Update on hypertension - diagnosis, monitoring and guideline treatment targets Prof. Richard...
56
Update on hypertension - diagnosis, monitoring and guideline treatment targets Prof. Richard McManus, Birmingham, United Kingdom
-
Upload
norah-briggs -
Category
Documents
-
view
215 -
download
0
Transcript of Update on hypertension - diagnosis, monitoring and guideline treatment targets Prof. Richard...

Update on hypertension - diagnosis, monitoring and guideline treatment targets
Prof. Richard McManus, Birmingham, United Kingdom

Overview Background Routine measurement of blood pressure
(is rubbish) Diagnosis of hypertension - ABPM? Management of hypertension – Home ? Treatment targets – any changes? Conclusions

Stroke Risk increases with age & usual BP
Similarly for Heart Disease
40-49
60-69
Low
Low
Risk
High
High

Bottom line BP vs Risk
10 mmHg
38% stroke risk
18% CHD risk

If you live long enough you get hypertension

The population is ageing
In mid-2008 the median age of the population was 39 years, up from 37 in 1998.

systolic2402302202102001901801701601501401301201101009080
Dotplot of systolic
Each symbol represents up to 12 observations.
Routine measurement is often flawed
Last_practice_systolic20019018017016015014013012011010090
Dotplot of Last_practice_systolic
Each symbol represents up to 4 observations.
Same population with routine and research measurement

Blood Pressure varies through the day and between seasons
Hypertension. 2006;47:155-161

Multiple measurements better estimate mean blood pressure

This variability means that measurement error can drown out the truth

occasion
systolic
654321
146
144
142
140
138
136
134
132
130
Interval Plot of systolic vs occasion95% CI for the Mean
occasions
diastolic
654321
83
82
81
80
79
78
77
Interval Plot of diastolic vs occasions95% CI for the Mean
Even on a single occasion BP drops
Approx 1500 patients
24 practices 6 readings at 1min
intervals 12 mmHg systolic
drop Stable after 5th
reading
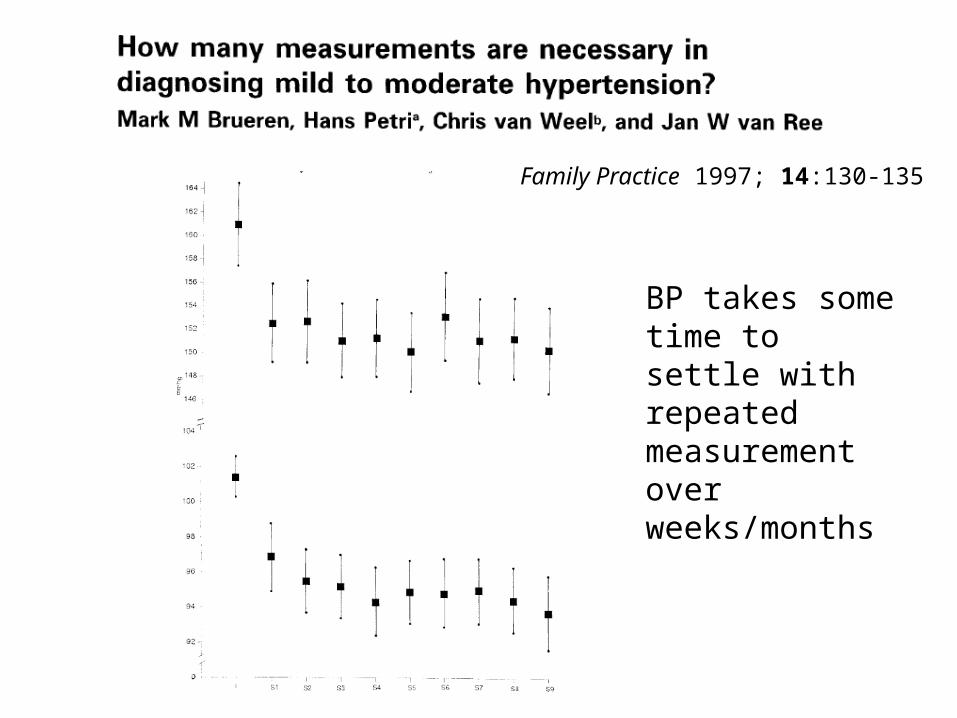
Family Practice 1997; 14:130-135
BP takes some time to settle with repeated measurement over weeks/months

