UPDATES ON GLAUCOMA MANAGEMENT - neos-eyes.org · UPDATES ON GLAUCOMA MANAGEMENT James Umlas, MD...
56
UPDATES ON GLAUCOMA MANAGEMENT James Umlas, MD MODERATOR Geoffrey Emerick, MD PROGRAM COMMITTEE COORDINATOR CONTROVERSIES: Anterior and Posterior Segment Debates/Panels Dean Eliott, MD, Bonnie An Henderson, MD, Joan Miller, MD MODERATORS Jay Duker, MD PROGRAM COMMITTEE COORDINATOR HECHT POSTER CONTEST Mary K. Daly, MD MODERATOR 765 th meeting June 2, 2017 Back Bay Event Center 180 BERKELEY STREET | BOSTON, MA 02110 New England Ophthalmological Society
Transcript of UPDATES ON GLAUCOMA MANAGEMENT - neos-eyes.org · UPDATES ON GLAUCOMA MANAGEMENT James Umlas, MD...
UPDATES ON GLAUCOMA MANAGEMENT
James Umlas, MDMODERATOR
Geoffrey Emerick, MD PROGRAM COMMITTEE COORDINATOR
CONTROVERSIES:Anterior and Posterior
Segment Debates/Panels Dean Eliott, MD, Bonnie An Henderson, MD, Joan Miller, MD
MODERATORS
Jay Duker, MD PROGRAM COMMITTEE COORDINATOR
HECHT POSTER CONTESTMary K. Daly, MD
MODERATOR
765th meeting
June 2, 2017 Back Bay Event Center180 BERKELEY STREET | BOSTON, MA 02110
New England Ophthalmological Society


764th Meeting | 2
Updates On Glaucoma Management James Umlas, MD, Moderator
Geoffrey Emerick, MD, Program Committee Coordinator
Controversies: Anterior and Posterior Segment Debates/Panels
Dean Eliott, MD, Bonnie An Henderson, MD, Joan Miller, MD, ModeratorsJay Duker, MD, Program Committee Coordinator
Hecht Poster Contest Mary K. Daly, MD, Moderator
PO Box 9165 • Boston, MA 02114 | tel: 617.227.6484 | fax: 617.367.4908email: [email protected] | www.neos-eyes.org
BACK BAY EVENT CENTER180 Berkeley StreetBoston, MA 02110
Accreditation:The New England Ophthalmological Society designates this live activity for a maximum of
7 AMA PRA Category 1 Credits™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
The New England Ophthalmological Society is accredited by the Massachusetts Medical Society to provide continuing medical education for physicians.
the 765th meeting of
New England Ophthalmological SocietyA Public Foundation for Education in Ophthalmology
June 2, 2017
3 | New England Ophthalmological Society
PRESIDENT’S MESSAGE
Our June 2nd meeting marks the final meeting of another stellar academic year. With your support, we have enjoyed valuable programs ranging from advances in anterior segment surgical techniques to imaging both the front and back of the eye; from complications of cataract surgery to controversies in our daily practices. With your support, we have continued to experience outstanding lecturers from across the country and from our own New England states. With your support,
we have continued to benefit from lively discussions in program panels, at luncheon seminars, and in subspecialty sessions; discussions that help to guide our outstanding care of patients. The common factor, and the key element to NEOS’ continued success, is your support! The Executive Committee is truly grateful and fully appreciative of this support, and recognizes it comes in many forms. It comes in the form of dedication to the important committees that many of you have joined; it comes in the support to the Educational Endowment Fund to which many of you have contributed; and most important, it comes in your support to the NEOS programs, as presenters, as moderators, and as an engaged audience.
As yet another example of our members’ commitment to education and collegiality, the support of our 1st NEOS Grand Rounds at the April meeting was outstanding, with a standing room only crowd, excellent presentations, and lively discussion. It is clear that NEOS members crave both the opportunity to learn as well as the environment to enjoy the camaraderie of their New England colleagues. We thank the Young Ophthalmologists Committee for sponsoring the 1st and 2nd Grand Rounds, and look forward to these continuing next year.
Finally, I would like to sincerely thank the Executive Committee for their support, the committees for their dedication and insight, Michael Bradbury for his guidance, Judy Cerone Keenan for her tireless efforts, and my family for their love and support and for allowing me the time to serve the Society. Most importantly, I would like to thank the membership for the opportunity of serving as NEOS President; it has truly been a privilege and an honor!
Respectfully,
Jeffrey S. Heier, MD President
764th Meeting | 4
DAVID S. GREENFIELD, MDDavid S. Greenfield, MD is Professor of Ophthalmology and serves as the Douglas R. Anderson Distinguished Chair in Ophthalmology, Vice Chair of Academic Affairs of the Department of Ophthalmology, Co-Director of the Glaucoma Service, and Director of the Glaucoma Fellowship Program at the Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, Miami, FL. He earned his medical degree
from the New York University School of Medicine in 1990 and completed his residency at the New England Eye Center, Tufts University School of Medicine, Boston, in 1994. Dr. Greenfield completed a 1994-5 Heed Fellowship in Glaucoma and a 1995 Heed-Knapp Fellowship in Neuro-ophthalmology at the Bascom Palmer Eye Institute, University of Miami School of Medicine. He previously joined The New York Eye & Ear Infirmary in 1996 as Clinical Assistant Professor of Ophthalmology and Neurology.
Dr. Greenfield is a clinician, surgeon, and scientist, and has held prestigious leadership positions throughout Ophthalmology. Dr. Greenfield is the immediate Past President of the American Glaucoma Society and the American Glaucoma Society Foundation (2014-16). He is the co-founder of the International Society for Imaging in the Eye (ISIE) and served as Secretary-Treasurer from 2002 – 2007, and is the Executive Vice President and co-founder of The Florida Glaucoma Society. Dr. Greenfield serves as the Executive Editor of American Journal of Ophthalmology, is a member of the editorial boards of Journal of Glaucoma and International Glaucoma Review, and has served as the Associate Editor of Ophthalmic Surgery Lasers and Imaging (2002-2013). Dr. Greenfield has served as past Chair of the AGS Scientific Program Committee, Bylaws and Strategic Planning Committees, and member of the AAO Glaucoma Subspecialty Day Committee, Technology Assessment Committee, and EyeCare America Glaucoma Education Committee. Dr. Greenfield has served as Co-Chair of the Glaucoma Subspecialty Day of the American Academy of Ophthalmology (2003-4), and was awarded the 2010 AGS Clinician-Scientist Lectureship, 2011 American Academy of Ophthalmology Senior Achievement Award, 2015 American Academy of Ophthalmology Robert N. Shaffer Lectureship, and 2016 AAO Secretariat Award.
Dr. Greenfield has taught and published extensively in all aspects of glaucoma diagnosis, monitoring, and therapy. His research interests include optic disc and retinal nerve fiber imaging, reflectance properties of the retinal nerve fiber layer, normal-tension glaucoma, bleb-related ocular infection, and complex glaucoma filtration surgery. He was the recipient of a National Eye Institute consortium grant studying advanced imaging technology in glaucoma, and received continuous funding from the NIH from 1999-2013. He has delivered numerous guest lectures and named lectures nationally and internationally, and has published over 300 original scientific papers, abstracts and book chapters. He has trained numerous clinical and research fellows, many of whom hold distinguished academic positions worldwide.
GUEST OF HONOR

5 | New England Ophthalmological Society
The Society was founded in 1982 in appreciation for the high ethical and moral values and ophthalmic education Dr. Paul A. Chandler and Dr. Morton Grant provided to their colleagues at the Massachusetts Eye and Ear Infirmary, Harvard Medical School and the New England Ophthalmological Society. Dr. Chandler as a clinician and Dr. Grant as a basic and clinical investigator served as inspirational leaders within New England Ophthalmological Society for decades.
The purpose of the Society is to focus on the prevention of blindness from glaucoma through the integration of research and the clinical disciplines that related to glaucoma and to sustain and promote high ethical and moral values in the practice of ophthalmology and subspecialty of glaucoma.
Previous Chandler-Grant lecturers:
CHANDLER-GRANT GLAUCOMA SOCIETY
Dr. Robert Schaffer
Dr. Richard J. Simmons
Dr. B. Thomas Hutchinson
Dr. Richard Brubaker, 1992
Dr. Michael van Buskirk, 1994
Dr. Bruce M. Shields, 1996
Dr. David L. Epstein, 1999
Dr. A. Robert Bellows, 2001
Dr. David G. Campbell, 2003
Dr. David Walton, 2005
Dr. Murray A. Johnston, 2007
Dr. Joel S. Schuman, 2009
Dr. Martin Wand, 2011
Dr. Mark Latina, 2013
Dr. Cynthia Mattox, 2015

764th Meeting | 6
JANEY L. WIGGS, MD, PhDJaney L. Wiggs, MD, PhD is a physician scientist at the Massachusetts Eye and Ear Infirmary and Harvard Medical School. She is currently the Paul Austin Chandler Professor of Ophthalmology at Harvard Medical School and is the Vice Chair for Clinical Research in Ophthalmology at the Massachusetts Eye and Ear Infirmary. She also directs the
CLIA-certified genetic testing laboratory at the Massachusetts Eye and Ear Infirmary and is a co-director of the Ocular Genomics Institute.
Dr. Wiggs received her B.A. and Ph.D. degrees in biochemistry from the University of California at Berkeley and her M.D. degree from Harvard Medical School. She did post-doctoral training in molecular genetics under the direction of Dr. Ted Dryja. Dr. Wiggs completed the ophthalmology residency at the Massachusetts Eye and Ear Infirmary and received fellowship training in glaucoma and also in medical genetics and is certified by the both the American Board of Ophthalmology and the American Board of Medical Genetics. Dr. Wiggs’ research program is focused on the discovery and characterization of genetic factors that contribute to the blinding eye disease glaucoma and is funded by the National Eye Institute (NEI) as well as other nonprofit foundations. She is the co-chair of the US-INDO joint working group (NEI) and is a member of the NEI eyeGENE consortium.
Dr. Wiggs was the inaugural chair of the Genetics Group for ARVO and is an ARVO gold fellow. She currently serves on the editorial boards of IOVS, JAMA Ophthalmology, Molecular Vision, Journal of Glaucoma, and Annual Reviews in Vision Science. She is a member of the scientific advisory boards for the Glaucoma Research Foundation, the Glaucoma Foundation and Research to Prevent Blindness and is a past member of the National Advisory Council of the National Eye Institute. She has received the Heed Award, the Heed/Knapp Award, the Research to Prevent Blindness Scholar Award, the AAO Honor Award, the Lew Wasserman Merit Award, the Alcon Research Award and was a winner of the NEI Audacious Goal competition. She is a member of the Glaucoma Research Society, the American Ophthalmological Society, and the Academia Ophthalmological Internationalis.
Dr. Wiggs’ principal clinical and research interests are inherited diseases of the eye, particularly glaucoma and optic neuropathies. She is investigating the genetic etiologies of both early-onset and adult forms of glaucoma and is the PI of the NEIGHBORHOOD consortium for gene discovery in primary open angle glaucoma.
2017 CHANDLER-GRANT GLAUCOMA SOCIETY LECTURER

