Urinary System Introduction The urinary system Filters the body of waste materials,Homeostaticaly...
112
Urinary System Introduction • The urinary system Filters the body of waste materials ,Homeostaticaly regulates bodys fluid status,electrolyte balance and acid base balance. Endocrine and Synthetic functions • EPO – Controls RBC production from stem cells in marrow – Stimulated by reduced PO 2 in kidney (not systemic PO 2 ) • Vitamin D – Active form (calcitrol) produced by a hydroxlation in kidney & liver – Important for calcium absortion from GI and also neuronal development in-utero • Renin – An enzyme. Synthesized in juxtaglomerular (granular) cells in afferent arteriole – Stimulated by a fall in circulating volume
-
Upload
arleen-georgiana-small -
Category
Documents
-
view
215 -
download
1
Transcript of Urinary System Introduction The urinary system Filters the body of waste materials,Homeostaticaly...

Urinary System Introduction • The urinary system Filters the body of waste materials ,Homeostaticaly regulates bodys fluid status,electrolyte balance and acid base balance.
Endocrine and Synthetic functions• EPO
– Controls RBC production from stem cells in marrow – Stimulated by reduced PO2 in kidney (not systemic PO2)
• Vitamin D – Active form (calcitrol) produced by a hydroxlation in kidney & liver – Important for calcium absortion from GI and also neuronal
development in-utero • Renin
– An enzyme. Synthesized in juxtaglomerular (granular) cells in afferent arteriole
– Stimulated by a fall in circulating volume – Leads to the production of Ang II and Aldosterone
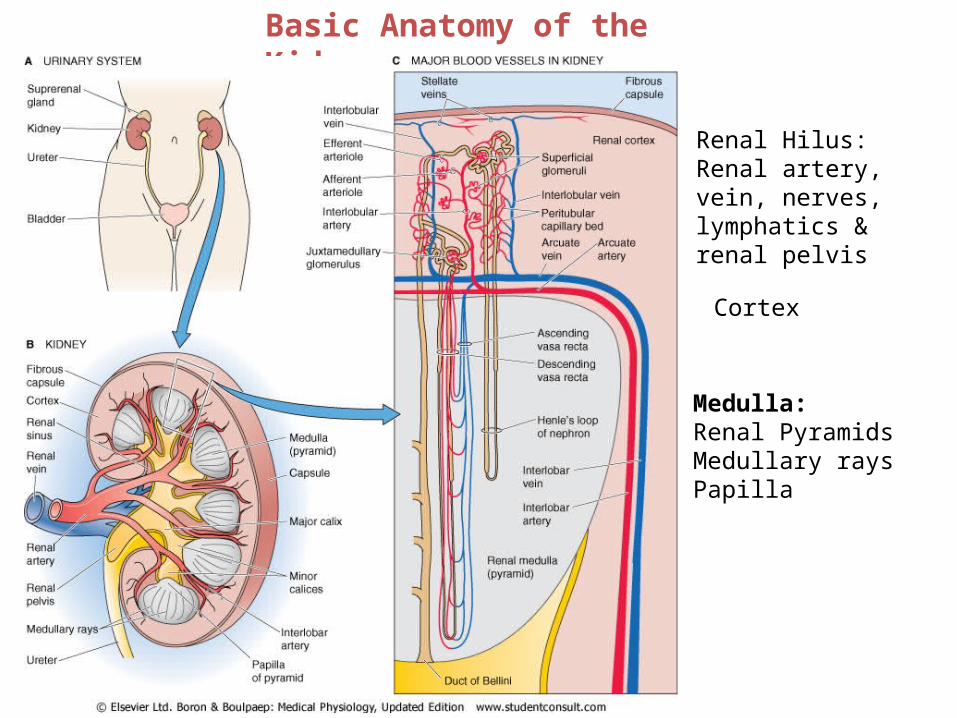
Basic Anatomy of the Kidney
Renal Hilus: Renal artery, vein, nerves, lymphatics & renal pelvis
Cortex
Medulla: Renal Pyramids Medullary rays Papilla

Internal Structure of the Kidney 85%
15%

Nephron Structure: Associated Blood Vessels
Renal → segmental → interlobar → arcuate → cortical radial (interlobular) → afferent → glomerulus → efferent
The Kidney Has The Highest Blood Flow Per Unit Mass Among Major Organs.
1250 ml/min = 25% of cardiac output
Two arterioles and two capillary beds in series
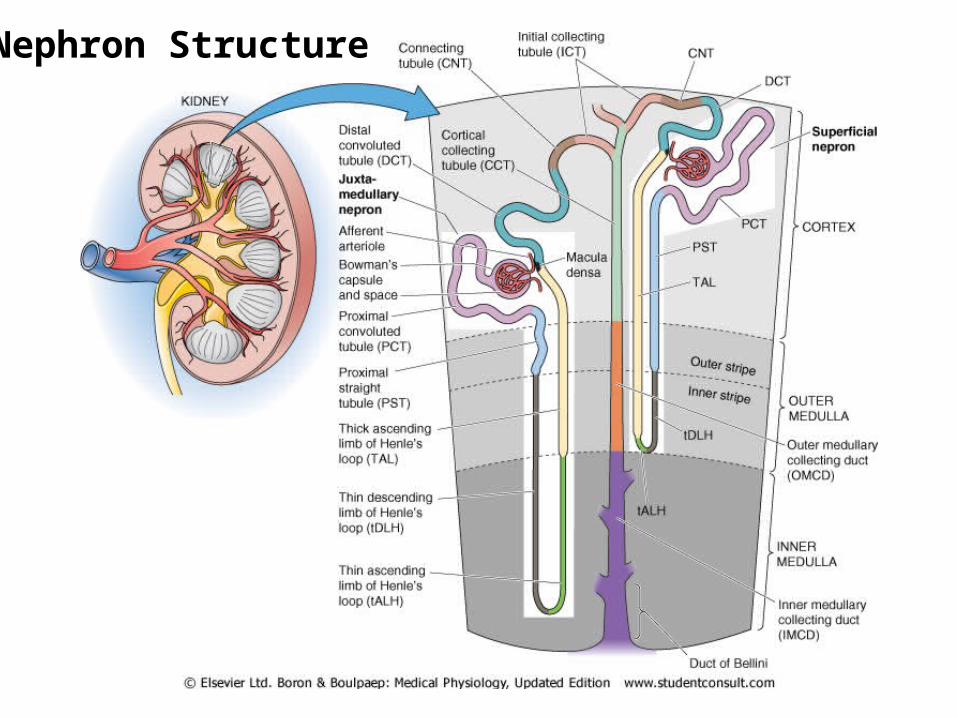
Nephron Structure

Cellular Features of the Renal Corpuscle

filtration membrane.

