
Unknown primary tumor by immunohistochemistry
79
J. Klos MD Department of Pathology Stavanger University Hospital Norway 1 Unknown primary tumor by immunohistochemistry Immunhistokjemi for patologer 17.03.2021 Stavanger
Transcript of Unknown primary tumor by immunohistochemistry

J. Klos MD
Department of Pathology
Stavanger University Hospital
Norway
1
Unknown primary tumor by
immunohistochemistry
Immunhistokjemi for patologer17.03.2021 Stavanger
Conflict of interests
NONE
2
Unknown Primary Tumor (Cancer of the Unknown Primary – CUP)
Histologically confirmed metastatic cancer for which primary site cannot be identified after standard diagnostic approach.
• Accounts for 2-5% of malignancies diagnosed in the US • 7th or 8th most frequent cancer • 4th or 5th most common cause of cancer death in both
sexes• The number of cases shows decreasing tendency …
Metastasis as a first presentation in 5 - 15% of cancers
3

Unknown primary tumor
• Adenocarcinomas (~80%)pancreas, lung, colon and rectum, liver and biliary tract, stomach, kidney, ovary, prostate, breast …
2/3 well differentiated and 1/3 poorly differentiated
• Squamous cell and urothelial carcinomas (~5-10%)• lung, head and neck, oesophagus, uterine cervix, …
• Nonepithelial neoplasms (~10-15%)malignant lymphomas (10%), melanomas (6%), sarcomas (1%), germ cell tumours (06%),
mesothelioma (0,2%), other (2%)
4

Relevance of cancer type/origin
• Differences in prognosis
• Differences in treatment regimes
carcinomas (breast, prostate, ovary, thyroid, . . .)
malignant lymphomas
germ cell tumours
neuroendocrine tumors
sarcomas (GIST, synovial sarcoma . . .)
5
Pathology is an effective method of investigating in CUP
Essentials for right diagnosis
• Quality and quantity of the material
• Quality of standard laboratory procedures
• Quality of immunohistochemistry
• Sufficient number of available antibodies
• Pathologist with sufficient knowledge of morphological spectrum of tumors as well as variation in their immunophenotype and at least basic knowledge of immunohistochemistry!
6
No “shot gun” immunohistochemistry!
How to approach the problem?
7
Step by step
• Review the slide - get your first morphological impression
• Get additional information
• Review the slide again - get your second morphological impression
• Determine the basic panel defining the broad category of neoplasm or go to the next step if needed
• Determine advanced panel defining subtype/origin of neoplasm considering transcription factors in the first line
Important to secure sufficient number of slides for additional stains at early stage of investigation!
8
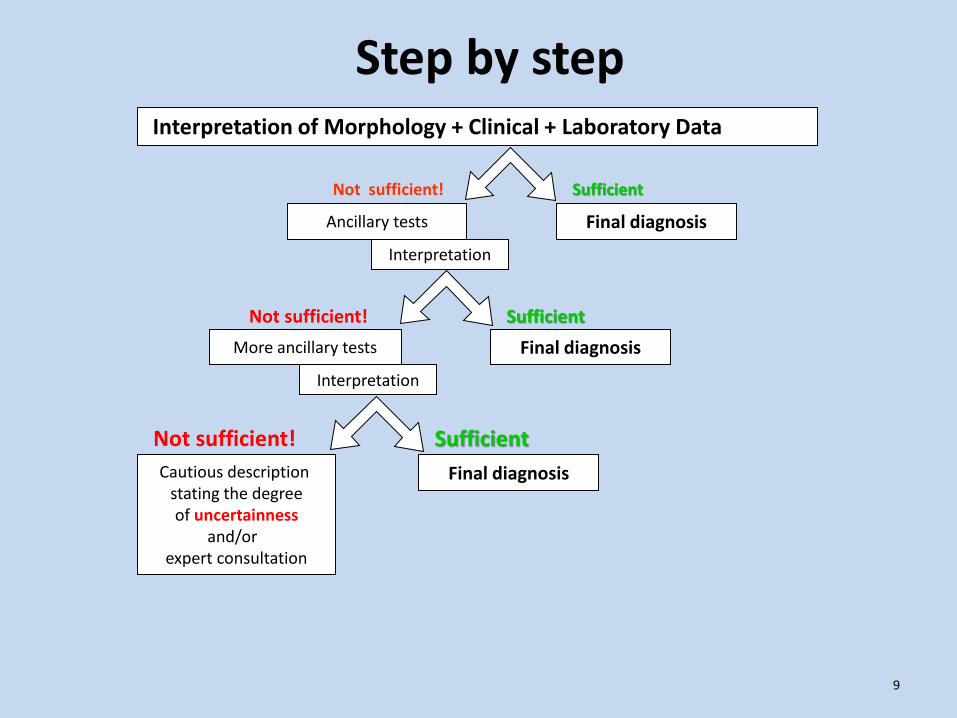
Final diagnosis
Interpretation of Morphology + Clinical + Laboratory Data
Sufficient
Sufficient
Sufficient
Not sufficient!
Not sufficient!
Ancillary tests
More ancillary tests Final diagnosis
Not sufficient!
Interpretation
Final diagnosisCautious description stating the degreeof uncertainness
and/or expert consultation
Interpretation
9
Step by step
Part IApproach to neoplasm with
non-characteristic morphology (panel for poorly differentiated tumors)
10
The most important factor in designing IHC panels is …user`s experience
11
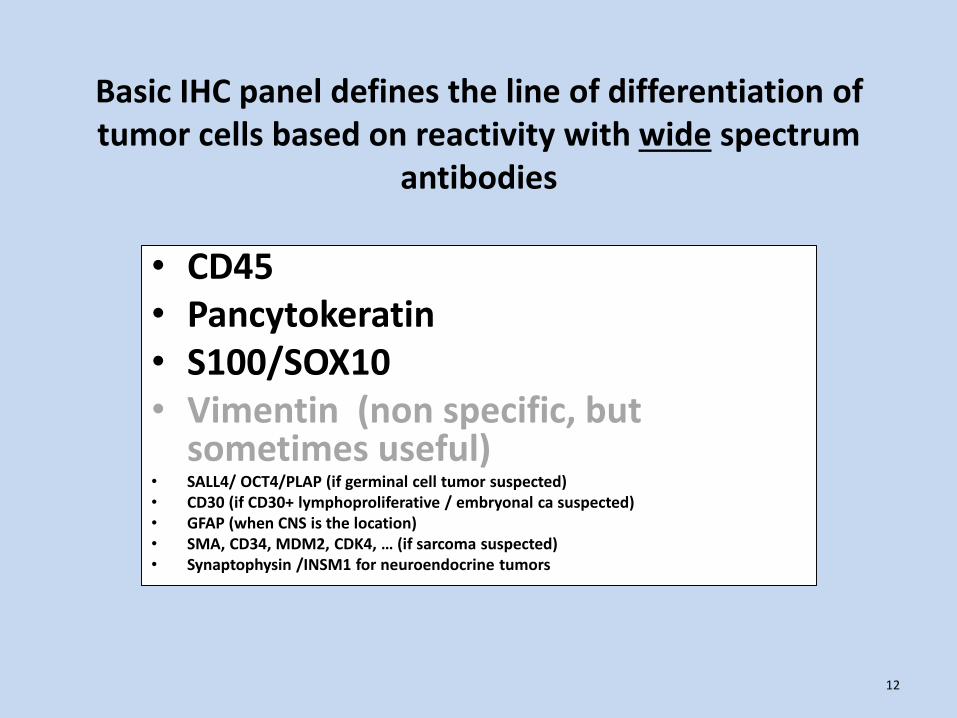
Basic IHC panel defines the line of differentiation of tumor cells based on reactivity with wide spectrum
antibodies
• CD45• Pancytokeratin• S100/SOX10• Vimentin (non specific, but
sometimes useful)• SALL4/ OCT4/PLAP (if germinal cell tumor suspected)• CD30 (if CD30+ lymphoproliferative / embryonal ca suspected)• GFAP (when CNS is the location)• SMA, CD34, MDM2, CDK4, … (if sarcoma suspected)• Synaptophysin /INSM1 for neuroendocrine tumors
12
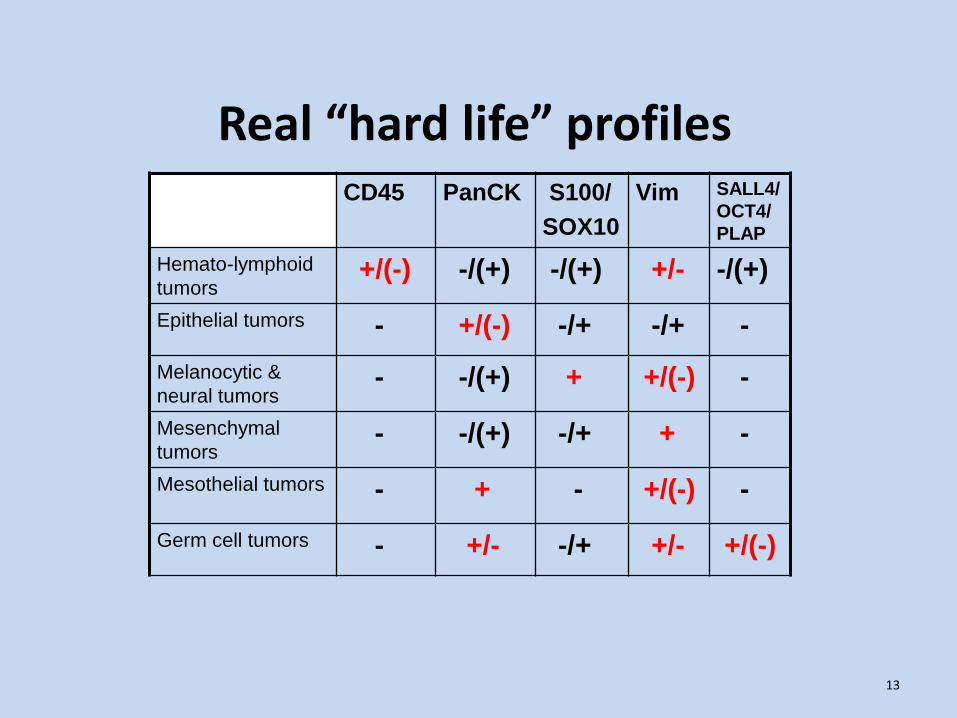
Real “hard life” profilesCD45 PanCK S100/
SOX10
Vim SALL4/
OCT4/
PLAP
Hemato-lymphoid
tumors+/(-) -/(+) -/(+) +/- -/(+)
Epithelial tumors - +/(-) -/+ -/+ -
Melanocytic &
neural tumors- -/(+) + +/(-) -
Mesenchymal
tumors- -/(+) -/+ + -
Mesothelial tumors - + - +/(-) -
Germ cell tumors - +/- -/+ +/- +/(-)
13

