Updates in Pediatrics · in management of severe bronchiolitis in PICU. Heliox for bronchiolitis...
92
Updates in Pediatrics Mimi Lu, MD Clinical Assistant Professor Director, Pediatric Emergency Medicine Education University of Maryland School of Medicine Baltimore, Maryland
Transcript of Updates in Pediatrics · in management of severe bronchiolitis in PICU. Heliox for bronchiolitis...
Updates in Pediatrics
Mimi Lu MD
Clinical Assistant Professor
Director Pediatric Emergency Medicine Education
University of Maryland School of Medicine
Baltimore Maryland
No relevant financial disclosures
Outline
Recent literature pertaining to
Acute respiratory illnesses
Sepsis
Abdominal disorders
Questions mluemumarylandedu
RESPIRATORY
Case
15 month male with 3 day cough
congestion rhinorrhea
VS T 384 HR 130 RR 26 BP 7540 94
Exam smiling wheezing mild retractions
Case
15 month male with 3 day cough
congestion rhinorrhea
VS T 384 HR 150 RR 50 BP 7540 90
Exam wheezing mod retractions
Bronchiolitis
Clinical Practice Guideline
Diagnosis
Based on HampP
No routine labs or radiographs
Risk factors
age lt 12 weeks prematurity underlying CP
disease immunodeficiency
Ralston et al Pediatrics 2014
Clinical Practice Guideline
Treatment
Albuterol
Epinephrine
Steroids
Hypertonic saline
Ralston et al Pediatrics 2014
Skjerven et al NEJM 2013
Eight center randomized double-blind trial
404 infants
Conclusion
Inhaled racemic adrenaline is not more effective than inhaled saline
The strategy of inhalation on demand appears to be superior to that of inhalation on a fixed schedule
Clinical Practice Guideline
Treatment
Supplemental oxygen
Continuous pulse oximetry
Antibiotics
Fluids
Ralston et al Pediatrics 2014
High Flow Nasal Cannula
Wing et al Pediatr Emerg Care 2012
PED to PICU with ARI over 4 years
HFNC success rates 84-88
Decreased intubation rate
Decreased ventilator utilization by 50
No difference PICU LOS mortality or mean
duration of mechanical ventilation
HFNC
Conclusion
HFNC decreased need for intubation and
mechanical ventilator utilization for
children in the PED admitted to PICU
with ARI particularly when initiated early
HFNC vs nCPAP
Metge et al Eur J Pediatr 2014 Jul
Retrospective review
French PICU
2 consecutive bronchiolitis seasons
Conclusion
No difference between RR HR FiO2 CO2
in management of severe bronchiolitis in PICU
Heliox for bronchiolitis
Chowdhury et al Pediatrics 2013
Bronchiolitis Randomized Controlled Trial
Emergency-Assisted Therapy with
HelioxmdashAn Evaluation (BREATHE)
Largest multicenter randomized
controlled trial investigating efficacy of
Heliox in acute bronchiolitis
Heliox for bronchiolitis
Conclusion
Heliox therapy does not reduce length of
treatment unless given via a tightfitting
facemask or CPAP
Nasal cannula heliox therapy is ineffective
Corticosteroid timing and length of stay for children with
asthma in the Emergency Department
Davis SR Burke G Hogan E Smith SR
Asthma
Asthma and steroids
Conclusion
Early steroid administration decreases time to
clinical improvement and discharge and reduced
admission rates in children presenting with
moderate to severe acute asthma
exacerbations
Steroids in asthma
Dexamethasone vs prednisone
Keeney et al Pediatrics 2014
Redman Arch Dis Children 2013
Williams et al Clin Pediatr 2013
Steroids in asthma
Conclusions (dexamethasone)
Equal efficacy
Shorter duration of treatment
Less vomiting
Improved compliance
Parental preference
Take home points
Consider high flow nasal cannula in
patients with acute respiratory illness
Early steroids for asthma
Dexamethasone gt prednisone
SEPSIS
Case Altered Mental Status
Case
65 yo ldquonot acting rightrdquo
rsaquo vomiting diarrhea fevers
PMHx None
Meds None
VS
T 392 P 118 RR 24 BP 8051 100 RA
101
128 38 7551187 58 6038
Recognition
Bimodal distribution
Predisposing conditions
Recent surgery
Unexplained tachycardia
Impaired perfusion
Delayed capillary refill
Lethargy
Irritability
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
No relevant financial disclosures
Outline
Recent literature pertaining to
Acute respiratory illnesses
Sepsis
Abdominal disorders
Questions mluemumarylandedu
RESPIRATORY
Case
15 month male with 3 day cough
congestion rhinorrhea
VS T 384 HR 130 RR 26 BP 7540 94
Exam smiling wheezing mild retractions
Case
15 month male with 3 day cough
congestion rhinorrhea
VS T 384 HR 150 RR 50 BP 7540 90
Exam wheezing mod retractions
Bronchiolitis
Clinical Practice Guideline
Diagnosis
Based on HampP
No routine labs or radiographs
Risk factors
age lt 12 weeks prematurity underlying CP
disease immunodeficiency
Ralston et al Pediatrics 2014
Clinical Practice Guideline
Treatment
Albuterol
Epinephrine
Steroids
Hypertonic saline
Ralston et al Pediatrics 2014
Skjerven et al NEJM 2013
Eight center randomized double-blind trial
404 infants
Conclusion
Inhaled racemic adrenaline is not more effective than inhaled saline
The strategy of inhalation on demand appears to be superior to that of inhalation on a fixed schedule
Clinical Practice Guideline
Treatment
Supplemental oxygen
Continuous pulse oximetry
Antibiotics
Fluids
Ralston et al Pediatrics 2014
High Flow Nasal Cannula
Wing et al Pediatr Emerg Care 2012
PED to PICU with ARI over 4 years
HFNC success rates 84-88
Decreased intubation rate
Decreased ventilator utilization by 50
No difference PICU LOS mortality or mean
duration of mechanical ventilation
HFNC
Conclusion
HFNC decreased need for intubation and
mechanical ventilator utilization for
children in the PED admitted to PICU
with ARI particularly when initiated early
HFNC vs nCPAP
Metge et al Eur J Pediatr 2014 Jul
Retrospective review
French PICU
2 consecutive bronchiolitis seasons
Conclusion
No difference between RR HR FiO2 CO2
in management of severe bronchiolitis in PICU
Heliox for bronchiolitis
Chowdhury et al Pediatrics 2013
Bronchiolitis Randomized Controlled Trial
Emergency-Assisted Therapy with
HelioxmdashAn Evaluation (BREATHE)
Largest multicenter randomized
controlled trial investigating efficacy of
Heliox in acute bronchiolitis
Heliox for bronchiolitis
Conclusion
Heliox therapy does not reduce length of
treatment unless given via a tightfitting
facemask or CPAP
Nasal cannula heliox therapy is ineffective
Corticosteroid timing and length of stay for children with
asthma in the Emergency Department
Davis SR Burke G Hogan E Smith SR
Asthma
Asthma and steroids
Conclusion
Early steroid administration decreases time to
clinical improvement and discharge and reduced
admission rates in children presenting with
moderate to severe acute asthma
exacerbations
Steroids in asthma
Dexamethasone vs prednisone
Keeney et al Pediatrics 2014
Redman Arch Dis Children 2013
Williams et al Clin Pediatr 2013
Steroids in asthma
Conclusions (dexamethasone)
Equal efficacy
Shorter duration of treatment
Less vomiting
Improved compliance
Parental preference
Take home points
Consider high flow nasal cannula in
patients with acute respiratory illness
Early steroids for asthma
Dexamethasone gt prednisone
SEPSIS
Case Altered Mental Status
Case
65 yo ldquonot acting rightrdquo
rsaquo vomiting diarrhea fevers
PMHx None
Meds None
VS
T 392 P 118 RR 24 BP 8051 100 RA
101
128 38 7551187 58 6038
Recognition
Bimodal distribution
Predisposing conditions
Recent surgery
Unexplained tachycardia
Impaired perfusion
Delayed capillary refill
Lethargy
Irritability
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Outline
Recent literature pertaining to
Acute respiratory illnesses
Sepsis
Abdominal disorders
Questions mluemumarylandedu
RESPIRATORY
Case
15 month male with 3 day cough
congestion rhinorrhea
VS T 384 HR 130 RR 26 BP 7540 94
Exam smiling wheezing mild retractions
Case
15 month male with 3 day cough
congestion rhinorrhea
VS T 384 HR 150 RR 50 BP 7540 90
Exam wheezing mod retractions
Bronchiolitis
Clinical Practice Guideline
Diagnosis
Based on HampP