7 | New England Ophthalmological Society
Updates On Glaucoma Management
Moderator: James Umlas, MD Program Committee Coordinator: Geoffrey Emerick, MD
Educational Gaps:From member feedback at prior NEOS meetings, potential practice gaps include a review of ongoing developments in medical therapy of glaucoma and the surgical management of glaucoma in the setting of concurrent corneal disease.
NEOS Program Objectives: At the conclusion of this session, participants will be able to assess the clinical features and underlying pathophysiology of low tension glaucoma, as well as recognize the specific challenges of managing this surprisingly common subset of glaucoma patients. Audience members will also have a better understanding of underlying retinal ganglion cell dysfunction in glaucoma and the potential for reversal of this process. Participants will also be able to summarize the most recent developments in glaucoma medical therapy, as well as discuss the current state of knowledge about ocular perfusion pressure and its relevance to glaucoma.
Finally, attendees will develop an understanding of the challenges inherent in operating on an increasingly elderly population with glaucoma.
7:00 am Registration/Exhibits
7:30– 8:30 NEOS GRAND ROUNDS – FREEDOM ROOM
7:30 Best of the NEOS Hal Freeman Video Library – MAIN HALL
8:30 Introduction .................................................................... James Umlas, MD
8:35 New Directions in Glaucoma Medical Treatment ..................................... Cynthia Grosskreutz, MD, PhD
8:45 Ocular Perfusion Pressure: A Bankrupt Concept in Primary Open Angle Glaucoma? ................................Louis Pasquale, MD
8:55 Introduction to Guest of Honor, David Greenfield, MD ..................................................... James Umlas, MD
9:00 Glaucoma at Low Tension: When Normal Isn’t Good Enough .............................David Greenfield, MD
9:20 Glaucoma Treatment and Surgery in the Advanced Elderly: Considerations and Conundrums....................................Samuel Solish, MD
9:30 Update on Cyclophotocoagulation ................................. Noelle Pruzan, MD
9:40 Business Meeting
MORNING SESSION
764th Meeting | 8
9:55 Refreshment break / Exhibits/ Posters – please visit posters
10:25 Introduction of Chandler-Grant Lecture .........................Joel Schuman, MD
10:30 Glaucoma Genetics: Bringing the Lab to the Clinic .................................. Janey Wiggs, MD, PhD
11:00 Short-Term Enhancement of Visual Field Sensitivity in Glaucomatous Eyes Following Surgical Intraocular Pressure (IOP) Reduction ...........................................David Greenfield, MD
11:20 Panel Discussion ............................................. James Umlas, MD, Moderator
11:45 LUNCHEON BREAK: NO LUNCHEON SEMINARS
Be Sure to Scan in for Afternoon Session Before Going to Room to Receive Credit
Be Sure to Return Your Audience Response Unit Before Leaving the Building!
MORNING SESSION (continued)
David Greenfield, MD Cynthia Grosskreutz, MD, PhD
Louis Pasquale, MD
Noelle Pruzan, MD Samuel Solish, MD

9 | New England Ophthalmological Society
AFTERNOON SESSION
Controversies: Anterior and Posterior Segment Debates/Panels Joan Miller, MD and Dean Eliott, MD, Moderators Posterior Segment Bonnie An Henderson, MD, Moderator Anterior Segment Program Committee Coordinator: Jay Duker, MD
Professional Practice Gaps: Management of ophthalmic diseases can be complicated. There can be different approaches for the same problem. In this session, we will focus on the controversies in cataract surgery, corneal refractive surgery, and pediatric ophthalmology. The advantages and disadvantages will be presented for each topic. The topics will include bilateral simultaneous cataract surgery, small incision lenticule extraction refractive surgery, atropine for the prevention of progressive myopia, and corneal vs intraocular approaches to treat presbyopia. Lastly, a panel will discuss their preferred method for continuing medical education, future trends in ophthalmology, and look back on their career choices.
Program Objectives: Management of ophthalmic diseases can be complicated. There can be different approaches for the same problem. In this session, we will focus on the controversies in cataract surgery, corneal refractive surgery, and pediatric ophthalmology. The advantages and disadvantages will be presented for each topic. The topics will include bilateral simultaneous cataract surgery, small incision lenticule extraction refractive surgery, atropine for the prevention of progressive myopia, and corneal vs intraocular approaches to treat presbyopia. Lastly, a panel will discuss their preferred method for continuing medical education, future trends in ophthalmology, and look back on their career choices
References: 1. Blum M, Täubig K, Gruhn C, Sekundo W, Kunert KS. Five-year results of Small
Incision Lenticule Extraction (ReLEx SMILE). Br J Ophthalmol. 2016 Jan 8. pii: bjophthalmol-2015-306822. doi: 10.1136/bjophthalmol-2015-306822.
2. Kessel L, Andresen J, Erngaard D, Flesner P, Tendal B, Hjortdal J. Immediate Sequential Bilateral Cataract Surgery: A Systematic Review and Meta-Analysis. J Ophthalmol. 2015;2015:912481. doi: 10.1155/2015/912481. Epub 2015 Aug 17.
3. Gil-Cazorla R, Shah S, Naroo SA. A review of the surgical options for the correction of presbyopia. Br J Ophthalmol. 2016 Jan;100(1):62-70. doi: 10.1136/bjophthalmol-2015-306663.
1:00 pm Introduction Posterior Segment ...........................................Joan Miller, MD
1:01 Debate #1: Glaucoma: Glaucoma can be managed by OCT alone ...... True: Geoffrey Emerick, MD
False: Laura Fine, MD Rebuttals
764th Meeting | 10
AFTERNOON SESSION (continued)
1:16 Debate #2: Neuro-ophthalmology: Corticosteroids should be used to treat non-arteritic ischemic optic neuropathy .............True: Thomas Hedges, MD
False: Joseph Rizzo, MD Rebuttals
1:31 Debate #3: Oculoplastics: There are no oculoplastics emergencies ............. True: Michael Migliori, MD
False: Michael Yoon, MD Rebuttals1:46 Debate #4: Retina:
Laser has no role in the management of diabetic retinopathy .............................................True: Jennifer Sun, MD
False: Jorge Arroyo, MD Rebuttals
2:01 Posterior Panel Discussion .........................................Michael Bradbury, MD Jay Duker, MD
Joan Miller, MD Claudia Richter, MD
2:15 Refreshment Break/Exhibits
2:45 Introduction: Anterior Segment ........................Bonnie An Henderson, MD
2:50 Debate #1: Bilateral simultaneous surgery ................Pro: Douglas Evans, MD Con: Brendan McCarthy, MD
3:00 Debate#2: SMILE ...........................................................Pro: Katie Luo, MD Con: Priyanka Sood, MD
3:10 Debate #3: Use of Atropine to Prevent Progression of Myopia.................................................. Pro: Amita Bhatt, MD
Con: Mitchell Strominger, MD
3:20 Debate #4: Surgical Correction of Presbyopia: Intraocular Lens Approach .......................................... Pro: Samir Melki, MD
Con: Charles Barsam, MD
3:30 Anterior Panel Discussion ................Bonnie An Henderson, MD, Moderator
4:00 Adjourn
Christopher Andreoli, MDStephen Christiansen, MDCynthia Grosskreutz, MD
Jeffrey Heier, MDJeffrey Marx, MDJean Ramsey, MD

11 | New England Ophthalmological Society
8:35 AM
New Directions in Glaucoma Medical TreatmentCynthia Grosskreutz, MD, PhD
NOVARTIS INSTITUTES FOR BIOMEDICAL RESEARCH | CAMBRIDGE, MA
Objective: The objective of the presentation is provide an update on new approaches to the medical treatment of glaucoma.
Despite advances in our ability to diagnose and surgically treat glaucoma, the medical management of the disease has remained largely unchanged for over 20 years. As the global population ages, however, the need for effective medical treatments for glaucoma (including strategies to enhance compliance) will continue to grow. Three major themes have emerged in the development of new glaucoma therapeutics: improved IOP lowering, improved delivery systems and neuroprotection. I will review several recent clinical trials of new compounds to lower IOP, novel drug delivery approaches for glaucoma medications and briefly discuss the promise and challenge of developing drugs for neuroprotection in glaucoma.
References: Schehlein EM, Novack GD, Robin AL. New classes of glaucoma medications. Curr Opin Ophthalmol. 2017 Mar;28(2):161-168.
Aref AA. Sustained drug delivery for glaucoma: current data and future trends. Curr Opin Ophthalmol. 2017 Mar;28(2):169-174.
De Moraes CG, Liebmann JM, Levin LA. Detection and measurement of clinically meaningful visual field progression in clinical trials for glaucoma. Prog Retin Eye Res. 2017 Jan;56:107-147.

764th Meeting | 12
8:45 AM
Ocular Perfusion Pressure: A Bankrupt Concept in Open Angle Glaucoma?
Louis R. Pasquale, MD
MASSACHUSETTS EYE AND EAR INFIRMARY | BOSTON, MA
Objective: Ophthalmologists should focus on achieving low target IOP in patients with progressive glaucoma, regardless of their BP.
A randomized clinical trial suggesting that intensive systolic blood pressure (BP) control <120 mm Hg results in fewer cardiovascular events raises concerns that adoption of intensive hypertension control will have adverse consequences for glaucoma patients. Observational studies report an inverse relation between ocular perfusion pressure and open-angle glaucoma (OAG). While a robust connection between higher IOP and glaucoma exists, there is actually a modest adverse relation between higher BP and OAG. A meta-analysis of 5 studies found no differences in systolic or diastolic BP during the day or night in OAG patients with progressive versus stable visual fields. Ophthalmologists should focus on achieving low target IOP in patients with progressive glaucoma, regardless of their BP.
References: The SPRINT Research Group. A Randomized Trial of Intensive versus Standard Blood Pressure Control NEJM 2015;373:2103-2116.
Leske MC, Wu SY, Hennis A, et al. Risk factors for incident open-angle glaucoma: the Barbados Eye Studies. Ophthalmology 2008; 115: 85-93.
Zhao D, Cho J, Kim MH, Guallar E. The association of blood pressure and primary open-angle glaucoma: a meta-analysis. Am J Ophthalmol 2014; 158: 615-627.

13 | New England Ophthalmological Society
9:00 AM
Glaucoma at Low Tension:When Normal Isn’t Good Enough
David Greenfield, MD
BASCOM PALMER EYE INSTITUTE, UNIVERSITY OF MIAMI MILLER SCHOOL OF MEDICINE | MIAMI, FL
Objective: To review the clinical approach for identification and management of open-angle glaucoma at low intraocular pressure
Glaucoma at low tension is a commonly observed, multifactorial disorder with IOP dependent and independent mechanisms. Routine diagnostic evaluation is not warranted and should be reserved for atypical patients. Most eyes respond to nonsurgical pressure lowering but filtration surgery may be required to achieve single digit pressure targets. Further progression despite maximal IOP lowering may occur in some individuals. Although the exact mechanisms are unclear, ongoing damage may be related in part to impaired ONH perfusion or alteration of the translaminar pressure gradient.
References: Greenfield DS, Siatkowski RM, Glaser JS, Schatz NJ, Parrish RK II. The cupped disc: Who needs neuroimaging? Ophthalmology, 1998:105:1866-74.
Krupin T, Liebmann JM, Greenfield DS, Ritch R, Gardiner S. A randomized double-masked trial of brimonidine versus timolol in preserving visual function: The Low-Pressure Glaucoma Treatment Study. Am J Ophthalmol 2011; 151:671-81.
Schultz SK, Iverson SM, Shi W, Greenfield DS. Safety and efficacy of achieving single digit intraocular pressure targets in eyes with progressive normal-tension glaucoma. J Glaucoma 2016;25:217-22.

764th Meeting | 14
9:20 AM
Glaucoma Treatment and Surgery in the Advanced Elderly:Considerations and Conundrums
Samuel P. Solish, MD
EYECARE MEDICAL GROUP | PORTLAND, ME
Objective: To discuss special considerations for glaucoma treatment in the advanced elderly.
Glaucoma in the advanced elderly (>85 yrs old) presents a unique set of issues for ophthalmologists. Treatment considerations often involve special medical and surgical considerations as well as co-morbidities and social concerns. This talk will outline the increasingly complex decisions in treating these patients. As the incidence of glaucoma increases with advancing age, there are the ophthalmic co-morbidities of cataract, corneal disease and AMD. Additionally, for example, cognitive impairment, mobility restrictions, arthritis and inability to self- administer drops can be significant limitations in the planning of a treatment regimen for the advanced elderly. Individualization of treatment is crucial in planning for success in this patient population. Although it is very difficult to completely understand a patients’ social and environmental situation direct questions and clues must be collected, family members consulted (with patient permission) and treatment limitations recognized. Medical and surgical “standard” paradigms may need reconsideration given a patient’s age. Many have discussed the possible over-aggressive treatment for mild disease in this age group, however, some patients in the extreme elderly group may indeed require aggressive treatment to save vision even with limited life expectancy. All surgical and medical options should be considered to treat these challenging patients but modifications in approach, perspective and technique may be necessary to accomplish the treatment goals.
References: Tsai JC. Comprehensive Perspective on Patient Adherence to Topical Glaucoma Therapy Ophthalmology, Volume 116, Issue 11,S30 - S36.
Keenan TDL, Goldacre, R, Goldacre, MJ. Associations between primary open angle glaucoma, Alzheimer’s disease and vascular dementia: record linkage study. Br J Ophthalmol. 2015 Apr;99(4):524-7.
Raczynska D, Glasner L, Serkies-Minuth E et al. Eye Surgery in the Elderly. Clinical Interventions in Aging 2016:11 407-414.

