Unusual case of stridor and wheeze in an infant: Tracheal bronchogenic cyst
4
Pediatric Pulmonology 34:320–323 (2002) Case Reports Unusual Case of Stridor and Wheeze in an Infant: Tracheal Bronchogenic Cyst Barbara Stewart, MD, 1 * Amalia Cochran, MD, 2 Kim Iglesia, MD, 3 V.O. Speights, DO, 4 and Tibor Ruff, MD 5 Summary. Bronchogenic cysts are congenital anomalies that represent aberrant development of the foregut. Bronchogenic cysts in the mediastinum have been documented in both children and adults, but only one case of tracheal bronchogenic cyst in an infant was found in the literature. We report on a case of an infant with wheeze, stridor, and retractions, caused by a midtracheal bronchogenic cyst. This entity, with its unusual location, should be considered in the differential diagnosis of respiratory distress, cyanotic spells, wheezing, and stridor in infants. Pediatr Pulmonol. 2002; 34:320–323. ß 2002 Wiley-Liss, Inc. Key words: bronchogenic cyst; stridor; wheezing; respiratory distress; children. INTRODUCTION Cough, wheeze, shortness of breath, tachypnea, and in- creased work of breathing are the most common symptoms associated with asthma. If symptoms do not resolve after a reasonable trial of asthma therapy, or a child has symptoms that do not fit the typical picture, further evaluation should be considered. Infectious agents (viral or bacterial) and anatomic etiologies must be ruled out. Although anatomic abnormalities are less common than asthma, the index of suspicion should remain high, and definitive diagnostic investigations should be pursued. 1 Bronchogenic cysts are congenital anomalies caused by aberrant development of the foregut. Abnormal bud- ding may occur at any point along the tracheobronchial tree, and migration of the cysts throughout the medias- tinum may occur. For that reason, many bronchogenic cysts documented in the early literature were asympto- matic mediastinal cysts in adults. One case in an infant was reported, i.e., an intramural cyst located just proxi- mal to the carina. 2 Our patient, a Latin-American infant girl, had an intraluminal bronchogenic cyst at midtra- cheal level. CASE REPORT A 7-month-old girl presented for evaluation of acute worsening of lower respiratory symptoms. This episode began with an upper respiratory tract infection, followed by cough and increasing respiratory distress. Past medical history described a term infant with no prenatal or neonatal complications. Persistent wheeze with some increased work of breathing was apparent in the neonatal period, when she was diagnosed clinically with tracheomalacia. No other medical problems were noted. Growth and development had been normal. 1 Department of Pediatric Pulmonology, Scott & White Clinic and Memorial Hospital, Scott, Sherwood and Brindley Foundation, Texas A&M University Health Science Center, College of Medicine, Temple, Texas. 2 Department of Surgery, University of Utah, Salt Lake City, Utah. 3 Department of Pediatric Radiology, Scott & White Clinic and Memorial Hospital, Scott, Sherwood and Brindley Foundation, Texas A&M University Health Science Center, College of Medicine, Temple, Texas. 4 Department of Pathology, Scott & White Clinic and Memorial Hospital, Scott, Sherwood and Brindley Foundation, Texas A&M University Health Science Center, College of Medicine, Temple, Texas. 5 Department of Otolaryngology, Scott & White Clinic and Memorial Hospital, Scott, Sherwood and Brindley Foundation, Texas A&M University Health Science Center, College of Medicine, Temple, Texas. *Correspondence to: Barbara Stewart, MD, 1920 Medi-Park Drive, Suite 2, Amarillo, TX 79106. E-mail: [email protected] Received 9 September 1998; Accepted 9 September 1999. DOI 10.1002/ppul.10129 Published online in Wiley InterScience (www.interscience.wiley.com). ß 2002 Wiley-Liss, Inc.
-
Upload
barbara-stewart -
Category
Documents
-
view
212 -
download
0
Transcript of Unusual case of stridor and wheeze in an infant: Tracheal bronchogenic cyst
Pediatric Pulmonology 34:320–323 (2002)
Case Reports
Unusual Case of Stridor and Wheeze in an Infant:Tracheal Bronchogenic Cyst
Barbara Stewart, MD,1* Amalia Cochran, MD,2 Kim Iglesia, MD,3 V.O. Speights, DO,4
and Tibor Ruff, MD5
Summary. Bronchogenic cysts are congenital anomalies that represent aberrant development ofthe foregut. Bronchogenic cysts in the mediastinum have been documented in both children and
adults, but only one case of tracheal bronchogenic cyst in an infant was found in the literature. We
report on a case of an infant with wheeze, stridor, and retractions, caused by a midtrachealbronchogenic cyst. This entity, with its unusual location, should be considered in the differential
diagnosis of respiratory distress, cyanotic spells, wheezing, and stridor in infants. PediatrPulmonol. 2002; 34:320–323. � 2002 Wiley-Liss, Inc.