No routine labs or radiographs
Risk factors
age lt 12 weeks prematurity underlying CP
disease immunodeficiency
Ralston et al Pediatrics 2014
Clinical Practice Guideline
Treatment
Albuterol
Epinephrine
Steroids
Hypertonic saline
Ralston et al Pediatrics 2014
Skjerven et al NEJM 2013
Eight center randomized double-blind trial
404 infants
Conclusion
Inhaled racemic adrenaline is not more effective than inhaled saline
The strategy of inhalation on demand appears to be superior to that of inhalation on a fixed schedule
Clinical Practice Guideline
Treatment
Supplemental oxygen
Continuous pulse oximetry
Antibiotics
Fluids
Ralston et al Pediatrics 2014
High Flow Nasal Cannula
Wing et al Pediatr Emerg Care 2012
PED to PICU with ARI over 4 years
HFNC success rates 84-88
Decreased intubation rate
Decreased ventilator utilization by 50
No difference PICU LOS mortality or mean
duration of mechanical ventilation
HFNC
Conclusion
HFNC decreased need for intubation and
mechanical ventilator utilization for
children in the PED admitted to PICU
with ARI particularly when initiated early
HFNC vs nCPAP
Metge et al Eur J Pediatr 2014 Jul
Retrospective review
French PICU
2 consecutive bronchiolitis seasons
Conclusion
No difference between RR HR FiO2 CO2
in management of severe bronchiolitis in PICU
Heliox for bronchiolitis
Chowdhury et al Pediatrics 2013
Bronchiolitis Randomized Controlled Trial
Emergency-Assisted Therapy with
HelioxmdashAn Evaluation (BREATHE)
Largest multicenter randomized
controlled trial investigating efficacy of
Heliox in acute bronchiolitis
Heliox for bronchiolitis
Conclusion
Heliox therapy does not reduce length of
treatment unless given via a tightfitting
facemask or CPAP
Nasal cannula heliox therapy is ineffective
Corticosteroid timing and length of stay for children with
asthma in the Emergency Department
Davis SR Burke G Hogan E Smith SR
Asthma
Asthma and steroids
Conclusion
Early steroid administration decreases time to
clinical improvement and discharge and reduced
admission rates in children presenting with
moderate to severe acute asthma
exacerbations
Steroids in asthma
Dexamethasone vs prednisone
Keeney et al Pediatrics 2014
Redman Arch Dis Children 2013
Williams et al Clin Pediatr 2013
Steroids in asthma
Conclusions (dexamethasone)
Equal efficacy
Shorter duration of treatment
Less vomiting
Improved compliance
Parental preference
Take home points
Consider high flow nasal cannula in
patients with acute respiratory illness
Early steroids for asthma
Dexamethasone gt prednisone
SEPSIS
Case Altered Mental Status
Case
65 yo ldquonot acting rightrdquo
rsaquo vomiting diarrhea fevers
PMHx None
Meds None
VS
T 392 P 118 RR 24 BP 8051 100 RA
101
128 38 7551187 58 6038
Recognition
Bimodal distribution
Predisposing conditions
Recent surgery
Unexplained tachycardia
Impaired perfusion
Delayed capillary refill
Lethargy
Irritability
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
RESPIRATORY
Case
15 month male with 3 day cough
congestion rhinorrhea
VS T 384 HR 130 RR 26 BP 7540 94
Exam smiling wheezing mild retractions
Case
15 month male with 3 day cough
congestion rhinorrhea
VS T 384 HR 150 RR 50 BP 7540 90
Exam wheezing mod retractions
Bronchiolitis
Clinical Practice Guideline
Diagnosis
Based on HampP
No routine labs or radiographs
Risk factors
age lt 12 weeks prematurity underlying CP
disease immunodeficiency
Ralston et al Pediatrics 2014
Clinical Practice Guideline
Treatment
Albuterol
Epinephrine
Steroids
Hypertonic saline
Ralston et al Pediatrics 2014
Skjerven et al NEJM 2013
Eight center randomized double-blind trial
404 infants
Conclusion
Inhaled racemic adrenaline is not more effective than inhaled saline
The strategy of inhalation on demand appears to be superior to that of inhalation on a fixed schedule
Clinical Practice Guideline
Treatment
Supplemental oxygen
Continuous pulse oximetry
Antibiotics
Fluids
Ralston et al Pediatrics 2014
High Flow Nasal Cannula
Wing et al Pediatr Emerg Care 2012
PED to PICU with ARI over 4 years
HFNC success rates 84-88
Decreased intubation rate
Decreased ventilator utilization by 50
No difference PICU LOS mortality or mean
duration of mechanical ventilation
HFNC
Conclusion
HFNC decreased need for intubation and
mechanical ventilator utilization for
children in the PED admitted to PICU
with ARI particularly when initiated early
HFNC vs nCPAP
Metge et al Eur J Pediatr 2014 Jul
Retrospective review
French PICU
2 consecutive bronchiolitis seasons
Conclusion
No difference between RR HR FiO2 CO2
in management of severe bronchiolitis in PICU
Heliox for bronchiolitis
Chowdhury et al Pediatrics 2013
Bronchiolitis Randomized Controlled Trial
Emergency-Assisted Therapy with
HelioxmdashAn Evaluation (BREATHE)
Largest multicenter randomized
controlled trial investigating efficacy of
Heliox in acute bronchiolitis
Heliox for bronchiolitis
Conclusion
Heliox therapy does not reduce length of
treatment unless given via a tightfitting
facemask or CPAP
Nasal cannula heliox therapy is ineffective
Corticosteroid timing and length of stay for children with
asthma in the Emergency Department
Davis SR Burke G Hogan E Smith SR
Asthma
Asthma and steroids
Conclusion
Early steroid administration decreases time to
clinical improvement and discharge and reduced
admission rates in children presenting with
moderate to severe acute asthma
exacerbations
Steroids in asthma
Dexamethasone vs prednisone
Keeney et al Pediatrics 2014
Redman Arch Dis Children 2013
Williams et al Clin Pediatr 2013
Steroids in asthma
Conclusions (dexamethasone)
Equal efficacy
Shorter duration of treatment
Less vomiting
Improved compliance
Parental preference
Take home points
Consider high flow nasal cannula in
patients with acute respiratory illness
Early steroids for asthma
Dexamethasone gt prednisone
SEPSIS
Case Altered Mental Status
Case
65 yo ldquonot acting rightrdquo
rsaquo vomiting diarrhea fevers
PMHx None
Meds None
VS
T 392 P 118 RR 24 BP 8051 100 RA
101
128 38 7551187 58 6038
Recognition
Bimodal distribution
Predisposing conditions
Recent surgery
Unexplained tachycardia
Impaired perfusion
Delayed capillary refill
Lethargy
Irritability
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Case
15 month male with 3 day cough
congestion rhinorrhea
VS T 384 HR 130 RR 26 BP 7540 94
Exam smiling wheezing mild retractions
Case
15 month male with 3 day cough
congestion rhinorrhea
VS T 384 HR 150 RR 50 BP 7540 90
Exam wheezing mod retractions
Bronchiolitis
Clinical Practice Guideline
Diagnosis
Based on HampP
No routine labs or radiographs
Risk factors
age lt 12 weeks prematurity underlying CP
disease immunodeficiency
Ralston et al Pediatrics 2014
Clinical Practice Guideline
Treatment
Albuterol
Epinephrine
Steroids
Hypertonic saline
Ralston et al Pediatrics 2014
Skjerven et al NEJM 2013
Eight center randomized double-blind trial
404 infants
Conclusion
Inhaled racemic adrenaline is not more effective than inhaled saline
The strategy of inhalation on demand appears to be superior to that of inhalation on a fixed schedule
Clinical Practice Guideline
Treatment
Supplemental oxygen
Continuous pulse oximetry
Antibiotics
Fluids
Ralston et al Pediatrics 2014
High Flow Nasal Cannula
Wing et al Pediatr Emerg Care 2012
PED to PICU with ARI over 4 years
HFNC success rates 84-88
Decreased intubation rate
Decreased ventilator utilization by 50
No difference PICU LOS mortality or mean
duration of mechanical ventilation
HFNC
Conclusion
HFNC decreased need for intubation and
mechanical ventilator utilization for
children in the PED admitted to PICU
with ARI particularly when initiated early
HFNC vs nCPAP
Metge et al Eur J Pediatr 2014 Jul
Retrospective review
French PICU
2 consecutive bronchiolitis seasons
Conclusion
No difference between RR HR FiO2 CO2
in management of severe bronchiolitis in PICU
Heliox for bronchiolitis
