Updates onCorneal Disclosures Cross‐Linking & MyopiaControl...Spadea L, et al. Corneal stromal...
24
6/2/2019 Daniel G. Fuller, OD, FAAO Dipl, FSLS Chief, Cornea Contact Lens Service Supervisor, Cornea Contact Lens Refractive Surgery Residency The Eye Center, Southern College of Optometry Updates on Corneal Cross‐Linking & Myopia Control Fuller, 2019 (COPE# 61275‐AS) Disclosures • Dr. Fuller – provides statistical support for a non‐funded, independent clinical evaluation of a CXL device • Educational consultant to • Alcon, • Allergan, • B+L, • Cooper Vision and • JJV Fuller, 2019 (COPE# 61275‐AS) Part 1: Objectives Fuller, 2019 (COPE# 61275‐AS) • Toclarify the underlying principles • Tocritically review the scientific literature • Toprovide an update on these technologies • To guide selection of the appropriate candidates • To assist in identifying and managing potential adverse events or loss of efficacy • Toguide the integration of these technologies into practice What is CXL? • Collagen fibrils branch and extend limbus to limbus • Cross‐linking occurs between fibrils in the same lamellar layer • Provides biomechanical stability Fuller, 2019 (COPE# 61275‐AS) 1 2 3 4
Transcript of Updates onCorneal Disclosures Cross‐Linking & MyopiaControl...Spadea L, et al. Corneal stromal...

6/2/2019
Daniel G. Fuller, OD, FAAO Dipl, FSLSChief, Cornea Contact Lens Service
Supervisor, Cornea Contact Lens Refractive Surgery Residency The Eye Center, Southern College of Optometry
Updates on Corneal Cross‐Linking & Myopia Control
Fuller, 2019 (COPE# 61275‐AS)
Disclosures
• Dr. Fuller – provides statistical support for a non‐funded, independent clinical evaluation of a CXL device
• Educational consultant to• Alcon,• Allergan,• B+L,• Cooper Vision and• JJV
Fuller, 2019 (COPE# 61275‐AS)
Part 1: Objectives
Fuller, 2019 (COPE# 61275‐AS)
• To clarify the underlying principles• To critically review the scientific literature• To provide an update on these technologies• To guide selection of the appropriate candidates
• To assist in identifying and managing potential adverse events or loss of efficacy
• To guide the integration of these technologies into practice
What is CXL?
• Collagen fibrils branch and extend limbus to limbus
• Cross‐linking occurs between fibrils in the same lamellar layer
• Provides biomechanical stability
Fuller, 2019 (COPE# 61275‐AS)
1 2
3 4

6/2/2019
Man‐made
• Polymer chemistry uses –this is responsible for some of the differences in modulus in SiHy lenses
• Reduction in biodegradation – collagen‐based bioprosthesis
https://www.medtronic.com/us‐en/healthcare‐professionals/products/cardiovascular/heart‐valves‐surgical/hancock‐ii‐hancock‐ii‐ultra‐bioprostheses.html
Fuller, 2019 (COPE# 61275‐AS)
Natural
Fuller, 2019 (COPE# 61275‐AS)
• Advanced glycation endproducts (AGE’s)– age & DM (prevent or decrease severity of KCN)
• Photo‐oxidative CXL – UV & ionizing radiation
• Enzymatic CXL – lysyl oxidase; a deficiency can lead to Ehlers‐Danlos; maybe a gene defect in KCN
• Non‐enzymatic CXL –glutaraldehyde; formaldehyde; diphenylphosphoryl; nitroalcohole; genipin
Initial Candidates
• Primary corneal ectasias• Keratoconus• Pellucid marginal degeneration
• Must demonstrate progression
• Age cut‐off is arguable• Secondary corneal ectasias
• LASIK/PRKFuller, 2019 (COPE# 61275‐AS)
Potential Candidates
• Off‐label• Combined procedures – with LASIK, INTACS, and cataract procedures
• PiXL – treat low amounts of myopia without LASIK
• Microbial keratitis – sterilize the wound
• Sclera – to strengthen grafts or melts
• Corneal dystrophies – Fuch’sand other Fuller, 2019 (COPE# 61275‐AS)
5 6
7 8

6/2/2019
Physical Properties
Fuller, 2019 (COPE# 61275‐AS)
CXL Process• Photochemical process• Non‐thermal• Comparison to photocoagulation
• Photocoagulation – 630 W/cm2
• Photochemical – 3 mW/cm2
• M◦aximum temp. increase of2‐
UV Spectrum• Ultraviolet spectrum
• UVA – 320‐400 nm• UVB – 280‐320 nm• UVC – 180‐280 nm
3 CMencucci R1, Mazzotta C, Rossi F, Ponchietti C, Pini R, Baiocchi S, Caporossi A, Menchini U. Riboflavin and ultraviolet A collagen crosslinking: in vivo thermographic analysis of the corneal surface.J Cataract Refract Surg. 2007 Jun;33(6):1005‐8.
Absorption of UVA/Emittance
• Riboflavin has two peak absorption maxima
• 375nm• 445nm
• Emits fluorescence at 534nm
Lombardo, M et al. Interaction of ultraviolet light with the cornea: Clinical implications for corneal crosslinking. J Cataract Ref Surg. 2015; 41(2):446‐459.
Fuller, 2019 (COPE# 61275‐AS)
Absorption of UVA
Fuller, 2019 (COPE# 61275‐AS)
• RF 0.1% sol.• Selected for an average KCN pach of 400 microns• Biomechanical effect is independent of concentration over a large area
• Higher conc. actually reduce CXL effect• Produces a large absorption coefficient of 90% in the stroma protecting the endothelium, lens and retina.
• 65% absorbed in the first 200 microns
Tissue Changes
Fuller, 2019 (COPE# 61275‐AS)
• Increase in modulus and firmness by a factor of 1.7x
• Increase in shrinkage temp. from 63◦C to 70◦C
• Decrease in swelling percentage• Increase in collagen fibril thickness by 4.5%
• Increased resistance to collagenase• Creation of molecular aggregates with higher molecular weights
• Decrease in permeabilityWollensak G1, Spoerl E, Seiler T. Stress‐strain measurements of human and porcine corneas after riboflavin‐ultraviolet‐A‐induced cross‐linking. J Cataract RefractSurg.2003 Sep;29(9):1780‐5.
9 10
11 12

