Update on clinical diabetes in older veterans Kristina Utzschneider, MD Assistant Professor of...
53
Update on clinical diabetes in older veterans Kristina Utzschneider, MD Assistant Professor of Medicine VA Puget Sound Health Care System and the University of Washington February 25, 2008
-
date post
20-Dec-2015 -
Category
Documents
-
view
214 -
download
2
Transcript of Update on clinical diabetes in older veterans Kristina Utzschneider, MD Assistant Professor of...

Update on clinical diabetes in older veterans
Kristina Utzschneider, MDAssistant Professor of Medicine
VA Puget Sound Health Care System and the University of Washington
February 25, 2008

Disclosure statement
I have nothing to disclose

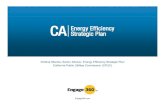
An epidemic on the way
NHANES 1999-2002 2011 20212031
20-29 40-49 60-69 ≥70
Age (years)50-5930-39
Prevalencediabetes(percent)
0
5
10
15
20
25
30
Mainous et al, Diabetologia 50:934, 2007

The burden of diabetes in the VA health care system
Prevalence of diabetes in the VA system:
16% VA vs. 7.2% US general population
6.8 million veterans were enrolled to receive VA care in 2002
4.5 million enrolled veterans made 46.5 million outpatient visits
564,700 veterans were hospitalized in VA medical centers in 2002
Diabetes was the third most common VA diagnosis
Diabetes accounted for 25% pharmacy costs and >1.7 million hospital bed days
Reiber et al, Diabetes Care 27: B3, 2004

Complications of diabetes
Increased mortality
Microvascular complications
Retinopathy
Nephropathy
Neuropathy
Macrovascular complications
Cardiovascular disease

Diabetic complications: burden of illness Approximately 12 million adults age ≥40 years have
diabetes in the United States32.7% have symptoms of diabetic peripheral neuropathy
27.4% have diabetic retinopathy
13.1% have comorbid neuropathy and retinopathyCandrilli et al, Journal of Diabetes and its Complication 21:306-314, 2007
In 2005 485,012 people in the United States had end stage renal disease (ESRD)
Over 30% ESRD due to diabetes:Type 1: 27,714 patients
Type 2: 150,875 patientsU.S. Renal Data System, USRDS 2007 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2007.

Can we prevent diabetes?

Diabetes Prevention Program (DPP)
ScreenScreen
RandomizeRandomize
Standard lifestyle teachingStandard lifestyle teaching
Intensive Intensive LifestyleLifestyle(n = 1079)(n = 1079)
MetforminMetformin(n = 1073)(n = 1073)
PlaceboPlacebo(n = 1082)(n = 1082)
TroglitazoneTroglitazonen= 585n= 585Until 6/98Until 6/98
Diabetes Prevention Program Research Group, Diabetes Care 22:623-34, 1999

DPP: Average weight changeDPP: Average weight change
0 6 12 18 24 30 36 42 48Months in study
Lifestyle
Metformin
+
-8-7-6-5-4-3-2-101
Wei
ght c
hang
e (K
g)
Diabetes Prevention Program Research Group, NEJM 346:393-403, 2002
Placebo

0 1 2 3 4
0
10
20
30
40
Placebo (n=1082)
Metformin (n=1073, p<0.001 vs. Plac)
Lifestyle (n=1079, p<0.001 vs. Met , p<0.001 vs. Plac )
Percent of subjects developing diabetesPercent of subjects developing diabetes
Years in study
Cum
ulat
ive
inci
denc
e (%
)
Lifestyle
Metformin
Placebo
Diabetes Prevention Program Research Group, NEJM 346:393-403, 2002

Diabetes incidence rates by age
0
3
6
9
12
15
25-44(n=1000)
45-59(n=1586)
>60(n=648)
Cas
es/1
00 p
erso
n-yr
Lifestyle Metformin Placebo
Diabetes Prevention Program Research Group, NEJM 346:393-403, 2002

Can we prevent diabetes complications?