Chowdhury et al Pediatrics 2013
Bronchiolitis Randomized Controlled Trial
Emergency-Assisted Therapy with
HelioxmdashAn Evaluation (BREATHE)
Largest multicenter randomized
controlled trial investigating efficacy of
Heliox in acute bronchiolitis
Heliox for bronchiolitis
Conclusion
Heliox therapy does not reduce length of
treatment unless given via a tightfitting
facemask or CPAP
Nasal cannula heliox therapy is ineffective
Corticosteroid timing and length of stay for children with
asthma in the Emergency Department
Davis SR Burke G Hogan E Smith SR
Asthma
Asthma and steroids
Conclusion
Early steroid administration decreases time to
clinical improvement and discharge and reduced
admission rates in children presenting with
moderate to severe acute asthma
exacerbations
Steroids in asthma
Dexamethasone vs prednisone
Keeney et al Pediatrics 2014
Redman Arch Dis Children 2013
Williams et al Clin Pediatr 2013
Steroids in asthma
Conclusions (dexamethasone)
Equal efficacy
Shorter duration of treatment
Less vomiting
Improved compliance
Parental preference
Take home points
Consider high flow nasal cannula in
patients with acute respiratory illness
Early steroids for asthma
Dexamethasone gt prednisone
SEPSIS
Case Altered Mental Status
Case
65 yo ldquonot acting rightrdquo
rsaquo vomiting diarrhea fevers
PMHx None
Meds None
VS
T 392 P 118 RR 24 BP 8051 100 RA
101
128 38 7551187 58 6038
Recognition
Bimodal distribution
Predisposing conditions
Recent surgery
Unexplained tachycardia
Impaired perfusion
Delayed capillary refill
Lethargy
Irritability
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Case
15 month male with 3 day cough
congestion rhinorrhea
VS T 384 HR 150 RR 50 BP 7540 90
Exam wheezing mod retractions
Bronchiolitis
Clinical Practice Guideline
Diagnosis
Based on HampP
No routine labs or radiographs
Risk factors
age lt 12 weeks prematurity underlying CP
disease immunodeficiency
Ralston et al Pediatrics 2014
Clinical Practice Guideline
Treatment
Albuterol
Epinephrine
Steroids
Hypertonic saline
Ralston et al Pediatrics 2014
Skjerven et al NEJM 2013
Eight center randomized double-blind trial
404 infants
Conclusion
Inhaled racemic adrenaline is not more effective than inhaled saline
The strategy of inhalation on demand appears to be superior to that of inhalation on a fixed schedule
Clinical Practice Guideline
Treatment
Supplemental oxygen
Continuous pulse oximetry
Antibiotics
Fluids
Ralston et al Pediatrics 2014
High Flow Nasal Cannula
Wing et al Pediatr Emerg Care 2012
PED to PICU with ARI over 4 years
HFNC success rates 84-88
Decreased intubation rate
Decreased ventilator utilization by 50
No difference PICU LOS mortality or mean
duration of mechanical ventilation
HFNC
Conclusion
HFNC decreased need for intubation and
mechanical ventilator utilization for
children in the PED admitted to PICU
with ARI particularly when initiated early
HFNC vs nCPAP
Metge et al Eur J Pediatr 2014 Jul
Retrospective review
French PICU
2 consecutive bronchiolitis seasons
Conclusion
No difference between RR HR FiO2 CO2
in management of severe bronchiolitis in PICU
Heliox for bronchiolitis
Chowdhury et al Pediatrics 2013
Bronchiolitis Randomized Controlled Trial
Emergency-Assisted Therapy with
HelioxmdashAn Evaluation (BREATHE)
Largest multicenter randomized
controlled trial investigating efficacy of
Heliox in acute bronchiolitis
Heliox for bronchiolitis
Conclusion
Heliox therapy does not reduce length of
treatment unless given via a tightfitting
facemask or CPAP
Nasal cannula heliox therapy is ineffective
Corticosteroid timing and length of stay for children with
asthma in the Emergency Department
Davis SR Burke G Hogan E Smith SR
Asthma
Asthma and steroids
Conclusion
Early steroid administration decreases time to
clinical improvement and discharge and reduced
admission rates in children presenting with
moderate to severe acute asthma
exacerbations
Steroids in asthma
Dexamethasone vs prednisone
Keeney et al Pediatrics 2014
Redman Arch Dis Children 2013
Williams et al Clin Pediatr 2013
Steroids in asthma
Conclusions (dexamethasone)
Equal efficacy
Shorter duration of treatment
Less vomiting
Improved compliance
Parental preference
Take home points
Consider high flow nasal cannula in
patients with acute respiratory illness
Early steroids for asthma
Dexamethasone gt prednisone
SEPSIS
Case Altered Mental Status
Case
65 yo ldquonot acting rightrdquo
rsaquo vomiting diarrhea fevers
PMHx None
Meds None
VS
T 392 P 118 RR 24 BP 8051 100 RA
101
128 38 7551187 58 6038
Recognition
Bimodal distribution
Predisposing conditions
Recent surgery
Unexplained tachycardia
Impaired perfusion
Delayed capillary refill
Lethargy
Irritability
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Bronchiolitis
Clinical Practice Guideline
Diagnosis
Based on HampP
No routine labs or radiographs
Risk factors
age lt 12 weeks prematurity underlying CP
disease immunodeficiency
Ralston et al Pediatrics 2014
Clinical Practice Guideline
Treatment
Albuterol
Epinephrine
Steroids
Hypertonic saline
Ralston et al Pediatrics 2014
Skjerven et al NEJM 2013
Eight center randomized double-blind trial
404 infants
Conclusion
Inhaled racemic adrenaline is not more effective than inhaled saline
The strategy of inhalation on demand appears to be superior to that of inhalation on a fixed schedule
Clinical Practice Guideline
Treatment
Supplemental oxygen
Continuous pulse oximetry
Antibiotics
Fluids
Ralston et al Pediatrics 2014
High Flow Nasal Cannula
Wing et al Pediatr Emerg Care 2012
PED to PICU with ARI over 4 years
HFNC success rates 84-88
Decreased intubation rate
Decreased ventilator utilization by 50
No difference PICU LOS mortality or mean
duration of mechanical ventilation
HFNC
Conclusion
HFNC decreased need for intubation and
mechanical ventilator utilization for
children in the PED admitted to PICU
with ARI particularly when initiated early
HFNC vs nCPAP
Metge et al Eur J Pediatr 2014 Jul
Retrospective review
French PICU
2 consecutive bronchiolitis seasons
Conclusion
No difference between RR HR FiO2 CO2
in management of severe bronchiolitis in PICU
Heliox for bronchiolitis
Chowdhury et al Pediatrics 2013
Bronchiolitis Randomized Controlled Trial
Emergency-Assisted Therapy with
HelioxmdashAn Evaluation (BREATHE)
Largest multicenter randomized
controlled trial investigating efficacy of
Heliox in acute bronchiolitis
Heliox for bronchiolitis
Conclusion
Heliox therapy does not reduce length of
treatment unless given via a tightfitting
facemask or CPAP
Nasal cannula heliox therapy is ineffective
Corticosteroid timing and length of stay for children with
asthma in the Emergency Department
Davis SR Burke G Hogan E Smith SR
Asthma
Asthma and steroids
Conclusion
Early steroid administration decreases time to
clinical improvement and discharge and reduced
admission rates in children presenting with
moderate to severe acute asthma
exacerbations
Steroids in asthma
Dexamethasone vs prednisone
Keeney et al Pediatrics 2014
Redman Arch Dis Children 2013
Williams et al Clin Pediatr 2013
Steroids in asthma
Conclusions (dexamethasone)
Equal efficacy
Shorter duration of treatment
Less vomiting
Improved compliance
Parental preference
Take home points
Consider high flow nasal cannula in
patients with acute respiratory illness
Early steroids for asthma
Dexamethasone gt prednisone
SEPSIS
Case Altered Mental Status
Case
65 yo ldquonot acting rightrdquo
rsaquo vomiting diarrhea fevers
PMHx None
Meds None
VS
T 392 P 118 RR 24 BP 8051 100 RA
101
128 38 7551187 58 6038
Recognition
Bimodal distribution
Predisposing conditions
Recent surgery
Unexplained tachycardia
Impaired perfusion
Delayed capillary refill
Lethargy
Irritability
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Clinical Practice Guideline
Diagnosis
Based on HampP
No routine labs or radiographs
Risk factors
age lt 12 weeks prematurity underlying CP
