UPDATE ON THE USE OF NEW GENERATION ANTIPSYCHOTICS IN...
28
1 UPDATE ON THE USE OF NEW GENERATION ANTIPSYCHOTICS IN ID/IDD Marco Bertelli, MD, Psychiatrist, MISP Chair WPA-SPID - World Psychiatric Association - Section Intellectual Disability Chair EAMH-ID - European Association on Mental Health in Intellectual Disability Secretary SIDiN - Società Italiana per i Disturbi del Neurosviluppo President Elect AISQuV - Società Italiana per lo studio della Qualità di Vita Scientific Director CREA - Research and Clinical Centre of Fondazione San Sebastiano, Florence (Italy) www.crea-sansebastiano.org office: [email protected] private: [email protected] DRUGS PRESCRIBING IN ID/IDD 1. Deb et al., 1994; Clarke et al., 1990 2. Tyrer et al., 2008; Deb, 2007; Aman et al., 2004; McGillivray et al., 2004; Clarke et al., 1990 3. Spreat et al., 1997 4. Brandford, 1994; Holden, 2004 5. Linaker, 1990 - Around 20-45% of PwID receive psychoactive drugs - 14-30% receive PD for the management of PBs, without an underlying psychiatric diagnosis 1 - high prescription is not supported by evidence on efficacy and safety 2 - Around 2/3 of prescribed drugs are antipsychotics 3 - At least 1 AP is prescribed to 20% of users of supported residential facilities 4 and to 45% of hospitalized persons 5
Transcript of UPDATE ON THE USE OF NEW GENERATION ANTIPSYCHOTICS IN...

1
UPDATE ON THE USE OF NEW GENERATION ANTIPSYCHOTICS IN ID/IDD
Marco Bertelli, MD, Psychiatrist, MISP
Chair WPA-SPID - World Psychiatric Association - Section Intellectual DisabilityChair EAMH-ID - European Association on Mental Health in Intellectual DisabilitySecretary SIDiN - Società Italiana per i Disturbi del NeurosviluppoPresident Elect AISQuV - Società Italiana per lo studio della Qualità di VitaScientific Director CREA - Research and Clinical Centre of Fondazione San Sebastiano, Florence (Italy)
www.crea-sansebastiano.orgoffice: [email protected]: [email protected]
DRUGS PRESCRIBING IN ID/IDD
1. Deb et al., 1994; Clarke et al., 19902. Tyrer et al., 2008; Deb, 2007; Aman et al., 2004; McGillivray et al., 2004; Clarke et al., 19903. Spreat et al., 19974. Brandford, 1994; Holden, 20045. Linaker, 1990
- Around 20-45% of PwID receive psychoactive drugs
- 14-30% receive PD for the management of PBs, without anunderlying psychiatric diagnosis1
- high prescription is not supported by evidence on efficacyand safety2
- Around 2/3 of prescribed drugs are antipsychotics3
- At least 1 AP is prescribed to 20% of users of supportedresidential facilities4 and to 45% of hospitalized persons5

2
� 50% psychiatric disorder� 13% severe problem behavior� 38% combination of PD and PB
REASONS FOR DRUG PRESCRIPTION IN ID/IDD
Tsiouris JA et al. Prevalence of psychotropic drug use in adults with intellectual disability: positive and negative findings from a large study. J Autism Dev Disord, 2012; 25 (Epub ahead of print)
N = 4069 adults
� 58% psychotropics in general� 6% typical antipsychotics� 39% atypical antipsychotics� 23% antidepressants� 19% mood stabilizers� 16% antianxiety agents� 1-2% anti-impulsivity drugs, stimulants and hypnotics
� 27% with diagnosis of psychotic disorder (ICD-10 F20-29)� 27% with diagnosis of affective disorder (ICD-10 F30-39)� 6% with borderline/mild ID, without any psychiatric diagnosis� 21% with severe/profound ID, without any psychiatric diagnosis
� most common indications for prescribing:• comorbid psychotic illness• anxiety• agitation• a range of behavioural disturbances
� the prevalence of use of AP to manage problem behaviour in the absence of concomitant mental illness increased with the severity of ID� almost 50% of prescriptions in those with severe/profound were for PB� adherence to the audit standards related to documentation of clinical indications and review of efficacy was high� side effect monitoring was less assiduous
ANTIPSYCHOTICS PRESCRIBING FOR ID IN PSYCHIATRIC SERVICES
Paton C, Flynn A, Shingleton-Smith A, et al. Nature and quality of antipsychotic prescribing practice in UK psychiatry of intellectual disability services. J Intellect Disabil Res. 2011 Apr 21.
n = 2319(clinical records of 39 mental health services in the UK)