6/2/2019
Cellular Changes
Fuller, 2019 (COPE# 61275‐AS)
• Epithelial cells• Epi‐off – cells grow back in 3‐4 days• Normal thickness at 3 to 6 months• Intact epithelium protects limbal stem cells
•Keratocytes• Increases apoptosis in first 250‐300 microns• New cells migrate from periphery• Alterations occur up to 36 mos.
Wollensak G1, Spoerl E, Reber F, Seiler T Keratocyte cytotoxicity of riboflavin/UVA‐treatment in vitro. Eye (Lond). 2004 Jul;18(7):718‐22.
Histological changes in human cornea after cross‐linkingwith riboflavin and ultravioletA
Acta Ophthalmologica Volume 88, Issue 2, pages e17‐e18, 23 APR 2009 DOI: 10.1111/j.1755‐3768.2008.01474.xhttp://onlinelibrary.wiley.com/doi/10.1111/j.1755‐3768.2008.01474.x/full#f1
Epithelium
Fuller, 2019 (COPE# 61275‐AS)
250 microns
Endo.
From: Collagen Cross-Linking Using Rose Bengal and Green Light to Increase Corneal StiffnessInvest. Ophthalmol. Vis. Sci.. 2013;54(5):3426-3433. doi:10.1167/iovs.12-11509
Figure Legend:Keratocytes in cornea after photo-cross-linking. (A, B) RB was applied to cornea and exposed to 100 or 200 J/cm2 green light (A)
or kept in dark (B). (C, D) Riboflavin/dextran was applied to cornea and exposed to 8.7 J/cm2 UVA (C) or kept in dark (D). Corneas were cultured for 24 hours then fixed, paraffin-embedded, and H&E-stained. (E) Cells in stroma of corneas treated with RB, then with 100 or 200 J/cm2 green light or kept in dark. Only cells in most anterior stroma (200 μm) on section were counted. (F) Cells in corneas treated with riboflavin, then with 8.7 J/cm2 UVA or kept in dark. Cells to a depth of 500 μm on the sections were counted. n= 3 to 4 cornea for each treatmentcondition.
Fuller, 2019 (COPE# 61275‐AS)The Association for Research in Vision and Ophthalmology Copyright © 2015. All rights reserved. Date of download: 6/10/2015
Cellular Changes
Fuller, 2019 (COPE# 61275‐AS)
•Endothelial cells• Statistically non‐significant reduction• Density and morphology unchanged at 1 year• Threshold for damage is 0.35 mW/cm2 ; exposure levels are 0.18 mW/cm2
• Assuming a 400 micron thick or greater cornea
Wollensak G1, Spörl E, Reber F, Pillunat L, Funk R. Corneal endothelial cytotoxicity of riboflavin/UVA treatment in vitro. Ophthalmic Res. 2003 Nov‐Dec;35(6):324‐8.
13 14
15 16

6/2/2019
Cellular Changes
•Nerves• Subepithelialnerve plexusdisappears
• Regenerates after 7 days and is normal by 6 mos.
Fuller, 2019 (COPE# 61275‐AS)Xia Y1, Chai X, Zhou C, Ren Q. Corneal nerve morphology and sensitivity changes after ultravioletA/riboflavin treatment. Exp Eye Res. 2011 Oct;93(4):541‐7.
Cellular Changes
Fuller, 2019 (COPE# 61275‐AS)
• Deeper structures• Lens – protected by the absorption of UVA by RF and cornea
• Retina – also protected by absorption and lack of irradiation being focused in its plane
Riboflavin Used in the US Trials
Fuller, 2019 (COPE# 61275‐AS)
•Riboflavin (vitamin B2) 0.1% sol. – m.w. 376 gm/mol (Photrexa 0.12% / Photrexa Viscous 0.12% with Dextran 20% from Avedro)
• Non‐toxic• Absorbs UVA light• Used to create free radicals which cross‐link the carbonyl groups within and between collagen fibrils in the same lamellae not between lamellae
• There may be some inter‐fibrillar bonds between proteoglycans
Riboflavin Overseas
Fuller, 2019 (COPE# 61275‐AS)
Riboflavin Formula Use Epithelum
MedioCROSS TE
0.25% Riboflavin, 1.2%HPMC, 0.01% BAC
Cross‐linking for keratoconus and corneal
ectasiaOn
MedioCROSSM0.1% Riboflavin, 1.1%
HPMC
Cross‐linking for keratoconus and corneal
ectasiaOff
VibeX Xtra0.22% Riboflavin, Saline,
Isotonic LASIKStromalBed
VibeX Rapid0.1% Riboflavin, Saline,
HPMC Accelerated CXL Off
ParaCel0.25% Riboflavin, HPMC,
BAC Accelerated CXL On
17 18
19 20

