Urinary Stone analysis
32
Stone analysis Stone analysis Mostafa Sabry Abdullah Demonstrator Department of Biochemistry, Faculty of Pharmacy, Al-Azhar University
-
Upload
mostafa-sabry -
Category
Health & Medicine
-
view
100 -
download
1
Transcript of Urinary Stone analysis

Stone analysis
Stone analysisMostafa Sabry Abdullah
Demonstrator Department of Biochemistry, Faculty of Pharmacy, Al-Azhar University

Definition: Stone formation is a genetic, nutritional or
environmental disease.
Incidence: Recent studies indicate that over 10% of adult males suffering from urinary stone at least one.
Mechanism of stone formation:
Urinary stones are always formed of
substances that normally excreted
in the urine.
These substances for unknown
causes are supersaturated to pass their solubility products leading to
their precipitation and formation of
crystals that bind together to form
stones.
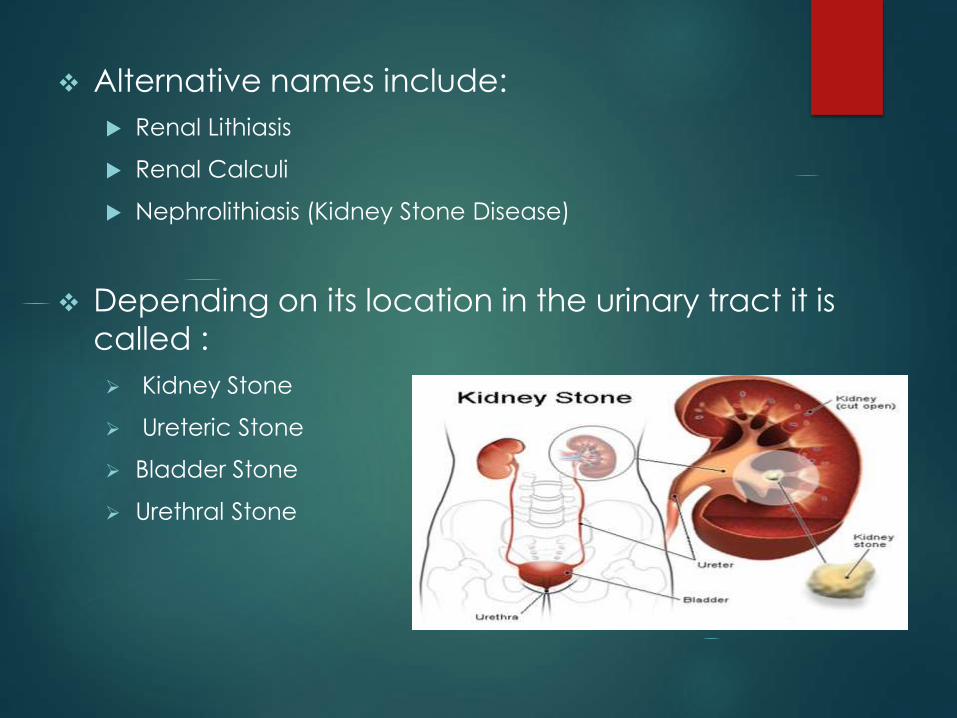
Alternative names include:
Renal Lithiasis
Renal Calculi
Nephrolithiasis (Kidney Stone Disease)
Depending on its location in the urinary tract it is
called :
Kidney Stone
Ureteric Stone
Bladder Stone
Urethral Stone

Classification of stones:Stones may be classified according to two methods:
A. According to number of components:
a) Simple stones: contain only single constituent e.g. Ca oxalate
b) Mixed stones: contain two or more constituent e.g. Ca oxalate+ Ca& Mg phosphate.
B. According to type of components:
1) Ca Oxalate stones: (the most common in Egypt)
2) Ca Phosphate stones.
3) Ca Carbonate stones.
4) Mg Ammonium Phosphate stones.
5) Uric acid stones: 4-10 %
6) Cystine stones: < 1%
7) Xanthin stones: very rare
8) Struvite Stones.
9) Foreign body stones: formed of foreign body that introduced into the body from outside.

