Upper genitourinary trauma Dr. Ibrahim alabdulaali Urology RKH.
82
Upper genitourinary trauma Dr. Ibrahim alabdulaali Urology RKH
-
Upload
homer-gilmore -
Category
Documents
-
view
217 -
download
2
Transcript of Upper genitourinary trauma Dr. Ibrahim alabdulaali Urology RKH.

Upper genitourinary trauma
Dr. Ibrahim alabdulaaliUrology
RKH

Approximately 10% of injuries involve the genitourinary tract ; with the kidney being the most commonly injured organ.
Only 2% of injuries involve the genitourinary tract alone .

Renal injury History: AMPIL A : allergies M : medications P : past history I : environment mechanism of injury
with its details ( most important is deceleration injury )
L : last meal

Examination: BP Fractures (lower ribs and upper lumbar
and lower thoracic vertebrae ) Flank ecchymosis Exit & entry wounds
Hematuria is the best indicator of traumatic urinary system injury. However, the degree of hematuria and the severity of the renal injury do not correlate consistently .

in up to 36% of renal vascular injuries from blunt trauma, hematuria is absent

Renal injury


segmental renal artery or vein injury is included in grade IV.
shattered kidney = multiple grade IV–type lacerations, but some authors have used grade V classification to report more than one laceration of any parenchymal depth.

Classification of renal injury

Indications for Renal Imaging all blunt trauma patients with gross
hematuria and those patients with microscopic hematuria (5 RBCs/HPF) and shock (systolic blood pressure of less than 90 mm Hg any time during evaluation and resuscitation) should undergo renal imaging, usually CT with intravenous contrast.
Those patients with microscopic hematuria without shock can be followed up clinically without imaging studies.

Indications for Renal Imaging
However, should one suspect any possible renal injury on the basis of history or examination, imaging should be performed; for example, patients sustaining blunt trauma from rapid deceleration are at risk for vascular injury, which can occur in the absence of microscopic hematuria.
Penetrating injuries with any degree of hematuria should be imaged.

Indications for Renal Imaging
All pediatric patients (younger than 16 years) sustaining blunt renal trauma must have an imaging study regardless of the degree of hematuria.

Imaging Studies The preferred imaging study for renal
trauma is contrast-enhanced CT. CT provides the most definitive staging
information: parenchymal lacerations are clearly defined; extravasation of contrast-enhanced urine can easily be detected associated injuries to the bowel, pancreas, liver, spleen, and other organs can be identified; and degree of retroperitoneal bleeding can be assessed by the size and dimensions of the retroperitoneal hematoma. Lack of contrast uptake in the parenchyma suggests arterial injury.

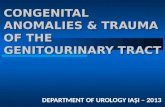
right renal stab wound (grade IV),

Imaging Studies
Findings on CT that suggest major injury are
(1) medial hematoma, suggesting vascular injury.
(2) medial urinary extravasation, suggesting renal pelvis or ureteropelvic junction avulsion injury.
(3) lack of contrast enhancement of the parenchyma, suggesting arterial injury.

Injury of Renal Artery

One major limitation of CT is the inability to define a renal venous injury adequately.
With normal arterial perfusion, the parenchyma appears normal and the collecting system may contain contrast material. A medial hematoma accompanying the preceding findings strongly suggests a venous injury.

Imaging Studies single-shot intraoperative excretory
urography indicated when the surgeon encounters an unexpected retroperitoneal hematoma surrounding a kidney during abdominal exploration.
only a single film is taken 10 minutes after intravenous injection of 2 mL/kg of contrast material. If findings are not normal or near normal, the kidney should be explored to complete the staging of the injury and reconstruct any abnormality found.

Shattered kidney

Arteriography is largely used to define arterial injuries suspected on CT or to localize arterial bleeding that can be controlled by embolization.

Nonoperative Management A hemodynamically stable patient with an
injury well staged by CT can usually be managed without renal exploration.
98% of renal injuries can be managed nonoperatively.
Grade IV and V injuries more often require surgical exploration, but even these high-grade injuries can be managed without renal operation if they are carefully staged and selected.
Penetrating trauma from gunshot or stab wounds to the kidney can be managed nonoperatively if carefully staged with CT.
.

