
Upstream Social Marketing ASU Wellness and Health Promotion May 13, 2008 Karen Moses, MS, RD, CHES...
43
Upstream Social Marketing ASU Wellness and Health Promotion May 13, 2008 Karen Moses, MS, RD, CHES and Jim Grizzell, MBA, Policies and Laws Living Conditions Discrimination Social Capital Culture Social Networks Social Gradients Violence Social Support Income Transportation Education Individual and Community Health
-
Upload
annabel-blair -
Category
Documents
-
view
219 -
download
0
Transcript of Upstream Social Marketing ASU Wellness and Health Promotion May 13, 2008 Karen Moses, MS, RD, CHES...

Upstream Social Marketing
ASU Wellness and Health PromotionMay 13, 2008
Karen Moses, MS, RD, CHES and Jim Grizzell, MBA, MA, CHES, HFI
Policies and Laws
Living ConditionsDiscrimination Social Capital
Culture
Social Networks
Social Gradients
ViolenceSocial Support
Income
Transportation
Education
Individual and Community Health

Learning Objectives
• Explain importance of moving upstream– Social determinants of health
– Policy makers, decision makers, implementers, regulators, funders, police, other influencers
• Describe upstream social marketing approaches
• Apply upstream social marketing to ASU health problems

Why Move Upstream
• It is unfair to expect individuals to use healthy behaviors– Even if motivated because barriers make it
difficult
• Social environment in which we live has a marked impact on our choices
• Our behavior is only partially under our own control

Why Use Upstream Social Marketing
• A social determinant may seem– Too big to tackle– Out of bounds because it is not specifically health-
related
• Can’t understand many health problems without acknowledging predisposing causal factors

Why Use Upstream Social Marketing
• Social marketing is appropriate– whenever you have a behavior to influence– for motivating a bureaucrat to implement
new or existing laws or regulations that would contribute to increase social welfare

• Customer orientation
• Behavior• Theory• Insight• Exchanges• Competition
• Audience segmentation and targeting
• Marketing mix
– Continuous and strategic formative & process research, monitoring and evaluating
Benchmarks
Green text are common tasks left out of social marketing programs.

Alan Andreasen’s Approach
• Process– Listening– Planning– Pretesting– Implementing– Monitoring– Revising
• Concepts and tools– Stages of change– BCOS
• Benefits, Costs, Others, Self-assurance
– Competition
• Others concepts– Segmentation, 4Ps,
Branding

CDCynergy Social Marketing Edition
• CDCynergy's Competitive Advantage– Extremely pre/post tested – Distills comprehensive best
practices – Vetted by major players in
social marketing – Over 700 resources – CDC originated – Use CDCynergy for funding
requests • Looked on very favorably!!
– Recognized nationally and internationally
• Phases1. Problem description2. Market research3. Market strategy4. Interventions5. Evaluation6. Implementation
Green text are common tasks left out of social marketing programs.

Logic Model

Phase 1: Problem Description
1. Write a problem statement2. List and map the causes of the health
problem3. Identify potential audiences*4. Identify the models of behavior change and
best practices*5. Form your strategy team6. Conduct a SWOT analysis
* These are Logic Model items

Phase 2: Market Research
1. Define your research questions2. Develop a market research plan3. Conduct and analyze market research4. Summarize research results

Phase 3: Market Strategy
1. Select your target audience segments*2. Define current and desired behaviors for
each audience segment*3. Describe the benefits you will offer*4. Write your behavior change goal(s)*5. Select the intervention(s) you will develop for
your program6. Write the goal for each intervention

Phase 4: Interventions
1. Select members and assign roles for your planning team
2. Write specific, measurable objectives for each intervention activity*
3. Write a program plan, including timeline and budget, for each intervention
4. Pretest, pilot test, and revise as needed5. Summarize your program plan and review the factors
that can affect it6. Confirm plans with stakeholders

Phase 5: Evaluation
1. Identify program elements to monitor2. Select the key evaluation questions3. Determine how the information will be
gathered4. Develop a data analysis and reporting plan

Phase 6: Implementation
1. Prepare for launch2. Execute and manage intervention
components3. Execute and manage the monitoring and
evaluation plans4. Modify intervention activities, as feedback
indicates

Learning Objectives
• Explain importance of moving upstream– Social determinants of health
– Policy makers, decision makers, implementers, regulators, funders, other influencers
• Describe upstream social marketing approaches
• Apply upstream social marketing to ASU health problems