15 | New England Ophthalmological Society
9:30 AM
Update on CyclophotocoagulationNoelle Pruzan, MD
PORTLAND, ME
Objective: The objective of this presentation is to improve the audience’s knowledge of cyclophotocoagulation, including traditional transscleral cyclophotocoagulation (TSCPC), micropulse cyclophotocoagulation (MP-CPC), and endoscopic cyclopho-tocoagulation (ECP).
Cyclophotocoagulation (CPC) is a cyclodestructive procedure that decreases the production of aqueous humor by the ciliary processes, thereby treating glaucoma by decreasing intraocular pressure. Traditional TSCPC has typically been reserved for refractory glaucoma, primarily due to concern over potential adverse effects. ECP has shown promise in eyes with more visual potential, including as a combination surgery with phacoemulsification. MP-CPC is a newer modification of TSCPC that uses repetitive “on” and “off” segments of laser energy (“micropulses”), allowing for more localized treatment and less collateral damage. These three ciliary body laser procedures will be reviewed, including indications, techniques, and efficacy.
References: Amoozgar B, Phan EN, Lin SC, Han Y. Update on ciliary body laser procedures. Curr Opin Ophthalmol. 2017;28(2):181-186.
Aquino MCD, Barton K, Tan AMW, et al. Micropulse transscleral diode laser cyclophotocoagulation in the treatment of refractory glaucoma. Clin Exp Ophthalmol 2010;38:266-272.
Cohen A, Wong SH, Patel S, Tsai JC. Endoscopic cyclophotocoagulation for the treatment of glaucoma. Surv Ophthalmol 2017;62(3):357-365.

764th Meeting | 16
10:30 AM CHANDLER-GRANT LECTURE
Glaucoma Genetics: Bringing the Lab to the Clinic
Janey Wiggs, MD, PhD
MASSSCHUSETTS EYE AND EAR INFIRMARY | BOSTON, MA
Objective: To present an update on gene discovery for glaucoma and to demonstrate how genetic information can be used clinically for diagnosis, risk assessment and treatment.
The discovery of genes responsible for glaucoma makes it possible to develop novel gene-based therapies and diagnostic tests. Genome-wide association studies (GWAS) have now identified 15 genes and loci contributing to POAG, 2 to XFG and 8 to PACG (primarily in Asian populations). Whole exome sequencing (WES) and genetic linkage analyses has identified 9 genes responsible for early onset (diagnosis before age 40) glaucoma. The clinical utility of this genetic information is emerging. Early-onset glaucoma genes can be used for gene-based testing which has important benefits for patients and family members. Two early-onset glaucoma genes (MYOC and TIE2) are targets for novel gene-based therapies. Primary open angle glaucoma (POAG) genetic risk factors have been correlated with specific clinical traits and risk scores based on POAG genetic factors are predictive of earlier disease onset. Several POAG genetic risk factors also point to novel therapeutic targets.
References: Souma T, Tompson SW, Thomson BR, Siggs OM, Kizhatil K, , et al. Angiopoietin receptor TEK mutations underlie primary congenital glaucoma with variable expressivity. J Clin Invest. 2016 Jul 1;126(7):2575-87.
Bailey JN, Loomis SJ, Kang JH, Allingham RR, et al. Genome-wide association analysis identifies TXNRD2, ATXN2 and FOXC1 as susceptibility loci for primary open-angle glaucoma. Nat Genet. 2016 Feb;48(2):189-94.
Loomis SJ, Kang JH, Weinreb RN, Yaspan BL et al. Association of CAV1/CAV2 genomic variants with primary open-angle glaucoma overall and by gender and pattern of visual field loss. Ophthalmology. 2014 Feb;121(2):508-16.

17 | New England Ophthalmological Society
11:00 AM
Short-term Enhancement of Visual Field Sensitivity in GlaucomatousEyes Following Surgical Intraocular Pressure
David Greenfield, MD
BASCOM PALMER EYE INSTITUTE, UNIVERSITY OF MIAMI MILLER SCHOOL OF MEDICINE | MIAMI, FL
Objective: To examine the hypothesis that surgical intraocular pressure reduction leads to enhancement of visual field sensitivity in glaucomatous eyes.
It has been a long-held tenet that glaucomatous field loss is permanent and irreversible. We present evidence that in patients with suboptimally controlled IOP, glaucoma surgery ( either trabeculectomy or aqueous shunt ) resulted in a significantly higher percentage of patients with short-term improvement of central and peripheral visual field sensitivities, compared to stable medically treated glaucoma patients. This may represent a potential biomarker for retinal ganglion cell response to therapeutic interventions in glaucoma.
References: Wright TM, Goharian I, Gardiner SK, Sehi M, Greenfield DS. Short-term enhancement of visual field sensitivity in glaucomatous eyes following surgical intraocular pressure reduction. Am J Ophthalmol 2015 Feb; 159 (2): 378-85.
Bhardwaj N, Niles PI, Greenfield DS, Hymowitz M, Sehi M, Feuer WJ, Budenz DL. The impact of surgical intraocular pressure reduction on visual function using various criteria to define visual field progression. J Glaucoma. 2013 Oct-Nov; 22 (8): 632-7.
Folgar FA, deMoraes CG, Teng CC, Tello C, Ritch R, Liebmann JM. Effect of successful and partly successful filtering surgery on the velocity of glaucomatous field progression. J Glaucoma. 2012 Dec; 21 (9): 615-8.
764th Meeting | 18
NEOS SCIENTIFIC POSTER PROGRAM
HECHT AWARDS for Best Resident and Fellow Posters
Residents and fellows from all the New England ophthalmologic teaching programs have submitted abstracts for our annual scientific poster presentation contest being conducted today. Posters will be judged on originality and scientific merit. Awards will be made for the first prize $500.00, second prize $300.00, third prize $200.00 and three honorable mentions of $50.00 each. Funding for the awards is derived from a gift to the NEOS Education Endowment Fund honoring the late Sanford Hecht, MD.
Please take some time to stop by these interesting posters in the lower lobby.
NEOS thanks Mary Daly, MD, the Moderator of the Poster Contest, and this year’s judges:
Nicholas Butler, MDPaul Greenberg, MD
Hyunjoo Lee, MD

19 | New England Ophthalmological Society
Risk Factors for Early Intraocular Pressure Elevation After Cataract Surgery
in a Cohort of United States VeteransKaushik Annam
Brown University, Providence, RI
Allison Chen, Irene Lee, Jorge Rivera, Paul Greenberg
Objective: To understand risk factors for intraocular pressure elevation one day after predominantly resident-performed cataract surgery in a cohort of Veterans Health Administration-treated patients, a population known to have a higher burden of co morbidities than the general population.
Purpose: To investigate the risk factors for intraocular pressure (IOP) elevation one day after cataract surgery in a cohort of United States veterans.
Methods: A retrospective study of 1137 cataract surgeries (784 patients) was performed between April 2013 and April 2016 at a single Veterans Affairs medical center. Logistic regression, adjusted for clustering in patients with bilateral surgeries, was used to evaluate risk factors for first postoperative day IOP elevation (28 mmHg).
Results: Twenty percent (232/1137) of eyes had elevated IOP. Independent risk factors were a history of ocular hypertension [OR: 8.74 (4.03-18.9)] or glaucoma [OR: 3.54 (2.17-5.75)], a preoperative 22 mmHg [OR: 2.51 (1.12-5.62)] and complicated cataract surgery (vitreous loss, anterior capsular tear, posterior capsular tear, or presence of zonular lysis) [OR: 2.45 (1.18-5.08)].
Conclusions: Cataract surgery patients with ocular HTN, glaucoma, a preoperative IOP >22 mmHg or significant intraocular complications may benefit from prophylactic ocular anti-hypertensive medication.
References: Coban-Karatas M, Sizmaz S, Altan-Yaycioglu R, Canan H, Akova Y. Risk factors for intraocular pressure rise following phacoemulsification. Indian Journal of Ophthalmology. 2013;61(3):115-118. doi:10.4103/0301-4738.99997.
Elfersy AJ, Prinzi RA, Peracha ZH, et al. IOP Elevation after Cataract Surgery. Journal of Glaucoma. 2016;25(10):802-806. doi:10.1097/ijg.0000000000000421.
Kim JY, Jo M-W, Brauner SC, et al. Increased intraocular pressure on the first postoperative day following resident-performed cataract surgery. Eye. 2011;25(7):929-936. doi:10.1038/eye.2011.93.
POSTER #1

764th Meeting | 20
POSTER #2
Choroidal Vascular Density and Volume in Intermediate Age-related Macular Degeneration: The Influence of Subretinal Drusenoid Deposits
Grayson Armstrong, MD, MPH Massachusetts Eye & Ear Infirmary, Boston, MA
Jay Wang, Ines Lains, Demetrios Vavvas, Ivana Kim, Joan Miller, Deeba Husain, John Miller
Objective: The objective of this study was to assess choroidal thickness, volume, and density in eyes with intermediate age-related macular degeneration, comparing eyes either with or without subretinal drusenoid deposits.
Purpose: Age-related Macular Degeneration (AMD) is the leading cause of blindness in developed countries. The pathophysiology of associated reticular pseudodrusen (RPD) remains only partially understood. This study aimed to compare macular choroidal vasculature density and volume in intermediate AMD eyes with and without RPD, using swept-source optical coherence tomography (SS-OCT).
Methods: Multicenter, prospective, observational study, including patients with intermediate AMD. Participants underwent complete ophthalmic exam, color fundus photography (used for AMD staging according to the AREDS system) and spectral-domain OCT (to evaluate for the presence of RPD by two independent graders). SS-OCT (3D horizontal volume, 12mm x 9mm) en face images of choroidal vasculature were captured (using Bruch’s membrane as reference for flattening) and converted to binary images. Choroidal vascular density was calculated as percent area occupied by choroidal vessels in a 6mm diameter circular submacular region centered on the fovea. Choroidal thickness was obtained using SS-OCT automated software. The submacular choroidal vascular volume was calculated by multiplying the average choroidal vascular density by macular area and choroidal thickness. Multilevel mixed effect linear models (accounting for correlated outcomes between 2 eyes) were used for analyses.
Results: We included 185 eyes of 118 patients with intermediate AMD (113 female, 61.1%). Ninety-two percent (n=171) had classic drusen, 50.3% (n=93) had RPD, and 44.9% (n=83) presented with both. Univariate analysis revealed that increased age was significantly associated with decreased choroidal vascular volume (ß=-0.0004, p<0.001) and mean choroidal density (ß=-0.003, p=0.001). After controlling for age, the presence of RPD was significantly associated with reduced macular choroidal volume (ß=-0.003, p=0.007). Macular choroidal thickness in eyes with RPD (n=93, 0.017 mm ± 0.01) was significantly lower than in eyes without RPD (n=92, 0.019 mm ± 0.01). However, reticular drusen were not correlated with mean choroidal density (p=0.063).

21 | New England Ophthalmological Society
POSTER #2 (continued)
Discussion: Submacular choroidal vascular volume is reduced in eyes with RPD as compared to eyes without these lesions. Our results are consistent with prior work showing reduced choroidal thickness in AMD patients with RPD, and provides evidence of choroidopathy as a possible factor in disease pathogenesis.
References: Yun C, Oh J, Ahn S-E, Hwang S-Y, Kim S-W, Huh K. Peripapillary choroidal thickness in patients with early age-related macular degeneration and reticular pseudodrusen. Graefes Arch Clin Exp Ophthalmol. 2016;254(3):427-435. Garg A, Oll M, Yzer S, et al. Reticular pseudodrusen in early age-related macular degeneration are associated with choroidal thinning. Invest Ophthalmol Vis Sci. 2013;54(10):7075-7081. Alten F, Clemens CR, Heiduschka P, Eter N. Localized reticular pseudodrusen and their topographic relation to choroidal watershed zones and changes in choroidal volumes. Investig Ophthalmol Vis Sci.2013;54(5):3250-3257.

