UPPER QUARTER: SHOULDER SENMOCOR TM
18
12/10/20 1 UPPER QUARTER: SHOULDER SENMOCOR TM M USCULOSKELETAL MANAGEMENT OF S HOULDER PAIN 1 TOUCHPOINTS • (PS) • (BD) • (PS) • S OMATOSENSORY E VIDENCE ( PS) • U PPER Q UARTER (PS) • ( BD) • IAOM - US 2 I NTENTIONS • • • IF IT WORKS, USE IT IAOM - US 3 The manual therapy is only as good as the sensorimotor control training that follows it Pain Generator Motion Segment Malfliet A, Kregel J, Coppieters I, De Pauw R, Meeus M, Roussel N, Cagnie B, Danneels L, Nijs J. Effect of Pain Neuroscience Education Combined With Cognition-Targeted Motor Control Training on Chronic Spinal Pain: A Randomized Clinical Trial. JAMA Neurol. 2018 Jul 1;75(7):808-817. doi: 10.1001/jamaneurol.2018.0492. Erratum in: JAMA Neurol. 2019 Mar 1;76(3):373. Moreside JM, McGill SM. Improvements in hip flexibility do not transfer to mobility in functional movement patterns. J Strength Cond Res. 2013 Oct;27(10):2635-43. 4
Transcript of UPPER QUARTER: SHOULDER SENMOCOR TM

12/10/20
1
UPPER QUARTER: SHOULDERSENMOCORTM
MUSCULOSKELETAL MANAGEMENT OF SHOULDER PAIN
1
TOUCHPOINTS
• (PS)• (BD)• (PS)• SOMATOSENSORY EVIDENCE (PS)• UPPER QUARTER (PS)• (BD)•IAOM-US
2
INTENTIONS
•
••
IF IT WORKS, USE ITIAOM-US
3
The manual therapy is only as good as the sensorimotor control training that follows it
PainGenera
tor
Motio
n Segm
ent
Malfliet A, Kregel J, Coppieters I, De Pauw R, Meeus M, Roussel N, Cagnie B, Danneels L, Nijs J. Effect of Pain Neuroscience Education Combined With Cognition-Targeted Motor Control Training on Chronic Spinal Pain: A Randomized Clinical Trial. JAMA Neurol. 2018 Jul 1;75(7):808-817. doi: 10.1001/jamaneurol.2018.0492. Erratum in: JAMA Neurol. 2019 Mar 1;76(3):373.
Moreside JM, McGill SM. Improvements in hip flexibility do not transfer to mobility in functional movement patterns. J Strength Cond Res. 2013 Oct;27(10):2635-43.
4

12/10/20
2
IAOM-US
System Function
Trunk Lumbar: Grand StabilizerCervicothoracic: Supporter
Shoulder Supporter / Placer
Elbow Attenuator
Forearm, Wrist, Thumb, Hand
Effector
5
IAOM-US
”YOU CAN’T FIRE A CANNONFROM A CANOE” •
https://en.wikipedia.org/wiki/Iowa-class_battleship
Lee BC, McGill SM. Effect of long-term isometric training on core/torso stiffness. J Strength Cond Res. 2015 Jun;29(6):1515-26.
Lee B, McGill S. The effect of short-term isometric training on core/torso stiffness. J Sports Sci. 2017 Sep;35(17):1724-1733.
6
IAOM-US
Somatosensory Neuromotor
Rectus Abdominis
External Oblique
Transverse Abdominis
Multifidus
Erector Spinae
Wikimedia Commons
Splenius Capitis & Cervicis
Scalenes
SCM
Longus Colli
Internal Oblique
7
Who 55 y/o male electrician
What & Where
• Right shoulder pain (C5)• Right shoulder tightness
IAOM-US
8

