Urinary tract stones, treatment possibilities Matyas Benyo MD FEBU Based on the guideline of the...
46
Urinary tract stones, Urinary tract stones, treatment treatment possibilities possibilities Matyas Benyo MD FEBU Based on the guideline of the European Association of Urology
-
Upload
timothy-taylor -
Category
Documents
-
view
214 -
download
0
Transcript of Urinary tract stones, treatment possibilities Matyas Benyo MD FEBU Based on the guideline of the...

Urinary tract stones, Urinary tract stones, treatment possibilities treatment possibilities
Matyas Benyo MD FEBU
Based on the guideline of the European Association of Urology

EpidemiologyEpidemiologyBetween 120 and 140 per
1000,000 will develop urinary stones each year with a male/female ratio of 3:1.

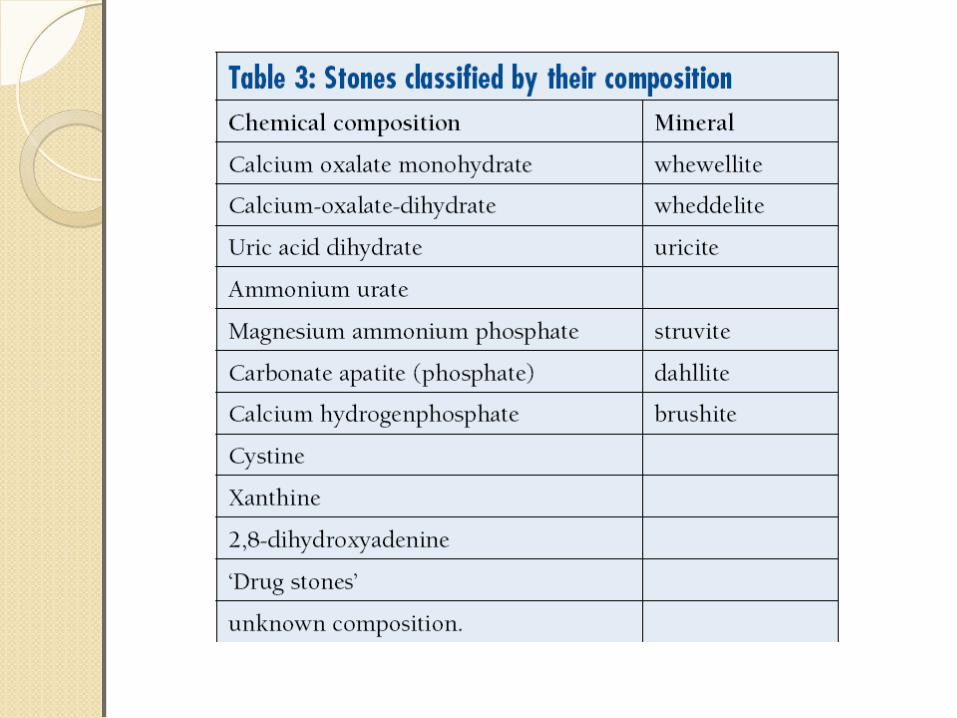
Classification of stonesClassification of stonesCorrect classification of stones is
important since it will impact treatment decisions and outcome.
Urinary stones can be classified according to the following aspects (tables 1-3): ◦stone size, ◦stone location, ◦X-ray characteristics of stone, ◦aetiology of stone formation, ◦stone composition (mineralogy), and ◦risk group for recurrent stone formation



High risk stone formersHigh risk stone formersGeneral factors
◦Early onset of urolithiasis in life (especially children and teenagers)
◦Familial stone formation◦Brushite containing stones (calcium
hydrogen phosphate; CaHPO4.2H2O)◦Uric acid and urate containing stones◦Infection stones◦Solitary kidney

High risk stone formersHigh risk stone formersDiseases associated with stone
formation◦Hyperparathyroidism◦Nephrocalcinosis◦Gastrointestinal diseases or
disorders◦Sarcoidosis
High risk stone formersHigh risk stone formersGenetically determined stone
formation◦Cystinuria (type A, B, AB)◦Primary hyperoxaluria (PH)◦Renal tubular acidosis (RTA) type I◦2,8-dihydroxyadenine◦Xanthinuria◦Lesh-Nyhan-Syndrome◦Cystic fibrosis

High risk stone formersHigh risk stone formersAnatomical abnormalities
associated with stone formation◦Medullary sponge kidney (tubular
ectasia)◦UPJ obstruction◦Calyceal diverticulum, calyceal cyst◦Ureteral stricture◦Vesico-uretero-renal reflux◦Horseshoe kidney◦Ureterocele◦Urinary diversion (via enteric
hyperoxaluria)◦Neurogenic bladder dysfunction
Diagnostic imagingDiagnostic imagingStandard evaluation of a patient includes
taking a detailed medical history and physical examination.
The clinical diagnosis should be supported by an appropriate imaging procedure.
Ultrasonography should be used as the primary procedure.
KUB should not be performed in case an NCCT is considered.
Non-contrast enhanced computed tomography (NCCT) has become the standard for diagnosis of acute flank pain and has higher sensitivity and specificity than IVU.