The Filtration Membrane and Glomerular Filtration
• Passage through the filtration membrane is limited not only on the basis of size but also by charge. • Glomerular filtration is a process of bulk flow driven by the hydrostatic pressure of the blood. • Small molecules pass rapidly through the filtration membrane, while large proteins and blood cells are kept out of the capsular space.
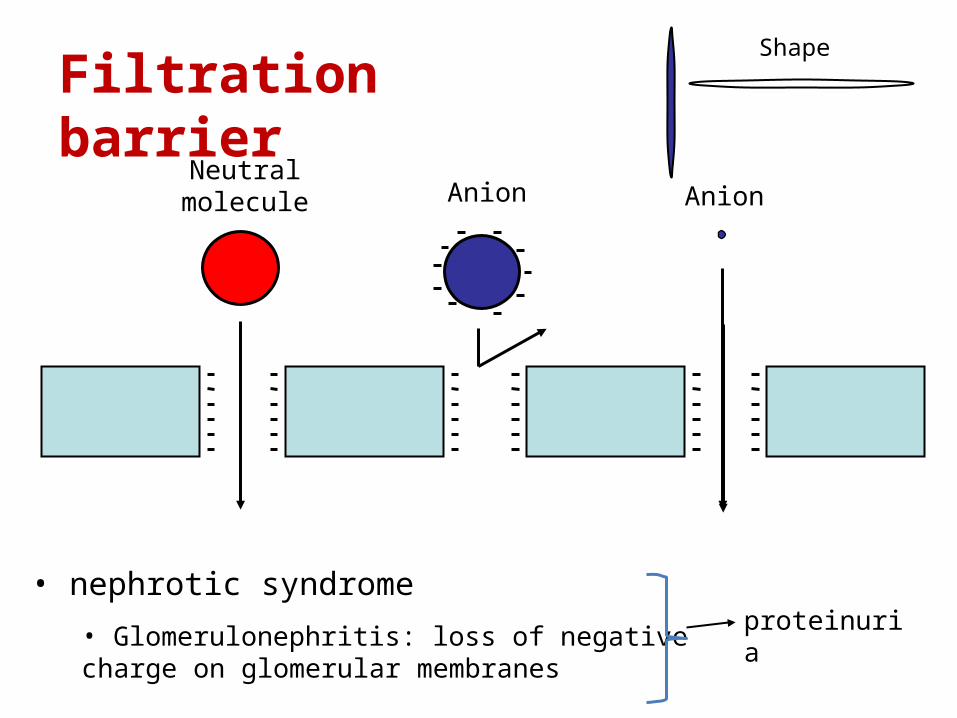
Filtration barrier
Neutral molecule Anion Anion
• Glomerulonephritis: loss of negative charge on glomerular membranes
proteinuria
Shape
• nephrotic syndrome

The Juxtaglomerular Apparatus
baroreceptors

Cells of the Proximal Convoluted Tubule (PCT)

Cells of the Thin Loop of Henle
• The key feature of these cells is that they are highly permeable to water but not to solutes.
Cells of the Thick Ascending Loop of Henle and DCT
• The key feature of the cells of the ascending limb is that they are highly permeable to solutes, particularly sodium chloride, but not to water. The cells of the DCT are more permeable to water than those of the ascending limb.

Cells of the Cortical Collecting Duct:-
1. Principal Cells
2. Intercalated Cells
• The key feature of principal cells is that their permeability to water and solutes is physiologically regulated by hormones.
• The key feature of intercalated cells is their secretion of hydrogen ions for acid/base balancing.

MicturitionOnce urine enters the renal pelvis, it flows through the ureters and
enters the bladder, where urine is stored.
Micturition is the process of emptying the urinary bladder.
Two processes are involved:
(1) The bladder fills progressively until the tension in its wall is raised above a threshold level, and then
(2) A nervous reflex called the micturition reflex occurs that empties the bladder.
The micturition reflex is an automatic spinal cord reflex; however, it can be inhibited or facilitated by centers in the brainstem and cerebral cortex.

stretchreceptors
Urine Micturition

Filling of the Bladder and Bladder Wall Tone - the Cystometrogram

•1) APs generated by stretch receptors•2) reflex arc generates APs that•3) stimulate smooth muscle lining bladder•4) relax internal urethral sphincter (IUS)•5) stretch receptors also send APs to Pons•6) if it is o.k. to urinate–APs from Pons excite smooth muscle of bladder and relax
IUS–relax external urethral sphincter
•7) if not o.k.–APs from Pons keep
EUS contracted
stretchreceptors

Automatic Bladder • Caused by Spinal Cord Damage Above the Sacral Region • micturition reflexes can still occur. However, they are no longer
controlled by the brain.
overflow incontinence.• Atonic Bladder and Incontinence Caused by Destruction of Sensory Nerve Fibers • the bladder fills to capacity and overflows a few drops at a time through the urethra.• common cause of atonic bladder is crush injury to the sacral region of the spinal cord.
Uninhibited Neurogenic Bladder Caused by Lack of Inhibitory Signals from the Brain

Three basic renal processes
Introduction • Formation of urine by the kidney involves three main processes:
1. Glomerular filtration(180ltrs/day,20% of plasma filtered) 2. Tubular reabsorption(178.5ltrs) 3. Tubular secretion (80% of plasma is involved in exchange with the renal tubules)

Glomerular Filtration Rate (GFR) • The total amount of filtrate formed by all the renal corpuscles in both kidneys per minute is called the glomerular filtration rate, or GFR. • In normal kidneys, the 17 millimeters of mercury of net filtration pressure produces approximately 125 milliliters of filtrate per minute. This translates to about 180 liters in 24 hours. Fortunately, 99% of this volume will be reabsorbed as the filtrate passes through the tubules.
• The glomerular filtration rate is directly proportional to the net filtration pressure, so a fluctuation in any of the three pressures previously discussed will change the GFR.• Prolonged changes in normal GFR will cause either too much or too little water and solutes to be removed from the blood.

Glomerular Filtrate • The fluid and solutes collecting in the capsular space is called glomerular filtrate. • The concentration of each of these substances in the glomerular filtrate is similar to its concentration in plasma.
Damage to Filtration Membrane • How might the contents of the filtrate be altered if the filtration membrane is damaged or destroyed?

Forces Affecting Filtration • There are three forces affecting filtration at the glomerulus:
1. Hydrostatic Pressure within the Glomerular Capillaries
2. Back Pressure from Fluid Within the Capsule
3. Osmotic Pressure within the Glomerular Capillaries
Net Filtration Pressure = 60 mm Hg - (15 mm Hg + 28 mm Hg) = 17 mm Hg
“kidney shut-down” or acute renal failure.

Glomerular Filtration Rate (GFR) • The total amount of filtrate formed by all the renal corpuscles in both kidneys per minute is called the glomerular filtration rate, or GFR. • In normal kidneys, the 17 millimeters of mercury of net filtration pressure produces approximately 125 milliliters of filtrate per minute. This translates to about 180 liters in 24 hours !!!• Fortunately, 99% of this volume will be reabsorbed as the filtrate passes through the tubules.
• The glomerular filtration rate is directly proportional to the net filtration pressure, so a fluctuation in any of the three pressures previously discussed will change the GFR.• Prolonged changes in normal GFR will cause either too much or too little water and solutes to be removed from the blood.

Autoregulation of GFR
During normal conditions, systemic blood pressure registers approximately 120 millimeters of mercury; the diameter of the afferent arteriole is normal, as is the glomerular hydrostatic pressure. These conditions provide a normal glomerular filtration rate of 125 milliliters per minute.
During mild exercise
During periods of relaxation
increase in GFR [of 21 milliliters per minute, to 146 milliliters per minute
reduction of glomerular hydrostatic pressure and GFR