Glycemic Control in the UKPDS
Patients followed for 10 years
IntensiveConventional
All patients assigned to regimen
IntensiveConventional
9
Median
HbA1c (%)
Time from Randomization (y)
0
7
8
6
0 3 6 9 12 15
UKPDS Group. Lancet: 352:837-853; 1998
ADA Goal

Effect of Glycemic Control in the UKPDS
* Combined microvascular and macrovascular events
Endpoints
Intensive (rate/1000
pt yrs
Conventional (rate/1000
pt yrs)
% Decrease p value
Any diabetes related * 40.9 46 11 0.029
Microvascular 8.6 11.4 25 0.0099
Myocardial Infarction 14.7 17.4 16 0.052
Stroke 5.6 5.0 - 0.52
PVD 1.1 1.6 - 0.15
UKPDS Group: Lancet 352:837–853; 1998

%Decrease in
Relative Risk **
Any diabetes-related endpoint
21%
**
Diabetes-related death
21% **
All cause
mortality
14%*
Stroke
12%
**
Peripheral vascular disease†
43%
**
Myocardial infarction
14%
**
Micro-vascular disease
37%
**
Cataract extraction
19%
†Lower extremity amputation or fatal peripheral vascular disease*p = 0.035; **p < 0.0001
Effect of 1% Decrease in A1c on Diabetes-relatedComplications - UKPDS Observational Analysis
UKPDS Group - UKPDS 35: Br Med J 321:405-412; 2000

DCCT – glycemic control
Diabetes Control and Complications Trial Research Group, NEJM 329:977-986, 1993.
Total 1441 patients with IDDM enrolledMean 6.5 years follow-up
0 1 2 3 4 5 6 7 8 9 10
Year of Study
Glycosylated hemoglobin (%)
5
6
7
8
9
10
11
Conventional
Intensive

DCCT – retinopathy
Diabetes Control and Complications Trial Research Group, NEJM 329:977-986, 1993.
Primary prevention Secondary prevention

DCCT: retinopathy progression by HbA1c and years of follow-up
0 1 2 3 4 5 6 7 8 9 Time during study (years)
Rate/100person-years
0
16
12
8
4
20
24
Diabetes Control and Complications Trial Research Group, Diabetes 44: 968-983, 1995.
7%
8%
9%10%
Conventional treatment
Mean HbA1c = 11%

DCCT: Results summary
Improved glycemic control reduced the risk of clinically meaningful:
Relative risk reduction
Retinopathy 76% p≤0.002
Nephropathy 54% p<0.04
Neuropathy 60% p≤0.002
Cardiovascular events 78% p=0.065
Diabetes Control and Complications Trial Research Group, NEJM 329:977-986, 1993.Diabetes Control and Complications Trial Research Group, Am J Cardiol 70:894-900, 1995.

DCCT/EDIC
DCCT Intervention Training
Study year
5
6
7
8
9
11
10
Gly
cosy
late
d he
mog
lobi
n (%
)
Conventional
Intensive
1 2 3 4 50 7 26 8 9
EDIC observation
3 4 5 6 71
DCCT/EDIC Study Research Group: N Engl J Med 353:2643–2653; 2005

Prior intensive glycemic control decreases subsequent CVD events in type 1 diabetes
DCCT/EDIC Study Research Group: N Engl J Med 353:2643–2653; 2005
RRR = 42% (95% CI 9-63); p=0.02Cumulativeincidence
of any predefinedCV outcome
0 2 4 6 8 10 12 14 16 18 20
0.10
0.08
0.06
0.04
0.02
0.00
0.12
CV Outcomes:Nonfatal MI, CVD death, subclinical MI, angina confirmed by ETT or angiography, revascularization with angioplasty or CABG
Conventional Rx: 98 events in 52 patientsIntensive Rx: 46 events in 31 patients
Years

