Update: Rheumatoid Arthritis ACR/ARHP 2008ACR/ARHP 2008.
87
Update: Rheumatoid Arthritis ACR/ARHP 2008
-
Upload
martin-lamb -
Category
Documents
-
view
215 -
download
2
Transcript of Update: Rheumatoid Arthritis ACR/ARHP 2008ACR/ARHP 2008.
Update:Rheumatoid Arthritis
ACR/ARHP 2008

ACR/ARHP 2008: Update on Rheumatoid Arthritis Efficacy and safety of repeat treatment courses of rituximab in rheumatoid arthritis patients
with inadequate response to tumour necrosis factor inhibitors: long-term experience from the REFLEX study
Long-term safety of rituximab: a six-year follow-up of the rheumatoid arthritis clinical trials and re-treatment population
Efficacy and safety of various dosing regimens of rituximab in patients with active rheumatoid arthritis: results of a phase III randomized study (MIRROR)
Safety of other biologic therapies following rituximab treatment in RA patients
Improved quality of life with rituximab as first-line biologic therapy in patients with active rheumatoid arthritis: results from a phase III, randomized, controlled study (SERENE)
Prospective follow-up of rituximab treatment in 965 patients with refractory rheumatoid arthritis: tolerance and efficacy data from the French Registry AIR (Autoimmunity and Rituximab)
ACR and DAS 28 response over 24 weeks in rheumatoid arthritis patients treated with rituximab after an inadequate response to one tumour necrosis factor inhibitor
Efficacy, safety, and dose frequency of re-treatment with rituximab in rheumatoid arthritis: results from a randomized, controlled trial (SUNRISE)
ACR = American College of RheumatologyARHP = Association of Rheumatology Health Professionals

Efficacy and safety of repeat treatment courses of rituximab (RTX) in RA patients (pts) with
inadequate response (IR) to tumour necrosis factor (TNF) inhibitors: long-term experience
from the REFLEX study
Keystone EC, et al. ACR/ARHP 2008; Abstract 367.

Clinical trials using rituximab as selective B-cell–targeted therapy have demonstrated significant efficacy and safety in modifying the signs and symptoms of rheumatoid arthritis (RA).1,2,3
In the phase III REFLEX study, Cohen and colleagues demonstrated the efficacy and safety of rituximab in RA patients who had an inadequate response to at least one tumour necrosis factor (TNF) inhibitor.1
ACR/ARHP 2008: Keystone and colleagues presented updated interim data from an open-label extension of the REFLEX study designed to evaluate long-term safety and efficacy of rituximab in this patient population.4
Background
ACR = American College of RheumatologyARHP = Association of Rheumatology Health Professionals
1. Cohen SB, et al. Arthritis Rheum 2006;54(9):2793–2806. 2. Edwards JC, et al. N Engl J Med 2004;350(25):2572–2581. 3. Emery P, et al. Arthritis Rheum 2006;54(5):1390–1400. 4. Keystone EC, et al. ACR/ARHP 2008; Abstract 367.
Criteria for re-treatment with rituximab included:
• reduction of ≥20% in both swollen joint count (SJC) and tender joint count (TJC) during any follow-up visit from week 16, following initial treatment in REFLEX;
• active RA with SJC ≥8 (66 joint count) and TJC ≥8 (68 joint count);
• need for repeated course as determined at the discretion of the physican.
Patients who received placebo in the initial treatment arm received open-label rituximab (2 x 1000 mg).
All treatment courses with rituximab consisted of two 1000 mg IV infusions separated by 2 weeks.
Study design: REFLEX extension study
Keystone EC, et al. ACR/ARHP 2008; Abstract 367.

Study design: REFLEX extension study (cont’d)

Study design: REFLEX extension study (cont’d)
Rituximab infusions were all premedicated with IV glucocorticoids (100 mg methylprednisolone).
A 14-day course of oral prednisone was also administered.
All patients continued to receive MTX (10–25 mg per week), with allowance for a dose reduction due to intolerance.
Primary and secondary efficacy measures included the ACR 20%, 50%, and 70% improvement criteria (ACR20/50/70), the EULAR responses (moderate/good), DAS28, low disease activity, and DAS remission.
Efficacy was calculated relative to the original baseline assessed prior to the administration of the first course of rituximab.
Keystone EC, et al. ACR/ARHP 2008; Abstract 367.
ACR = American College of RheumatologyDAS = Disease Activity ScoreEULAR = European League Against Rheumatism
Key findingsBaseline characteristics and disposition
Of the 502 patients randomized to REFLEX, a total of 480 patients were treated with rituximab, either as randomized treatment or following a switch from placebo (n = 172, 35.8%).
Of these patients, 307 received two courses (C2), 235 patients received three courses (C3), 146 patients received four courses (C4), and 58 patients received five courses (C5)
Over four courses, a total of 230 patients withdrew from treatment. The primary reason for withdrawal was lack of efficacy/other reasons (192 patients, 40%), with 26 patients (5.4%) withdrawing because of adverse events (AEs).
The majority of the withdrawals (157 patients, 33%) occurred during the first course (C1). Of the remaining patients, 12%, 9%, and 11% withdrew following C2, C3, and C4, respectively.
Of the 235 patients who received a third course, 179 had an efficacy analysis at 24 weeks, following C3, and were included in the efficacy analysis.
Keystone EC, et al. ACR/ARHP 2008; Abstract 367.