3
ANTIPSYCHOTICS PRESCRIBING IN PEOPLE WITH INTELLECTUAL DISABILITIES
Hannah Griffiths, N. Halder and N. Chauudhry. Antipsychotics prescribing in people with intellectual disabilities: a clinical audit. Advances in Mental Healthand Intellectual Disabilities, 2012; 6(4): 215-222.
� 126 (72%) were prescribed antipsychotic medication� 11 (9%) were prescribed 2 antipsychotic drugs concurrently
- 67% had a co-occurrent psychiatric diagnosis- 33% off-label
first prescriber
� 64% GP on recommendation from secondary care� 28% unknown� 8% GP alone or pharmacy
n = 178(patient attending Salford Intellectual Disability Psychiatric Unit, UK)

4
DEFINITION OF MENTAL DISORDER IN ID
� There is no consensus about which MH problem should be included1
� Diverse conceptualization of both ID and mental health are evident in the research literature1
� Difficulties with the determination of functional impairmentPwID have fewer role expectations and symptoms do not necessarily relate to the degree of impairment in daily life2
� Difficulties with the determination of clinically significant distressPwID are constantly exposed to many stressors and symptoms do not necessarilyrelate to the degree of distress in daily life
1. Holland A, Koot HM. Mental health and intellectual disability: An international perspective. J Intellect Disabil Res 1998; 42:505–512.2. Costello H. and Bouras N. Assessment of mental health problems in people with intellectual disabilies. Isr J Psychiatry Relat Sci Vol 43 No. 4 (2006): 241-251
Costello H. and Bouras N. Assessment of mental health problems in people with intellectual disabilies. Isr J Psychiatry Relat Sci Vol 43 No. 4 (2006): 241-251Mental health and intellectual disabilities addressing the mental health needs of people with id. Report by the Mental Health Special Interest Research Group of the IASSID to the World Health Organisation. Final version – September, 20011. Reiss S, Syszko J. Diagnostic overshadowing and professional experience with mentally retarded persons. Am J Ment Deficiency 1993;87:396–402.
DIFFICULTIES WITH THE DIAGNOSTIC PROCESS IN ID
� What the person says they are experiencing• Difficulties in communication skills or language impairment• Even in verbally competent, auditory hallucination resulted to be the only first-rank
symptom that can be detected
� What other say about them and how they are seen to behave• A confounding factor is the belief that such problems are inevitable and unchangeable.
This means that help is not sought.• ‘Diagnostic overshadowing’ whereby someone’s general mental state or behaviour is
attributed to the fact that he or she has an intellectual disability1
� Hystory of complaint• The development, for example, of maladaptive behaviours, increasing withdrawal, or
changes in a person’s state of general well-being may be a marker for a possible mentalhealth problem (baseline exaggeration).
• Establishing a baseline and recording changes are central to the diagnostic process
� The presentation of symptoms

