Update on Diagnostic Testing for Tick-borne Diseases · PDF fileUpdate on Diagnostic Testing...
25
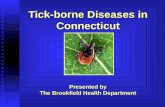
J. Stephen Dumler, M.D. J. Stephen Dumler, M.D. Division of Medical Microbiology Division of Medical Microbiology Department of Pathology Department of Pathology The Johns Hopkins University School of Medicine The Johns Hopkins University School of Medicine Baltimore, Maryland Baltimore, Maryland Update on Diagnostic Update on Diagnostic Testing for Tick Testing for Tick-borne borne Diseases Diseases * * ≥ 147 cases in CT, NY, MA, and RI, 1999 147 cases in CT, NY, MA, and RI, 1999 ** 247 cases in AR, CA, CO, ID, MT, NV, NM, TX, UT, WA, WY, 1990 ** 247 cases in AR, CA, CO, ID, MT, NV, NM, TX, UT, WA, WY, 1990-2000 2000 *** 11,302 cases in Europe, 1999; rare in US ** 11,302 cases in Europe, 1999; rare in US Tick-borne agents of human disease of world-wide importance not reported*** not reported*** not reported** not reported** 95 95 not reported* not reported* 578 578 646 646 1,550 1,550 14,536 14,536 US cases 2005 US cases 2005 relapsing fever relapsing fever Borrelia spp. Borrelia spp. (>10 species) (>10 species) tularemia tularemia Francisella tularensis Francisella tularensis human babesiosis human babesiosis Babesia microti Babesia microti Powassan virus Powassan virus encephalitis (TBE, RSSE) encephalitis (TBE, RSSE) Flavivirus/tick Flavivirus/tick-borne borne encephalitis viruses encephalitis viruses human monocytic human monocytic ehrlichiosis (HME) ehrlichiosis (HME) Ehrlichia chaffeensis Ehrlichia chaffeensis human granulocytic human granulocytic anaplasmosis (HGA) anaplasmosis (HGA) Anaplasma phagocytophilum Anaplasma phagocytophilum Rocky Mountain spotted Rocky Mountain spotted fever fever Rickettsia rickettsii Rickettsia rickettsii Lyme disease Lyme disease Borrelia burgdorferi Borrelia burgdorferi disease disease agent agent Tick-borne infections: a clinical dilemma? blood smear blood smear Fever, malaise, myalgia, arthralgia Fever, malaise, myalgia, arthralgia Babesiosis Babesiosis * IFA * IFA – indirect fluorescent antibody indirect fluorescent antibody ELISA and ELISA and Western blot Western blot serology serology early localized (erythema migrans) early localized (erythema migrans) early disseminated (multiple EM, early disseminated (multiple EM, neuritis, carditis, arthralgis, neuritis, carditis, arthralgis, meningitis meningitis…) Late (arthritis, acrodermatitis, Late (arthritis, acrodermatitis, encephalopathy) encephalopathy) Lyme disease Lyme disease IFA serology IFA serology blood smear blood smear Acute fever, headache; infrequent Acute fever, headache; infrequent rash rash HME and HGA HME and HGA IFA* serology IFA* serology skin biopsy skin biopsy Acute fever, headache (d0 Acute fever, headache (d0-5), rash 5), rash (median d6) (median d6) RMSF RMSF major lab major lab diagnostics diagnostics clinical presentations clinical presentations tick tick-borne borne disease disease
-
Upload
trinhxuyen -
Category
Documents
-
view
221 -
download
5
Transcript of Update on Diagnostic Testing for Tick-borne Diseases · PDF fileUpdate on Diagnostic Testing...

J. Stephen Dumler, M.D.J. Stephen Dumler, M.D.Division of Medical MicrobiologyDivision of Medical Microbiology
Department of PathologyDepartment of PathologyThe Johns Hopkins University School of MedicineThe Johns Hopkins University School of Medicine
Baltimore, MarylandBaltimore, Maryland
Update on Diagnostic Update on Diagnostic Testing for TickTesting for Tick--borne borne
DiseasesDiseases
* * ≥≥ 147 cases in CT, NY, MA, and RI, 1999147 cases in CT, NY, MA, and RI, 1999** 247 cases in AR, CA, CO, ID, MT, NV, NM, TX, UT, WA, WY, 1990** 247 cases in AR, CA, CO, ID, MT, NV, NM, TX, UT, WA, WY, 1990--2000 2000 **** 11,302 cases in Europe, 1999; rare in US** 11,302 cases in Europe, 1999; rare in US
Tick-borne agents of humandisease of world-wide importance
not reported***not reported***
not reported**not reported**
9595
not reported*not reported*
578578
646646
1,5501,550
14,53614,536
US cases 2005US cases 2005
relapsing feverrelapsing feverBorrelia spp. Borrelia spp. (>10 species)(>10 species)
tularemiatularemiaFrancisella tularensisFrancisella tularensis
human babesiosishuman babesiosisBabesia microtiBabesia microti
Powassan virus Powassan virus encephalitis (TBE, RSSE)encephalitis (TBE, RSSE)
Flavivirus/tickFlavivirus/tick--borne borne encephalitis virusesencephalitis viruses
human monocytic human monocytic ehrlichiosis (HME)ehrlichiosis (HME)Ehrlichia chaffeensisEhrlichia chaffeensis
human granulocytic human granulocytic anaplasmosis (HGA) anaplasmosis (HGA) Anaplasma phagocytophilumAnaplasma phagocytophilum
Rocky Mountain spotted Rocky Mountain spotted feverfeverRickettsia rickettsiiRickettsia rickettsii
Lyme diseaseLyme diseaseBorrelia burgdorferiBorrelia burgdorferi
diseasediseaseagentagent
Tick-borne infections:a clinical dilemma?
blood smearblood smearFever, malaise, myalgia, arthralgiaFever, malaise, myalgia, arthralgiaBabesiosisBabesiosis
* IFA * IFA –– indirect fluorescent antibodyindirect fluorescent antibody
ELISA and ELISA and Western blot Western blot serologyserology
early localized (erythema migrans)early localized (erythema migrans)early disseminated (multiple EM, early disseminated (multiple EM, neuritis, carditis, arthralgis, neuritis, carditis, arthralgis, meningitismeningitis……))Late (arthritis, acrodermatitis, Late (arthritis, acrodermatitis, encephalopathy)encephalopathy)
Lyme diseaseLyme disease
IFA serologyIFA serologyblood smearblood smear
Acute fever, headache; infrequent Acute fever, headache; infrequent rashrash
HME and HGAHME and HGA
IFA* serologyIFA* serologyskin biopsyskin biopsy
Acute fever, headache (d0Acute fever, headache (d0--5), rash 5), rash (median d6)(median d6)
RMSFRMSF
major lab major lab diagnosticsdiagnostics
clinical presentationsclinical presentationsticktick--borne borne diseasedisease

