counties of Busia, Tharaka Nithi, Kitui, Samburu and Marsabit to improve food and nutrition
security. In the counties of Busia, Tharaka Nithi, Kitui and Samburu the program is implementing
Maternal Newborn and Child Health (MNCH) activities that aims at ending preventable child and
maternal deaths through ensuring a greater effect for women and children under two years with regards to nutrition.
The key results areas of the Nutrition and Health Program plus are improving access and demand for
quality nutrition interventions at community and facility levels, strengthening nutrition commodity
management and improving food and nutrition security. This report describes in detail the project’s
accomplishments, successes and challenges faced during the period of April 1 through June 30, 2016.
II. KEY ACHIEVEMENTS (QUALITATIVE IMPACT)
1. IMPROVED ACCESS AND DEMAND FOR QUALITY NUTRITION INTERVENTIONS AT COMMUNITY AND FACILITY LEVELS.
1.1. Strengthening Leadership, Advocacy and Policy Planning
During the quarter, the program developed a draft concept to conduct Kenya PROFILES on nutrition.
PROFILES uses models and country-specific data to project the economic and health consequences of
not adequately addressing a country’s nutrition problems, illustrating what the negative consequences
would be with no improvement and no change in nutrition problems over a defined time period. It
simultaneously estimates the benefits of improved nutrition over the same time period, including lives
improved and saved and economic productivity losses averted. Based on the projected consequences
and benefits, PROFILES results can be used to engage government and other high-level stakeholders
in a collaborative nutrition advocacy process to identify, prioritize, and advocate for evidence-based
actions to improve nutrition. The next steps include forming a core working group that oversees the
process and bringing together key stakeholders from multiple sectors, donors, and implementing
agencies to agree on a national approach for implementation of nutrition advocacy activities.
Towards strengthening leadership, the program is in discussions with the Busia County Government
to agree on a suitable candidate who can undertake Senior Management Course at The Kenya School
of Government, scheduled for August 2016 semester. When completed the cause will enable the
selected candidate to acquire competencies in strategic thinking and leadership that will impact the
county by improving her ability to provide informed insights and more effective analysis of key nutrition
issues in the county. Additionally, this will assist in retention of senior personnel who can fill in senior
positions that may arise such as CNC.
1.2. Improving Nutrition Service Delivery Management, Coordination and Implementation
During the quarter, a total of 56 HiNi target facilities were identified in Kitui, Samburu, Marsabit and
Busia. These facilities were identified through facility capacity assessment conducted in collaboration
with the County Health Management Teams (CHMT) using a standardised national HiNi Gap
assessment tool. This tool is used to assess health facilities capacity to manage acute malnutrition.
Facilities are ranked based on total scores achieved during assessment as either having limited capacity
(0 – 25%); moderate capacity (26 – 50%); good capacity (51 – 75%) and excellent capacity (76 – 100%).

USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
In Kitui, the 26 facilities assessed scored above 26% indicating they have good capacity to manage acute
malnutrition. However, one facility had limited capacity due to limited infrastructure. In Busia, of the
18 facilities assessed 15 health facilities were identified as having adequate capacity to manage acute
malnutrition. In Samburu county, of the 5 facilities assessed all scored above 50% indicating that they
have a satisfactory capacity to manage acute malnutrition. In Marsabit, all 7 facilities assessed attained
a score of above 50% indicating that they have adequate capacity to manage acute malnutrition. The
mains gaps identified in most of the facilities included lack of functional anthropometric equipment and
insufficient staff trained on IMAM. The results of this assessment will be disseminated at county level to assist each county in development of mitigation strategies to address the identified gaps.
Table 1: Distribution of Facilities with Capacity to Manage Acute Malnutrition
County No of facilities
assessed
Ranking of Facilities Based on Total Scores
Achieved
<25% 26-50% 51-75% >76%
Kitui 26 1 18 6 1
Samburu 5 0 0 5 0
Marsabit 7 0 1 6 0
Busia 18 3 9 6 0
Total 56 4 28 23 1
As part of program support to MOH in improving Vitamin A supplementation coverage, the program
participated in the Malezi Bora activities held in May 2016. The theme for this years’ Malezi Bora
celebrations was “Afya ya Jamii, Ustawi wa nchi”. Activities conducted in the five focus counties of Kitui,
Tharaka Nithi, Busia, Samburu and Marsabit included participation in the County Malezi Bora planning
meetings, joint support supervision during vitamin A supplementation activities and support for
administration of deworming medication at health facility. In Tharaka Nithi, the program supported
Vitamin A supplementation for 6,110 children under five years in 190 ECD centres located in the
Chuka Igambangombe sub-county. This represented a coverage of 96.4% of vitamin A supplementation
in the sub county. In Marsabit, Saku sub-county, a total of 8,747 children under five years were
provided with vitamin A supplementation, with 5,641 children aged 12-59 months being dewormed.
This represents 82.1% coverage of vitamin A supplementation (VAS) within the sub-county. As part of
the program’s strategy of targeting children aged 3-5 years in ECD centres in Sololo sub-county 40
ECD centres were identified with a catchment of 1,460 children. In subsequent quarters, Moyale and
Loyangalani sub-counties will be profiled. In Kitui, within the
sub-counties of Mwingi East, Mwingi central, Mwingi West,
and Kitui south, a total of 25,099 children under five years
received vitamin A supplementation and deworming
medication. In the sub-counties of Matayos and Teso North
in Busia County’s, 9,826 children under five years received
Vitamin A supplementation. In Samburu, 78 ECD centres in
Samburu central and Samburu East were supported where
a total of 7,856 children under five were provide with Vitamin A supplementation.
Table 2: Summary of Vitamin A Supplementation and Deworming in Focus Counties. County No. of Children
supplemented with
vitamin A
No. of
children
dewormed
No of ECD
covered
% Coverage based
population of children
under 5 yrs.*
Tharaka Nithi 6,110 - 190 32%
Marsabit 8,747 - - 103%
Kitui 25,099 25,099 642 42%
Busia 9,826 - 244 21%
Samburu 7,856 - 78 35%
Total 57,638 * Coverage is based on population of children under five years in the respective sub-counties where Malezi bora activities were conducted

USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
1.3. Improved Nutrition Related Behaviour
During the quarter, the program supported pre-testing of the MIYCN counselling card in Tharaka
Nithi county. The objective of the pretesting was to determine viability of the messages in catalyzing
appropriate behavior change. Key informant interviews (KII) and focus group discussions (FGD) were
conducted to collate required feedback, targeting audiences within urban and rural settings. These
target audiences included Health Care Workers, Mentor Mothers and Community Leaders (Local
Administration and Religious Leaders). Health Workers, Mothers, Community Health Volunteers
(CHVs), Youth Leaders, Fathers, Mother-to-Mother Support Group (MtMSG) and Grandmothers
participated in the FGDs during the pretesting. In addition, nine (9) FGDs with community groups of
ten (10) participants each were also conducted. Also, four (4) individual interviews targeting health
workers and community leaders were conducted. Preliminary recommendations to improvement of
the counselling card include the need for a counselling card with only illustrations and key messages for health care workers and community health volunteers.
During the quarter, the program conducted four (4) CMEs in the four (4) high volume health facilities
in Tharaka Nithi. The CMEs were attended by 89 health workers and provided an opportunity to brief
the HCWs on expectations for successful implementation of the Malezi Bora activities, addressed
reporting gaps for growth monitoring services, Vitamin A supplementation, Zinc, Deworming and the
entire Malezi Bora interventions; provided updates to HCWs on the integrated package of preventive
services for improving child health, survival, and maternal health; increased the utilization and improved
capacity for delivery of the 13 HiNi interventions based health and nutrition services for children,
expectant women, lactating mothers and women of reproductive age in Kenya and aided achievement of a complete implementation of breastfeeding policy in maternity facilities.
Towards increasing uptake of key nutrition behaviors, the program leveraged on campaigns held during
the Malezi Bora events to provide key messages regarding breastfeeding practices and complimentary
feeding practices. In Tharaka Nithi 1,154 people were reached with the key messages on
complimentary feeding. In Busia, Teso North and Matayos sub counties, 155 people were reached
with messages on appropriate complementary feeding and handwashing during critical times including
timely introduction of complementary foods, frequency, amount of feeds and consistency based on
age, use of variety of nutrient-rich foods, responsive feeding method and hygienic food preparation
were discussed. Messages for handwashing with soap during critical times, use of toilets and point of
use water treatment were also provided. In Samburu, similar messages were provided to 22 women
from Nyuat self-help group, Lkurotto village in Samburu central as well as 168 mothers in Kitui and 29 Women of reproductive age in Marsabit county.
Similarly, during the Malezi Bora activities held in May 2016 the program printed 1,000 Malezi Bora
Posters of Vitamin A (500 posters) and Good Nutrition (500 posters). The posters were in English
and Swahili versions and were distributed in the focus counties of Tharaka Nithi, Marsabit, Kitui, Busia and Samburu.
1.4. Increasing Opportunities for Learning and Sharing of Best Practices in
Nutrition
Towards supporting the government to determine national nutrition research priorities, the program
supported a one-day consultative meeting organized by Nutrition and Dietetics Unit and Scaling up
Nutrition (SUN) Academia and Research Network (ARN). The meeting was attended by 42
participants representing Tegemeo Institute, University of Nairobi, Egerton University, Kenyatta
University, Jomo Kenyatta University, KEMRI, Maseno University and Moi University; NDU, NASCOP,
MOALF-Home Economic Department, Ministry of Devolution and Planning-Planning unit, USAID
Kenya and UNICEF. During the consultative meeting key research areas were identified, scope of
research defined, as well as identification of analysis and synthesis required to support nutrition based
research. The program will continue to support the process of identifying key operational research
priorities areas for eventual implementation support by the program.

USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
1.5. Increased knowledge and skills for health care workers
To ensure high quality of delivery and management of nutrition program activities, the program
conducted a two-day NACS training for 29 Nutrition officers and monitoring and evaluation officers
from Implementing Partners(IP). The participants were drawn from MCSP (2), APHIAplus Imarisha (3),
APHIAplus Kamili (3), CHS (2), AMPATHplus (2), APHIAplus Nuru ya Bonde (3), APHIAplus Western
(3), Department of Defense (3), APHIAplus Jijini (3), Lea Toto COGRI (3), EGPAF (2) and DHMH (1).
The purpose of the NACS training was to strengthen the technical capacity of the USG funded
programs to support quality implementation of NACS approach beyond HIV services; scale up
horizontal integration of NACS within health facilities, provide better commodity management and
nutrition reporting including routine mentorship and OJT activities at health facility and community
level.
During the quarter, as a follow up of the HiNi gap assessment activities, a five-day training on Integrated
Management of Acute Malnutrition (IMAM) was conducted in Busia County. The IMAM key areas of
training included in-patient management and outpatient management of severe and moderate acute
malnutrition. A total of 34 participants attended the training comprising of 3 sub county nutrition
officers, 7 Facility Nutritionists, 13 nurses, 5 clinical officers, 2 AMPATHplus Nutrition officers, and 4
APHIAplus Western Nutrition staff. 28 health care workers were drawn from 18 health facilities in Busia. The goal of this training is to improve health facilities capacity to manage acute malnutrition.
2. STRENGTHENED NUTRITION COMMODITY MANAGEMENT
The main objective of this intermediate result area is to improve the impact of all interventions by
ensuring efficiency in nutrition commodity procurement, management and distribution including ensuring high quality and safety of nutrition commodities procured.
2.1. Improving Production, Supply and Distribution of Nutrition Commodities
During the reporting period, approval to contract Equatorial Nut Processors for procurement of
Fortified Blended Flours (FBF) and Insta Products (EPZ) Ltd for procurement of RUTF, was provided
by USAID Contracting Officer for the period beginning from April, 2016 to December 31, 2017. The
approval allows for procurement of 205,550 cartons of FBF with a value of US$ 5,998,557.42 that can
cover approximately 157,587 patients. This will contribute to a more efficient and effective supply
chain where nutrition commodities are expected to be readily available with minimal delays in production and/or distribution to the health facilities.
During the quarter, 29,667 cartons of Fortified Blended Flours were procured from Equatorial Nut
Processors comprising of 17,800 cartons (60%) of FBF for Adolescents and Adults; 8,900 cartons (30%)
of FBF for Children less than 9 years and 2,967 cartons (10%) of FBF for Pregnant and post-partum
mothers. The procured FBF quantities exceeded quarterly procurement targets by 15.5% and can
serve approximately 15,000 patients.
Due to delay in DA1 Form approvals, RUTF procurement and delivery has been affected from
September, 2015. The program is working closely with the Insta Products (EPZ) Ltd to ensure that RUTF is procured and distributed during the coming quarter.
During the reporting period, 23,000 (77.5%) of FBF procured was distributed to 378 health facilities.
During the month of April, no distribution of commodities was conducted due to buffer stock provided
to the health facilities during the previous quarter. During the same period the number of health
facilities directly receiving FBF was increased from 350 to 378, an 8% increase from previous quarter.
Through the continued NACS trainings and collaboration with county governments and other Implementing Partners, it is envisaged that this number will rise significantly in the coming quarter.

USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
Table 3: Summary of Procured and Distributed Nutrition Commodities FBF
Type
Jul-Sep 2015 Oct-Dec 2015 Jan-Mar 2016 Apr-Jun 2016
Procured Distributed Procured Distributed Procured Distributed Procured Distributed
FBF
Adults 17,667 14,610 21,200 18,268 18,578 19,392 17,800 13,872
FBF
Children 8,833 6,822 10,600 8,398 7,067 10,858 8,900 6,955
FBF
Mothers 2,944 2,045 3,533 3,596 4,022 12,007 2,967 2,177
TOTAL
(FBF) 29,444 23,477 35,000 30,261 29,667 42,257 29,667 23,004
RUTF 0 0 8,178 2,044 0 0
During the May 2016, Malezi Bora activities, the program provide support to Nutrition and Dietetics
Unit (NDU) in distribution of Vitamin A Supplements. 6,205 tins of 200,000IU and 5,445 tins of 100,000IU of Vitami A were distributed to 21 counties for use during the Malezi Bora campaigns
Towards improving reporting rates, site visits were conducted in Busia and Nairobi Counties. Five (5)
health facilities were visited namely Angurai Health Centre, Busia CRH, Kocholya SCH, Moding H/C.
Busia County, being a focus county for the program, was of particular interest as commodity supply
had not yet been decentralized. Facilities visited were previously supported by AMPATH and had
requisite capacity to receive, store and dispense commodities. As a result of the site visits, a follow up
refresher training is planned during the forthcoming quarters to strengthen commodity management
and reporting. In addition, coverage within the county will be increased to support reducing
malnutrition in the county.
During the quarter, the program supported a total of 857 health facilities with data management and
reporting representing an overall reporting rate of 85.7% (857/1000) of target facilities. Overall, there
was increased facility reporting rate of 29.0% from the preceding quarter (857 vs 609). 383 of these
facilities have been designated as commodity delivery points. To ensure improved facility reporting
rates in subsequent quarters, the program will continue to engage with CNCs, facility nutrition contact
persons and local APHIA+ partners to support joint CME/OJT, supervision sessions as well as sharing
of monitoring data reports. The program also plans to transition 17 additional high volume facilities
into EMR facilities. The program will also seek to promote previously designated “satellite sites” to delivery points to ensure wider reach in provision of NACS.
In addition to the site visits, reports received from Tharaka Nithi indicated that the quality of the
packaging material (cartons) had improved such that the corrugated boxes could be stacked up to 6 boxes high.
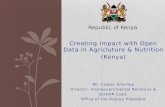
To mitigate against the reported stock out MOH 733B (Facility Summary for Nutrition Services) and
MOH 734B (Facility Consumption Data Report and Request for Nutrition Commodities), printing of
Jan-Mar 2015 Apr-Jun 2015 Jul-Sep 2015 Oct-Dec 2015 Jan-Mar 2016 Apr-Jun 2016
Procured - 16,869 29,444 35,000 29,667 29,667
Distributed - 15,357 23,477 30,261 42,257 23,004
-
16,869
29,444
35,000
29,667 29,667
- 5,000
10,000 15,000 20,000 25,000 30,000 35,000 40,000 45,000
NO
. O
F C
AR
TO
NS
QUARTER PERIOD
VOLUME OF FBF PROCURED AND DISTRIBUTED

USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
additional data collection tools has been initiated. Distribution of MOH 733B is planned to completed in FY16 Quarter 4.
During the reporting period, personnel from the program continued to actively participate during the
NASCOP Monthly Commodity Security Steering Committee meetings. The focus within the quarter
was on strengthening Logistics Management Information Systems (LMIS) where NASCOP undertook
trainings in various counties on forecasting and quantification of commodities including nutrition
commodities mainly targeting the County Health Management Teams. Additionally, the program
continues to provide monthly consumption summaries to NASCOP to inform development of the two pager report.
During the quarter, the program continued to provide support on commodity and service data
reporting to approximately 857 health facilities in 43 Counties during implementation of Nutrition
Assessment, Counselling and Support (NACS)/FBP mainly within the CCC and MCH clinics.
Specifically, the program supported commodity and service data reporting from facility to National
(DHIS) levels through support for data management, provision of reporting tools and support
supervision/OJT activities.
2.2. Improving Quality and Safety of Food Commodities and Agricultural Products
Towards improving quality and safety of nutrition commodities, the program conducted a Supplier
Quality Audits (SQA) in Equatorial Nut Processors and Soy Afric Ltd. Due to ongoing maintenance
works and equipment installations, Insta Products (EPZ) Ltd did not participate during the biannual
SQA activity. Insta Products (EPZ) Ltd will be included in the next cycle of Suppler Quality Audits
programed for December 2016. The main objective of the Supplier Quality Audit is to monitor
progress made on implementation plans that the food processors had provided during December 2015
SQA. In addition, ISO 22000 and ISO 22002-2009 attainment status was checked. The 3 companies
were expected to have attained the ISO 22000 Food Safety certification before audit period. The
assessment criteria changed slightly from a hybrid of requirements in the previous audit to a pure ISO
22000:2005 and 22002-1:2008 during the current assessment.
ENP scored an overall average of 85.3%, a minimal improvement from the previous score of 84.9%.
The notable improvements especially by observation were in cleaning and sanitation in the factory and
staff facilities, as well as premises repairs and maintenance. The previous audit identified corrective
actions on documentation as a non-conformance. The documentation was either missing or actions
were not clear in various areas. Little or nothing has been done to improve on documentation. However, overall there were no major non-conformances found during the SQA.
Soy Afric Ltd scored an average of 38.8%, a minimal improvement from previous score of 32.4%.
Despite the Soy Afric Lt having a good facility, the client lacks historical evidence to demonstrate due
diligence as observed in production of their food products. The client has also attempted to document
food safety system, but there seems to be lack of internal capacity to complete documentation of food
safety system. The Supplier Quality Audit report will be disseminated to the respective processors in the coming quarter.
2.3. Strengthening Sustainability and Innovation in Nutrition Commodity Development and Management
Working closely with Equatorial Nut Processors, a concept paper has been prepared for development
of alternative FBF for management of moderate malnutrition. The concept paper provides a clear
description of the proposed products to be developed including a summary of what is already known
about the current products available for management of moderate malnutrition, a description of how
ENP will develop the proposed products including formulation of premixes in line with WHO/CODEX
recommendation for new micronutrient formulation for specialized FBF products, the data that will
be gathered or used; how the subcontractor will analyze the data; and how the data and analytic method will be used to develop the new product.

USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
During the quarter, Equatorial Nut Processors was able to procure 111,420 Kg of Soya Beans from
Busia County, with a value of US$ 62,950. Soya beans is a key raw materials used in FBF production.
The program is working closely with Equatorial Nut Processors to link more farmers in the key focus
counties of Busia, Kitui, Tharaka Nithi, Marsabit and Samburu with the FBF processors to develop
sustainable markets for Maize, Soya Beans and Sorghum. Additionally, for traceability of agricultural
raw materials used in FBF processing, Equatorial Nut Processors have vetted 4 local suppliers of maize
and soya beans who have consistently met the minimum requirements. This is an important aspect of ensuring quality FBF procured through the program.
3. IMPROVED FOOD AND NUTRITION SECURITY
The main objective of this intermediate area is to break the cycle of malnutrition through providing
food and nutrition security to ensure prevention of recurrent malnutrition. Through targeted
interventions and smart integrations and linkages with other partners the programs enable individuals
and groups vulnerable to undernutrition to improve their overall food and nutrition security. Towards
improving food and nutrition security and in reducing stunting the program conducted several activities
that included promotion of dietary diversity practices especially focusing on food production through
improving physical access and consumption using appropriate food preparation techniques. Population
based surveys were also conducted to provide baseline data on the prevailing nutrition related
indicators. Linkages with various stakeholders were established to provide synergies and leverage on existing opportunities for bridging agri-nutrition gaps for increased nutrition outcomes.
3.1. Increasing Market Access and Consumption of Diverse and Quality Foods
To promote dietary diversity practices, cooking demonstrations were conducted in the key focus
counties. In Samburu county the program conducted cooking demonstration using sorghum and
pumpkin as key ingredients and source of vitamin A. The cooking demonstrations targeted 22 women
from Lkurotto Village, Nyuan Self Help Group who were shown how to prepare pilau, mandazi and
chapatis using sorghum and pumpkin. Sorghum is one
of the cereal in the market and also supplied through
GFD (General food distribution) but has a poor
utilization due to community’s lack of knowledge on its
utilization and the perception that sorghum is food for
the poor. Pumpkin leaves and fruits are good source of
vitamin A and can be prepared either as vegetables or
snacks. The group was also provided with key messages
on hand washing during food preparation to prevent common food contamination.
In Busia County three cooking demonstration were conducted within the communities living in Teso
North and Matayos sub-counties. The cooking demonstrations and nutrition education sessions were
used to address the energy, protein and micronutrient gaps that breastfeeding alone is not able to
meet after the 6 months. These included use of fats, peanut paste and sugar
in preparation of cereals and staples such as to improve energy and protein
density including taste, foods of animal origin, milk, vegetables and fruits to
meet protein, Iron, Calcium and Vitamin A requirements. 155 people were
reached during the cooking demonstrations, 120 people coming from Kolait
and Katotoi community groups in Teso North Sub-County and 35 people
from Burumba community group in Matayos Sub-County. The group was
provided with key information on breastfeeding and complimentary feeding
timing and age appropriate amount of feeds required, food consistency e.g. thin porridge and inappropriate feeding method e.g. forceful feeding.
In Tharaka-Nithi county, cooking demonstrations were conducted during
the Malezi Bora week targeting 30 mothers from Kibugua Mother-to-Mother support group. The
mothers were trained on preparing baby porridge made from Millet & Sorghum flour enriched with
cooking oil and sugar to make it energy dense and preparation of complementary food of mashed

USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
bananas, potatoes, cow peas, pumpkin leaves and carrots. The gaps addressed being cooking
demonstrations included importance of timely introduction of appropriate complementary feeding,
safe preparation of foods, correct recipe and consistency of baby’s porridge.
In Kitui County, cooking demonstrations were conducted in 4 sub-counties of Kitui South, Mwingi
North, Mwingi west and Mwingi Central during the Malezi Bora week. The
cooking demonstrations focused on promotion of utilization of Sorghum
and cowpeas. Sorghum and cowpeas are common food grown in the
region but less consumed at the household level. The two crops do very
well in this semi-arid region and their nutritive value is high. The two crops
are good sources of iron, and more so the cowpeas leaves. Most of the
people consider the two as cash crops. The recipes used during the
cooking demonstrations were cereal porridge (sorghum & millet) and
mashed pumpkin, potatoes, bananas & cowpeas with cowpeas, spinach and
pumpkin leaves. The recipes are important in mitigating Vitamin A
deficiency and Anemia among women of reproductive age. During the
sessions 168 pregnant and lactating mother with children of up to 2 years
of age, who were trained on preparation of complementary feeds using
locally available nutritious foods and appropriate hygiene practices during
food preparation.
In Marsabit county one participatory cooking demonstration was conducted targeting 29 mother to
mother support group members during Malezi Bora week. The overall objective of the demonstration
was to impart practical know how on the best practices to prepare locally existing food hence
developing caregivers’ skills and confidence to prepare nutritionally sound meals. Sorghum was used
as the recipe of choice. Sorghum grows very well in Marsabit and drought tolerance, but has very
utilization mainly attributed to lack of adequate knowledge on its nutrient content as well as lack of
Knowledge on how to prepare sorghum appropriately. It is one of the cereal introduced in the region
by USAID due to its potential role in enhancing food security.
Towards improving physical access and consumption of nutritious foods, demonstrations gardens were
established in Busia. In Busia County, Matayos Sub-County two demonstration gardens were setup in
Mayenje and Burumba Primary school ECDE centres. The demonstration gardens were established
to promote production and utilization of Vitamin A rich foods (green leafy vegetables, carrots, orange
fleshed sweet potato, fruits tree (mangos, and custard apple). The 4K club members from the primary
school section participated in all the activities from land preparation, planting and management of the
gardens. The goal was for the 4K club members to learn how to grow the target nutrient dense foods and their importance. In Burumba 45 pupils participated during demonstration garden preparation.
In Tharaka Nithi County, Kibugua Mother-to-Mother Support Women group has been identified. The
Kibugua Mother-to-Mother Support group has been allocated a demonstration garden within Kibugua
Health Centre but garden has not been in use. The program intends to prepare this group’s
demonstration garden as a model garden where other groups can visit and learn from. The Women
group enthusiasm and organizational capacity will be utilised as a model group where other women
groups from the County and Sub-County will visit and learn from. Towards strengthening Kibugua
Mother-to-Mother Support Women demonstration garden a site assessment was conducted. The
assessment determined the type and number of seedlings required, tools and equipment needed to
establish the demonstration garden. When established the garden will produce a significant quantity
of food to eat and sell and act as a demonstration garden and agricultural trainings garden for other
groups within the community. Additionally, Kibugua mother-to-mother support women group and
their individual households group profiling was conducted. The group has the capacity to engage in
several activities that includes production and utilization through dietary diversification and increased
production technologies for food, nutrition security and resilience building.

USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
3.2. Increasing Resilience of Vulnerable Households and Communities
Towards improving resilience of vulnerable households and communities, the program in collaboration
with National Disaster Management Authority (NDMA) trained 61 NDMA Early Warning System Field
Monitors on correct screening of undernourished persons using MUAC within the communities.
Those trained included 15 NDMA staff from Samburu, 22 from Marsabit and 24 from Kitui county.
The monitors will use the skills acquired to identify malnourished cases during their monthly
assessments and refer them to facilities for medication. Those found vulnerable will be referral to
safety net programs and livelihood activities within community structures. The vulnerable households
will also be linked to community livelihood programs that will help them avoid relapse. Already in
Samburu NDMA Field Monitors have identified 2 children with MUAC of less than 12cm from Arsim
location within community during their monthly routine assessments. These have been referred to
Arsim dispensary for nutrition support. Additionally, 114 vulnerable clients have been identified from
Busia (71), Kitui (4), Marsabit (2), Samburu (30) and Tharaka Nithi (7) health facilities that requires
linkages to safety net programs and livelihood activities within the communities.
In Marsabit County, a mapping exercise for the existing social safety net programs was conducted. The
social safety net programs identified includes Hunger safety net plan, disabled cash transfers, orphans and vulnerable children and older persons.
During the quarter, a SMART survey was initiated in Samburu County. The population based surveys
are necessary for providing baseline data on the prevailing nutrition related indicators with a view to
setting targets. The overall objective was to determine the prevalence of malnutrition among the
children aged 6-59 months old and women of reproductive age of 15 to 49 years. The specific
objectives were to determine the prevalence of acute malnutrition among children aged 6-59 months;
estimate prevalence of maternal malnutrition using MUAC, determine the immunization coverage for
measles, Oral Polio Vaccines (OPV 1 and 3), and vitamin A supplementation in children aged 6-59
months; determine de-worming coverage for children aged 12 to 59 months; estimate the use of zinc
in diarrheal treatment in children; determine the prevalence of common illnesses; determine Iron folic
acid supplementation rates among PW and to collect information on possible underlying causes of
malnutrition such as household food security, water, sanitation, and hygiene practices. The target
population were household with children 6-59 months and pregnant and lactating women. When
completed the SMART survey will provide critical information that will guide reduction of stunting in Samburu County.

USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
III. ACTIVITY PROGRESS (QUANTITATIVE IMPACT)
Nutrition and Health Program plus MEP has provided for the following indicators and their target.
Below is a summary of each indicators progress by the end of FY16 Quarter 3.
Number of health facilities with established capacity to manage acute under nutrition:
The FY16 target for this indicator was set at 54 health facilities. By the end of the FY16 quarter 3, the
program has identified 56 facilities within the focus counties with capacity to manage acute malnutrition
against an annual target of 54 heath facilities. This is an achievement of 103.7% against the set annual
target. These facilities were identified through assessment of health facilities within the county’s using
the HINI gap assessment tool. Additional facilities from Marsabit are in the process of being identified.
Number of people trained in child health and nutrition through USG-supported
programs: A total of 354 HCWs have been trained from the beginning of FY16. This is an
achievement of 164.7%. against the set target of 215. Of those trained 183, have been trained in child
health and nutrition from Busia and Tharaka Nithi county. Once target facilities for management of
malnutrition have been fully identified, additional MIYCN training will be conducted during FY16
Quarter 4 for the remaining focus counties.
Number of children under five years reached by USG supported nutrition programs: The
program has successfully reached a total of 92,931 out of a target of 92,484 of under five children from
the five focus counties,100.5% achievement against the FY16 set target. Those reached includes clients
provided with Vitamin A supplement provide through the ECD centers during the Malezi Bora week.
Number of children under 5 who received Vitamin A from USG supported programs:
Through provision of TA (support for CMEs and OJT) during Malezi Bora, distribution of Vitamin A
from NDU and KEPHI the program has supported Vitamin A supplementation for a total of 63,557 of
under five children out of a target of 72,387, an achievement of 87.8% against the set target. The
program will continue to provide capacity building and reporting tools to ECD centers and health
facilities in support of Vitamin A supplementation for the under-fives. It is expected that by the end
of FY16 the program will exceed the annual target.
Number of children under five who are wasted: Number of under-five wasted children from
the five focus counties was reported to be 12,356 out of an overall target of 3,747 for the financial year.
Number of children under five who are underweight: Underweight children under five were
reported to be 184 against an expected target of 8,033 for the financial year. Additional training and
mentorship for client assessment will be conducted within the focus counties to ensure competence
in case identification. In addition, the program will provide anthropometric equipment, reporting tools
and EMR systems at CCC and MNCH service points to strengthen data quality.
Percentage of PLHIV who are nutritionally assessed via anthropometric measurement:
During FY16, 140,122 clients were to be provided with the nutrition assessment using anthropometric
measurement. By the end of FY16 Quarter 3, cumulatively 292,945 clients had undergone nutritional
assessment using anthropometric measurement, an achievement of 209%.
During the quarter, a total of 67,641 against a target of 62,285 clients were provided with Nutrition
Assessment, Counselling and Supports. Of those provided with NACS, approximately 48.9% were
newly enrolled clients. CCC service points recorded the largest of patients seeking nutrition services,
followed by MCH and Inpatient/Other clinics at 67.0%, 4.0% and <2% respectively. Of the total clients
provided with NACS, 74.6% and 25.4% were children and adult clients respectively. Table below shows
the distribution of clients provided with Nutrition Assessment, Counselling and Supports. 13,832 adult
and 2,767 child clients from EDARP have not been included for luck of client-identification information in their records.

USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
Table 4: Distribution of assessed clients
Client category Number* of clients (%)
Adult PLHIV 34,885 (68.3%)
OVC 6-59 months 9,472 (18.6%)
Pregnant 1,774 (3.5%)
5-17 years 4,911 (9.6%)
Total *51,042 (100.0%)
*13,832 adult and 2,767 child clients from EDARP missing client-identification information
Proportionately, 7.6% (n=22,797) of the assessed adult clients were reported to be severely
malnourished with BMI of <16. Clients with BMI>18.5 seeking nutrition services during the visit 1 was
69.5% of non-PPP clients (n=22,797). Overall BMI reporting Rae for adult clients was reported at
93.3% (n=34,885). Of the 1,774 PPP clients supported during the reporting period, 54.3% were newly enrolled clients. Overall MUAC reporting rate for PPP clients was recorded at 44.4%
Table 5: Nutrition Status of adult Clients
BMI Category Visit Type Total
New Revisit
<16 1,730 (7.6%) 831 (8.2%) 2,561 (7.8%)
16-17 1,554 (6.8%) 915 (9.1%) 2,469 (7.5%)
17-18.5 3,660 (16.1%) 2,132 (21.1%) 5,792 (17.6%)
>18.5 15,853 (69.5%) 6,220 (61.6%) 22,073 (67.1%)
Total 22,797 (100.0%) 10,098 (100.0%) 32,895 (100.0%)
Table 6 below shows the weight-for-height status for the 9,472 under five children who were
provided with Nutrition Assessment, Counselling and Supports during the FY16 Quarter 3. 200 children have not been included due to missing anthropometric data in the records.
Table 6: Nutrition Status of Newly Enrolled Under 5-Year-Old Clients
WHZ 6-24 months 24-59 months Total
< -3 1,084 (14.7%) 202 (10.8%) 1,286 (13.9%)
-3 to -2 1,292 (17.5%) 251 (13.4%) 1,543 (16.6%)
-2 to -1 1,803 (24.4%) 395 (21.1%) 2,198 (23.7%)
> -1 3,217 (43.5%) 1,028 (54.8%) 4,245 (45.8%)
Total 7,396 1,876 **9,272
**200 children missing anthropometric data
Proportion of clinically undernourished PLHIV who received therapeutic or
supplementary food: By the end FY16 Quarter 3, cumulatively, a total of 64,690 clinically
malnourished clients were provided with therapeutic or supplementary food through the program.
The FY16 program target is to provide 99,885 clinically undernourished PLHIV with therapeutic or
supplementary food. By the end FY16 Quarter, using the data already received 64.8% of the target had
been achieved. Data for the month of June has not yet been received for entry in the data base. When
received, the number of clinically malnourished clients provided with therapeutic or supplementary
food through the program will be higher. The program will continue to engage implementing partners,
community groups, field extension workers, and in building capacity for HCWs, CHVs and facilities
through provision of job aids, tools and electronic support to support identification for the PLHIV
requiring therapeutic or supplementary food. It is envisaged that this will stimulate improved case
finding and improved case detection of clients in need of intervention.
During FY 16 Quarter 3, a total of 14,490 clients were provided prescriptions for therapeutic or
supplementary food through supported facilities, representing a 26.2% (14,490 vs 18,285) reduction
from the previous quarter. An additional 15,638 client records provided with nutrition assessments
have been received during the writing of the report. Digitization of these reports will be completed
early August, 2016, with subsequent feedback reports to respective CNCs and the NDU/NASCOP

USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
commodity security committee prepared and shared. A profile of clients receiving therapeutic or supplementary food during FY 16 Quarter 3 is shown in Table 6.
Table 7: Number of clients receiving commodities by “client category”
Client category Number* of clients (%)
Adult PLHIV 8,190 (58.6%)
OVC 6-59 months 4,180 (29.9%)
Pregnant 529 (3.8%)
5-17 years 1,077 (7.7%)
Total 13,976 (100.0%)
514 cases are not included due to missing data for categorization comprising of 112 and 402 Adult and
Child clients respectively. Figure 1 below provides the trend in commodity dispensing (prescriptions)
between July 2015 and June 2016.
Figure 1: Trend in Commodity Prescriptions Between July 2015 And June 2016
Number of mechanisms created to facilitate coordination on an ongoing basis as a result
of USG Assistance at national level: The program supported 10 MOH led county multidisciplinary
coordination meetings during this financial year as per required target.
Number of people trained. Mentored, provided TA at National Level: The program is in the
final phases of actualizing the first program supported intake of county nutrition coordinators from the focus counties into the management program at Kenya School of Government.
% of county officials trained who demonstrate increased knowledge in training as result
of USG support: The program has recently supported constitution of Ministry of Health Operational
Research TWG to consultatively determine the country’s nutrition research priorities. The first
consultative meeting with interested partners research and academia was conducted and supported
by NHPplus during the third quarter. Arising from these, the program will support TWG secretariat
operations and additionally support dissemination forums during FY16 Quarter 4 and subsequent
financial years. These forums will not only support dissemination to research and academia peers but
also to county and national HCWs and implementers. Capacity building for focus county health executives in Samburu to develop and implement SMART surveys has also been completed.
Number of people trained: During the financial year, the program has supported SCALE ToT
training for 31 out of an expected target of 125 comprising of MOH and USG Implementing Partner ToTs from designated focus counties.
-
2,000
4,000
6,000
8,000
10,000
12,000
June July August September October November December January February
Y6-Q2 Y6-Q3 Y6-Q4
2014
Met
ric
To
ns
(FB
F)
FBFNew FBFRevisits FBF Total

USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
Number of mechanisms created to facilitate coordination on an ongoing basis as a result
of USG Assistance at county level: The program supported drafting and adoption of terms of
reference for establishment or re-activation of county nutrition technical forums in Busia, and Kitui:
The program will utilize additional expert TA during the fourth quarter to cascade SCALE methodology to the focus counties.
Number of people trained. Mentored, provided TA at County Level: (people/TOTs trained
in SBC strategies, dietary diversification and financial inclusion, L/FFS, Food nutrition resilience, Income
generating value chains targeting women): The programs in the process of identifying community
groups within the counties Parallel to this, the program is in contact with USG Implementing Partners and MOALF to develop and implement a suitable training curriculum on dietary diversification.
Number of tools/templates/models provided by target institutions in order to facilitate
devolution at the local level as a result of USG assistance: During the quarter, the program
sought to identify community settings as potential channels for targeted messages and associated
information gaps specific to each county. Based on this, the program is finalizing acquisition of GOK
approved material for subsequent contextualization of nutrition and agri-nutrition job aids and tools
to assist CHVs in targeting and identification of vulnerable groups. Nutrition specific job aids targeting
ECD centers and MNCH service points will be distributed in FY16 Quarter 4. During the FY16
Quarter 4, 1,000 Malezi Bora Posters of Vitamin A (500 posters) and Good Nutrition (500 posters)
were printed and distributed to key focus counties.

14
USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
Table 8: Performance data table: Commodities Distributed in MT INDICATOR TITLE: Number of MT of Commodities Distributed
INDICATOR NUMBER: SC_STOCK
UNIT: DISAGGREGATE BY: COUNTY
Geographic Location Activity Title Date: M
All counties except Mandera Reporting
Results:
Additional Criteria Baseline (January
2015)
Results Achieved
Prior Periods
Reporting Period 31/Dec/15
Reporting Period 31/Mar/16
Reporting Period 30/Jun/16
FY 2016 Target % Achievement If other criteria are
important, add lines for setting targets and tracking
County % December
2015
Target Achieved Target Achieved Target Achieved Target Achieved
N N N N N N N N N N
Baringo 1.7% 27 36.15 10.36 26.19 10.36 4.55 10.36 4.09 31 35 >100%
Bomet 0.9% 14 29.64 5.29 17.91 5.29 4.16 5.29 3.28 16 25 >100%
Bungoma 0.9% 15 60.56 5.65 19.87 5.65 31.24 5.65 10.04 17 61 >100%
Busia 0.3% 5 84.95 1.72 20.76 1.72 53.67 1.72 18.32 5 93 >100%
Elgeyo
Marakwet
0.4% 6 22.39 2.21 13.77 2.21 3.11 2.21 1.46 7 18 257%
Embu 4.6% 72 40.83 27.49 14.94 27.49 11.76 27.49 - 82 27 33%
Garissa 0.8% 12 2.57 4.75 0.54 4.75 1.53 4.75 - 14 2 14%
Homa Bay 4.9% 77 128.51 29.41 30.68 29.41 63.25 29.41 35.83 88 130 >100%
Isiolo 0.6% 9 18.59 3.33 - 3.33 9.31 3.33 2.47 10 12 >100%
Kajiado 1.2% 19 29.60 7.25 3.35 7.25 20.63 7.25 0.86 22 25 >100%
Kakamega 1.9% 30 51.49 11.44 22.05 11.44 12.07 11.44 12.80 34 47 >100%
Kericho 2.4% 38 9.48 14.32 4.05 14.32 1.12 14.32 - 43 5 12%
Kiambu 2.2% 34 76.58 13.15 15.92 13.15 40.66 13.15 10.06 39 67 >100%
Kilifi 1.2% 18 21.31 6.95 - 6.95 6.60 6.95 9.63 21 16 76%
Kirinyaga 1.7% 27 42.68 10.31 19.28 10.31 16.04 10.31 26.86 31 62 >100%
Kisii 0.9% 15 22.46 5.63 6.43 5.63 1.80 5.63 4.59 17 13 76%
Kisumu 4.2% 65 156.66 24.95 58.73 24.95 28.39 24.95 18.43 75 106 >100%
Kitui 1.0% 16 45.90 6.17 6.75 6.17 15.28 6.17 6.52 18 29 >100%
Kwale 0.5% 8 20.09 2.94 4.23 2.94 7.11 2.94 2.02 9 13 >100%
Laikipia 0.2% 4 12.26 1.39 - 1.39 7.52 1.39 7.74 4 15 >100%
Lamu 0.9% 14 6.86 5.49 - 5.49 3.73 5.49 2.61 16 6 38%
Machakos 2.8% 43 48.42 16.61 29.84 16.61 5.18 16.61 7.34 50 42 84%
Makueni 0.7% 11 30.24 4.36 10.84 4.36 11.97 4.36 11.43 13 34 >100%
Mandera 0.0% - - - - - - - - - -
Marsabit 0.6% 8 6.49 3.18 1.98 3.18 1.98 3.18 8.03 10 12 >100%
Meru 1.6% 24 40.28 9.19 9.00 9.19 8.37 9.19 8.86 28 26 93%
Migori 2.9% 45 99.01 17.19 29.93 17.19 25.33 17.19 9.61 52 65 >100%
Mombasa 5.4% 86 52.09 32.80 3.60 32.80 12.37 32.80 11.70 98 28 29%
Murang'a 2.2% 34 29.50 12.91 - 12.91 7.81 12.91 12.19 39 20 51%
Nairobi 6.4% 100 194.42 38.19 55.56 38.19 54.58 38.19 23.60 115 134 >100%
Nakuru 1.8% 29 49.01 10.95 11.63 10.95 15.13 10.95 17.08 33 44 >100%
Nandi 1.8% 29 27.40 10.96 4.70 10.96 18.18 10.96 - 33 23 70%
Narok 0.8% 12 34.65 4.74 5.87 4.74 21.10 4.74 1.40 14 28 >100%
Nyamira 0.0% - 9.78 - 2.36 - 2.68 - 1.67 - 7 -
Nyandarua 1.8% 29 33.83 10.96 4.93 10.96 17.27 10.96 8.24 33 30 91%
Nyeri 2.1% 32 40.13 12.26 0.72 12.26 18.35 12.26 11.65 37 31 84%
Samburu 0.6% 9 28.86 3.30 - 3.30 17.55 3.30 14.03 10 32 >100%
Siaya 5.0% 78 139.50 29.96 35.71 29.96 66.35 29.96 35.80 90 138 >100%
Taita Taveta
1.3% 20 19.59 7.69 - 7.69 12.17 7.69 3.44 23 16 70%
Tana River 0.1% 1 10.97 0.36 - 0.36 6.84 0.36 - 1 7 >100%
Tharaka Nithi
1.6% 25 31.66 9.57 10.89 9.57 11.88 9.57 3.83 29 27 93%
Trans Nzoia
0.4% 6 24.41 2.47 6.48 2.47 16.88 2.47 3.38 7 27 >100%
Turkana 2.6% 40 55.13 15.35 16.67 15.35 16.24 15.35 29.26 46 62 >100%
Uasin
Gishu
0.0% - 37.99 - - - 36.98 - 3.26 - 40 -
Vihiga 0.7% 11 24.80 4.30 10.75 4.30 5.39 4.30 10.66 13 27 >100%
Wajir 0.1% 2 4.39 0.64 2.32 0.64 1.57 0.64 - 2 4 >100%
West Pokot
0.3% 5 12.24 1.84 5.47 1.84 5.01 1.84 - 6 10 >100%
Blank 0.4% 7 - 2.57 2.57 2.57 8 - -
Total 100.0% 1,211 2,004 462.50 544.70 463 760.63 463 414 1,800 1,719 96%

15
USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
Table 9: Performance data table: Number of PLHIV Nutritionally Assessed INDICATOR TITLE: Number of PLHIV nutritionally assessed via anthropometric measurement
INDICATOR NUMBER: FN_ASSESS
UNIT: DISAGGREGATE BY: COUNTY
Geographic Location Activity Title
M
ALL Data Management, Reporting
Results:
Additional Criteria Baseline (January
2015)
Results Achieved
Prior Periods
Reporting Period 31/Dec/15
Reporting Period 31/Mar/16
Reporting Period 30/Jun/16
FY 2015/16 Target % achievement If other criteria are
important, add lines for setting targets and tracking
County % alloc
Target Achieved Target Achieved Target Achieved Target Achieved
N N N N N N N N N N
Baringo 1.7% 4,904 2,363 709 1,418 709 945 709 1,259 2,838 3,622 >100%
Blank 0.4% 1,215 2,813 167 1,644 167 1,169 167
668 2,813 >100%
Bomet 0.9% 2,504 1,722 376 714 375.59 1,008 376 724 1,502 2,446 >100%
Bondo
- 1,013 - 1,013 -
-
- 1,013 -
Bungoma 0.9% 2,674 2,865 376 24 375.59 2,841 376 2,510 1,502 5,375 >100%
Busia 0.3% 815 5,390 125 1,524 125 3,866 125 2,718 501 8,108 >100%
Elgeyo Marakwet
0.4% 1,045 553 167 245 167 308 167 27 668 580 86.9%
Embu 4.6% 13,019 2,772 1,920 2,550 1,920 222 1,920 985 7,679 3,757 48.9%
Garissa 0.8% 2,250 1,472 334 1,175 334 297 334 634 1,335 2,106 >100%
HomaBay 4.9% 13,928 3,455 2,045 75 2,045 3,380 2,045 3,875 8,180 7,330 89.6%
Isiolo 0.6% 1,575 1,243 250 696 250 547 250 531 1,002 1,774 >100%
Kajiado 1.2% 3,431 1,985 501 1,985 501
501 694 2,003 2,679 >100%
Kakamega 1.9% 5,415 2,171 793 1,451 793 720 793 2,013 3,172 4,184 >100%
Kericho 2.4% 6,782 217 1,002 217 1,002
1,002
4,006 217 5.4%
Kiambu 2.2% 6,225 3,419 918 1,557 918 1,862 918 1,930 3,672 5,349 >100%
Kilifi 1.2% 3,293 435 501 435 501
501 513 2,003 948 47.3%
Kirinyaga 1.7% 4,882 3,493 709 2,334 709 1,159 709 161 2,838 3,654 >100%
Kisii 0.9% 2,664 1,170 376 963 376 207 376 183 1,502 1,353 90.1%
Kisumu 4.2% 11,812 3,112 1,753
1,753 3,112 1,753 1,618 7,011 4,730 67.5%
Kitui 1.0% 2,919 674 417 212 417 462 417 119 1,669 793 47.5%
Kwale 0.5% 1,391 378 209 161 209 217 209 137 835 515 61.7%
Laikipia 0.2% 657 1,978 83 1,805 83 173 83 115 334 2,093 >100%
Lamu 0.9% 2,598 1,737 376 1,737 376
376
1,502 1,737 >100%
Machakos 2.8% 7,865 2,523 1,169 181 1,169 2,342 1,169 2,403 4,674 4,926 >100%
Makueni 0.7% 2,062 1,865 292 271 292 1,594 292 2,567 1,169 4,432 >100%
Mandera 0.0% - 1,177 - 1,177 -
-
- 1,177 -
Marsabit 0.6% 1,507 4,730 250 4,605 250 125 250
1,002 4,730 >100%
Meru 1.6% 4,350 327 668
668 327 668 458 2,671 785 29.4%
Migori 2.9% 8,139 28,983 1,210 27,988 1,210 995 1,210 494 4,841 29,477 >100%
Mombasa 5.4% 15,531 7,019 2,254 1,592 2,254 5,427 2,254 2,842 9,014 9,861 >100%
Murang'a 2.2% 6,115 6,822 918 4,694 918 2,128 918 581 3,672 7,403 >100%
Nairobi 6.4% 18,084 21,780 2,671
2,671 21,780 2,671 20,640 10,684 42,420 >100%
Nakuru 1.8% 5,184 4,073 751 485 751 3,588 751 3,776 3,005 7,849 >100%
Nandi 1.8% 5,190 4,032 751 1,178 751 2,854 751 2,033 3,005 6,065 >100%
Narok 0.8% 2,244 169 334
334 169 334 226 1,335 395 29.6%
Nyamira 0.0% - 1,059 - 1,059 -
-
- 1,059 -
Nyandarua 1.8% 5,188 401 751 106 751 295 751 278 3,005 679 22.6%
Nyeri 2.1% 5,803 854 876 25 876 829 876 821 3,506 1,675 47.8%
Samburu 0.6% 1,565 996 250 794 250 202 250 291 1,002 1,287 >100%
Siaya 5.0% 14,188 1,156 2,087 442 2,087 714 2,087 601 8,347 1,757 21.1%
Taita
Taveta
1.3% 3,643 2,730 543 2,708 543 22 543 88 2,170 2,818 >100%
Tana River 0.1% 172 442 42 442 42
42
167 442 >100%
Tharaka
Nithi
1.6% 4,530 627 668
668 627 668 640 2,671 1,267 47.4%
TransNzoia 0.4% 1,169 598 167
167 598 167 1,132 668 1,730 >100%
Turkana 2.6% 7,268 1,618 1,085
1,085 1,618 1,085 1,331 4,340 2,949 67.9%
Uasin
Gishu
0.0% - 4,846 -
- 4,846 - 2,693 - 7,539 -
Vihiga 0.7% 2,034 59 292 40 292 19 292 2,940 1,169 2,999 >100%
Wajir 0.1% 302 - 42
42
42
167 - 0.0%
West Pokot
0.3% 871 1,058 125 1,044 125 14 125 60 501 1,118 >100%
Total 100.0% 219,000 146,374 32,301 72,766 32,301 73,608 32,301 67,641 166,931 214,015 >100%