Key findings (cont’d)
Efficacy
Of the 408 patients treated with rituximab, 235 patients received ≥3 courses. Of these, 179 patients had completed 24 weeks of follow-up after each treatment course, which permits a within-patient analysis by course.
Within-patient comparison of ACR 20, 50, and 70 scores at 24 weeks following C1, C2, and C3 showed that repeated treatment with rituximab was effective over multiple courses.
ACR 20 responses at week 24 following each course were maintained or increased with subsequent courses, while ACR 50 and 70 responses improved. ACR70 responses increased from 14% following C1 to 26% following C3.
The proportion of patients with a EULAR response was comparable for C1 to C3, with over 80% of patients achieving a EULAR good/moderate response with each course.
The proportion of patients receiving a EULAR good response showed an increase with each treatment (C1, 17%; C2, 26%; C3 34%).
Sustained improvement in DAS2 low disease activity and remission was observed during C2 and C3, with remission rates increasing from 8.8% to 17.6% from C1 to C3.
Keystone EC, et al. ACR/ARHP 2008; Abstract 367.
ACR = American College of RheumatologyC = courseEULAR = European League Against Rheumatism
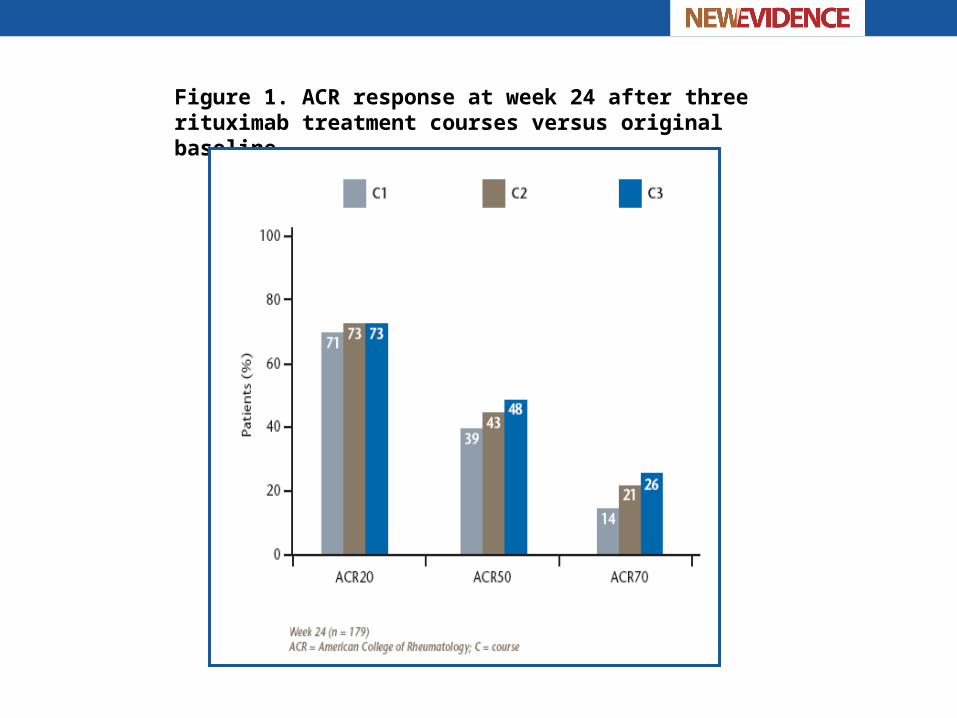
Figure 1. ACR response at week 24 after three rituximab treatment courses versus original baseline

Figure 2. EULAR response at week 24 after three rituximab treatment courses versus original baseline

Figure 3. Percentage of patients achieving DAS28 low disease activity or remission at week 24 after three rituximab treatment courses versus original baseline

Key findings (cont’d)Safety
AE rates per 100 patient-years (95% CIs) in each treatment course remained relatively stable between courses (377–399 events per 100 patient years).
Majority of AEs reported were mild to moderate (grade 1/2) in severity, with an observed reduction in reported AEs over treatment courses.
AE rate leading to withdrawal decreased significantly from C1 (3.5%) to C3 (1.7%).
Incidence of commonly reported AEs remained stable with each treatment course, although incidences of RA exacerbations declined over subsequent courses.
SAE rates per 100 patient-years did not vary significantly between courses.
Incidence of infusion-related reactions (IRRs) decreased with each repeat course, with 26% of patients experiencing an IRR during C1, 17% during C2, and 12% during C3.
IRRs were most frequent during the initial infusion of the first course (22%).
The rate of all infections showed a general increase from C1 (96.8 events/100 patient years) to C3 (119.9 events/100 patient years), although confidence intervals (CIs) were wide and overlapping.
In total, 87 serious infection events (SIEs) were reported, providing an overall rate of 6.75 events/100 patient-years. The SIE rate remained stable from C1 to C3, with wide and overlapping CIs.
No opportunistic infections or cases of tuberculosis were reported.
Keystone EC, et al. ACR/ARHP 2008; Abstract 367.


Key conclusions
In patients with active RA and an IR to TNF inhibitors, repeated courses of rituximab showed a comparable degree of sustained efficacy relative to the original baseline.
The safety profile observed over this extended observation period is consistent with that previously reported for rituximab, with no evidence of newly emerging safety concerns.
Keystone EC, et al. ACR/ARHP 2008; Abstract 367.

Long-term safety of rituximab:6-year follow-up of the RA clinical trials
and re-treatment population
Van Vollenhoven RF, et al. ACR/ARHP 2008; Abstract 361.

Background
Rituximab has been shown to be effective and well tolerated in the treatment of patients with active rheumatoid arthritis (RA).1–3
Rituximab acts by selectively depleting CD20-positive B cells. This novel mode of action differs from that of other biologic agents and DMARDs.1–3
Treatment with rituximab produces peripheral B-cell depletion, which is either maintained or re-induced with multiple courses. The safety of long-term B-cell depletion is currently being evaluated in open-label studies with rituximab.1–3
ACR/ARHP 2008: van Vollenhoven and colleagues presented a pooled analysis of safety data collected from RA patients treated with rituximab in combination with methrotrexate (MTX) from several of the international clinical trials such as the phase II DANCER and SIERRA trials, and the phase III SERENE, SUNRISE, MIRROR, and REFLEX studies.4
ACR = American College of RheumatologyARHP = Association of Rheumatology Health ProfessionalsDMARD = disease-modifying anti-rheumatic drug
1. Cohen SB, et al. Arthritis Rheum 2006;54(9):2793–2806. 2. Edwards JC, et al. N Engl J Med 2004;350(25):2572–2581. 3. Emery P, et al. Arthritis Rheum 2006;54(5):1390–1400. 4. Van Vollenhoven RF, et al. ACR/ARHP 2008; Abstract 361.

Study design The safety data for this analysis was collected from RA patients treated with
rituximab in combination with methrotrexate (MTX) in an international clinical trials program
Patients initially randomized to placebo and subsequently treated with rituximab were also included in the analysis, from the start of treatment with rituximab.
Prior to each infusion of rituximab, patients received peri-infusional corticosteroids (methylprednisolone 100 mg IV), and, in some cases, additional oral corticosteroids, depending on the specific study.
Data were available from 2578 patients, accounting for 5013 patient-years of exposure to rituximab.
A total of 2244 patients were observed for ≥1 year, 851 for ≥2 years, 720 for ≥3 years, 317 for ≥4 years, and 97 for ≥ 5 years.
All 2578 patients received at least one treatment course, and a total of 1890, 1043, 425, and 133 patients received ≥2, ≥3, ≥4, and ≥5 courses, respectively.
The maximum number of courses administered was 10 (n = 1).
Van Vollenhoven RF, et al. ACR/ARHP 2008; Abstract 361. RA = rheumatoid arthritis
Key findings The rate of adverse events (AEs) by rituximab course decreased after the first
course (C1), and subsequently stabilized, following multiple courses of rituximab.
The most commonly reported AEs were those associated with infusion reactions, especially during C1.
Infusion reactions
Infusion reactions during the first infusion of each course decreased from 25% in C1 to 13%, 9%, 9%, and 3% in C2, C3, C4, and C5, respectively.
The most common events reported during infusions were headache, pruritus, throat irritation, flushing, rash, uticaria, hypertension, and pyrexia. Most reactions were mild or moderate in severity.
Thirteen patients (0.5%) experienced a total of 18 serious infusion reactions. These reactions were variable in nature and included rash, headache, blood pressure changes, anaphylactic reactions, and edema. Twelve of these 18 events occurred following the first infusion of C1. There were no serious infusion-related reactions (IRRs) beyond C2.
The proportion of patients who reported IRRs that required slowing, stopping, or interruption of treatment with rituximab was the highest after C1 (9%), and subsequently decreased to 5%, 3%, and 2% after C2, C3, and C4, respectively.
Overall, <1% of patients withdrew because of IRRs.
Van Vollenhoven RF, et al. ACR/ARHP 2008; Abstract 361. C = course

