Update on Papillary Lesions of the Breast
46
Update on Papillary Lesions of the Breast Victor P. Carlo, MD, FCAP Laboratory Director Anatomic Pathology Hospital Auxilio Mutuo Integrated Pathology, PSC
Transcript of Update on Papillary Lesions of the Breast

Update on Papillary Lesions of
the Breast
Victor P. Carlo, MD, FCAP
Laboratory Director
Anatomic Pathology
Hospital Auxilio Mutuo
Integrated Pathology, PSC

Importance of papillary lesions
• Often challenging histologic
diagnoses
– Benign vs. malignant
– In situ vs invasive
• Management issues
– Papilloma without atypia on core needle
biopsy
– Sentinel node biopsy for papillary
carcinoma
– Staging of encapsulated papillary
carcinoma

Papillary neoplasm:
Definition
• Neoplasms
characterized by
fibrovascular
cores with
surrounding cells
in an arborizing
or wart-like
growth pattern

Main patterns of papillary
neoplasms
• Ovoid well circumscribed mass
• Multiple smaller ducts
• Infiltrative

Ovoid well-
circumscribed
mass
• Papilloma
• Atypical papilloma
• Solid papillary
carcinoma
• Encapsulated
papillary
carcinoma

Multiple smaller ducts
• Papillomatosis
• DCIS, papillary
pattern

Isolated or associated with other
forms of carcinoma
Papillary
neoplasm
DCISINFILTRATING
CARCINOMA

WHO 5th edition
Papillary Tumors of the breast• Intraductal papilloma
– Without atypia
– Atypical papilloma / ADH in papilloma
– Papilloma with ductal carcinoma in situ (within papilloma)
• Ductal carcinoma in situ, papillary pattern
• Encapsulated papillary carcinoma
• Solid papillary carcinoma
– In situ
– With invasion
• Invasive Papillary Carcinoma


Intraductal papilloma (IDP)
• Central and solitary
– Unilateral clear, sometimes bloody
nipple discharge
– Palpable mass
– Any age
– Size: mm to more than 5 cm
• Peripheral papillomas
– Rare, usually incidental

Intraductal papilloma (IDP)
WHO Classification of Breast
Tumors, 5th edition, 2019
• Benign neoplasm within a duct
composed of papillary projections
with fibrovascular cores covered by
an epithelial and myoepithelial layer

Papillomas have variable
morphologic spectrum• Usual ductal hyperplasia
• Apocrine metaplasia
• Sclerosis
• Infarction
• Epithelial cell displacement post core bx
– Stroma
– Vessels
• ADH or DCIS within a papilloma (atypical
papilloma)
• ADH or DCIS in ducts adjacent to
papilloma





Displaced cells

Atypical papilloma has been
variably defined
• Page: Papilloma with a focus of DCIS
measuring less than 3 mm
• Tavasolli:
– Histology consistent with DCIS
involving less than 30% of a papilloma
• Schnitt: qualitative rather than
determined by extent
– Papilloma with DCIS
– Papilloma with ADH

Atypical papilloma vs DCIS in
papilloma
WHO 5th classification
• Atypical papilloma
• ADH in papilloma
• Papilloma with
ADH
– ADH is less than 3
mm in size
– Within the
papilloma
• DCIS in papilloma
– Low nuclear grade
and more than 3
mm
– Intermediate or
high nuclear grade,
any size

Atypical papilloma

Diagnostic criteria
Kraus and Neubecker
Cancer, 1962;15:444-455.
• PAPILOMA
– Epithelial +
myoepithelial
– Normochromatic nuclei
– Complex glandular
pattern
– Often prominent
fibrosis with epithelial
entrapment
– Hyperplasia in adjacent
ducts
– Sclerosing adenosis
sometimes present
• PAPILLARY CA.
– Epithelial only
– Hyperchromatic nuclei
– Cribriform pattern
– Delicate or absent
fibrosis
– ADH, DCIS often
present in adjacent
ducts
– Sclerosing adenosis
usually absent

PAPILLOMA PAPILLARY CARCINOMA

Sources of error
• Heterogenous morphology of
papillomas
• Papillary carcinoma is rare (<1% of
all carcinoma)
• Sampling on core biopsy
• Dimorphic papillary carcinoma
• Misinterpretation of IHC or lack of
correlation with H&E stains

Problems with papillary lesions
on core needle biopsy
• US features of benign and malignant
papillary neoplasms overlap
• Reliability of diagnoses
• Reliability of sampling
– Atypia is unevenly distributed in
papillomas
– Surrounding breast stroma

Dimorphic encapsulated papillary
carcinoma (EPC)

Prospective Excision of Papilloma
without atypia multi-institutional
study (TBCRC 034)
116 papillomas w/o atypia (LOCAL)
31 (27%) NOT confirmed
2 (6%) Atypical papilloma
8 (26%) ADH near IDP
21 (68%) benign mimics of IDP
85 (73%) confirmed
Nakhlis, Ann Surg Oncol. 2021 May;28(5):2573-2578
CENTRAL REVIEW

Should all papillary neoplasms
be excised?
… including benign papillomas
diagnosed on core biopsy?