Basic analysisBasic analysisEmergency stone patientEmergency stone patientUrine
◦Urinary sediment/dipstick test out of spot urine sample for: red cells / white cells / nitrite / urine pH
◦Urine culture or microscopy Blood
◦Serum blood sample creatinine / uric acid / ionized calcium / sodium / potassium
◦Blood cell count◦CRP
If intervention is likely or planned:◦Coagulation test (PTT and INR)

Stone analysisStone analysisAnalysis of stone composition should be
performed in:◦All first-time stone formers ◦Recurrence under pharmacological
prevention◦Early recurrence after interventional
therapy with complete stone clearance◦Late recurrence after a prolonged stone-free
periodThe preferred analytical procedures
are:◦X-ray diffraction◦ Infrared spectroscopy

High-risk patients: High-risk patients: Stone-specific metabolic work-up Stone-specific metabolic work-up andand pharmacological recurrence pharmacological recurrence ppreventionreventionPharmacological stone
prevention is based on a reliable stone analysis and the laboratory analysis of blood and urine including two consecutive 24-hours urine samples.

Acute treatment of a patient Acute treatment of a patient with renal colicwith renal colicPain relief is the first therapeutic
step in patients with an acute stone episode.
If pain relief cannot be achieved by medical means, drainage, using stenting or percutaneous nephrostomy, or stone removal, should be carried out.

Management of sepsis in the Management of sepsis in the obstructed kidneyobstructed kidneyThe obstructed, infected kidney is a
urological emergency.The collecting system should be urgently
decompressed (percutaneous drainage or ureteral stenting).
Definitive treatment of the stone should be delayed until sepsis is resolved.
Collect urine following decompression for antibiogram.
Start antibiotic treatment immediatedly thereafter (+ intensive care if necessary).
Revisit antibiotic treatment regimen following antibiogram findings.

TreatmentTreatmentKidney stones should be treated in
case of stone growth, formation of de novo obstruction, associated infection, and acute and/or chronic pain.
Patient’s comorbidities and preferences (social situation) need to be taken into consideration when making a treatment decision.
If kidney stones are not treated, periodic evaluation is needed.

Medical expulsive therapy Medical expulsive therapy (MET)(MET)For patients with ureteral stones that are
expected to pass spontaneously, NSAID tablets or suppositories (i.e. diclofenac sodium, 100-150 mg/day, over 3-10 days) may help to reduce inflammation and the risk of recurrent pain.
Alpha-blocking agents, given on a daily basis, also reduce the number of recurrent colic.
Patients, who elect for an attempt at spontaneous passage or MET, should have wellcontrolled pain, no clinical evidence of sepsis, and adequate renal functional reserve.

Chemolytic dissolution of Chemolytic dissolution of stonesstonesOral or percutaneous irrigation
chemolysis of stones can be a useful first-line therapy or an adjunct to ESWL, PNL, URS, or open surgery to support elimination of residual fragments.
However, its use as first-line therapy may take weeks to be effective.
Oral chemolitholysis is efficient for uric acid calculi only.
The urine pH should be adjusted to between 7.0 and 7.2.

ESWL ESWL (extracorporeal shock wave (extracorporeal shock wave lithotripsy)lithotripsy)The success rate for ESWL will
depend on the efficacy of the lithotripter and on:◦Size, location of stone mass
(ureteral, pelvic or caliceal), and composition (hardness) of the stones
◦Patient’s habitus◦Performance of ESWL

Shock waves- a special form of sound waves that have a sharp peak in positive pressure followed by a trailing negative wave
The change in density and acoustic impedance when traveling from water to stone results in fragmentation
•The positive pressure and the short rise time are responsible for the direct shock wave effect •the tensile wave for the cavitation, which is called the indirect shock wave effect. •The disintegration of a kidney stone is a combination between direct and indirect shock wave

February 1980 in Germany by Dornier1983 First commercial lithotripter HM3 (Dornier)
HistoryHistory

•Shock wave generator•Electrohydraulic,•Electromagnetic•Piezoelectric
•Localisation system during the operation•Fluoroscopic x-ray•Ultrasound
•Shock wave coupling •(water bath)•Ultrasonography gel
•Auxiliary equipment (table) (control of pain)

Figure 1: The Electrohydraulic Electrode Generating Acoustic Pressure on the Focal Point
The urinary stone is positioned on the focal point and disintegrates aftermultiple shots.