6/2/2019
Procedures: Dresden v. AthensBunsen‐Roscoe Law (Intensity x Time=Exposure)
• Dresden protocol• Intensity is 3 mW/cm2
• Treatment time 30 mins. at 2 to 5 min. intervals
• Applied over an 8 mm diameter area to protect limbus, sclera and goblet cells
• Athens protocol• Maximum intensity up to 43 mW/cm2; Treatment time 2 min.
• Typical protocols (Kymionis et al.)
• 9mW/cm2 for 14min• 18mW/cm2 for 7min• May pulse doses
Fuller, 2019 (COPE# 61275‐AS)Kymionis GD, et al. Accelerated versus conventional corneal crosslinking for refractive instability: an update. Curr Opin Ophthalmol. 2017;28:343‐347
Comparison of outcomes
• Outcomes of treatment efficacy• Accelerated CXL – shallower• Conventional CXL – deeper• Regression > with A‐CXL
• Problem• Less available oxygen in accelerated CXL with epi‐on.
• Solution• 30mW Pulsed therapy at 1s intervals of 3‐ 8min; allows O2more time to penetrate
• Demarcation line depth is the measure of treatment efficacy.
epi‐off 3mW/cm2
epi‐on 3mW/cm2epi‐on Ionto. 10mW/cm2
epi‐off 10 mW/cm2
Spadea L, et al. Corneal stromal demarcation line after 4 protocols of corneal crosslinking in keratoconus determined with anterior segment optical coherence tomography. J CataractRef Surg. 2018; 44(5)596‐602.
Fuller, 2019 (COPE# 61275‐AS)
Epithelium‐off Delivery of Riboflavin
• RF 0.1% every 1 to 5 mins. for 30 mins.
• Eliminates the barrier to diffusion presented by the epithelium
• Diffusion achieves a maximum in the anterior stroma at 20 to 30 mins., protecting the endothelium/lens/retina
Fuller, 2019 (COPE# 61275‐AS)
Epithelium‐on (Transepithelial) Delivery of Riboflavin• Improving penetration
• Increase contact time (viscous sol. or ring application)
• Change permeability (pilocarpinewith either BAK and EDTA;tetracaine; hypo‐osmotic riboflavin sol.)
• Dextran inhibits conductancewhen added, whereas 0.01% BACand 0.44% NaCl increase permeability.
• Using a Daya disrupter you canpock‐mark the epithelium improving permeability
Fuller, 2019 (COPE# 61275‐AS)
21 22
23 24

6/2/2019
Direct Application of Riboflavin
• Create a pocket as in Intacs• Inject riboflavin into the pocket or after flap creation in LASIK
Fuller, 2019 (COPE# 61275‐AS)
Iontophoresis Delivery of Riboflavin
Int J Ophthalmol. 2017; 10(5): 717–722.
http://www.eyegatepharma.com/technology/iontophoresis‐delivery‐system/
• Riboflavin in negatively charged• Current is delivered for 5 mins. across the intact epithelium
• CONCLUSION: I‐CXL using 0.1%riboflavin halts keratoconusprogression within 24mo,resulting in a significantimprovement in visual andtopographic parameters.Moreover, the depth of thedemarcation line is similar to thatpreviously reported in standard epithelium‐off CXL procedures.
Fuller, 2019 (COPE# 61275‐AS)
Devices
• Overseas• CBM VEGA X‐linker (Constuzione Strumenti, Oftalmici, FL, IT)
• CCL‐365 (PESCHKEMeditrade GmbH,Huenberg, SW)
• UV‐X (IROC GmbH, Zurich, SW) acquired by Avedro
Fuller, 2019 (COPE# 61275‐AS)
Devices
• United States FDA Trials• Avedro (Waltham, MA) KXL wasthe submission device but UVXused in trials
• 30 min. induction every 2 mins. with Photrexa Viscous or until flare is observed in the AC continues throughout tx.
• 3 mW/cm2 for 30mins.• 5.5 J/cm2 maximum energy density
Fuller, 2019 (COPE# 61275‐AS)
25 26
27 28

6/2/2019
Devices
Fuller, 2019 (COPE# 61275‐AS)
• United States FDA Trials• Selectable apertures deliver beams 7.5 mm, 9.5 mm & 11.5 mm
• Subjective alignment by fluorescence• Touchscreen interface• Internal battery• Delivered through a gantry, upright or supine
• Software lockout ensures operators stay within allowable parameters
Case #1
Fuller, 2019 (COPE# 61275‐AS)
• 17 y.o. w/m with decreasing vision and contact lens intolerance
• Dx with KCN Oct. 2012• Cornea OD: Inf. Temp. scarring; Vogt’s striae; Fleischer’s ring
• Cornea OS: clear• Rapid progression to PK OD Mar. 2015• Referred for trans‐epithelial CXL OS July 2015
MRE 10/8/12 MRE 9/29/14 MRE 6/11/15
‐8.00‐5.25 x140 (20/200) ‐6.00‐12.00 x025 (20/30) ‐7.00‐6.00 x025 (20/30)
‐‐3.25‐325 x095 (20/20) ‐2.75‐2.75 x095 (20/20) ‐1.75‐3.00 x095 (20/20)
54.4/61.5 37.6/39.4 42.7/48.8
42.1/45.3 46.2/48.7 44.0/49.4
Case #1
Fuller, 2019 (COPE# 61275‐AS)
OD Lens History Date BCVA Comments
Rose K 1/11/13 20/30
Synergeyes Clear Kone 1/18/13 20/30
Office visit 6/12/13 Corneal abrasion FTK
Essilor Jupiter 6/19/13 20/30
Surgery OD 5/14 20/30 PK
Synergeyes PS 9/14 20/15
Episode of rejection 3/15 20/20 PF 1% Maintenance
Switch to UltraHealth 6/15 20/20 Not tolerating PS/UH
Valley Contax Cust. Stable Elite 7/15 20/20
54.4/61.5 Kmax 57.9
Fuller, 2019 (COPE# 61275‐AS)
42.1/45.3 Kmax 43.7
29 30
31 32