CD45
Family of membrane bound glycoproteins with tyrosine phosphatase properties involved in signal transduction and cell activation
• Present at cell membranes of lymphocytes, monocytes and blast cells except erythropoietic cells, plasma cells and mature megakaryocytes
• Not found on cells of other lineages!
• Membranous reactivity pattern
14
The concentrated mAb clones 2B11+PD7/26 and X16/99 and RTU with above clones as well as mAb clone RP2/18 can give optimal results.
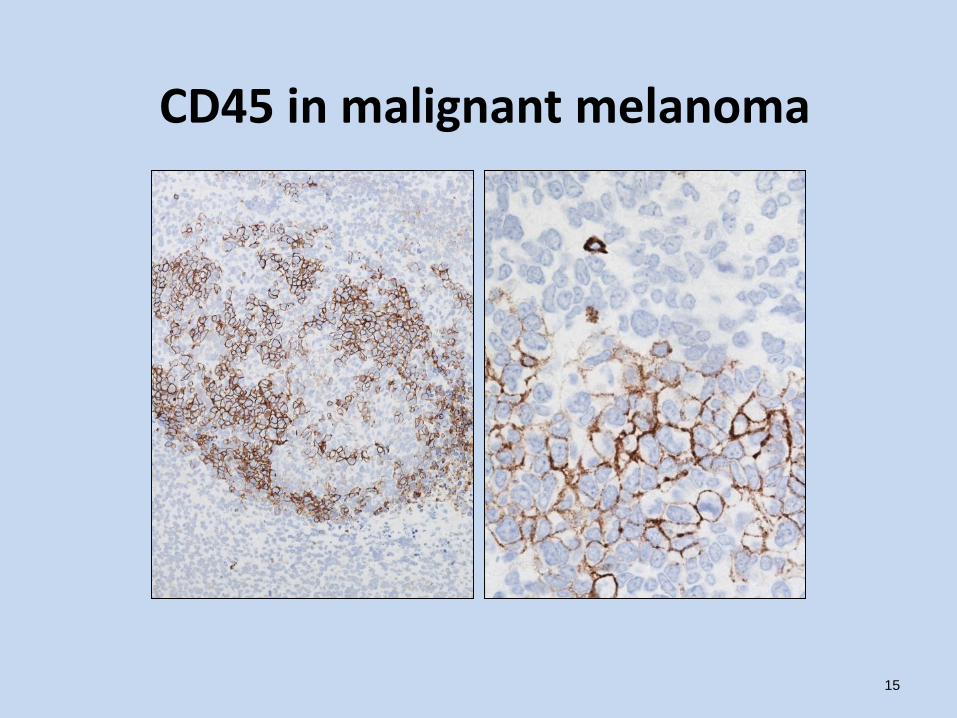
CD45 in malignant melanoma
15
Case 1
• 50 yrs.
• Anemia, growing tumor of testis
• No relevant medical history
• Orchidektomy
16
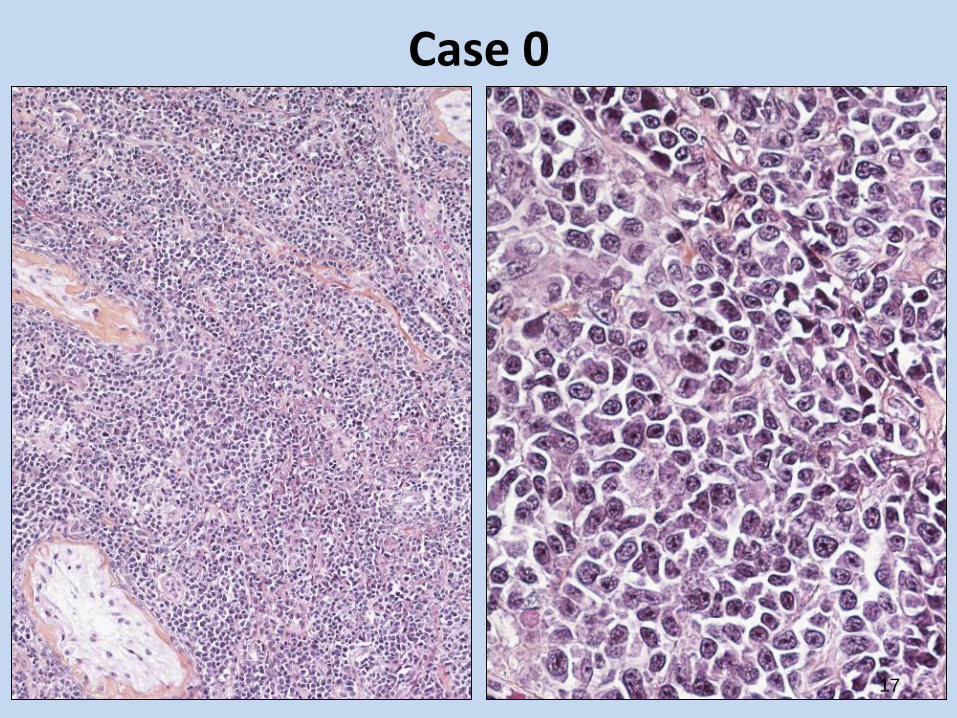
Case 0
17