Figure 2: Cylindric Electromagnetic Shock Wave Source Within the Parabolic Reflector

Figure 3: Piezoelectric Shock Wave Source with Multiple Piezoelements

Example of a High-End Urologic Workstation
The highly effective shock wave source is integrated in a multipurpose table with afluoroscopic and ultrasound imaging system.

Pressure Distribution and Configuration of Focal Point Depending onShock Wave Source

EEfficacy of the lithotripterfficacy of the lithotripter
size, location (ureteral, pelvic or calyceal)
composition (hardness) of the stones
best result: 4 mm and 2 cm in diameter that are still located in the kidney
ureters - a lower rate of successpatient’s habitus (non-obese)

Contraindications of extracorporeal shock wave lithotripsypregnancy, due to the potential effects on the foetusbleeding diatheses, which should be compensated for at least 24 h before and 48 h after treatmentuncontrolled urinary tract infectionssevere skeletal malformations and severe obesity, which prevent targeting of the stone;arterial aneurysm in the vicinity of the stoneanatomical obstruction distal to the stone.

Routine use of internal stents before SWL does not improve stone-free rate - JJ stent reduces the risk of renal colic and obstruction
Lowering shock wave frequency from 120 to 60-90 shock waves/min improves stone-free rate
Tissue damage increases with shock wave frequencyThe optimal shock wave frequency is 1.0-1.5 HzThe number of shock waves that can be delivered at
each session depends on the type of lithotripterShock wave power. There is no consensus on the
maximum number of shock waves.Maximum threshold of 3000 shocks for renal stones70SW/min (better) than 100SW/min
Optimizing ESWL
Starting SWL on a lower energy setting with stepwise power ramping can achieve vasoconstriction during treatment which prevents renal injury.
Repeate SWL sessions within 1 day for ureteral stones

Percutaneous Percutaneous nephrolitholapaxy (PNL)nephrolitholapaxy (PNL)Ultrasonic, ballistic and Ho:YAG
devices are recommended for intracorporeal lithotripsy using rigid nephroscopes.
When using flexible instruments, the Ho:YAG laser is currently the most effective device available.


ContraindicationsContraindicationsAll contraindications for general
anaesthesia apply.Untreated urinary infection.Atypical bowel interposition.Tumour in the presumptive access tract
area.Potential malignant tumour of the
kidney.Pregnancy (conservative stone
treatment should be considered first, where possible.

Open SurgeryOpen SurgeryMost complex (staghorn) stones,
should be approached primarily with PNL or a combination of PNL and ESWL. Open surgery may be a valid primary treatment option in selected cases.
Laparoscopic urological surgery has increasingly replaced open surgery.

Indications for open (/lap) Indications for open (/lap) surgerysurgery Complex stone burden Treatment failure of ESWL and/or PNL, or failed
ureteroscopic procedure Intrarenal anatomical abnormalities: infundibular
stenosis, stone in the calyceal diverticulum, obstruction of the ureteropelvic junction, stricture
Morbid obesity Skeletal deformity, contractures and fixed
deformities of hips and legs Co-morbid medical disease Concomitant open surgery Non-functioning lower pole (partial nephrectomy),
nonfunctioning kidney (nephrectomy) Stone in an ectopic kidney where percutaneous
access and ESWL may be difficult or impossible

Indication for active stone Indication for active stone removalremovalUreter:
◦Stones with a low likelihood of spontaneous passage
◦Persistent pain in spite of adequate pain medication
◦Persistent obstruction◦Renal insufficiency (renal failure,
bilateral obstruction, single kidney)
Indication for active stone Indication for active stone removalremovalKidney:
◦Stone growth◦Stones in high-risk patients for stone
formation◦Obstruction caused by stones◦ Infection◦Symptomatic stones (e.g. pain, haematuria)◦Stones > 15 mm◦Stones < 15 mm if observation is not the
option of choice◦Patient preference (medical and social
situation)◦> 2-3 years persistent stones



Ureter stones - treatmentUreter stones - treatment

General considerations forGeneral considerations for recurrence preventionrecurrence prevention(all stone patients)(all stone patients)
Drinking advice (2.5 – 3L/day, neutral pH)
Balanced dietLifestyle advice

Thank you for your Thank you for your attention!attention!