764th Meeting | 22
POSTER #3
Progression to Surgery for Epiretinal Membranes with Good Vision
Xuejing Chen Tufts Medical Center, Boston, MA
Chirag Shah, Jeffrey Heier
Objective: This study answers a common question from patients with idiopathic ERMs that are not considered initial candidates for surgical intervention: What is my risk of my ERM progressing?
This is a retrospective review of all eyes with idiopathic ERMs with VA 20/40 without intolerable symptoms referred to a retina service between 2009 and 2012. Surgery was offered when VA worsened to 20/50 and/or eyes developed intolerable symptoms attributable to the ERM. Primary outcome measure was time to surgery. Eyes were categorized by foveal contours (FC) on baseline OCT and by presence of initial symptoms. 107 eyes from 99 patients were identified, averaging 66 10 years old. Presenting VA averaged 20/27. The Kaplan Meier survival curve for progression to surgery at 7 years was 14%. 18.8% of initially symptomatic eyes and 12.3% of initially asymptomatic eyes progressed to surgery (p=0.34). Eyes without loss of FC did not progress. Eyes with complete loss of FC progressed faster than eyes with mild loss of FC, but the curves converge at 4 years leading to 18.5% at 7 years. References: Byon IS, Pak GY, Kwon HJ, Kim KH, Park SW, Lee JE. Natural History of Idiopathic Epiretinal Membrane in Eyes with Good Vision Assessed by Spectral-Domain Optical Coherence Tomography. Ophthalmologica. 2015;234(2):91-100.
Bell SF, Guzowski M, Rochtcina E. Five-Year Cumulative Incidence and Progression of Epiretinal Membranes. Vol 110. The Blue Mountains Eye Study. Ophthalmology; 2003:34-40.
Moisseiev E, Kinori M, Moroz I, Priel E, Moisseiev J. 25-Gauge Vitrectomy with Epiretinal Membrane and Internal Limiting Membrane Peeling in Eyes with Very Good Visual Acuity. Curr Eye Res. 2016;41(10):1387-1392.
23 | New England Ophthalmological Society
POSTER #4
Invasive Orbital Aspergillosis in Immunocompetent Patients from the Northeastern United States
Danny Diaz, MD Massachusetts Eye and Ear Infirmary, Boston, MA
Suzanne Freitag, Durand Marlene
Objective: Invasive orbital aspergillosis, a potentially fatal disease, is especially rare in immunocompetent patients who live in temperate or cold climates. We sought to characterize several such cases treated at the Massachusetts Eye and Ear Infirmary over an 18-year period.
Purpose: Invasive orbital aspergillosis is especially rare in immunocompetent patients who live in temperate or cold climates. We characterized several such cases treated at the Massachusetts Eye and Ear Infirmary over an 18-year period.
Methods: Records of 5 immunocompetent patients diagnosed with orbital aspergillosis 1995-2014 were reviewed. Demographic, clinical, radiologic, and laboratory findings were noted.
Results: The 3 male and 2 female patients, ages 41-76 years (mean 54) lived in New England or northern New York. The mean time from symptom onset to diagnosis was 5 months (range 3-9); initial misdiagnoses included bacterial orbital infection, Tolosa Hunt, and optic neuropathy. Symptoms in all patients were unilateral headache, eye pain, and decreased vision. All had MRI evidence of orbital apex and cavernous sinus involvement. Three patients recovered fully except for a blind eye in 2.
Conclusions: This study highlights cases of invasive aspergillosis in immunocompetent patients from a relatively cold climate, while most series have been from hot, humid countries such as India. Ocular complaints are common initial symptoms, and increased awareness by ophthalmologists is crucial in providing an early diagnosis.
References: Pushker N, Meel R, Kashyap S et al - Invasive Aspergillosis of orbit in immunocompetent patients: treatment and outcome - Ophthalmology 2011 Sep: 118(9):1886-91.
Arakawa H, Suto C, Notani H et al - Selection of the antifungal agent decides prognosis of invasive aspergillosis: case report of a successful outcome with voriconazole. Int Ophthalmol 2014 Feb;34(1):85-9.
Kim JW, Rha MS, Kim JH et al - Orbital Apex Syndrome caused by invasive aspergillosis. J Craniofac Surg 2014;25(2):e191-3.

764th Meeting | 24
POSTER #5
The Effect of Topical Prostaglandins on Migraine HeadachesLaura Hall
Yale School of Medicine, New Haven, CT
Venkatesh Brahma, Robert Lesser, B. Thomas Hutchinson, Bradford Shingleton, Martin Wand, Christopher Teng
Objective: Prostaglandin analogues could prove to be a novel treatment modality for the management of migraine headaches.
Purpose: To study the ability of topical prostaglandin analogues applied to the fingernail bed or eye in reducing the frequency, severity and duration of migraines.
Methods: We conducted retrospective expanded Migraine Disability Assessment (MIDAS) questionnaires on 17 migraine patient’s pre- and post- treatment.
Results: Subjects (average age 54.4; 4 males) used prostaglandins (2 in the eye and 15 on the nail) for 15.8 months on average. There was a decrease in the number of headache days from the 3 months pre-treatment (mean 24.7 headache days) to the 3 months post-treatment (mean 7.5 days) (p 0.05). There was a decrease in headache severity from 6.1 to 3.7 (scale 0-10) (p 0.05) and headache duration from 3-12 hours to 1-3 hours (p 0.05). The MIDAS score reduced from 18.4 to 3.9 (p 0.05). No adverse effects were reported with nail application however it was noted that nail growth accelerated.
Conclusion: Prostaglandin analogues may prove to be a novel treatment modality for headache management.
References: The Migraine Disability Assessment (MIDAS) Test. Innovative Medical Research, 1997, AstraZenaca Pharmaceuticals, LP 2007.
Stewart WF, et al. Development and testing of the Migraine Disability Assessment (MIDAS) Questionnaire to assess headache-related disability. Neurology. 2001; 56(6 Suppl):S20-8.
Headache Impact Test (HIT-6). QualityMetric, Inc and GlaxoSmithKline. 2001.

25 | New England Ophthalmological Society
POSTER #6
Oculomotor Outcomes in Children Treatedfor Brain Tumors of the Posterior Fossa
Maanasa Indaram, MD Boston Children’s Hospital, Boston, MA
Jane Edmond, Yan Guo, Crandall Peeler, Jeffrey Hollander, Gena Heidary
Objective: As oculomotor dysfunction, including cranial neuropathies and nystagmus, commonly occur in the setting of posterior fossa brain tumors in children, we sought to evaluate incidence and management of oculomotor sequelae in a large cohort of pediatric patients seen at two tertiary care centers.
Introduction: Oculomotor dysfunction including cranial neuropathies and nystagmus may occur in the setting of posterior fossa brain tumors. Data regarding incidence and management of oculomotor sequelae for children treated for posterior fossa tumors are limited. We sought to evaluate these outcomes in a large cohort of pediatric patients seen at two tertiary care centers.
Methods: A retrospective chart review from 2005 to 2011 was performed. Data including tumor type, treatment, and ophthalmic findings relevant to oculomotor outcomes pre- and post- tumor treatment were recorded. Results: We identified 127 patients with a mean age of 7 years ( 4.48 years) at tumor diagnosis who fulfilled inclusion criteria. The most common tumor type was medulloblastoma. Prior to tumor treatment, strabismus occurred in 19/127 (15%) patients of whom, 12 (63%) had an abducens palsy, 2 (11%) had a trochlear nerve palsy, and 4 (21%) had a variable exotropia. Following tumor treatment, 33/127 (26%) patients had nystagmus and 45/127 (35%) had strabismus, among whom an abducens palsy was the most common cranial neuropathy occurring in 31/45 (69%) patients. Spontaneous resolution of strabismus occurred in 28/56 (50%) of patients. Of the patients with persistent strabismus, 20/56 (36%) underwent surgery with modest outcomes. Good motor alignment <10PD was achieved in 9/20 patients (45%) with 7/20 (35%) patients demonstrating the presence of stereopsis.
Discussion: Oculomotor dysfunction is common in children treated for posterior fossa tumors. Spontaneous resolution of strabismus may occur in a small percentage of some patients.
Conclusion: Oculomotor dysfunction is common in children treated for posterior fossa tumors. Spontaneous resolution of strabismus may occur in a small percentage of patients. Surgical management of strabismus is difficult with modest post-operative results.
References: Weiss AH, Ojemann JG, Ellenbogen RG, et al. Eye movement deficits in children with posterior fossa tumors. JAAPOS 2007; 11:104-5.
Shalev B, Repka MX. Restoration of fusion in children with intracranial tumors and incomitant strabismus. Opthalmology 2000; 107(10):1880-3.
Williams AS, Hoyt CS. Acute comitant esotropia in children with brain tumors. Arch Ophthalmol 1989;107(3):376-8.

764th Meeting | 26
POSTER #7
Divergence in the Management of Closed Orbital Blowout Fractures: A Retrospective Comparison Among Different
Surgical Subspecialties at a Single InstitutionJenna Kim, MD
Yale Eye Center, New Haven, CT
Alberto Distefano
Objective: Understand the clinical significance of various models of orbital floor management.
Purpose: Without consensus on the management of orbital floor fractures (OFFx) across surgical subspecialties, patients may be subject to various models of surgical decision-making.
Method: A retrospective chart review study assessed interdepartmental concordance of OFFx management, timing of surgery, and reoperation rates. Results: For 227 patients with OFFx, concordance of plan in the emergency department between ophthalmology and other surgical subspecialties was 92%, decreasing to 64% in outpatient follow-ups. For the 35 patients who had non-urgent surgical repair, the average time to surgery by ophthalmology was 42.5 days compared to 13.9 days between ophthalmology and other surgical subspecialties (p=0.04). Need for reoperation by ophthalmology was 11% compared to 3.7% by other subspecialties (p=0.55).
Conclusion: The discordance in surgical management on the OFFx by the various subspecialties may be related to time from ED visit to surgery, although reoperation rates are similar.
References: Richards NQ, Brown NH, Kidwell ED Jr. Visual Acuity in Orbital Floor Fractures: Does Surgical Subspecialty Management Matter? J Craniofac Surg. 2015 Jul;26(5):1668-72.
Scawn RL, Lim LH, Whipple KM, Dolmetsch A, Priel A, Korn B, Kikkawa DO. Outcomes of Orbital Blow-Out Fracture Repair Performed Beyond 6 Weeks After Injury. Ophthal Plast Reconstr Surg. 2016 Jul-Aug;32(4):296-301.

27 | New England Ophthalmological Society
POSTER #8
Cataract Surgery in the Very Elderly: A Systematic Review
Emily Li, MD Yale University School of Medicine, New Haven, CT
Curtis Margo, Paul Greenberg
Objective: Our systematic review assessed the effect of very elderly age (85 years and older) on cataract surgery outcomes.
The prevalence of very elderly patients (aged 85 years and older) with visually significant cataracts continues to rise in the United States. We conducted a systematic review of literature using PRISMA guidelines to investigate the impact of very old age on cataract surgery outcomes. The studies suggest that very elderly patients, relative to their younger counterparts, had similar complication rates after adjusting for their higher rates of age-related ocular and systemic comorbidities. In addition, most very elderly patients gained improvement in visual acuity, enjoyed increased quality of life, and had survival rates that extend beyond one year after surgery. However, many of the studies were small and lacked statistical power to exclude clinically important differences in outcome when one truly existed. Further studies are needed to predict meaningful visual outcomes in elderly persons with ocular comorbidities.
References: Aging NIo: Global Health and Aging, Vol. 2017, National Institutes of Health, 2011.
Song E, Sun H, Xu Y, et al.: Age-related cataract, cataract surgery and subsequent mortality: a systematic review and meta-analysis. PLoS One 9:e112054, 2014.
Yu WK, Chen YT, Wang SJ, et al.: Cataract surgery is associated with a reduced risk of dementia: a nationwide population-based cohort study. Eur J Neurol 22:1370-7, e79-80, 2015.