Case 0
• PanCK negative
• S-100 negative
• CD45 weaker then normal lymphocytes
Vimentin
Vimentin
CD45
18
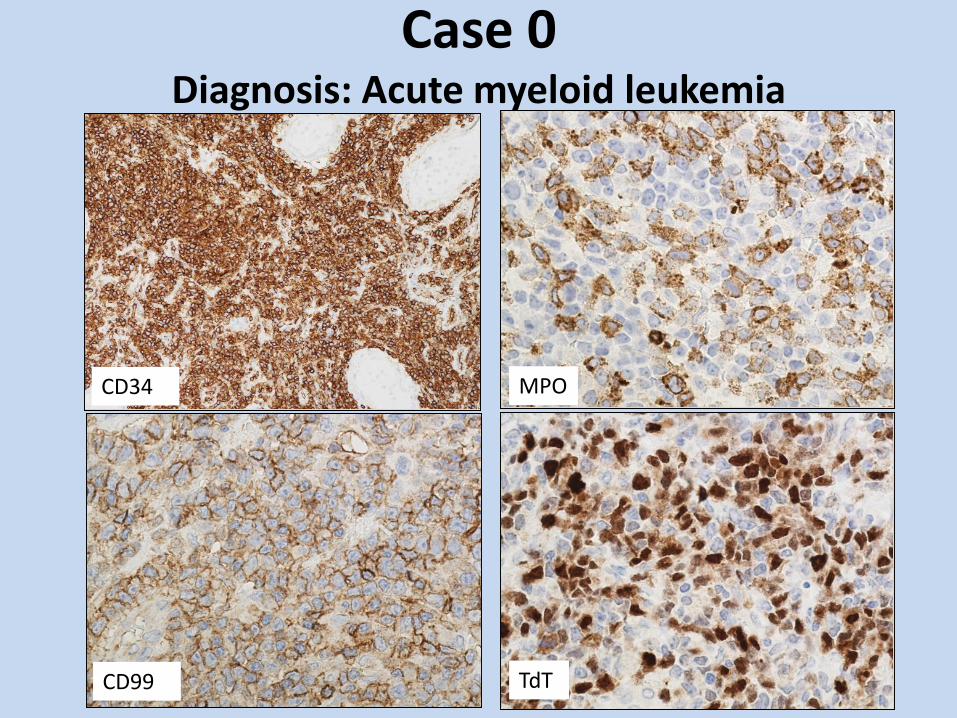
Case 0 Diagnosis: Acute myeloid leukemia
CD34
TdT
MPO
CD99