Figure 1. Incidence of acute infusion reactions by treatment course of rituximab

Key findings (cont’d)
Infections1
A total of 1663 patients (65%) experienced ≥1 infection (both non-serious and serious), with an overall rate of infection of 97.7 events/100 patient-years (95% CI, 95–100.5).
The most common infections were upper respiratory tract infections (19%), nasopharyngitis (13%), urinary tract infections (11%), bronchitis (10%), diarrhea (9%), sinusitis (8%), and influenza (5%).
A total of 170 (7%) patients experienced a serious infection event (SIE), providing an SIE rate of 4.31/100 patient-years (95% CI, 3.77–4.92).
The most common serious infection was pneumonia, affecting 2 (1%) patients. No cases of tuberculosis were reported in this population.
Rates of overall and serious infections were stable between courses.
Analysis of infections during consecutive twelve-month intervals, irrespective of multiple courses, showed no evidence of increased risk of infection over time.
The rate of overall, but not serious, infection was highest in the initial year of treatment with rituximab.
The overall rate of infection for rituximab-treated patients was similar to that previously reported for other therapies in patients with RA.2,3
1. Van Vollenhoven RF, et al. ACR/ARHP 2008; Abstract 361.2. Dixon WG, et al. Arthritis Rheum 2006;54(8):2368–2376. 3. Listing J, et al. Arthritis Rheum 2005;52:3403–3412.
CI = confidence intervalRA = rheumatoid arthritis

Figure 2. Overall rate of infections per 100 patient-years

Figure 3. Rate of serious infections per 100 patient-years

Figure 4. Incidence of serious infections per 100 patient-years

Key findings (cont’d)
Immunoglobulins
At baseline, prior to receiving rituximab, 38 (1.5%) and 41 (1.7%) patients had IgM and IgG below the lab lower limit of normal (LLN), respectively.
Serum immunoglobulins (Ig), expecially IgM, decreased following multiple courses of rituximab; 620 (23%) and 141 (5%) of patients developed IgM and IgG below the LLN, respectively.
Median Ig levels were >LLN during the entire follow-up period. There were no cases of undetectable Ig levels.
IgG decreases were often transient and sustained low IgG (<LLN for at least one year) was observed in 32 (1.2%) of patients. Decreases in IgG were related to corticosteroidal use and older age.
Older age was an independent predictor of sustained low IgG (HR 1.43; 95% CI, 1.24–1.63, p <0.001 for every 10 years of increased baseline age).
Serious infection rates were similar prior to and after the detection of low IgM or IgG.
Patients with low IgM did not have increased rates of serious infection. Patients with low IgG had increased point estimates of infection rates, both prior to and after detection of low levels.
It is unclear if rituximab-treated patients with low IgG are at increased risk of infection.
Van Vollenhoven RF, et al. ACR/ARHP 2008; Abstract 361.CI = confidence intervalHR = hazard ratio
Key findings (cont’d)
Malignancies1
The overall incidence of malignancies (excluding non-melanoma skin cancer) was 1.06/100 patient-years, of which 41 were reported as serious adverse events (SAEs) (0.82/100 patient-years).
The incidence of malignancy did not increase with multiple courses or rituximab.
There was no difference in the overall rate of pattern of malignancy in patients treated with rituximab, when compared with other patients with RA described in epidemiologic studies.2–4
1. Van Vollenhoven RF, et al. ACR/ARHP 2008; Abstract 361.2. Mellemkjaer L, et al. Eur J Cancer 1996;32(10):1753–1757. 3. Watson K, et al. Rheumatology 2006;45(Suppl 1):i10. 4. Wolfe F , et al. Arthritis Rheum 2007;56:2886–2895. RA = rheumatoid arthritis

Key conclusions
In this update on safety in RA clinical trials, rituximab was well tolerated over multiple courses and consistent with previous studies. No new safety concerns were identified.
The overall rates for AEs and SAEs were stable over time and subsequent treatment courses.
Infections, including serious infections—a potential concern for prolonged B-cell depletion—did not increase over time, or with multiple courses of rituximab.
Ig levels, in particular IgM, decreased with multiple courses of rituximab, although this was not associated with increased risk of infection.
The rate of malignancies was consistent with previous studies and with the incidence of malignancy in patients with RA.
Van Vollenhoven RF, et al. ACR/ARHP 2008; Abstract 361.AE = adverse event; Ig = immunoglobulinRA = rheumatoid arthritis; SAE = serious adverse event

Efficacy and safety of various dosing regimens of rituximab in patients with active RA:
results of a phase III randomized study (MIRROR)
Rubbert-Roth A, et al. ACR/ARHP 2008; Abstract 363.
Background
Rituximab (2 x 1000 mg) has been shown to successfully treat patients with an intolerance or an inadequate response (IR) to tumour necrosis factor (TNF) inhibitor therapies.1
Significant clinical improvements in disease symptoms have also been reported in patients with an IR to disease-modifying anti-rheumatic drugs (DMARDs) treated with rituximab (2 x 500 mg and 2 x 1000 mg) in combination with methotrexate (MTX).2
The effects of repeat treatment and of dose escalation were not explored.
ACR/ARHP 2008: Rubbert-Roth and colleagues presented the results of the phase III, randomized MIRROR study to evaluate the efficacy and safety of three dosing regimens of rituximab in combination with MTX in patients with active RA who respond inadequately to MTX and who had been previously treated with no more than one biologic agent approved for use in RA.3
1. Cohen SB, et al. Arthritis Rheum 2006;54(9):2793–2806. 2. Emery P, et al. Arthritis Rheum 2006;54(5):1390–1400. 3. Rubbert-Roth A, et al. ACR/ARHP 2008; Abstract 363. RA = rheumatoid arthritis

Study design Key inclusion criteria were as follows:
• patients ≥18 years old who had been diagnosed with RA for ≥6 months;
• Swollen joint count (SWC) ≥8 (66 joint count), and tender joint count (TJC) ≥8 (68 joint count) at screening and baseline;
• elevated baseline values of C-reactive protein (CRP) ≥0.6 mg/dL (6 mg/L), or erythrocyte sedimentation rate (ESR) ≥28 mm/h;
• Inadequate response to methotrexate (MTX) at 10–25 mg/week for ≥12 weeks;
• Absolute neutrophil count ≥1500/μL, hemoglobin level ≥8 g/dL, immunoglobin (Ig)M and IgG levels ≥40 and 500 mg/dL.
A total of 30% of the study population were permitted to have received ≤1 previous biologic agent approved for use in RA.
Rubbert-Roth A, et al. ACR/ARHP 2008; Abstract 363. RA = rheumatoid arthritis

