Erythropoietin Improves Atrophy, Bleeding and Cognition in ...
Upload
doug-jonesCategory
view
216download
1
British Journal of Haernatobgy, 1992, 80, 406-41 5
Case Reports
IJNMAINTAINED TRILINEAGE RESPONSE TO KECOMRTNANT HUMAN ERYTHROPOIETIN IN A PATIENT WITH MYELODYSPLASIA
Kecombinant human erythropoietin (r-HuEPO) improves anaemia in patients with diseases where there is a deficiency of erythropoietin (Abels & Rudnick, 19 9 1 ). Myelodysplasia ( M I X ) differs in that erythropoictin levels are significantly higher (Jacobs et al. 1989). There is little information on the use of rHuEPO for MDS. This report shows a trilineage response to rHuEPO in a n MDS patient.
A 75-year-old man had pancytopenia (since May 1989) and bone marrow findings ofrefractory anaemia. He required monthly transfusions (two units) to maintain a haemoglobin of 8.0 g/dl. The pancytopenia had not responded to treatment with cyanocobalamin, folate, pyridoxine, or granulocyte- niacrophage colony stimulating factor (GM-CSF). The patient's last GM-CSF was in November 1989. Physical examination was non-contributory.
Blood counts were a WBC of 2.1 x 10y/l, an absolute neutrophil count (ANC) of 0 4 x 1 Oy/L a haemoglobin of 7.9 g/dl, a haematocrit of 23.5%. reticulocyte count of 1.0% and platelets were 13 x lOY/l. Bone marrow was normocellular (50%) with decreased megakaryocytes ( < 1 low power field
(LPF), and dysplastic erythroblasts (59%). The erythroblasts were megaloblastic with double-nucleated cells. In addition, multiple mitotic figures were seen. Myeloblasts were 2.3%. and cytogenetics were normal. Erythropoietin level was 400 mU/ml (normal 0-20).
In February 1990, intravenous r-HuEPO (Ortho Biotech Corp., Raritan, N.J.) was initiated (500 U/kg thrice weekly). Weekly doses were adjusted by haemoglobin levels (if 4 weeks or greater post-transfusion) as follows: Hb 9.1-10.5 g/dl, two doses; 10.6-1 2 g/dl. once, and held if Hb > 12 g/dl. This protocol was approved by the Institutional Keview Boards of Montefiore and Western Pennsylvania Hospitals, and written consent was obtained.
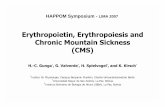
After starting rHuEPO. the times to a doubling of ANC, reticulocyte count and platelet count were 2, 3 and 5 months. respectively (Fig 1). After 10 mmths the erythro- poietin level was 84.3 mlJ/ml. when Hb was 12 .3 g/dl. He remains transfusion-independent 19 months off therapy. Recent blood counts (4 September 1991) were a WBC of 5.3 x 10"/1. a n ANC of 2 .9 x lOY/ l , a haemoglobin and
rHuEPO I I
- 80 - 70 Absolute - 60 retics - 50 109 IL
( 0 ) - 40 - - 50
- 40 Platelets 1 0 ~ 1 ~ ( B )
- 30
- 20
- 10 I
+lo 0 I I I I I I I I I I I I I I I I
-2 0 +5 Time (months)
Fig 1. Trilineage response to rHuEPO in MDS (RA). rHuEPO administration is represented by the filled bar. Blood transfusions (2 U) are indicated by arrows. Hb is represented by filled circles and absolute retics by open circles. ANC is depicted by x and platelets by closed squares. l'ime is shown as months in relationship to rHuEPO. The times to a doubling of ANC. retics and platelets were 2 , 3 and 5 months respectively. The patient has not required further rHuEPO and has remained stables for 22 months.
406

Crrse Reports 407
haematocrit of 13.9 g/dl and 42.2%. and a platelet count of 54 x 1 O Y / I .
A bone marrow aspirate (post-rHuEPO) was hypocellular ( 3 0 % ) with megakaryocytes (4/LPF) and showed normoblas- tic erythroid cells ( 30.4%). There were 3.2% myeloblasts. Erythroid progenitors improved following r-HuEPO therapy. Before r-HuEPO. erythroid colony forming unit (CFU-E)/I O5 bone marrow cells were 6 . 0 f 2 . 3 (SD). n = 3 compared to 18.5f4.1. post therapy (P=O.O2) . Sirnilarlyerythroid blast forming units (BFU-E) increased from 1.8 f 0 . 3 to 20.2 f 2 . 3 colonies/ 1 Oi bone marrow cells ( P < 0.0 1 ).
This patient with MDS. resistant to other therapies, had a trilineage response to rHuEPO. The haematologic response was associated with an increase in erythroid progenitors, and his bone marrow showed resolution of erythroid hyperplasia with a decrease in dysplastic cells. Moreover, the response has been maintained after discontinuation of the rHuEPO. This response pattern contrasts with that in other MDS patients. Most responses have been erythroid and required continued rHuEPO administration (Bessho et a/. 1990: Schouten et al. 1991: Stebler et al. 1990: Stein e t a l , 1991).