0
5
10
15
20
25
30
1920
1925
1930
1935
1940
1945
1950
1955
1960
1965
1970
1975
1980
1985
1990
1995
2000
2005
(thou
sand
s)nu
mbe
r of c
ases
RMSF HME HGALyme disease ehrlichiosis nos total TBD
Cases of tick-borne disease in the U.S.1920-2006
Ticks and tickTicks and tick--borne diseases in the Midborne diseases in the Mid--AtlanticAtlantic
Amblyomma americanumAmblyomma americanum
Ixodes scapularisIxodes scapularis
Dermacentor variabilisDermacentor variabilis
Ixodes scapularisIxodes scapularis
Tick vectorTick vector
Lone star tickLone star tickHMEHME
Deer tick, blackDeer tick, black--legged ticklegged tickHGAHGA
American dog tickAmerican dog tickRMSFRMSF
Deer tick, blackDeer tick, black--legged ticklegged tickLyme diseaseLyme disease
Common tick nameCommon tick nameDiseaseDisease
Lyme disease – caused by members of theBorrelia burgdorferi sensu lato group
general characteristicsgeneral characteristicsspiralspiral--shaped bacterium, 0.2 x shaped bacterium, 0.2 x 10 10 -- 30 um in size30 um in sizetypical cell wall with thin typical cell wall with thin peptidoglycan layerpeptidoglycan layerflagella in periplasmic space > flagella in periplasmic space > twisting motilitytwisting motilityobligate parasite found in obligate parasite found in association with mammals, association with mammals, birds, ticksbirds, ticks

Lyme diseaseBorrelia burgdorferi sensu lato group
ecological characteristicsecological characteristicsmaintained in a small maintained in a small mammal mammal -- IxodesIxodes species species tick cycletick cycleeastern U.S. eastern U.S. -- Peromyscus Peromyscus leucopusleucopus and and I. scapularisI. scapulariswestern U.S. ? reservoir, western U.S. ? reservoir, I. I. pacificuspacificusEurope and Asia Europe and Asia -- small small mammals, mammals, I. ricinus I. ricinus andand I. I. persulcatuspersulcatus
Lyme disease Lyme disease -- seasonalityseasonality
bimodal distributionbimodal distributionmost cases occur in most cases occur in May through JulyMay through Julyassociated with emergence associated with emergence and activity of nymphal deer and activity of nymphal deer ticksticks
secondary peak in secondary peak in late Falllate Fallassociated with emergence associated with emergence and activity of adult deer ticksand activity of adult deer ticks
adults
nymphs
adultslarvae
Number of Cases of Lyme disease, by yearUnited States, 1983-2006
0
5000
10000
15000
20000
25000
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
num
ber o
f cas
es

6Georgia10District of Columbia15South Carolina39Rhode Island47Florida49North Carolina54Vermont61West Virginia
247Maine265New Hampshire274Virginia400New York City646Delaware
1,2351,235MarylandMaryland1,810Connecticut2,336Massachusetts3,363New Jersey4,287Pennsylvania5,165New York (Upstate)
23,305United StatesLyme diseaseArea
Reported cases of Lyme disease by Division of Geographic region, 2005
Adult Ixodes scapularis and Borrelia burgdorferiin the Mid-Atlantic States, 1997-98JE Bunnell, PhD dissertation thesis, JHU School of Hygiene & Public Health
Number of ticks examined 649
Number of B. burgdorferi-infected ticks 151 (23%)
Northern Virginia - 0%
Pennsylvania - 14%
New Jersey - 19%Delaware - 19%
Maryland - 27%
Central Maryland - 33%
North Maryland - 23%
Southern Maryland - 11%
Eastern Shore Maryland - 48%