Study design (cont’d)
Patients were randomized to three treatment groups. All patients received a first course of two infusions of rituximab on days 1 and 15, with a second course administered between weeks 24 and 26 according to the treatment group:
• reduced dose group (RD) (2 x 500 mg at baseline and week 24);
• dose escalation group (DE) (2 x 500 mg at baseline and 2 x 1000 at week 24);
• standard dose group (SD) (2 x 1000 mg at baseline and week 24).
Primary endpoint was ACR20 response at week 48.
Secondary endpoints included ACR50/70 and EULAR moderate/good responses.
Rubbert-Roth A, et al. ACR/ARHP 2008; Abstract 363.ACR = American College of RheumatologyEULAR = European League Against Rheumatism

Study design (cont’d)
Key findings Because of errors in a medication pack list which rendered an intent-to-treat (ITT)
analysis as randomized invalid, results presented are from a modified ITT analysis performed with patients analyzed by treatment received (mITT population).
Sensitivity analyses using the standard ITT as randomized were conducted and were consistent with the modified ITT presented.
Demographic and baseline disease activity were well balanced across the 3 treatment groups.
Of the 378 patients recruited, 346 patients were treated with a protocol-defined regimen, and 334 (88%) patients completed 24 weeks of follow-up. From all three treatment groups, 321 (85%) patients received a second treatment course, and 314 (83%) patients completed the full 48-week period of the study.
A majority of patients (66%) across all three treatment arms achieved at least an ACR20 response at week 48.
Response rates in the SD group were somewhat higher than those in both the RD and DE arms, but the difference was not statistically significant.
The proportion of patients achieving ACR50 and ACR70 was also higher in the SD arm, but no statistically significant difference between the treatment arms was achieved.
Distribution of EULAR responses was significantly better in the SD group, compared with the RD group, with 89.2% versus 73% achieving a EULAR good or moderate response, respectively (p = 0.0495).
Rubbert-Roth A, et al. ACR/ARHP 2008; Abstract 363.
ACR = American College of Rheumatology; DE = dose escalation group;EULAR = European League Against RheumatismRD = reduced dose group; SD = standard dose group

Figure 1. ACR responses at week 48 following treatment with reduced dose, dose escalation, or standard dose rituximab
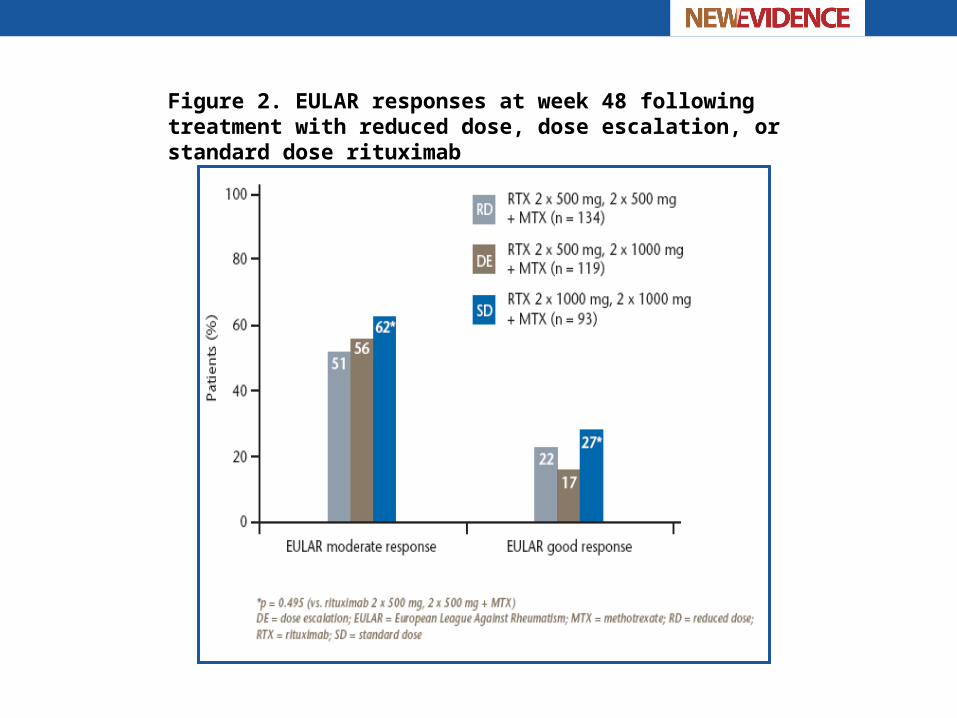
Figure 2. EULAR responses at week 48 following treatment with reduced dose, dose escalation, or standard dose rituximab

Key findings (cont’d)
A subgroup analysis examined the effect at week 48 of repeat treatment on patients who had not achieved an ACR20 response to the initial course of rituximab.
In total, 42% to 48% of these patients achieved an ACR20 response after a second course of treatment. The dose regimen did not appear to have a significant impact; however, response rates were higher in those patients who had received initial treatment and repeated treatment with 2 x 1000 mg.
Over 80% of patients who achieved at least an ACR20 response to their first course of treatment maintained this response during the second course of treatment, irrespective of dose.
A comparison of ACRn score by category (<20, >20) using a shift analysis showed that 28% to 37% of patients who achieved an ACRn ≥20 at week 24 improved their ACR response category at week 48.
Conversely, 35% of patients receiving RD had a worse ACR response at week 48, compared with 22% of SD patients.
Regardless of prior biologic therapy, ACR and EULAR outcomes for the SD regimen were consistently higher than those of the RD regimen. But patient numbers are small and no statistical significance was observed.
Rubbert-Roth A, et al. ACR/ARHP 2008; Abstract 363.
ACR = American College of Rheumatology; DE = dose escalation group;EULAR = European League Against RheumatismRD = reduced dose group; SD = standard dose group

Figure 3. ACR responses at 48 weeks: prior/no prior biologic subgroups (mITT)

Figure 4. EULAR moderate/good responses at 48 weeks:prior/no prior biologic subgroups (mITT)

Key findings (cont’d)
Safety
All three rituximab regimens were well tolerated and demonstrated comparable safety through 48 weeks.
The most common adverse events (AEs) were infusion-related reactions (IRRs) at 39%, 30%, and 30% for RD, DE, and SD, respectively.
The proportion of patients experiencing infusion reactions was highest with the first infusion of the first course, lower with subsequent infusions, and similar across dosing regimens.
Other common AEs included RA flares (18%, 20%, and 15%, for RD, DE, and SD, respectively), and upper respiratory tract infections (12%, 14%, and 11% for RD, DE, and SD, respectively).
Incidences of serious AEs leading to withdrawal, infections, lower gastrointestinal events, cardiac events, vascular events, and malignancies, were similar across treatment arms.
Overall rate of infections (non-serious and serious) across the three treatment groups was 120.81–159.16 infections per 100 patient-years; the rate of serious infection was 2.36–4.73 per 100 patient-years. No clear difference in rates of infections was observed across the dosing regimens.
No deaths were reported during this study.
Rubbert-Roth A, et al. ACR/ARHP 2008; Abstract 363.DE = dose escalation group; RA = rheumatoid arthritisRD = reduced dose group; SD = standard dose group

Key conclusions
Rituximab is effective and well tolerated in patients with an inadequate response to methotrexate, including patients receiving one prior biologic agent.
The reduced dose and standard dose could not be clearly differentiated after 48 weeks of treatment, although some efficacy outcomes suggest improved outcomes in the standard dose group.
Dose escalation did not appear to be associated with improved responses.
Overall, repeat treatment maintained response to the first course and may have incremental benefits.
Repeat treatment may also elicit response in patients non-responsive to their initial treatments.
Rubbert-Roth A, et al. ACR/ARHP 2008; Abstract 363.
Safety of other biologic therapies following rituximab treatment in RA patients
Genovese M, et al. ACR/ARHP 2008; Abstract 1671.