12/10/20
3
IAOM-US
Why Original MOI: 1 week ago that began after shovelingsnow after chopping wood
When Aggravating Factors: • Right arm elevation• Lifting• Reaching• Pulling• Carrying• Driving• Right Side lying Relieving Factors: • Mild AROM exercises • Rest (not too much)
To What Extent
Pain: 1/10 through 7/10. Difficulties w/ overhead and lifting activities. May lose job.
9
IAOM-US
Test Result ProvocationCervical screening Grossly WNL 0/10
Active shoulder girdle motions
Grossly WNL 0/10
Scapulothoracic Dyskinesis Tests
Active flexion R: Conc & Ecc Elevation Dysfunction
Active Abduction R: Downward Rotation
Hands on Hips R: Winging
Inspection: Mild thoracic kyphosis, rounded shoulders, forward head
10
IAOM-US
Arm Elevation Result ProvocationActive Abduction R: Painful arch (80-110o) Yes
Active Flexion R: Painful arch (80-110o) Yes
Active Scaption R: Painful arch (80-110o) Yes
Passive GHJ Motions
External Rotation Not limited NilAbduction Not limited Nil
Internal Rotation Not limited Nil
11
IAOM-US
Passive Elevation Result Provocationw/ Contra Fixation R: 10-degree limit R: 3/10 pain
w/ Ipsi Fixation: Medial OP
Nil R: 5/10 pain
w/ Ipsi Fixation: Posterior OP
Nil R: 7/10 pain
Resistive Testing Strength ProvocationAdd R: 5/5 Nil
Abd R: 5/5 5/10
ER R: 4/5 5/10
IR R: 5/5 Nil
Elbow Flex / Ext R: 5/5 Nil
12

12/10/20
4
IAOM-US
Extra Tests ResultPull Test Abd Pain Free
Pull Test ER Improved strength & less pain
ACJ Mobility Hypomobile glide (Pain free)
SCJ Mobility Normal
Palpation Infraspinatus insertional tenderness
13
IAOM-US
Clinical Syndromes
Pain Generating
Tissues
Tissue Dysfunctions
Neuromotor Dysfunctions
• External Impingement Syndrome
• Upper Crossed Syndrome
• Infraspinatus tendinopathy
• Subacromial Bursitis
Elevation chain limits• ACJ stiffness
Myofascial (need to assess)• Pec Minor?• Posterior
Shoulder?
• Scapular Dyskinesia
• Posterior Rotator Cuff Imbalance / Inhibition
14
Pain Genera
tor
Motio
n Segment
NeuroM
otor
Control
Somato
senso
ry
Control Adva
nced
Perform
anceFu
nctional
Advance
ment
Fundam
ental
Perform
ance
Active 55 y/o Electrician
• Shovel• Chop Wood• Overhead work• Prolonged mid-arc
work
15
PREPARATORY�
�
�
STIFFER
UNCONCIOUS
Lephart SM, Riemann BL, Fu FH. Introduction to the sensorimotor system. In: Lephart SM & Fu F, eds. Proprioception and Neuromuscular Control in Joint Stability. Champaign, IL: Human Kinetics; 2000.
Neuromuscular Control
REACTIVE (REFLEXIVE)
• FEEDBACK CONTROL (FB)
• CONSTANT ADJUSTMENT
• POSTURE AND “SLOW”
MOVEMENT
16

12/10/20
5
ScapulothoracicInitial
Activation
Stabilizer TrainingObjective
Program Surface EMG BioFB
Pain Genera
tor
Motio
n Segment
NeuroM
otor
Control
RUSI
Fundamental Activation
HistoryInstability Checklist
ExaminationMRI XSA & Fatty Infiltration
Rehab Ultrasound Imaging (RUSI) Isometric Dynomometry
Electromyography
Qualitative Activation Assessment
VPAC & DNF’s
Rotator Cuff
17
VOLITIONAL PRE-EMPTIVE ABDOMINAL CONTRACTION(VPAC)
IAOM-US
ADIM
Local Brace
Global Brace Sturdiness Compression
O’Sullivan et al 1992, Robison et al 1992, Tokuno et al 2011, Hodges et al 1987, 1997a, b, Foster et al 1999,Grenier et al 2007, Vera-Garia et al 2007
18
PainGenerator
MotionSegment
NeuromotorControl
VPAC Strategies§ Abdominal Drawing In
Maneuver (ADIM)§ Abdominal Bracing
Maneuver (ABM)§ Multifidus Activation (Mf)§ Pelvic Floor Muscle
Activation (PFM)
Volitional Pre-emptive Abdominal Contraction
IAOM-USSenMoCorTM
19
PainGenerator
MotionSegment
NeuromotorControl
DNF ActivationProposed Mechanism: CORInstruction: § Think “LOOK DOWN”§ Think “LOOK DOWN & TO THE RIGHT”§ Think “LOOK DOWN & TO THE LEFT
Deep Neck Flexors
Jull et al, 2005; O'Leary S, Jull G, Kim M, 2007
Precedence: Personal Communication with G. Jull & M. Sterling
IAOM-USSenMoCorTM
20