COUNTY population 2000 cases 2000-2006 00-06 avg incid/105
Queen Anne's County 40,563 284 100.0Kent County 19,197 113 84.1Talbot County 33,812 155 65.5Carroll County 150,897 628 59.5Cecil County 85,951 351 58.3Calvert County 74,563 292 55.9Caroline County 29,772 115 55.2Frederick County 195,277 501 36.7Harford County 218,590 557 36.4How ard County 247,842 570 32.9Somerset County 24,747 52 30.0Worcester County 46,543 73 22.4Washington County 131,923 204 22.1Charles County 120,546 162 19.2Anne Arundel County 489,656 652 19.0Wicomico County 84,644 106 17.9St. Mary's County 86,211 83 13.8Dorchester County 30,674 27 12.6Montgomery County 873,341 605 9.9Prince George's County 801,515 381 6.8Allegany County 74,930 13 2.5Baltimore County 754,292 108 2.0Garrett County 29,846 4 1.9Baltimore city 651,154 61 1.3Maryland 5,296,486 6099 16.5
Lyme disease in Maryland 2000-2066, cases and incidence (2000 census) by county or subdivision
020406080
100
Per
cent
age
of
ticks
infe
cted
Central West TotalBaltimore County region
Percentage of I. scapularis ticks infected withB. burgdorferi in regions of Baltimore County, 2001
NymphFemaleMaleTotal
Courtesy Doug Norris, PhD; JHU Bloomberg School of Public Health
Lyme disease Lyme disease –– early disseminatedearly disseminated
Systemic manifestationsSystemic manifestationsfeverfevermultiple EMsmultiple EMsperipheral nervous systemperipheral nervous system
radiculopathyradiculopathycranial neuropathycranial neuropathymononeuropathymononeuropathy multiplexmultiplex
central nervous systemcentral nervous systemlymphocytic meningitislymphocytic meningitisrarely, encephalomyelitis rarely, encephalomyelitis (parenchymal inflammation of (parenchymal inflammation of brain and/or spinal cord, with brain and/or spinal cord, with focal abnormalities)focal abnormalities)
atrioventricularatrioventricular heart block heart block ±±clinical clinical myopericarditismyopericarditis

Lyme diseaseLyme diseaseclinical aspectsclinical aspectslate infectionlate infection
RheumatologicRheumatologicmonomono-- or oligoarticular arthritisor oligoarticular arthritis
knee, large joints, TMJknee, large joints, TMJsynovial fluid mean 24,250 WBC/mmsynovial fluid mean 24,250 WBC/mm33
neutrophil predominanceneutrophil predominanceantibioticantibiotic--refractory chronic arthritisrefractory chronic arthritis
HLAHLA--DR4DR4
Central nervous systemCentral nervous systemunifocalunifocal or or multifocalmultifocal encephalomyelitisencephalomyelitis
very rare in U.S.; CSF pleocytosisvery rare in U.S.; CSF pleocytosisperipheral neuropathyperipheral neuropathy
““stocking glovestocking glove”” paresthesiasparesthesias; ; radicularradicular painpainencephalopathyencephalopathy
mild memory and cognitive function mild memory and cognitive function abnormalities abnormalities
Lyme diseaseLyme diseasediagnosisdiagnosis
cultureculturePCRPCRserologyserology-- enzyme immunoassayenzyme immunoassay-- western blotwestern blot
Cultivation yield (%) of Borrelia burgdorferi from clinical samples
>40% (≥9 mL)Blood (plasma)AnecdotalSynovial fluidNo data availableCerebrospinal fluid>50% (max 86%)Erythema migrans

NonNon--chronicchronic
Sensitivity and specificity metaSensitivity and specificity meta--analyses of published assays for the Lyme disease analyses of published assays for the Lyme disease diagnosis by PCR.diagnosis by PCR.
66--76%76%21%21%17%17%
100%100%66--91%91%24%24%19%19%OverallOverallCSFCSF
99%99%2323--100%100%65%65%73%73%Synovial fluidSynovial fluid
100%100%00--52%52%29%29%26%26%Plasma / serumPlasma / serum
100%100%5959--80%80%71%71%67%67%Erythema migransErythema migrans
MetaMeta--Analysis Analysis SpecificitySpecificity
Range of Range of sensitivitysensitivity
MedianMedianSensitivitySensitivity
MetaMeta--Analysis Analysis SensitivitySensitivity
Specimen typeSpecimen type
Laboratory Diagnosis of Lyme diseaseLaboratory Diagnosis of Lyme diseaseSerologySerologyEnzyme immunoassay (EIA) methodsEnzyme immunoassay (EIA) methods
very sensitive, limited specificity (false positives)very sensitive, limited specificity (false positives)whole bacterial cell lysates or individual recombinant whole bacterial cell lysates or individual recombinant
proteinsproteinsgenerally not immunoglobulin class specificgenerally not immunoglobulin class specific
Western blot assays to aid specificity Western blot assays to aid specificity supplemental method for EIA positivessupplemental method for EIA positivesrequires presence of specific antigen bands onrequires presence of specific antigen bands on
IgM or IgG immunoblotsIgM or IgG immunoblots
Pitfalls in serologic diagnosisPitfalls in serologic diagnosislack of early responselack of early responseabrogation by early Rxabrogation by early Rxpersistent antibody in absence of active diseasepersistent antibody in absence of active diseaselack of standardizationlack of standardizationno FDAno FDA--cleared test for detection of CSF antibodiescleared test for detection of CSF antibodies
Serology in Lyme disease; % reactivity in patients with:
ArthritisNeurological involvement
EM, convalescent
phase
EM,acute phaseTest
978729-7829-40Two-tier testing
96-10064-7215-21, 800-13, 43.6IgG IB
168075-8443-44IgM IB
100 (IgG ELISA)79 (IgG ELISA)76-8633-49Whole-cell ELISA

FlgBFlgB
OspCOspC
OspAOspAOspBOspB
BmpABmpA
IgGIgG
(5 of 10)(5 of 10)
18182121--24 OspC24 OspC2828303039 (39 (BmpABmpA))41 (41 (FlaFla))454558 (not GroEL)58 (not GroEL)66669393
IgMIgM
(2 of 3)(2 of 3)
2121--24 OspC24 OspC39 (39 (BmpABmpA))41 (FlgB)41 (FlgB)
IgM
IgG
EM < 7 days EM ≥ 7 days