Key words: bronchogenic cyst; stridor; wheezing; respiratory distress; children.
INTRODUCTION
Cough, wheeze, shortness of breath, tachypnea, and in-creased work of breathing are the most common symptomsassociated with asthma. If symptoms do not resolveafter a reasonable trial of asthma therapy, or a child hassymptoms that do not fit the typical picture, furtherevaluation should be considered. Infectious agents (viralor bacterial) and anatomic etiologies must be ruled out.Although anatomic abnormalities are less common thanasthma, the index of suspicion should remain high, anddefinitive diagnostic investigations should be pursued.1
Bronchogenic cysts are congenital anomalies causedby aberrant development of the foregut. Abnormal bud-ding may occur at any point along the tracheobronchialtree, and migration of the cysts throughout the medias-tinum may occur. For that reason, many bronchogeniccysts documented in the early literature were asympto-matic mediastinal cysts in adults. One case in an infantwas reported, i.e., an intramural cyst located just proxi-mal to the carina.2 Our patient, a Latin-American infantgirl, had an intraluminal bronchogenic cyst at midtra-cheal level.
CASE REPORT
A 7-month-old girl presented for evaluation of acuteworsening of lower respiratory symptoms. This episodebegan with an upper respiratory tract infection, followedby cough and increasing respiratory distress.
Past medical history described a term infant with noprenatal or neonatal complications. Persistent wheezewith some increased work of breathing was apparent inthe neonatal period, when she was diagnosed clinicallywith tracheomalacia. No other medical problems werenoted. Growth and development had been normal.
1Department of Pediatric Pulmonology, Scott &White Clinic andMemorial
Hospital, Scott, Sherwood and Brindley Foundation, Texas A&M
University Health Science Center, College of Medicine, Temple, Texas.
2Department of Surgery, University of Utah, Salt Lake City, Utah.
3Department of Pediatric Radiology, Scott & White Clinic and Memorial
Hospital, Scott, Sherwood and Brindley Foundation, Texas A&M
University Health Science Center, College of Medicine, Temple, Texas.
4Department of Pathology, Scott & White Clinic and Memorial Hospital,
Scott, Sherwood and Brindley Foundation, Texas A&M University Health
Science Center, College of Medicine, Temple, Texas.
5Department of Otolaryngology, Scott & White Clinic and Memorial
Hospital, Scott, Sherwood and Brindley Foundation, Texas A&M
University Health Science Center, College of Medicine, Temple, Texas.
*Correspondence to: Barbara Stewart, MD, 1920 Medi-Park Drive, Suite 2,
Amarillo, TX 79106. E-mail: [email protected]
Received 9 September 1998; Accepted 9 September 1999.
DOI 10.1002/ppul.10129
Published online in Wiley InterScience (www.interscience.wiley.com).
� 2002 Wiley-Liss, Inc.
On physical examination, she was afebrile and happy,but in moderate to severe respiratory distress. Respiratoryrate was in the 50s/min, with subcostal, intercostal, andsuprasternal retractions noted. Nasal flaring was alsopresent. Lung examination revealed a few expiratorypolyphonic wheezes and a prominent high-pitched mono-phonic expiratory wheeze that was more like an ex-piratory stridor. In the emergency department, oxygensaturations by pulse oximetry were initially in the low90% range, but after admission, documented saturationsranged from > 95–100%. Initial therapy was withnebulized albuterol and intravenous steroids. Chestx-ray showed hyperinflation with everted diaphragmsand an indistinct right heart border (Fig. 1). The childcontinued to appear to have difficulty breathing, despiteher happy demeanor and saturations > 95%.
