Upper Tract Urodynamics

of 30
-
Upload
srivathsan-ramani -
Category
Documents
-
view
237 -
download
0
Transcript of Upper Tract Urodynamics
-
8/4/2019 Upper Tract Urodynamics
1/30
UPPER TRACTURODYNAMICS
DR.R.SRIVATHSAN1ST YEAR
MCH UROLOGY
-
8/4/2019 Upper Tract Urodynamics
2/30
CELLULAR ANATOMY
The primary functional anatomic unit of the ureteris the ureteral smooth muscle cell.
The cell is extremely small
250 to 400 m in length
5 to 7 m in diameter
Endoplasmic reticulum and sarcoplasmic reticulumfor Ca2+ storage.
Contractile proteins - actin and myosin
Dark bands along the cell surface are referred to as attachmentplaques
Caveolae - function is not known - ? Nutritive ? Ion transport. A double-layer cell membrane surrounds the cell -inner plasma
membrane & the outer basement membrane which is absent at areasof close cell-to-cell contact - intermediate junctions.
-
8/4/2019 Upper Tract Urodynamics
3/30
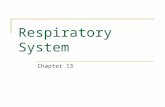
General organization of the guinea-pig upper urinary tractLow magnification electron micrographsthrough the pelvi-calyceal junction (A), the proximal renal pelvis (B) and the ureter (C) of the guinea-
pig, illustrating the layered appearance of the epitheliUM
Klemm M F et al. J Physiol 1999;519:867-884
-
8/4/2019 Upper Tract Urodynamics
4/30
DEVELOPMENT OF THE URETER
The ureter arises as an outpouching from the mesonephric
duct.
Ureteric bud formation & branching is induced by glial cellline derived neurotrophic factor (GDNF) derived from
adjacent metanephrogenic mesenchyme.
GDNF signals through the c-Ret receptor tyrosine kinasewhich results in increased phosphatidylinositol 3-kinase
(PI3K) activity and AKT/PKB phosphorylation.
-
8/4/2019 Upper Tract Urodynamics
5/30
[Transforming growth factor (TGF-), hepatocyte
growth factor (HGF), fibroblast growth factors (FGF 1, 2,
7, and 10)
Matrix molecules such as heparin sulfate proteoglycans,
laminins, integrins, and matrix metalloproteinases(MMPs).
Apoptosis is involved in branching of the ureteric bud and
subsequent nephrogenesis.
Inhibitors of caspases inhibit ureteral bud branching.
Angiotensin II acting through the Angiotensin II type I
receptor is involved in the recanalisation process of ureter.
-
8/4/2019 Upper Tract Urodynamics
6/30
ELECTRICAL ACTIVITY
Pacemaker Potentials and Pacemaker Activity:
Electrical activity arises in a cell either spontaneously or in response to
an external stimulus. Spontaneously pacemaker cell.
The ionic conduction underlying pacemaker activity is due to the
opening and slow closure of voltage activated L ca channels
amplified by prostanoids.
Nervous system has little or no role in maintaining pyeloureteral
motility.
The pacemaker cells are located near the pelvicalycealborderC-kit containing Cajal cell?
Latent pacemaker cells are present in all regions of the ureter
-
8/4/2019 Upper Tract Urodynamics
7/30
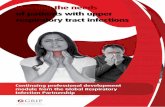
Immunohistochemical staining for Kit in the rat
2009 by American Physiological Society
-
8/4/2019 Upper Tract Urodynamics
8/30
URETERAL CONTRACTION
The ureter is a functional syncytium. Engelmann -stimulation contraction propagates
proximally and distally
But under normal conditions, electrical activity
arises proximally and is conducted distally thru
intermediate junctions
Gap junctions - groups of channels in the plasma
membrane - enable exchange of ions and smallmolecules and play a role in electrical coupling
between adjacent cells and in electromechanical
coupling (18-Glycyrrhetinic acid)
-
8/4/2019 Upper Tract Urodynamics
9/30
URETERAL FUNCTION
Ureter transports urine from the kidney to the bladder. Under normal conditions,
ureteral peristalsis originates at pacemaker sites located inthe proximal portion of collecting systemelectricalactivity propagated distallymechanical event of
peristalsis - ureteral contraction which propels the bolusof urine distally.
Efficient propulsion of the urinary bolus depends on theureter's ability to coapt its walls completely
Urine passes into the bladder by way of the ureterovesicaljunction (UVJ), which, under normal conditions, permitsurine to pass from the ureter into the bladder but not viceversa.