Is lower better? the ACCORD Study
10,251 patients with type 2 diabetes and at high risk for CVD were randomized to:
Intensive glucose control arm: A1c <6%Standard glucose control arm: A1c 7-7.9%
Treatment algorithms included all types of oral and injectable medications
Half were then further randomized to the lipid trial and the other half to the blood pressure trial
THE TRIAL WAS STOPPED EARLY DUE TO EXCESS MORTALITY IN THE INTENSIVE GLUCOSE CONTROL ARM
257 deaths intensive arm vs. 203 deaths in the control armThe reason for the increase in mortality is not clear

Steno 2: Effect of a multifactorial intervention
on mortality in type 2 diabetes
Gaede et al: N Engl J Med 358:580-591, 2008
160 subjects stratified by urine albumin
then randomized
80 intensive therapy 80 conventional therapy
67 completed intervention 63 completed intervention
12 died 7 CVD1 withdrew
15 died 7 CVD2 withdrew
12 died 2 CVD 10 other
25 died 12 CVD 13 other
55 completed follow-up study 38 completed follow-up study

Steno 2: Intensive treatment reduced mortality and CV events
Gaede et al: N Engl J Med 358:580-591, 2008

Current standards of medical care
(ADA guidelines)Glycemic controlA1c <7.0% (primary target)
Pre-prandial glucose 90-130 mg/dl
Peak post-prandial glucose <180 mg/dl
LipidsLDL <100 mg/dl
HDL >40 mg/dl
Triglycerides <150 mg/dl
Blood pressure <130/80mm Hg
Aspirin therapy
Smoking cessation
American Diabetes Association: Diabetes Care 30:S4-S41, 2007

Geriatric guidelines for diabetes
American Geriatrics Society (AGS)A1c <7% in healthy adults
Target A1c <8% in older adults with life expectancy <5 years
BP goal <140/80 mm Hg
Screen for comorbid conditions:
depression
polypharmacy
urinary incontinence
falls
pain
cognitive impairment
Brown et al, J Am Geriat Soc 51:S265-S280, 2003

Nathan et al, Diabetes Care 31:173-175, 2008
Treatment of type 2 diabetes: ADA consensus algorithm

Current treatment optionsOral agents:
MetforminSulfonylureas: 2nd generation: glipizide, glyburide 3rd generation: glimepirideMeglitinides: repaglinide, nateglinideThiazolidinediones: pioglitazone, rosiglitazoneAlpha glucosidase inhibitors: acarboseDipeptidyl peptidase 4 (DPP-4) inhibitors: sitagliptin
Injected medications:Insulin
long acting: NPH, ultralente, detemir, glargineshort acting: Regular, aspart, lispro, glulisine
GLP-1 analogues: exenatideAmylin analogues: pramlintide
*Medications in white available at the VA (some are non-formulary)

Expected decrease A1c
Advantages Disadvantages
lifestyle 1-2% Low cost, many benefits Fails for most in first year
metformin 1-2% Low cost, weight neutral GI side-effects, rare lactic acidosis
sulfonylureas 1-2% Low cost Weight gain, hypoglycemia
thiazolidinediones 0.5-1.4% Pioglitazone: improved lipid profile
Fluid retention, CHF, weight gain,
osteoporosis, ? Increased risk MI?,
expensive
insulin 1.5-3.5% Low cost, no dose limit Weight gain, injections, monitoring
Nathan et al, Diabetes Care 31:173-175, 2008
Comparison diabetes medications

Medical treatment in the elderly;
things to keep in mindSulfonylureas more frequent severe hypoglycemia in the elderlyrenal impairment can increase half-life of glyburide
Metforminincreased risk lactic acidosis if renal impairment – especially if >80 years old (check estimated GFR), CHF, hepatic impairment
TZDsincreased risk of fractures (elderly already at high risk)
co-morbid illness: CHF/CAD
Insulin risk hypoglycemia
visual acuity