6/2/2019
37.6/39.4 [9/14] 46.2/48.7 [9/14]42.7/48.8 [6/15] 44.0/49.4 [6/15]
Fuller, 2019 (COPE# 61275‐AS)
Case #2
Fuller, 2019 (COPE# 61275‐AS)
• 21 y.o w/m; applying to the US Navy• Dx: KCN in 2010• Sx: CXL and Intacs Feb 2015• Successfully fit with Custom Stable Elite (Valley Contax) scleral lenses
MRE BCVA Sim K’s‐5.50‐2.75 x070 20/25 46.6/52.0‐6.00‐5.00 x170 20/100 31.60/37.50CS Elite 7.85/15.8 ‐3.50 20/20‐3CS Elite 7.85/15.8 pl‐2.00 x022 20/25+
Case #2
Fuller, 2019 (COPE# 61275‐AS)
Approval granted for the treatment of progressive keratoconus in April 2016• The KXL system and the two photoenhancers,
• Photrexa 0.146% (riboflavin 5’‐phosphate ophthalmic solution)
• Photrexa Viscous 0.146% (riboflavin 5’‐phosphate in 20% dextran ophthalmic solution)
• 12 months results• Reduction in mean Kmax of 1 D
in study 1 and 0.5 D in study 3 compared with increase of 1 D in study 1 and 0.5 D in study 3 in sham-controlled eyes.
• Adverse events included corneal opacity, corneal epithelium defect, corneal striae, dry eye, eye pain, punctate keratitis, photophobia, reduced visual acuity and blurred vision.
Fuller, 2019 (COPE# 61275‐AS)
33 34
35 36

6/2/2019
Overseas Experience
1998 – First CXL in C.G. CarusFUullneri,v2e01r9si(CtyOPHE#o6s1p27i5ta‐AlS,) Dresden, GE.
Primary Keratoconus
Author Follow‐up (mos.) Kmax dec. (D) BCVA’s Inc. lines
Wollensak et al. 2003 3‐47 2.01D in 70% 1.26 lines in 65%
Raiskup‐Wolf et al.2008 6‐72 2.68D in 62% >1 in 53%
Wittig‐Silva et al. 2008 3‐12 1.45D 0.12 LogMAR
Vinciguerra et al. 2009 12 1.35D 0.15 LogMAR
Hersh et al. 2011 48‐60 2.0D >2 in 21.1%
Asri et al. 2011 12 >2.0D in 21.3% 40% improved
Poli et al. 2012 12‐36 No significant trend Significant Improvement
Overseas Experience
Fuller, 2019 (COPE# 61275‐AS)
Secondary Ectasia
Author Follow‐up (mos.) Kmax dec. (D) BCVA’s Inc. lines
Kohlhaas et al. 2005 18 Stable Not recorded
Hafezi et al. 2007 12‐25 Dec. in all Improved in 90%
Vinciguerra et al. 2010 12 2.02D 0.1 LogMAR
Kissner et al. 2011 96 Stable in 60% Stable in 60%
Salgado et al. 2011 12 Not statistically significant Not statistically significant
Hersh et al. 2011 12 1.0D Significantly improved
Meta‐Analysis
Fuller, 2019 (COPE# 61275‐AS)
• Review of efficacy epi‐off KCN or surgical ectasia
Craig JA, Mahon J, Yellowlees A, Barata T, Glanville J, Arber M, Mandava L, Powell J, Figueiredo F. Epithelium‐Off Photochemical Corneal Collagen Cross‐Linkage Using Riboflavin and Ultraviolet A for Keratoconus and Keratectasia: A Systematic Review and Meta‐Analysis. The Ocular Surface 2014;12:202‐214 .
Analysis of epithelium‐off CXL papers by study type Number (%)
Randomized controlled trial 8 (16%)Prospective case series 25 (51%)Prospective comparative case series 4 (8%)Retrospective case series 7 (14%)Case series 5 (10%)
TOTAL N= 49
Final Data Included
• 39 of 49 papers graded as very low quality evidence• Only 46 of 49 papers included efficacy & AE data• Data included for analysis from 40 studies out of these 46 papers
49 papers 46 papers efficacy + AE 40 studies
Fuller, 2019 (COPE# 61275‐AS)
37 38
39 40