-
8/4/2019 Upper Tract Urodynamics
10/30
Conduction velocity in the ureter is 2 to 6 cm/sec
Vary with temperature, the time interval between stimuliand the pressure within the ureter.
CV : 1.5 to 2 m/sec in Purkinje fibers
: 10 to 100 m/sec in the dorsal and ventral roots.
Conduction is similar to that in cardiac tissue [evenWenckebach phenomenon (a partial conduction block) hasbeen demonstrated]
-
8/4/2019 Upper Tract Urodynamics
11/30
MECHANICAL PROPERTIES OF URETER
Force-length relations: HYSTERESIS
Express the relation between the force developed bymuscle when it is stimulated under isometric conditionsand the resting length of the muscle at the time of
stimulation. The resting or contractile force developed at any given
length depends on the direction in which the change inlength is occurring and on the rate of length changehysteresis
For the ureter, at any given length, the resting force is lessand the contractile force is greater when the ureter isallowed to shorten than when the ureter is being stretched
-
8/4/2019 Upper Tract Urodynamics
12/30
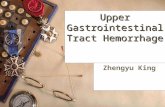
HYSTERESIS
Resting and contractile (active) forceof cat ureter during musclelengthening and shortening.
Force is on the ordinate;
change in length (L) is on theabscissa.
Solid symbols and solid lines showdata obtained during musclelengthening.
Open symbols and dashed lines showdata obtained during muscle
shortening. Circles show resting force, and
triangles show active or contractileforce.
Length and the direction of lengthchange influence resting andcontractile force
-
8/4/2019 Upper Tract Urodynamics
13/30
Stress Relaxation:
When the ureter is stretched, the resting force increases. If the
length is kept constant at its new longer length after a
stretch, changes occur that result in a decrease in the
resting force, or stress relaxation
-
8/4/2019 Upper Tract Urodynamics
14/30
Creep:
Ureteral muscle arrangement: longitudinal, circumferential
& spiral configuration.
After application of an intraluminal pressure, the ureter
increases in both length and diameterCREEP
-
8/4/2019 Upper Tract Urodynamics
15/30
ROLE OF THE NERVOUS SYSTEM IN
URETERAL FUNCTION
The ureter is a syncytial type of smooth muscle without
discrete neuromuscular junctions
Ureteral peristalsis can occur without innervation.
[Transplant]
However, analysis of the data in the literature clearly
indicates that the nervous system plays at least a
modulating role in ureteral peristalsis
-
8/4/2019 Upper Tract Urodynamics
16/30
Parasympathetic Nervous System
The prototypic cholinergic agonist is ACh, which serves as the
neurotransmitter at
(1) neuromuscular junctions of somatic motor nerves (nicotinic
sites)
(2) preganglionic parasympathetic and sympathetic neuroeffector
junctions (nicotinic sites)(3) postganglionic parasympathetic neuroeffector sites (muscarinic
sites).
Cholinergic agonists (ACh, methacholine,carbachol, bethanechol) -Excitatory effect on ureteral and renal pelvic function, that is, to
increase the frequency and force of contractions.
Atropine itself has little direct effect on ureteral activity effects are
frequently minimal and inconsistentno use in ureteric colic
-
8/4/2019 Upper Tract Urodynamics
17/30
Sympathetic Nervous System
The ureter contains excitatory -adrenergic and inhibitory
-adrenergic receptors
(NA inc, IP dec)
-
8/4/2019 Upper Tract Urodynamics
18/30
OTHERS
Tachykinins and calcitonin generelated peptide (CGRP)(peripheral endings of sensory nerves)
Tachykinins stimulate and CGRP inhibits electrical and
contractile activity.
Capsaicin-sensitive sensory nerves are located in the ureter
Renal pelvic sensory nerves contain both substance P and
CGRP
CGRP potentiates the afferent renal nerve activity responses
to substance P by retarding the metabolism of substance P
-
8/4/2019 Upper Tract Urodynamics
19/30
RENAL PELVIC PHYSIOLOGY
The pressure within the renal pelvis is normally close to zero.
When this pressure increases (obstruction or reflux) pelvicalycesdilate.
The degree of hydronephrosis that develops depends on theduration, degree, and site of the obstruction (output pbl) or inputpbl (diuresis)
The higher the obstruction, the greater the effect on the kidney.
Intrarenal pelvis all the pressure will be exerted on theparenchyma.
Extrarenal pelvis only part of the pressure is exerted on theparenchyma (extrarenal renal pelvis embedded in fat dilates more
readily) In the earlier stages, the pelvic musculature hypertrophy in its
effort to force urine past the obstruction.