Recommendations for Two-Step Testing and Interpretation of Lyme borreliosis Serology
later samplecan't exclude LD alonerepeat in 2 - 4 weeksif strongly suspected
early samplecan't exclude LD alonerepeat in 2 - 4 weeks
negative result
no reliable evidence of infectioncan't exclude LD alonerepeat in 2 - 4 weeks
if LD strongly suspected
negative result
serologic evidence of infectionmay not be current infectionsupports clinical diagnosis
positive result
supplemental testimmunoblot (Western blot)
positive or equivocal result
Clinical diagnosis of Lyme diseaseInitial testELISA, EIA, IFA
Appropriate use of ELISA test for Appropriate use of ELISA test for Lyme disease diagnosisLyme disease diagnosis((TugwellTugwell et al Ann Intern Med 1997)et al Ann Intern Med 1997)
Pretest probabilityPretest probabilityincidence of disease in communityincidence of disease in communityconstellation of clinical findingsconstellation of clinical findings
ELISA (and IFA) accurate if:ELISA (and IFA) accurate if:standardizedstandardizedappropriate cutoffsappropriate cutoffsappropriate quality controlappropriate quality control
Only to be used if pretest probability exceeds 0.20 but is Only to be used if pretest probability exceeds 0.20 but is less than 0.80less than 0.80Arthralgia, myalgia, headache, fatigue, palpitations alone Arthralgia, myalgia, headache, fatigue, palpitations alone not sufficient to raise pretest probability to clinically usefulnot sufficient to raise pretest probability to clinically usefulrangerange
Review of laboratory predictive value and likelihood ratios
Sensitivity = test + / true +Sensitivity = test + / true +Specificity = test Specificity = test -- / true / true ––Positive predictive value =Positive predictive value =
true + / (true +) + (false +)true + / (true +) + (false +)
Therefore, a test with sensitivity and specificity of Therefore, a test with sensitivity and specificity of 95% used to test 1000 persons in which prevalence 95% used to test 1000 persons in which prevalence of disease is 1% would identify 60 positives, 10 true of disease is 1% would identify 60 positives, 10 true positives and 50 false positives.positives and 50 false positives.
Positive likelihood ratio (LHR) = true + rate / false + Positive likelihood ratio (LHR) = true + rate / false + raterate((used in calculation of post test odds or post test used in calculation of post test odds or post test probabilityprobability))Pretest odds x LHR = post test oddsPretest odds x LHR = post test odds


Selected recombinant and peptide antigens used for detection of Selected recombinant and peptide antigens used for detection of IgM, IgG, or IgM, IgG, or polyvalent antibodies to polyvalent antibodies to B. burgdorferiB. burgdorferi
1545-68FlgA (37 kDa)
83-986470-90Convalescent
94-10060-9545-74Acute
Invariable region 6 (IR-6, C6 peptide)
879739100100736344-6319-40VlsE
35-5243-53P41 internal fragment
95340-53pepC10
35-4341-73OspC
IgIgGIgMIgIgGIgMIgIgGIgM
LateLateNeurologicalNeurologicalEMEMRange % positive in the indicated LB disease stage Range % positive in the indicated LB disease stage
Recombinant antigen or peptide
CSF serology in Lyme disease
ELISA indicated only with prior ELISA indicated only with prior positive serum ELISApositive serum ELISANo FDANo FDA--approved test or cutoff approved test or cutoff criteriacriteriaNeed to implicate intrathecal antibody Need to implicate intrathecal antibody synthesis (IgG index)synthesis (IgG index)
Predictive value of PCR forB. burgdorferi in skin
0
0.2
0.4
0.6
0.8
1
0.80
00
0.50
00
0.20
00
0.10
00
0.01
00
0.00
10
0.00
01
pretest probability (prevalence)
prob
abili
ty o
f tru
e te
st
overall PPVoverall NPV

PCR on CSF for
B. burgdorferi
Predictive value of B. burgdorferiPCR on plasma
0
0.2
0.4
0.6
0.8
1
0.80
00
0.50
00
0.20
00
0.10
00
0.01
00
0.00
10
0.00
01
pretest probability (prevalence)
prob
abilit
y of
a tr
ue te
st
overall NPVoverall PPV

Other tests for Lyme diseaseOther tests for Lyme diseaseDetection of Detection of B. burgdorferiB. burgdorferi antigen in urineantigen in urine
Alternative lab testing atAlternative lab testing at““Lyme literateLyme literate”” facilitiesfacilities
TP = true Positive; TN = true Negative; FP = false Positive; FN = false Negative
35 (TN)LDA, PCR, and RWB Negative
6 (TP) PCR only Positive
94 (TN)LDA, PCR, and RWB Negative
4 (TP)LDA, PCR, and RWB Positive
0RWP Positive2 (TP)LDA and RWB Positive
0PCR Positive4 (TP)LDA and PCR Positive
1 (FP)LDA Positive 4 (FP)LDA only Positive
General Population (n=95) Patients with Lyme Disease Like Symptoms (n=55)
• Fatigue• Low grade fevers, ‘hot flashes’ or chills• Night sweats• Sore throat• Swollen glands• Stiff neck• Migrating arthralgias, stiffness and, less
commonly, frank arthritis• Myalgia• Chest pain and palpitations• Abdominal pain, nausea• Diarrhea• Sleep disturbance• Poor concentration and memory loss
• Irritability and mood swings• Depression• Back pain• Blurred vision and eye pain• Jaw pain• Testicular/pelvic pain• Tinnitus• Vertigo• Cranial nerve disturbance (facial
numbness, pain, tingling,palsy or optic neuritis)• Headaches• ‘Lightheadedness’• Dizziness
9. Symptoms of Lyme diseaseFrom International Lyme and Associated Disease Society: Evidence-based guidelines for the management of Lyme disease. 2004. Expert Rev Anti-Infect Ther 2: S1-S13