5
COMPLEXITY OF PHENOMENOLOGY OF PSYCHIATRIC DISORDERS IN ID
� Level of cognitive ('intellectual distorsion'1), communicative, physical and social functioning
� Level of development ('developmentally appropriateness'2)
� Interpersonal, cultural and environmental influences (psychosocial masking3)
� 'ID overshadowing'4
Differentiate between psychiatic symptoms and signs and symptoms of underlying braindamage
� Atypical or masked presentationAggressivity, screaming, maladaptive behaviours, etc.
� Neurovegetative vulnerabilitySomatic complaints, changes in circadian rhythm, NV dystonias
� 'Cognitive disintegration'3
Coping impairment and lower threshold
1. Sovner R, DesNoyers Hurley A. Four factors affecting the diagnosis of psychiatric disorders in mentally retarded persons. Psychiatric Aspects of Mental Retardation Reviews 1986; 5: 45–48.2. Cooper SA., Salvador-Carulla L. (2009) Intellectual Disabilities. in I.M. Salloum and J.E. Mezzich Eds. Psychiatric Diagnosis: Challenges and Prospects. John Wiley & Sons, Ltd3. Sovner R. Limiting factors in the use of DSM-III criteria with mentally ill/ mentally retarded persons. Psychopharmacol Bull 1986; 24:1055–1059.4. Reiss S, Syszko J. Diagnostic overshadowing and professional experience with mentally retarded persons. Am J Ment Deficiency 1993;87:396–402.
• 15-25%1
• 60% at least 1 PB(N=2202)2
HIGH RATE OF PROBLEM BEHAVIOUR IN ID/IDD
1. Emerson, 1998; Keirnan, 1996; Borthwick-Duffy, 1994; Jacobson, 1982; Bertelli, 2003;2. Smith et al, 19963. Cooper et al, 2007;4. Cooper et al, 2009;5. Smith e Matson, 2010
�22.5% (with clinical diagnosis)�18.7% (with DC-LD diagnosis)
(N=1023)3
�aggressivity (9.8%)5
�SIB (4.9%)4
� higher rate when co-occurringASD or epilepsy

6
1. Cooper at al, 2009;2. Totsika et al, 2008
PB IN ID: HIGH PERSISTENCE
2 yrs remission rate 1
SIB 38.2%aggressivity 27.7%
11 yrs permanence rate2
all PB 79%physical aggressivity 70%stereotypies 65%SIB 49%
PROBLEM BEHAVIOURS IN ID
� Persistence levels tended to be high in adults and seem to be stable overtime, especially in individuals with autism1
� The presentation of BPs is determined by a complexity of factors
� The causal value of organic conditions, psychiatric disorders, environmentalinfluences, life-events, operators misinterpretation or a combination of these, has to be carefully established for every single case
� Influence of ID and developmental levels2
� Functional behavioural assessment has gained widespread use in allsettings in which people with ID might present behavioural problems
� Recent research has shown promise in training professionals and non-professionals in learning to carry out such assessments and in implementingeffective behavioural interventions3
M. Bertelli, A. Hassiotis, S. Deb, L. Salvador-Carulla. New Contributions Of Psychiatric Research In The Field Of Intellectual Disability, WPA 20081. Totsika V. and Hastings RP., 2009; 2. Hove O. and Havik OE., 2009; 3. Tassé, 2006

7
S. Deb, L. Salvador-Carulla, J.Barnhill, J. Torr, E. Bradley, H. Kwok, M. Bertelli & N. Bouras. Problem Behaviours in Adults withIntellectual Disabilities: An International Guide for Using Medication. http://www.wpanet.org/uploads/Sections/Psychiatry_Intellectual/WPA-SPID-International-Guide.pdf

8
Deb S., Kwok H., Bertelli M.O. et al. International guide to prescribing psychotropic medication for the management of problem behaviours in adults with intellectual disabilities. World Psychiatry, 2009; 8:181-186
Evidence to support poly prescribing
� There is a lack of studies of combinations of psychotropic medications to manage problem behaviour among adults with ID
� it is not possible to recommend any combination of medications as enhancing the efficacy of medications prescribed on their own
� the evidence based on observational studies suggests that the reduction in poly prescribing not only improves behaviour but also the quality of life of the person for whom medication is prescribed
Problem Behaviour in Adults with Intellectual Disabilities: International Guide for Using Medication, WPA 2008
POLY PRESCRIBING
It is not uncommon for people with intellectual disabilities to take medications for a wide variety of disorders and illnesses. However, the term poly prescribing in this document is used to describe the prescribing of more than one medication for a particular indication, in this case problem behaviour.