Later, however, the muscle becomes stretched and atonic (anddecompensated).
-
8/4/2019 Upper Tract Urodynamics
20/30
Three phases of urine transport.
At flow rates from 0 to 2 ml per minute, transport occurs atlow pressure with a low resistance to flow through ureter.
Between 2 ml and 4 ml per minute significant increasein intrapelvic pressure due to increased resistance in theureter, probably caused by an impediment to passive filling(due to the previous ureteral contraction)
Above 4 ml per minute, transport takes place as acontinuous flow through the ureter, which functions as atube
-
8/4/2019 Upper Tract Urodynamics
21/30
In many cases of UPJ obstruction there is no gross
narrowing at the UPJ but abnormal propagation of the
peristaltic impulse is a causative factor in the obstruction.
It appears possible that, at least in some instances,
disruption of cell-to-cell propagation of peristaltic activity
results in impairment of urine transport across the UPJ
-
8/4/2019 Upper Tract Urodynamics
22/30
Theories of PUJO
Murnaghan - an alteration in the configuration of the musclebundles at the UPJ
Foote et al - decrease in musculature at the UPJ
Hanna - abnormalities in the musculature of the renal pelvis anddisruption of intercellular relations at the UPJ itself.
Murakumo - Increased accumulation of collagen (differences intype I and type III collagen)
Wang - decrease in nerves and in NGF messenger RNA(mRNA) expression
A vessel or adhesive band crossing the UPJ may potentiate thedegree of dilatation in any of the forms of UPJ obstruction
-
8/4/2019 Upper Tract Urodynamics
23/30
URINE TRANSPORTBOLUS
At normal urine flows, the frequency of calyceal and renalpelvic contractions is greater than that in the upper ureter,and there is a relative block of electrical activity at the UPJ
At these flows, the renal pelvis fills; as renal pelvic
pressure rises, urine is extruded into the upper ureter,which is initially in a collapsed state
Ureteral contractile pressures that move the bolus of urineare higher than renal pelvic pressures, and a closed UPJmay be protective of the kidney in dissipating backpressure
from the ureter. As the flow rate increases, the block at the UPJ ceases and
a 1:1 correspondence between pacemaker and ureteralcontractions develops
-
8/4/2019 Upper Tract Urodynamics
24/30
The contraction wave originates in the most proximalportion of the ureter and moves the urine in front of it in adistal direction.
The urine that had previously entered the ureter is formedinto a bolus.
In order to propel the bolus of urine efficiently, thecontraction wave must completely coapt the ureteral wallsand the pressure generated by this contraction waveprovides the primary component of what is recorded byintraluminal pressure measurements.
The bolus that is pushed in front of the contraction wavelies almost entirely in a passive, noncontracting part of theureter
-
8/4/2019 Upper Tract Urodynamics
25/30
Baseline, or resting, ureteral pressure is approximately 0 to
5 cm H2O, and superimposed ureteral contractions ranging
from 20 to 80 cm H2O occur two to six times per minute.
At extremely high flows (Whitaker) the ureteral walls do
not coapt, and a continuous column of fluid, rather than a
series of boluses, is transported.
Effects of diuresis and obstruction appear to be
complementary and additive with respect to thedevelopment of renal pelvic and calyceal dilatation
-
8/4/2019 Upper Tract Urodynamics
26/30
Griffiths andNotschaele (1983)
-
8/4/2019 Upper Tract Urodynamics
27/30
Physiology of the Ureterovesical
Junction
Impediment of efficient bolus transfer across
the UVJ occurs
1. when there is an obstruction at the UVJ
2. when intravesical pressure is excessive,
3. when flow rates are so high as to exceedthe transport capacity of the normal UVJ.
-
8/4/2019 Upper Tract Urodynamics
28/30
the pressure within the bolus increases & exceedsthe pressure in the contraction wave inability ofthe contraction wave to occlude the ureter
completely retrograde flow of urine from thebolus fraction of the urinary bolus passes acrossthe UVJ into the bladder.
large boluses occurring at high-flow conditionswould not be completely discharged into thebladder because the contraction wave pushing thebolus would be forced open and intraureteralreflux would occur.
-
8/4/2019 Upper Tract Urodynamics
29/30
VESICAL PRESSURE
The pressure within the bladder during the storage phase isof paramount importance in determining the efficacy of
urine transport across the UVJ
The ureter has been shown to decompensate whenintravesical pressure approaches 40 cm H2O
-
8/4/2019 Upper Tract Urodynamics
30/30
Thank you