Extra Slides

Resources

Resources

Moving to a Health Agenda 20
Positive outcomes and ROI
Reduced utilization
Reinforcement Management: Finding intrinsic and extrinsic rewards for new ways of working;
Environmental Reevaluation: Appreciating that the change will have a positive impact on the social and work environment;
Self-Liberation: Believing that a change can succeed and making a firm commitment to the change
Self-Reevaluation: Appreciating that the change is important to one’s identity, happiness, and success
Dramatic Relief: Emotional arousal, such as fear about failures to
change and inspiration for successful change
Consciousness Raising: Becoming more aware of a problem and potential solutions
Processes of Change

Customer Orientation• Customer in the round’ Develops a robust understanding of
the audience, based on good market and consumer research, combining data from different sources– A broad and robust understanding of the customer is
developed, which focuses on understanding their lives in the round, avoiding potential to only focus on a single aspect or features
– Formative consumer / market research used to identify audience characteristics and needs, incorporating key stakeholder understanding
– Range of different research analysis, combining data (using synthesis and fusion approaches) and where possible drawing from public and commercial sector sources, to inform understanding of people’s everyday lives

Insight
• Based on developing a deeper ‘insight’ approach – focusing on what ‘moves and motivates’– Focus is clearly on gaining a deep understanding and
insight into what moves and motivates the customer– Drills down from a wider understanding of the customer to
focus on identifying key factors and issues relevant to positively influencing particular behaviour
– Approach based on identifying and developing ‘actionable insights’ using considered judgement, rather than just generating data and intelligence

23
Health in Higher Education
• Health in higher education supports 18 million students in 4,200 IHEs
• Many college and university professionals work in higher education to promote health– 250 professionally prepared ACHA HEs - 1:72,000*– 19,000 faculty and staff – 1:947
• Health problems– Campus wide– Specific to college or major
• Influences quality and productivity
* See notes section

24
Traditional Health Programs
• Use the Medical Model– Health services has primary responsibility– Staff trained in clinical practice
• Health care agenda focus is on the physical– Healing sickness/injury– Wellness for physical health
• Methods focus on the individual– Awareness activities, written information, didactic
presentations

25
The Traditional Approach
• Limits our understanding of health – Physical health is what counts most– Ignores role of environment/community on health– Lacks prevention focus
• Financially costly and ineffective– Lacks cost-effectiveness, positive ROI, reach, impact
• Removes responsibility for health outcomes by non-health entities– Gives medical systems a lot of power

26
Traditional Health Programs
• Based on tradition, convention, belief, anecdotal evidence
• Pressure to be seen as acting• Desire to help• Poorly developed skills and understanding of
population behaviour change• Short term policy planning, budgeting and
review

