UNRAVELING THE LABYRINTH OF SINUSOIDAL DEPOSITS IN...
45
UNRAVELING THE LABYRINTH OF SINUSOIDAL DEPOSITS IN THE LIVER OF A 68-YEAR-OLD MAN Taofic Mounajjed, M.D
Transcript of UNRAVELING THE LABYRINTH OF SINUSOIDAL DEPOSITS IN...

UNRAVELING THE LABYRINTH OF SINUSOIDAL DEPOSITS IN THE LIVER OF A 68-YEAR-OLD
MAN
Taofic Mounajjed, M.D

Clinical History A 68 year-old man presented with chronic recurrent pleural
effusions
During laboratory workup, abnormal liver biochemistries were discovered
Past medical history End stage renal disease (on dialysis for 1.5 year) Monoclonal Gammopathy Congestive heart failure (EF: 30-35%) Prostate cancer (s/p prostatectomy in 1998) Hypertension Hypercholesterolemia

Laboratory Workup
Serum free light chains • Kappa: 706 mg/dL (normal: 0.33-1.94 mg/dL)
• Lambda: 3.2 mg/dL (normal: 0.57-2.63 mg/dL)
Bone marrow biopsy and flow cytometry
Plasma cell myeloma 10-20% kappa light chain restricted
Subcutaneous fat aspirate Negative for amyloid

Liver Biochemistries Alkaline phosphatase (ALP) 304 U/L (normal: 45-115 U/L)
ALP: liver isoenzyme 265 IU/L (normal: 16.2-70.2 IU/L)
Aspartate transaminase 51 U/L (normal: 8-48 U/L)
Alanine transaminase 42 U/L (normal: 7-55 U/L)
Direct/total bilirubin 0.1/0.6 mg/dL (normal: 0.0-0.3/≤1.2 mg/dL)
Negative serology Viral hepatitis
ANA, AMA, ASMA
Normal alpha-1 antitrypsin levels and phenotype (MM)

HISTOLOGIC FINDINGS

Low power view

Portal tracts

Acinar parenchyma


PAS-D


PAS-D PAS-D: normal

Trichrome Trichrome: normal

Iron

Differential Diagnosis
Diabetic Hepatosclerosis
Steatohepatitis
Venous Outflow Impairment
Amyloidosis
Col
lage
n

Differential Diagnosis: Diabetic Hepatosclerosis
H&E Trichrome

Differential Diagnosis: Steatohepatitis
H&E Trichrome

Differential Diagnosis: Venous Outflow Impairment
H&E Trichrome

Differential Diagnosis: Amyloidosis
Portal Linear
Globular

Differential Diagnosis: Amyloidosis
Congo Red

Differential Diagnosis Diabetic Hepatosclerosis
Steatohepatitis
Venous outflow impairment
Amyloidosis Special studies helpful to further investigate diagnosis: IHC
EM
MS

SPECIAL STUDIES

Congo Red Stain

Immunohistochemistry
Kappa light chain Lambda light chain

Electron Microscopy

Mass Spectrometry Powerful method of substance identification and quantification, by accurate
determination of its molecular mass
Identifies ionized molecules by measuring their m/z ratio
Vrana, Game, Madden et al. Blood. 2009 Dec 3;114(24):4957-9
Proteomics methods using MS have emerged as a useful method in protein identification in FFPE tissue
Amyloid identification/typing

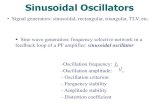
Mass Spectrometry: Proteomics in FFPE Tissue
Proteome Software Inc.