12/10/20
6
UE CONTROL?
21
LS Spine-Stability CT Spine-Vision & BalanceShoulder-Placement ControlElbow-Guides & AttenuatesFAWTH-Responder
Control considerations: STJ, Girdle & GHJ
Scapular Control
• Key role in kinetic chain• THE link between the upper & Lower Extremitiess
Scapular Motions
Motions:
• vs Rot, Ant vs Post Tilting, IR vs ER
Normal STJ motion during elevation:
• Rot, ER, vs Post Tilts
• Post Tilt Primarily > 90o
McClure PW, 3-dimensional measurement of scapular kinematics during dynamic movements in vivo. J Shoulder Elbow Surg. 2001;10:260-277.
Michner LA, Sennett BJ, Karduna AR. Direct McClure P, Greenberg E, KarehaArthrosc Rev. 2012;20:39-48.S. Evaluation and management of scapular dysfunction. Sports Med
McClure PW, Michner LA, Sennett BJ, Karduna AR. Direct 3-dimensional measurement of scapular kinematics during dynamic movements in vivo. J Shoulder Elbow Surg. 2001;10:260-277.
22
STJ REQUIREMENTS
•
•
•
RESULT-
ELEVATION: •
1.
2.3.
McClure PW, Michner LA, Sennett BJ, Karduna AR. Direct 3-dimensional measurement of scapular kinematics during dynamic movements in vivo. J Shoulder Elbow Surg. 2001;10:260-277.
23
PASSIVE VS. ACTIVE MOVEMENT
•
•
•
•
Ebaugh DD, McClure PW, Karduna AR. Three-dimensional scapulothoracic motion during active and passive arm elevation. Clin Biomech. 2005;20:700-709.
Depression & Ant Tilt Pec Minor & Serratus Ant
Depression & Post Tilt Low Trap
Scapular Abd Serratus Ant & Pec Minor
Scapular Add Rhomboids & Mid & Low Trap
Scapular Control
Eckenrode BJ, Kelley MJ, Kelly JD. Anatomic and biomechanical fundamentals of the thrower shoulder. Sports Med Arthorsc Review. 2012;20:2-10.
24