16
USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
Table 10: Performance data table: Number of clinically malnourished clients receiving commodities INDICATOR TITLE: Number of HIV positive clinically malnourished clients who received therapeutic and/or supplementary food
INDICATOR NUMBER: FN_THER
UNIT: DISAGGREGATE BY: COUNTY
Geographic Location Activity Title
M
ALL Data Management, Reporting
Results:
Additional Criteria Baseline
(January
2015)
Results Achieve
d Prior Periods
Reporting Period 31/Dec/15
Reporting Period 31/Mar/16
Reporting Period 30/Jun/16
FY 2015/16 Target %Achievem
ent
If other criteria are
important, add lines for setting targets and tracking
County % Target Achieved
Target Achieved
Target Achieved
Target Achieved
N N N N N N N N N N
Baringo 1.7% 1,668 68 425 425 68 425 163 1,698 231 13.6%
Blank 0.4% 852 219 100 132 100 87 100 400 219 54.8%
Bomet 0.9% 910 272 225 144 225 128 225 135 899 407 45.3%
Bondo 277 - - - - - - -
Bungoma 0.9% 356 550 225 56 225 494 225 616 899 1,166 >100%
Busia 0.3% 4,429 563 75 152 75 411 75 587 300 1,150 >100%
Elgeyo
Marakwe
t
0.4% 766 43 100 23 100 20 100 8 400 51 12.8%
Embu 4.6% 4,739 336 1,149 249 1,149 87 1,149 398 4,595 734 16.0%
Garissa 0.8% 536 - 200 200 200 56 799 56 7.0%
Homa Bay
4.9% 1,167 2,646 1,224 1369 1,224 1277 1,224 1185 4,894 3,831 78.3%
Isiolo 0.6% 1,842 373 150 276 150 97 150 209 599 582 97.1%
Kajiado 1.2% 2,308 41 300 41 300 300 98 1,199 139 11.6%
Kakamega
1.9% 2,118 616 474 306 474 310 474 344 1,898 960 50.6%
Kericho 2.4% 1,120 36 599 36 599 599 2,397 36 1.5%
Kiambu 2.2% 1,661 1,479 549 433 549 1046 549 1079 2,197 2,558 >100%
Kilifi 1.2% 906 126 300 126 300 300 88 1,199 214 17.9%
Kirinyaga 1.7% 4,019 1,435 425 683 425 752 425 67 1,698 1,502 88.5%
Kisii 0.9% 993 605 225 408 225 197 225 175 899 780 86.8%
Kisumu 4.2% 473 1,766 1,049 756 1,049 1010 1,049 422 4,195 2,188 52.2%
Kitui 1.0% 224 465 250 252 250 213 250 74 999 539 54.0%
Kwale 0.5% 884 8 125 125 8 125 71 499 79 15.8%
Laikipia 0.2% 2,676 314 50 182 50 132 50 105 200 419 >100%
Lamu 0.9% 702 40 225 40 225 225 899 40 4.4%
Machako
s
2.8% 513 1,262 699 639 699 623 699 287 2,797 1,549 55.4%
Makueni 0.7% 1,480 118 175 52 175 66 175 127 699 245 35.0%
Mandera 0.0% 2,769 - - - - - - -
Marsabit 0.6% 5,284 85 150 58 150 27 150 319 599 404 67.4%
Meru 1.6% 2,080 362 400 139 400 223 400 1,598 362 22.7%
Migori 2.9% 6,153 1,414 724 781 724 633 724 404 2,897 1,818 62.8%
Mombasa 5.4% 1,764 811 1,348 372 1,348 439 1,348 405 5,394 1,216 22.5%
Murang'a 2.2% 1,766 189 549 549 189 549 196 2,197 385 17.5%
Nairobi 6.4% 764 5,799 1,598 3794 1,598 2005 1,598 1928 6,393 7,727 >100%
Nakuru 1.8% 1,765 1,179 449 608 449 571 449 776 1,798 1,955 >100%
Nandi 1.8% 1,974 74 449 31 449 43 449 208 1,798 282 15.7%
Narok 0.8% 532 4 200 200 4 200 18 799 22 2.8%
Nyamira 0.0% 4,827 40 - 40 - - - 40 -
Nyandarua
1.8% 1,239 530 449 343 449 187 449 228 1,798 758 42.2%
Nyeri 2.1% 58 652 524 394 524 258 524 415 2,098 1,067 50.9%
Samburu 0.6% 1,541 35 150 150 35 150 242 599 277 46.2%
Siaya 5.0% 398 1,157 1,249 626 1,249 531 1,249 406 4,994 1,563 31.3%
Taita
Taveta
1.3% 2,473 57 325 51 325 6 325 1,299 57 4.4%
Tana River
0.1% 692 24 25 24 25 25 71 100 95 95.1%
Tharaka Nithi
1.6% 103 813 400 367 400 446 400 550 1,598 1,363 85.3%
Trans
Nzoia
0.4% 296 159 100 51 100 108 100 383 400 542 >100%
Turkana 2.6% - 1,563 649 968 649 595 649 524 2,597 2,087 80.4%
Uasin Gishu
0.0% - 270 - - 270 - 759 - 1,029 -
Vihiga 0.7% - 169 175 169 175 175 364 699 533 76.2%
Wajir 0.1% - 5 25 25 5 25 100 5 5.0%
West
Pokot
0.3% 413 14 75 75 14 75 300 14 4.7%
Total 100.0% 74,511 43,276 19,328 15,171 19,328 13,615 19,328 14,490 99,885 43,276 43.3%

17
USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
Table 11: Performance data table: Number of clients found to be clinically malnourished INDICATOR TITLE: Number of PLHIV that were nutritionally assessed and found to be clinically undernourished
INDICATOR NUMBER: FN_THER
UNIT: DISAGGREGATE BY: COUNTY Geographic Location Activity Title Date M
ALL Data Management, Reporting
Results:
Additional Criteria Baseline
(January
2015)
Results
Achieved
Prior
Periods
Reporting Period
31/Dec/15
Reporting Period
31/Mar/16
Reporting Period 30/Jun/16 FY 2015/16
Target
%
Achievement If other criteria are
important, add lines
for setting targets and
tracking
County %
Target Achieved Target Achieved Target Achieved Target Achieved
N N N N N N N N N N
Baringo 1.7% 1,930 578 425 360 425 218 425 301 1,698 879 51.8%
Blank 0.4% 985 575 100 295 80 280 100 400 575 >100%
Bomet 0.9% 1,052 512 225 333 180 179 225 132 899 644 71.6%
Bondo
321 - - - -
-
- - -
Bungoma 0.9% 411 816 225 110 180 706 225 618 899 1,434 >100%
Busia 0.3% 5,124 1,321 75 243 60 1,078 75 684 300 2,005 >100%
Elgeyo
Marakwet
0.4% 886 50 100 8 80 42 100 8 400 58 14.5%
Embu 4.6% 5,481 783 1,149 693 919 90 1,149 386 4,595 1,169 25.4%
Garissa 0.8% 620 147 200 26 160 121 200 132 799 279 34.9%
Homa Bay 4.9% 1,350 2,279 1,224 990 979 1,289 1,224 1,225 4,894 3,504 71.6%
Isiolo 0.6% 2,131 565 150 392 120 173 150 217 599 782 >100%
Kajiado 1.2% 2,669 51 300 51 240 300 95 1,199 146 12.2%
Kakamega 1.9% 2,450 557 474 251 380 306 474 475 1,898 1,032 54.4%
Kericho 2.4% 1,296 223 599 223 479
599
2,397 223 9.3%
Kiambu 2.2% 1,921 2,003 549 919 439 1,084 549 1,322 2,197 3,325 >100%
Kilifi 1.2% 1,048 135 300 135 240
300 201 1,199 336 28.0%
Kirinyaga 1.7% 4,649 1,494 425 763 340 731 425 66 1,698 1,560 91.9%
Kisii 0.9% 1,149 444 225 272 180 172 225 137 899 581 64.6%
Kisumu 4.2% 547 1,971 1,049 836 839 1,135 1,049 578 4,195 2,549 60.8%
Kitui 1.0% 259 463 250 311 200 152 250 94 999 557 55.8%
Kwale 0.5% 1,022 239 125 152 100 87 125 56 499 295 59.1%
Laikipia 0.2% 3,095 196 50 - 40 196 50 93 200 289 >100%
Lamu 0.9% 812 25 225 25 180
225
899 25 2.8%
Machakos 2.8% 593 1,391 699 647 559 744 699 656 2,797 2,047 73.2%
Makueni 0.7% 1,712 482 175 239 140 243 175 504 699 986 >100%
Mandera 0.0% 3,203 - - - -
-
- - -
Marsabit 0.6% 6,112 115 150 69 120 46 150 599 115 19.2%
Meru 1.6% 2,406 412 400 172 320 240 400 314 1,598 726 45.4%
Migori 2.9% 7,117 1,246 724 596 579 650 724 289 2,897 1,535 53.0%
Mombasa 5.4% 2,040 2,200 1,348 1,225 1,079 975 1,348 1,006 5,394 3,206 59.4%
Murang'a 2.2% 2,042 512 549 - 439 512 549 313 2,197 825 37.5%
Nairobi 6.4% 883 7,088 1,598 4,185 1,279 2,903 1,598 2,123 6,393 9,211 >100%
Nakuru 1.8% 2,042 1,437 449 643 360 794 449 1,161 1,798 2,598 >100%
Nandi 1.8% 2,284 1,037 449 672 360 365 449 355 1,798 1,392 77.4%
Narok 0.8% 616 34 200 - 160 34 200 58 799 92 11.5%
Nyamira 0.0% 5,584 25 - 25 - - - 25 -
Nyandarua 1.8% 1,434 452 449 265 360 187 449 171 1,798 623 34.7%
Nyeri 2.1% 68 1,140 524 701 420 439 524 407 2,098 1,547 73.8%
Samburu 0.6% 1,783 165 150 - 120 165 150 220 599 385 64.2%
Siaya 5.0% 460 906 1,249 471 999 435 1,249 388 4,994 1,294 25.9%
Taita Taveta 1.3% 2,860 222 325 34 260 188 325 66 1,299 288 22.2%
Tana River 0.1% 801 12 25 12 20 25 100 12 12.0%
Tharaka
Nithi
1.6% 119 803 400 480 320 323 400 377 1,598 1,180 73.8%
Trans Nzoia 0.4% 343 153 100 84 80 69 100 307 400 460 >100%
Turkana 2.6% - 2,243 649 1,319 519 924 649 724 2,597 2,967 >100%
Uasin Gishu 0.0% - 989 - - - 989 - 976 - 1,965 -
Vihiga 0.7% - 154 175 149 140 5 175 489 699 643 92.0%
Wajir 0.1% - - 25 - 20
25
100 - 0.0%
West Pokot 0.3% 478 7 75 - 60 7 75 50 300 57 19.0%
Total 100% 86,187 38,652 19,328 19,376 15,547 19,276 19,328 17,774 99,885 56,426 56.5%