“Lyme literate” lab 1SpecificitySpecificityAny sample positive by LDA, and confirmed by either PCR or RWB oAny sample positive by LDA, and confirmed by either PCR or RWB or r both, was considered a true positive. Any sample that was negatiboth, was considered a true positive. Any sample that was negative by ve by all 3 methods was considered a all 3 methods was considered a ““true negative.true negative.”” Of the 162 individuals Of the 162 individuals samples, 146 were considered true negatives.samples, 146 were considered true negatives.
141 individuals were negative by LDA. 4 patients suspected of Ly141 individuals were negative by LDA. 4 patients suspected of Lyme me Disease and 1 normal control were positive by LDA, but negative Disease and 1 normal control were positive by LDA, but negative by by either PCR or RWB. Therefore, these were considered false positieither PCR or RWB. Therefore, these were considered false positives. ves. Based on this data, the Based on this data, the specificity of LDA is >96%.specificity of LDA is >96%.
SensitivitySensitivityOf the 16 true positives, 10 samples were positive by LDA. BasedOf the 16 true positives, 10 samples were positive by LDA. Based on on the limited data, the limited data, the sensitivity of the LDA is approximately 60%.the sensitivity of the LDA is approximately 60%.The number of The number of ““true positives" increased from 10 to 16 (88%) when true positives" increased from 10 to 16 (88%) when PCR was performed. PCR was performed.
Note that LDA and other unproven lab tests are part of Note that LDA and other unproven lab tests are part of the definition of the definition of ““true positivetrue positive”” and and ““true negativetrue negative””
Sensitivity and specificity of LDA based on alternate gold standards
True positive = clinical diagnosis onlyTrue positive = clinical diagnosis onlySensitivity 25% (14/55)Sensitivity 25% (14/55)Specificity 99% (106/107)Specificity 99% (106/107)
True positive = clinical diagnosis + PCRTrue positive = clinical diagnosis + PCRSensitivity 50% (6/12)Sensitivity 50% (6/12)Specificity 95% (143/150)Specificity 95% (143/150)
True positive = clinical diagnosis + RWBTrue positive = clinical diagnosis + RWBSensitivity 100% (6/6)Sensitivity 100% (6/6)Specificity 95% (148/156)Specificity 95% (148/156)
Other tests for Lyme diseaseT-cell proliferative assay
Suggested for partiallySuggested for partially--treated or seronegative treated or seronegative personspersonsLT positive in 75% of normal, healthy subjectsLT positive in 75% of normal, healthy subjectsAssay not amenable to clinical laboratoryAssay not amenable to clinical laboratory

Prophylaxis after tick bites in Lyme disease
NadelmanNadelman et al. (NEJM 2001):et al. (NEJM 2001):prophylaxis with single 200 mg dose prophylaxis with single 200 mg dose doxycycline prevents Lyme disease after doxycycline prevents Lyme disease after Ixodes scapularisIxodes scapularis bites in 87%bites in 87%adverse reactions occur 3X more often than adverse reactions occur 3X more often than placebosplacebos
Lyme diseaseLyme diseasetreatment and outcome
antibiotic therapyantibiotic therapylocalized infection: localized infection: popo amoxicillin, doxycyclineamoxicillin, doxycyclinedisseminated infection without neurologic or cardiac disseminated infection without neurologic or cardiac involvement: involvement: popo amoxicillin, doxycycline, amoxicillin, doxycycline, cefuroximecefuroximedisseminated neurologic or cardiac infection: IV ceftriaxonedisseminated neurologic or cardiac infection: IV ceftriaxone
vaccine (adults 85% effective)vaccine (adults 85% effective)Withdrawn from market by SKBWithdrawn from market by SKB
chronic Lyme diseasechronic Lyme diseasemisdiagnosesmisdiagnosestrue persistence of infectiontrue persistence of infection
Health-related quality of life is not affected by prolonged antibiotic treatment in patients with persistent manifestations of Lyme disease
antibioticantibiotic: IV ceftriaxone: IV ceftriaxone 2 g daily x 30 days, and PO 2 g daily x 30 days, and PO doxycycline, 200 mgdoxycycline, 200 mg daily for 60 days;daily for 60 days;
placeboplacebo: matching intravenous and oral placebos: matching intravenous and oral placebos
Klempner MS, et al. Two controlled trials of antibiotic treatment in patients with persistent symptoms and a history of Lyme disease. N Engl J Med. 2001; 345:85-92.