27
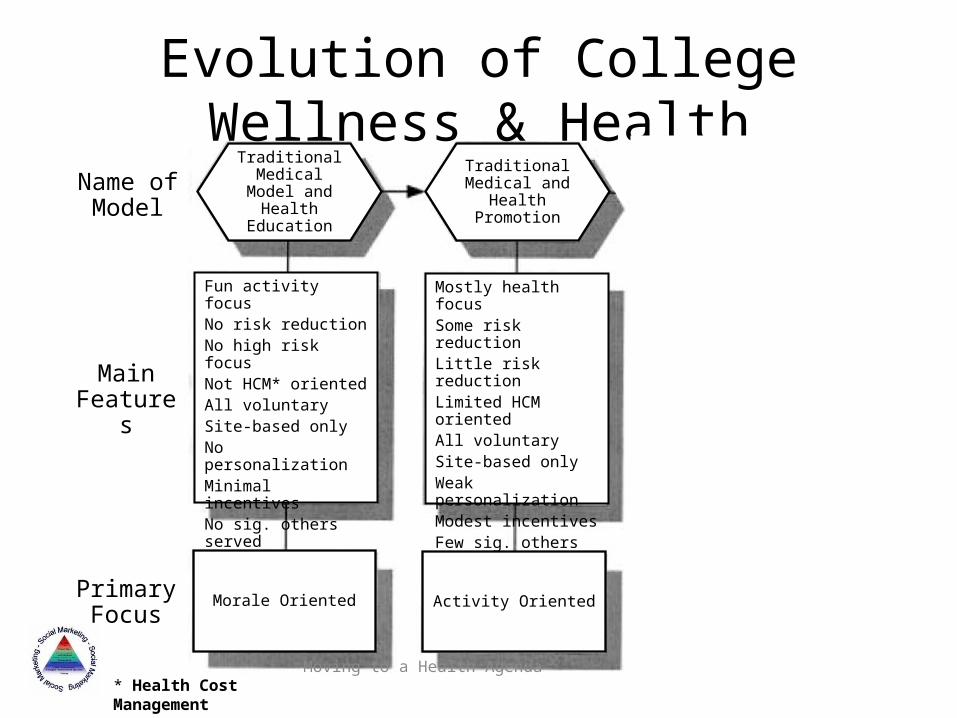
Evolution of College Wellness & Health
1850s 1970s 1980s ~1995 2010
Instruction, Treatment, Exercise Health Education/Promotion EB/CE-HP*
1st Generation 2nd Generation 3rd Generation
* Evidence-based / Cost Effective Health Promotion
HealthyCampus
Objectives
Moving to a Health Agenda 28
Evolution of College Wellness & Health
Results / Outcome Oriented
Evidence-Based & Cost-
Effective Health
Promotion
* Health Cost Management
Focus on student learningStrong risk reductionStrong high risk focusSome required activitySite and virtualEnvironmental changesStrongly personalMajor incentivesSig. others servedRigorous assess/eval
Traditional Medical and
Health Promotion
Traditional Medical Model
and Health Education
Mostly health focusSome risk reductionLittle risk reductionLimited HCM orientedAll voluntarySite-based onlyWeak personalizationModest incentivesFew sig. others servedWeak assess/eval
Fun activity focusNo risk reductionNo high risk focusNot HCM* orientedAll voluntarySite-based onlyNo personalizationMinimal incentivesNo sig. others servedNo assessment/eval
Activity OrientedMorale Oriented
Name of Model
Main Features
Primary Focus

Social MarketingCommercial vs. Social
• Marketing is about behavior change– The bottom line– ROI and CEA
• If your intervention won’t change behavior– Don’t do it!!!!
• Theory– Distillation of previous work– Simplify complex phenomena

Some Questions to Guide Theory Selection
• Where are people in relation to a particular behavior?
• What factors cause this position?• How can they be moved in the desired
direction?

32
Keys to Effective Use of the Ecological Perspective
• Expand the focus beyond health information and programming
• Integrate responsibility for health across student affairs and academic units
• Provide supportive environments and reduce barriers to optimal outcomes
• Promote leadership and involvement by multiple partners

33
Intervention Pyramid
High
Low
Cost
High
Low
Reach
Policies
Health Communication, SocialEcological Model & Social Marketing
Activities no feedbackHealth Systems
Activities w/ Health Education
SpecialtyCare
Community &Neighborhood Collaboration
Primary Care

Moving to a Health Agenda 34
Business Case
Levels of Interventions & Wellness Program ROIs
Program Levels
Intervention Levels
Quality of Life
TraditionalHealth &
Productivity
I. Awareness Information, no feedback
<1:1
IIa. Behavior Change Health education w follow-up
3:1
IIb. Behavior Change Targeted priority health
issues with Social Marketing
6:1 to >15:1
III. Supportive Environment Ecological Approach, Policies
>15:1

35
Continuum of Services
Intensive
Early Intervention
Universal Prevention
For students at highest risk of engaging in high
behaviors or already having a health problem
For students at risk of engaging in high
behaviors or already having the health
problemFor all
students, regardless of
risk to delay or prevent health
problems
From Dept of Education Safe Schools / Healthy Students Grant Guidelines

36
Health in Higher Education
Karen S. Moses, MS, RD, CHES*Director, Wellness and Health PromotionArizona State University
Chair, NASPA Health in Higher Education Knowledge CommunityMember at Large, ACHA Board of Directors Deputy Coordinator, Coalition of National Health Education Organizations
* Certified Health Education Specialist

37
The Ecological Perspective
The science and art of helping people change their lifestyle to move toward a state of optimal health….Lifestyle change can be facilitated through a combination of efforts to enhance awareness, change behavior, and create environments that support good health practices. Of the three, supportive environments will probably have the greatest impact in producing lasting changes.
• M. P. O’Donnell, American Journal of Health Promotion (1986)
38
A New Paradigm: The Ecological Approach to Campus Health
• Views the connections among health, learning, and the campus structure
• Explores relationships between and among individuals and the learning communities that comprise the campus environment