18
USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
IV. CONSTRAINTS AND OPPORTUNITIES
Staff Constrains: Currently, staffing level for the program stands at 23 Full Time Employees (FTE), with
additional 8 personnel providing administrative support from the shared services. Of the 23 FTE, 5 are
drivers, 7 are nutritionists including the DCOP, 4 are M&E specialist, 2 are in finance, 2 are administrative
staff, 1 agricultural specialist and 2 supply chain specialists that includes the COP. Currently, we have
nutritionist officer and driver located in each focus. The nutrition officers are providing crosscutting
services from nutrition to nutrition-sensitive agriculture programing. The program requires to
demonstrate reduction in stunting in each of the key focus counties of Tharaka Nithi, Kitui, Busia, Samburu
and Marsabit. This requires intensive programming and adequate personnel to provide stewardship in
nutrition-sensitive agriculture programing. Additional personnel are therefore required for the program to effectively deliver on its mandate.
DA1 Form Delay: The program procures RUTF from Insta Products (EPZ), located at the Export
Processing Zone. Procurement originating from the Export Processing Zone requires waiver processing
using the DA1 Form. The program has put in applications for exemption of duty and VAT for RUTF
procured from Insta Products (EPZ) duly accompanied by supporting documents. Beginning January 2016,
the program has put in two DAI Forms for approval, one in October 2015 and the second one in February
2016, but none has received any approval for exception. Due to the exemption approval process taking
long than expected the program has not been able to supply RUTF to the needy clients thereby making it difficult for the program to reach its target.
Facility Reports: Challenges continues to be encountered of receiving commodity and service data from
the facility. These are mainly attributed to GoK staff turnover at facility level due to decentralization of
health services to county level; Inadequate number of HCWs trained to support nutrition assessment and
reporting; Inadequate number and insufficient resources to support CHVs to conduct active case finding,
follow up and provide linkage through community program.
Financial Management: Funds to for the program’s use are held in a common bank account shared by
all projects within the country office. It is therefore not possible to separately determine direct charges
arising from the transactions directly related to the project. Similarly, the interests earned on funds in the bank accounts cannot be verified and separated/isolated for reporting requirements.
Billing to the project is also done from a central pool for both direct and indirect costs. Expenses related
to the indirect costs are not reviewed at project level before being posted to the system. Consequently,
there have been challenges which have arisen in the past, mainly resulting from over billing especially on
administrative related costs and incidences of labor costs billing to the project for staff not in the approved
agreement.
Further due to the centralized billing of shared costs, VAT charges for shared costs are also allocated to
the program proportionately. This approach has posed challenges especially during preparation of the
annual VAT reports. Programs are required to report on VAT status every year and where costs and
expenses are shared, it has been difficult to isolate and track the status for VAT related to shared costs.
V. PERFORMANCE MONITORING
Updates for performance relating to survey base indicators is expected to be updated during the fourth
quarter once surveys for Tharaka and Busia are completed.
During the quarter, the program supported a total of 857 health facilities with data management and
reporting representing an overall reporting rate of 85.7% (857/1000) of target facilities. Overall, there was
increased facility reporting of 29.0% from the preceding quarter (857 vs 609). 383 of these facilities have
been designated as commodity delivery points. To ensure improved facility reporting rates, the program
will continue to engage with CNCs, facility nutrition contact persons and APHIA+ partners’, increase
CME/OJT and joint supervision and sharing of monitoring data reports. The program will also plan to
transition 17 additional high volume facilities into EMR facilities.
Of the to 857 health facilities supported with data management and reporting, 122 submitted their service
data sets and commodity orders electronically. From data already processed during the quarter, a total
of 83,911 clients were assessed with 14,490 of these found to be malnourished being provided with FBF
supplementation during the FY16 Quarter. By the time of compilation of this report, an additional 54,653
client assessments and 15,638 client FBF prescriptions reports are in the process of being entered into the database.
During the quarter, fourteen (14) additional high volume facilities were supported with customized
nutrition electronic software to support data management at facility level. This will enhance timeliness on
data reporting. HCWs who will be responsible for delivery of NACS services were inducted on use of
the nutrition reporting software. However, challenges relating to source documentation errors, high staff
turnover, acceptance of EMR system and existence of parallel partner reporting systems continued to be
observed. During the site visits the following observations were made:

19
USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
• Service and commodity data reporting challenges.
• Some facilities are not willing to share all required datasets especially prescriptions forms.
• Facilities are not consistently submitting assessment data but submit only prescription data.
• Reporting delays.
• Some EMR sites are submitted hardcopies of their data claiming increased workload due to
multiple registers and reporting requirements from other IPs. E.g. Tigoni DH, Lumumba HC,
Nandi Hills DH, Tharaka DH, Muranga DH and Thika Level 5 Hospital.
• Use of standardized quantification units for MOH734 still a challenge.
In mitigation of the above challenges, the program will continue scheduled NACS training and re-
sensitization activities. The program will also work to bridge the knowledge gap through partnership with IPs to support OJT and CME sessions at facility level.
Despite the program having supported successful installation of the nutrition EMR at Memorial AF
Hospital and sensitization of the nutritionist on how to use the system for both service and commodity
data reporting, the facility did not submit service data and commodity orders as expected. The facility
also requested the program to remove personal patient details from their system as this would cause a
security risk. Plans are under way to have all Forces hospitals/clinics report through the Mbagathi
Memorial Hospital. The program will schedule additional training session in the next quarter to induct the newly appointed nutritionist. The program will also target to induct HCWs from other cadres.
To improve data quality, increase data use at facility and county/sub-county levels, the program conducted
a re-sensitization of eight (8) health facilities within Nairobi, Muranga, Kajiado and Nyeri counties primarily
due to staff re-deployment. The facilities were re-sensitized during the quarter included Nyahururu SC
Referral Hospital, Nyeri Provincial General Hospital (PGH), Muriranjas Sub-District Hospital, Makuyu Health Centre, Gatundu DH, KNH, Kajiado County Hospital, Kibera Community HC AMREF.
The customized nutrition EMR system was developed to support management of both service and
commodity functions relating to delivery of NACS at facility level. In addition, the system has the capability
to produce summary data for national service and commodity reporting through DHIS and patient level
data for the yearly forecasting and quantification process for nutrition commodities. The system also
ensures accountability of delivered commodities by rationalizing facility orders based on their reported
consumption.
In support of enhanced provision of NACS at facility level, the program supported electronic nutrition
reporting scale up in 10 high volume facilities. All these facilities received both HW and SW support from
the program. Overall, a total of 15 HCWs comprising of 13 nutritionists, 1 in-charge and 1 nursing officer
were trained on the use of the electronic reporting system. Installation at AIC Litein’s did not proceed as
planned as the base OS was not compatible with the current version of the nutrition EMR. The facility is
in the process of upgrading their in-house OS software’s to allow installation. The program will conduct
site supervision support in collaboration with WRP to explore ways of assisting this and other high volume
facilities within the South Rift region. Facilities scaled up this quarter are: Mbita District Hospital, Homa
Bay District Hospital, Rachuonyo District Hospital, Boro Dispensary, Nyahera Sub District Hospital,
Rabuor Health Centre, Suba District Hospital, Rangwe Sub-District Hospital, Bar Agulu Dispensary, Kaluo
Dispensary.
In an effort to support electronic reporting for 54 focus county MNCH facilities/service points, the
program has finalized database architecture and draft validation rules for MOH 511, CWC register. To
further ensure continuum of client services, the system will be integrated with the current NACS facility
reporting system to support tracking of referral cases. It is expected that pilot testing will be concluded
in FY16 Quarter 4 with deployment commencing once identification of facilities with capacity is completed.
With support from SCNO Dagoretti County, the program conducted site support/supervision visits at
Riruta H.C. and Waithaka H.C. The purpose of this visits was to pilot test a supervision tool jointly
developed by the program and sub-county. The following services, activities and systems were reviewed and challenges and observations documented for further action:
• Type of services provided at the facility (GMP, VAS, MNP, Deworming, IMAM, Maternal
Nutrition, Maternity, TB, HIV, Nutrition)
• Availability of other health system strengthening activities (Scheduled Capacity Building,
quality improvement approaches and Community Linkages/referrals)
• Availability and use of nutrition guidelines and/or job aids
• Stock and Inventory Management
• Dispensing and Storage
• Reporting/ICT support including quality of nutrition reports
Additional support visits to Lea Toto Dagoretti and Kawangware will be scheduled for the next quarter
to review progress of mitigation activities for commodity and reporting challenges observed in the
previous quarter. It was observed that due to lack of adequate human resource capacity at Waithaka HC,
interns had been recruited to run nutrition activities at the CWC and CCC service points; Inadequate