12/10/20
7
CAUSED BY STRUCTURAL OR MUSCULAR COMPONENTS
STRUCTURAL
••
•
•
McClure PW, Michner LA, Sennett BJ, Karduna AR. Direct 3-dimensional measurement of scapular kinematics during dynamic movements in vivo. J Shoulder Elbow Surg. 2001;10:260-277.
Endo K, Yukata K, Yasui N. Influence of age on scapulo-thoracic orientation.Clin Biomech. 2004;19:1009-1013.
Borsa PA, Laudner KG, Sauers EL. Mobility and stability adaptations in the shoulder of the overhead athlete: a theoretical and evidence-based perspective. Sports Med 2008;38(1):17-36.
Kibler WB. The role of the scapula in athletic shoulder function. Am J Sports Med 1998 March;26(2):325-37.
Kibler WB, McMullen J. Scapular dyskinesis and its relation to shoulder pain. J Am Acad Orthop Surg 2003 March;11(2):142-51.
25
MUSCULAR
• IMPINGEMENT
•
•
•
••
• INHIBITORY PAINFUL CONDITIONS AROUND THE SHOULDER
Kibler WB, McMullen J. Scapular dyskinesis and its relation to shoulder pain. J Am Acad Orthop Surg 2003 March;11(2):142-51.
26
MUSCLE INHIBITION
••
•
Kibler WB. The role of the scapula in athletic shoulder function. Am J Sports Med 1998 March;26(2):325-37.
Effects of FatigueImpingement:
• SA & LT Activity
• UT Activity
Effects of AfflictionImpingement
• SA & LT Activity
• UT Activity
Szucs K1, Navalgund A, Borstad JD. Scapular muscle activation and co-activation following a fatigue task. Med Biol Eng Comput. 2009 May;47(5):487-95.
Struyf F, Cagnie B, Cools A, Baert I, Van Brempt J, Struyf P, Meeus M. Scapulothoracic muscle activity and recruitment timing in patients with shoulder impingement symptoms and glenohumeral instability. J Electromyo Kinesiol 2014; 24(2): 277-284.
27
Found Increased scapular dyskinesia during push-up plus and diagonal shoulder elevation in pts with painful shoulder.
Different muscle activation between middle and lower serratus anterior could represent in group with scapular dyskinesis.
Suggests need for selective activation of the lower serratus anterior in patients with scapular winging and tipping
Park SY, Yoo WG. Activation of the serratus anterior and upper trapezius in a population with winged and tipped scapulae during push-up-plus and diagonal shoulder-elevation. J Back Musculoskelet Rehabil. 2015;28(1):7-12.
28
12/10/20
8
PainGenerator
MotionSegment
NeuromotorControl
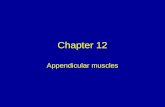
Scapular Activation
§ Low Row
§ Inferior Glide
§ Robbers
Kibler BW et al. Electromyographic analysis of specific exercises for scapular control in early phases of shoulder rehabilitation. Am J Sports Med. 2008;36:1789-98.
IAOM-USSenMoCorTM
29 30
DYNAMIC STABILITY
•••
•
••
•••
•Eckenrode BJ, Kelley MJ, Kelly JD. Anatomic and biomechanical fundamentals of the thrower shoulder. Sports Med Arthorsc Review. 2012;20:2-10.
Borsa PA, Laudner KG, Sauers EL. Mobility and stability adaptations in the shoulder of the overhead athlete: a theoretical and evidence-based perspective. Sports Med 2008;38(1):17-36.Wilk KE, Meister K, Andrews JR. Current concepts in the rehabilitation of the overhead throwing athlete. Am J Sports Med 2002 January;30(1):136-51.
31
SHOULDER FLEXION
FLEXIONRESULTS-
(FEEDFORWARD).
Wattanaprakornkul et al, 2011b
32

12/10/20
9
SHOULDER FEEDFORWARD
MUSCLES
STIMULI EXPECTED UNEXPECTED
RESULTS- PRE-ACTIVATION
DAY et al, 2012
33
SHOULDER FEEDFORWARD
MUSCLESSTIMULI CONCENTRIC ECCENTRIC
RESULTS- PRIOR TOPRIOR TO
REGARDLESS OF DIRECTION
DAVID et al, 2000
34
PainGenerator
MotionSegment
NeuromotorControl
Rotator Cuff Reactivation
§ SL ER
§ SL Flexion
§ Ecc Open Can
Reinold MM, Wilk KE, Fleisig GS, Zheng N, Barrentine SW, Chmielewski T, Cody RC, Jameson GG, Andrews JR. Electromyographic analysis of the rotator cuff and deltoid musculature during common shoulder external rotation exercises. J Orthop Sports Phys Ther. 2004 Jul;34(7):385-94.
Reinold MM, Escamilla RF, Wilk KE. Current concepts in the scientific and clinical rationale behind exercises for glenohumeral and scapulothoracic musculature. J Orthop Sports Phys Ther. 2009 Feb;39(2):105-17.
Cools AM, Dewitte V, Lanszweert F, Notebaert D, Roets A, Soetens B, Cagnie B, Witvrouw EE. Rehabilitation of scapular muscle balance: which exercises to prescribe? Am J Sports Med. 2007 Oct;35(10):1744-51.
IAOM-USSenMoCorTM
35
SENSORIMOTOR CONTROL
REACTIVE
•
•
• “SLOW”
PREPARATORY (ANTICIPATORY)� FEEDFORWARD CONTROL (FF)� PREVIOUS EXPERIENCE
� INTEGRATED WITH ONGOINGINFORMATION
STIFFER
UNCONSCIOUS
Lephart SM, Riemann BL, Fu FH. Introduction to the sensorimotor system. In: Lephart SM & Fu F, eds. Proprioception and Neuromuscular Control in Joint Stability. Champaign, IL: Human Kinetics; 2000.
36