9
� some evidence on efficacy of TAPs in reducing aggressive behaviour in PwID
� most studied and prescribed are haloperidol, thioridazine, and chlorpromazine
� many studies pointed out low safety and low tolerability, showing a number of side effects with very high negative impact on PwID (tardivedyskinesia, neuroleptic malignant syndrome, sedation, dystonia, reduction of cognitive performance, extrapyramidal effect)
� use limited to very acute phases and at the minimum effective dose
Santosh & Baird, 1999; La Malfa & Bertelli., 2006; Deb et al., 2007; Deb & Unwin ,2007.La Malfa & Bertelli, 2006. Advokat et al., 2000.
TYPICAL ANTIPSYCHOTICS IN PwID/IDD
Owen R et al. Pediatrics. 2009, Aripiprazole in the treatment of irritability in children and adolescents with autistic disorder.
NGAs IN AUTISM SPECTRUM DISORDERS
RISPERIDONE is approved for the treatment of irritabilityassociated with autistic disorder in children and adolescents(ages 5-16 years ), including symptoms of aggression, self-injury, tantrums, and quickly changing moods. It is the first prescriptionmedication approved by the FDA for this purpose.
ARIPIPRAZOLE is approved for the treatment of irritabilityassociated with autistic disorder in children and adolescents(ages 6-17 years ), including symptoms of aggression, self-injury, tantrums, and quickly changing moods.

10
� less effective than placebo for PBs in PwID1
� same effectiveness than placebo for PBs in PwID2
� much more effective than placebo, across the life span3,4,5
1Tyrer et al., ,2008. 2Brylewski et al., 2007. 3Aman et al., 2002; Snyder et al., 2002; Turgay et al., 2002.4 Buitelaar et al., 2001; Franco et al., 2000; McDonough et al., 2000; Zarcone et al., 2001.5McAdam et al., 2002; Janowsky et al., 2003; Bokszanska et al., 2003. 6La Malfa et al., 2006.
NGAs IN ID/IDD
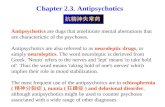
OLANZAPINE VS RISPERIDONE IN TREATING AGGRESSIVE BE HAVIOURS IN ADULTS WITH INTELLECTUAL DISABILITY: A SINGLE BLIND STUDY
Mario Amore1, Marco Bertelli2,3,5, Daniele Villani4, Stefania Tamborini4 and Michele Rossi2,3,5
1. Division of Psychiatry, Department of Neurosciences, University of Parma (Italy)2. AMG Research and Evolution Centre, Florence (Italy)3. Operative Unit of Psychiatry, Department of Neurosciences, University of Florence, Florence (Italy)4. Psychiatric Hospital, “Fondazione Sospiro”, Cremona (Italy)5. MAPPsi, Medics Associated for Psychiatry and Psychotherapy, Florence (Italy)
Journal of Intellectual Disability Research, 2011 Feb;55(2):210-8
aggressività verbale
0
100
200
300
400
-24 -16 -8 0 8 16 24
T vis ita
n° e
piso
di
r isperidone
olanzapina
aggressività verso oggetti
0
50
100
150
200
-24 -16 -8 0 8 16 24T visita
n° e
piso
di
aggressività verso sé stessi
050
100150200
250300
-24 -16 -8 0 8 16 24
T visita
n° e
pis
odi
aggressività verso gli altri
020406080
100120140
-24 -16 -8 0 8 16 24
T visita
n° e
pis
odi