Kidney Stone
type
Occurrence in
Population
When do they form
Calcium oxalate 80 % when urine is acidic or alkaline
Calcium
phosphate
0 % when urine is alkaline (high pH)
Uric acid 5-10 % when urine is persistently acidic
Struvite 10-15 % infections in the kidney
Cystine 0 % rare genetic disorder
Calcium stones Uric Acid stones
Struvite Stones Cystine Stones
Factors affecting stone formation:-
1- Change urine pH:
Bacteria
Urea NH3 pH stone.
2- Vitamins disturbances: e.g.
- Exss Vit. D Ca absorption Ca stones.
- Exss Vit. C oxalate stones
- Vit. A Roughness of epithelial cells lining to the urinary tract ppt of crystals crystal formation.
3- Hormonal disturbance :-
e.g. Hyperparathyroidism Ca2+ stones.
4- uric acid level uric acid stones.
5- mucoprotein: which act as a cement material to bind crystals stones.

Risk factors for stone formation
1. Renal risk factor
1- Infections,
2- Obstructions,
3- Parasitic infections, as:- schistosomiasis.
4- Congenital anomalies.

2. Pre-urinary risk factors:
A) Intrinsic:
1-Hereditary:
2- Age:
3- Sex:
4. Mechanical factors :

A) Intrinsic:1-Hereditary:
Renal tubular acidosis :;
Primary hyperoxaluria;
Cystinuria;
Hyperuricosuria;
Absorptive hypercalciuria: this is the most common
Cushing syndrome.

2- Age: stones are rare in children, why??
who have a high level of inhibitors and
low level of urinary calcium, who have a low saturation of
calcium salts.
3- Sex: Urolithiasis is more common in men; the male : female ratio is 4 : 1. why??
Men excrete more calcium oxalate and uric acid leading to
higher urinary concentration of these salts.
Estrogens in women increases the concentration of citrate.

4. Mechanical factors :
a- Anatomical:
e. g. bifid ureters, horse show kidney;
b- Medullary sponge kidney:
this is abnormality of the renal pyramids stemming from the
obstruction and cystic dilatation of the collecting ducts at the papillary tips

Horse-shaped kidneyBifid ureter
B) Extrinsic Geography
Climate
Diet
Occupation
Water:
Hot climate
Hot occupation
Low fluid intake
Composition:
soft water and hard water.
Infection stones:

B) Extrinsic
1- Geography:
In Europe the Mediterranean region have
higher incidence than northern Europe.
…….This may be due to climate.
2- Climate:
The highest rate occurs in the hottest parts
of the high-incidence countries.
Urinary calcium rises in the summer.
3- Diet :
a) Protein: Protein can increase the supersaturating of the urine .
b) Hyper-calci-uria:- results from renal tubular acidosis.
c) Hyper-phosphate-uria; results from the renal tubular acidosis ;
d) Hyper-uricosuria:is produced from the high purine intake and ammonium production forming amm. Acid urate.
e) Hyper-oxaluria:increased synthesis of oxalate from amino acids e.g. glycine, tyrosine, and hydroxy proline.

f) Carbohydrate:
Administration of glucose or sucrose is accompanied by increase
calcium in urine ,
due to the calciuric effect of insulin.
h) Excess sodium intake:
Most factors that cause natriuresis (excretion of sodium in urine)
increase calcium excretion.
sodium and calcium are reabsorbed from common sites in the
tubules.


4- Occupation:
There is a higher incidence of stone in sedentary workers (in the
armed force, office personal have a higher risk than active units
such as the royal marine).
5- Water:
a) Amount: chronic dehydration stone disease
b) Hot climate
c) Hot occupation
d) Low fluid intake:
patients whose 24h urinary volumes are less than 1400 ml show an
increased recurrence rate.
e) Composition:
stone formation is higher in soft water areas than in hard water
areas
6- Infection stones:
Chronic infections in the urinary tract can cause renal calculi
that are
Struvite: magnesium ammonium phosphate (Mg NH4.6H2O;)
and
Carbonate appetite: (Ca10PO4.6CO3).
The most common found in stone patients are Proteus and
Pseudomonas.