12/10/20
10
Examination
Initial Activation
Progressive Program
TTDPM
Angle Reproduction
Balance Testing
Pain Genera
tor
Motio
n Segment
NeuroM
otor
Control
Somato
senso
ry
Control
Postural Control Assessment
Fundamental Activation
Reflex Ensemble
??????
Relocation Training
Balance Ensemble
Postural Training
37
SHOULDER COMPLEX AS AN SUPPORTER / PLACER•••
•
The Shoulder Complex is at the BASE of the UQ Sensorimotor Control Universe!!!!
38
SHOULDER KINESIS SOMATOSENSORY FUNCTION
Due to its unconstrained nature, the glenohumeral joint must necessarily have several mechanisms to regulate its position in space
Guanche CA, Noble J, Solomonow M, Wink CS. Periarticular neural elements in the shoulder joint. Orthopedics. 1999 Jun;22(6):615-7.
39
SOMATOSENSORY (FEEDBACK) SYSTEMS:
SOMATOSENSORY FUNCTION / DYSFUNCTION
••
•
•
40

12/10/20
11
SOMATOSENSORY (FEEDBACK) SYSTEMS:PROPRIOCEPTION
• SALLES ET AL, 2013
• TENG CC, CHAI H, LAI DM ET AL 2007
• SUPRAK, 2011
• WASSINGER F ET AL 2007
Proprioception : Influenced by?ú Neoprene sleeve Ulker et al, 2004
ú CryotherapyWassinger CA, et al 2007
ú Starting Position Ulker et al, 2004
ú Blunt Trauma Morgan & Herrington 2014
41
SHOULDER REFLEX REACTIVATION
•• REFLEX ACTIVATION
••
••
Huxel et al, 2008
42
SHOULDER IMPINGEMENT
•
•
•
•
SHOULDER PROPRIOCEPTION
Machner et al, 2003
Maenhout et al, 2012Bandholm et al, 2006
Machner et al, 2003
ROTATOR CUFF DISORDERS
•
•
•
Anderson & Wee, 2011
Martins et al, 2012
Anderson & Wee, 2011
Roy et al, 2008
43
PainGenerator
MotionSegment
NeuromotorControl
SomatosensoryControl
IAOM-USSenMoCorTM
§ Proprioception
ú TTDPM
ú JRE
§ Reflex
Reactivation
§ Closed Chain Response
§ Balance
44

12/10/20
12
PainGenerator
MotionSegment
NeuromotorControl
SomatosensoryControl
IAOM-USSenMoCorTM
§ Proprioception
ú TTDPM
ú JRE
§ Reflex
Reactivation
§ Closed Chain Response
§ Balance
45
Pain Genera
tor
Motio
n Segment
NeuroM
otor
Control
Somato
senso
ry
Control
Upper Quarter Functional Examination (UQFE)
IDENTIFY MOVEMENT DYSFUNCTIONS•
•
•
•
46
THE UQFE
• STATICTESTS
••••
§ Functionally Available PROMú Supine 90/90 IR-ER
ú Supine Sh Flex & ABD ú Standing Elevation x 3
§ Muscle Length / Elongationú Lateral Rotator Length
ú Pec Minor Lengthú Elbow Flexor Lengthú Lat Length
§ Functional Mvmnt Patternsú A. Sh Flexion (standing)
ú A. Sh ABD (standing)ú A. Sh IR-ER (standing)ú A. Sh IR-ER (prone)
§ Muscle Recruitmentú Posterior Deltoid
ú Lower Traps ú Middle Traps
47
THE UQFE
STATIC TESTS
• CERVICAL
• FRONTAL PLANE
• SAGITTAL PLANE
DYSFUNCTIONS:
•
•
•
Static Tests
§ Humeral
ú Translation
ú Rotation
Dysfunctions:
§ Ant vs. Post glide
§ IR’d vs. ER’d
48