Post-therapy, the patient's erythropoietin level was lower than before therapy. Similar declines have been observed following red cell responses to rHuEPO in MUS (Bessho rt a/. 1990). It is possible that rHuEPO may selectively stimulate normal cells or induce maturation of an abnormal clone. In this patient, his marrow aspirate was less dysplastic post- therapy. suggesting that rHuEPO selectively stimulated growth of his normal clone of cells. However, since this patient's chromosomes were normal, the exact mechanism could not be determined. A similar situation has been reported by Vadhan-Raj r t a1 (1989) in an MUS patient who had a sustained trilineage response to GM-CSF. that was associated with loss of abnormal chromosomes.
This case illustrates an occasional patient with MDS may respond to pharmacological doses of r-HuEPO. even after failure of previous growth factors. One cannot exclude whether GM-CSF treatment prior to r-HuEPO was responsible for the dramatic response in this patient. Nevertheless. this suggests that rHuEPO, alone or in combination with other growth factors, deserves further evaluation in MDS.
ACKNOWLEDGMENTS
The authors thank Carolyn Elwood for preparing the manu- script.
This work was supported by a grant from the R. W. Johnson Pharmaceutical Research Institute, Raritan. N.J.
Montefiore University Hospital, DOIIG JONES
Univrrsitg of Pittsburgh School of Medicine, CRAIG S . ROSENFELI) Pittsburgh. Pa., U.S.A.
ZELLA R. ZEICLER
RICHARD K. SHALILI~ICK
REFERENCES
Abcls. R.I. & Rudnick. S.A. (1 99 1) Erythropoictin: evolving clinical applications. Experitnet~tal Hematologg. 19. 842-8 50.
Bessho. M.. Jinnai. I., Matsuda. A,. Saito. M. & Hirashima. K. ( 1 990) Improvement of anemia by recombinant erythropoietin in patients with myclodysplastic syndromes and aplastic anemia. Irtter- nntioriul jourrtnl of Cell Cloning. 8. 445-458.
lacobs. A.. Janowska-Wieczorek, A,. Caro. 1.. Bowen. D.T. &Lewis. T. ( 1989 1 Circulating erythropoietin in patients with myelodysplas- tic syndromes. British ]ourrial of Hrerternatologg. 73, 3 h.
Schoutcn. H.C.. Vellenga. E.. van Rhenen. U.. deWolf. J.T.H.M.. Coppens. P.J.W. & Blijham. G.H. ( 1 99 1 I Recombinant human erythropoietin (rhEPO) for patients with myclodysplastic syn- drome (MDS). Irrrkcrnin. 5, 432-41h.
Stebler. C.. Tichelli. A,. Dami. H.. Gratwohl. A.. Nissen. C. & Speck. B. ( 1990) High-dose recombinant human erythropoietin for treat- mcnt of anemia in myelodysplastic syndromes and paroxysmal nocturnal hemoglobinuria: a pilot study. Exprririwritnl Hcrmtolog,q. 18. 1204-1208.
Stein. R.S.. Ahcls, R.I. & Kranti. S.B. [ 199 1 ) Pharmacologic doses of recombinant human erythropoietin in the treatment of myelodys- plastic syndromcs. Blood. 78, 1658-1 hh3.
Vadhan-Raj. S.. Broxmeyer. H.E.. Spitzr. C.. LeMaistre. A.. Hultmm. S.. Vcntura. G.. Tigaud. 1.D.. Cork, M.A.. Trujillo. J.M.. (httcrrniin. J,[J. & Hittelman. W.N. (1989) Stimulation of non-clonal hemato- poiesis and suppression of the neoplastic clone after treatment with recombinant human granulocyte-macrophage colony-stimulat- ing factor in a patient with thcrapy-related myelodysplastic syndrome. Hlood. 74, 1491-1498.
A S E C O N D B O N E MARKOW BIOPSY AS A CAIJSE OF A FALSE DIAGNOSIS O F MYELOFIBROSIS
fiealing of bone fractures follows a specific sequence as described by Revell ( 1 9 86) which includes the disappearance of haemopoietic and fat tissues, the migration of polymorpho- nuclears and macrophages to the fracture area. the forma- tion of granulation tissue with development of fibrous tissue. iind the formation of primary and secondary callus. the latter implying important osteoblastic activity which takes place 3 weeks after the injury.
A bone marrow biopsy (BMB) performed on ii previously injured bone may show ii myelofibrotic pattern identical to that observed in several haeniatologic and non-haematologic disorders. We obscrved this phenomenon in two patientv who
underwent a second 13M13 in the same site of previous bone damage.
Cnsr 1 , A 72-year-old man with severe peripheral pancyto- penia underwent a BMH on the right anterior iliac crest. Because of technical problems. the exploration was repeated. and by chance performed at thc same site of the same iliac crest. Bone marrow histology showed abnormal marrow architecture with intense reticulin arid collagen tibrosis and presence of bone neoforniation. The only cellularity was constituted by some erythroblastic nests (Fig 1 a) . In conse- quence, the diagnosis of idiopathic myelofibrosis was estab- lished. However. since the clinical and peripheral picture