Background
ACR/ARHP 2008: Genovese and colleagues presented results of a study to assess the rate of serious infection events (SIEs) in rheumatoid arthritis (RA) patients previously treated with rituximab and who subsequently received a further biologic RA therapy.
Genovese M, et al. ACR/ARHP 2008; Abstract 1671.

Study design
Patients with moderate-to-severe active RA who had been treated with rituximab plus methotrexate within an international clinical trial program were included in the study.
Following withdrawal from their respective studies, patients entered a safety follow-up (SFU) during which peripheral B-cell counts were monitored at regular intervals for ≥48 weeks.
During SFU, patients were permitted to receive addition biologic therapies.
Data on all serious infection events (SIEs) were collected throughout the SFU period.
SIEs were defined as infections that required intravenous antibiotics or where at least one of the following applied:
• patient required hospitalization or existing hospitalization was prolonged;
• infection was immediately life-threatening;
• infection caused persistent or significant disability or incapacity;
• intervention was required to prevent one of the previously mentioned outcomes;
• infection was fatal.
Genovese M, et al. ACR/ARHP 2008; Abstract 1671.

Key findings At the time of data cut-off (November 2007), 2578 RA patients had received at least one
course of rituximab (some patients may have received multiple courses), providing 5013 patient-years of follow-up.
Overall rate of SIE in this population was 4.31 (95% CI, 3.77–4.92) per 100 patient-years.
Of patients who withdrew into SFU, 185 patients were subsequently treated with another biologic (150 received tumour necrosis factor (TNF) inhibitors, 25 received abatacept, and 10 received anakinra or experimental biologics).
Median follow-up time after receipt of the subsequent biologic was 11 months (range: 0–45 months).
Majority of patients had peripheral B-cell depletion with CD19 levels below the lower limit of normal at the time of receiving further RA treatment.
This group of patients reported a total of 13 SIEs in 186.05 patient-years follow-up(6.99 events/100 patient-years; 95% CI, 4.06–12.03) during treatment with rituximab and prior to the receipt of the biologic.
Ten SIEs in 182.31 patient-years were reported following the initiation of the biologic (5.49 events/100 patient-years; 95% CI 2.95–10.19).
Median time to SIE after initiating biologic therapy was 4 months (range: 0–23 months).
Overall, infections were variable and typical for RA patients.
No opportunistic or fatal infections occurred.
Genovese M, et al. ACR/ARHP 2008; Abstract 1671.CI = confidence intervalRA = rheumatoid arthritis

Figure 1. Subsequent treatment with another biologic


Key conclusions
In this updated, exploratory analysis, the use of other biologic therapies in RA patients previously treated with rituximab was not associated with an increase in the rate of serious infections.
Controlled trials of combination therapy of rituximab and other biologics is ongoing.
Genovese M, et al. ACR/ARHP 2008; Abstract 1671. RA = rheumatoid arthritis

Improved quality of life (QoL) with rituximab (RTX) as first-line biologic therapy in
patients (pts) with active rheumatoid arthritis (RA): results from a phase III randomized
controlled study (SERENE)
Deodhar A, et al. ACR/ARHP 2008; Abstract 365.

Background
Rituximab, a monoclonal antibody that selectively targets CD20-positive B cells, has demonstrated significant efficacy and a good safety profile in clinical trials conducted in patients with active rheumatoid arthritis (RA).1–3
RA is associated with progressive functional decline and decreased quality of life (QoL), making the use of patient-reported outcomes (PROs) of interest in evaluating patient response to rituximab.
ACR/ARHP 2008: Deodhar and colleagues presented data from the SERENE study evaluating the effect of rituximab on physical function, disability, and health-related QoL in patients with active RA who have had an inadequate response to methotrexate, and have not received prior biologic therapy.4
1. Edwards JC, et al. N Engl J Med 2004;350(25):2572–2581. 2. Smolen JS, et al. Ann Rheum Dis 2007;66:143–150.3. Cohen SB, et al. Arthritis Rheum 2006;54(9):2793–2806. 4. Deodhar A, et al. ACR/ARHP 2008; Abstract 365.
ACR = American College of RheumatologyARHP = Association of Rheumatology Health Professionals

Study design The SERENE study was a multicentre, randomized, double-blind, placebo-
controlled, phase III trial conducted at 105 centres in 11 countries.
Key eligibility criteria was as follows:
• age 18–80 years with active RA for ≥6 months according to ACR criteria;
• SJC and TJC ≥8 at screening and baseline with C-reactive protein (CRP) ≥0.6 mg/dL and/or erythrocyte sedimentation rate (ESR ) ≥28 mm/h at screening;
• IR to methotrexate (MTX) (10–25 mg/week for at least 12 weeks) and no prior biologic therapy for RA;
• Absolute neutrophil count ≥1500 μL, hemoglobin level ≥8 g/dL, immunoglobulin (Ig)M and IgG levels ≥40 and 500 mg/dL, respectively.
Patients received prophylactic treatment with intravenous methylprednisone (100 mg) to reduce the incidence and severity of infusion reactions.
All patients continued to receive MTX (10–25 mg/week) at a stable dose with folic acid (≥5 mg/week or equivalent).
Deodhar A, et al. ACR/ARHP 2008; Abstract 365.
ACR = American College of RheumatologyIR = inadequate response; RA = rheumatoid arthritisSJC = swollen joint count; TJC = tender joint count

Study design (cont’d)

Study design (cont’d)
From week 24, all eligible patients (DAS ≥2.6 and all safety criteria met) were re-treated with rituximab.
Patients who received placebo for the first 24 weeks were switched to rituximab (2 x 500 mg), while patients in the original active arms were re-treated with the same dose of rituximab (2 x 500 mg or 2 x 1000 mg).
The study remained double-blinded to treatment and dose through week 48.
Clinical assessments were made according to the ACR core set of disease-activity measures at baseline every 4 weeks from week 4 to week 24, and every 8 weeks thereafter.
Primary endpoint was assessment of the proportion of patients in each treatment arm achieving an ACR20 response.
Secondary endpoints included the PRO measures presented in this report.
Deodhar A, et al. ACR/ARHP 2008; Abstract 365.
ACR = American College of RheumatologyDAS = Disease Activity ScorePRO = patient-reported outcome