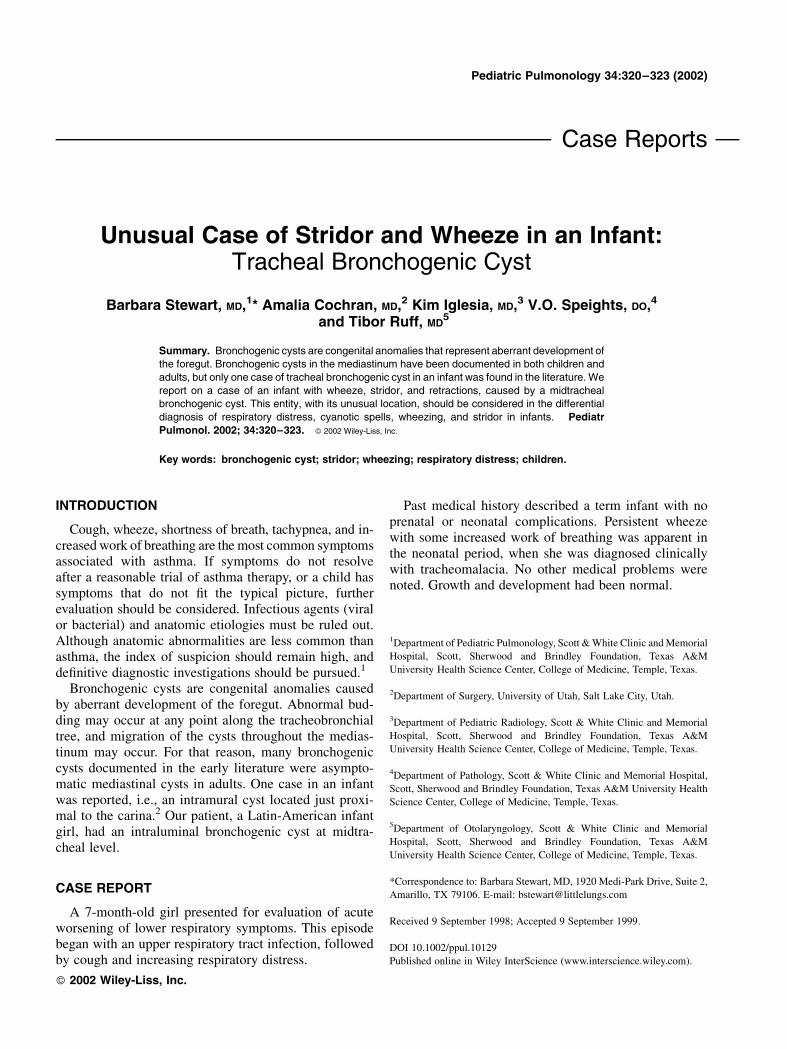
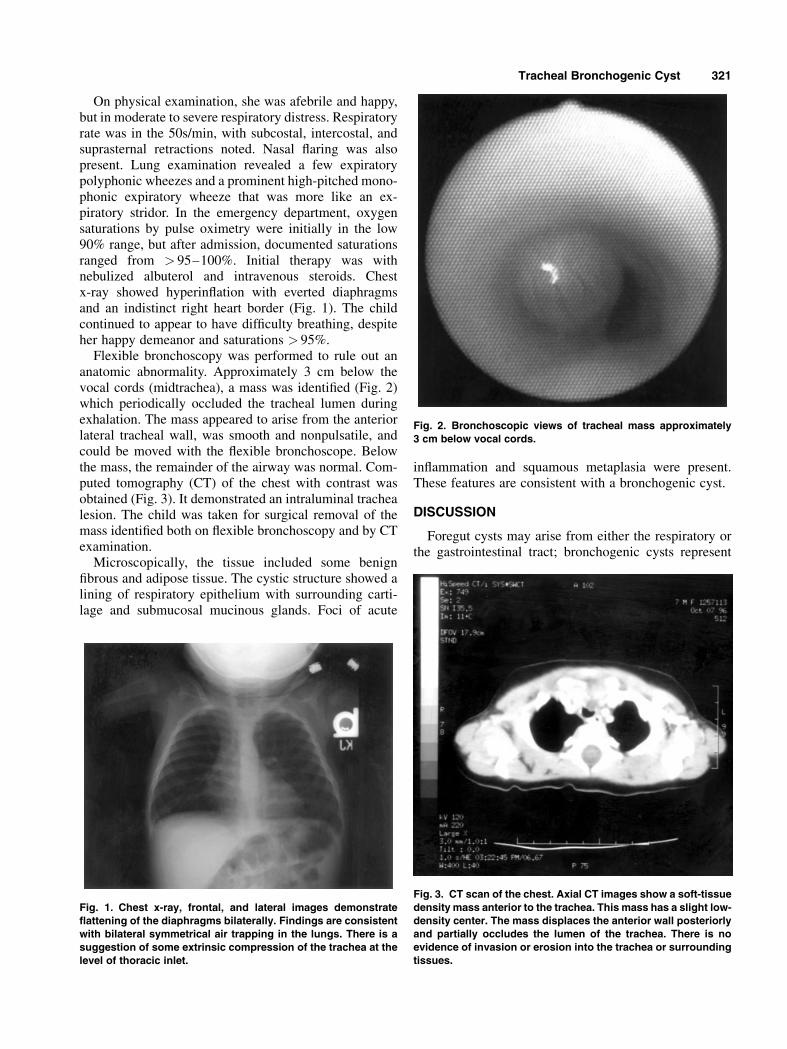
Flexible bronchoscopy was performed to rule out ananatomic abnormality. Approximately 3 cm below thevocal cords (midtrachea), a mass was identified (Fig. 2)which periodically occluded the tracheal lumen duringexhalation. The mass appeared to arise from the anteriorlateral tracheal wall, was smooth and nonpulsatile, andcould be moved with the flexible bronchoscope. Belowthe mass, the remainder of the airway was normal. Com-puted tomography (CT) of the chest with contrast wasobtained (Fig. 3). It demonstrated an intraluminal trachealesion. The child was taken for surgical removal of themass identified both on flexible bronchoscopy and by CTexamination.