764th Meeting | 28
POSTER #9
Glycated Hemoglobin Levels and Risk of Clinically Significant MacularEdema after Cataract Surgery in Veterans: Results from the Veterans
Affairs (VA) Ophthalmic Surgery Outcomes Data (OSOD) Project
Michael Lin Massachusetts Eye and Ear, Boston, MA
Objective: This research analyzed the association of elevated HgbA1c levels and risk of diabetic CSME after cataract surgery in veterans.
Purpose: Risk of clinically significant macular edema (CSME) at various glycated hemoglobin (HbA1c) levels is an important yet underreported aspect of cataract surgery and its management. We explored the association of elevated HbA1c levels and risk of diabetic CSME after cataract surgery in veterans.
Methods: Retrospective cohort study of the Veterans Affairs Ophthalmic Surgery Outcomes Data Project Results: Of 4923 cases, 2003 had HbA1c data available. Mean HbA1c level was 7.34% (range 4.4%-17.5%, SD 1.6, median 7%). HbA1c levels 7.0 were all statistically significantly associated with increased OR for development of CSME, and magnitude of OR for development of CSME increased with increasing HbA1c levels. Adjusted OR for CSME in those with HbA1c >6.5% compared to <6.5% was 4.75 (95% CI 1.57-21.06, p=0.004).
Conclusions: Risk of diagnosis of CSME after cataract surgery increases significantly with increase in preoperative HbA1c levels.
References: Shah AS, Chen SH. Cataract surgery and diabetes. Curr Opin Ophthalmol. 2010;21(1):4-9.
Yang J, Cai L, Sun Z, et al. Risk factors for and diagnosis of pseudophakic cystoid macular edema after cataract surgery in diabetic patients. J Cataract Refract Surg. 2017;43(2):207-214.

29 | New England Ophthalmological Society
POSTER #10
Endoscopic Visualization of Haptic Position in Glued IOL Implantation
Erica Liu Tufts Medical Center, Boston, MA
Zeina Salem, Amer Althawabi, David Lazar, Adam Lipma, David Ramsey, Susan MacDonald, Naveen Rao
Objective: To demonstrate the endoscopic view of haptic position in glued intraocular lens implantation, and to determine the potential consequences of using existing IOL models for glued IOL fixation.
Purpose: To demonstrate the endoscopic view of haptic position in glued IOL implantation, and to determine the potential consequences of using existing IOL models for glued IOL fixation.
Methods: A Marfan’s patient with lens subluxation underwent pars plana vitrectomy/lensectomy and glued IOL implantation with a 3-piece acrylic IOL. The IOL was inserted and the haptics were externalized and tucked into scleral tunnels 1mm posterior to the limbus. An endoscope was used to visualize the internal position of the haptics prior to closure.
Results: The haptics were seen going through the ciliary body. There was a right-angled kink of the haptic. Placing the sclerotomy sites 1.0 mm posterior the limbus may not be adequate to clear the ciliary body. This could increase the risk of vitreous hemorrhage.
Conclusion: To our knowledge, this is the first reported use of the intraocular endoscope for internal visualization of the haptics in glued IOL implantation.
References: Agarwal A, Kumar DA, Jacob S, Baid C, Agarwal A, Srinivasan S. Fibrin glue-assisted sutureless posterior chamber intraocular lens implantation in eyes with deficient posterior capsules. J Cataract Refract Surg. 2008 Sep;34(9):1433-8.
Kumar DA, Agarwal A, Packialakshmi S, Agarwal A. In vivo analysis of glued intraocular lens position with ultrasound biomicroscopy. J Cataract Refract Surg. 2013 Jul;39(7):1017-22.
Kumar DA, Agarwal A. Glued intraocular lens: a major review on surgical technique and results. Curr Opin Ophthalmol. 2013 Jan;24(1):21-9.

764th Meeting | 30
POSTER #11
Scleral-fixated Intraocular Lenses: Comparison Between Gore-tex-sutured Akreos and Fibrin-glued MA60AC
Melina Morkin, MD Tufts Medical Center, Boston, MA
Gregory Blaha, Shiyoung Roh, Susan MacDonald, David Ramsey, Jeffrey Chang, Fina Barouch, Naveen Rao
Objective: To compare scleral-sutured and scleral-glued intraocular lenses (IOLs).Methods: Retrospective review of demographics, surgical indications, best-corrected visual acuity (BCVA), and complications.
Results: n=15 (9 Gore-Tex-sutured B&L Akreos AO60, 6 fibrin-glued Alcon MA60AC). No significant differences were noted in demographics and preop VA, although some aphakes portended worse visual prognosis. Most common indications were IOL dislocation in the suture group (6/9) and aphakia in the glue group (4/6). LogMAR BCVA improved from 0.81±0.71 (20/132 Snellen) to 0.21±0.17 (20/32- p=0.02) with Akreos, and from 0.98±0.92 (20/193) to 0.58±0.78 (20/75- p=0.1) with MA60AC. Postoperative ocular hypertension (56% vs 17%) and inflammation (33% vs 17%) were more frequent in the suture compared to the glue group. Hypotony was more common in glued IOLs (33% vs 22%). Follow-up was 3.3 (1-13) and 8.4 months (1.3-15.5) for sutured and glued IOLs.
Conclusion: Sutured Akreos showed better visual outcomes but more complications compared to glued MA60ACs.
References: Khan MA, Gupta OP, Smith RG, Ayres BD, Raber IM, Bailey RS, Hsu J, Spirn MJ. Scleral fixation of intraocular lenses using Gore-Tex suture: clinical outcomes and safety profile. Br J Ophthalmol. 2016 May;100(5):638-43.
Ganekal S, Venkataratnam S, Dorairaj S, Jhanji V. Comparative evaluation of suture-assisted and fibrin glue-assisted scleral fixated intraocular lens implantation. J Refract Surg. 2012 Apr;28(4):249-52.
Brunin G, Sajjad A, Kim EJ, Montes de Oca I, Weikert MP, Wang L, Koch DD, Al-Mohtaseb Z. Secondary intraocular lens implantation: Complication rates, visual acuity, and refractive outcomes. J Cataract Refract Surg. 2017 Mar;43(3):369-376.

31 | New England Ophthalmological Society
POSTER #12
Incidence of Superior Oblique Palsy After Spacer Surgery for Treatment of Browns Syndrome:
An Honest Look at Residual Superior Oblique FunctionMedha Sharma, MD
Boston Children’s Hospital, Boston, MA
Sarah MacKinnon, Linda Dagi
Objective: The aim of our study was to describe the post-surgical outcomes in patients with Browns syndrome, and in particular, evaluating whether the alternative, suture spacer weakening procedure, causes less problems when looking down
Retrospective chart review of patients diagnosed with Brown syndrome and treated with suture spacer surgery was performed. Patients with simultaneous surgery on other vertical rectus or insufficiently detailed sensorimotor evaluation were excluded. Of 23 patients treated with suture spacer, 21 met inclusion criteria. Median age at surgery was 59 months (IQR 32 to 78 months). Pre-operative hypotropia in primary position, direct upgaze and affected side gaze was 10 PD (IQR 3 to 11PD), 18PD (IQR 14 to 25 PD) and 18 PD (IQR 10 to 23 PD) respectively. Browns limitation was -4 (IQR -3 to -4) and evidence of preoperative fusion or stereopsis was present in 71%. Spacers ranged from 2 to 9 mm with median of 6mm. At final outcome visit occurring median 16.5 months (IQR 5.5 to 26.5 months) post procedure, median residual Browns limitation was -1 (IQR 0 to -2) and vertical alignment in primary position was orthotropia (IQR 0 to 5 PD hypertropia), direct upgaze was 1 PD hypotropia (IQR 8 hypotropia to 2 PD hypertropia) and affected side gaze was 1 PD hypertropia (IQR 4 hypotropia to 5 PD hypertropia) .Twelve patients had good to excellent superior oblique function however 9 developed clinically significant superior oblique palsy, 4 of whom had surgical intervention. Size of spacer did not predict development of palsy.
References: Yazdian Z, Alamdari MA, Yazdian MA, et al.Superior oblique tendon spacer with application of non absorbable adjustable suture for treatment of Brown syndrome. JAAPOS 2008;405-408.
Santiago AP, Rosenbaum AL. Grave complications after superior oblique tenotomy for brown syndrome. JAAPOS 1997;1:8-15.
Suh DW, Oystreck DT, Hunter DG. Long term results of an intraoperative adjustable suture oblique tendon suture spacer using non absorbable suture for brown syndrome. Ophthalmology 2008;115:1800-1804.
764th Meeting | 32
POSTER #13
Bilateral Papilledema as Initial Presentation of Neurocysticercosis
Aubrey Tirpack, MD Tufts Medical Center, Boston, MA
Geetha Athappilly
Objective: To describe a unique case of bilateral papilledema as the initial presenting sign of subarachnoid neurocysticercosis.
A previously healthy 39-year-old male, with history of recent travel to Mexico, presented with a three-month history of headaches and blurred vision. Visual acuity was 20/70 OD and 20/25 OS with decreased color vision OD. Fundus examination showed bilateral pallid optic disc edema. Visual fields demonstrated bilateral blind spot enlargement and dense peripheral field loss. Initial MRI/MRV showed ventricular prominence. Lumbar puncture confirmed an elevated opening pressure of 37cm/H2O and CSF analysis revealed a leukocytosis with eosinophilic predominance. Repeat MRI with FIESTA (fast imaging employing steady state acquisition) sequence showed small cysts in the subarachnoid space. CSF cysticercosis IgG antibody was positive. The patient was started on albendazole, dexamethasone, and acetazolamide with subsequent resolution of optic disc edema and interval decrease in size of the subarachnoid cysts.
References: Brutto OHD. Neurocysticercosis. Handbook of Clinical Neurology Neurologic Aspects of Systemic Disease Part III. 2014:1445-1459.
Filho FEFM, Machado LDR, Lucato LT, Leite CC. The role of 3D volumetric MR sequences in diagnosing intraventricular neurocysticercosis: preliminary results. Arquivos de Neuro-Psiquiatria. 2011;69(1):74-78.
Mezo RC, García JL, Arroyo M, Fleury A. Relevance of 3D magnetic resonance imaging sequences in diagnosing basal subarachnoid neurocysticercosis. Acta Tropica. 2015;152:60-65.

33 | New England Ophthalmological Society
POSTER #14
Evaluation of Choroidal Lesions With Swept-source Optical Coherence Tomography
Cindy Ung, MD Massachusetts Eye and Ear Infirmary, Boston, MA
Ines Lains, Russell Woods, Anne Marie Lane, Thanos Papakostas, Deeba Husain, Joan Miller, Evangelos Gragoudas, Ivana Kim, John Miller
Objective: To explore the ability of swept-source optical coherence tomography (SS-OCT) to properly image choroidal lesions, and to identify the morphologic characteristics associated with optimal visualization.
Purpose: To explore the ability of swept-source optical coherence tomography (SS-OCT) to properly image choroidal lesions, and to identify the morphologic characteristics associated with optimal visualization.
Methods: Prospective, cross-sectional study, including patients with choroidal melanocytic lesions < 3 mm in thickness on ultrasound. All participants underwent color fundus photography (CFP), ultrasonography, and SS-OCT. For SS-OCT, we obtained a 3D horizontal volume (12 mm x 9 mm) and a radial protocol (12 lines) over the choroidal lesions. All images were evaluated by two independent graders. CFP were used to assess the degree of pigmentation of lesions. On SS-OCT we evaluated both qualitative (e.g. lesion outline, detection of scleral-choroidal interface, and quality of the image) and quantitative parameters (measurement of maximum lesion thickness and the largest basal diameter) defined a priori. The main outcome measure was the quality of the choroidal lesion images on SS-OCT, defined as: optimal - all margins of the lesion well visible; suboptimal - at least one margin not properly imaged; or poor - more than one margin not properly imaged. Probability of optimal image quality was examined using ordered logistic regression models.
Results: We included 85 choroidal lesions of 82 patients, mean age 65.8 ± 11.8 years. Fifty-nine percent (n=48) were female. There were 24 choroidal lesions (29%) for which image quality was classified as optimal, 31 lesions (37%) as suboptimal, and 30 lesions (36%) as poor. The factors associated with optimal image quality were distance closer to the fovea (OR 0.76, P < 0.001), posterior pole location (OR 3.87, P = 0.05), lower ultrasound thickness (OR 0.44, P = 0.04), lighter lesion pigmentation (OR 0.12, P = 0.003) and smaller lesion diameter (OR 0.73, p<0.001). In the multi-variable analysis, closer distance to the fovea (OR 0.81, P = 0.005), lighter lesion pigmentation (OR 0.11, P = 0.01) and smaller lesion diameter (OR 0.76, p=0.006) remained statistically significant.