20
USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
equipment for nutrition assessment observed; Service points were not adhering to reporting protocols
in the utilization of bin cards and tally sheets when reporting nutrition commodities; In adequate capacity
for proper follow up of NACS patients due to lack of support for CHVs; Disjointed commodity
management across service points; OTP register and Daily Activity Register for Nutrition Services have
the same MOH number (MOH409); Vitamin A issued at CWC clinic not reported consistently due to
lack of tally sheets; High defaulter rate for ART and NACS/FBP program. Recommends made includes
integrating management of existing nutrition pipelines to ensure central administration; Scale up HIV
testing for all clients at CCC; upgrading of Waithaka HC from satellite to delivery point; Encouraging
CHVs attached to the TB program to also support case finding and follow up for nutrition at community
level.
With the initial version of the nutrition portal complete, the program through NDU has reached out to
county nutrition managers, stakeholders and IPs to provide feedback that will inform final revision. The
second version, to be completed within the next quarter will incorporate interactive and dynamic data
visualization user interfaces. These will allow authorized users to upload, analyze and view data from
routine data sets, surveys and research studies. It is expected that this will allow nutrition health managers to consume this information for informed decision making.
To further support nutrition service reporting at CWC service points, the program is in the process of
finalizing a simple MS Access/SQL based system for data management and reporting. The system will also
be integrated with the facility NACS EMR system to ensure continuity of care through patient monitoring across service points.
VI. PROGRESS ON ENVIRONMENTAL MITIGATION AND MONITORING
The program finalized development of Environmental Review Report (ERR) for the purpose of screening
program food manufacturing activities undertaken by selected Food Manufacturing Factories (Equatorial
Nuts Processors Ltd. and Insta Products (EPZ) Ltd.) as per USAID requirement. Specifically, the program
aimed to identify potential levels of environmental risk due to food manufacturing activities that would
lead to the occurrence of adverse environmental impacts. Arising from this, the program developed and
an Environmental Mitigation and Monitoring Plan (EMMP) to ensure mitigation measures are implemented
to prevent or minimize the occurrence of adverse impacts, to make food manufacturing and storage
activities environmentally-sound. Continuous monitoring during program implementation will hence forth
be undertaken to assess the status and progress of recommended mitigation measures during the program
lifecycle to ensure that timely remedial measures are undertaken. Appropriate indicators and tools have
been developed with sensitization scheduled to be finalized during FY16 Quarter 4.
VII. PROGRESS ON LINKS TO OTHER USAID PROGRAMS
Continuous engagement has been made with all the PREG partners geared towards carrying activities
through collaboration and linkages towards pursuing NHPplus objectives of reducing stunting and
improving nutritional status through nutrition programming in agriculture. During the USAID mission visit,
one opportunity of infusing nutrition messages through training and establishment of the demonstration
garden at the Moyale livestock market came out glaring. The program continues to work with all PREG partners and APHIAplus partners.
A preliminary and ground setting visit by the DCOP mid-June after discussions with the community
revealed that dietary diversity in terms of access, production technologies and consumption of especially
vegetables is a big challenge to the community. Also mentioned were local poultry keeping especially for
mothers and youth. The specific vegetables mentioned include kale, spinach, tomatoes, sweet pepper, hot
pepper and fruits especially melons. These if community trained to raise would go a long way in improving
diets as well as providing some source of income as the current source for the scarce products is Meru county. Already over half acre of land is available downstream of the Moyale market ideal for the activity.
VIII. PROGRESS ON LINKS WITH GOK AGENCIES
The program has been working closely with the NDU, NASCOP, MOE and MOALF. One of the successful
activity accomplished during this reporting period i.e. Malezi bora is attributed to their combined efforts
as program engaged all the mentioned line ministries.

21
USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
1X. SUBSEQUENT QUARTER’S WORK PLAN
Table 12: Planned activities from previous quarter
Planned Actions from Previous Quarter Actual Status this
Quarter
Explanations for Deviations
1.0 Improve access and demand for Quality Nutrition Interventions at Community and Facility levels
1.1 Strengthened leadership, advocacy and policy planning
1.1.1 Support expenses for multi-stakeholder one-day planning
meeting for PROFILES activities with core group
Scope of work developed.
Stakeholder workshop
scheduled for Feb 2017
More time required for planning
and multisector engagement
1.1.11 Participate and support meeting expenses monthly
MIYCN TWG
Attended meeting No meeting expenses supported
1.1.12 Participate and support monthly Food and Nutrition
Linkages TWG
1.1.13 Support meeting expenses and participate in the national
Nutrition commodity pipeline subcommittee
Participated in HIV
commodity security TWG
1.1.14 Support meeting expenses and participate in Quarterly
National Commodity steering committee
Attended tech specs
subcommittee meeting
1.1.15 Support meeting expenses and participate in the Nutrition
Information TWG meetings
1.1.16 Support meeting expenses and provide TA Clinical
Nutrition and Dietetics TWG
Received draft and had
discussions with secretariat
1.1.17 Support meeting expenses for County Nutrition
technical forum (CNTF) meetings in Marsabit, Samburu,
Tharaka-Nithi, Kitui and Busia
No CNTF Scheduled next quarter
1.2 Improved Nutrition service delivery management, coordination and implementation
1.2.1 Support expenses for review of training materials, job aids
and NACS protocols beyond HIV, to include, HiNi, Agri-
Nutrition messages and linkages to livelihood activities
NACS FBP flip chart under
procurement
1.2.2 Facilitate training expenses for Training of USG IP's
including FtF Partners using the revised NACS curriculum
Completed
1.2.3 Conduct training at County level to build capacity of
additional health facilities to provide NACS services
beyond HIV and report service and consumption data
Planned for next quarter
1.2.4 Support upgrade of High volume lower level facilities to
delivery points (desk review no cost activity)
This is continuous activity
1.2.5 Support logistics expenses (lunch & transport) for health
facility HiNi gap assessment in Tharaka, and Samburu
focus counties
HiNi gap assessment
conducted in 2 counties
1.2.11 Support Quarterly OJT and mentorship activities with
sub-county teams in focus counties
Conducted in Nairobi
1.2.17 Support Training of data officers for piloting of Nutrition
monitoring and reporting system into an interoperable
web based system
Training conducted in
Nyanza region
1.2.18 Rollout of web based system to 100 facilities into
electronic nutrition reporting system
1.2.19 Revision of existing Nutrition portal into a robust/scalable
interoperable platform to support KM/KT to support a
multi sectorial nutrition programming
1.2.20 Analyze data for submission of APR PEPFAR Report
1.2.21 Conduct quarterly joint data quality facility assessments
and mentorship visits
1.2.25 Distribute NACS inclusive of HiNi job aid (desktop flip
chart)
1.3 Improve nutrition related behavior
1.3.9 Support expenses for identified National MNCH/
Nutrition activities & county festivals/ shows
Malezi bora activities
conducted
1.3.9.1 MALEZI BORA
Printing of branded materials: t-shirts, caps, banners, leso,
posters
Done
Support planning meeting for Malezi Bora at sub-county
level
Done
Conduct social mobilization at community level (5-day
maximum)
Done
Facilitate cooking demonstration expenses at the
community & Malezi Bora Day (ECDE/CU)
Done
Malezi bora Post review meeting at sub county level
1.5 Increased knowledge and skills of health care workers (HCWs) in nutrition
1.5.4 Support NACS training expenses for IPs and MOH Done
2.0 Strengthened Nutrition Commodity Management
2.1 Improved production, supply and distribution of nutrition commodities
2.1.1 Facilitate procurement and distribution of 424MT (23,556
Cartons) of FBF comprising:
FBF Adults: 254MT (14,133 cartons)
FBF Children: 127.2 MT (7,067 cartons)
FBF Pregnant/postpartum: 42.4 MT (2,356 cartons)
Done
2.1.2 Print Data Collection/Reporting tools
MOH 407A: 1,000
MOH 407B: 1,000
On course

22
USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
MOH 733B, 900
MOH 734B: 900 and Appointment Cards: 100,000
2.1.3 Print 2,000 copies of NACS/FBP Desktop job aids On course
2.1.4 Distribute job aids and data collection/reporting tools Not done Awaiting finalization of
procurement process
2.1.5 Procure and distribute anthropometric equipment for
MCH service point in level 4 facilities
Sourcing for quotations -
done
Evaluation of received
quotations - on-going;
2.1.6 Participate and contribute to development of
Quantification plan for Nutrition Sector
Not done Postponed to coming quarter by
MOH
2.1.7 Participate and contribute to development of
procurement plan for Nutrition Sector
Not done Postponed to coming quarter by
MOH
2.1.8 Roll-out of Electronic CDRR to all nutrition service points On course – xxx number of
facilities pretesting the e-
CDRR
2.1.9 Contribute to the Monthly NHPplus Supply Chain
Information workbook for NDU/NASCOP
Done
2.1.10 Provide service and commodity data for the monthly
Two-page summary for NDU pipeline subcommittee &
NASCOP
Done
2.1.11 Participate and/or support in the nutritional commodity
security technical working group
Done
2.1.12 Conduct facility monitoring visits Done
2.2 Improved quality and safety of food commodities and agricultural products
2.2.1 Conduct Supplier Quality Audit for Equatorial Nut
Processors and Insta Products
Done Summary of findings to be shared
in the coming quarter
2.2.2 Conduct post procurement batch testing Sampling completed
Testing/Results to be Done
in the coming quarter
2.3 Strengthened sustainability and innovation in nutrition commodity development and management
2.3.2 Track proportion of locally sourced agricultural raw
materials used in FBF and RUTF procured through
NHPplus
Done
3.0 Improved food and nutrition security
3.1 Increased market access and consumption of diverse and quality foods
3.1.1 Conduct consultative meetings with focus counties Done in Busia MOALF and
MOH staff during FtF
evaluation visit
Meeting for Kitui scheduled 4th
quarter
3.1.2 Conduct inception meetings in the FtF focus counties with
multi-sectoral stakeholders and partners at county & sub-
county levels
Consultative discussions
held with multi-sectoral
stakeholders and partners
on agri-nutrition during
national meetings
County based meetings to
continue quarter 4
3.1.3 Conduct baseline/ Mid-term assessment on multi-sectoral
nutrition programing (health, agriculture, WASH and
nutrition) 5 focus counties i.e. Zones of influence
(including SBCC, food varieties, consumption patterns,
nutrition status, social economic status, demographics)
Done for Samburu Quarter 4 planned for Marsabit,
Tharaka Nithi and Kitui
Training of enumerators Done for Samburu To be trained for the other
counties during survey
3.1.4 Identification of zones of influence Done
3.1.5 Conduct Identification of community groups (women,
youth, Mother to mother support groups, farmer groups)
Done for Busia, Tharaka
Nithi, Kitui, Samburu
Process to continue quarter 4
3.1.6 Conduct contextualization workshop for Applied Basic
Agri-Nutrition Manual (KHCP Manual) for Busia, Kitui,
Marsabit, Samburu & Tharaka Nithi
Process initiated 2-day technical workshop planned
for quarter 4
3.1.7 Conduct county Validation workshops for the
contextualized draft Agri-Nutrition Manual
Not done Awaiting manual
3.1.8 Conduct meetings to develop contextualized recipe
guides: e.g., maternal nutrition, complementary feeding
(Vit. A, iron rich foods, other nutrient dense foods)
Tech team constituted for
Busia
Cassava recipe guide for Busia and
Kitui to support printing
3.1.9 Conduct TOT Trainings for sub-county (FEWs, CHEWs,
DICECEs, community resource persons) on use and
adoption of appropriate technologies e.g., kitchen
gardens, food preservation, water harvesting to increase
household food production and consumption (ref 1.5 for
MSN trainers guide)
Not done To be quarter 4 all counties
3.1.10 Define a demonstration kit for the focus counties based
on identified appropriate technologies
Not Done To be done during the MSN
training
3.1.11 Conduct demonstrations to showcase the application of
simple appropriate technologies for increasing household
food production, consumption of iron, vit. A rich food e.g.,
kitchen gardens, cooking demos, water harvesting to community groups
Done in 2 counties
Cooking demos done
Gardens planned for quarter 4 in
the 3 counties
3.1.12 Train CHEWS/PHTs, ECDE teachers, and FEWS on
Maternal nutrition, IYCF, dietary diversity (Iron & Vit A)
and WASH, key messages for social mobilization
Not done To be done by ToTs from MSNS
training
3.1.13 Sensitize NDMA field monitors, CHCs, CHVs on
Maternal nutrition, IYCF, dietary diversity (Iron & Vit A)
and WASH, key messages for social mobilization
Not done To be done by ToTs from MSNS
training