Reference Sample
size
Papilloma
(%)
Atypia
(%)
Malignant
(%)
Upgrade (%) Recommendatio
n
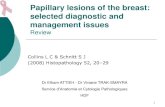
Rozentsvayg 67 81 12 7 19 Excision
Sakr 48 79 6 15 21 Excision
Rizzo 86 75 14 10 25 Excision
Skandarajah 80 68 14 19 33 Excision
Ashkenazi 20 65 20 35 35 Excision
Valdes 36 84 0 14 14 Excision
Liberman 25 80 0 20 20 Excision
Mercado 36 39 22 6 28 Excision
Gendler 13 69 16 16 31 Excision
Puglisi 31 94 0 6 6 Excision
Rosen 14 78 14 7 21 No excision
Ahmadiyeh 29 97 0 3 3 No excision
Renshaw 8 8 0 0 0 No excision
Agoff 11 10 0 0 0 No excision
Plantade 37 86 0 14 14 No excision
Ivan 6 100 0 0 0 No excision
Sydnor 38 97 0 3 3 No excision

Ipsilateral carcinomas and ADH on excision after core biopsy dx of papilloma w/o atypia
Brogi,E, USCAP 2021

Rad path concordant CNB of
papillary lesion without atypia
• American Society of Breast Surgeons-
Guidelines for management of high-risk
lesions
• Decision to excise based on risk,
including such criteria as size,
symptomatology, including palpability and
presence of nipple discharge; and breast
cancer risk factors
• Follow closely with imaging those that are
not excised

Management of atypical papillomas
Atypical papilloma
• Complete excision with
close follow up
Atypical papilloma + DCIS
in surrounding tissue
• Manage according to
findings in adjacent
tissue

Diagnostic criteria
Kraus and Neubecker
Cancer, 1962;15:444-455.
• PAPILOMA
– Epithelial +
myoepithelial
– Normochromatic nuclei
– Complex glandular
pattern
– Often prominent
fibrosis with epithelial
entrapment
– Hyperplasia in adjacent
ducts
– Sclerosing adenosis
sometimes present
• PAPILLARY CA.
– Epithelial only
– Hyperchromatic nuclei
– Cribriform pattern
– Delicate or absent
fibrosis
– ADH, DCIS often
present in adjacent
ducts
– Sclerosing adenosis
usually absent

Myoepithelial cell markers
• SMA
• SMMHC
• Calponin
• P63
• Ck 5/6
• 34BE12
• CD10


Collins LC, Carlo VP, et al. Am J Surg Pathol 2006:30 (8):1002-1007

Immunohistochemistry in papillary
breast lesions
• Myoepithelial cell markers (MEC)
• Lack of MEC at the periphery of
encapsulated papillary carcinoma (EPC)
and solid papillary carcinoma (SPC)
suggests these may represent
circumscribed forms of invasive tumors

Encapsulated Papillary Carcinoma
(EPC) with invasion (NOS)

Solid Papillary Carcinoma with
extracellular mucin secretion

Prognosis of encapsulated
papillary carcinoma
• Data is limited, mostly retrospective
studies
– Reports of lymph node metastasis in
older reports of “intracystic”papillary
carcinoma
– Recent data report excellent prognosis
when EPC occurs as an isolated lesion
• Carter D, et al. Cancer. 1983;52:14–19.
• Lefkowitz M. Hum Pathol. 1994;25:802–809.

Staging of encapsulated papillary
carcinoma (EPC)
WHO
• EPC only: stage as pTis
• EPC + other infiltrating carcinoma
(NOS): stage as per infiltrating
component

Lymph node mets in pure EPC
• Mulligan AM, O’Malley F., Int J Surg Pathol. 2007 • 15(2): 143-147

Rakha EA, Ellis IO, et al.Am J Surg Pathol 2011; 35(8): 1093-1103
IPC (n=207) SPC (n=30)
Age, median 69 76
Size, median (range) cm 1.7 (0.3-9.0) 1.5 (0.3- 3.2 cm)
Grade 1 63 (47%) 12 (40%)
Grade 2 67 (50%) 15 (50%)
Grade 3 3 (3%) 3 (10%)
No DCIS 43 (30%) 9 (33%)
DCIS present 102 (70%) 18 (67%)
LVI absent 165 (98%) 19 (95%)
LVI present 4 (2%) 1 (5%)
Lymph node negative 61 (97%) 15 (88%)
Lymph node metastasis 2 (3%) 2 (12%)
No recurrence 78 (86%) 24 (96%)
Diagnosed as recurrent 6 (6%) 1 (4%)
Recurred during follow up 7 (8%) 0 (0%)

Sentinel node biopsy
in encapsulated papillary
carcinoma and solid papillary
carcinoma
• Limited data available
• Wang, Clin Breast Cancer 2017
Apr;17(2):127
• Risk tolerance?
• Age
• Infiltrating component on core
biopsy?
• Imaging findings

Summary
• Papillary lesions show considerable
morphologic overlap
• MEC markers are very useful in the
differential dx of papillary
neoplasms
• For papilloma without atypia,
pathologic-radiologic
correlation and other clinical
features are crucial for management
– Low risk of DCIS or invasive on excision

Pure EPC:
Diagnostic and Management
Recommendations
• Perform MEC markers on all EPC
• Some may represent true DCIS, manage
accordingly
• Some (about 85%) represent invasive carcinoma,
special type
– Staging with sentinel node may be reasonable
– Exclude associated infiltrative carcinoma,
stage accordingly
– Manage similar to DCIS if node(s) are negative
Summary Cont.

EPC + invasive carcinoma NOS
• Report only the size of the NOS
invasive carcinoma
• Manage accordingly to stage of NOS
component
Summary Cont.