764th Meeting | 34
POSTER #14 (continued)
Conclusion: SS-OCT is useful in imaging most choroidal melanocytic lesions. Image quality is best when the choroidal lesion is closer the fovea, has a smaller diameter and a lighter choroidal pigmentation.
References: Torres VL, Brugnoni N, Kaiser PK, et al. Optical coherence tomography enhanced depth imaging of choroidal tumors. Am J Ophthalmol 2011;151:586-593 e2. Shah SU, Kaliki S, Shields CL, et al. Enhanced depth imaging optical coherence tomography of choroidal nevus in 104 cases. Ophthalmology 2012;119:1066-72
Francis JH, Pang CE, Abramson DH, et al. Swept-source optical coherence tomography features of choroidal nevi. Am J Ophthalmol 2015;159:169-76 e1.

35 | New England Ophthalmological Society
POSTER #15
Choroidal Vascular Density and Volume in Diabetic Retinopathy with Swept Source Optical Coherence Tomography
Jay Wang, MD Massachusetts Eye and Ear Infirmary, Boston, MA
Ines Lains, Joana Providencia, Grayson Armstrong, Katherine Talcott, Pedro Gil, Joao Gil, Joao Heitor Marques, Joao Figueira, Ivana Kim, Joan Miller,
Deeba Husain, Silva Rufino
Objective: To understand the choroidal vascular changes that occur in diabetic retinopathy.
Purpose: To compare choroidal vascular density (CVD) and volume (CVV) of eyes with diabetic retinopathy (DR) with controls using en face swept-source optical coherence tomography (SS-OCT).
Methods: A multicenter, prospective, cross-sectional study of diabetic and non-diabetic eyes using SS-OCT. CVD and CVV were analyzed from binarized en face SS-OCT images. Diabetic eyes were divided into 4 groups: no DR, non-proliferative DR (NPDR), NPDR with macular edema (NPDR + DME), and proliferative DR (PDR). Multilevel mixed linear regression models were performed.
Results: We included 143 diabetic and 64 non-diabetic control eyes. CVD was significantly lower in eyes with NPDR + DME (ß = -0.0236, p = 0.045) and eyes with PDR (ß = -0.0350, p = 0.039). CVV was significantly lower in eyes with PDR (ß = -0.0061, p = 0.02).
Conclusions: CVD and CVV are significantly reduced with increasing DR severity. These findings provide further evidence for diabetic vascular choroidopathy.
References: Laíns I, Talcott KE, Santos AR, et al. Choroidal thickness in diabetic retinopathy assessed with swept-source optical coherence tomography. Retina. February 2017:1. doi:10.1097/IAE.0000000000001516. Tan K-A,
Laude A, Yip V, Loo E, Wong EP, Agrawal R. Choroidal vascularity index - a novel optical coherence tomography parameter for disease monitoring in diabetes mellitus? Acta Ophthalmol. 2016;94(7):e612-e616. doi:10.1111/aos.13044.
Melancia D, Vicente A, Cunha JP, Abegão Pinto L, Ferreira J. Diabetic choroidopathy: a review of the current literature. Graefe’s Arch Clin Exp Ophthalmol. 2016;254(8):1453-1461. doi:10.1007/s00417-016-3360-8.
764th Meeting | 36
POSTER #16
Outcomes in Micropulse Transcleral DiodeCyclophotocoagulation for Treatment of Refractory Glaucoma
Astrid Werner Tufts New England Eye Center, Boston, MA
Cynthia Mattox
Objective: To provide data from early experience with a new technology (micro-pulse CPC) in the treatment of refractory glaucoma.
Purpose: To examine the efficacy and side effect profile of micropulse CPC in the treatment of refractory glaucoma.
Methods: Retrospective chart review of patients who underwent micropulse CPC (mCPC) at the Tufts New England Eye Center and Ophthalmic Consultants of Boston between October 2015 and June 2016 (N=33 eyes). Included patients had refractory glaucoma, defined as IOP above target on maximal tolerated medical therapy. Success was defined as a drop in IOP to 21mmHg or lower and 20% or more decrease in IOP at 3 months. Failure was defined as not meeting success criteria, or need for incisional surgery.
Results: At 3 months, the average IOP change was 27 % (-8.5 mmHg), and the success rate was 52% - lower than reported in prior studies. There were no serious complications.
Conclusion: Micropulse CPC is safe and reasonably effective in reducing IOP in patients with glaucoma that is refractory to medical therapy.
References: D Aquino, MC et al., Micropulse versus continuous wave transscleral diode cyclophotocoagulation in refractory glaucoma: a randomized exploratory study, Clinical and Experimental Ophthalmology 2015; 43: 40–46.
Kuchar, S. et al, Treatment outcomes of micropulse transscleral cyclophotocoagulation in advanced glaucoma, Lasers Med Sci (2016) 31:393–396.
Tam, AM et al., Micropulse transscleral diode laser cyclophotocoagulation in the treatment of refractory glaucoma, Clinical and Experimental Ophthalmology 2010; 38: 266–272.

37 | New England Ophthalmological Society
POSTER #17
Nyctalopia as Presenting Symptom of New Onset Alcoholic Liver Failure
Astrid Werner Tufts New England Eye Center, Boston, MA
Thomas Hedges III
Objective: To guide appropriate clinical work up when evaluating patients presenting with nyctalopia and ERG changes secondary to Vitamin A deficiency.
Introduction: Vitamin A plays a crucial role in retinal phototransduction, and deficiency of this essential nutrient commonly produces nyctalopia and ERG changes as an early sign. In the United States, vitamin A deficiency due to dietary deficiency is rare. It is typically secondary to fat malabsorption or poor Vitamin A metabolism in the setting of systemic disease.
Method: Herein, we describe a case report of a 35 year old previously healthy male presenting with nyctalopia and ERG changes due to severe vitamin A deficiency. This was initially attributed to a fast-food only diet, but ultimately proved to be the presenting sign of new onset alcoholic liver failure.
Conclusion: In the United States, diet-related Vitamin A deficiency should be considered a diagnosis of exclusion, and a patient presenting with nyctalopia and ERG changes concerning for vitamin A deficiency, should have a systemic work up looking for another etiology.
References: Imdad A, Herzer K, Mayo-Wilson E, et al. Vitamin A supplementation for preventing morbidity and mortality in children from 6 months to 5 years of age. Cochrane Database Syst Rev 2010; :CD008524. World Health Organization, Global Prevalence of Vitamin A Deficiency in Populations at Risk 1995–2005. WHO Global Database on Vitamin A Deficiency. Geneva, Switzerland World Health Organization2009

764th Meeting | 38
POSTER #18
Evaluation of Postoperative Refractive Outcomes of Glued Intraocular Lens Implantation
Astrid Werner Tufts New England Eye Center, Boston, MA
Naveen Rao, Susan MacDonald
Objective: To assist surgeons when selecting the intraocular power for glued IOL implantation for a plano refractive result, as this can be difficult due to uncertainty about effective lens position and variability in patient anatomy.
Purpose: To determine the ideal refractive target for glued IOL implantation.
Methods: Non-comparative case series. 6 patients with aphakia and no capsular support underwent glued IOL implantation with a plano refractive target from 2015–2016.
Results: For 4 patients, IOL power was adjusted for sulcus positioning (reduced by 0.5-1.0 D from in-bag power) and mean post-op spherical equivalent was +0.25 D (plano, plano, +2.00 D, and -1.00 D). In this group, the two patients with a refractive surprise had prior corneoscleral surgery. The remaining 2 patients had no sulcus-adjustment made to IOL power, and were plano, but had limited visual potential prior to surgery.
Conclusion: For glued IOL implantation in patients without prior corneoscleral surgery, selecting an IOL for a plano target and adjusting for sulcus positioning is likely to achieve a plano refractive outcome.
References: Kumar DA, et al., Glued posterior camber IOL in eyes with deficient capsular support: a retrospective analysis of 1-year post operative outcomes, Eye, 2010 24, 1143-1148.
Kumar DA et al., Complications and visual outcomes after glued foldable intraocular lens implantation in eyes with inadequate capsules. J Cataract Refract Surg 2013; 39:1211-1218.

39 | New England Ophthalmological Society
As a provider accredited by the Massachusetts Medical Society, NEOS must ensure balance, independence, objectivity, and scientific rigor in all its individually and jointly provided educational activities. All individuals in a position/role to control the content of an activity are expected to disclose to NEOS any relevant financial relationships they and their spouse/partner have with commercial interests.
The ACCME defines a commercial interest as any entity producing, marketing, reselling or distributing health care goods or services consumed by, or used on, patients. Relevant financial relationships are financial relationships in any amount, which occurred in the twelve-month period preceding the time that the individual was asked to assume a role controlling content of the CME activity, and which relate to the content of the educational activity.
Financial relationships are those relationships in which the individual benefits by receiving a salary, royalty, intellectual property rights, consulting fee, honoraria, ownership interest (e.g., stocks, stock options or other ownership interest, excluding diversified mutual funds), or other financial benefit. Financial benefits are usually associated with roles such as independent contractor (including contracted research), consulting, promotional speaking and teaching, membership on advisory committees or review panels, board membership, and other activities for which remuneration is received or expected. The MMS/ACCME considers relationships of the person involved in the CME activity to also include financial relationships of a spouse or partner.
Bradbury, Michael: Ownership Interest: Regeneron, Chase and Associates, Inc (Iviews imaging system)
Christiansen, Stephen: Other type: AbbVie, provide in-house training for uveitis team
Duker, Jay: Consulting Fees: Alcon/Novartis, CoDa Therapeutics, Thrombogenics, Allergan Lumenis, Santen Contracted Research: Carl Zeiss Meditec, Optovue Ownership Interest: Hemera Biosciences, EyeNetra, Ophthotech Other Types - Eleven Biotherapeutics (Board of Directors)
Greenfield, David Consultant: Allergan, Alcon, Bausch & Lomb, Aerie, Quark, Glaukos Grosskreutz, Cynthia Salary: Novartis
FINANCIAL DISCLOSURE INFORMATION
764th Meeting | 40
FINANCIAL DISCLOSURE INFORMATION (continued)
Heier, Jeffrey:Consulting Fees: Aerpio, Alcon/LPath, Allergan, Avalanche, Bayer, Dutch Oph-thalmics, Endo Optiks, EyeGate, Foresight Biotherapeutics, Forsight Vision4, Genentech, Heidelberg Engineering, Icon Therapeutics, Janssen R&D, Kala Pharmaceuticals, Kanghong, Kato Pharmaceuticals, Notal Vision, Novartis, Ohr Pharmaceuticals, Optovue, QLT, Quantel, Regeneron, RestorGenex, RetroSense, Santen, Shire, Stealth Biotherapeutics, Thrombogenics, Valeant, Vision Medi-cines, XcoveryContracted Research: Acucela, Alcon/LPath, Allergan, Astellas, Corcept, Genentech, Kala Pharmaceuticals, Kato Pharmaceuticals, Novartis, Ohr Pharmaceuticals, Ophthotech, QLT, Quantel, Regeneron, Sanofi/Genzyme, Stealth Biotherapeutics, Thrombogenics
Miller, Joan Royalty: Valeant Pharmaceuticals (licensee); Massachusetts Eye and Ear Infirmary
(assignee): Royalties related to photodynamic therapy for conditions involving unwanted ocular neovascularization. Elsevier: Royalties related to textbook
Receipt of Intellectual Property Rights / Patent Holder: Valeant Pharmaceuticals (licensee); Massachusetts Eye and Ear Infirmary (assignee): Intellectual property rights related to photodynamic therapy for conditions involving unwanted ocular neovascularization ONL Therapeutics (licensee); Massachusetts Eye and Ear Infirmary (assignee): Intellectual property rights related to methods and compositions for preserving photoreceptor viability.
Consulting Fees: Alcon Research Council (advisory board), 2011-09-01 to present Amgen, Inc., 2014-09-18 to 2015-09-18 KalVista Pharmaceuticals, 2012-03-31 go present Maculogix, Inc., 2013-10-03 to present (non-remunerative 2013-10-03 to 2015-05-01).
Contracted Research: Lowy Medical Research, Ltd., A natural history observation and registry study for macular telangiectasia type 2: The Mactel Study
Noecker, RobertConsulting Fees: Allergan, Alcon, Inotek, Aerie, Ocular Therapeutics, Kateena, BVI, Iridex, Quantel, Santen, Glaukos, Shire, Sun, Polyactiva, Diopsys, Ethis Communications, SOLXFees for Non-CME Services Received Directly from Commercial Interest or their Agents - Allergan, Alcon, Inotek, Aerie, Ocular Therapeutics, Kateena, BVI, Iridex, Santen, Iridex, Glaukos, DiopsysContracted Research: Allergan, Glaukos, SantenOwnership Interest: Ocular Therapeutics