Patients with high-grade injuries (grades III to V) selected for nonoperative management should be observed closely with serial hematocrit readings and abdominal CT scans. Should bleeding persist or delayed bleeding occur, angiographic studies with embolization of bleeding vessels often suffice and obviate surgical intervention.

Patients with grade IV parenchymal lacerations who have well-contained hematomas can be observed expectantly.
If urinary extravasation is present, serial renal CT scanning should be instituted. If significant urinary extravasation persists beyond 48 hours, placement of an internal ureteral stent for drainage often prevents prolongation of the extravasation and decreases the chance of perirenal urinoma formation.


Nonoperative Management If nonoperative management is selected
in a patient with gross hematuria whose injury has been well staged with appropriate imaging, hospital admission and bed rest are required. Once the gross hematuria clears, ambulation is allowed.
Ambulation without any sequelae allows hospital discharge with close clinical follow-up.

Operative Management Indications for renal exploration after trauma
can be separated into absolute and relative. Absolute indications include evidence of
persistent renal bleeding, expanding perirenal hematoma and pulsatile perirenal hematoma.
Relative indications include urinary extravasation, nonviable tissue, delayed diagnosis of arterial injury, segmental arterial injury, and incomplete staging.

Operative Management Urinary extravasation alone from a
grade IV parenchymal laceration or forniceal rupture can be managed nonoperatively with an expectation of spontaneous resolution in 87.1% of patients (Matthews et al, 1997).
combination of relative indications necessitates renal exploration.

Operative Management Surgical exploration of the acutely injured
kidney is best done via a transabdominal approach.
Renal vessels are isolated before exploration to provide the immediate capability to occlude them if massive bleeding accurse once Gerota's fascia is opened.
The procedure for renal reconstruction after trauma includes complete renal exposure, débridement of nonviable tissue, hemostasis by individual suture ligation of bleeding vessels, watertight closure of the collecting system, and coverage or approximation of the parenchymal defect .

surgical approach The transverse colon is lifted superiorly,
and the small bowel is lifted superiorly and to the right. This exposes the midretroperitoneum. An incision is made over the aorta in the retroperitoneum just superior to the inferior mesenteric artery. The incision is extended superiorly to the ligament of Treitz.


Large hematomas may extend over the aorta and obscure the landmarks for the planned initial retroperitoneal incision. In such instances, the inferior mesenteric vein can be used as an anatomic guide for an appropriate incision. By making the retroperitoneal incision just medial to the inferior mesenteric vein and dissecting through the hematoma, the anterior surface of the aorta can be identified and followed superiorly to the crossing left renal vein.

The kidney is exposed by incising the peritoneum lateral to the colon, followed by mobilization off Gerota's fascia.
Gerota's fascia is then opened and the kidney with injury is completely dissected from the surrounding hematoma. Should troublesome bleeding develop, the previously isolated vessels can be temporarily occluded with a vascular clamp or a vessel loop tourniquet.

Renal reconstruction

Operative Management Renorrhaphy denotes repair of a
parenchymal laceration, involves complete exposure of the kidney, débridement of nonviable tissue, hemostasis obtained with absorbable 4–0 chromic sutures on bleeding vessels, closure of the collecting system, and approximation of the margins of the laceration (3–0 absorbable suture) with the use of renal capsule and Gelfoam bolster.

Renorrhaphy

Renorrhaphy

Renorrhaphy

Operative Management When polar injuries cannot be
reconstructed, a partial nephrectomy should be done .
Drains should be used liberally in these repairs.
perforated main renal vessels injured by penetrating trauma can be repaired with 5–0 nonabsorbable vascular suture using vascular clamps to occlude the involved vessel.


Operative Management In case of main renal artery thrombosis;
Prompt diagnosed by CT or angiography should lead to immediate renal exploration in appropriate candidates in an attempt to salvage the kidney.
the area of injury should be excised and a replacement graft done, preferably with hypogastric or splenic artery .
Most of these patients end up by nephrectomy .