6/2/2019
Outcomes Assessed
Craig JA, Mahon J, Yellowlees A, Barata T, Glanville J, Arber M, Mandava L, Powell J, Figueiredo F. Epithelium‐OffPhotochemical Corneal Collagen Cross‐LinkageFuUllesri,n2g01R9ib(oCfOlaPvEin# 6a1n2d75U‐lAtrSa)violet A for Keratoconus and Keratectasia: A Systematic Review and Meta‐Analysis. The Ocular Surface 2014;12:202‐214 .
• Time points 6, 12 and 24 months• Topography– Mean, Max and Min K• Visual acuity – corrected and uncorrected• Refraction• Central corneal thickness (CCT)
Results
Craig JA, Mahon J, Yellowlees A, Barata T, Glanville J, Arber M, Mandava L, Powell J, Figueiredo F. Epithelium‐OffPhotochemical Corneal Collagen Cross‐LinkageFuUllesri,n2g01R9ib(oCfOlaPvEin# 6a1n2d75U‐lAtrSa)violet A for Keratoconus and Keratectasia: A Systematic Review and Meta‐Analysis. The Ocular Surface 2014;12:202‐214 .
Topography• Changing up to 12 mo.• Mean and Max K’s –Reduction of 1.00D
• Min K – reduction of 0.75 D
Visual Acuity Results• Statistically significant improvement at all time periods
• UCVA improved more than BCVA Maintained over time
Results
Craig JA, Mahon J, Yellowlees A, Barata T, Glanville J, Arber M, Mandava L, Powell J, Figueiredo F. Epithelium‐OffPhotochemical Corneal Collagen Cross‐LinkageFuUllesri,n2g01R9ib(oCfOlaPvEin# 6a1n2d75U‐lAtrSa)violet A for Keratoconus and Keratectasia: A Systematic Review and Meta‐Analysis. The Ocular Surface 2014;12:202‐214 .
Refraction• Statistically significant improvement in cylinder (approx. 0.50 D)
• Stable by 12 mo. and stable thereafter
• Statistically significant improvement in spherical equivalent
Central Pachs• Statistically significant decrease in central corneal thickness of approx. 0.14 microns
Summary Adverse Events
Fuller, 2019 (COPE# 61275‐AS)
A Matter of Record from the Advisory Panel Report (301) 890‐4188….“the most common adverse events for either indication (keratoconus or surgical ectasia) at greater than or equal to 10 percent are corneal epithelial defect, corneal opacity, corneal striae, eye pain, and punctate keratitis. Most of these events appear to represent sequelae following corneal epithelial debridement.”
41 42
43 44

6/2/2019
Integration into Practice
Fuller, 2019 (COPE# 61275‐AS)
• Understand criteria• Look for progressing cones and surgical ectasias• Younger patients without scarring are prime candidates• Results are clinically and statistically significant• Results are long lasting• The safety profile based on the evidence is great• Work with your state boards, this may be in your scope of practice already.
• Reimbursement varies
Part 2 Myopia Control
Daniel G. Fuller, OD, FAAO, FSLSChief, Cornea Contact Lens Service
Supervisor, Cornea Contact Lens Refractive Surgery Residency The Eye Center, Southern College of Optometry
Fuller, 2019 (COPE# 61275‐AS)
Part 2: Objectives
Fuller, 2019 (COPE# 61275‐AS)
•To understand the scope of the epidemic of myopia progression
•To appreciate the impact on public health•To provide an evidenced‐based summary•To review contact lens applications•To guide practice implementation
Epidemic of Myopia Progression
Fuller, 2019 (COPE# 61275‐AS)
•Worldwide prevalence – 22% or 1.5 B people1•United States2 (ages 12‐54 years)
• 1971‐1972 – 25%• 1999‐2004 – 41.6%• Myopes >8.00D increased 8x
•Varies with ethnicity1• East Asia – 70‐80%• Western countries – 25‐40%
45 46
47 48

6/2/2019
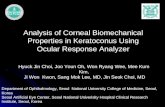
Global Prevalence of Myopia and High Myopia from 2000 through 2050
2000
Fuller, 2019 (COPE# 61275‐AS)
2010 2020 2030 2040
Holden, BH et al. Ophthalmology 2016 123, 1036-1042. DOI: (10.1016/j.ophtha.2016.01.006)
2050
7
6
5
4
3
2
1
0
BILLIONS
Ophthalmology 2016 123, 1036-1042 DOI: (10.1016/j.ophtha.2016.01.006)
Graph showing the distribution of people estimated to have myopia across age groups in 2000 and 2050.70%
Fuller, 2019 (COPE# 61275‐AS)
60%
50%
40%
30%
20%
10%
0%0 25 75 10050
AGE
Myopia Prevalence 2050
Myopia Prevalence 2000
Increased Prevalence of Myopia in the United States Between 1971‐1972 and 1999‐2004
Fuller, 2019 (COPE# 61275‐AS)
Arch Ophthalmol. 2009;127(12):1632-1639. doi:10.1001/archophthalmol.2009.303
SEX & AGE 1971‐1972 (%) 1999‐2004 (%) P‐VALUE
Female
Total 27.1 45.8 <0.001
Male
45‐54 22.8 37.4 <0.001
Arch Ophthalmol. 2009;127(12):1632-1639. doi:10.1001/archophthalmol.2009.303
Fuller, 2019 (COPE# 61275‐AS)
Increased Prevalence of Myopia in the United States Between 1971‐1972 and 1999‐2004
AGE 1971‐1972 (%) 1999‐2004 (%) P‐VALUE
18‐24 31.4 42.6 0.004
25‐34 32.3 51.6 <0.001
35‐44 39.3 49.4 0.02
45‐54 39.5 51.8 0.01
49 50
51 52

6/2/2019
Ocular Changes Associated withMyopia
Fuller, 2019 (COPE# 61275‐AS)
Retinal/Posterior Complications3‐11• Chorioretinal atrophy• Lattice degeneration• Pigmentary degeneration• Lacquer cracks• Posterior staphyloma• Fuch’s spot
• Myopic macular degeneration (leading cause of vision loss across the world)
• Rhegematogenous defects
• Posterior vitreal detachment
Fuller, 2019 (COP E# 61275‐AS)
SRNVM
High Myopia with rhegmatogenous detachment
Eye Refractive Error BCVA
OD ‐17.00‐6.00x045 20/50
OS ‐16.00‐1.50x090 20/400
Fuller, 2019 (COPE# 61275‐AS)
Rhegmatogenous Detachment
Fuller, 2019 (COPE# 61275‐AS)
53 54
55 56