Cases and incidence of TBRD in the U.S.,1920-20062006 data extrapolated from MMWR August 5, 2006
0
500
1000
1500
2000
2500
3000
3500
4000
1920
1925
1930
1935
1940
1945
1950
1955
1960
1965
1970
1975
1980
1985
1990
1995
2000
2005
num
ber o
f cas
es
RMSF HME HGA ehrlichiosis nos total TBRD
1 10 100
1000
1000
0
1000
00
no. cases* TBRDx4 = estimated true cases of TBRD
SARSHantavirus Pulmonary Syndrome
Hemolytic Uremic Syndrome (E. coli O157:H7)Toxic Shock SyndromeMeningococcal disease
LegionellosisInvasive pneumococcal disease
Arbovirus and West Nile VirusTBRD
Hepatitis A/B/CTuberculosis
TBRDx4*AIDS
Comparison of reported life-threateningdomestic infectious diseases in the U.S., 2005
(MMWR 2006; 54:1320)

Rocky Mountain spotted fever (RMSF)Tick vectors of R. rickettsii
• Known tick vectors– Dermacentor variabilis -
American dog tick (eastern U.S.)
– Dermacentor andersoni -Wood tick (western U.S.)
• Possible tick vectors• Rhipicephalus sanguineus
- brown dog tick• Amblyomma cajennense
(Central and South America)
DermacentorDermacentor variabilisvariabilis
DermacentorDermacentorandersoniandersoni
Rhipicephalus sanguineusRhipicephalus sanguineus
Amblyomma cajennenseAmblyomma cajennense
Pathogenesis of Rickettsial infectionsPathogenesis of Rickettsial infections
Rickettsiaendothelial cells
phagsome escape
macrophages and neutrophilsEhrlichia and Anaplasma
phagolysosome fusioninhibition
Clinical manifestations of RMSF
fever, headache, myalgias, fever, headache, myalgias, rashrashrash rash -- macular, macular, maculopapular, petechialmaculopapular, petechialshock and multishock and multi--organ failureorgan failuregastrointestinal systemgastrointestinal systemrenal systemrenal system
acute tubular necrosis 2acute tubular necrosis 2°° to to hypotensionhypotension
cardiopulmonary systemcardiopulmonary systemnonnon--cardiogenic pulmonary cardiogenic pulmonary edemaedema
central nervous system central nervous system ––meningoencephalitismeningoencephalitis
cerebral edema, herniationcerebral edema, herniation
macularmacular maculopapularmaculopapular
petechialpetechial
ecchymosisecchymosis

Lymphocyticvasculitis
Lymphocyticvasculitis
immunohistochemistryimmunohistochemistry
InterstitialpneumonitisInterstitial
pneumonitis meningoencephalitismeningoencephalitis
Leukocytoclastic vasculitisLeukocytoclastic vasculitis
Rocky Mountain spotted feverdiagnosis and risk
risk of death 5 x in patients after day 5 of risk of death 5 x in patients after day 5 of illnessillnessmost patients are initially examined before most patients are initially examined before day 5, but not treated until after day 5day 5, but not treated until after day 5major factors for ineffective diagnosis and major factors for ineffective diagnosis and delayed therapy:delayed therapy:-- absence of typical rashabsence of typical rash-- presentation during nonpresentation during non--peak tick activity seasonpeak tick activity season-- presentation during first 3 days of illnesspresentation during first 3 days of illness
1414Opening pressure Opening pressure ≥≥ 250 mm H250 mm H22OO
44443535Protein Protein ≥≥ 50 mg/50 mg/dLdL
141488Glucose Glucose ≤≤ 50 mg/50 mg/dLdL
rarerare606067673333
484846465050
PleocytosisPleocytosismononuclear cell predominancemononuclear cell predominanceneutrophil predominanceneutrophil predominance
Cerebrospinal fluidCerebrospinal fluid
717176766262ALT or AST ALT or AST ≥≥ 2X normal2X normal
5656Serum sodium < 132 Serum sodium < 132 mEqmEq/L/L
717172725252< 150,000< 150,000
Platelet count/Platelet count/μμLL
76766969> 10% bands> 10% bands
49496666<5,000/<5,000/μμLL
11112828> 10,000/> 10,000/μμLL
White blood cell countWhite blood cell count
HGAHGAHMEHMERMSFRMSFLaboratory findingLaboratory finding
(%)(%)Laboratory abnormalities in TBRDLaboratory abnormalities in TBRD

* IFA = indirect fluorescent antibody; LA = latex agglutination94 – 100%79 –94%LA100%83 – 85%IFA IgM99 – 100%89 – 100%IFA IgGRMSFSpecificitySensitivitySerological assay*Disease
Sensitivity and specificity of serological tests for confirmatioSensitivity and specificity of serological tests for confirmation of RMSFn of RMSF
Laboratory diagnosis in TBRD
CultureCultureIHCIHCPCRPCRBlood Blood smearsmear
SerologySerology≥≥ 14 days14 days
CultureCultureIHCIHCPCRPCRBlood Blood smearsmear
SerologySerology< 14 days< 14 days
Lab testLab test
++++±±++++++HGAHGA
++++++++++++HMEHME
++++++++++++++RMSFRMSF
Lab test Lab test availabilityavailability
convalescentconvalescentacuteacutePhase of illnessPhase of illness
Laboratory diagnosis in TBRD
CultureCultureIHCIHCPCRPCRBlood Blood smearsmear
SerologySerology≥≥ 14 days14 days
CultureCultureIHCIHCPCRPCRBlood Blood smearsmear
SerologySerology< 14 days< 14 days
Lab testLab test
++++±±++++++HGAHGA
++++++++++++HMEHME
++++++++++++++RMSFRMSF
±±±±++Lab test Lab test availabilityavailability
convalescentconvalescentacuteacutePhase of illnessPhase of illness