With delayed diagnosis (xs>8 hours), the kidney typically cannot be salvaged .
Segmental renal arterial injuries result in ischemic infarction to a segment of the kidney. These should be observed nonoperatively unless associated with a parenchymal laceration. Should the laceration with infarction be greater than 20% of the parenchyma, careful consideration should be given to surgical correction.

Operative Management
Total nephrectomy is immediately indicated in extensive renal injuries or when the patient's life would be threatened by attempted renal repair .
Segmental venous injuries are best managed by ligation of the vessel.

Damage Control
The wound and area around the injured kidney are packed with laparotomy pads to control bleeding with a planned return in 24 hours to explore and evaluate the extent of injury.
It may well be useful in managing complex renal injuries to avoid total nephrectomy.

Complications Persistent urinary extravasation can result
in urinoma, perinephric infection, and renal loss; treated by ABx and if persist, placement of an internal ureteral stent often corrects the problem.
Delayed renal bleeding managed by bed rest and hydration and if persist angiography to localize the bleeding vessel, and embolization can often gain control .

Complications Perinephric abscess rarely occurs after
renal injury and treated by Percutaneous drainage which offers a good initial method of management, followed by surgical drainage if necessary.
Hypertension secondary to (1) renal vascular injury; (2) compression of the renal parenchyma with extravasated blood or urine; and (3) post-trauma arteriovenous fistula.

Uretral trauma

Etiology
Iatrogenic Traumatic

Etiology
(Dobrowolski et al) in Poland. identified 452 ureteral injuries. Of these,340 (75%) were iatrogenic, 81 (18%) were from blunt trauma, and 31 (7%) were from penetrating trauma.
Of the 340 iatrogenic injuries, 247 (73%) were gynaecological in origin, 46 (14%) were general surgical and 47 (14%) were urological.

Etiology
External Trauma Rare, occurring in less than 4% and 1% of
penetrating and blunt traumas, respectively. These patients often have significant associated
injuries and a devastating mortality rate that approaches 33%
Ureteropelvic junction disruption after blunt trauma is rare and can be missed because patients often do not exhibit hematuria and the injury is difficult to palpate during intraoperative manual examination, So an intraoperative "one-shot" intravenous pyelogram is recommended in patients with hypotension or a history of significant deceleration, despite absence of gross hematuria .

American Association for the Surgery of Trauma Organ Injury Severity Scale for the Ureter

Diagnosis
Suspicion (hematuria absent in 30%) The most common signs are fever,
leukocytosis, and local peritoneal irritation.
Intraoperative Recognition . Methylene Blue

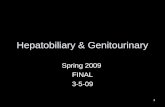
right medial extravasation of contrast material in a patient with a renal pelvis laceration.

Imaging Studies
Excretory Urography : Signs of upper tract obstruction, extravasation, delayed function and ureteral dilation or deviation.
Computed Tomography . Retrograde Ureterography :used to
delineate the extent of injury seen on CT or excretory urography if further clinical information is needed.

I.V.U

Management

External Trauma Ureteral contusions often heal with
stricture or break down later if microvascular injury results in ureteral necrosis.
Minor ureteral contusions can be treated with stent placement.
Severe or large areas of contusion should be treated with excision and ureteroureterostomy.
Repair must be meticulous sticking to certain general principles to increases the success rate and to avoid complications.

External Trauma
Principles of Ureteroureterostomy :1. Mobilize the injured ureter.2. Débride the ureter until the edges bleed.3. spatulated, tension-free, stented
watertight anastomosis. 4. place retroperitoneal drain.
5. Consider omental interposition.


External Trauma Ureteroureterostomy in injuries to the
upper two thirds of the ureter, is common and has a reported success rate as high as 90%.
Complications, usually urinary leakage, occur in 10% to 24%. Other acute complications include abscess and fistula. Chronic complications, usually ureteral stenosis, are less common, occurring in 5% to 12%.

External Trauma Rarely, nephrectomy is required to treat
ureteral injury after external violence. Reasons include severe associated visceral injuries, severe injury to the ipsilateral kidney when renal repair is not possible, poor renal function, severe panureteral injury, or persistent ureteral fistula despite previous intervention.