6/2/2019
Rhegmatogenous Detachment
Fuller, 2019 (COPE# 61275‐AS)
Other Potential Complications
Fuller, 2019 (COPE# 61275‐AS)
•Glaucoma12‐14 – odd ratio of 1.5 to 3.3x greater risk
•Cataracts15 – nuclear and subcapsular•Optic disc anomalies3,16
•Crescents•Tilted discs•Larger disc areas
Nature• Genetics17‐33
• Biometric components of myopic eye
• Axial length (AL)– longer; heritability 40‐94%
• Anterior chamber depth (ACD) – deeper
• Keratometry – flatter• Lens thickness – thinner
Fuller, 2019 (COPE# 61275‐AS)
Nature• Genetics17‐33
• If two parents myopic risk is 5x to 6x greater compared to no or one parent
• Myopic children shown to spend more time indoors and reading than those of emmetropic parents
• If of east Asian ethnicity 8x risk
Fuller, 2019 (COPE# 61275‐AS)
57 58
59 60

6/2/2019
Nurture•Environmental34‐40
•Time outdoors seems to be protective regardless of race – BUT only prior to onset of myopia
•Urban populations at higher risk•Myopia shown to progress during winter months
•Sunlight exposure inversely related to myopia independent of aFculletr,i20v19i(CtOPyE# 61l27e5‐AvS) el
Nurture• Environmental34‐40
• Increased near work increases risk of myopia
• Duration reading at close distances have significant associations rather than total time on all near activities
http://inventorspot.com/articles/antimyopia_school_desks_bar_chinese_students_nearsightedness
Fuller, 2019 (COPE# 61275‐AS)
Proposed mechanisms of action (MOA)
Fuller, 2019 (COPE# 61275‐AS)
•Animal models from past 30 years – chickens, mice, monkeys, tree shrews
•Emmetropization process – matches AL to optical power
•Structural protein control defective – retina, RPE, choroid and/or sclera
MOA Takeaways41–57
•Form deprivation – plus lens AL
•Peripheral focus – hyperopic
and minus lens
and myopic AL•Animal studies suggest association not causation•CLEERE Study – excessive accommodation does not cause myopia
Fuller, 2019 (COPE# 61275‐AS)
61 62
63 64

6/2/2019
MOA Takeaways41–57• (Kang et al, 2010; Sng et al, 2011)
• Emmetropes & hyperopes exhibit peripheral myopia relative to central refraction and an oblate ocular shape
• Myopes exhibit more hyperopic peripheral defocus relative to central refraction and less oblate ocular shapes T
Fuller, 2019 (COPE# 61275‐AS)
Central N
Hyperopia
Emmetropia
Low Myopia
Mod. To High Myopia
MOA Limitations
Fuller, 2019 (COPE# 61275‐AS)
• (Mutti et al, 2007,2011) – Collaborative Longitudinal Evaluation of Ethnicity and Refractive Error (CLEERE)
• “A more negative refractive error, longer axial length, and more hyperopic relative peripheral refractive error in addition to faster rates of change in these variables may be useful for predicting the onset of myopia, but only within a span of 2 to 4 years before onset.”
• The inconsistent link between retinal peripheral hyperopia and axial elongation suggests other mechanisms are in play
Comparative Overview of Treatments
Leo SW, Young TL. An evidenced‐based update on myopia and interventions to retard its progression. JAAPOS. 2011;15(2):181‐189.
Favors Control Favors TreatmentUnder‐minus CL’s
PAL
Bifocals
Pirenzepine
Atropine
Fuller, 2019 (COPE# 61275‐AS)
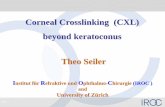
Comparative Overview of Treatments
Huang J, et al. Efficacy Comparison of 16 Interventions for Myopia Control in Children A Network Meta‐analysis. Ophthalmology 2016;123:697‐708
SVSL/Placebo
USVL
SCL
Timolol
GPCL
BSL
PDMSL
PAL
MOA
PDMFCL
PBSL
Pir
Cyc
AtL
AtM
AtH
‐0.2 ‐0.1 0
Decrease in Myopia (D)
0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 ‐0.25 ‐0.2 ‐0.15 ‐0.1 ‐0.05 0 0.05
Decrease in Axial Length (mm)
SVSL/Placebo
USVL
SCL
GPCL
BSL
PDMSL
PAL
PDMFCL
PBSL
Pir
OK
AtL
AtM
AtH
Fuller, 2019 (COPE# 61275‐AS)
65 66
67 68

6/2/2019
Treatment Options•Pharmacological
• Atropine65–96 (ATOM Study)• statistically and clinically significant decrease inprogression over two years (77% reduction in myopia and no change in AL)
• SE are significant• Rebound effect is concerning• Counter both with low dose (0.01%)
• Pirenzipine 2% gel bid82–85,88,89,92–102• M1 selective antagonist (accommodation and mydriasis)
Fuller, 2019 (COPE# 61275‐AS)
Treatment Options
Fuller, 2019 (COPE# 61275‐AS)
•Optical•Undercorrection85,86,92,94,96,103–107
• Seems to promote progression in humans but not animals
• Human studies– more myopia in group treated with0.75D under correction (Chung et al, 2002); no significant affect (Alder & Millodot, 2006)
• Bifocals84,85,88,92,96,108–123 – (US, Finland andDenmark)no significant slowing•PAL (COMET Study) 47,85,93,96,101,104,113,124–142 –statistically but not clinically significant
Treatment Options
Fuller, 2019 (COPE# 61275‐AS)
•Contact lenses56,84–86,88–96,102,103,105,138,143–186•GP lenses – Differing results but they do not slow progression in children92
• Soft lenses – “myopic creep” not found in randomized studies and SCL do not prevent progression
•Comparing GP to SCL – lower amounts of myopia in GP wearers but no difference based on AL. Corneal flattening accounts for the difference
Soft Multifocals
Fuller, 2019 (COPE# 61275‐AS)
•Bifocals/Dual focus85,86,91,92,94,163,165,173,180• Average reduction in myopic progression of 46% versus 43% for OK lenses
• Only center distance lenses investigated
Walline J . Myopia Control: A Review. Eye & Contact Lens: Science & Clinical Practice. 42(1):3‐8, January 2016. DOI: 10.1097/ICL.0000000000000207
Author Bifocal Design Add Power Study Bifocal (D) Single Vision Control (D)
Anstice Concentric +2.00 Contralateral ‐0.44+0.33 ‐0.69+0.38
Lam Concentric +2.50 Randomized ‐0.59+0.49 ‐0.79+0.56
Sankaridurg Progressive +2.00 Prospective, historical control ‐0.28+0.28 ‐0.84+0.47
Walline Progressive +2.00 Prospective, historical control ‐0.51+0.06 ‐1.03+0.06
69 70
71 72