Microscopically, the tissue included some benignfibrous and adipose tissue. The cystic structure showed alining of respiratory epithelium with surrounding carti-lage and submucosal mucinous glands. Foci of acute
inflammation and squamous metaplasia were present.These features are consistent with a bronchogenic cyst.
DISCUSSION
Foregut cysts may arise from either the respiratory orthe gastrointestinal tract; bronchogenic cysts represent
Fig. 1. Chest x-ray, frontal, and lateral images demonstrateflattening of the diaphragms bilaterally. Findings are consistentwith bilateral symmetrical air trapping in the lungs. There is asuggestion of some extrinsic compression of the trachea at thelevel of thoracic inlet.
Fig. 2. Bronchoscopic views of tracheal mass approximately3 cm below vocal cords.
Fig. 3. CT scan of the chest. Axial CT images show a soft-tissuedensity mass anterior to the trachea. This mass has a slight low-density center. The mass displaces the anterior wall posteriorlyand partially occludes the lumen of the trachea. There is noevidence of invasion or erosion into the trachea or surroundingtissues.
Tracheal Bronchogenic Cyst 321

those which contain respiratory epithelium. These con-genital cysts may be found throughout the mediastinum,and efforts have been made to classify them based onanatomic location.3 Other causes of wheezing and stridorare more common, but bronchogenic cysts are alwaysimportant to consider in the differential diagnosis. Cor-rect diagnosis of bronchogenic cysts is particularlyimportant because of the potential sequelae and thecorrectable nature of the problem.
The embryologic basis for bronchogenic cysts is well-described.2,4,5 Although a majority of bronchogenic cystsdevelop between days 26–40 of gestation from abnormalbudding of the ventral foregut, they may occur anywherealong the respiratory tract or esophagus, depending onthe specific timing of their origin. Foregut cysts constitute10% of thoracic masses in children, and bronchogeniccysts compose 10% of mediastinal masses in children.6,7
They were rarely diagnosed in children before 1960, untilwhich time they were usually noted at autopsy.
Bronchogenic cysts appear slightly more often on theright than the left, and show a definite male predominancein the literature.6 The most widely used description ofcysts is the anatomic classification of Maier3 includingparatracheal, carinal, hilar, paraesophageal, and miscel-laneous categories. However, cysts may also be describedbased on their relationship with the trachea, in groupssuch as paratracheal, intraluminal, and intramural.8 Re-gardless how they are classified, bronchogenic cysts areusually unilocular and contain clear fluid. They mayrarely contain hemorrhagic secretions or air, and if apatent connection with the airway is present, a risk ofchronic infection is likely.7
Bronchogenic cysts are often an asymptomatic radio-logic finding in adults, which when unrecognized can bedevastating.9 Children may have a variety of symptomsrelated to airway obstruction, including stridor, wheez-ing, cough, nasal flaring, retractions, and intermittent andsevere cyanotic spells.7,8 Infants under 1 year of age oftenpresent with respiratory distress as a result of distortionand angulation of the tracheobronchial tree; further, acheck-valve mechanism is often present that leads toenlargement of the cyst, with compression of the eso-phagus and neighboring vasculature.6,10 As the childrengrow older and the airways stabilize, the cysts take ona less compressive character, and are usually asympto-matic until infection occurs. Symptomatic older childrenand adults typically present with fever, cough, hemopty-sis, and sputum production, and often have recurrentpneumonia.6,7,10 Further complications in patients with abronchogenic cyst may include hemorrhage, pleuralperforation, cyst rupture into adjacent structures, malig-nancy, and sudden death.11–13