Upper Ureteral Injuries Ureteroureterostomy Reimplantation of the ureter into the
renal pelvis in case of Ureteral avulsion or very proximal ureteral injury.
Ureterocalycostomy when there is profound damage to the renal pelvis and ureteropelvic junction.
Autotransplantation used in profound ureteral loss or multiple failed attempts at repair.
Ileal Interposition.

Midureteral Injuries
Ureteroureterostomy Transureteroureterostomy, A rarely
used but often (97%) successful surgery that involves bringing the injured ureter across the midline through a retroperitoneal window above the level of the inferior mesenteric artery and anastomosing it end-to-side to the uninjured ureter.

Midureteral Injuries
Transureteroureterostomy Used in middle or distal ureteral injury,
where ureteroureterostomy or bladder flap/hitch repair is impossible.
Some authors feel this operation is contraindicated in patients with a history of urothelial cancer or calculi.



Lower Ureteral Injuries
Ureteroneocystostomy used to repair distal ureteral injuries that
are so close to the bladder. Steps in ureteroneocystostomy include
creation of a submucosal tunnel and the new ureteral orifice is constructed with interrupted 6–0 monofilament absorbable sutures in a watertight and nonobstructing fashion. The repair should be stented postoperatively.

Lower Ureteral Injuries Psoas bladder hitch
Prevents tension on the reimplanted ureter and carries a successful rate of 95%.
Boari flap Injuries to the lower ureter with long
ureteral defects (too long to be bridged by bringing the bladder up in the psoas hitch procedure) in which a pedicle of bladder is swung cephalad and tubularized to bridge the gap to the injured ureter.

Psoas bladder hitch


Ureteral Injuries
Partial Transection Primary repair of a partial transection is used in
the majority of patients. Principles include spatulated, watertight closure
with interrupted or running 5–0 or 6–0 absorbable monofilament.
The ureteral injury is closed by converting a longitudinal laceration into a transverse one, so as not to narrow the ureteral lumen. An internal stent and retroperitoneal drain are placed.

Damage Control.
(1) do nothing, but plan a reoperation when the patient is more stable, usually within 24 hours .
(2) place a ureteral stent and do nothing else.
(3) exteriorize the ureter. (4) tie off the ureter and plan
percutaneous nephrostomy .

Surgical Injury
Ligation Ligation of the ureter should be treated by
removal of the ligature or surgical clip and assessing the viability of the ureter.
If viable ureter placing an internal ureteral stent is advisable.
When viability is in question, ureteroureterostomy should be performed.

Surgical Injury
Immediately recognized Transection
Ureteral injuries are recognized intraoperatively in approximately 34% of patients undergoing open operation.
treated as for ureteral injury after external violence, usually by ureteroureterostomy.

Ureteral injuries that occur during vascular graft surgery are a special case.
Intraoperative management of these injuries is debated and can uncommonly include nephrectomy, if the patient has an adequately functioning contralateral kidney, versus primary ureteroureterostomy with isolation of the repair with omentum .

Surgical Injury Post op. recognition of Transection
Repair of these delayed-recognition injuries is controversial.
If transection recognized within the first 7 to 10 days post op. and no infection, abscess, or other complications exist, immediate reexploration and repair are indicated.
If transection recognized late or if the patient has significant complications, proximal urinary diversion by nephrostomy tube should be consedered.

Surgical Injury Some authors are going with DJ
stenting, but this is possible in only 20% to 50%. When stenting is possible, they reported an ultimate success rate as high as 73% without the need for open surgery. If retrograde DJ stenting failed PCN and a trail of antegrade DJ stentin is tried.
Remove the stent in 6 to 8 weeks and do a retrograde pylogram or nephrostogram and if there is still a leak or a stricture go for open repair.

Surgical Injury If DJ stenting is not possible, insert PCN
and allow several months for complete wound healing and attempt open repair.
Ureteroscopic Injury Ureteral avulsion during ureteroscopy is
treated in the same manner as ureteral injuries in open surgery.
Ureteral perforation can be treated by ureteral stenting.

Ureteroscopy attempting to retrieve a miduretral stone resulted in perforation. Note extravasation of contrast medium in the periureteric space as well as lateral deviation of the ureter, indicating the presence of a urinoma.