Many factors affect BP measurement
BMJ 2001;322;908-911

Diagnosing hypertension
Traditionally based on clinic measurement Most outcome trials use clinic measures But
– Flawed measure (one off from continuum)– Takes weeks / months to make diagnosis

What about ABPM?Half hourly measurements during the day
Better measure usual BP
Hourly at night Main outcome is mean day time ABPMOther info available (dipping etc)

International Thresholds for hypertension diagnosis (clinic and ABPM)
Mean daytime BP
UK (ABPM) = 135/85 mmHg

What’s normal for ABPM (and home)?
Based on Head et al BMJ 2010
adjust by 5/5 mmHg at lower threshold
(stage 1 hypertension, 140/90 mmHg clinic)
– ie < 135/85 mm Hg
10/5 mmHg at higher threshold
(stage 2 hypertension, 160/100 mmHg clinic)
– Ie < 150/95 mmHg

How do clinic and ABPM compare?
Reviewed literature: 2914 studies of which 20
were relevant 7 compared ABPM with clinic monitoring for
diagnosis Full details:
BMJ 2011;342:d3621 doi: 10.1136/bmj.d3621

Many people currently potentially misdiagnosed...
Worse if only studies around diagnostic threshold used:sensitivity of 86% andspecificity of 46%

What about Home Monitoring?
Relative sensitivity and specificity of clinic and home measurement vs ABPM

Better correlation with end organ damage and outcome (ABPM)
1963 patients
Mean FU 5 yrs
Baseline ABPM
CVD events

1700 patients, 10 years FU, 150 CVAs
Screening = 2 clinic measurements one occasion
Home = 25 measurements over 4 weeks
Journal of Hypertension 2004, 22:1099–1104
Better correlation with end organ damage and outcome (Home)

Detection of white coat and masked HT

But what about costs?
Treatment – ↓drug costs
Follow up – ↓clinician costs
But do additional costs of ABPM out weigh
these?

Is ABPM cost effective?
Modelling to evaluate the most cost-effective
method of confirming a diagnosis of
hypertension in a population suspected of
having hypertension
ABPM vs Home vs clinic
Further details Lovibond et al, Lancet 2011

Markov Model
Health service perspective Lifetime horizon Assume all have raised clinic screening People aged 40 and over

Markov Model
Costs from published sources and NHS Test performance from systematic review Risk calculated using Framingham equation

Results
ABPM most cost effective for every age group

Results
ABPM most cost effective for every age group
Robust to wide range of sensitivity analyses

Results – sensitivity analysis

Results
ABPM most cost effective for every age group
Robust to wide range of sensitivity analyses
Sensitive to
– Assumption of equal test performance
– Assumption of no effect of Rx below
140/90 mmHg

ABPM
Don’t forget ABPM need to be validated and have yearly calibration (bhsoc.org.uk website)
Lack of night time dipping is additional risk (hence rationale for night readings)
Currently limited in PC as most practices either need to refer or only have one ABPM machine
Commissioners need to consider whole health economy

Self Monitoring reduces BP
Bray et al. Annals of Medicine 2010
Small reductions in
blood pressure from
self-monitoring:
– SBP by 3.8 mmHg
– DBP by 1.5 mmHg

Self monitoring costs equivalent to usual care
BMJ 2005;331;493

How many measurements?
Conclusion = at least 4 days monitoring and discard 1st
European (& UK) Guideline is 1 week, 2 readings bd,
discard day 1, take mean (limited rationale)

What is the place of home monitoring?
Management after diagnosis, especially if proven significant white coat effect
More outcome and test performance data needed for diagnosis
Adjunct to other co-interventions and self management...