Autoregulation of GFR
During normal conditions, systemic blood pressure registers approximately 120 millimeters of mercury; the diameter of the afferent arteriole is normal, as is the glomerular hydrostatic pressure. These conditions provide a normal glomerular filtration rate of 125 milliliters per minute.
During mild exercise
During periods of relaxation
increase in GFR [of 21 milliliters per minute, to 146 milliliters per minute
reduction of glomerular hydrostatic pressure and GFR
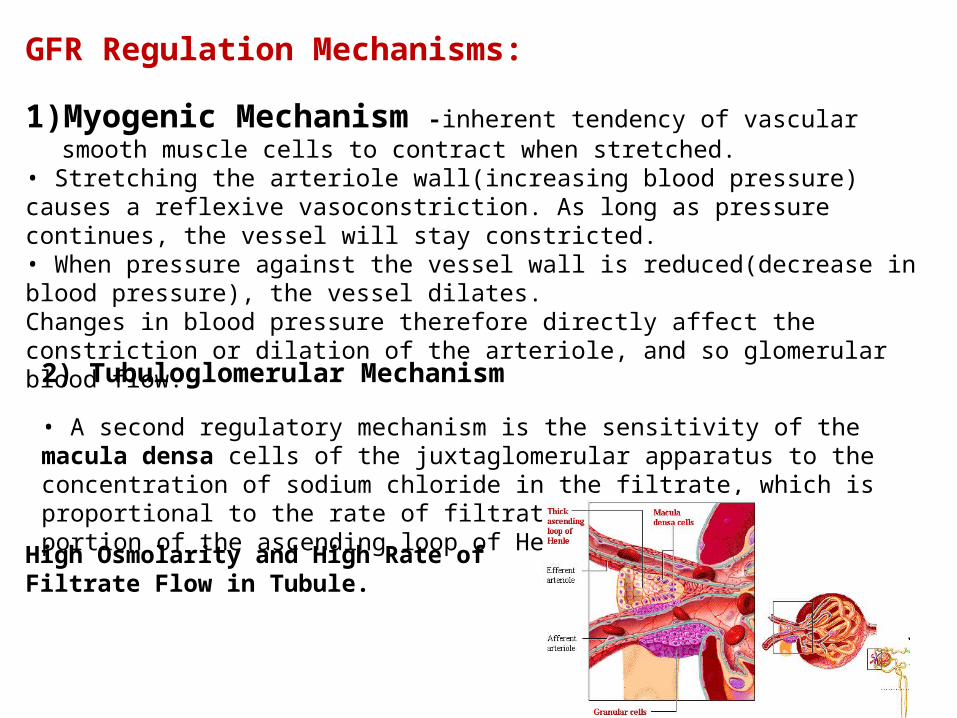
GFR Regulation Mechanisms:
1) Myogenic Mechanism -inherent tendency of vascular smooth muscle cells to contract when stretched.
• Stretching the arteriole wall(increasing blood pressure) causes a reflexive vasoconstriction. As long as pressure continues, the vessel will stay constricted. • When pressure against the vessel wall is reduced(decrease in blood pressure), the vessel dilates. Changes in blood pressure therefore directly affect the constriction or dilation of the arteriole, and so glomerular blood flow.
2) Tubuloglomerular Mechanism • A second regulatory mechanism is the sensitivity of the macula densa cells of the juxtaglomerular apparatus to the concentration of sodium chloride in the filtrate, which is proportional to the rate of filtrate flow in the terminal portion of the ascending loop of Henle.
High Osmolarity and High Rate of Filtrate Flow in Tubule.

Low Osmolarity and Low Rate of Filtrate Flow in Tubule
• A low rate of filtrate flow and, therefore, low sodium chloride in the terminal portion of the ascending loop of Henle is also sensed by the macula densa cells. This condition is usually the result of low GFR caused by low blood pressure. • In response, these cells initiate two effects: 1) They decrease secretion of the vasoconstrictor chemicals. This leads to dilation of the arteriole and so increases blood flow, glomerular hydrostatic pressure, and the GFR 2) The macula densa cells signal the granular cells of the afferent and efferent arterioles to release renin into the bloodstream.
What is the Effect of Renin on the Regulation of the GFR ?1- angiotensin II formed from renin causes constriction of the efferent arteriole 2- release of the hormone aldosterone

GFR Regulation Mechanisms: Sympathetic Nervous System Control
Sympathetic nerve fibers innervate all blood vessels of the kidney as an extrinsic regulation mechanism. During normal daily activity they have minimal influence. However, during periods of extreme stress or blood loss, sympathetic stimulation overrides the autoregulatory mechanisms of the kidney.
• Increased sympathetic discharge causes intense constriction of all renal blood vessels. Two important results occur: 1) The activity of the kidney is temporarily lessened or suspended in favor of shunting the blood to other vital organs 2) The lower GFR reduces fluid loss, thus maintaining a higher blood volume and blood pressure for other vital functions.
• Reduction in filtration cannot go on indefinitely, as waste products and metabolic imbalances increase in the blood. Autoregulation mechanisms are now ineffective in preventing acute renal failure. • When fluid is given intravenously, the blood volume increases. With increasing blood volume there will be gradual rise in blood pressure, reduction in sympathetic discharge, and restoration of renal functioning.

Three basic renal processes
Introduction • Formation of urine by the kidney involves three main processes:
1. Glomerular filtration(180ltrs/day,20% of plasma filtered) 2. Tubular reabsorption(178.5ltrs) 3. Tubular secretion

Glomerular Filtration Rate (GFR) • The total amount of filtrate formed by all the renal corpuscles in both kidneys per minute is called the glomerular filtration rate, or GFR. • In normal kidneys, the 17 millimeters of mercury of net filtration pressure produces approximately 125 milliliters of filtrate per minute. This translates to about 180 liters in 24 hours !!!• Fortunately, 99% of this volume will be reabsorbed as the filtrate passes through the tubules.
Filtration Fraction (FF)using a value of GFR of 125 ml/min and ERPF = 700 ml/min,the fraction of plasma that is filtered is 125/700 = 18%. FF is typically in the range 15-25%. That is 15-25% of the plasma volume becomes filtrate in the nephrons of the kidney.

The Filtration Membrane and Glomerular Filtration
• Passage through the filtration membrane is limited not only on the basis of size but also by charge. • Glomerular filtration is a process of bulk flow driven by the hydrostatic pressure of the blood. • Small molecules pass rapidly through the filtration membrane, while large proteins and blood cells are kept out of the capsular space.

Filtration barrier
Neutral molecule Anion Anion
• Glomerulonephritis: loss of negative charge on glomerular membranes
proteinuria
Shape
• nephrotic syndrome

Glomerular filtration
Afferent arteriole Efferent arterioleGlomerular capillaries
Bowman’s space • no protein
• all other molecules and ions at ~same
concentration as plasma
Determinants of GFRThe rate of filtration in any of the body's capillaries, including the glomeruli, is determined by the hydraulic permeability of the capillaries, their surface area, and the net filtration pressure (NFP) acting across them.
Rate of filtration = hydraulic permeability x surface area x NFP
Because it is difficult to estimate the area of a capillary bed, a parameter called the filtration coefficient (Kf) is
used to denote the product of the hydraulic permeability and the area.

Net Filtration Pressure• There are three forces affecting net filtration at the glomerulus:
1. Hydrostatic Pressure within the Glomerular Capillaries
2. Back Pressure from Fluid Within the Capsule
3. Osmotic Pressure within the Glomerular Capillaries
Net Filtration Pressure = 60 mm Hg - (15 mm Hg + 28 mm Hg) = 17 mm Hg
“kidney shut-down” or acute renal failure.
NFP = (PGC – Л GC) – (PBC – Л BC) GFR = Kf (PGC – PBC – ЛGC).
Sum of filtration rates of all the nephrons = total glomerular filtration rate
= total GFR= GFR
If total number of functioning nephrons is reduced
(chronic renal failure)
GFR
Measurement of GFR is the best single means of assessing kidney function quantitatively