Diagnostic studies of bronchogenic cysts remain con-troversial. A chest x-ray may show a bronchogenic cyst asa homogenous fluid density with sharply defined margins,
although it will not show intraluminal cysts and is ofquestionable value in children.7,8 Direct visualizationusing bronchoscopy is usually diagnostic, particularly forintramural or intraluminal cysts, but is not infallible.7
CT scan is the prefered imaging study, particularly ininfants with a paratracheal or intraluminal cyst.8,14
Magnetic resonance imaging (MRI) may also be ex-tremely valuable for confirmation of a diagnosis.8,14
Pulmonary function tests may be helpful if the presenceof fixed airway obstruction is detected, but they do notprovide specific diagnoses.8
Total surgical excision of bronchogenic cysts, even ifasymptomatic, should be performed to avoid possiblecardiorespiratory compromise and infection.6,7 If there isa common membrane between the cyst and a critical ana-tomic structure,5 a small portion of the cystic wall mustbe left behind. If the cyst is large and air-filled, cystotomycan be used to preserve normal lung tissue by deflatingthe cyst and oversewing the edges.15 One report describedthe endoscopic removal of an intramural tracheal cyst,although the cyst type and its location were imperativefor successful removal.2 Use of video-assisted thoraco-scopy for visual diagnosis and definitive treatment hasbeen suggested, but has not yet been studied. As in ourcase, an anterior cervical approach may be technicallymore satisfactory.
Bronchogenic cysts are congenital abnormalities result-ing from aberrant development of the tracheobronchialtree. They are a rare but important cause of respiratorydistress and infections in pediatric patients. Our casereport is the first of an intraluminal midtracheal cyst in aninfant causing severe airways obstruction.
REFERENCES
1. Chernick V, Boat T. Disorders of the respiratory tract in children.6th edition. Philadelphia: W.B. Saunders Co.; 1998. p 129–142.
2. WenigBL,AbramsonAL.Tracheal bronchogenic cyst: a newclini-cal entity? Ann Otol Rhinol Laryngol 1987;96:58–60.
3. Maier HC. Bronchogenic cysts of the mediastinum. Ann Surg1948;127:467–502.
4. Cohen SR, Geller KA, Birns JW, Thompson JW, Meyer BW,Lindesmith GG. Foregut cysts in infants and children. Diagnosisand management. Ann Otol Rhinol Laryngol 1982;91:622–627.
5. Ribet ME, Copin MC, Gosselin B. Bronchogenic cysts of themediastinum. J Thorac Cardiovasc Surg 1995;109:1003–1010.
6. Ombrellaro M, Feola M, Goldthorn JF, Shires GT. Bronchogeniccysts: an overview. Contemp Surg 1993;42:167–171.
7. Yerman HM, Holinger LD. Bronchogenic cyst with trachealinvolvement. Ann Otol Rhinol Laryngol 1990;99:89–93.
8. Klin B, Springer C, Segal M, Eshel G, Tabachnik E, Vinograd I.Recurrent cyanotic spells caused by a segmental intramural cystof the upper trachea. Pediatr Pulmonol 1994;18:119–121.
9. Zaugg M, Kaplan V, Widmer URS, Baumann PC, Russi EW. Fatalair embolism in an airplane passenger with a giant intrapulmonarybronchogenic cyst. Am J Respir Crit Care Med 1998;157:1686–1689.
10. Ribet ME, Copin MC, Gosselin BH. Bronchogenic cysts of thelung. Ann Thorac Surg 1996;61:1636–1640.
322 Stewart et al.

11. Womack NA, Graham EA. Epithelial metaplasia in congenitalcystic disease of the lung. Its possible relation to carcinoma of thebronchus. Am J Pathol 1941;17:645–653.
12. Bauer S. Carcinoma arising in a congenital lung cyst. Dis Chest1961;40:552–555.
13. Behrend A, Kravitz CH. Sarcoma arising in a bronchogenic cyst.Surgery 1951;29:142–144.
14. Suen HC, Mathisen DJ, Grillo HC, LeBlanc J, McLoud TC,Moncure AC, Hilgenbreg AD. Surgical management and radio-logical characteristics of bronchogenic cysts. Ann Thorac Surg1993;55:476–481.
15. Stewart B, Farah AS, Kimura K, McCray PB Jr. Cystoplasty fortreatment of a congenital lung cyst. Pediatr Pulmonol 1995;19:185–187.
Tracheal Bronchogenic Cyst 323