Co-interventions enhance self monitoring effect
Weighted Mean diff.-30 -15 0 15 30
Study % Weight Weighted Mean diff. (95% CI)
-10.10 (-20.61,0.41) Mehos (2000) 5.4
-9.30 (-11.80,-6.80) Green b (2008) 15.3
-4.40 (-10.52,1.72) Zillich (2005) 9.9
-2.00 (-16.33,12.33) Broege(2001) 3.4
-25.60 (-41.78,-9.42) Artinian (2001) 2.8
-8.50 (-14.16,-2.84) Rudd (2004) 10.5
-3.40 (-5.91,-0.89) Green a (2008) 15.2
-0.20 (-3.84,3.44) Parati (2009) 13.6
-5.00 (-10.45,0.45) Mulhauser (1993) 10.8
-0.90 (-4.98,3.18) Freidman (1996) 12.9
-5.29 (-8.26,-2.32) Overall (95% CI)
5.3 mmHg
2.5 mmHg
Weighted Mean diff.-30 -15 0 15 30
Study % Weight Weighted Mean diff. (95% CI)
-0.14 (-2.05,1.77) Baque (2005) 15.3
5.00 (-6.07,16.07) Bailey (1999) 2.5
0.50 (-3.65,4.65) Verberk (2007) 9.8
-18.00 (-27.13,-8.87) Binstock (1988) 3.5
-2.30 (-5.47,0.87) McManus (2005) 12.1
-4.60 (-9.01,-0.19) Marquez-Contreras (2006) 9.2
-2.60 (-7.26,2.06) Midanik (1991) 8.7
-3.30 (-6.77,0.17) Soghikan (1992) 11.3
-0.50 (-3.07,2.07) Vetter (2000) 13.6
-3.10 (-7.93,1.73) Halme (2005) 8.4
-7.50 (-14.28,-0.72) Carnaham (1975) 5.5
-2.52 (-4.43,-0.61) Overall (95% CI)

What’s a co-intervention?
Nurses
Telemonitoring
Patient Education
Self Management

Theoretical basis for self management
Patients Increased patient involvement in management
decisions will result in:
Cues to action Adherence
Increased self efficacy Behaviour change Better use of medication likely to have most effect
Professionals Systematic titration of medication effective Evidence of clinical inertia


TASMINH2 Research Questions
Does self management with telemonitoring and titration of antihypertensive medication by people with poorly controlled treated hypertension result in:1. Better control of blood pressure?2. Changes in reported adverse events or
health behaviours or costs?3. Is it achievable in routine practice and is it
acceptable to patients?

The Trial Eligibility
– Age 35-85– Treated hypertension (no more than 2 BP meds)– Baseline BP >140/90 mmHg– Willing to self monitor and self titrate medication
Patients individually randomised to self-management vs usual care stratified by practice and minimised on sex, baseline SBP, DM status,
Practice GPs determine management

Intervention Self Monitoring – 1st week of every month

Intervention
Blood Pressure Targets: – NICE (140/90 or 140/80
mmHg)– minus 10/5 mmHg
i.e. 130/85 mmHg or 130/75 mmHg
Patients agreed titration schedule with their GP after randomisation
Traffic Light system to adjust medication

Outcomes
Follow up at 6 & 12 months Main outcome Systolic Blood Pressure Secondary outcomes: Diastolic BP / costs /
anxiety / health behaviours/ patient preferences / systems impact
Recruitment target 480 patients (240 x 2) Sufficient to detect 5mmHg difference
between groups

ResultsInvited (n = 7637)
Declined Invitation (n = 5987)
Assessed for eligibility (n = 1650)
Excluded (n = 1123) Not Eligible (n = 1044) Declined to participate (n=79)
Control (n = 264)Received usual care
(n = 264)
Randomised (n = 527)
Analysed (n = 246)Incomplete cases excluded
(n = 18)
Did not attend follow up (n=14)*
Discontinued usual care (n = 0)
Intervention (n = 263)Received intervention
training (n = 241)
Did not attend follow up (n=26)#
Discontinued intervention (n = 53)
Analysed (n = 234)Incomplete cases excluded
(n = 29)
110% recruitment
91% follow up
80% completed intervention