11
� 2 naturalistic studies
� olanzapine more prescribed for psychosis
� risperidone more prescribed for problem behaviours associated with PD
� both resulted to be effective
� results limited by indirect assessment of PBs (through CGI)
Williams et al. 2000; Bokszanska et al. 2003
Bymaster FP, et al. Neuropsychopharmacology. 1996;14(2):87-96. Schotte A, et al. Psychopharmacology (Berl). 1996;124(1-2):57-73.Lawler CP, et al. Neuropsychopharmacology. 1999;20(6):612-627.Corbett R, et al. CNS Drug Reviews. 1997;3(2):120-147.
Aripiprazole
Risperidone
Olanzapine
Quetiapine
Clozapine
Ziprasidone
Haloperidol
D1
D4.2
D2
5-HT2A
5-HT2C
5-HT1A
5-HT6
αααα1αααα2Musc
H1
ANTIPSYCHOTICS RECEPTORS BINDING PROFILE

12

13

14
Janowsky DS et al., 2003; Singh AN et al., 2010; Zuddas et al., 2011
CLOZAPINE
� mostly used for PBs
� some evidence of efficacy in case series
� efficacy on aggressivity, SIB, and disruptive behavior, even at low dose
� rare but relevant side effects (attention to neutropenia and seizures)

15
� most studied among NGA
� more effective than TAPs on problem behaviours with lower extrapyramidal side effects.
� first choice drug for PBs in ID/IDD
� frequent hyperprolactinemia
Connor and Posever,1998. Advokat et al., 2000. La Malfa et al., 2006. Janowsky et al.,2003;
RISPERIDONE

16
Janowsky DS et al., 2003; Singh AN et al., 2010; Zuddas et al., 2011
OLANZAPINE
� mostly used for PBs
� some evidence of efficacy in case series
� good efficacy on disorders different from schizofrenia, particularly mood disorders
� efficacy on aggressivity, SIB, and disruptive behavior
� good tolerability (attention to risk of metabolic disorders)
Owen R et al. Pediatrics. 2009, Aripiprazole in the treatment of irritability in children and adolescents with autistic disorder.
ARIPIPRAZOLE
is approved for the treatment of irritability associated with autistic disorder in children and adolescents (ages 6-17 years), including
� symptoms of aggression,
� self-injury,
� tantrums,
� quickly changing moods

17
Erickson CA et al., 2011; Shastri M. et al., 2006
ARIPIPRAZOLE
prospective open label study, 12 weeks12 young participants (6-25 aa) with FXSdaily mean dose: 9,8 mg
Significative improvement (CGI and ABC)
2 discontinuations:1 for akathisia and tiredness1 for tiredness
4 cases with psychotic disorder1 case with PB and ASDgood efficacy and tolerability
� 15 cases (26-45 yrs; ID from mild to moderate)
� 14 monotherapy; 1 in combination with valproate and
escitalopram
� 11 bipolar disorder; 4 schizophrenia
� 5 drug naive, 10 switched from clozapine, olanzapine,
valproate, clotiapine, delorazepam, clorpromazine,
carbamazepine
� clinical improvement (CGI at 1, 3, 6 months)
� minor side effects i.e (vomit,nausea, headache, sedation)
ASENAPINE

18
Cohen S et al, 2003
ZIPRASIDONE
� prevalent use on PBs
� some evidence of efficacy in case series
� good tolerability (weight neutral)
40 persons with ID and PB, overweight and dyslipidemia (total colesterol, HDL, LDL, TG)
� efficacy on PB
�weight and dyslipidemia improvement
THE CONCEPT OF EFFECTIVENESS OF INTERVENTION
Efficacy Tolerability and Safety
Adeherence/Stay on treatment
Effectiveness
Lieberman JA, et al. N Engl J Med. 2005;353(12):1209-1223; Lehman AF, et al. Am J Psychiatry. 2004;161(2 suppl):1-56; Swartz MS, et al. Schizophr Bull. 2003;29(1):33-43.