disease immunodeficiency
Ralston et al Pediatrics 2014
Clinical Practice Guideline
Treatment
Albuterol
Epinephrine
Steroids
Hypertonic saline
Ralston et al Pediatrics 2014
Skjerven et al NEJM 2013
Eight center randomized double-blind trial
404 infants
Conclusion
Inhaled racemic adrenaline is not more effective than inhaled saline
The strategy of inhalation on demand appears to be superior to that of inhalation on a fixed schedule
Clinical Practice Guideline
Treatment
Supplemental oxygen
Continuous pulse oximetry
Antibiotics
Fluids
Ralston et al Pediatrics 2014
High Flow Nasal Cannula
Wing et al Pediatr Emerg Care 2012
PED to PICU with ARI over 4 years
HFNC success rates 84-88
Decreased intubation rate
Decreased ventilator utilization by 50
No difference PICU LOS mortality or mean
duration of mechanical ventilation
HFNC
Conclusion
HFNC decreased need for intubation and
mechanical ventilator utilization for
children in the PED admitted to PICU
with ARI particularly when initiated early
HFNC vs nCPAP
Metge et al Eur J Pediatr 2014 Jul
Retrospective review
French PICU
2 consecutive bronchiolitis seasons
Conclusion
No difference between RR HR FiO2 CO2
in management of severe bronchiolitis in PICU
Heliox for bronchiolitis
Chowdhury et al Pediatrics 2013
Bronchiolitis Randomized Controlled Trial
Emergency-Assisted Therapy with
HelioxmdashAn Evaluation (BREATHE)
Largest multicenter randomized
controlled trial investigating efficacy of
Heliox in acute bronchiolitis
Heliox for bronchiolitis
Conclusion
Heliox therapy does not reduce length of
treatment unless given via a tightfitting
facemask or CPAP
Nasal cannula heliox therapy is ineffective
Corticosteroid timing and length of stay for children with
asthma in the Emergency Department
Davis SR Burke G Hogan E Smith SR
Asthma
Asthma and steroids
Conclusion
Early steroid administration decreases time to
clinical improvement and discharge and reduced
admission rates in children presenting with
moderate to severe acute asthma
exacerbations
Steroids in asthma
Dexamethasone vs prednisone
Keeney et al Pediatrics 2014
Redman Arch Dis Children 2013
Williams et al Clin Pediatr 2013
Steroids in asthma
Conclusions (dexamethasone)
Equal efficacy
Shorter duration of treatment
Less vomiting
Improved compliance
Parental preference
Take home points
Consider high flow nasal cannula in
patients with acute respiratory illness
Early steroids for asthma
Dexamethasone gt prednisone
SEPSIS
Case Altered Mental Status
Case
65 yo ldquonot acting rightrdquo
rsaquo vomiting diarrhea fevers
PMHx None
Meds None
VS
T 392 P 118 RR 24 BP 8051 100 RA
101
128 38 7551187 58 6038
Recognition
Bimodal distribution
Predisposing conditions
Recent surgery
Unexplained tachycardia
Impaired perfusion
Delayed capillary refill
Lethargy
Irritability
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Clinical Practice Guideline
Treatment
Albuterol
Epinephrine
Steroids
Hypertonic saline
Ralston et al Pediatrics 2014
Skjerven et al NEJM 2013
Eight center randomized double-blind trial
404 infants
Conclusion
Inhaled racemic adrenaline is not more effective than inhaled saline
The strategy of inhalation on demand appears to be superior to that of inhalation on a fixed schedule
Clinical Practice Guideline
Treatment
Supplemental oxygen
Continuous pulse oximetry
Antibiotics
Fluids
Ralston et al Pediatrics 2014
High Flow Nasal Cannula
Wing et al Pediatr Emerg Care 2012
PED to PICU with ARI over 4 years
HFNC success rates 84-88
Decreased intubation rate
Decreased ventilator utilization by 50
No difference PICU LOS mortality or mean
duration of mechanical ventilation
HFNC
Conclusion
HFNC decreased need for intubation and
mechanical ventilator utilization for
children in the PED admitted to PICU
with ARI particularly when initiated early
HFNC vs nCPAP
Metge et al Eur J Pediatr 2014 Jul
Retrospective review
French PICU
2 consecutive bronchiolitis seasons
Conclusion
No difference between RR HR FiO2 CO2
in management of severe bronchiolitis in PICU
Heliox for bronchiolitis
Chowdhury et al Pediatrics 2013
Bronchiolitis Randomized Controlled Trial
Emergency-Assisted Therapy with
HelioxmdashAn Evaluation (BREATHE)
Largest multicenter randomized
controlled trial investigating efficacy of
Heliox in acute bronchiolitis
Heliox for bronchiolitis
Conclusion
Heliox therapy does not reduce length of
treatment unless given via a tightfitting
facemask or CPAP
Nasal cannula heliox therapy is ineffective
Corticosteroid timing and length of stay for children with
asthma in the Emergency Department
Davis SR Burke G Hogan E Smith SR
Asthma
Asthma and steroids
Conclusion
Early steroid administration decreases time to
clinical improvement and discharge and reduced
admission rates in children presenting with
moderate to severe acute asthma
exacerbations
Steroids in asthma
Dexamethasone vs prednisone
Keeney et al Pediatrics 2014
Redman Arch Dis Children 2013
Williams et al Clin Pediatr 2013
Steroids in asthma
Conclusions (dexamethasone)
Equal efficacy
Shorter duration of treatment
Less vomiting
Improved compliance
Parental preference
Take home points
Consider high flow nasal cannula in
patients with acute respiratory illness
Early steroids for asthma
Dexamethasone gt prednisone
SEPSIS
Case Altered Mental Status
Case
65 yo ldquonot acting rightrdquo
rsaquo vomiting diarrhea fevers
PMHx None
Meds None
VS
T 392 P 118 RR 24 BP 8051 100 RA
101
128 38 7551187 58 6038
Recognition
Bimodal distribution
Predisposing conditions
Recent surgery
Unexplained tachycardia
Impaired perfusion
Delayed capillary refill
Lethargy
Irritability
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Skjerven et al NEJM 2013
Eight center randomized double-blind trial
404 infants
Conclusion
Inhaled racemic adrenaline is not more effective than inhaled saline
The strategy of inhalation on demand appears to be superior to that of inhalation on a fixed schedule
Clinical Practice Guideline
Treatment
Supplemental oxygen
Continuous pulse oximetry
Antibiotics
Fluids
Ralston et al Pediatrics 2014
High Flow Nasal Cannula
Wing et al Pediatr Emerg Care 2012
PED to PICU with ARI over 4 years
HFNC success rates 84-88
Decreased intubation rate
Decreased ventilator utilization by 50
No difference PICU LOS mortality or mean
duration of mechanical ventilation
HFNC
Conclusion
HFNC decreased need for intubation and
mechanical ventilator utilization for
children in the PED admitted to PICU
with ARI particularly when initiated early
HFNC vs nCPAP
Metge et al Eur J Pediatr 2014 Jul
Retrospective review
French PICU
2 consecutive bronchiolitis seasons
Conclusion
No difference between RR HR FiO2 CO2
in management of severe bronchiolitis in PICU
Heliox for bronchiolitis
Chowdhury et al Pediatrics 2013
Bronchiolitis Randomized Controlled Trial
Emergency-Assisted Therapy with
HelioxmdashAn Evaluation (BREATHE)
Largest multicenter randomized
controlled trial investigating efficacy of
Heliox in acute bronchiolitis
Heliox for bronchiolitis
Conclusion
Heliox therapy does not reduce length of
treatment unless given via a tightfitting
facemask or CPAP
Nasal cannula heliox therapy is ineffective
Corticosteroid timing and length of stay for children with
asthma in the Emergency Department
Davis SR Burke G Hogan E Smith SR
Asthma
Asthma and steroids
Conclusion
Early steroid administration decreases time to
clinical improvement and discharge and reduced
admission rates in children presenting with
moderate to severe acute asthma
exacerbations
Steroids in asthma
Dexamethasone vs prednisone
Keeney et al Pediatrics 2014
Redman Arch Dis Children 2013
Williams et al Clin Pediatr 2013
Steroids in asthma
Conclusions (dexamethasone)
Equal efficacy
Shorter duration of treatment
Less vomiting
Improved compliance
Parental preference
Take home points
Consider high flow nasal cannula in