ml/min
Renal blood flow
50 100 150 200
Mean arterial pressure (mmHg)
1500
500
1000
GFR
50
100
150
Flow = Δ Pressure Resistance
Autoregulation
Normally, renal blood flow doesn’t change much
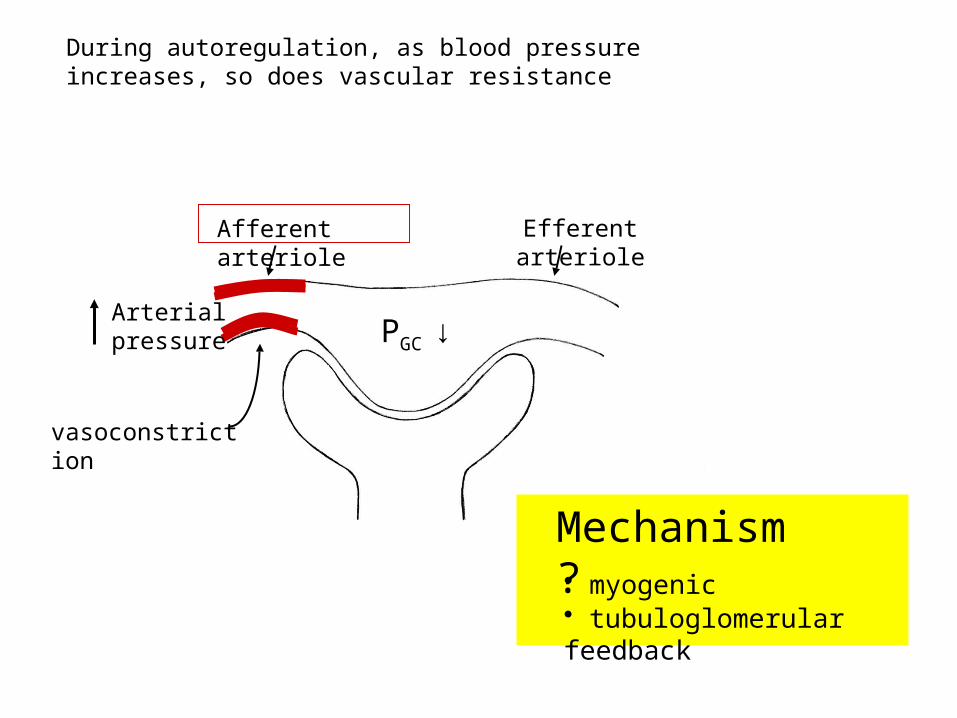
During autoregulation, as blood pressure increases, so does vascular resistance
Arterial pressure
vasoconstriction
Afferent arteriole Efferent arteriole
Mechanism?• myogenic• tubuloglomerular feedback
PGC ↓
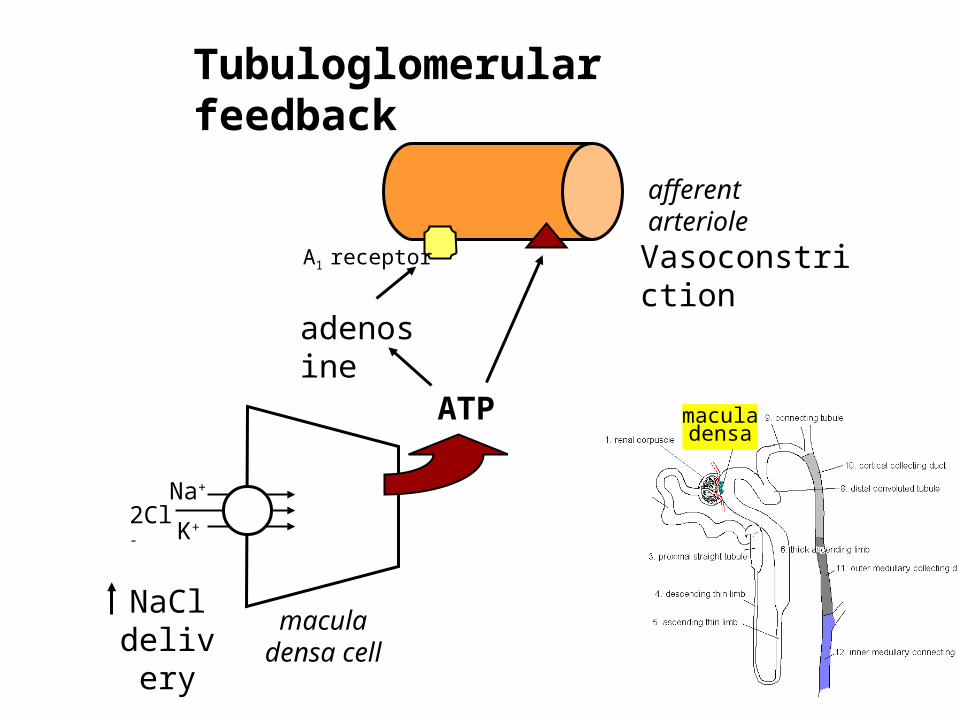
NaCl delivery
macula densa cell
Na+ 2Cl-
K+
afferent arteriole
Vasoconstriction
Tubuloglomerular feedback
ATP
adenosine
A1 receptor
macula densa

hemorrhage
MAP
Arterial baroreceptors activated
Renal nerves stimulated Renal
arteriolesconstrict
Renin-angiotensin system activated
RBF and GFRfall
Autoregulation does not mean that RPF and GFR never change.

A drug is noted to cause a decrease in GFR. Identify 4 possible actions of the drug that might decrease GFR.
A person is given a drug that dilates the afferent arteriole and constricts the efferent arteriole by the same amounts. Assuming no other actions of the drug, what happens to this person's GFR
A clamp around the renal artery is partially tightened to reduce renal arterial pressure from a mean of 120 to 90 mm Hg. do you predict RBF will change?
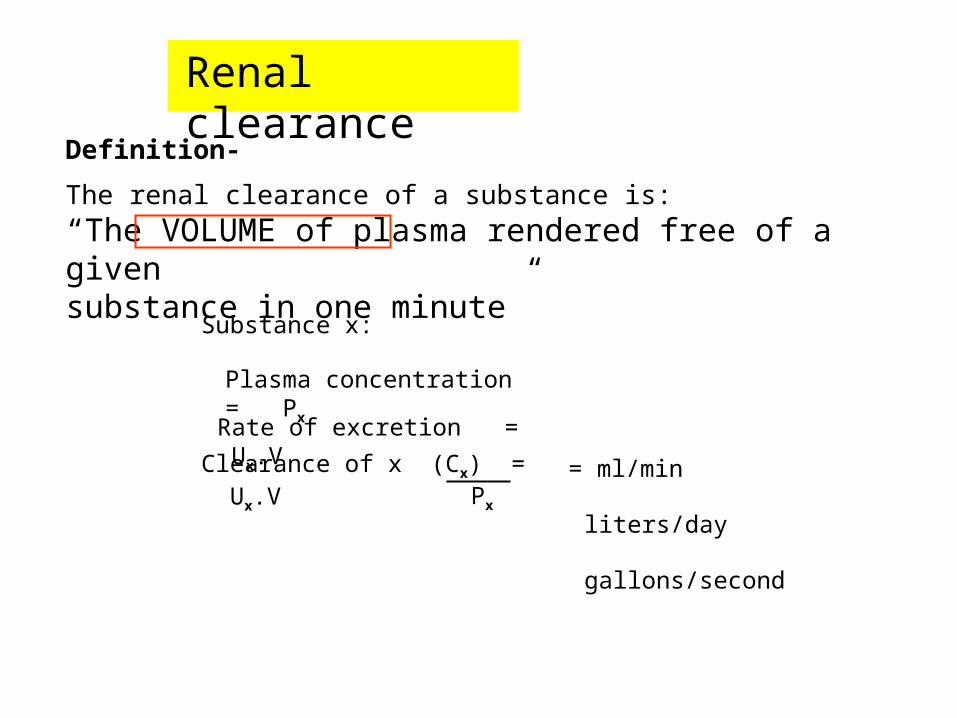
Renal clearance
Definition-
The renal clearance of a substance is:
“The VOLUME of plasma rendered free of a givensubstance in one minute”
Rate of excretion = Ux.V
Substance x:
Plasma concentration = Px
Clearance of x (Cx) = Ux.VPx
= ml/min
liters/day
gallons/second