19
OUTCOME MEASURES IN PSYCHOPHARMACOTHERAPY OF ASD
Risperidone (1)Meta-analysis was possible for three outcomes. Some evidence of the benefits of risperidone in irritability, repetition and social withdrawal were apparent .
Tryciclic Antidepressants (2)The objectives are to determine if treatment with tricyclic antidepressants:- improves the core features of autism, including restricted social interaction, restrictedcommunication and stereotypical and repetitive behaviours- improves non-core features such as challenging behaviours- improves co-morbid states, such as depression and anxiety- causes adverse effects.
SSRIs (3)The objectives are to determine if treatment with SSRIs: - improves the core features of autism (social interaction, communication and behaviourproblems) - improves non-core aspects of behaviour or function such as self-injurious behaviour- improves the quality of life of children and their carers- has short and long term effects on outcome- causes additional harms.
1. Jesner OS, Aref-Adib M, Coren E. Risperidone for autism spectrum disorder. Cochrane Database of Systematic Reviews 2010, Issue 1.2. Hurwitz R, Blackmore R, Hazell P, et al. Tricyclic antidepressants for autism spectrum disorder (Protocol). Cochrane Database of Systematic Reviews 2010, Issue 2.3. Wheeler DM, Hazell P, Silove N, Williams K. Selective serotonin reuptake inhibitors for the treatment of autism spectrum disorders(Protocol). Cochrane Database of Systematic Reviews 2004, Issue 1
THE CONCEPT OF EFFECTIVENESS OF INTERVENTION
Efficacy Tolerability and Safety
Adeherence/Stay on treatment
Effectiveness
Lieberman JA, et al. N Engl J Med. 2005;353(12):1209-1223; Lehman AF, et al. Am J Psychiatry. 2004;161(2 suppl):1-56; Swartz MS, et al. Schizophr Bull. 2003;29(1):33-43.

20
5.0 µµµµM
Terry AV Jr, et al. Psychopharmacology (Berl). 2002;164(4):360-368
Vehicle OlanzapineHaloperidol
ChAT is an abbreviation for choline acetyltransferase which is a marker for cholinergic neurons that are highly involved in cognitive processes. ChAt is labeled as bright green dots.
EFFECT OF 90 DAY TREATMENT WITH HALOPERIDOL OR OLANZAPINE ON RAT CORTICAL CHAT* LEVELS

21
ASSESSMENT OF METABOLIC SYNDROME IN PEOPLE WITH ID ON ANTIPSYCHOTIC MEDICATION
Hannah Griffiths, N. Halder and N. Chauudhry. Antipsychotics prescribing in people with intellectual disabilities: a clinical audit. Advances in Mental Healthand Intellectual Disabilities, 2012; 6(4): 215-222.

22
MONITORING FOR METABOLIC SYNDROME IN PEOPLE WITH ID ON ANTIPSYCHOTIC MEDICATION
Raghu Baburaj and Mohamed El Tahir. Monitoring for metabolic syndrome in people with intellectual disability on antipsychotic medication. Advances in Mental Health and Intellectual Disabilities, 2011; 5(3): 38-44.
Frighi V, Stephenson MT, Morovat A, Jolley IE, Trivella M, Dudley CA, Anand E, White SJ, Hammond CV, Hockney RA, Barrow B, Shakir R, Goodwin GM. Safety of antipsychotics in people with intellectual disability. Br J Psychiatry. 2011Oct;199(4):289-95
� metabolic indices were the same or more favourable in the ID group than in the general population control group
� overweight/obesity and type 2 diabetes were more prevalent in the women in the ID group than the control group
� a total of 100% and 70% of participants on amisulpride/sulpiride and risperidonerespectively had hyperprolactinaemia, with secondary hypogonadism in 77% and 4% of affectedwomen and men.