patients with acute respiratory illness
Early steroids for asthma
Dexamethasone gt prednisone
SEPSIS
Case Altered Mental Status
Case
65 yo ldquonot acting rightrdquo
rsaquo vomiting diarrhea fevers
PMHx None
Meds None
VS
T 392 P 118 RR 24 BP 8051 100 RA
101
128 38 7551187 58 6038
Recognition
Bimodal distribution
Predisposing conditions
Recent surgery
Unexplained tachycardia
Impaired perfusion
Delayed capillary refill
Lethargy
Irritability
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Clinical Practice Guideline
Treatment
Supplemental oxygen
Continuous pulse oximetry
Antibiotics
Fluids
Ralston et al Pediatrics 2014
High Flow Nasal Cannula
Wing et al Pediatr Emerg Care 2012
PED to PICU with ARI over 4 years
HFNC success rates 84-88
Decreased intubation rate
Decreased ventilator utilization by 50
No difference PICU LOS mortality or mean
duration of mechanical ventilation
HFNC
Conclusion
HFNC decreased need for intubation and
mechanical ventilator utilization for
children in the PED admitted to PICU
with ARI particularly when initiated early
HFNC vs nCPAP
Metge et al Eur J Pediatr 2014 Jul
Retrospective review
French PICU
2 consecutive bronchiolitis seasons
Conclusion
No difference between RR HR FiO2 CO2
in management of severe bronchiolitis in PICU
Heliox for bronchiolitis
Chowdhury et al Pediatrics 2013
Bronchiolitis Randomized Controlled Trial
Emergency-Assisted Therapy with
HelioxmdashAn Evaluation (BREATHE)
Largest multicenter randomized
controlled trial investigating efficacy of
Heliox in acute bronchiolitis
Heliox for bronchiolitis
Conclusion
Heliox therapy does not reduce length of
treatment unless given via a tightfitting
facemask or CPAP
Nasal cannula heliox therapy is ineffective
Corticosteroid timing and length of stay for children with
asthma in the Emergency Department
Davis SR Burke G Hogan E Smith SR
Asthma
Asthma and steroids
Conclusion
Early steroid administration decreases time to
clinical improvement and discharge and reduced
admission rates in children presenting with
moderate to severe acute asthma
exacerbations
Steroids in asthma
Dexamethasone vs prednisone
Keeney et al Pediatrics 2014
Redman Arch Dis Children 2013
Williams et al Clin Pediatr 2013
Steroids in asthma
Conclusions (dexamethasone)
Equal efficacy
Shorter duration of treatment
Less vomiting
Improved compliance
Parental preference
Take home points
Consider high flow nasal cannula in
patients with acute respiratory illness
Early steroids for asthma
Dexamethasone gt prednisone
SEPSIS
Case Altered Mental Status
Case
65 yo ldquonot acting rightrdquo
rsaquo vomiting diarrhea fevers
PMHx None
Meds None
VS
T 392 P 118 RR 24 BP 8051 100 RA
101
128 38 7551187 58 6038
Recognition
Bimodal distribution
Predisposing conditions
Recent surgery
Unexplained tachycardia
Impaired perfusion
Delayed capillary refill
Lethargy
Irritability
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

High Flow Nasal Cannula
Wing et al Pediatr Emerg Care 2012
PED to PICU with ARI over 4 years
HFNC success rates 84-88
Decreased intubation rate
Decreased ventilator utilization by 50
No difference PICU LOS mortality or mean
duration of mechanical ventilation
HFNC
Conclusion
HFNC decreased need for intubation and
mechanical ventilator utilization for
children in the PED admitted to PICU
with ARI particularly when initiated early
HFNC vs nCPAP
Metge et al Eur J Pediatr 2014 Jul
Retrospective review
French PICU
2 consecutive bronchiolitis seasons
Conclusion
No difference between RR HR FiO2 CO2
in management of severe bronchiolitis in PICU
Heliox for bronchiolitis
Chowdhury et al Pediatrics 2013
Bronchiolitis Randomized Controlled Trial
Emergency-Assisted Therapy with
HelioxmdashAn Evaluation (BREATHE)
Largest multicenter randomized
controlled trial investigating efficacy of
Heliox in acute bronchiolitis
Heliox for bronchiolitis
Conclusion
Heliox therapy does not reduce length of
treatment unless given via a tightfitting
facemask or CPAP
Nasal cannula heliox therapy is ineffective
Corticosteroid timing and length of stay for children with
asthma in the Emergency Department
Davis SR Burke G Hogan E Smith SR
Asthma
Asthma and steroids
Conclusion
Early steroid administration decreases time to
clinical improvement and discharge and reduced
admission rates in children presenting with
moderate to severe acute asthma
exacerbations
Steroids in asthma
Dexamethasone vs prednisone
Keeney et al Pediatrics 2014
Redman Arch Dis Children 2013
Williams et al Clin Pediatr 2013
Steroids in asthma
Conclusions (dexamethasone)
Equal efficacy
Shorter duration of treatment
Less vomiting
Improved compliance
Parental preference
Take home points
Consider high flow nasal cannula in
patients with acute respiratory illness
Early steroids for asthma
Dexamethasone gt prednisone
SEPSIS
Case Altered Mental Status
Case
65 yo ldquonot acting rightrdquo
rsaquo vomiting diarrhea fevers
PMHx None
Meds None
VS
T 392 P 118 RR 24 BP 8051 100 RA
101
128 38 7551187 58 6038
Recognition
Bimodal distribution
Predisposing conditions
Recent surgery
Unexplained tachycardia
Impaired perfusion
Delayed capillary refill
Lethargy
Irritability
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

HFNC
Conclusion
HFNC decreased need for intubation and
mechanical ventilator utilization for
children in the PED admitted to PICU
with ARI particularly when initiated early
HFNC vs nCPAP
Metge et al Eur J Pediatr 2014 Jul
Retrospective review
French PICU
2 consecutive bronchiolitis seasons
Conclusion
No difference between RR HR FiO2 CO2
in management of severe bronchiolitis in PICU
Heliox for bronchiolitis
Chowdhury et al Pediatrics 2013
Bronchiolitis Randomized Controlled Trial
Emergency-Assisted Therapy with
HelioxmdashAn Evaluation (BREATHE)
Largest multicenter randomized
controlled trial investigating efficacy of
Heliox in acute bronchiolitis
Heliox for bronchiolitis
Conclusion
Heliox therapy does not reduce length of
treatment unless given via a tightfitting
facemask or CPAP
Nasal cannula heliox therapy is ineffective
Corticosteroid timing and length of stay for children with
asthma in the Emergency Department
Davis SR Burke G Hogan E Smith SR
Asthma
Asthma and steroids
Conclusion
Early steroid administration decreases time to
clinical improvement and discharge and reduced
admission rates in children presenting with
moderate to severe acute asthma
exacerbations
Steroids in asthma
Dexamethasone vs prednisone
Keeney et al Pediatrics 2014
Redman Arch Dis Children 2013
Williams et al Clin Pediatr 2013
Steroids in asthma
Conclusions (dexamethasone)
Equal efficacy
Shorter duration of treatment
Less vomiting
Improved compliance
Parental preference
Take home points
Consider high flow nasal cannula in
patients with acute respiratory illness
Early steroids for asthma
Dexamethasone gt prednisone
SEPSIS
Case Altered Mental Status
Case
65 yo ldquonot acting rightrdquo
rsaquo vomiting diarrhea fevers
PMHx None
Meds None
VS
T 392 P 118 RR 24 BP 8051 100 RA
101
128 38 7551187 58 6038
Recognition
Bimodal distribution
Predisposing conditions
Recent surgery
Unexplained tachycardia
Impaired perfusion
Delayed capillary refill
Lethargy
Irritability
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

HFNC vs nCPAP
Metge et al Eur J Pediatr 2014 Jul
Retrospective review
French PICU
2 consecutive bronchiolitis seasons
Conclusion
No difference between RR HR FiO2 CO2
in management of severe bronchiolitis in PICU
Heliox for bronchiolitis
Chowdhury et al Pediatrics 2013
Bronchiolitis Randomized Controlled Trial
Emergency-Assisted Therapy with
HelioxmdashAn Evaluation (BREATHE)
Largest multicenter randomized
controlled trial investigating efficacy of
Heliox in acute bronchiolitis
Heliox for bronchiolitis
Conclusion
Heliox therapy does not reduce length of
treatment unless given via a tightfitting
facemask or CPAP
Nasal cannula heliox therapy is ineffective