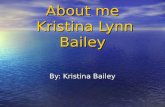
Rosiglitazone: rates of MI and CVD Death
Study Rosiglitazone Control Odds Ratio (95% CI) p value
# of events / Total # (%)
Myocardial Infarction
All small trials 44/10280 (0.43) 22/6105 (0.36) 1.45 (0.88-2.39) 0.15
DREAM 15/2635 (0.57) 9/2634 (0.34) 1.65 (0.74-3.68) 0.22
ADOPT 27/1456 (1.85) 41/2895 (1.44) 1.33 (0.80-2.21) 0.27
Overall 1.43 (1.03-1.98) 0.03
Death from CVD Causes
All small trials 25/6557 (0.38) 7/3700 (0.19) 2.40 (1.17-4.91) 0.02
DREAM 12/2365 (0.51) 10/2634 (0.38) 1.20 (0.52-2.78) 0.67
ADOPT 1/1456 (0.14) 5/2854 (0.18) 0.80 (0.17-3.86) 0.78
Overall 1.64 (0.98-2.74) 0.06
Nissen SE and Wolski K: N Engl J Med 356:2457-2471; 2007

Limitations of meta-analyses
• Validity is dependent upon the quality of the systematic review and the quality of trials included in the review
• Different estimates of treatment effect (data and outcomes)
• Meta-analysis is not the most rigorous way to reach definite conclusions about adverse events
• Meta-analyses are designed to generate hypotheses and do not provide definitive answers

RECORD: adjudicated primary events
0 12 24 36 48 600
4
8
12
16
Numbers at riskRosiglitazonePlacebo
22272220
20872080
19801958
18781856
16941692
445444
Rosiglitazone(217 events)
HR=1.08 (95% CI 0.89-1.31)p=0.43
CumulativeIncidence
(%)
Time from Randomization (months)
Control(202 events)
Primary OutcomeHospitalization andDeath from CVD
Home P et al: N Engl J Med 357:28-38; 2007

Pioglitazone: Rates of CVD Events
Lincoff AM et al: JAMA 298:1180-1188; 2007
Pioglitazone(n=8,554)
n (%)
Control(n=7,836)
n (%)
Hazard Ratio(95% CI)
p value
Death/MI/stroke 375 (4.38) 450 (5.74) 0.82 (0.72-0.94) 0.005
Death 209 (2.44) 224 (2.86) 0.92 (0.76-1.11) 0.38
MI 131 (1.53) 159 (2.03) 0.81 (0.64-1.02) 0.08
Death/MI 309 (3.61) 357 (4.56) 0.85 (0.73-0.99) 0.04
Stroke 104 (1.22) 131 (1.67) 0.80 (0.62-1.04) 0.09
Serious heart failure 200 (2.34) 139 (1.77) 1.41 (1.14-1.76) 0.002
Death/serious heart failure 361 (4.22) 321 (4.10) 1.11 (0.96-1.29) 0.17
Death/MI/stroke/serious heart failure 508 (5.94) 523 (6.67) 0.96 (0.85-1.09) 0.54

Increased fractures with rosiglitazone in women
Time (years)
Cumulative Incidence of First Fracture (%)
0 1 2 3 4 50
5
10
15
20
Rosiglitazone
GlyburideMetformin
0 1 2 3 4 50
5
10
15
20
Rosiglitazone
GlyburideMetformin
Time (years)
Men Women
Kahn et al, Diabetes Care, published online Feb 5, 2008

Fractures with pioglitazone
Takeda Healthcare Provider Letter - March 2007
• Pioglitazone (n >8100) and comparator (n >7400), with a maximum duration of follow up of 3.5 years
• <12,000 patient years of exposure in each group
• No increased risk of fractures in men
• More fractures in women taking pioglitazone (1.9 / 100 patient years) than comparator (1.1 / 100 patient years)
• The majority of fractures in women taking pioglitazone were in the distal upper limb (forearm, hand and wrist) or distal lower limb (foot, ankle, fibula and tibia)