6/2/2019
How they work
Fuller, 2019 (COPE# 61275‐AS)
•MOA•Aspheric designs with center distance increase peripheral retinal SA in a positive direction(Atchison et al, 2006; Kang et al, 2013; Ticak et al, 2013)
• (Walline et al, 2013) Compared aspheric dist. Center to spherical soft lens over 2 years•50% reduction in progression•29% reduction in AL
How they work
Fuller, 2019 (COPE# 61275‐AS)
•Challenges•Power profiles for adds vary across spherical power ranges even in the same lens design (de la Jara et al, 2014)
• Effects on accommodation were not considered• (Bickle and Walline, 2013) Add powers above+2.50 in center distance design may not be tolerated by myopic children
Dual‐focus Soft Multifocals• Dual‐Focus design (MiSight, Cooper Vision)
• Proclear material• +2.00 add; 3.36 mmOZ• MOA – center drives accommodation, treatment zones create myopic peripheral defocus
Fuller, 2019 (COPE# 61275‐AS)
Dual‐focus Soft Multifocals
Fuller, 2019 (COPE# 61275‐AS)
•Dual‐Focus design (MiSight, Cooper Vision)• (Anstice and Phillips, 2011) Cross‐over design•MiSight v. Spherical control•10 month duration; N=34•30% reduction in myopia in MiSight eye•No significant loss of CSF in this study, but……
Anstice NS, Phillips JR. Ophthalmology 2011; 118(6):1152–1161
73 74
75 76

6/2/2019
Dual‐focus Soft Multifocals
Fuller, 2019 (COPE# 61275‐AS)
• Limitations• No significant loss of CSF in this study, but……
• (Kollbaum et al, 2013) compared dual‐focus & near centered designs against spectacle correction finding more ghosting for both and loss of one line of LogMAR VA in dual focus
• Small sample size• Short duration• Paired‐eye is not binocular as will be used• At cross‐over the fellow eye has progressed and is not matched to the treated eye
• Duration of effect and rebound issues are unknown
Aspheric Concentric Soft Multifocals
Fuller, 2019 (COPE# 61275‐AS)
• Unnamed Myopia Control Lens (Alcon)• Air Optix (Lotrafilcon B)• 8.6/14.2• +0.25 in central 1.5mm progresses to +1.00 at 2.0 mm and+2.00 at edge of the 9.0 mm zone
• Peripheral plus powered aspheric design• Not commercially available unlike the MiSight which is available overseas and Canada
Aspheric Concentric Soft Multifocals
Fuller, 2019 (COPE# 61275‐AS)
• Alcon myopia control lens• Methods:
• Chinese children (n = 45) aged 7 to 14 years,• −0.75 to −3.50 D and cylinder ≤1.00 D)• Followed up for 12 months• Control group (n = 40) matched for age, sex, refractive error, axial length, and parental myopia wearing single‐vision spectacles.
Aspheric Concentric Soft Multifocals
Fuller, 2019 (COPE# 61275‐AS)
•Alcon myopia control lens•Results:
•Progression in SER at 12 months was 34% less (−0.57 D) with the novel contact lenses (95% confidence interval [CI], −0.45 −0.69 D) than(−0.86 D) SRx (95% CI, −0.74 to −0.99 D).
• Estimated increase in axial length (AL) was 33% less for CL group [0.27 mm (95% CI, 0.22–0.32 mm)] than SRx group [0.40 mm (95% CI, 0.35–0.45 mm
77 78
79 80

6/2/2019
EODF Soft Multifocals
Fuller, 2019 (COPE# 61275‐AS)
• EDOF (Novel design, BHVI; NaturalVue, VTI)• Tilia et al, 2016
• BHVI design compared against Air Optix MF (Hi,Med, Lo adds); N=52; prospective, randomized,cross‐over design
• Results:• No difference at 6m• EODF better in all other distances, betterstereopsis, fewer complaints of glare andghosting, preferred 5x more often
EODF Soft Multifocals
Fuller, 2019 (COPE# 61275‐AS)
• Tilia et al., 2016• BHVI against Acuvue Oasys for Presbyopia; N=41; prospective, cross‐over, randomized, single masked trial
• Results: EODF lenses provided better intermediate and near vision without compromising the distance.
EODF Soft Multifocals
Fuller, 2019 (COPE# 61275‐AS)
• Sha et al., 2018• BHVI design compared to 1‐Day Acuvue Moist MF; N=57, double‐masked, prospective, randomized, cross‐over design.
• Results: No difference in HCVA at dist or stereopsis. EODF better at intermediate and near with fewer photic complaints
EODF Soft Multifocals
Fuller, 2019 (COPE# 61275‐AS)
• EODF for Myopia Control• Cooper et al
• VTI lens, retrospective, case series from 10 practices• Results: Reduction in annualized myopia progression by 95.4%‐96.25%; 98.4% of children showed reduced progression, 81.25% showed complete halting; 6.25% showed regression of progression
• Limitations: Numerous
81 82
83 84