CD45 PanCK S-100/
SOX10
Vimentin
Hematolymphoid
tumors+/(-) -/(+) - (+) +/-
Hematolymphoid neoplasms which are most likely negative for CD45:
• Acute Lymphatic Leukemia/Lymphoblastic lymphoma • Plasmacytoma • Plasmablastic lymphoma*• ALCL*• HRS cells in classic Hodgkin lymphoma
* ALCL and plasmablastic lymphoma may show positivity for
cytokeratin (CK8/18) - most often in form of paranuclear dots• S-100 is positive in dendritic cell and histiocytic neoplasms• Vimentin is positive in ~70% of hematolymphoid neoplasms and
is positive in many other tumors
20
Pancytokeratin (PanCK)Cytokeratins (CK): intermediary filament type important for intracellular transport and physical cell properties.• 20 different CK identified (+ 34 trichokeratins)
• PanCK antibody should react with as many CK types as possible including CK8/18
• Cytoplasmic reactivity pattern
• Often (~70%) true positive in necrotic areas
• More cytokeratin positivity is seen in alcohol fixed tissues/cells
21
Concentrated mAbs:
AE1/AE3 (CK1-8,10,14-16 and 19, but does not detect CK17 or CK18),
AE1/AE3/5D3 and AE1/AE3/CAM5.2 (does not detect CK17) and mAb BS5 as well as RTU: AE1/AE3 and AE1/AE3/PCK26 may give optimal results.
MNF116 stains CK 5, 6, 8, 17 and 19? - gave inferior performance last runs.
34βE12 stains CK1, 5, 10, 14 and ? CK19? - sensitive, but not appropriate for detection of CKHMW (use CK5 or CK5/6 instead).
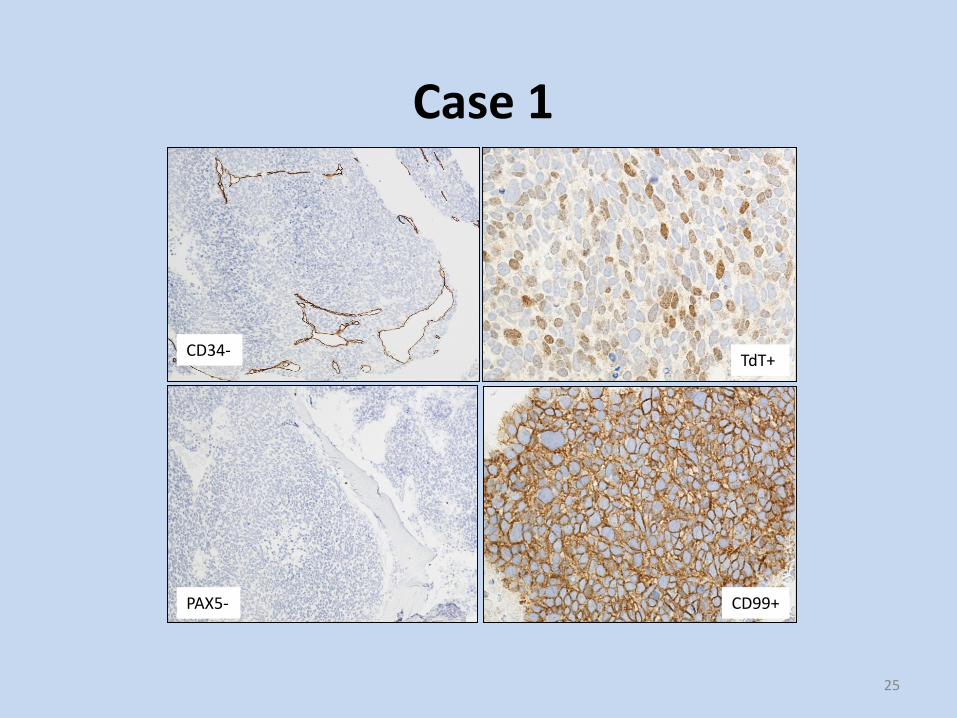
Case 1
• Male 65 years• Investigated for anemia/pancytopenia• Smear from BM: massive with
monotonous blast-like malignant cells. • Lymphoproliferative disease? • Trephine biopsy of BM
22

23
Case 1

Case 1
24
PANCK PANCK-/+
CD45- S-100- and Vimentin-
Case 1
25
CD34-
CD99+
TdT+
PAX5-

CD56+Synaptophysin+
EPCAM+ TTF1+
Case 1
Case 1
• Cytokeratin is absent by IHC staining ~10% of small cell carcinoma.
• EP-CAM and CD56 are more often positive than cytokeratin.
• EPCAM and EMA may be used in panel as secondary broad spectrum epithelial markers if knowing their limitations.
• TTF1 is absent in about 10% of small cell carcinoma of the lung.
• TTF1 is positive in 20-30% of extra pulmonary small cell carcinomas.
• In discrepant cases additional panel of antibodies should be applied.
27
Diagnosis: Metastatic small cell neuroendocrine carcinoma (PANCK negative by IHC staining) probably from lung.
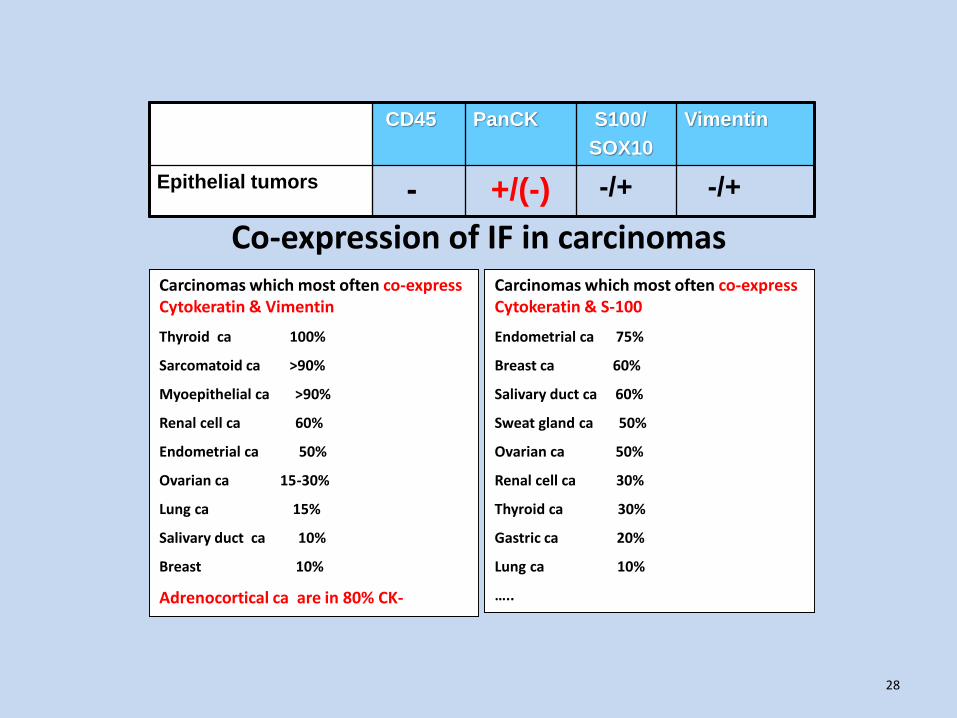
Carcinomas which most often co-express Cytokeratin & Vimentin
Thyroid ca 100%
Sarcomatoid ca >90%
Myoepithelial ca >90%
Renal cell ca 60%
Endometrial ca 50%
Ovarian ca 15-30%
Lung ca 15%
Salivary duct ca 10%
Breast 10%
Adrenocortical ca are in 80% CK-
Carcinomas which most often co-express Cytokeratin & S-100
Endometrial ca 75%
Breast ca 60%
Salivary duct ca 60%
Sweat gland ca 50%
Ovarian ca 50%
Renal cell ca 30%
Thyroid ca 30%
Gastric ca 20%
Lung ca 10%
…..
Co-expression of IF in carcinomas
CD45 PanCK S100/
SOX10
Vimentin
Epithelial tumors - +/(-) -/+ -/+
28