12/10/20
13
THE UQFE
STATIC TESTS
• SCAPULA
• FRONTAL
• SAGITTAL
• TRANSVERSE
DYSFUNCTIONS:
••
•••
Static Tests
§ Thoracic
ú Sagittal ú Frontal
Dysfunctions:§ Dec’d or Inc’d Kyph
§ (L) vs. (R) Lat Shift
49
THE UQFE
FUNCTIONALLY AVAILABLE PROM
•
DYSFUNCTIONS:
••••
50
THE UQFE
FUNCTIONALLY AVAILABLE PROM
•
DYSFUNCTIONS:
••
•
51
THE UQFE
FUNCTIONALLYAVAILABLE PROM•
DYSFUNCTIONS:•••••
52

12/10/20
14
THE UQFE
MUSCLE LENGTH / ELONGATION
•
DYSFUNCTIONS:
•
53
THE UQFE
MUSCLE LENGTH / ELONGATION
•
•
DYSFUNCTIONS:
••
54
THE UQFE
FUNCTIONAL MVMNT PATTERNS
•
DYSFUNCTIONS:
•••
••
55
THE UQFEFUNCTIONAL MVMNT PATTERNS
•
DYSFUNCTIONS:
•••
••
56

12/10/20
15
THE UQFE
FUNCTIONAL MVMNT PATTERNS
•
DYSFUNCTIONS:
••
•
57
THE UQFE
FUNCTIONAL MVMNT
PATTERNS
•
DYSFUNCTIONS:
•••
58
THE UQFE
MUSCLE RECRUITMENT
•
DYSFUNCTIONS:
•
•
•
59
THE UQFE
MUSCLE RECRUITMENT
••
DYSFUNCTIONS:
•••
•
60