23
THE CONCEPT OF EFFECTIVENESS OF INTERVENTION
Efficacy Tolerability and Safety
Adeherence/Stay on treatment
Effectiveness
Lieberman JA, et al. N Engl J Med. 2005;353(12):1209-1223; Lehman AF, et al. Am J Psychiatry. 2004;161(2 suppl):1-56; Swartz MS, et al. Schizophr Bull. 2003;29(1):33-43.
SCHIZOPHRENIC PATIENTS COMPLETINGTHE TREATMENT HAVE A QoL IMPROVEMENT
Zhao F, et al. Schizophr Bull 2005;31(2):508.
45
50
55
60
65
0 4 8 12 16 20 24
Weeks on Antipsychotic Therapy
QLS
Tot
al S
core
(O
C)
Completers
Discontinued
Number of patients at each time point:Completers:
856 851 844 838Discontinued:
961 707 274 83
*
*p<.05

24
T1 T2 T3
Risperidone 2 8,70 6,5 5,5 5,0Clozapine 10 43,48 235,00 220,50 212,50Olanzapine 6 26,09 20,00 19,17 19,17Quetiapine 5 21,74 1140,00 1100,00 1030,00
Haloperidol 11 50,00 44,55 38,18 37,27Clorpromazine 4 18,18 200,00 162,50 137,50Levomepromazine 3 13,64 91,67 91,67 83,33Promazine 2 9,09 210,00 195,00 180,00Perfenazine 2 9,09 16,00 8,00 7,00
COMPOUND N % MEAN DOSAGE (mg/day)
M. Bertelli et al. Antipsychotics drugs for the management of behavioural disorders in pwid: generic quality of life as an outcome measure. Proceedings of the International WPA Congress, Florence 2009
ANTIPSYCHOTIC MEDICATION(% by sample and dosage by time)

25
Temperamento bizzoso
Rumorosità
Distruttività
Iperattività
Mancanza di cooperazione
Comportamento in luoghi pubblici
Comportamento aggressivo
Vagare
Abitudini personali negative
Altri problemi del comportamento
Rompere o gettare oggetti
Gridare o piangere
Wing’s Handicap Behaviours and Skills schedule (HBSs)
L. Wing. The MRC Handicaps, Behaviour & Skills (HBS) schedule. Acta Psychiatrica Scandinavica, 1980, 62; S285: 241-248
Behaviour rated for:
Severity (consequences)
0 = Not at all a problem1 = the behaviour is a problem, but SLIGHT in degree2 = the problem isMODERATELY SERIOUS 3 = the problem is SEVERE in degree
Frequency (n/day)1 = <12 = 1-33 = 3-54 = >5
HBSs SCORES by TIME
M. Bertelli et al. Antipsychotics drugs for the management of behavioural disorders in pwid: generic quality of life as an outcome measure. Proceedings of the International WPA Congress, Florence 2009

26
OVERALL QoL-IP SCORE by TIME
*
* = p<.001
M. Bertelli et al. Antipsychotics drugs for the management of behavioural disorders in pwid: generic quality of life as an outcome measure. Proceedings of the International WPA Congress, Florence 2009
BECOMING SUBAREA SCORES by TIME
PRACTICAL LEISURE-TIME
GROWTH
* = p<.001
* *
*
M. Bertelli et al. Antipsychotics drugs for the management of behavioural disorders in pwid: generic quality of life as an outcome measure. Proceedings of the International WPA Congress, Florence 2009

27
QoL-IP ‘BEING - PSYCHOLOGICAL’ SCORE by TIME
*
* = p<.001 T3 Self-esteem 1,21 (0,58) vs 3,76 (0,48)*
M. Bertelli et al. Antipsychotics drugs for the management of behavioural disorders in pwid: generic quality of life as an outcome measure. Proceedings of the International WPA Congress, Florence 2009
Scientific Director CREA (Research and Clinical Centre) of San Sebastian FoundationVia del Sansovino, 176 - 50142 Firenze (Italy)
www.wpanet.org/spidwww.crea-sansebastiano.org
[email protected]@crea-sansebastiano.org
MARCO O. BERTELLI
MD, Psychiatrist, Psychotherapist

28