Non epithelial tumors and PanCK
• Mesothelioma (Calretinin, Podoplanin, WT1, Vimentin, …)
• Myoepithelial tumors (S-100, SMA, GFAP, Calponin, Vimentin, …)
• Chordoma, Parachordoma (S-100, EMA, Vimentin, …)
• Some myofibroblastic proliferations (Actin , Vimentin, …)
• Sex cord stromal tumors (SF1, Inhibin, Vimentin, EMA-, ...)
• Carcinosarcoma (biphasic growth pattern - Vimentin, …)
• Sarcomas (synovial, epithelioid, leiomyosarcoma, …- Vimentin, …)
• Chorioid plexus tumors (GFAP, S-100, … )
• Aberrant expression in different tumors (e.g. lymphomas, melanomas)
• Occasional astrocytic tumors with true epithelial component (Vimentin, GFAP, …) otherwise it`s cross-reactivity with AE1!
29

Expression of epithelial markers is not uncommon in hematolymphoid tumors: ALCL (majority of cases), Plasma cell tumors, NLPHL, DLBCL, TCHRLBCL, ALK+ LBCL, Plasmablastic lymphoma, FDS …Certain soft tissue and bone tumors show also positivity: liposarcoma, synovial sarcoma, solitary fibrous tumor, rhabdomyosarcoma, epithelioid hemangioma and angiosarcoma, perineurioma, myoepithelial tumors, epithelioid sarcoma, DSRCT, extrarenal rhabdoid tumor, osteosarcoma, chordoma …
30
Expression of epithelial markers (CKs and EMA/MUC1) in nonepithelial tumors
Aberrant cytokeratin (CK8/18) expression in Plasmablastic lymphoma
EMA expression in ALK+ ALCL in pleural fluid

S100Member of a family of calcium binding proteins. Exact function is not known, but protein is involved in activation of protein kinases, cell growth and proliferation, cell motility and adhesion.
• Present (often with co-expression of IF) in gliomas, neural and melanocytic tumors, sweat and salivary gland tumors, PNET, liposarcoma, chondrosarcoma, serous and endometrioid carcinoma, myoepithelial tumors, renal cell carcinoma, papillary and follicular thyroid carcinoma, chordoma, rhabdomyosarcoma, ….
• Cytoplasmic and nuclear reactivity pattern
31
The concentrated mAb clone 4C4.9, pAb Z0311, pAb NCL-L-S100p as well as RTU pAb IR504, pAb GA504, pAb 760-2523 can give good or optimal results.

S-100 staining in epithelioid melanoma
32
SOX10SOX10 is a transport protein between nucleus and cytoplasm and acting as a transcriptional activator involved in embryonic development.Nuclear staining in virtually all cases of melanocytic nevi and malignant melanoma (reactivity may be focal in desmoplastic and spindle cell melanomas), schwannoma, neurofibroma, granular cell tumor, clear cell sarcoma of tendons and aponeuroses. Majority of myoepithelial and salivary gland tumors, oligodendroglioma, astrocytoma and glioblastoma are positive.
Cave!
SOX10 is expressed in about half of cases of basal-like and metaplastic triple-negative breast carcinomas and less than half of malignant peripheral nerve sheath tumor (MPNST).
All other epithelial and mesenchymal tumors are negative in more than 95%.
The mAb clones BC34 and BS7 and the rmAb clones EP268 and SP267 can give optimal staining.
33
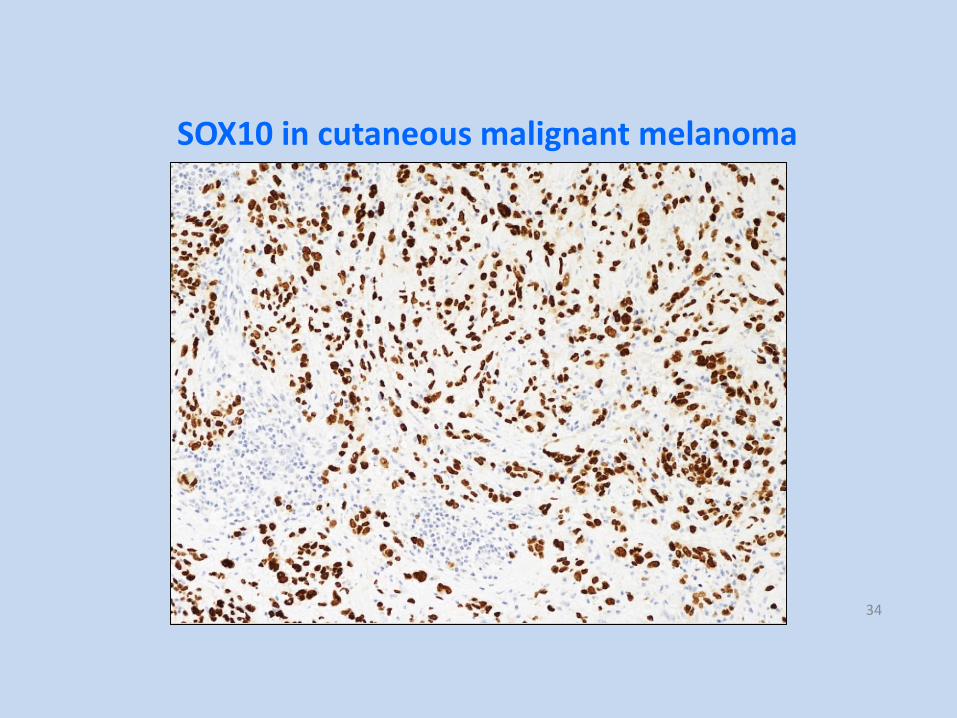
SOX10 in cutaneous malignant melanoma
34