Study design (cont’d)
Patient-reported outcomes (PROs) included:
• Health Assessment Questionnaire-Disability Index (HAQ-DI) score;
• patient rating of fatigue, assessed using the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-Fatigue);
• health-related QoL, assessed using the Medical Outcomes Study Short Form (36-item) health survey (SF-36).
HQ-DI score was collected at every visit, FACIT-Fatigue at weeks 12, 24, and 48, and SF-36 at weeks 24 and 48.
Minimal clinically important differences (MCIDs) from individual patient baselines were defined as ≥0.22, ≥4, >5.42, and >6.33 for HAQ-DI, FACIT-Fatigue, and physical and mental component scores (PCS and MCS) of the SF-36, respectively.
Deodhar A, et al. ACR/ARHP 2008; Abstract 365. QoL = quality of life

Key findings
Demographic and baseline disease characteristics were generally well balanced across the three arms.
Primary intent-to-treat (ITT) population comprised 509 patients:
• 167 patients receiving 2 x 500 mg rituximab;
• 170 patients receiving 2 x 1000 mg rituximab;
• 172 patients receiving placebo.
Of these patients, 487 completed 24 weeks of treatment and 468 completed 48 weeks.
After week 24, 460 patients (90%) received a second course of treatment, and 451 of them completed 48 weeks of the study.
Deodhar A, et al. ACR/ARHP 2008; Abstract 365.

Key findings (cont’d)
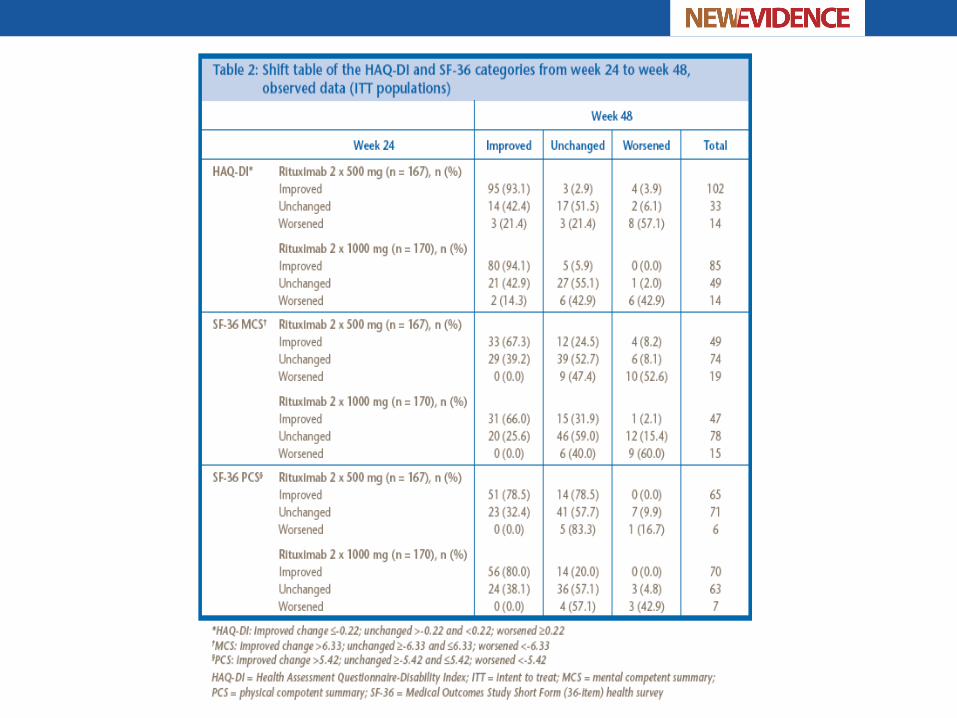
Week 24 results (placebo-controlled period)
Mean decrease from baseline in HAQ-DI was significantly greater (p <0.0001) in both rituximab arms, compared with the placebo arm, resulting in a clinically meaningful improvement in HAQ-DI (≥MCID of 0.22).
A significantly greater mean increase from baseline in SF-36 PCS score was observed in the two rituximab arms compared with the placebo arm.
Mental component scores (MCS) were also improved in both rituximab arms, but achieved statistical significance at the 5% level only with the 2 x 1000 mg dose, compared with the placebo arm.
Significantly greater proportions of patients treated with rituximab plus MTX achieved clinically relevant improvements in SF-36 PCS (>MCID of 5.42) compared with those receiving placebo plus MTX.
A significantly greater proportion of patients treated with rituximab 2 x 1000 mg plus MTX achieved clinically relevant improvements in SF-36 MCS (>MCID of 6.33), compared with those treated with placebo plus MTX.
A significantly greater mean increase from baseline in the FACIT-Fatigue score was observed in the two rituximab arms, compared with the placebo arm.
A significantly greater proportion of patients in the rituximab 2 x 1000 mg arm and the rituximab 2 x 500 mg arm (p <0.01 and p <0.05, respectively) showed a clinically meaningful improvement in the FACIT-Fatigue score (≥MCID of 4.0).
Deodhar A, et al. ACR/ARHP 2008; Abstract 365. MTX = methotrexate


Key findings (cont’d)
Week 48 results
Improvements in HAQ-DI with rituximab plus methotrexate (MTX) was first observed by week 8 of treatment.
MCID improvements for HAQ-DI, SF-36 physical and mental components, and FACIT-Fatigue endpoints were sustained at week 48 with both rituximab arms.
Of the rituximab-treated patients with an MCID improvement in HAQ-DI at week 24, ≥93% had sustained improvement at week 48.
Of the rituximab-treated patients with an MCID improvement in SF-36, >78% and >67% had sustained improvement at week 48 in the PCS and MCS, respectively.
Deodhar A, et al. ACR/ARHP 2008; Abstract 365.
FACIT = Functional Assessment of Chronic Illness TherapyHAQ-DI = Health Assessment Questionnaire-Disability Index MCID = minimal clinically important difference MCS = mental component score; PCS = physical component scoreSF-36 = Medical Outcomes Study Short Form (36-item) health survey

Key conclusions
Rituximab as a first-line biologic therapy in patients with active RA taking a stable dose of methotrexate (MTX) resulted in statistically significant and sustained clinically important improvements for both doses over a 48-week period.
Improvements were seen in physical function, as indicated by the HAQ-DI score, and in the fatigue and health-related QoL parametres assessed by the FACIT-Fatigue and SF-36 physical and mental component summary scores.
Deodhar A, et al. ACR/ARHP 2008; Abstract 365.
FACIT = Functional Assessment of Chronic Illness TherapyHAQ-DI = Health Assessment Questionnaire-Disability Index MTX = methotrexate ; RA = rheumatoid arthritis;SF-36 = Medical Outcomes Study Short Form (36-item) health survey

Prospective follow-up of rituximab treatment in 965 patients with refractory
rheumatoid arthritis (630 patients/year): tolerance and efficacy data from the French Registry AIR (autoimmunity and rituximab)
Gottenberg J-E, et al. ACR/ARHP 2008; Abstract 1190.