Laboratory diagnosis in TBRD
CultureCultureIHCIHCPCRPCRBlood Blood smearsmear
SerologySerology≥≥ 14 days14 days
CultureCultureIHCIHCPCRPCRBlood Blood smearsmear
SerologySerology< 14 days< 14 days
Lab testLab test
++++±±++++++HGAHGA
++++++++++++HMEHME
++++++++++++++RMSFRMSF
±±±±++++++++++++++++Lab test Lab test availabilityavailability
convalescentconvalescentacuteacutePhase of illnessPhase of illness
Laboratory diagnosis in TBRD
CultureCultureIHCIHCPCRPCRBlood Blood smearsmear
SerologySerology≥≥ 14 days14 days
CultureCultureIHCIHCPCRPCRBlood Blood smearsmear
SerologySerology< 14 days< 14 days
Lab testLab test
++++±±++++++++++++HGAHGA
++++++++++++++++HMEHME
++++++++++++++00±±RMSFRMSF
±±±±++++++++++++++++Lab test Lab test availabilityavailability
convalescentconvalescentacuteacutePhase of illnessPhase of illness
Laboratory diagnosis in TBRD
CultureCultureIHCIHCPCRPCRBlood Blood smearsmear
SerologySerology≥≥ 14 days14 days
Lab testLab test
00
00
00
±±
000000++++++++HGAHGA
000000++++++++HMEHME
000000++++++++RMSFRMSF
±±++++++++++++++++Lab test Lab test availabilityavailability
convalescentconvalescentacuteacutePhase of illnessPhase of illness

Rocky Mountain spotted feverRocky Mountain spotted fevertreatmenttreatment
adults: doxycycline, tetracyclineadults: doxycycline, tetracyclinechildren: doxycycline, tetracycline, children: doxycycline, tetracycline, chloramphenicol, rifampin?chloramphenicol, rifampin?chloramphenicol associated with excess chloramphenicol associated with excess mortality as compared with doxycycline or mortality as compared with doxycycline or tetracycline when controlled for all other tetracycline when controlled for all other factorsfactors
Human Human AnaplasmataceaeAnaplasmataceae infectionsinfections(human ehrlichiosis)(human ehrlichiosis)
human monocytic ehrlichiosis (HME) human monocytic ehrlichiosis (HME) --Ehrlichia chaffeensisEhrlichia chaffeensisHuman granulocytic anaplasmosis Human granulocytic anaplasmosis (HGA) (HGA) -- Anaplasma phagocytophilumAnaplasma phagocytophilumehrlichiosis ehrlichiosis ““EwingiiEwingii”” -- caused by caused by E. E. ewingiiewingii, genetically like , genetically like E. chaffeensisE. chaffeensis, , phenotypically like human anaplasmosisphenotypically like human anaplasmosisHME and human anaplasmosis are HME and human anaplasmosis are undifferentiated febrile illnesses with undifferentiated febrile illnesses with typical laboratory findings.typical laboratory findings.
E. chaffeensisE. chaffeensis
A. phagocytophilumA. phagocytophilum
E. ewingiiE. ewingii
0
200
400
600
800
1000
1200
1400
1600
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1999
2000
2001
2002
2003
2004
2005
2006
** no data available for 1998
num
ber o
f cas
es
HME
HGA
not specifiedall ehrlichiosis
Cases of ehrlichiosis and anaplasmosis in the U.S. Cases of ehrlichiosis and anaplasmosis in the U.S. reported to the CDC, 1986 reported to the CDC, 1986 -- 20062006

HME HME -- Ehrlichia chaffeensisEhrlichia chaffeensisepidemiology and ecologyepidemiology and ecology
•• risk for disease increased with risk for disease increased with age, male sexage, male sex
•• south central and southeastern south central and southeastern US; WorldUS; World--wide?wide?
•• transmitted by transmitted by A. americanum A. americanum active in summer monthsactive in summer months
•• reservoir whitereservoir white--tailed deertailed deer
HGA HGA –– Anaplasma phagocytophilumAnaplasma phagocytophilumepidemiology and ecologyepidemiology and ecology
•• risk for disease increased with age, risk for disease increased with age, male sexmale sex
•• upper Midwest and northeast US, upper Midwest and northeast US, northern California, Europenorthern California, Europe
•• transmitted by transmitted by Ixodes Ixodes sppspp. . nymphs nymphs and adultsand adults
•• reservoir whitereservoir white--footed mice footed mice ((PeromyscusPeromyscus leucopusleucopus), deer), deer
Amblyomma americanumAmblyomma americanum Ixodes scapularisIxodes scapularis Ixodes ricinusIxodes ricinus
1414Opening pressure Opening pressure ≥≥ 250 mm H250 mm H22OO
44443535Protein Protein ≥≥ 50 mg/50 mg/dLdL
141488Glucose Glucose ≤≤ 50 mg/50 mg/dLdL
rarerare606067673333
484846465050
PleocytosisPleocytosismononuclear cell predominancemononuclear cell predominanceneutrophil predominanceneutrophil predominance
Cerebrospinal fluidCerebrospinal fluid
717176766262ALT or AST ALT or AST ≥≥ twice normal valuetwice normal value
5656Serum sodium < 132 Serum sodium < 132 mEqmEq/L/L
717172725252< 150,000< 150,000
Platelet count/Platelet count/μμLL
76766969> 10% bands> 10% bands
49496666<5,000/<5,000/μμLL
11112828> 10,000/> 10,000/μμLL
White blood cell countWhite blood cell count
HGAHGAHMEHMERMSFRMSFLaboratory findingLaboratory finding
(%)(%)Laboratory abnormalities in TBRDLaboratory abnormalities in TBRD
HME and HGA clinical and epidemiologic HME and HGA clinical and epidemiologic featuresfeatures
HMEHMEInterval to medical Interval to medical attention attention –– 4 days4 daysIncubation period:Incubation period: 10.6 d 10.6 d mean (9 d median )mean (9 d median )
range: 0 range: 0 -- 34 days34 days
Tick exposure Tick exposure –– 80%80%SeveritySeverity
40 to 62% hospitalized40 to 62% hospitalizedMedian length of illness Median length of illness –– 23 23 daysdaysCase fatality rate Case fatality rate –– 2.7%2.7%
HGAHGA•• Interval to medical attention Interval to medical attention
–– 4 to 8 days4 to 8 days•• Incubation period Incubation period –– median median
6 to 10 d6 to 10 d–– range 1 to 60 daysrange 1 to 60 days
•• Tick exposure Tick exposure –– 75 to 85%75 to 85%•• SeveritySeverity
–– 56% hospitalized56% hospitalized–– 7% require ICU admission7% require ICU admission–– Median hospitalization Median hospitalization –– 6 6
daysdays–– Case fatality rate Case fatality rate –– 0.5 to 1%0.5 to 1%