Purea = 0.2 mg/ml
Uurea = 6 mg/ml
V = 2ml/min
Questions:
• How much urea is excreted per min?
• What is the clearance of urea?
Answers: • Urea excretion = 6 mg/ml x 2 ml/min = 12 mg/min
• Urea clearance = 12 mg/min = 60 ml/min
0.2 mg/ml
i.e. 60 ml of plasma loses its urea into the urine in one minute
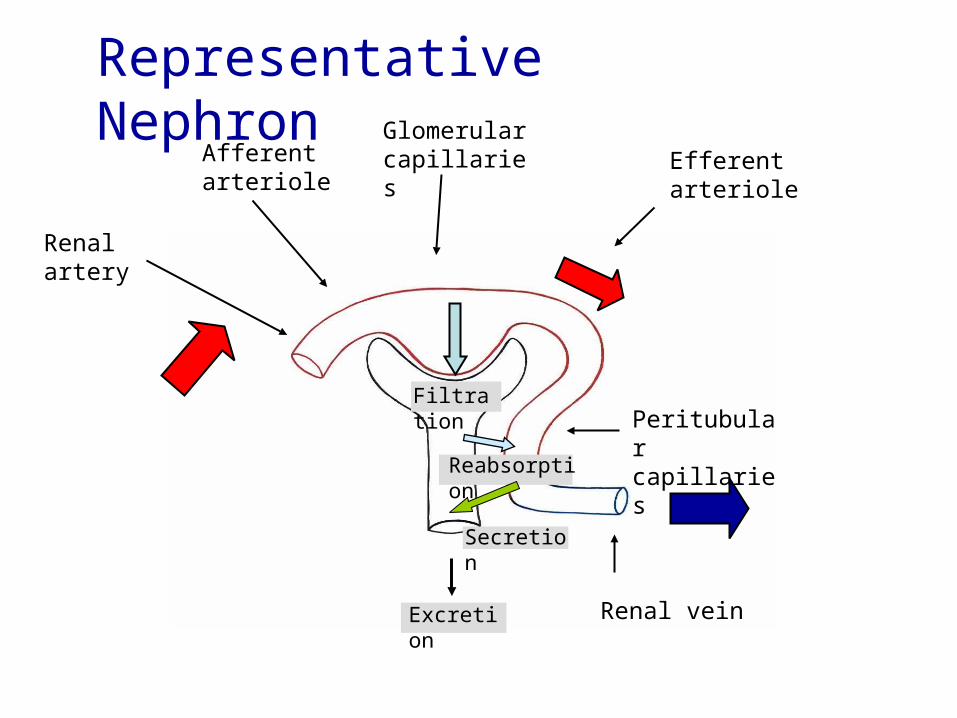
Renal artery
Glomerular capillaries Efferent
arteriole
Peritubular capillaries
Renal vein
Representative Nephron
Afferent arteriole
Excretion
Filtration
Reabsorption
Secretion
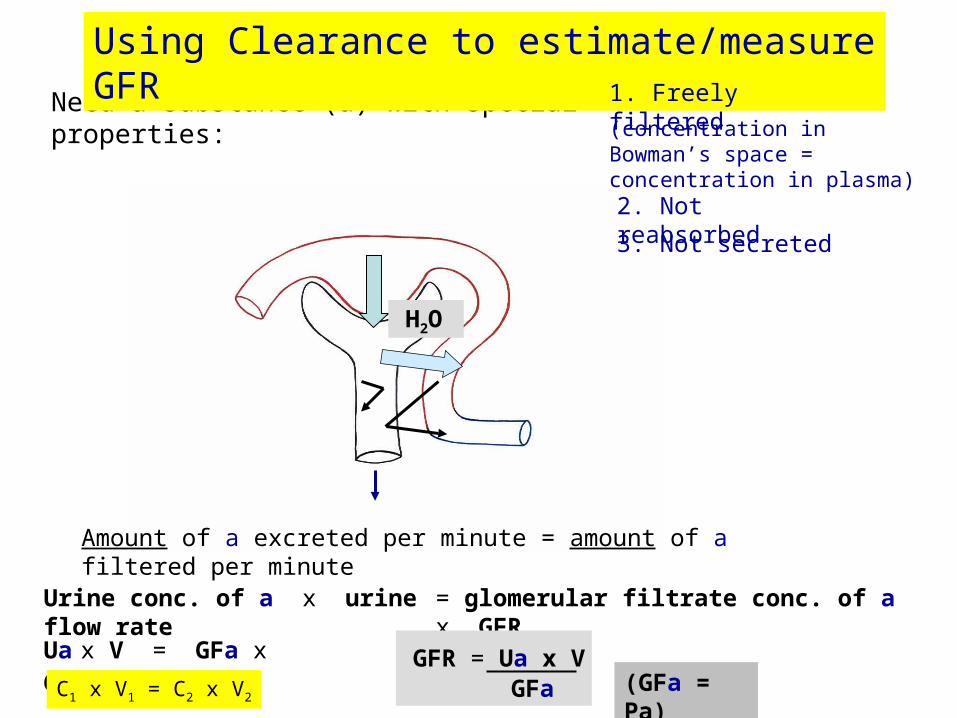
Need a substance (a) with special properties:
Using Clearance to estimate/measure GFR
(concentration in Bowman’s space = concentration in plasma)
1. Freely filtered
2. Not reabsorbed
Amount of a excreted per minute = amount of a filtered per minute
H2O
3. Not secreted
Urine conc. of a x urine flow rate = glomerular filtrate conc. of a x GFR
GFR = Ua x VGFa (GFa = Pa)
Ua x V = GFa x GFR
C1 x V1 = C2 x V2

Very few substances meet the criteria required to measure GFR
Best known: Inulin• polysaccharide of fructose
• molecular weight ~5000 daltons
• molecular diameter ~3 nm
Typical value for GFR ~120 ml/min ~180 liters/day!
• Inulin clearance = GFR
Inulin is cleared from plasma by filtration alone.
Since none of filtered inulin returns to the plasma, volume of plasma cleared of inulin per min must equal the volume of plasma filtered per min (= GFR)