Background
ACR/ARHP 2008: Gottenberg and colleagues presented data from the French AIR (Autoimmunity and Rituximab) Registry, the objective of which is to prospectively assess the safety and efficacy of rituximab in off-trial patients with rheumatoid arthritis (RA) and other autoimmune diseases over a period of 5 years.
Gottenberg J-E, et al. ACR/ARHP 2008; Abstract 1190.

Study design
The French Society of Rheumatology has developed an electronic registry named AIR (Autoimmunity and Rituximab), which is available online at www.air-cri.org.
The registry has been collecting data on tolerance and efficacy of rituximab in RA and in other refractory autoimmune diseases (AID) since September 2005.
Gottenberg J-E, et al. ACR/ARHP 2008; Abstract 1190.

Key findingsPatients with RA
Demographical data:
• RA patients (n = 965 ), of whom 78.7% were women and 72.7% were RF-positive;
• mean age was 57.5 years; disease duration was 11.7 years; number of prior disease-modifying anti-rheumatic drugs (DMARDs) was 3.4;
• 21 .8% of patients had not previously received any anti-TNF (tumour necrosis factor) inhibitors; 21.4% had received one anti-TNF; 32.7% had received 2 anti-TNFs; 24.1% had received 3 anti-TNFs;
• 3.3% had received abatacept;
• mean baseline DAS28 was 5.7 ± 1.2;
• 81.3% of patients received prednisone (mean dose: 12.6 ± 10.7 mg/day);
• mean gammaglobulin level, assessed in 56.3% of the patients, was 11.9 ± 8.5 g/l.
Treatment:
• monotherapy with rituximab was prescribed in 31.8% of patients;
• 68.2% of patients received a concomitant immunosuppressant.
Gottenberg J-E, et al. ACR/ARHP 2008; Abstract 1190.

Key findings (cont’d)
Patients with RA (cont’d)
Follow-up:
• 729 patients have already had at least one follow-up visit;
• mean follow-up duration is currently 44.9 weeks (630 patients/year).
Tolerance:
• 157 infusion-reactions;
• three deaths (related to infection in two patients and worsening of a pre-existing lymphoma in one patient) occurred;
• 43 severe infections occurred (6.8 severe infections/100 patients/year, including 19 broncho-pulmonary, 6 osteo-articular, 8 skin/soft tissues, 6 pyelonephritis, 2 digestive, and 2 ENT), mainly (81.3%) within the 6 months following rituximab;
• 5 venous thromboses, 3 pulmonary embolisms, and 10 cancers were observed.
Efficacy:
• EULAR response was observed in 53.5% of 316 patients who already had a 6-month follow-up visit;
• remission was observed in 5% of patients.
Gottenberg J-E, et al. ACR/ARHP 2008; Abstract 1190.
Key findings (cont’d)
Patients with RA (cont’d)
Re-treatment:
• 328 patients (34%) were re-treated after a mean period of 10 months since the last infusion of the first rituximab cycle;
• 76 patients had 3 cycles or more.
Patients with other refractory autoimmune diseases
195 patients (systemic lupus: 41; primary Sjögren’s syndrome: 45; vasculitis: 24; myositis: 21; other: 64) were included in the registry.
5 deaths (worsening of pre-existing cancer: 2; infection: 1; worsening of AID: 2) and 9 severe infections occurred.
Gottenberg J-E, et al. ACR/ARHP 2008; Abstract 1190. AID = autoimmune disease

Key conclusions
Results show good short-term tolerance of rituximab in daily rheumatological practice, comparable to data from clinical trials, which has to be confirmed in the long-term by the ongoing prospective follow-up.
Gottenberg J-E, et al. ACR/ARHP 2008; Abstract 1190.
ACR and DAS28 response over 24 wks inRA patients treated with rituximab after
an inadequate response to one TNF
Haraoui B, et al. ACR/ARHP 2008; Abstract 762.
Background
Despite the use of tumour necrosis factor (TNF) inhibitors and disease-modifying anti-rheumatic drugs (DMARDs), many patients with rheumatoid arthritis (RA) do not respond adequately to treatment.
Rituximab, a monoclonal antibody that selectively targets CD20 B-cells, is currently approved for use in patients who have failed treatment with an anti-TNF agent. A post-hoc analysis of the REFLEX study1 suggested that the efficacy of rituximab is optimized if used after one TNF agent.2
Prospective studies in RA patients that have failed treatment with only one TNF inhibitor are needed to provide additional evidence to guide the optimal use of rituximab in this refractory group of patients.
ACR/ARHP 2008: Haraoui and colleagues presented interim data from a study designed to evaluate the safety of rituximab in combination with methotrexate (MTX) in RA patients who had an inadequate response (IR) or were intolerant to treatment with only one prior anti-TNF inhibitor.3
1. Cohen SB, et al. Arthritis Rheum 2006;54(9):2793–2806. 2. Kremer MJ, et al. Ann Rheum Dis 2006;65(Suppl II):326. 3. Haraoui B, et al. ACR/ARHP 2008; Abstract 762.

Study design
The study was an open-label, multicentre clinical trial conducted in 26 centres in Canada and 9 centres in Sweden.
Results are from a pre-defined interim analysis of 50 patients who had 24 weeks of follow-up.
Patients with an IR to one prior TNF inhibitor received rituximab (1000 mg on days 1 and 15) in accordance with approved labelling.
Primary safety endpoints were evaluated at days 1 and 15 (rituximab infusions) and at 4, 8, 12, and 24 weeks after the initial infusion.
Efficacy was evaluated at 4, 12, 24, 36, and 48 weeks after theinitial infusion.
Intensity of adverse events (AEs) was graded according to the scale detailed in the National Cancer Institute (NCI) Common Terminology Criteria for Adverse Events (CTCAE), version 3.0.
Haraoui B, et al. ACR/ARHP 2008; Abstract 762.IR = inadequate responseTNF = tumour necrosis factor

Study design (cont’d)

Key findings Of the 50 patients, 68% were female with a mean age of 55.6 years and a
mean disease duration of 13.6 years. All patients received 2 infusions on days 1 and 15.
Ninety-two percent of patients had discontinued their previous TNF inhibitor because of inadequate efficacy (25% due to lack of initial response, 64% due to loss of response over time), and 8% because of AEs/tolerability. Thirty-two percent of patients were using concomitant glucocorticoids.
Robust ACR responses were achieved at week 24 by the refractory patient population with long-standing disease.
Improvements in DAS28 were significant (p <0.0001) at week 4 (-1.1 versus baseline) with an absolute decrease of -2.2 at week 24.
Seventy-eight percent of patients achieved a moderate to good DAS response, 20% had low disease activity and 8% were in DAS remission (DAS28 <2.6).
Major improvements (>50%) were observed in all ACR core components with the exception of the Health Assessment Questionnaire (HAQ) score (28%) and the erythrocyte sedimentation rate (ESR) (48%).
Haraoui B, et al. ACR/ARHP 2008; Abstract 762.
ACR = American College of RheumatologyAE = adverse event; DAS = Disease Activity ScoreIR = inadequate response; TNF = tumour necrosis factor