41 | New England Ophthalmological Society
FINANCIAL DISCLOSURE INFORMATION (continued)
Pasquale, Louis Salary: Bausch & Lomb Inc. Consulting Fees: Eyenovia Contracted Research: NEI
Sun, Jennifer Other Type: Boston Micromachines – loaned research equipment; Optovue – loaned research equipment
NO FINANCIAL INTERESTNone of the other individuals in a position to control the content of this activity, including planners, CME Review Committee members, faculty presenters, moderators, panelists and reviewers have any relevant financial relationship with an ACCME-defined commercial interest to disclose.
764th Meeting | 42
The following candidates have submitted application for membership and letters of support have been received by sponsors:
Candidate Sponsor Sponsor
Robert Levy, MD Randall Patkin, MD Robert Freedman, MD marblehead, ma salem, ma salem, ma
Veena Mathew, MD, MPH Anita Shukla,MD Kimberly Hsu, MD needham, ma boston, ma boston, ma
John Miller, MD Demetrios Vavvas, MD John Loewenstein, MD boston, ma boston, ma boston, ma Veena Rao, MD Angela Turalba, MD Silas Wang, MD boston, ma boston, ma boston, ma
Melissa Wong, MD Anthony Correnti, MD Kimberly Licciardi, MD salem, nh manchester, nh manchester, nh
CANDIDATES FOR MEMBERSHIP
43 | New England Ophthalmological Society
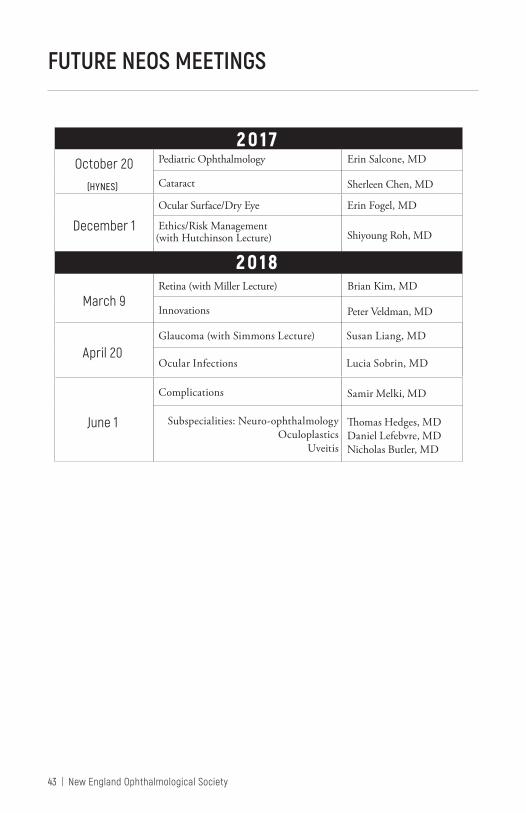
FUTURE NEOS MEETINGS
20 1 7 October 20
(HYNES)
Pediatric Ophthalmology Erin Salcone, MD
Cataract Sherleen Chen, MD
December 1
Ocular Surface/Dry Eye Erin Fogel, MD
Ethics/Risk Management (with Hutchinson Lecture) Shiyoung Roh, MD
20 18
March 9 Retina (with Miller Lecture) Brian Kim, MD
Innovations Peter Veldman, MD
April 20 Glaucoma (with Simmons Lecture) Susan Liang, MD
Ocular Infections Lucia Sobrin, MD
June 1
Complications Samir Melki, MD
Subspecialities: Neuro-ophthalmology Oculoplastics
Uveitis
Thomas Hedges, MD Daniel Lefebvre, MD Nicholas Butler, MD
764th Meeting | 44
THE BOARD AND COMMITTEES 2016-2017
The BoardPresident, Jeffrey Heier, MD John Dagianis, MD, President-elect Laura Fine, Vice-President; Chair Admissions Committee Mary Daly, MD, Secretary Joseph Levy, MD, Treasurer, Chair Finance Committee David Lawlor, MD, Immediate Past President, Chair Policies and Nominating Committees Joel Geffin, MD, Past President, Chair Program Committee Joan Miller, MD, Past President Michael Price, MD, Chair Educational Endowment Fund Committee Phil Aitken MD, Chair Ophthalmic Services Committee Brendan McCarthy, MD, Chair Public Health and Education Committee Jorge Arroyo, MD, Chair Information Technology Committee Michael Bradbury, MD, Executive Director c omm i t t e e s :
Executive CommitteeJeffrey Heier, MD, President John Dagianis, MD, President-elect Joseph Levy, MD, Treasurer Michael Bradbury, MD, Executive Director (ex officio) Admissions CommitteeLaura Fine, MD, Chair John Dagianis, MD Jeffrey Heier, MD
Finance CommitteeJoseph Levy, MD Chair Joel Geffin, MD Jeffrey Heier, MD John Dagianis, MD (ex officio) Michael Bradbury, MD (ex officio) Nominations CommitteeDavid Lawlor, MD, Chair Ann Bajart, MD (MA) Mitchell Gilbert, MD (CT) Elliot Perlman, MD (RI) Christopher Soares, MD (VT) David Weinberg, MD (NH) Charles Zacks, MD (ME) ex officio members: Drs. Bradbury, Daly, Dagianis, Heier, Levy Program CommitteeJoel Geffin, MD, Chair Fina Barouch, MD Jay Duker, MD Geoffrey Emerick, MD Gena Heidary, MD Jeremy Kieval, MD Carolyn Kloek, MD Robert Noecker, MD Lawrence Piazza, MD Michael Yoon, MD David Lawlor, MD (ex officio) Jeffrey Heier, MD (ex officio) Michael Bradbury (ex officio) Joan Miller, MD (ex officio) Public Health and Education CommitteeBrendan McCarthy, MD, Chair Macie Finkelstein, MD

45 | New England Ophthalmological Society
THE BOARD AND COMMITTEES 2016-2017 (continued)
Magdalena Krzystolik, MD Joseph Levy, MD Robert Lytle, MD Vasiliki Poulaki, MD Susannah Rowe, MD Cathryn Welch, MD Michael Wiedman, MD Laura Fine, MD (ex officio) Jeffrey Heier, MD (ex officio) Society Policies CommitteeDavid Lawlor, MD, Chair Jeffrey Heier, MD John Dagianis, MD Michael J. Bradbury, MD Ophthalmic Services CommitteePhil Aitken, MD, Chair Timothy Blake, MD Nicoletta Fynn-Thompson, MD Kathryn Hatch, MD Edward Jaccoma, MD Marc Leibole, MD Erin Lichtenstein, MD Cynthia Mattox, MD Lauren Shatz, MD Trexler Topping, MD David Vazan, MD Peter Zacharia, MD Laura Fine, MD (ex officio) John Dagianis, MD (ex officio) Committee for Educational Endowment FundMichael Price, MD, Chair Thomas Coghlin, MD Francis D’Ambrosio, MD Richard Dornfeld, MD Mathew Gardiner, MD Grace Lee, MD
Christopher Newton, MD David Lawlor, MD Joseph Levy, MD Information Technology CommitteeJorge Arroyo, MD, Chair Ankoor Shah, MD Johanna Seddon, MD Nauman Chaudhry, MD Elliot Perlman, MD, (emeritus) Young Ophthalmologists CommitteeJeffrey Heier, MD, Chair Steven Anesi, MD Jorge Arroyo, MD Thomas Berenberg, MD Michael Bradbury, MD Jennifer Garvey, MD Gena Heidary, MD Elizabeth House, MD Daniel Lefebvre, MD Christina Moon, MD Joshua Ney, MD Michael Price, MD Anita Shukla, MD
Judith Cerone Keenan, Executive Assistant