Problems with measuring Cin clinically:
• Must be infused intravenously
• Continual blood sampling required
• Chemical analysis cumbersome
Useful alternative:
Creatinine (not creatine)• Endogenous (by-product of muscle metabolism)
• Released into blood at relatively constant rate (plasma concentration fairly stable; therefore only need one blood sample)
• Freely filtered • Not reabsorbed • Not secreted ( true Ccr normally overestimates GFR by ~10-20%)
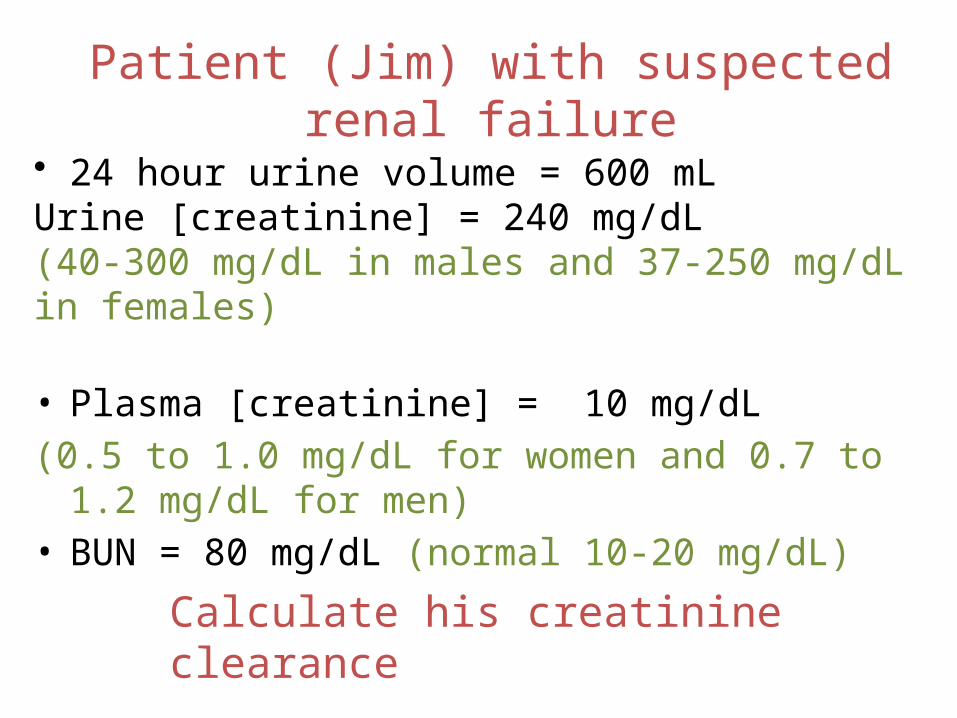
Patient (Jim) with suspected renal failure
• 24 hour urine volume = 600 mL Urine [creatinine] = 240 mg/dL(40-300 mg/dL in males and 37-250 mg/dL in females)
• Plasma [creatinine] = 10 mg/dL
(0.5 to 1.0 mg/dL for women and 0.7 to 1.2 mg/dL for men)
• BUN = 80 mg/dL (normal 10-20 mg/dL)
Calculate his creatinine clearance
BUN:creatinine ratio ?

Jim’s creatinine clearance (Ccr):
Ccr = Ucr x V / Pcr
Ccr = 10ml/min = GFR for Jim.
(normal = 90-140 mL/min)
Ccr = 240 mg/dL x 600 mL/day (0.42 ml/min)10 mg/dL
Low GFR means renal insufficiency

GFR can be estimated from Pcr
Jim
GFR is lower in young children and declines in old age.
The Gault-Cockroft formula is usedclinically to estimate GFR in the steadystate from a measurement of plasmacreatinine:
%GFR(ml /min) = [(140 - age)XWeight(kg)] (Pcr(mg / dL)x72)

Renal clearance of selected substances provides special information
• Clearance of inulin = GFR
• Clearance of creatinine = ~ GFR
• Clearance of para-amino hippurate =
renal plasma flow
Para-amino hippurate (PAH)• organic anion
• freely filtered
• avidly secreted by peritubular capillaries into proximal tubule
• at low plasma concentrations, the combination of filtration and secretion means that all PAH arriving in the renal plasma is excreted in the urine
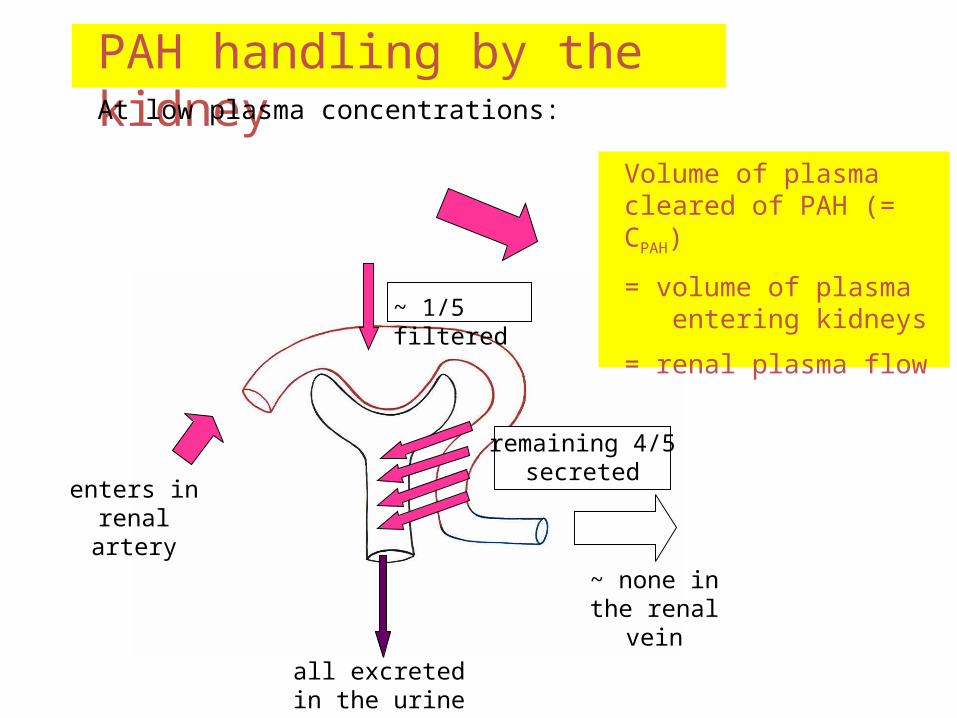
PAH handling by the kidneyAt low plasma concentrations:
enters in renal artery
~ 1/5 filtered
remaining 4/5 secreted
all excreted in the urine
~ none in the renal vein
Volume of plasma cleared of PAH (= CPAH)
= volume of plasma entering kidneys
= renal plasma flow
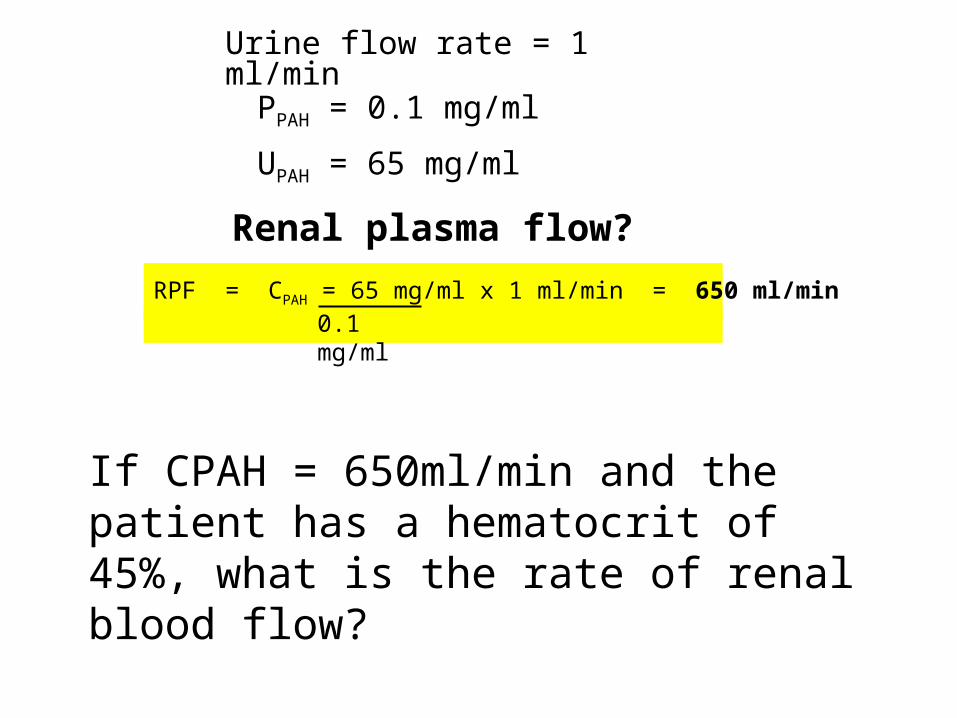
Urine flow rate = 1 ml/min
UPAH = 65 mg/ml
PPAH = 0.1 mg/ml
Renal plasma flow?
RPF = CPAH = 65 mg/ml x 1 ml/min = 650 ml/min0.1 mg/ml
If CPAH = 650ml/min and the patient has a hematocrit of 45%, what is the rate of renal blood flow?