Immunoreactivity S100 vs. SOX10
• S100+ /SOX10-• Adipocytic, chondroid tumors, chordoma,
• Some adenocarcinomas (
• Histiocytic/dendritic cell tumors
• Some sarcomas: synovial sarcoma (15%), Ewing sarcoma (21%), rhabdomyosarcoma (24%), chondrosarcoma (75%), extraskeletalmyxoid chondrosarcoma (45%), ….
• S100-/SOX10-• Most carcinomas and sarcomas, • Mesothelioma, germ cell tumors• Half of MPNST, but more often S100+ than
SOX10+• Neuroblastoma, paraganglioma,
pheochromocytoma - only sustentacularcells in are positive, but tumor cells are negative.
• S100-/SOX10+• Some melanomas
• Some myoepithelial carcinomas
• Few MPNST
• S100+/SOX10+• Melanoma
• Nerve Sheath Tumors
• Majority of myoepithelial carcinomas
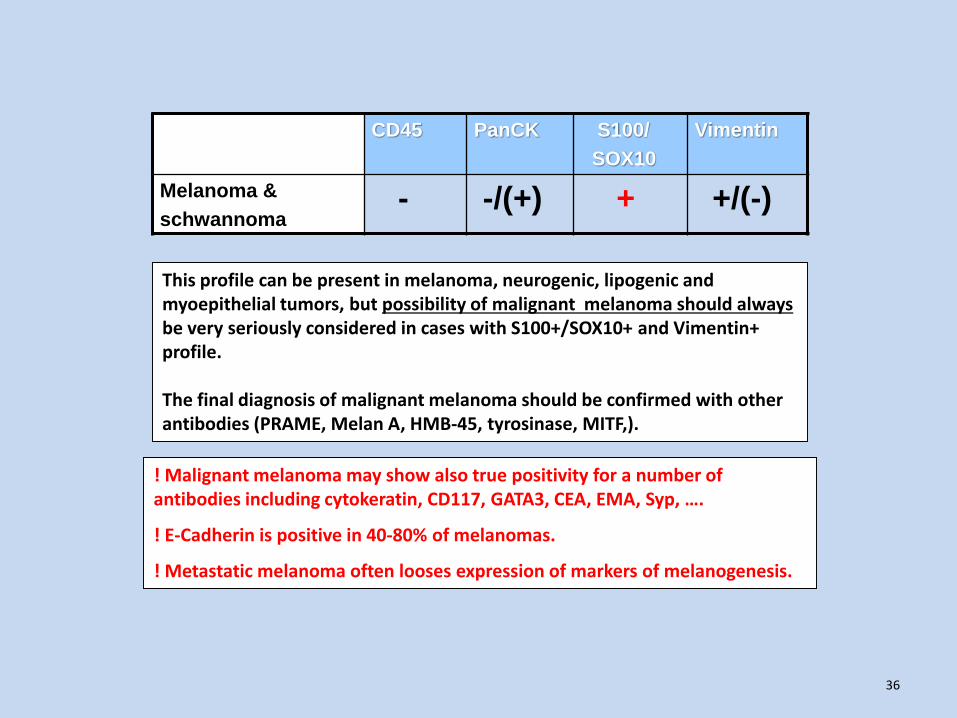
CD45 PanCK S100/
SOX10
Vimentin
Melanoma &
schwannoma- -/(+) + +/(-)
! Malignant melanoma may show also true positivity for a number of antibodies including cytokeratin, CD117, GATA3, CEA, EMA, Syp, ….
! E-Cadherin is positive in 40-80% of melanomas.
! Metastatic melanoma often looses expression of markers of melanogenesis.
This profile can be present in melanoma, neurogenic, lipogenic and myoepithelial tumors, but possibility of malignant melanoma should always be very seriously considered in cases with S100+/SOX10+ and Vimentin+ profile.
The final diagnosis of malignant melanoma should be confirmed with other antibodies (PRAME, Melan A, HMB-45, tyrosinase, MITF,).
36