Corticosteroid timing and length of stay for children with
asthma in the Emergency Department
Davis SR Burke G Hogan E Smith SR
Asthma
Asthma and steroids
Conclusion
Early steroid administration decreases time to
clinical improvement and discharge and reduced
admission rates in children presenting with
moderate to severe acute asthma
exacerbations
Steroids in asthma
Dexamethasone vs prednisone
Keeney et al Pediatrics 2014
Redman Arch Dis Children 2013
Williams et al Clin Pediatr 2013
Steroids in asthma
Conclusions (dexamethasone)
Equal efficacy
Shorter duration of treatment
Less vomiting
Improved compliance
Parental preference
Take home points
Consider high flow nasal cannula in
patients with acute respiratory illness
Early steroids for asthma
Dexamethasone gt prednisone
SEPSIS
Case Altered Mental Status
Case
65 yo ldquonot acting rightrdquo
rsaquo vomiting diarrhea fevers
PMHx None
Meds None
VS
T 392 P 118 RR 24 BP 8051 100 RA
101
128 38 7551187 58 6038
Recognition
Bimodal distribution
Predisposing conditions
Recent surgery
Unexplained tachycardia
Impaired perfusion
Delayed capillary refill
Lethargy
Irritability
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Heliox for bronchiolitis
Chowdhury et al Pediatrics 2013
Bronchiolitis Randomized Controlled Trial
Emergency-Assisted Therapy with
HelioxmdashAn Evaluation (BREATHE)
Largest multicenter randomized
controlled trial investigating efficacy of
Heliox in acute bronchiolitis
Heliox for bronchiolitis
Conclusion
Heliox therapy does not reduce length of
treatment unless given via a tightfitting
facemask or CPAP
Nasal cannula heliox therapy is ineffective
Corticosteroid timing and length of stay for children with
asthma in the Emergency Department
Davis SR Burke G Hogan E Smith SR
Asthma
Asthma and steroids
Conclusion
Early steroid administration decreases time to
clinical improvement and discharge and reduced
admission rates in children presenting with
moderate to severe acute asthma
exacerbations
Steroids in asthma
Dexamethasone vs prednisone
Keeney et al Pediatrics 2014
Redman Arch Dis Children 2013
Williams et al Clin Pediatr 2013
Steroids in asthma
Conclusions (dexamethasone)
Equal efficacy
Shorter duration of treatment
Less vomiting
Improved compliance
Parental preference
Take home points
Consider high flow nasal cannula in
patients with acute respiratory illness
Early steroids for asthma
Dexamethasone gt prednisone
SEPSIS
Case Altered Mental Status
Case
65 yo ldquonot acting rightrdquo
rsaquo vomiting diarrhea fevers
PMHx None
Meds None
VS
T 392 P 118 RR 24 BP 8051 100 RA
101
128 38 7551187 58 6038
Recognition
Bimodal distribution
Predisposing conditions
Recent surgery
Unexplained tachycardia
Impaired perfusion
Delayed capillary refill
Lethargy
Irritability
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Heliox for bronchiolitis
Conclusion
Heliox therapy does not reduce length of
treatment unless given via a tightfitting
facemask or CPAP
Nasal cannula heliox therapy is ineffective
Corticosteroid timing and length of stay for children with
asthma in the Emergency Department
Davis SR Burke G Hogan E Smith SR
Asthma
Asthma and steroids
Conclusion
Early steroid administration decreases time to
clinical improvement and discharge and reduced
admission rates in children presenting with
moderate to severe acute asthma
exacerbations
Steroids in asthma
Dexamethasone vs prednisone
Keeney et al Pediatrics 2014
Redman Arch Dis Children 2013
Williams et al Clin Pediatr 2013
Steroids in asthma
Conclusions (dexamethasone)
Equal efficacy
Shorter duration of treatment
Less vomiting
Improved compliance
Parental preference
Take home points
Consider high flow nasal cannula in
patients with acute respiratory illness
Early steroids for asthma
Dexamethasone gt prednisone
SEPSIS
Case Altered Mental Status
Case
65 yo ldquonot acting rightrdquo
rsaquo vomiting diarrhea fevers
PMHx None
Meds None
VS
T 392 P 118 RR 24 BP 8051 100 RA
101
128 38 7551187 58 6038
Recognition
Bimodal distribution
Predisposing conditions
Recent surgery
Unexplained tachycardia
Impaired perfusion
Delayed capillary refill
Lethargy
Irritability
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Corticosteroid timing and length of stay for children with
asthma in the Emergency Department
Davis SR Burke G Hogan E Smith SR
Asthma
Asthma and steroids
Conclusion
Early steroid administration decreases time to
clinical improvement and discharge and reduced
admission rates in children presenting with
moderate to severe acute asthma
exacerbations
Steroids in asthma
Dexamethasone vs prednisone
Keeney et al Pediatrics 2014
Redman Arch Dis Children 2013
Williams et al Clin Pediatr 2013
Steroids in asthma
Conclusions (dexamethasone)
Equal efficacy
Shorter duration of treatment
Less vomiting
Improved compliance
Parental preference
Take home points
Consider high flow nasal cannula in
patients with acute respiratory illness
Early steroids for asthma
Dexamethasone gt prednisone
SEPSIS
Case Altered Mental Status
Case
65 yo ldquonot acting rightrdquo
rsaquo vomiting diarrhea fevers
PMHx None
Meds None
VS
T 392 P 118 RR 24 BP 8051 100 RA
101
128 38 7551187 58 6038
Recognition
Bimodal distribution
Predisposing conditions
Recent surgery
Unexplained tachycardia
Impaired perfusion
Delayed capillary refill
Lethargy
Irritability
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Asthma and steroids
Conclusion
Early steroid administration decreases time to
clinical improvement and discharge and reduced
admission rates in children presenting with
moderate to severe acute asthma
exacerbations
Steroids in asthma
Dexamethasone vs prednisone
Keeney et al Pediatrics 2014
Redman Arch Dis Children 2013
Williams et al Clin Pediatr 2013
Steroids in asthma
Conclusions (dexamethasone)
Equal efficacy
Shorter duration of treatment
Less vomiting
Improved compliance
Parental preference
Take home points
Consider high flow nasal cannula in
patients with acute respiratory illness
Early steroids for asthma
Dexamethasone gt prednisone
SEPSIS
Case Altered Mental Status
Case
65 yo ldquonot acting rightrdquo
rsaquo vomiting diarrhea fevers
PMHx None
Meds None
VS
T 392 P 118 RR 24 BP 8051 100 RA
101
128 38 7551187 58 6038
Recognition
Bimodal distribution
Predisposing conditions
Recent surgery
Unexplained tachycardia
Impaired perfusion
Delayed capillary refill
Lethargy
Irritability
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Steroids in asthma
Dexamethasone vs prednisone
Keeney et al Pediatrics 2014
Redman Arch Dis Children 2013
Williams et al Clin Pediatr 2013
Steroids in asthma
Conclusions (dexamethasone)
Equal efficacy
Shorter duration of treatment
Less vomiting
Improved compliance
Parental preference
Take home points
Consider high flow nasal cannula in
patients with acute respiratory illness
Early steroids for asthma
Dexamethasone gt prednisone
SEPSIS
Case Altered Mental Status
Case
65 yo ldquonot acting rightrdquo
rsaquo vomiting diarrhea fevers
PMHx None
Meds None
VS
T 392 P 118 RR 24 BP 8051 100 RA
101
128 38 7551187 58 6038
Recognition
Bimodal distribution
Predisposing conditions
Recent surgery
Unexplained tachycardia
Impaired perfusion
Delayed capillary refill
Lethargy
Irritability
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Steroids in asthma
Conclusions (dexamethasone)
Equal efficacy
Shorter duration of treatment
Less vomiting
Improved compliance
Parental preference
Take home points
Consider high flow nasal cannula in
patients with acute respiratory illness
Early steroids for asthma
Dexamethasone gt prednisone
SEPSIS
Case Altered Mental Status
Case
65 yo ldquonot acting rightrdquo
rsaquo vomiting diarrhea fevers
PMHx None
Meds None
VS
T 392 P 118 RR 24 BP 8051 100 RA
101
128 38 7551187 58 6038
Recognition
Bimodal distribution
Predisposing conditions
Recent surgery
Unexplained tachycardia