Quantifying tubular function
Filtration = GFR x PZ
(“filtered load”)
Excretion = UZ x V
(“excretion rate”)
Excretion = filtration – reabsorption + secretion
Reabsorpn = (GFR x Pz) – (Uz x V)
Secretn = (Uz x V) - (GFR x Pz)
Useful data about the transport of a substance by the renal tubule can be obtained by applying a few simple calculations:

Fractional excretion
Fractional excretion of Z (FEZ) = rate of excretion of Zrate of filtration of Z
i.e. excretion of Z as a percentage of the filtered load
= CZ / GFR FEZ = UZ x V GFR x PZ
Proportion of the filtered load was excreted = fractional excretion

Where Does Na+ Reabsorption Occur?
[Na+] =145
FE = 35%
FE = 10%
FE = 3%
FE = 0.1 - 2%[Na+] units = mmole/L
FE= Fractional excretion

The hospital lab reports that your patient's creatinine clearance is 120 g/day. This value is
A. Normal B. Significantly below normal C. Not an interpretable number as presented
List, in order of decreasing renal clearance, the following substances: glucose, urea, sodium, inulin, creatinine, PAH.

The following test results were obtained during a clearance experiment:
UIn = 50 mg/L
PIn = 1 mg/L
V = 2 mL/min UNa = 75 mmol/L
PNa = 150 mmol/L
What is the fractional excretion of sodium?

MicturitionOnce urine enters the renal pelvis, it flows through the ureters and
enters the bladder, where urine is stored.
Micturition is the process of emptying the urinary bladder.
Two processes are involved:
(1) The bladder fills progressively until the tension in its wall is raised above a threshold level, and then
(2) A nervous reflex called the micturition reflex occurs that empties the bladder.
The micturition reflex is an automatic spinal cord reflex; however, it can be inhibited or facilitated by centers in the brainstem and cerebral cortex.

stretchreceptors
Urine Micturition

•1) APs generated by stretch receptors•2) reflex arc generates APs that•3) stimulate smooth muscle lining bladder•4) relax internal urethral sphincter (IUS)•5) stretch receptors also send APs to Pons•6) if it is o.k. to urinate–APs from Pons excite smooth muscle of bladder and relax
IUS–relax external urethral sphincter
•7) if not o.k.–APs from Pons keep
EUS contracted
stretchreceptors





REGIONAL TRANSPORT
LEARNING OBJECTIVES
• Describe the contribution of the major nephron segments to the reabsorption of the filtered load of solute and water.
• Describe the cellular mechanisms for the transport of Na+, Cl-, K+, HCO3-, Ca2+, phosphate, organic solutes (e.g., glucose, amino acids, and urea), and water by the major tubular segments.
• Describe the function of the following renal transporters and their predominant localization along the tubules with regard to nephron segment and apical versus basolateral membranes
• Transport ATPases (Na+/K+-ATPase, H+/K+-ATPase, H+-ATPase, and Ca2+-ATPase)
• Ion and water channels (K+, ENaC, Cl-, Ca2+, aquaporins)
• Coupled transporters (Na+-glucose, Na+/H+-antiporter, Na+-K+-2Cl--symporter, Na+-phosphate symporter, Na+-Cl--symporter, Na+-HCO3 --symporter, Cl-/HCO3--antiporter)


• Solutes that are reabsorbed by both active and passive processes include glucose, amino acids, urea, and ions such as (sodium), (potassium),(calcium),(chloride),(bicarbonate), and (phosphate).
• Secreted substances include hydrogen ions ,potassium, ammonium ions, creatinine, and certain drugs such as penicillin.
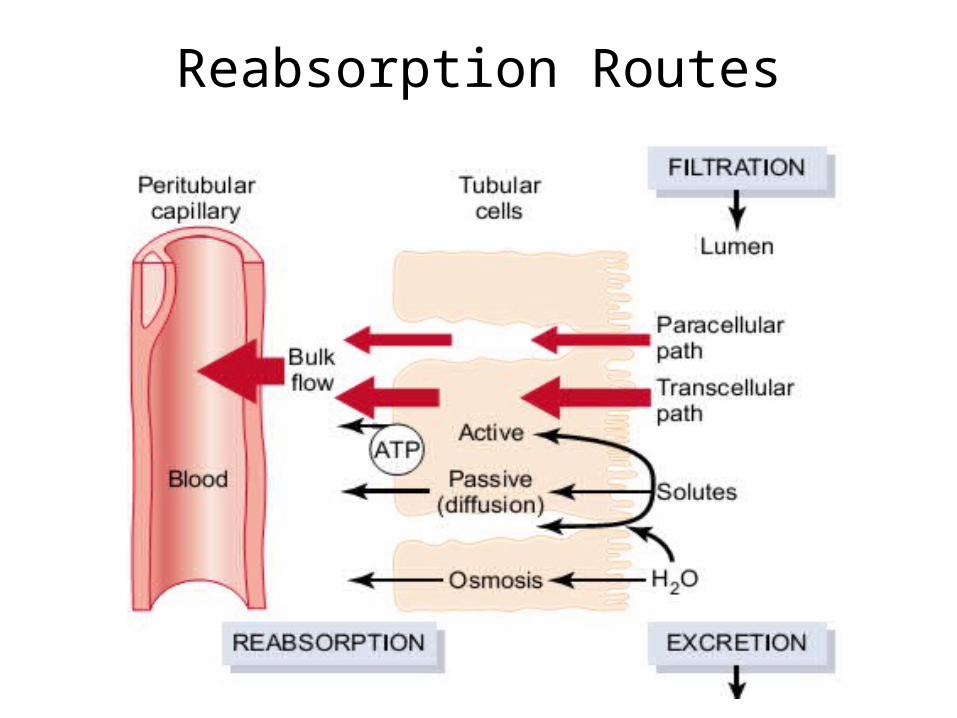
Reabsorption Routes

Reabsorption and Secretion in the Proximal Convoluted Tubule


Actions of Na/H + antiporters in proximal convoluted tubule cells.
• (a) Reabsorption of sodium ions (Na and secretion of hydrogen ions via secondary active transport through the apical membrane;
• (b) reabsorption of bicarbonate ions via facilitated diffusion through the basolateral membrane.


Q
Na +is reabsorbed from the basolateral surface of the renal epithelial cells bya. Na/H exchangeb. Na-glucose cotransportc. Na-K pumpd. Facilitated diffusione. Solvent drag