Aberrant antigen expression in malignant melanoma
PANCK CD45S-100
37

Metastatic CD117+ melanoma in liver
38
CD117
S-100+/ Vimentin+/ PanCK-/ CD45 ND
Melan A
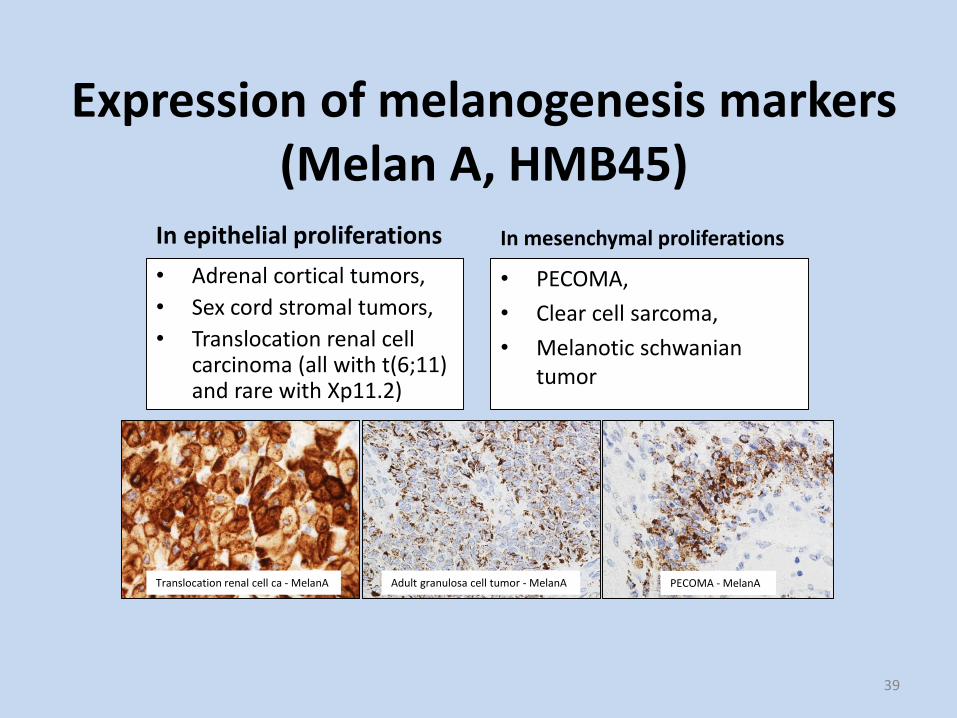
Expression of melanogenesis markers(Melan A, HMB45)
In epithelial proliferations
• Adrenal cortical tumors,
• Sex cord stromal tumors,
• Translocation renal cell carcinoma (all with t(6;11) and rare with Xp11.2)
In mesenchymal proliferations
• PECOMA,
• Clear cell sarcoma,
• Melanotic schwaniantumor
39
PECOMA - MelanAAdult granulosa cell tumor - MelanATranslocation renal cell ca - MelanA
Vimentin
Vimentin – intermediary filament (IF) with structural function in the cytoplasm.
• Present in all cell types during early development, but replaced in later development by other IF types. In mature tissues present in mesenchymal cells, mesothelium, epithelia of mesodermal derivation, thyroid gland, Sertoli and granulosa cell tumours.
• Found in wide variety mesenchymal tumors, many lymphomas, gliomas, carcinomas of some organs and poorly differentiated carcinomas in general.
• Cytoplasmic staining pattern.• More Vimentin positivity is seen in tumors from effusions.
40
The mAbs clones Vim 3B4 and V9 and the rmAb clone SP20 can give optimal staining.

CD45 PanCK S100 Vimentin
Mesenchymal
tumours- -/(+) -/+ +
Mesenchymal tumors which often co-express vimentin and cytokeratin:
• Epithelioid sarcoma (80%)
• DRSCT (>80%)
• Dendritic cell sarcoma (>70%)
• Synovial sarcoma (>60%)
• Chordoma/Parachordoma (40%)
• Angiosarcoma (epitheloid) (>30%)
• Leiomyosarcoma (> 15-30%)
. ….
Mesenchymal tumors which rarely express vimentin:
• Alveolar soft part sarcoma (0-25%)
41

CD45 PanCK S100 Vimentin
Malignant
mesothelioma- + - +/(-)
In addition to malignant mesothelioma should vimentin positive carcinomas and cytokeratin positive sarcomas be included in differential diagnosis.
Final diagnosis of mesothelioma has to be confirmed with the panel of Abs. Positive staining for Calretinin, Podoplanin (D2-40), HBME-1, WT-1, CK5/6 mesotheliomas and negative staining for EPCAM, E-cadherin, CEA, CK20, p63/p40, … is seen in ~ 90% cases.
Negative nuclear BAP1 (50% cases) is a strong argument for mesothelioma.
Diagnostic problems may arise in cases expressing GATA3 (40%), RCC (20%) and in 5-10% PAX8, CD138, CD31, CD30, Synaptophysin/Chromogranin A, SMA …
42
Carcinomas with rare co-expression Cytokeratin & Vimentin
• Breast ductal and lobular carcinoma
• Gastrointestinal carcinoma
• Lung adenocarcinoma and squamous cell carcinoma
• Prostate carcinoma
• Small cell carcinoma
• Endocervical carcinoma
• Ovary mucinous tumors
43
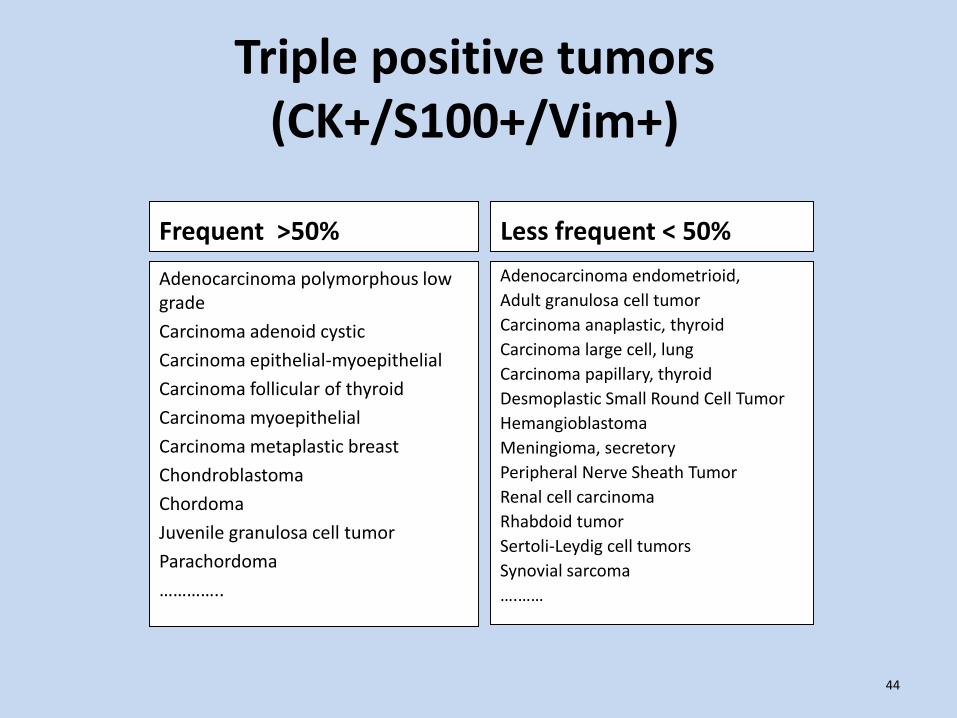
Triple positive tumors (CK+/S100+/Vim+)
Frequent >50%
Adenocarcinoma polymorphous low grade
Carcinoma adenoid cystic
Carcinoma epithelial-myoepithelial
Carcinoma follicular of thyroid
Carcinoma myoepithelial
Carcinoma metaplastic breast
Chondroblastoma
Chordoma
Juvenile granulosa cell tumor
Parachordoma
…………..
Less frequent < 50%
Adenocarcinoma endometrioid,
Adult granulosa cell tumor
Carcinoma anaplastic, thyroid
Carcinoma large cell, lung
Carcinoma papillary, thyroid
Desmoplastic Small Round Cell Tumor
Hemangioblastoma
Meningioma, secretory
Peripheral Nerve Sheath Tumor
Renal cell carcinoma
Rhabdoid tumor
Sertoli-Leydig cell tumors
Synovial sarcoma
….……
44
Case 2
• 38 yrs old man enlarged cervical nodes and mediastinal mass.• No relevant clinical history.• Core biopsy of cervical node.
45