Impaired perfusion
Delayed capillary refill
Lethargy
Irritability
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Take home points
Consider high flow nasal cannula in
patients with acute respiratory illness
Early steroids for asthma
Dexamethasone gt prednisone
SEPSIS
Case Altered Mental Status
Case
65 yo ldquonot acting rightrdquo
rsaquo vomiting diarrhea fevers
PMHx None
Meds None
VS
T 392 P 118 RR 24 BP 8051 100 RA
101
128 38 7551187 58 6038
Recognition
Bimodal distribution
Predisposing conditions
Recent surgery
Unexplained tachycardia
Impaired perfusion
Delayed capillary refill
Lethargy
Irritability
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
SEPSIS
Case Altered Mental Status
Case
65 yo ldquonot acting rightrdquo
rsaquo vomiting diarrhea fevers
PMHx None
Meds None
VS
T 392 P 118 RR 24 BP 8051 100 RA
101
128 38 7551187 58 6038
Recognition
Bimodal distribution
Predisposing conditions
Recent surgery
Unexplained tachycardia
Impaired perfusion
Delayed capillary refill
Lethargy
Irritability
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Case Altered Mental Status
Case
65 yo ldquonot acting rightrdquo
rsaquo vomiting diarrhea fevers
PMHx None
Meds None
VS
T 392 P 118 RR 24 BP 8051 100 RA
101
128 38 7551187 58 6038
Recognition
Bimodal distribution
Predisposing conditions
Recent surgery
Unexplained tachycardia
Impaired perfusion
Delayed capillary refill
Lethargy
Irritability
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Case
65 yo ldquonot acting rightrdquo
rsaquo vomiting diarrhea fevers
PMHx None
Meds None
VS
T 392 P 118 RR 24 BP 8051 100 RA
101
128 38 7551187 58 6038
Recognition
Bimodal distribution
Predisposing conditions
Recent surgery
Unexplained tachycardia
Impaired perfusion
Delayed capillary refill
Lethargy
Irritability
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Recognition
Bimodal distribution
Predisposing conditions
Recent surgery
Unexplained tachycardia
Impaired perfusion
Delayed capillary refill
Lethargy
Irritability
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Physiology differences
Decr O2 delivery
Clinical exam
More myocardial
dysfunction
High CO low SVR
Low CO high SVR
(60)
Low CO low SVR
(20)
Decr O2 extraction
Lab parameters
Hypotension
High CO low SVR
Peds Adults
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
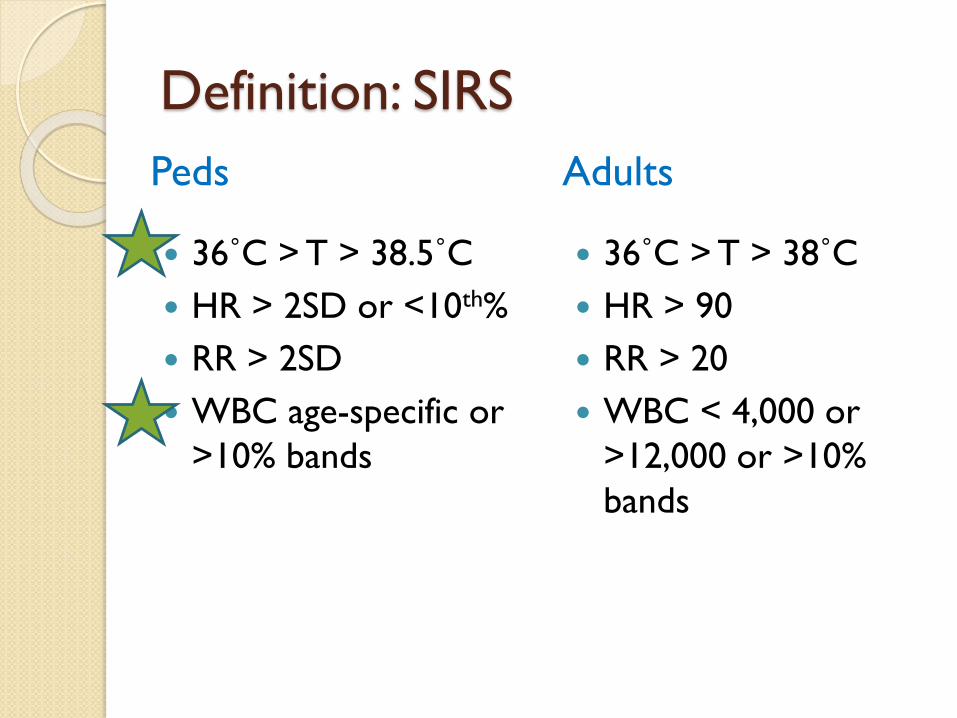
Definition SIRS
36˚C gt T gt 385˚C
HR gt 2SD or lt10th
RR gt 2SD
WBC age-specific or
gt10 bands
36˚C gt T gt 38˚C
HR gt 90
RR gt 20
WBC lt 4000 or
gt12000 or gt10
bands
Peds Adults
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
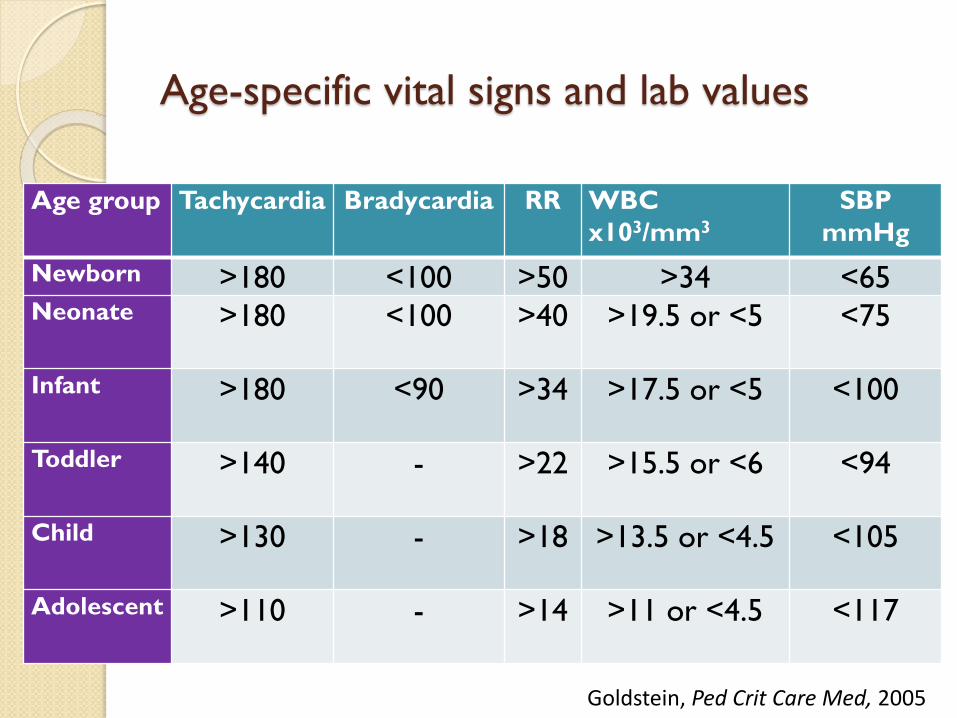
Age-specific vital signs and lab values
Age group Tachycardia Bradycardia RR WBC
x103mm3
SBP
mmHg
Newborn gt180 lt100 gt50 gt34 lt65Neonate gt180 lt100 gt40 gt195 or lt5 lt75
Infant gt180 lt90 gt34 gt175 or lt5 lt100
Toddler gt140 - gt22 gt155 or lt6 lt94
Child gt130 - gt18 gt135 or lt45 lt105
Adolescent gt110 - gt14 gt11 or lt45 lt117
Goldstein Ped Crit Care Med 2005
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
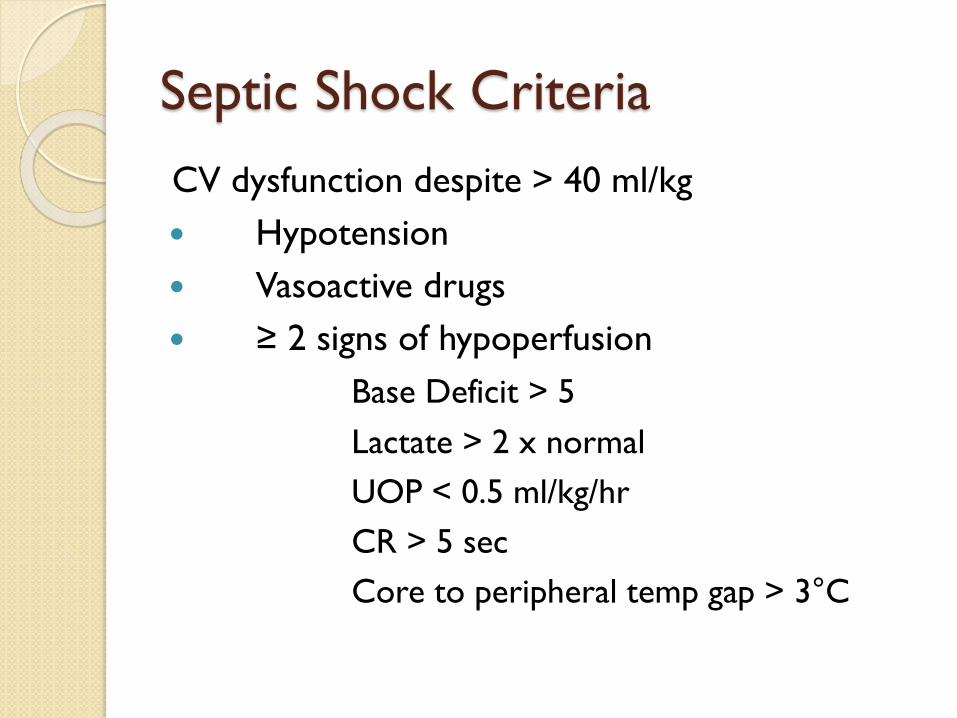
Septic Shock Criteria
CV dysfunction despite gt 40 mlkg
Hypotension
Vasoactive drugs
ge 2 signs of hypoperfusion
Base Deficit gt 5
Lactate gt 2 x normal
UOP lt 05 mlkghr
CR gt 5 sec
Core to peripheral temp gap gt 3degC
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90[2 x age] + 70
Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Clinical practice parameters
Children with septic shock
Proportionately larger fluid quantities
First hour fluid resuscitation
Inotrope and vasodilator therapies
Hydrocortisone
ECMO for refractory shock
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Clinical practice parameters
Children with septic shock
Earlier use of inotropic support through
peripheral access (incl intraosseous)
High flow humidified oxygen
Antibiotics within 1 hour
Therapeutic endpoints
Brierley et al Crit Care Med 2009Dellinger et al Crit Care Med 2013
Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Brierley Crit Care Med 2009
Infa
nts
an
d c
hild
ren
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
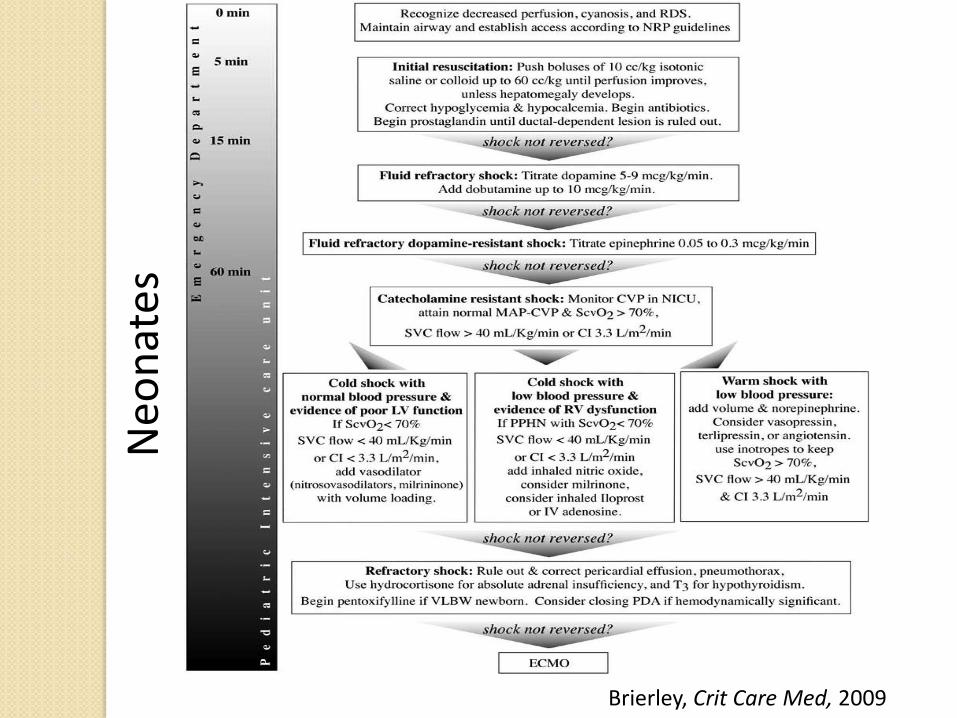
Brierley Crit Care Med 2009
Neo
nat
es
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
The Golden Hour
FIRST HOUR
Rapid access
HFNC
IVF bolus
Inotropes
Antibiotics
Prostaglandin
until ductal-dependent lesion ruled out
Hydrocortisone for adrenal insufficiency
Kissoon et al Pediatr Emerg Care 2010
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
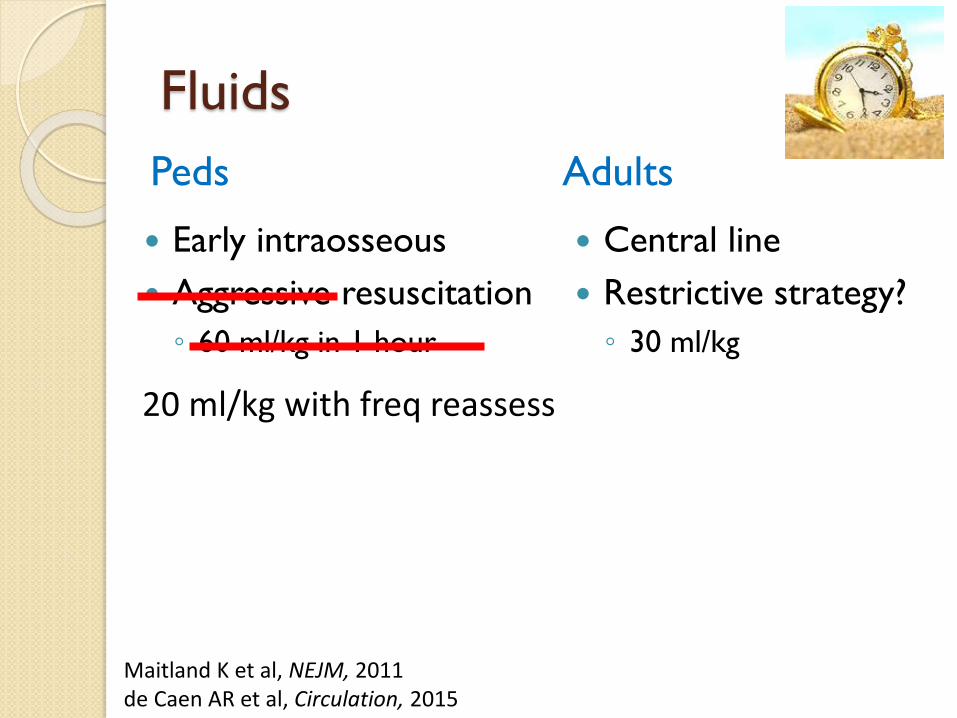
Fluids
Early intraosseous
Aggressive resuscitation
60 mlkg in 1 hour
Central line
Restrictive strategy
30 mlkg
Maitland K et al NEJM 2011de Caen AR et al Circulation 2015
20 mlkg with freq reassess
Peds Adults
Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Antimicrobials
Vancomycin
Ceftriaxone
Neonates
Ampicillin +
cefotaxime plusmn
Vancomycin
Acyclovir
Vancomycin
Zosyn
Peds Adults
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
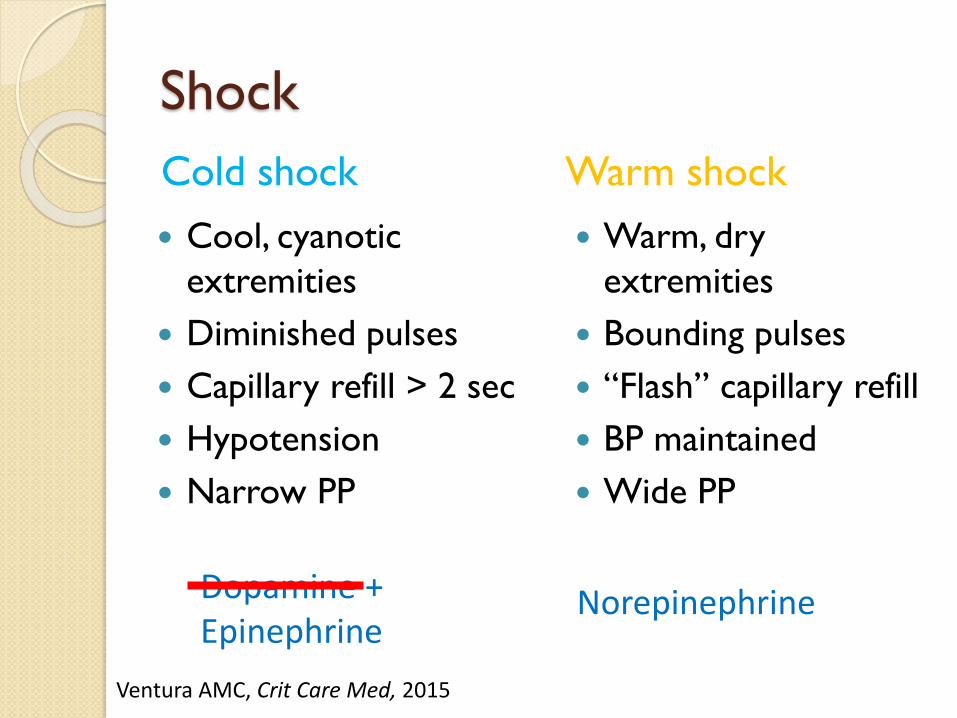
Shock
Cool cyanotic
extremities
Diminished pulses
Capillary refill gt 2 sec
Hypotension
Narrow PP
Warm dry
extremities
Bounding pulses
ldquoFlashrdquo capillary refill
BP maintained
Wide PP
Cold shock Warm shock
Dopamine + Epinephrine
Norepinephrine
Ventura AMC Crit Care Med 2015
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Vasopressors
Epinephrine= 1st line
Cold shock vs warm
shock
Peripheral or IO
Norepinephrine
No dopamine
Central line
Ventura AMC Crit Care Med 2015
Peds Adults
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Adjuncts
Dextrose
Vasopressin
Hydrocortisone
ECMO
Prostaglandin
Inhaled NO
Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Labs
VBG
Glucose
CBC
CMP
Lactate
Urinalysis culture
Blood culture
CRP
Procalcitonin
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Intubation ventilation
Induction ketamine
Atropine (lt 1 year)
Avoid etomidate
Paralytic agent
Tidal volume 6-8
mlkg
Plateau pressure
lt 30 mmHg
Jones P Pediatr Crit Care Med 2013Jones P PLoS One 2013de Caen AR et al Circulation 2015Fastle RK Pediatr Emerg Care 2004
Different Same
Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Optimize cardiovascular status prior to intubation
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Goals
Normalization of vitals
Improved perfusion
Capillary refill UOP gt 1 mlkghr mental status
Lactate clearance
ScvO2 gt 70
Transfusion
Ranjit Pediatr Crit Care Med 2014Sankar Pediatr Crit Care Med 2014
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Differences
Unexplained tachycardia
Cold shock
Epinephrine
Adrenal insufficiency
More fluids ()
Hypotension
Warm shock
Norepinephrine
Peds Adults
Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Summary
Understand age-specific parameters
Hypotension is a late sign
Time-specific goals
Early (and aggressive) fluid management
Early antibiotics
ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

ABDOMINAL DISORDERS
Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Ultrasound
Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Appendicitis
Clinical Scores
Alvarado A Ann Emerg Med 1986
Samuel M J Pediatr Surg 2002
Escriba Pediatr Emer Care 2011
Salo M Surg Res Pract 2014
Pogorelic et al Pediatr Emer Care 2015
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Alvarado score
Retrospective study
in adults
Sensitivity 75
Specificity 84
Prospective
validation in kids
Sensitivity 72-90
Specificity 72-79
Migration of pain 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Rebound pain 1
Elevation in temperature
(gt373˚C)
1
Leukocytes gt10000uL 2
Segmented neutrophilia
gt75
1
Alvarado Ann Emerg Med 1986
MANTRELS
Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Pediatric Appendicitis Score
Migration 1
Anorexia 1
Nausea vomiting 1
Tenderness RLQ 2