39
Using the Ecological Perspective on Campus
• Establish a Working Group• Identify Campus Values• Assess Student Health Data• Analyze Campus Health Concerns
Through an Ecological Lens• Environmental influences• Individual influences
• Develop a Plan

40
Influencing Factors
Individual
People
Community
Characteristics of the:
Place
Organization

41
Environmental Influences
Behavior settings: Rituals,student organizationsCultural Influences: Customs, traditions, valuesEconomic Forces: Student financial stability, budgetInhabitants: Diversity, Athletics,Greek, campus communities, etc.
The location of the campusThe weatherThe constructed designsLandscapes
Organizational StructurePoliciesOrganizational Climate
Political ClimateConservative/liberal Pro education?Reinforcement and RewardsFor healthy org & indiv behaviors
Place People
Organization Community

42
Stress: Environmental Influences
Financial concernsISO – global troubles
Relationships w/friendsLack of friends/commuters
Irresponsible drinkersUninvolved students
Warm climateLack of parking
High trafficCampus size—distances
Crowding—long lines
Services--lack of info Depts disconnected
Too many stepsWeak policy enforcement
Inconsistent messages
State budget crisisIncrease in tuition/fees
Rewards for over commitment
Culture of stress
Place People
Institution Community
Social Marketing in Health Promotion 43
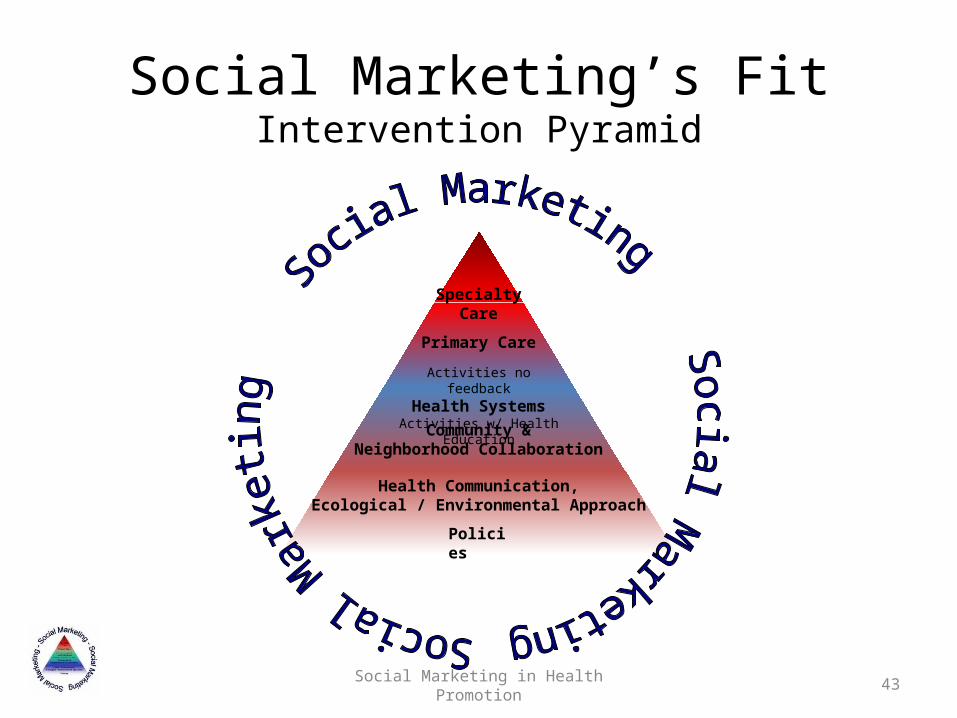
Policies
Health Communication,Ecological / Environmental Approach
Activities no feedback
Health SystemsActivities w/ Health Education
SpecialtyCare
Community &Neighborhood Collaboration
Primary Care
Social Marketing’s FitIntervention Pyramid

Moving to a Health Agenda 44
Historical Snapshot: Think Health Agenda & Business Case
Corporate & College Health & Wellness
1850s 1970s 1980s ~1995 2010
Recreation Fitness Health Education > Promotion HPM*
1st Generation 2nd Generation 3rd Generation 4th Generation
Instruction, Treatment, Exercise Health Education > Promotion HAPM*
1st Generation 2nd Generation 3rd Generation
* Health & Productivity Management, Health & Academic Performance Management


