23
USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
3.1.14 Support community based resource persons (FEWs,
CHEWs, DICECEs,) to disseminate key agri-nutrition and
WASH messages at sub-county level platforms e.g. Farmer
Field schools, community units, chief barazas, MtMSGs, 4K
clubs
Done To continue in all counties
3.2 Improved Resilience
3.2.1 Support workshop expenses for capacity building to
conduct SMART surveys for 2 sub counties in selected
focus counties
Done for Samburu Other counties planned quarter 4
3.2.2 Support SMART survey expenses (transport & stationery)
every 2 years in Marsabit, Samburu & Kitui
Done Other years planned
3.2.3 Support dissemination of survey results (Baseline/ Mid-
term)
Done Awaits survey results
3.2.4 Map existing food security, livelihood and economic
support in the focus counties/ zones of influence (desk
review)
Done Busia to be done quarter 4
3.2.5 Support consultative meeting expenses to define
contextualized food security, livelihood and economic
support package
Not done To be done alongside MSNS
training
3.2.6 Collect and collate data on referral cases from 2 facilities
per ward in 2 sub-counties per county
Done Data got for all counties and 144
in-patient referral cases identified,
process on-going
3.2.8 Support group meeting expenses for linked vulnerable
households to economic strengthening activities
Not done Working with NDMA
3.2.9 Support logistics expenses to identify vulnerable
children/adults through NDMA sentinel site assessment
(drought early warning & monitoring household
questionnaire or Household Hunger score) tool
Done for Samburu Other counties data not compiled
3.2.12 Support training expenses for (change agents) DICECEs,
Gender & Social services agents and NDMA officers
dealing with OVC, Older persons, People with disability
cash transfers on key MIYCN messages for social safety
net programs
Not done Planned for quarter 4 after NDMA
training
3.2.13 Support logistics expenses for DICECEs, Gender social
services, NDMA officers, FtF IPs to conduct community
forums on how to effective use of cash transfers for
improved nutrition
Not done Planned for quarter 4 after NDMA
training
3.2.14 Support workshop expenses to develop food production
and consumption pamphlet based on cash transfer amount
to inform vulnerable households
Not done Planned for quarter 4 after NDMA
training
3.2.15 Facilitate expenses for a TOT at sub-county level on
community managed disaster risk reduction
Not done Community level CMDRR planned
for Kitui and Tharaka Nithi quarter
4
3.2.16 Support meeting expenses conduct participatory disaster
risk reduction assessment at ward level
Not done Community level CMDRR planned
for Kitui and Tharaka Nithi quarter
4
3.2.17 Support meeting expenses for Dissemination of Disaster
Risk Reduction plans at sub-county, ward levels
Not done Community level CMDRR planned
for Kitui and Tharaka Nithi quarter
4
3.2.18 Support expenses to train NDMA early warning system
field monitors on Nutrition screening & referral using
MOH 100
Done 39 staff trained others planned for
quarter 4
3.2.19 Support printing of seasonal planner Not done Waiting for season
3.2.20 Support the FEWs to conduct dissemination meetings of
seasonal planner at the ward level
Not done Waiting for season
3.2.21 Support meeting expenses for PREG Monthly consultative
forum
Rotational Planned in October

24
USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
X. FINANCIAL INFORMATION

25
USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
XI: ANNEXES & ATTACHMENTS:
ANNEXE I: PERFORMANCE MONITORING Type Indicator Name FY16
Target Oct-Dec 2015 Jan-Mar 2016 Apr-June 2016 FY 2 %
Achievement
as of June 2016
Target Achieved Target Achieved Target Achieved Target Achieved
PMP # of mechanisms created to facilitate coordination on an ongoing basis as a
result of USG Assistance (e.g. forum, working group, MOU, shared plans,
associations, budgeting work planning, projects) Note that it is important to identify best practices as they emerge. (NICC, NICC-TWG, NICC-TWG
Subcommittees, CNTF)
10 2 0 2 4 2 6 6 10 >100%
PMP # of people trained. Mentored, provided TA at National Level. 10 0 0 2 0 6 0 8 0 -
PMP Number of policies affected by USG supported efforts and advocacy campaigns)
0 0 0 1 1 0 0 1 1 100.0%
PPR Number of health facilities with established capacity to manage acute
undernutrition (S)
54 0 0 54 0 54 56 54 56 >100%
PMP % of facilities submitting timely, complete and accurate information - 92.0% 67.0% 38.2% 67.0% 62.8% 67.0% 88.4% 92.0% 88.4% 96.1%
PPR Number of people trained in child health and nutrition through USG-supported programs
215 54 14 54 227 54 113 215 354 >100%
PMP Percentage of PLHIV who are nutritionally assessed via anthropometric
measurement
100% 100% 100% 100% 100% 100% 100% 100% 100% 100%
PEPFAR Proportion of clinically undernourished PLHIV who received therapeutic or
supplementary food 78.9% 48.1% 83.2% 48.1% 78.5% 48.1% 58.1% 78.9 58.1 73.6%
PPR Number of children under 5 who received Vitamin A from USG supported programs
72,387 18,097 0 18,097 6,866 18,097 56,691 54,291 63,557 >100%
PPR Number of children under five who are wasted (WHZ) 3,747 937 4,508 937 7,848 937 0 2,811 12,356 >100%
PPR Number of children under five who are Underweight (WAZ) 8,033 2,008 80 2,008 104 2,008 0 6,024 184 3.1%
PMP # of Advocacy guides on IYCF developed 1 0 0 0 0 1 0 1 0 -
Contract # of communication materials updated and distributed for HCWs, CHVs
and mass mobilization;
19,320 4,830 0 4,830 0 4,830 0 14,490 0 -
PMP % of county officials trained who demonstrate increased knowledge in training as result of USG support
1 0 0 1 0 0 0 1 0 -
PEPFAR The percentage of storage sites where commodities are stored according to
plan, by level in supply system.
350 0 0 0 0 0 0 350 400 >100%
PMP Numbers of Policies/Regulations/Administrative Procedures in each of the following stages of development as a result of USG assistance
1 0 0 1 1 0 0 1 1 100%
PMP Number of private enterprises producer organizations, water users’
associations, women’s groups, trade and business associations and community based organizations [C0Bs] that applied improved technologies or management practices as a result of USG assistance
1 0 1 0 0 0 0 0 1 -
PMP # of people trained. Mentored, provided TA at National/County Level on SCALE,
125 31 31 8 0 0 0 125 31 24.8%
Contract % change of cost for nutrition commodities 2% 0 0 0 0 0 0 0 0 -

26
USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
Contract # of active health facilities reporting stock outs for FBF and RUTF in the preceding six months)
<20% <20% <20% <20% <20% <20% <20% <20% <20% 100.0%
Contract # of mechanisms created to facilitate coordination on an ongoing basis as a result of USG Assistance
2 1 0 1 0 0 2 2 2 100.0%
Contract Number of facilities implementing comprehensive NACS at health facilities (beyond CCC/ART sites)
400 100 0 100 150 100 161 400 161 40.3%
Contract Number of standardized SBC nutrition materials distributed (and revised if
necessary) to community health and agricultural extension workers supported by USAID IPs
33,324 4,830 0 9,498 0 0 33,324 14,328 0 -
Contract # of mechanisms created to facilitate coordination on an ongoing basis as a
result of USG Assistance (e.g. forum, working group, MOU, shared plans, associations, budgeting work planning, projects) Note that it is important to
identify best practices as they emerge. (counties using SCALE)
3 0 0 1 0 1 0 2 0 -
PMP # of mechanisms created to facilitate coordination on an ongoing basis as a result of USG Assistance (e.g. forum, working group, MOU, shared plans,
associations, budgeting work planning, projects) Note that it is important to identify best practices as they emerge (Linkages with FtF partners)
2 0 0 0 0 1 1 1 1 50.0%
Kitui -
T. Nithi -
Samburu 1 1 1 1 100%
Marsabit -
Busia -
PPR Number of children < 5 years reached by USG supported nutrition
programs
90,484 22,621 3,770 22,621 12,409 22,621 76,752 67,863 92,931 >100%
PPR Prevalence of wasted children under five years of age TBD 0 0 0 0 0 0 0 0 -
PPR Prevalence of underweight women TBD 0 0 0 0 0 0 0 0 - Kitui 0 0 -
T. Nithi 0 0 -
Samburu 0 0 0 -
Marsabit 0 0 -
Busia 0 0 -
PPR Prevalence of children 6-23 months receiving a minimum acceptable diet
(RiA)
TBD 0 0 0 0 0 0 0 0 - Kitui 0 0 -
T. Nithi 0 0 -
Samburu 0 0 0 -
Marsabit 0 0 -
Busia 0 0 -
PPR Prevalence of households with moderate or severe hunger (RiA) TBD 0 0 0 0 0 0 0 0 -
PPR Prevalence of exclusive breastfeeding of children under six months of age TBD 0 0 0 0 0 0 0 0 -
PPR Number of people implementing risk-reducing practices/actions to improve resilience to climate change as a result of USG assistance (S)
14,001 0 0 4,667 0 4,667 0 9,334 0 -
PMP # of people trained. Mentored, provided TA at National/County Level. 2 0 0 1 0 0 0 1 0 -

27
USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
PMP # of tools/templates/models provided by target institutions in order to facilitate devolution at the local level as a result of USG assistance
4,500 0 0 1,500 0 1,500 0 3,000 0 -
Contract Number of additional food manufacturers in the private sector meeting quality standards
1 0 0 1 0 1 1 2 1 50.0%
Contract % of nutrition commodity distribution (procured by NHPplus) managed by KEMSA
>90% 0 0 0 0 0 >90% 0 - -
Contract # of mechanisms created to facilitate coordination on an ongoing basis as a
result of USG Assistance (e.g. forum, working group, MOU, shared plans, associations, budgeting work planning, projects) Note that it is important to identify best practices as they emerge (joint work plans addressing:
promoting nutrition at HH level, increasing HH income for vulnerable
farmers, and strengthening linkages between vulnerable farmers and market actors/private sector)
2 0 0 0 0 0 2 0 2 -
Contract % of FTF partners trained and provided TA on inclusion of poor farmers in value chain tool
TBD 0 0 0 0 0 0 0 0 -
Contract # of FtF partners provided technical assistance to adopt existing agri-nutrition tools to include HH production and consumption of nutritious foods
TBD 0 0 0 0 0 0 0 0 -
PMP = NHPplus Performance Monitoring Plan; PPR = USAID Program Performance Reporting: Contract = NHPplus Contractual Paid up indicator

28
USAID/KENYA NUTRITION AND HEALTH PROGRAM PLUS PROGRESS REPORT FOR Q3 FY 2016
Annex II: Schedule of Future Events
This is a chronological list of significant events planned in the coming quarter that will contribute to
accomplishment of the activity’s indicators, such as trainings, opening ceremonies, conferences, etc.
This is not a place to list administration tasks, e.g., hiring of staff.
DATE LOCATION ACTIVITY
August Nairobi
Meeting to establish multi-stakeholder core working group
for PROFILES Kenya coordinated by Ministry of Devolution
and Planning – Food and Nutrition Planning Unit
August Nairobi - KSG Facilitate tuition fees for Busia CNC and NDU officer to
attend senior management course
September Nairobi PROFILES core group meeting
August Nairobi National World Breast Feeding week exhibition
August Nairobi Agri Nutrition TWG meeting
Aug Nairobi Finalization of MIYCN counselling card (MIYCN TWG)
August Nairobi NACS ToT for Nairobi county / Afya Jijini
Sept Nairobi NACS Nairobi Sub county training
Jul – Sept Coast, Transmara, Nakuru NACS Orientation coast region, Transmara, APHIA Rift
Jul – Aug Nairobi Development of Agri Nutrition Training Manual
Jul – Sept Nairobi Nutrition symposium/ conference planning meetings and
venue lockdown
July, August Busia, Tharaka Nithi, Kitui,
Marsabit
Training of ToTs on Multi-Sectoral Agri-Nutrition
Strategies
July-August-September Busia, Tharaka Nithi, Kitui,
Marsabit SMART Survey
25th to 29th July 2016 Nakuru Quantification for Nutrition Commodities workshop
29th July 2016 Busia - County Offices Busia County Nutrition Technical Forum (Tea and Lunch)
August Nairobi/Counties Workshop to finalize agri-nutrition modules
8th to 11th August Mwingi/Kitui NACS training
15th – 16th August 2016 Busia NACS Training (Conference and accommodation)
15th to 18th August Kitui Development of Recipe manual (small conference)
17th – 19th August 2016 Busia MIYCN Training (Conference and Accommodation)
18th to 22ndAugust Kitui IMAM training
25th to 27th August Kitui IFAS training
29th August – 1st
September Busia
Contextualization of recipe manual (Conference and
Accommodation)
September Nairobi Training of partners on nutrition sensitive interventions
19th to 23rd Sep Kitui MIYCN training.
5th – 7th September 2016 Busia IFAS TOT Training (Conference and Accommodation)