Inhibitors of stone formation:
a) Ions: citrate, magnesium, and pyrophosphate
b) Larger molecules:
Glycosaminoglycans (GAGs):
Nephrocalcin:
Complexers:

Glycosaminoglycans (GAGs):
They are polysaccharides chains of repeating disaccharides
derived by degradation of high molecular weight proteoglycans;
GAG excretion is greater in male subjects, rising post- prandially
and at night ; excretion rises by 50% in summer;
GAGs inhibit calcium oxalate crystallization.
Nephrocalcin:
It is a recently isolated γ- carboxy-glutamic acid-containing protein ;
it inhibits calcium oxalate crystallization and may be structurally
abnormal or deficient in some stone patients.
Complexers:
Specific charged ions combine with potential crystalline
components to form soluble complexes reducing the free ionic
concentration:
Anions such as citrate , phosphate , and sulphate complex
calcium.
Cations such as magnesium complex oxalate .

Promoters of stone formation:
Tamm- Horsfall protein and the organic matrix.
The composition of the urine diurnal variation.
The times associated with the highest supersaturation occur between 6 and 10 a.m. and between 6 and 10 p.m.
Meals cause variations, especially in the concentration of
calcium.
The highest excretion of oxalate and urate occurs early in the morning.

Tamm- Horsfall protein
It is the matrix of urinary casts derived from the
secretion of renal tubular cells
When this protein is concentrated at low pH, it forms a gel.
act as a constitutive inhibitor of calcium
crystallization in renal fluids,provide defense against urinary tract infections .

PromotersInhibitors
•Calcium
•Sodium
•Oxalate
•Urate
•Low urine pH
•Tamm- Horsfall
protein
•Low urine volume
• Citrate
• Magnesium
• Pyrophosphate
• Glycosaminogly
can
• Nephrocalcin
• High urine volume

Prevention and treatment: 1- Predisposing factors
2- Sterilize the urine with antimicrobials.
3- Inhibitors, e.g. Mg citrate. Also, urease inhibitors
such as aceto-hydroxamic acid.
4- Promotors: see above.
5- Substrate depletions with the use intestinal phosphate binders to lower the urinary phosphate
excretion.
6- Surgical removal of the stone.
7- Ultrasonic lithotripsy.
5- Medication: ascorbic acid, acetazolamide and triamterene are a therapeutic agents which may
lead to stone formation.

Fate of stone: 1- Still as it is (dominant stone).
2- May increase in size.
3- Migration stone: it is the causative agents
of pain (very common).to pass out with urine
must not increase than (1) cm in size.
4- Very common complications:
a) Renal spasm and pain.
b) Haematourea, renal infection and pus in
urine may be also present.
c) Multiple stone may lead to obstructions of
urinary tract , consequently back pressure occur in the kidney which may lead to renal
failure.
Method of stone analysis:
a) Preparation of stone:
Wash from casts and attached epithelia, dry and
grind the stone to a fine powder, then carry out
the following tests as described in the following procedures:

b) Sample: grinded renal stone

Test Procedure Observation
1- pH
Sample + 1 drop of universal indicator
(R1)
Yellow- red: Acidic
Green: Neutral
Blue: Alkaline
2-Carbonate Sample + 2 drops of 2N HCL (R4) Effervescence
3-Oxalate Sample mixed with equal portion of
resorcinol (R3) +1 drop of conc.
Sulphuric acid (R2)
Dark blue green color
4-Phosphate Sample + mixture of [2 drops of (R5)+
2 drops of (R6)]+ 1 drop of (R7)
Blue color
5-Calcium Sample + 2 drops of H2O + 2 drops of
2N HCL (R4) + 5 drops of 10N NaOH
(R7) add gradually.
Gelatinous PPt.

6- Cystine
Sample + 2 drops of NaOH 10%
(R10) + 1 drop of amm. Hydroxide
25% (R12) + 2 drops of Na CN
(R8)allow to stand for 5 min. + few
crystals of sodium nitroprusside
(R9)
Red color
7- Ammonium
salts
Sample+ 2 drops NaOH 10% (R10)
+ 5 drops of cobalt chloride (R11)
Blue color
8-Uric acid Sample + 2 drops of NaOH (R10)
mix. + 3 drops of phosphotungestic
acid (R13)
Blue color
9- Magnesium Sample + 2 drops of NH4OH 25%
(R12) + 2 drops Na2 PO4 0.1M (R14)
Gelatinous white
PPt.









![Urinary Stone Management [Dr. Edmond Wong]](https://static.fdocuments.in/doc/165x107/55d4fd91bb61eba4528b46ca/urinary-stone-management-dr-edmond-wong.jpg)