Figure 1. ACR response at week 24

Figure 2. EULAR/DAS response at week 24

Key findings (cont’d)
The mean baseline values versus week 24, respectively, were as follows:
• swollen joint count (SJC): 13.7 versus 6.8;
• tender joint count (TJC): 15.5 versus 6.2;
• patient global: 67.3 versus 36.4;
• physician global: 65.5 6 versus 28.9;
• HAQ: 1.8 versus 1.3;
• C-reactive protein (CRP) (mg/dL): 3.0 versus 1.2;
• ESR (mm/hour): 39.0 versus 20.4.
Improvements were also observed in the level of fatigue as measured by the FACIT-Fatigue score with a decrease of 34% in fatigue by week 24 (baseline of 28.3; week 24: 18.6).
Safety
Only 3 patients (6%) experienced a serious AE. No patients withdrew from the primary treatment period because of an AE.
Forty-four infections were observed in 54% of patients during the 24-week observation period. Only one serious infection (urinary tract) occurred during the 24-week period.
Haraoui B, et al. ACR/ARHP 2008; Abstract 762.
AE = adverse event; ESR = erythrocyte sedimentation rateFACIT = Functional Assessment of Chronic Illness Therapy HAQ = Health Assessment Questionaire

Figure 3. Significant improvements across ACR core set at 6 months (ITT)
Key conclusions
At 24 weeks, a single course of rituximab (2 x 1000 mg) with methotrexate (MTX) provided clinically significant improvements in disease activity in patients with active, long-standing RA who had an inadequate response (IR) to one prior TNF inhibitor.
Improvements were observed in DAS28 and the proportion of ACR responders in this patient population.
Smaller improvements in HAQ are probably due to the irreversible damage seen in this cohort with long-standing disease.
These data confirm early findings that rituximab is an effective treatment option for RA patients.
Haraoui B, et al. ACR/ARHP 2008; Abstract 762.
ACR = American College of RheumatologyDAS = Disease Activity ScoreHAQ = Health Assessment QuestionaireRA = rheumatoid arthritis; TNF = tumour necrosis factor

Efficacy, safety, and dose frequency of retreatment with rituximab in RA: results from
a randomized, controlled trial (SUNRISE)
Mease PJ, et al . ACR/ARHP 2008; Abstract 1212.

Background
Clinical trials using rituximab as selective B-cell–targeted therapy have demonstrated significant efficacy and safety in modifying the signs and symptoms of rheumatoid arthritis (RA).1,2,3
In open-label extension studies, sustained efficacy has been observed over multiple courses of treatment,4 but an optimal re-treatment paradigm has not been established.
ACR/ARHP 2008: Mease and colleagues presented results of the phase III, randomized, placebo-controlled SUNRISE study, designed to assess the efficacy and safety of one versus two courses of rituximab over 48 weeks.5
1. Cohen SB, et al. Arthritis Rheum 2006;54(9):2793–2806. 2. Edwards JC, et al. N Engl J Med 2004;350(25):2572–2581. 3. Emery P, et al. Arthritis Rheum 2006;54(5):1390–1400. 4. Keystone EC, et al. ACR/ARHP 2008; Abstract 367.5. Mease PJ, et al. ACR/ARHP 2008; Abstract 1212.

Study design
The SUNRISE study was a controlled re-treatment study of one versus two courses of rituximab.
Adult patients (n = 550) with active RA on stable methotrexate (MTX) (10–12 mg/week ≥12 weeks) and with a previous inadequate response to ≥1 tumour necrosis factor (TNF) inhibitor were enrolled.
All enrolled patients received one course of open-label rituximab (1000 mg IV on days 1 and 15) at baseline.
From week 24, patients not in DAS28 remission (< 2.6) were randomized in a 2:1 ratio to receive an additional course of re-treatment with rituximab or to receive re-treatment with placebo.
Re-treatment could occur until week 40.
Primary endpoint was ACR20 response in re-treated patients at week 48, relative to baseline.
An intention-to-treat analysis was used for efficacy.
Mease PJ, et al. ACR/ARHP 2008; Abstract 1212.ACR = American College of RheumatologyDAS = Disease Activity Score; RA = rheumatoid arthritis

Study design (cont’d)

Key findings The study enrolled 550 patients, who received the first course of
rituximab at baseline.
At week 24, 42 patients were in DAS remission, and 475 patients were randomized to a second course in two arms:
• re-treatment with rituximab (n = 318);
• re-treatment with placebo (n = 157).
Most randomized patients (n= 426, 90%) were re-treated between weeks 24 and 28.
In both groups at baseline, approximately 80% of patients were female, mean age was 54, disease duration was 11–12 years, baseline DAS28-ESR was 6.7, and HAQ-DI was 1.5.
Relative to baseline, patients re-treated with rituximab had significantly improved efficacy at week 48 compared with those re-treated with placebo, respectively (ACR20: 53.5% versus 44.6%, p = 0.0195; change in DAS28 mean: -1.9 versus -1.5, p= 0.0058).
Mease PJ, et al. ACR/ARHP 2008; Abstract 1212.
ACR = American College of RheumatologyDAS = Disease Activity Score; ESR = erythrocyte sedimentation rateHAQ-DI = Health Assessment Questionnaire-Disability Index

Figure 1. ACR20 response at week 48 (ITT)

Figure 2. Change in DAS28-ESR at week 48 (ITT)

Key findings (cont’d)
Differences in efficacy between groups were first observed following weeks 28 to 32, at which time worsening disease activity was observed in the patients re-treated with placebo. Patients re-treated with rituximab maintained efficacy responses.
Patients with strong initial clinical responses were most likely to benefit from a second course.
Randomized patients who achieved ACR70 following the first course (n = 45) had more than 4-fold greater odds of maintaining response if re-treated with rituximab, compared with placebo (OR: 4.5, p = 0.037).
Following re-treatment, the proportion of patients experiencing any adverse events (AEs) were comparable between the placebo versus rituximab re-treatment groups, respectively: total AEs (76.8% versus 70.6%), serious AEs (7.1% versus 6.9%), infections (38.1% versus 37.5%), and serious infections (1.9% versus 2.2%)
Mease PJ, et al. ACR/ARHP 2008; Abstract 1212.ACR = American College of RheumatologyOR = overall response


Key conclusions
Two courses of rituximab approximately 6 months apart resulted in improved and sustained efficacy at one year, as compared with a single course.
Safety profile with two courses of rituximab was comparable to that of a single course.
Mease PJ, et al. ACR/ARHP 2008; Abstract 1212.