Coughhoppingpercus
sion tenderness in
RLQ
2
Pyrexia 1
Leukocytes
gt10000uL
1
Polymorphonuclear
neutrophilia gt75
1
1170 children age 4-15 yrs
Score ge 6 - appendicitis
Sensitivity 100
Specificity 92
PPV 96
NPV 90
Samuel J Ped Surg 2002Salo M Surg Res Pract 2014
Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Scoring systems
Score 1-3 no
appendicitis
Score 4-7 further
imaging (ultrasound)
Score 8-10 +appendicitis
Score 1-4 no
appendicitis
Score 5-8 further
imaging (ultrasound)
Score 9-10 +appendicitis
Alvarado score Pediatric Appendicitis Score
Escriba Ped Emerg Care 2011
Sens 933Spec 100
Sens 972Spec 976
Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Appendicitis
Timing
Narsule CK et al Am J Emerg Med 2011
Mendeville et al Pediatr Emer Care 2015
Analgesia
Delaney et al Pediatr Emer Care 2015
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
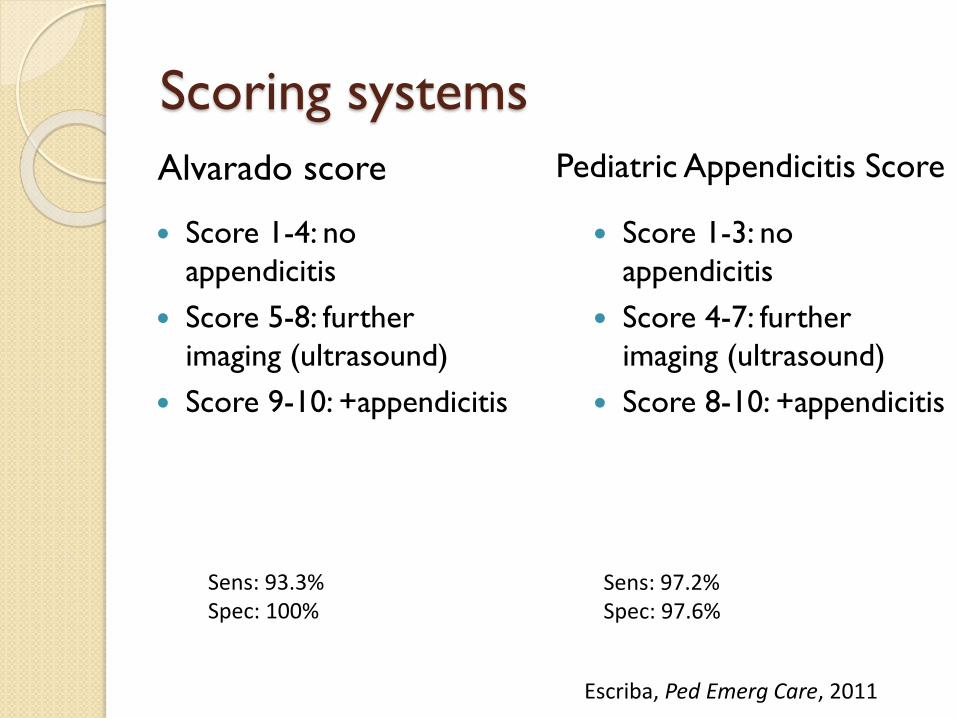
Appendicitis
Imaging
Aspelund G et al Pediatrics 2014
Sivitz AB et al Ann Emerg Med 2014
Elikashvili I et al Acad Emerg Med 2014
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
ABDOMINAL TRAUMA
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
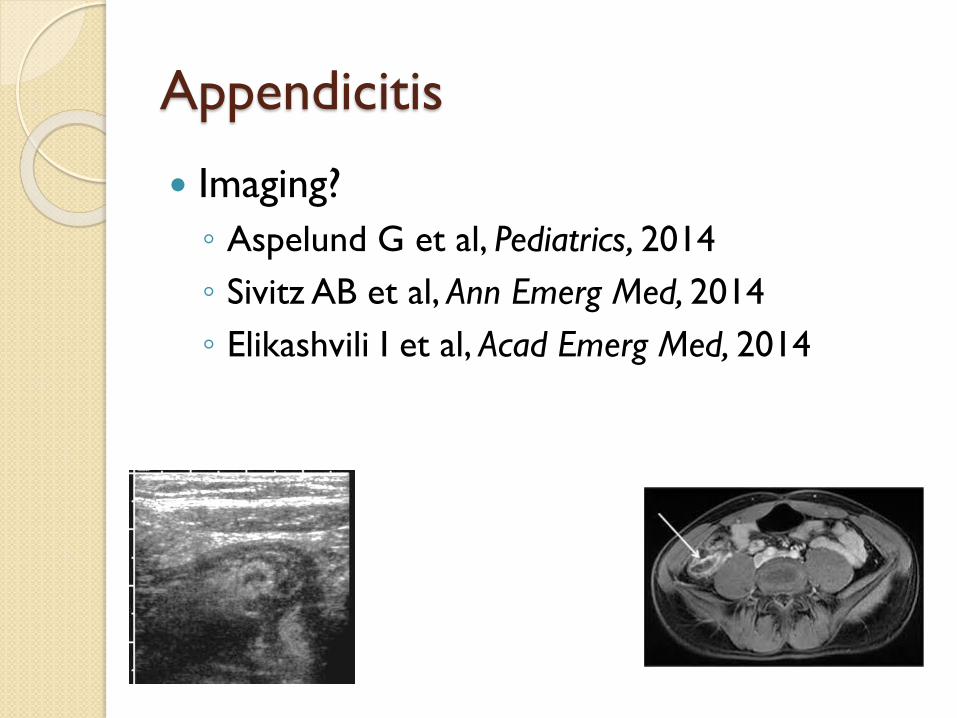
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
[2 x age] + 90
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
abdominal tenderness
Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Low risk
Ann Emerg Med 2012
Prospective observational cohort
Prediction rule to identify children with blunt
torso trauma at very low risk of intraabdominal
injuries requiring acute intervention
12044 children
761 (63) with intra-abdominal injuries
203 (267) received acute interventions
Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Blunt abdominal injuries
Prediction rule
No abdominal wall trauma or seat belt sign
Glasgow Coma Scale score gt13
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds and
No vomiting
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Blunt abdominal injuries
Results
NPV 999
Sensitivity 97
Specificity 425
Missed 65028 (01) with IAI
5 had lab abnormalities
All had hemoperitoneum
Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Holmes et al Ann Emerg Med 2012
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Fig 3 Suggested algorithm for evaluation of children with blunt torso trauma IAI ntra-abdominal injury
Holmes et al Ann Emerg Med 2002
Labs
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
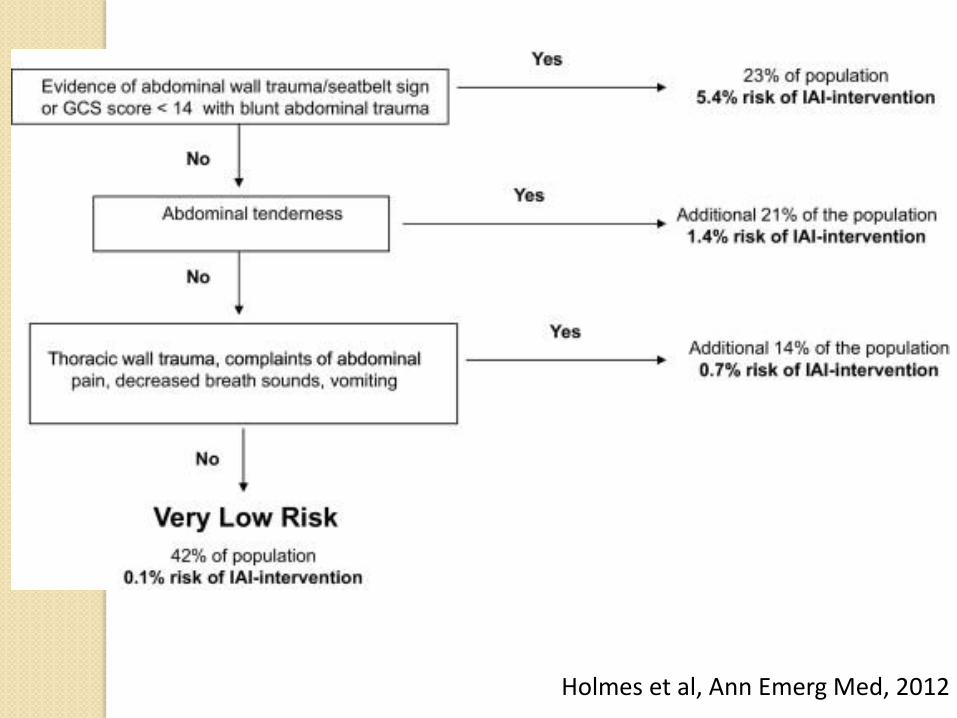
FAST in pediatrics
Less well defined vs adults
Poor sensitivity
may miss injury without associated fluid
Positive with IAI often non-operative
FF suprapubic region if prepubertal
Part of clinically integrated picture
Fox JC et al Acad Emerg Med 2011Scaife et al J Pediatr Surg 2013Menaker et al J Trauma Acute Care Surg 2014Mahajan et al Acad Emerg Med 2015Ben-Ishay et al World J Emerg Surg 2015
Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Case
8 yo male involved in MVC
VS 374 HR 96 RR 18 BP 11085 97
Exam well-appearing no complaints
Abdominal tenderness elevated LFTs
CT scan negative
Dispo
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Blunt abdominal injuries
Conclusion
A prediction rule based on HampP (without
laboratory or ultrasonographic information)
identifies children with blunt torso trauma who
are at very low risk for intra-abdominal injury
CT scan rarely misses clinically important blunt
abdominal traumatic injuries
Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Intussusception
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Intussusception plain films
Roskind et al Pediatr Emerg Care 2012
Conclusion
Findings on the 3-view abdominal radiograph
can decrease and potentially exclude the
diagnosis of ileocolic intussusception
In children with low pretest probability of
intussusception 3-view radiographs may obviate
the need for additional studies
Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Intussusception disposition
Chien et al J Emerg Med 2013
Retrospective chart review
98 children
10 recurrences in 7 children
Overall recurrence rate 71
Early recurrence rate 2
No adverse events
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Intussusception disposition
Conclusion
ED observation for 6 hours is safe alternative
to inpatient management for enema-reduced
intussusception
Colo-colonic reduced intussusception may have
an increased risk for recurrence
Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Summary
Ultrasound
Ultrasound
Ultrasound
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Point-of-Care Ultrasound for Pediatric ShockPark Daniel Presley Bradley Cook Thomas Hayden GeoffreyPediatric Emergency Care 31(8)591-598 August 2015
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Image gently
One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

One exceptionhellip
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Skeletal survey in abuse
Duffy et al Pediatrics 2011
2006 gt14000 child victims
703 consecutive patients
Retrospective descriptive study
Use of skeletal survey (SS) to identify children
most likely to have unsuspected fractures
How often SS results directly influence
diagnosis of abuse
Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Skeletal survey in abuse
Positive SS result = previously unsuspected
fracture
703 SS 108 positive results
79 had gt1 healing fracture
Highest rates
lt 6 months
ALTE or seizure
Suspected abusive head trauma
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Skeletal survey in abuse
Conclusion
Almost 11 of SS positive
In 50 positive SS cases results directly
influenced the decision to make the diagnosis of
abuse
Obtain SS in infants lt6 months with suspected
abuse
Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Take home points
Respiratory
HFNC
Early steroids (dexamethasone)
Sepsis
Early recognition fluids antibiotic
Abdominal disorders
LFTs for blunt abdominal trauma
Ultrasound
Be vigilant about NAT
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Questions
mluemumarylandedu
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Resuscitation pearls
Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Airway endotracheal tube
Children gt 2 yearsETT size (Age4) + 4
ETT depth (lip) ETT size x 3
Cuffed tube okay
Except newborns (lt30 days)
ETT size (Age4) + 35
Uncuffed tube
Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Airway pre-term tube sizes
ETT = uncuffed endotracheal tube size
20-25 week gestation
25-30 week gestation
30-35 week gestation
35-40 week gestation
20-25 ETT
25-30 ETT
30-35 ETT
35-40 ETT
Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Breathing
Age RR
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-aged 18-30
Adolescent 12-16
gt 60
gt30
gt15
Normal RR may reflect fatigue
Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Circulation
Heart rate
Pulse quality
Capillary refill time
Skin temperature
Blood pressure
([2 x age] + 70)
[2 x age] + 90
Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Delayed cap refill thready pulses cool extremities
Hypotension is a LATE sign
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
[2 x age] + 90
Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Dextrose
Ill patients with depressed mental status are
hypoglycemic until proven otherwise
Treat for BS lt 50
Rule of 50
D10 5 mlkg (age lt 1 year)
D25 2 mlkg (age 1 ndash 8 year)
D50 1 mlkg (age gt 8 year)
Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube

Vital signs
[2 x age] + 10 kg
Estimate weight in kilograms
Broselow tape
PAWPER tape
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Apps
PalmPEDi
BlueCardCNMC
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube
Resuscitation Numbers
SBP (2 x age) +90
Wt (2 x age) + 10 kg
RR 603015 rule
1 x ETT (Age4) + 4
2 x ETT NGOGFoley
3 x ETT Depth
4 x ETT Chest tube