764th Meeting | 46
1884-86 Hasket Derby 1887-88 Oliver F. Wadsworth 1889-90 H. G. Miller 1891-92 B. Joy Jefferies 1893-94 Henry L. Shaw 1895-96 Samuel B. St. John 1897-98 Myles Standish 1899-00 J. J. Putnam 1901-02 Franklin P. Capron 1903-04 H. Beckles Chandler 1905 David Coggin 1906-07 Alexander Quackenboss 1908 Charles H. Williams 1909 Edwin E. Jack 1910 Frederick F. Rodgers 1911 Allen Greenwood 1912 Henry W. Kilburn 1913 David Harrower 1914-15 Walter B. Lancaster 1916-17 Henry H. Haskell 1918-19 Ralph Carlton 1920 Fred M. Spalding 1921-22 Frederick H. Verhoeff 1923 William N. Souter 1924 George S. Derby 1925 Peter H. Thompson 1926-27 Edward K. Ellis 1928-29 W. Holbook Lowell 1930-31 S. Judd Beach 1932 David W. Wells 1933-34 Hugo B. C. Reimer 1935-37 James J. Regan 1938 Edwin B. Goodall 1939 J. Herbert Waite 1940 William D. Rowland 1941 Erastus E. Holt, Jr. 1942 Harry C. Messinger
1943 Paul A. Chandler 1944 Warren E. Kershner 1945 Theodore L. Terry 1946 Howard Hill 1947 Edwin B. Dunphy 1948 John E. Rice 1949 Benjamin Sachs 1950 Milton F. Little 1951 William P. Beetham 1952 Andrew L. MacMillan, Jr 1953 Merrill J. King 1954 Frank W. Dimmitt 1955 Trygve Gundersen 1956 Edward A. Cramton 1957 Virgil G. (Glenn) Casten 1958 Henry L. Birge 1959 Brendan D. Leahy 1960 David G. Cogan 1961 Lawrence Dame 1962 Mahlon T. Easton 1963 Dewey Katz 1964 Garrett L. Sullivan 1965 Albert E. Sloane 1966 H. Frederick Stephens 1967 Earl S. Seale 1968 Richard H. Dennis 1969 Henry A. Mosher 1970 Carl C. Johnson 1971 Sumner Liebman 1972 Harry E. Braconier 1973 Karl Reimer 1974 Abraham Pollen 1975 W. Morton Grant 1976 William B. Brewster, Jr 1977 Taylor R. Smith 1978 Hanford I. Auten 1979 Robert J. Brockhurst
1980 David H. Scott 1981 Joseph Dowling 1982 Robert Lawlor 1983 Dexter Clough II 1984 Hal M. Freeman 1985 Thomas Kleh 1986 Ralph H. Hinckely 1987 Irwin T. Mancall 1988 Richard J. Simmons 1989 Andrew J. Gay 1990 George P. Santos 1991 Y. Jacob Schinazi 1992 Lloyd M. Aiello 1993 Phil A. Aitken 1994 George Edw. Garcia 1995 Lewis N. Stieglitz 1996 B. Thomas Hutchinson 1997 Martin Wand 1998 C. Davis Belcher III 1999 Harold A. Woodcome Jr. 2000 Sheldon M. Buzney 2001 William E. Clark, Jr 2002 Michael J. Bradbury 2003 Kathleen J. Maguire 2004 Ann M. Bajart 2005 Paul M. Pender 2006 Joseph J. Greco 2007 Elliot M. Perlman 2008 Stuart M. DuBoff 2009 Charles Zacks 2010 C. Mitchell Gilbert 2011 Gerald Spindel2012 Shiyoung Roh 2013 Joan Miller 2014 Joel Geffin2015 David Lawlor2016 Jeffrey Heier
NEOS PAST PRESIDENTS 1884–2016
The New England Ophthalmological Society is one of the oldest continually meeting regional ophthalmological societies in the United States. Dedicated to education in ohthalmology and the public, as well as the highest standards in opthalmic care and ethics, the New England Ophthalmological Society stands as a keystone of our New England ophthalmic heritage.
47 | New England Ophthalmological Society
TODAY’S EXHIBITORS (at time of printing)
Akorn847.739.5764www.akorn.com
Alcon - SPONSOR817.615.2448www.alconlabs.com
Allergan - SPONSOR714.246.4491www.allergan.com
Bausch and Lomb- SPONSOR949.916.9352www.bausch.com
Beaver-Visitec Intl 781.906.7939www.beaver-visitec.com
Bio-Tissue508.808.3017www.biotissue.com
Carl Zeiss Meditec925.557.4158www.meditec.zeiss.com
Carr Healthcare Realty303.242.2224www.carrhr.com
Codex Techworks614-486-9900 www.codextechworks.com
Eversight CT860.223.2020Eversightvision.org
Heidelberg Engineering 800.931.2230www.HeidelbergEngineering.com
Johnson & Johnson Vision
KeraLink, Int.410.752.3800Keralink.org Lumenis408.764.3824 www.lumenis.com
Mallinckrodt Pharmaceuticals908.238.6758www.mallinckrodt.com
Marco904.642.9330www.marco.com
Microsurgical Technology425.556.0544www.microsurgical.com
Nova Bay351.201.9593Novabay.com
Novartis862.778.8300www.novartis.com
Ocular Therapeutix781.357.4049www.ocutx.com
OIC 781-341-1070www.OIC2020.com
Optovue510.897.1576 optovue.com
Prodigy Health508.254.7520Prodigyhealth.com
Regeneronwww.regeneron.com
Rhein Medical 727.209.2244
Sightlife 336.516.9600 sightlifesurgical.com
Sun Ophthalmics609.720.1155www.sunpharma.com
TearScience919.459.4837Tearscience.com
Vision Share312.469.5509www.visionshare.org
764th Meeting | 48
All Donors, please pick up an EEF Ribbon at registration towear at meetings.
Diamond Patrons $100,000 or moreDr. Michael J. Bradbury In memory of Dr. C. Davis Belcher In honor of Dr. Hal M. Freeman Massachusetts Eye and Ear InfirmaryIn honor of Dr. Joan MillerDr. and Mrs. Paul M. Pender In Memory of Paul D. Pender and Harry V. CareyDr. and Mrs. Richard J. Simmons In memory of Dr. Ruthanne SimmonsOphthalmic Consultants of BostonPhysicians and Patients In honor of Dr. B. Thomas Hutchinson
Platinum Patrons $10,000 to $99,999Boston Eye Research In memory of Dr. Sanford HechtDr. John Dagianis In honor of Dr. Hal M. Freeman, James and Eleanor Dagianis, and Paul and Verna DobbinsDr. and Mrs. Stuart DuBoff In memory of Dr. Ruthanne Simmons In honor of Samuel and Gloria DuBoff and William and Diane BrownDr. Hal M. FreemanDr. Albert R. Frederick, Jr. In honor of B. Thomas HutchinsonDr. and Mrs. Joseph J. Greco HOYA Optical LaboratoriesDr. B. Thomas HutchinsonNew Hampshire Society of Eye Physicians and Surgeons
Dr. Delia Sang and Dr. Mark Hughes In memory of Dr. Charles L. SchepensDr. Gerald Spindel In honor of Israel and Rose Spindel and Benjamin Burch
Gold Patrons $3,000-$9,999Drs. A. Robert and Jean Bellows In memory of Dr. W. Morton Grant Dr. and Mrs. Paul P. Dunn In memory of Dr. C. Davis Belcher and in honor of Dr. A. Robert Bellows
Dr. C. Mitchell Gilbert In honor of Drs. Claes Dohlman, Kenneth Kenyon, and Martin Wand The Health Foundation of Central Massachusetts In honor of Dr. Michael J. BradburyDr. Jean Keamy for the Keamy Family Foundation In memory of Donald and Yvonne KeamyMaine Society of Eye Physicians and SurgeonsNew England Lens Implant Society In memory of Dr. Sanford HechtDr. and Mrs. Donald Kaplan In memory of Dr. Robert VernlundDr. and Mrs. Elliot Perlman In memory of Drs. C. Davis Belcher and Kathleen MaguireDr. Shiyoung Roh and Mrs. Myung Ja RohDrs. Helen and Jack Schinazi In memory of Dr. C. Davis BelcherDr. and Mrs. John Sebestyen In memory of Dr. Taylor R SmithDr. Bradford J. Shingleton In honor of Drs. Albert R. Frederick, B. Thomas Hutchinson, Silvio Von Pirquet
EDUCATIONAL ENDOWMENT FUND DONORS
49 | New England Ophthalmological Society
and A. Robert BellowsDrs. Richard and Ruthanne Simmons In memory of Dr. W. Morton GrantDr. and Mrs. Richard J. Simmons In memory of Drs. Paul A Chandler, W. Morton Grant, Ruthanne Simmons, and C. Davis BelcherDr. and Mrs. Paul Wasson In memory of Dr. Paul Wasson In memory of Dr. Oscar HollanderDr. and Mrs. Hal Woodcome In memory of Dr. Harold Woodcome, Sr.Estate of Dr. Leon Zimmerman
Silver Patrons$1,000-$2,999
Dr. Reid S. Appleby, Jr. In honor of Dr. Harold Woodcome, Jr., and AssociatesDr. and Mrs. Lloyd M. AielloDr. Jorge ArroyoDr. Ann BajartDr. C. Davis Belcher In honor of Dr. Richard SimmonsDr. Harry Braconier In memory of Drs Taylor Smith, Karl Riemer, Carl C. Johnson. In honor of Dr. Hal M. FreemanDr. and Mrs. Sheldon M. BuzneyChildren’s Hospital Ophthalmology FoundationDr. and Mrs. William E. Clark, Jr.Dr. Thomas Coghlin In honor of Dr. Ira Asher and Dr. Kevin O’Brien Dr. Joseph L. Dowling, Jr.Dr. Jay S. DukerEye Health Services In memory of Dr. C. Davis BelcherDr. Laura FineDr. Joel Geffin
Dr. and Mrs. David GreenseidDr. Bernard HeersinkDr. Jeffrey Heier Dr. Ralph HinckleyDr. William S. Holt Dr. Robert T. LacyDr. Joseph Levy In honor of Dr. Thomas Hedges IIIDr. Byron S. LingemanDr. Richard LowDr. Kathleen Maguire and Stephen Burke In honor of Dr. Hal M. FreemanDr. Lisa McHamDr. Clifford Michaelson In memory of Dr. Jesse and Mrs. Ruth Lee MichaelsonDr. Stanislaw Milewski In memory of Dr. Taylor R. Smith Dr. Peter B. Mooney In memory of Dr. Henry F. AllenDr. Paul MoultonDr. Stephen J. PhippsDr. and Mrs. Michael PriceDr. Michael RaizmanDrs. Shiyoung Roh and John WeiterDr. and Mrs. George Santos Dr. Delia Sang In honor of Dr. Lloyd M. AeilloDrs. Jack and Helen Schinazi In memory of Mrs. Mary Santos In honor of Dr. Irving L. PavloDr. Roger F. Steinert In honor of Drs. A. Robert Bellows, S. Arthur Boruchoff, Albert R. Frederick, and B. Thomas HutchinsonDr. J. Elliott TaylorDr. Felipe I. Tolentino In honor of Drs. Hal M. Freeman and Roland Houle In memory of Dr. Charles L. SchepensDr. Trexler R. ToppingVermont Ophthalmological SocietyDr. Martin Wand
EDUCATIONAL ENDOWMENT FUND DONORS (continued)

764th Meeting | 50
In memory of Dr. W. Morton GrantDrs. Peter Wassermann, T. Gordon Hand, Christie Morse and Bradford Hall, In memory of Dr. John Detwiller In honor of Dr. Lewis StieglitzMaster William Weiter In honor of Ann Bajart and Tony Schemmer, and Deborah and Elliot PerlmanDr. Kenneth WolfDr. Allen Zieker Benefactors $500-$999
Dr. Phil Aitken In memory of Drs. Robert Guiduli and Simmons LessellDr. William AtleeDrs. Elliot and Macie FinkelsteinDr. May DalyDr. David Fleishman In memory of Dr. Gary B. Fleishman Dr. George GarciaDr. Robert Guiduli In memory of Dr. Kathleen J. MaguireDr. Lynne KaplinskyDr. Robert LytleMaine Eye CenterDr. and Mrs. Howard MartonDr. Christopher NewtonOphthalmic Consultants of BostonRetina Center of MaineRhode Island Society of Physicians and Surgeons Dr. Joel SchumanDr. Lewis StieglitzDr. Dennis StolerDr. Barry WepmanDr. Charles Wingate
Sponsors $250-$499 Dr. Caroline Baumal In memory of Dr. Jose BerrocalDr. Michael Cooper In memory of Dr. Robert Haimovici and Dr. Behrooz KoleiniDr. Francis Y. Falck, Jr.Dr. Ralph A. Goodwin, Jr.Dr. Timothy GosleeDr. Dana GraichenDr. Payson B. Jacobson In memory of Dr. Abraham Pollen Dr. Glenn P. KimballDr. Peter LouDr. Brendan McCarthy In Memory of Dr. Behrooz KoleiniDr. Carmen PuliafitoDr. Sarkis Soukiasian In Honor of Dr. Roger SteinertDr. Caldwell W. SmithDr. Neal G. SneboldDr. Jonathan TalamoDr. Yvonne Tsai In memory of Helena ToksozDr. Andrew Wong In memory Dr. Charles L. Schepens Worcester Ophthalmology Associates Dr. Charles Zacks
Friends Up to $250
In Memory of C. Davis Belcher Accent Eyewear James Bernson Dr. Charles Beyer-Machule Philip Cacciatore Eye Health Services Milton Feinson Dr. Richard Getnick Evelyn John Dr. Ernest Kornmehl Don Lesieur Joyce Marshall
EDUCATIONAL ENDOWMENT FUND DONORS (continued)

51 | New England Ophthalmological Society
Rebecca Murphy Therese O’Keefe Dr. Stephen Poor, III Eileen Raffferty Elizabeth Reece Dr. Richard Simmons Marian Spilner Dr. Ann Stromberg Elizabeth Sullivan Andrienne Tashjian The Rivers SchoolIn Memory of Dr. Peter Gudas: Naomi Litrowinik Mercedes Sayler Needham Psychotherapy Associates New England Carpenters Health Fund Norfolk Lodge A.F. and A.M. James and Jean TwyningJacqueline PepperJeanne SmithDr. Peter BatsonDr. Richard BrownDr. David CorbitDr. Paul Cotran In memory of Dr. Mariana Mead Dr. Peter DonshikDr. Stuart Fay In honor of Dr. Michael Bradbury and Dr. TuckMelvyn and Eleanor Galin Foundation In honor of B. Thomas HutchinsonDr. Andrew Gillies In memory of Dr. Moshe LahavDr. Timber GormanDr. Jay Gooze In memory of Kirstyn SmithDr. Amy GregoryDr. Walter GriggsDr. Robert HermDr. Ted HouleDr. Glenn P. KimballDr. Howard M. Leibowitz In memory of Dr. Behrooz Koleini
Dr. Clifford Michaelson In memory of Dr. Behrooz KoleiniDr. Lawrence PiazzaDr. Theodore RennaMolly-Jane Isaacson Rubinger In honor of Trexler ToppingDr. Domenic M. StrazzullaDr. Carter TallmanDr. Michael Wiedman In honor of Dr. Claes Dohlman
EDUCATIONAL ENDOWMENT FUND DONORS (continued)
764th Meeting | 52
NOTES
53 | New England Ophthalmological Society
NOTES

Please mark your calendar to join us!
Annual meetings for Ophthalmic Personnel
OCTOBER 20, 2017 | HYNES CONVENTION CENTER
OPHTHALMIC NURSES AND TECHNICIANS
OPHTHALMIC PRACTICE ADMINISTRATIONS, MANAGERS
AND SUPERVISORS
WATCH WEB SITE FOR TOPICS/UPDATES/REGISTRATIONwww.neos-eyes.org

www.neos-eyes.org