Baseline Results

Results - primary outcome SBP
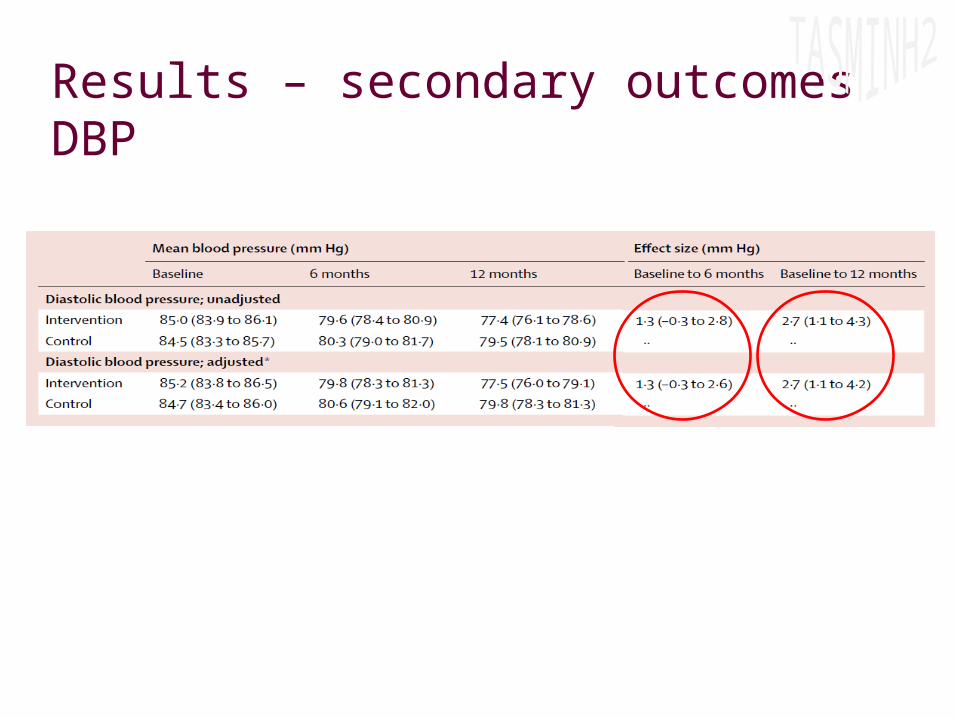
Results – secondary outcomes DBP

Results - subgroups

Results - medications
212 (80%) self managed for full 12 months
148 (70%) made at least one
medication change
At 12m intervention group prescribed
0.46 (0.34, 0.58) additional antiHT (p=0.001)
Main changes seen in thiazides and
calcium channel blockers
(60% on ACEI/ARB at baseline)

Results – side effects
Similar side effects in intervention vs control

Treatment targets Observational data shows that achieved
blood pressure correlates with CVD outcome Wald meta analysis suggests that treatment
effects similar regardless of baseline– But low baseline BP trials almost exclusively
secondary prevention

Treatment targets
Little convincing benefit from lower than 140/90 mmHg target in uncomplicated HT
Evidence for systolic targets sparse Note reduced targets if out of office measure

What about old people?
Meta analysis – 6701 patients; mean FU 3.5 yrs; mean entry SBP 175Target 150 mmHg systolic; Mean reduction SBP around 12mmHgJournal of Hypertension 2010, 28:1366–1372

Bottom Line Consider enhanced use of out of office
measurement, especially for diagnosis Ambulatory monitoring for diagnosis is cost
effective due to better targeting of treatment Home monitoring useful for ongoing management Patients can do it too! 140/90 mmHg best evidence target unless
secondary prevention or over 80