Proximal Tubule Changes
1. Water and electrolytes• Approximately 2/3 of the filtered sodium is
reabsorbed in the proximal tubule by primary and secondary active transport.
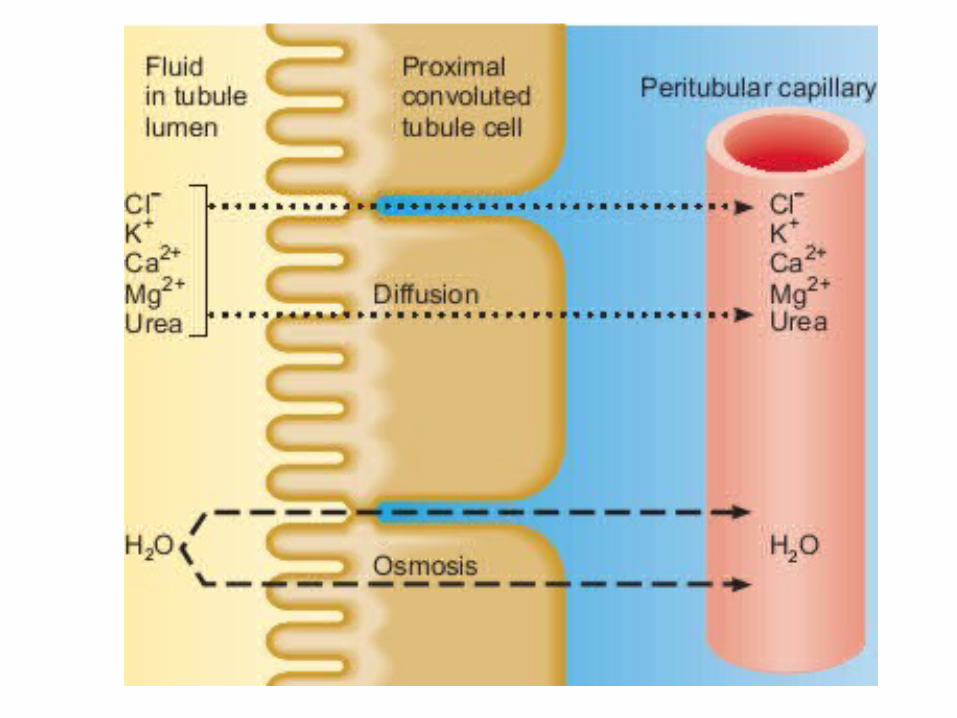
• About two-thirds of the filtered H2O, K+, and almost two-thirds of the filtered Cl– follow the sodium (leaky system to these substances), and the osmolarity at the end of the proximal tubule remains close to 300 mOsm/L (isosmotic reabsorption).
• As water leaves the tubular fluid, the concentrations of the remaining filtered solutes increase.
• In the second half of the PCT, electrochemical gradients for Cl-,K+,Ca2+,Mg2+, and urea promote their passive diffusion into peritubular capillaries via both paracellular and transcellular routes.

Proximal Tubule Changes
• The chloride concentration rises slightly through the proximal tubule because of the large percentage of bicarbonate reabsorbed here.
• Therefore, at the end of the proximal tubule, osmolarity and the concentrations of Na+ and K+ have not changed significantly from plasma, but only a third of the amount originally filtered remains.

Proximal Tubule Changes
2. Metabolites• Normally, all carbohydrates, proteins,
peptides, amino acids, and ketone bodies are reabsorbed here via secondary active transport (requires luminal sodium, linked to sodium reabsorption).
• Therefore, the concentration of the above should be zero in the tubular fluid leaving the proximal tubule (clearance is zero)

3. Bicarbonate • About 80–90% of the filtered bicarbonate is
reabsorbed indirectly here.• Because the process simply recovers the
amount filtered, there is no net gain or loss of bicarbonate by the body.
• The small amount of bicarbonate that leaves the proximal tubule is normally re-absorbed in subsequent segments.



• Thus, for every H+ secreted into the tubular fluid of the proximal convoluted tubule, one HCO3 and one Na are reabsorbed.

Secretion in the proximal tubule
• Many organic anions and cations are secreted and cleared from the circulation including PAH, penicillin, atropine, and morphine.
Energy requirements
• All of the active processes are powered by the Na/K- ATPase primary active pump. It represents the most energy-demanding process of the nephron. The nephron also has a H-ATPase that contributes to the active H+ secretion.




Ratio of the concentration of the substance in the proximal tubular fluid (TF) to the concentration in the
plasma (P)
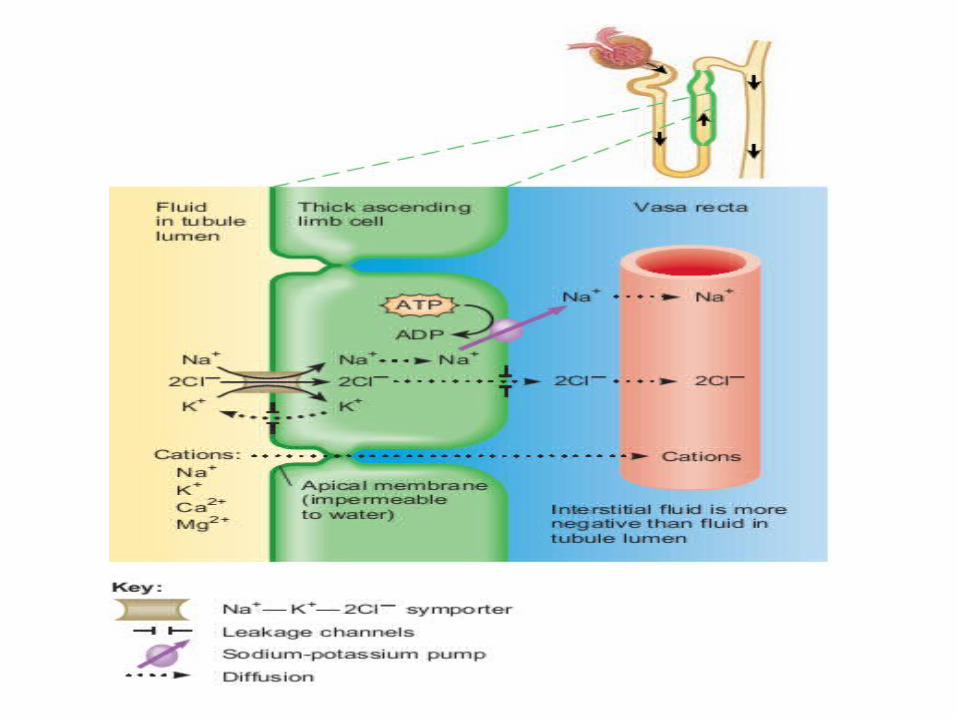
Reabsorption in the Loop of Henle
• The loop of Henle reabsorbs about 25% of the filtered electrolytes, which include Na+, Cl–, K+, Ca++and HCO3–.
• About 15% of the filtered water is also reabsorbed here.
• Again this is powered by the Na/K-ATPase located on the basolateral membrane.



DISTAL TUBULE AND COLLECTING DUCT
• Early distal tubule reabsorbs Na, Cl, and Ca. The NaCl crosses the apical membrane via a Na-Cl symporter.
• The Na is pumped across the basal membrane via the Na/K-ATPase proteins and the Cl diffuses down its electrochemical gradient through channels. This section is impermeable to water. Thus osmolarity decreases further.

Early DISTAL TUBULE
• Calcium transport is similar throughout the nephron.
• Calcium enters the cell from the luminal fluid passively through calcium channels.
• It is actively extruded into the peritubular fluid via Ca2+ATPase or a 3Na+ - Ca2+antiporter.



Late distal tubule and collecting duct They are composed of principal cells and intercalated cells.• Principal cells reabsorb sodium with some chloride and
water. They secrete potassium.• Intercalated cells are represented by 2 different
populations of cells.• Some secrete H+ and in doing so generate brand new
bicarbonate, which is secreted into the circulation. • The second population secretes bicarbonate into the
lumen of the tubule. Both are involved in acid–base regulation. This is the section of the nephron responsible for eliminating fixed acids produced by body metabolism



Reabsorption and Secretion in the Late Distal Convoluted Tubule and Collecting Duct
• The principal cells reabsorb Na and secrete K; the intercalated cells reabsorb K and HCO3 and secrete H.
• In the late distal convoluted tubules and collecting ducts, the amount of water and solute reabsorption and the amount of solute secretion vary depending on the body’s needs.



Most of the glucose that is filtered through the glomerulus undergoes reabsorption in thea. Proximal tubuleb. Descending limb of the loop of Henlec. Ascending limb of the loop of Henled. Distal tubulee. Collecting duct

Which of the following substances will be more concentrated at the end of the proximal tubule than at the beginning of the proximal tubule?a. Glucoseb. Creatininec. Sodiumd. Bicarbonatee. Phosphate

Q