6/2/2019
Summary comparison of selected designs
Fuller, 2019 (CO PE# 61275‐AS)
Study DesignSubjects
Completing Study(n=)
Reduction inMyopia
Progression (%)
Reduction inAxial Length (%)
Duration
(mos.)
Proclear® Multifocal (CoopperVision, Pleasanton, CA)83
Center-distance, aspheric, concentric 5 51 29 24
Novel design Alcon(Duluth, GA).84
Center-distance, aspheric,concentric 43 34 32 12
MiSight (CooperVision, Pleasanton, CA)62,85
Center-distance, concentriczones
40
(144)
54
(59)
80
(52)
20
(36)Defocus IncorporatedSoftContact (DISC) [Centre for Myopia Research,the Hong Kong Polytechnic University]86
Center-distance,concentriczones 65 25 31 24
Acuvue Bifocal (JJV,Jacksonville, FL)87 Distance-center zonular 78 72 79 12Novel designs (Brien Holden Vision PtLtd., Sydney, NSW, AU)88
EODF low and (high) adds 508 in 5 groups 27 to (33) 38 to (56)
6
(12)NaturalVue Multifocal 1Day® (VTI, Alpharetta, GA)57
EODF 32 95 to 96 No data 6 to 25
Orthokeratology lenses
Fuller, 2019 (COPE# 61275‐AS)
• Many players in this space (Paragon CRT, B+L Specialty Vision Products; Emerald, Euclid, etc.)• MOA
• Myopic peripheral retinal defocus (Kang et al, 2011)
• Increase in spherical aberration (Gifford et al, 2013)
• Increase in amplitude of accommodation (Zhu et al, 2014)
Orthokeratology lenses
Fuller, 2019 (COPE# 61275‐AS)
•Orthokeratology lenses27,86,88,91–94,96,116,147,149,160,166–172,181,182,184,187–193
•Average reduction in myopic progression of43%•AL 0.36+0.24 mm OK v. 0.09+0.09 mm sph GP(Swarbrick et al, 2015)
•ROMIO study – effective in children already with >5.00 DS myopia(Cho and Cheung, 2012)
• AL for OK group 0.19+0.1 mm v. spectacles only 0.51+0.32 mm (P=0.005)
Orthokeratology lenses
Fuller, 2019 (COPE# 61275‐AS)
•Rebound effect found (Swarbrick, 2015)• Design – Cross‐over OK in one eye GP sphere in the other after 6 mos.
• OK eye had less of an inc. in AL• Switching the GP lens to the OK eye caused AL growth rate to double until it caught up
• Similar results seen in atropine v. placebo studies• Conclusion – slows progression up to 3 years but not clear how long treatment should be continued to maintain the effect. Rebound may be an issue.
85 86
87 88

6/2/2019
Environmental options
Fuller, 2019 (COPE# 61275‐AS)
•Environmental33,194–198,86,92,95,96,103,107,115,116,142,167,199–206•Outdoor time (Jones et al, 2007)
• Possibly reduces onset but not progression• Recommendations for 8‐15 hours a week• Supported by human and animal studies as being protective
From: Parental History of Myopia, Sports and Outdoor Activities, and Future Myopia Invest. Ophthalmol. Vis. Sci.. 2007;48(8):3524‐3532. doi:10.1167/iovs.06‐1118
Summary
Fuller, 2019 (COPE# 61275‐AS)
• Take‐aways• Low dose atropine provides best effect• OK, Soft Dual Focus/BF contacts are second best effect but more practical
• Center distance designs are preferred in DF/BF contact lenses or EDOF
• Multiple profiles in lens designs are indicated (Cooper, Alcon and Essilor are players)
• Combining low dose atropine with OK/DF/BF CL’s is likely additive
Implementation into Practice
• FDA• There are no FDA approved treatments for myopia control or prevention – all are off‐label in the United States
• Public Workshop ‐ Controlling the Progression of Myopia: Contact Lenses and Future Medical Devices, September 30, 2016
• Purpose was to discuss increasing prevalence and reach a consensus on best study designs for devices
https://wayback.archive‐it.org/7993/20170404181842/https://www.fda.gov/MedicalDevices/NewsEvents/Work shopsConferences/ucm500404.htm
IOVS 2019;60:M184‐2013
Fuller, 2019 (COPE# 61275‐AS)
Implementation into Practice
• FDA• If a lens was submitted today it would likely take 7 years to approve (2017)
• A 33% decrease in myopia progression could reduce myopia >‐5.00D by 73% according to the Brien Holden Institute
Fuller, 2019 (COPE# 61275‐AS)
89 90
91 92

6/2/2019
Doctrine of Informed ConsentApplies
Fuller, 2019 (COPE# 61275‐AS)
• Risks‐Benefits‐Alternatives• Must tread lightly
• Must inform parents/patient this is an off‐label treatment
• The science of underlying cause is not definitively established
• The MOA of various devices is not completely understood
• Study the evidence, attend major meetings (e.g. AAO, AOA, GSLS, IAO, AAOMC)
Fee Agreements
Fuller, 2019 (COPE# 61275‐AS)
•Vary widely•Global fee• Fee per visit• Should disclose approach clearly•Parents/Patients must be committed to the long haul
Equipment
• Topographers, Tomographers and Swiss Army knives
•Axial length biometry•Cycloplegic refractions
Fuller, 2019 (COPE# 61275‐AS) Fuller, 2019 (COPE# 61275‐AS)
93 94
95 96