12/10/20
16
THE UQFE
MUSCLE RECRUITMENT: ALL-4’S SERRATUSACTIVATION
FOUNDATION:
• COMPONENTS:
61
Pain Genera
tor
Motio
n Segment
NeuroM
otor
Control
Somato
senso
ry
Control
Upper Quarter Functional Examination (UQFE) Lite
Fundam
ental
Perform
ance
CORRECTIVE STRATEGIES• Mobility• Scapulothoracic• Glenohumeral
62
PainGenerator
NeuromotorControl
SomatosensoryControl
FundamentalPerformance
IAOM-USSenMoCorTM
Correctives: Mobility Dysfunction
• Thoracic Spine
• Latissimus Dorsi
• Pec Minor
• Posterior Shoulder
M otionSegment
Wilk KE, Hooks TR, Macrina LC. The modified sleeper stretch and modified cross-body stretch to increase shoulder internal rotation range of motion in the overhead throwing athlete. J Orthop Sports Phys Ther. 2013 Dec;43(12):891-4.
63
PainGenerator
MotionSegment
NeuromotorControl
SomatosensoryControl
FundamentalPerformance
IAOM-USSenMoCorTM
Correctives: Scapular Protraction Training
• All 4’s 2 arms
• All 4’s 1 arm
• Low Plank
• Banded Low Plank
64
12/10/20
17
PainGenerator
MotionSegment
NeuromotorControl
SomatosensoryControl
FundamentalPerformance
IAOM-USSenMoCorTM
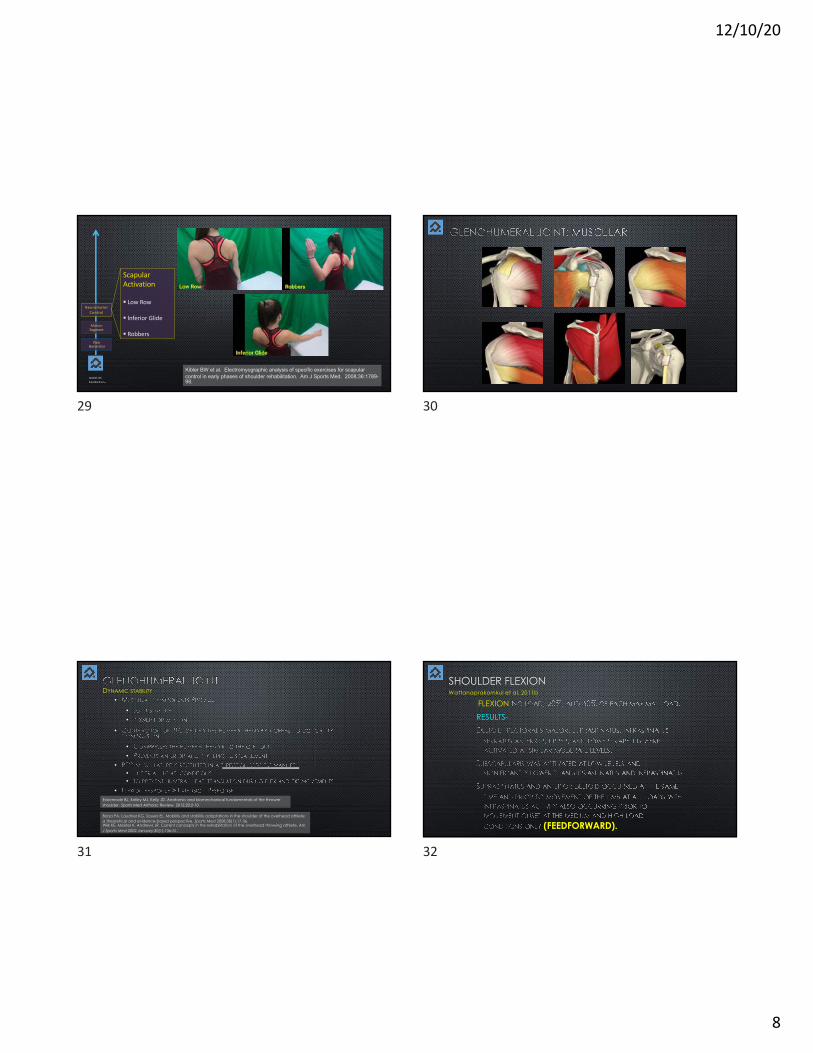
Correctives: Scapulothoracic Integration
• Manual Packing
• SL Packing
• All 4’s Pack/Rot
65
PainGenerator
MotionSegment
NeuromotorControl
SomatosensoryControl
FundamentalPerformance
IAOM-USSenMoCorTM
Correctives: Overhead Training
• Y-Wall Slides• Serratus Ant• Lower
Trapezius
• Landmine
66
PainGenerator
MotionSegment
NeuromotorControl
SomatosensoryControl
Advanced Performance
FundamentalPerformance
IAOM-USSenMoCorTM
Composite MovementsUpper Quarter (UQ)Lower Quarter (LQ)
Fundamental Movements
• Hinge• Squat• Lunge• Push
• Pull• Twist• Ambulation
Whole Body Movement
Patient Specific Rotatory
67
PainGenerator
MotionSegment
NeuromotorControl
SomatosensoryControl
Advanced Performance
FundamentalPerformance
Functional Advancement Log Splitting
§ Maul Swingú Elevation Chainú Thoracic Ext/Rotú Lumbar Neutralú Hinge (drive
w/Hips)
ú Stable BOS
https://www.ochsenkopf.com/en/magazine/chopping-wood-right/
68

12/10/20
18
FUNCTIONAL MANAGEMENTEXAM à PRESCRIPTION
•PROGRESSION:
Structural Mgmnt Functional Mgmnt
69
GOAL: PERFORMANCE ENHANCEMENT Preliminary:
Clinical Examination / Structural Diagnosis
Functional Examination / Functional Diagnosis
Manage Pain/Dysfunction
Fundamental Activation
Dx Specific Dx Inclusive Client Specific
OMTBiopsychosocial-Interpersonal Management
GOAL: PAIN MANAGEMENTPreliminary:
Biopsychosocial Assessment
FUNCTIONAL SCREENMEDICAL SCREEN
Composite Training
Corrective Strategies
SenMoCORTM
Pain G
enerato
r M
otion Segm
entNeuro
Moto
r
Control
Somato
senso
ry
Control
Advanced
Perform
ance
Functi
onal
Advance
ment
Fundam
ental
Perform
ance
70
•
••
•
•
IAOM-US
QUESTIONS or COMMENTS?
71