HME and HGA HME and HGA -- diagnosisdiagnosis
blood smear (acute phase only)blood smear (acute phase only)HME HME –– 2% sensitive2% sensitiveHGA HGA –– 25 to 75% sensitive25 to 75% sensitive
PCR on blood (acute phase only)PCR on blood (acute phase only)Sensitivity ~50Sensitivity ~50--60% during acute phase60% during acute phaseno chronic phase in humans, brief persistence no chronic phase in humans, brief persistence of DNA after therapyof DNA after therapy
SerologySerology (paired acute and convalescent)(paired acute and convalescent)IFA IFA -- preferredpreferredWestern blot Western blot –– rarely usedrarely usedRecombinant protein EIA Recombinant protein EIA –– no proven benefitno proven benefit
Ehrlichioses and Anaplasmosis:Ehrlichioses and Anaplasmosis: ComplicationsComplications
++++myocarditis or heart failuremyocarditis or heart failure
0.5%0.5%3%3%deathdeath
++
++++++
++++
++++
++
++++++
++++
HMEHME
++++opportunistic infectionsopportunistic infections
++meningoencephalitismeningoencephalitis
++++++increased severity with preincreased severity with pre--existing diseaseexisting disease
--fulminant infections in immunocompromisedfulminant infections in immunocompromised
++++Toxic or septic shockToxic or septic shock--like syndromelike syndrome
++++peripheral neuropathiesperipheral neuropathies
++pneumonia/ARDSpneumonia/ARDS
HGAHGAClinical complicationClinical complication
Results of diagnostic laboratory testing for HGA and outcome of tests of 144 patients with HGA in the upper Midwest and from lower New York State
A. phago.
A. phago.

Acute 1 6 12 18 24 30 36 42
Months
0
200
400
600
800
1000
1200
1400
1600
1800
GM
T
Early treatment
No treatment
Effect of therapy and kinetics of serologic reactions in HGAEffect of therapy and kinetics of serologic reactions in HGA
Sensitivity and specificity of serological tests for
confirmation of HME and HGA.
8383--100%100%2727--37%37%IFA IgMIFA IgM
8282--100%100%8282--100%100%IFA IgGIFA IgG
HGAHGA
Not determinedNot determined86%86%IFA IgMIFA IgM
Not determinedNot determined88%88%IFA IgGIFA IgG
HMEHME
SpecificitySpecificitySensitivitySensitivitySerological AssaySerological AssayDiseaseDisease
HME and HGA HME and HGA -- therapytherapyDoxycyclineDoxycycline
200 mg 200 mg popo twice daily for 3twice daily for 3--5 days after afebrile5 days after afebrileempirical clinical efficacyempirical clinical efficacygood in vitro activitygood in vitro activity
Rifampin for pregnancy and children?Rifampin for pregnancy and children?scant empirical efficacy datascant empirical efficacy datagood in vitro activitygood in vitro activityPotentially useful in children, pregnancyPotentially useful in children, pregnancy
Fluoroquinolones?Fluoroquinolones?Potentially active against Potentially active against A. phagocytophilumA. phagocytophilum(HGA), but apparently non bactericidal(HGA), but apparently non bactericidalNot active against Not active against E. chaffeensisE. chaffeensis (HME)(HME)
gyrAgyrA QRDR serine 83 (susceptible) QRDR serine 83 (susceptible) →→ alanine (resistant)alanine (resistant)

Prevention of Lyme disease, RMSF, HME, and HGA Prevention of Lyme disease, RMSF, HME, and HGA in humansin humansprompt tick removalprompt tick removaltransmission of transmission of A. phagocytophilumA. phagocytophilum may require as little as 4hmay require as little as 4h
No vaccine currently available for humans
Prophylaxis for HME and HGA after tick bite not investigated
Thanks forlistening.
Questions?
Thanks forlistening.
Questions?
Human monocytic and granulocytic ehrlichiosisHuman monocytic and granulocytic ehrlichiosiswhen and what to testwhen and what to test……
Fever, headache, history of tickFever, headache, history of tick--bite or bite or ––exposure during atexposure during at--risk risk seasonseason
leukopenia, thrombocytopenia, leukopenia, thrombocytopenia, elevated elevated LFTsLFTs
acute phase EDTAacute phase EDTA-- or citrateor citrate--anticoagulated bloodanticoagulated blood
obtain blood prior to or at the obtain blood prior to or at the time of first therapytime of first therapy
do not withdo not with--hold therapy until hold therapy until laboratorylaboratory--confirmedconfirmed
E. chaffeensisE. chaffeensis
A. phagocytophilumA. phagocytophilum
E. ewingiiE. ewingii