Mass Spectrometry: Bioinformatics
Three distinct statistical algorithms used to identify proteins from MS data
Mascot Seaquest X-Tandem
Zenka, Johnson and Bergen, Exploring Proteomics Metadata using Spotfire and Companion User Interface (ASMS 2011)


Patient
Normal liver control0
20
40
60
80
100
120
11 kDa12 kDa
12 kDa25 kDa
36 kDa
Cluster of Iglambda chain C
regionsIg kappa chain C
region Cluster of Igkappa chain V-I
regionSerum amyloid P-
component Apolipoprotein E
Patient
Normal liver control
Molecular mass
Sig
nal
inte
nsi
ty

DIAGNOSIS Summary of findings: Perisinusoidal deposit
Congo Red: negative
EM: granular deposit in space of Disse
MS: kappa light chain deposit
Diagnosis: Light Chain Deposition Disease (LCDD)
involving the liver

DISCUSSION

LCDD Systemic disease characterized by: Clonal proliferation of plasma cells
Deposition of non-amyloid monoclonal immunoglobulin light chains in tissue
Occurs in 5% of multiple myeloma patients
Median age is 58 years

LCDD Tissue deposits cause organ
dysfunction kidney is the most frequently
involved organ
Laboratory diagnosis SPEP/UPEP
IFE
Immunoglobulin FLC
Bone marrow Bx/flow cytometry
Tissue biopsy
Nodular mesangial sclerosis with silver positive mesangial matrix
H&E Silver Jones
IF: Lambda IF: Kappa

LCDD: Liver Involvement
Occurs in 23% of cases Often accompanied by renal involvement
Liver involvement is most frequently asymptomatic
Variable clinical presentation
Abnormal liver biochemistries: Alkaline phosphatase most frequent
Portal hypertension is a frequent result

Microscopy Perisinusoidal deposits
PAS-D positive
Congo Red negative
Involvement by plasma cell neoplasm frequently absent
LCDD: Liver Pathology
Ultrastructure Granular deposit in
space of Disse

Perisinusoidal deposits spare portal tracts
LCDD: Liver Pathology

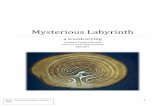
LCDD vs. Amyloidosis
Klabunde et al. Crystal structure of human transthyretin. Nature Structural & Molecular Biology 7, 312 - 321 (2000)
Protein deposits differ between the 2 entities: LCDD: light chains are unaltered
Amyloidosis (AL): misfolded proteins (beta-pleated sheet formation) Unique tinctorial properties
Association with universal amyloid protein

LCDD
Amyloid
LCDD vs. Amyloidosis: Ultrastructure

LCDD vs. Amyloidosis Systemic Amyloidosis LCDD
Plasma cell neoplasm Present (AL type) Present
Deposit location Variable perisinusoidal
Deposit appearance Variable Linear
Congo Red Positive Negative
PAS-D Negative or weak Positive
EM of deposits Randomly oriented fibrils Granular: space of Disse
MS • Monoclonal light chains (AL type) • Universal amyloid proteins
• Apolipoprotein E • SAP
• Monoclonal light chains • Low levels of universal
amyloid proteins

FOLLOW-UP

FOLLOW-UP Kidney biopsy: Kappa-light chain deposition disease
Liver involvement by LCDD initiation of treatment by Cyclophosphamide, Bortezomib and Dexamethasone
Pleural effusions Resolved by treatment with thoracocentesis
CHF Patient was diagnosed with dilated cardiomyopathy:
medical management with good control

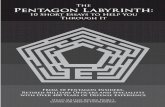
FOLLOW-UP
0
100
200
300
400
500
600
0 2 4 6 8
Serum kappa-FLC
Serum kappa-FLC
0
20
40
60
80
100
120
140
160
0 2 4 6 8
Kappa/lambda FLC ratio
Kappa/lambdaFLC ratio
0
50
100
150
200
250
300
350
0 2 4 6 8
Alkaline phosphatase
Alkalinephosphatase
months
months
months

Conclusion LCDD is a rare but important entity to consider in the
differential diagnosis of amyloid-like deposits in the liver
LCDD has a characteristic perisinusoidal deposition pattern
The H&E histology of LCDD can be very subtle PAS-D can be helpful
Special studies can differentiate LCDD from amyloidosis: Congo Red EM MS

THANK YOU!
Questions/Comments?