Who should use insulin?
Type 1 diabetes-Basal and prandial insulin
Type 2 diabetes patients not well controlled on oral agents or those who cannot tolerate or have contraindications to oral agents-Add basal insulin (hs NPH or glargine) to achieve fasting glucose < 130 mg/dl
-Add prandial insulin if A1c does not reach goal

Insulin analogues
Action times for insulin
Insulin Starts Peaks Ends Low most likely at
aspart/lispro 10-20 min 1.5-2.5 hr 4-5 hr 2-5 hr
regular 30-45 min 2-4 hr 5-7 hr 3-7 hr
NPH 1-3 hr 4-9 hr 14-20 hr 4-16 hr
lente 2-4 hr 8-14 hr 16-24 hr 6-16 hr
ultralente 2-4 hr 8-14 hr 18-24 hr 8-18 hr
glargine 1-2 hr 6 hr 18-26 hr 5-10 hr
detemir 1-3 hr 8-10 hr 18-24 hr 8-16 hr

Treatment of type 2 diabetes:
ADA consensus algorithm1. Initiate lifestyle intervention and metformin at time of
diagnosis
2. Optimize glycemic control – within or as close to non-diabetic range as possible
3. Monitor A1c at regular intervals and add medications and transition to new regimen if not meeting goals
4. Early addition of insulin in patients not meeting target A1c goals
Nathan et al, Diabetes Care 31:173-175, 2008

Adding basal insulin: glargine vs. NPH
-110 type 2 DM patients, A1c >8% on oral meds-90% were on a sulfonylurea plus metformin-Randomized to receive:
bedtime glargine + metformin (G+MET)bedtime NPH + metformin (NPH+MET)
-Starting dose:10 units if metformin alone20 units if had been on SU + metformin
-Subjects self-titrated insulin:increase 2 units if FPG>100 mg/dl x 3dincrease 4 units if FPG>180 mg/dl x 3d
-Followed for 36 weeks
Yki-Jarvinen et al, Diabetologia 49:442-451, 2006

Symptomatic hypoglycemia:
glargine vs. NPH
Yki-Jarvinen et al, Diabetologia 49:442-451, 2006
Symptomatic hypoglycemia (episodes/patient-year)
Run-in period 0-12 weeks
13-24 weeks 25-36 weeks
0
4
8
12
0
4
8
12
0
4
8
12
0
4
8
12
Glargine NPH
Glargine NPH
Glargine NPH
Glargine NPH
*
Symptomatic hypoglycemia (episodes/patient-year)

Expected decrease A1c
Advantages Disadvantages
α-glucosidase inhibitors (acarbose, miglitol)
0.5-0.8% Weight neutral Expensive, frequent GI side-effects, 3x/day
dosing
GLP-1 agonists (exenatide)
0.5-1.0% Weight loss Expensive, injections, frequent GI side-effects,
little experience
DPP-4 inhibitors (Sitagliptin)
0.5-0.8% Weight neutral Expensive, little experience
Meglitinides 1-1.5% Short duration Expensive, 3x/day dosing, hypoglycemia
Amylin analogues (pramlintide)
0.5-1.0% Weight loss Expensive, injections, 3x/day dosing, frequent
GI side effects, little experience
Nathan et al, Diabetes Care 31:173-175, 2008
Comparison diabetes medications: newer therapies

Measurement of the incretin effect:
OGTT and matched IV infusion
Nauck MA et al: J Clin Endocrinol Metab 63:492-498; 1986
0
50
100
150
200
-30 0 60 120 180
Time (min)
Glucose (mg/dl) Insulin (pmol/l)
-30 0 60 120 180
Time (min)
0
50
100
150
200OralIV

GLP-1 release and its effects
Brain• Satiety
Islets of Langerhans• Increases insulin secretion • May increase ß-cell mass• Inhibits glucagon secretion
Stomach• Delays gastric emptying
GLP-1 release from L
cells
Meal ingestion

GLP-1 release and inactivation
GLP-1(9-36)Inactive
DPP4
Rapid Inactivation(>80% of pool)
Mixed MealIntestinal
GLP-1Release
GLP-1 (7-36)Active
t1/2 = 1-2 min

Exenetide: glucose control and body weight
Blonde L et al: Diabetes Obes Metab 8:436-447; 2006
0.0
-0.5
-1.5
-1.0
0 20 40 60 80
∆ A1c(%)
Treatment (weeks)
Placebo-controlled
trials
Open-label Extensions(10 µg exenatide bid)
Intent-to-treat (n=551)82-week completer (n=314)
-0.8±0.1%
-1.1±0.1%
0
1
3
2∆ BodyWeight
(kg)
4
50 20 40 60 80
Treatment (weeks)
Placebo-controlled
trials
Open-label Extensions(10 µg exenatide bid)
-4.4±0.3 kg
-3.5±0.2 kg

Incidence of significant adverse events with exenatide and insulin glargine
Heine RJ et al: Ann Intern Med 143:559-569; 2005
Adverse Event Exenatide
(n=282), n (%)
Insulin Glargine
(n=267), n (%)
p
ValueNausea 161 (57.1) 23 (8.6) <0.001
Vomiting 49 (17.4) 10 (3.7) <0.001
Diarrhea 24 (8.5) 8 (3.0) 0.006
Upper abdominal pain 12 (4.3) 2 (0.7) 0.012
Constipation 10 (3.5) 1 (0.4) 0.011
Dyspepsia 10 (3.5) 1 (0.4) 0.011
Anorexia 10 (3.5) 0 (0) 0.002
Decreased appetite 9 (3.2) 1 (0.4) 0.021

Inhibition of DDP-4 increases active GLP-1 levels
GLP-1(9-36)Inactive
DPP4
Rapid Inactivation(>80% of pool)
Mixed MealIntestinal
GLP-1Release
GLP-1 (7-36)Active
t1/2 = 1-2 min

DPP-4 Inhibition Increases GLP-1 Levels and Improves Glucose Tolerance in Type 2 Diabetes
Ahrén B et al: J Clin Endocrinol Metab 89:2078-2084; 2004
2
6
10
14
60
80
100
120
-30 0 30 60 90 1200
100
200
300
Placebo (19)Vildagliptin (18)
125
175
225
275
Glucose(mg/dl)
Insulin(pmol/l)
GLP-1(pmol/l)
Time (min)Time (min)
Glucagon(pmol/l)
-30 0 30 60 90 120

Sitagliptin lowers HbA1c
0
-0.4
-0.8
-1.2
-1.6
Placebo-Subtracted
HbA1c(%)
Baseline HbA1c (%)<7 7 - 8.5 ≥8.5
100 mg qDWeek 12
Herman G et al: Diabetes 54 (Suppl 1):A134; 2005
-0.30 -0.64 -1.13

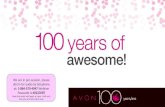
Kupersmith et al, Health Affairs 26:w156-168w, 2007
Diabetes care: How is the VA doing?
HbA1c measured Foot examvisuala
Foot examsensorya
Eye exam
SOURCE: VHA External Peer Review ProgramNOTE: results for VHA primary care outpatients with DMaData for 2004 and 2005 not provided
0
20
40
60
80
100
%
1995
200020012002200320042005
199719981999

Copyright ©2007 by Project HOPE, all rights reserved.
Kupersmith et al, Health Affairs 26:w156-168w, 2007
A1c: How is the VA doing?

Summary
Diabetes is a major health problem in the VA system
Good glycemic control decreases the risk of diabetes complications
Lifestyle changes remain a cornerstone of diabetes prevention and treatment
Multiple medications with different mechanisms of action now exist for the treatment of diabetes
Diabetes treatment should be tailored to the patient, especially in the geriatric population