CD45-
S100-
PANCK-
VIM-46
Case 2

OCT4+Podoplanin+
Case 2
47
Dg: Metastatic seminoma in cervical lymph node
SALL4+

CD45 PanCK S100 Vimentin SALL4/
OCT4/
PLAP
Germ cell tumors - +/- -/+ +/- +/(-)
48
SALL4 - transcription factor interacting with NANOG and regulating expression of OCT4 • The first choice marker of germ cell tumours other than choriocarcinoma
• Gives nuclear staining in gonadal and extragonadal germ cell tumors: seminoma, spermatocytic seminoma, embryonal carcinoma, gonadoblastoma, yolk sac tumour, choriocarcinoma (not all cases), majority of immature teratomas, some elements of metastatic and mediastinal mature teratomas. Reported positive also in some cases of ALL and AML.
• Negative in monodermal and majority of mature teratomas
• <7% of clear cell carcinoma may show focal, weak positivity
The mAb clone 6E3 can give optimal results both in concentrated and RTU forms

CD45 PanCK S100 Vimentin SALL4/
OCT4/
PLAP
Germ cell
tumours- +/- -/+ +/- +/(-)
PLAP is positive in 95% of seminomas (spermatocytic seminoma is often negative!) and with decreasing frequency in embryonal carcinomas, yolk sac tumors and choriocarcinomas
Few cases of carcinomas of female genital tract, intestines, lung and breast are also reported PLAP+
OCT4 is positive in classic seminoma and embryonal carcinoma
49
Seminomas are in 10 % CK+ (spermatocytic seminoma is more often CK+), and Vimentin+ (in ~50% of classic seminomas). Embryonal carcinomas are 100% CK+, but Vimentin+ only in 20%.
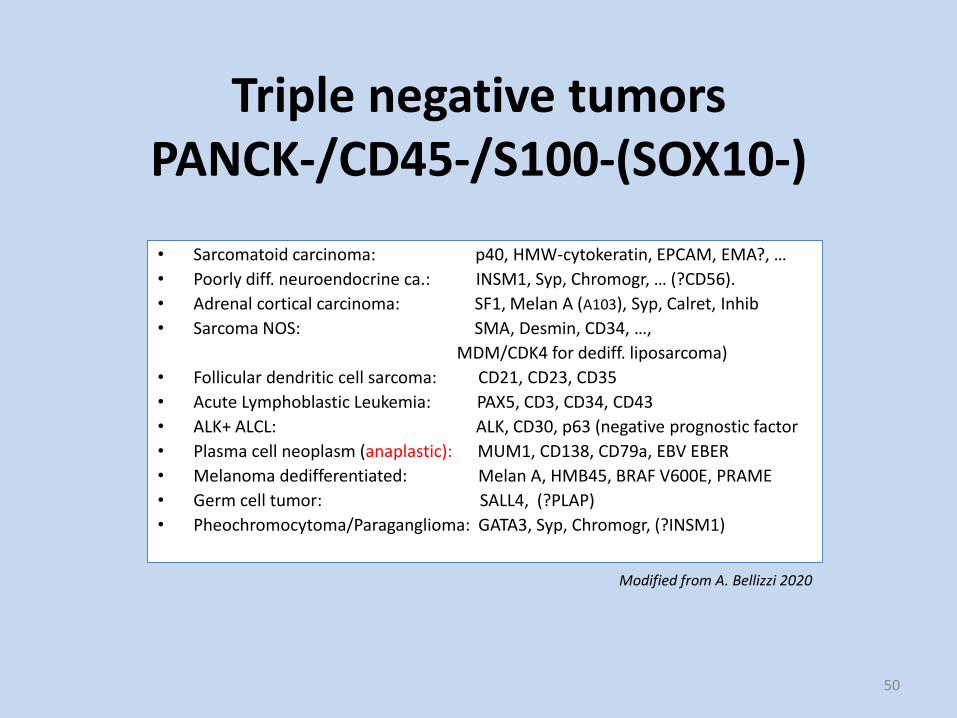
Triple negative tumorsPANCK-/CD45-/S100-(SOX10-)
• Sarcomatoid carcinoma: p40, HMW-cytokeratin, EPCAM, EMA?, …
• Poorly diff. neuroendocrine ca.: INSM1, Syp, Chromogr, … (?CD56).
• Adrenal cortical carcinoma: SF1, Melan A (A103), Syp, Calret, Inhib
• Sarcoma NOS: SMA, Desmin, CD34, …,
MDM/CDK4 for dediff. liposarcoma)
• Follicular dendritic cell sarcoma: CD21, CD23, CD35
• Acute Lymphoblastic Leukemia: PAX5, CD3, CD34, CD43
• ALK+ ALCL: ALK, CD30, p63 (negative prognostic factor
• Plasma cell neoplasm (anaplastic): MUM1, CD138, CD79a, EBV EBER
• Melanoma dedifferentiated: Melan A, HMB45, BRAF V600E, PRAME
• Germ cell tumor: SALL4, (?PLAP)
• Pheochromocytoma/Paraganglioma: GATA3, Syp, Chromogr, (?INSM1)
50
Modified from A. Bellizzi 2020

Part IIApproach to neoplasm with characteristic morphology
(differentiated tumor panel)
51

Advanced panels used to define specific type of tumor or site of origin - various individually designed
combinations of antibodies with narrow spectrum of reactivity including transcription factors (oligospecific
antibodies)
52
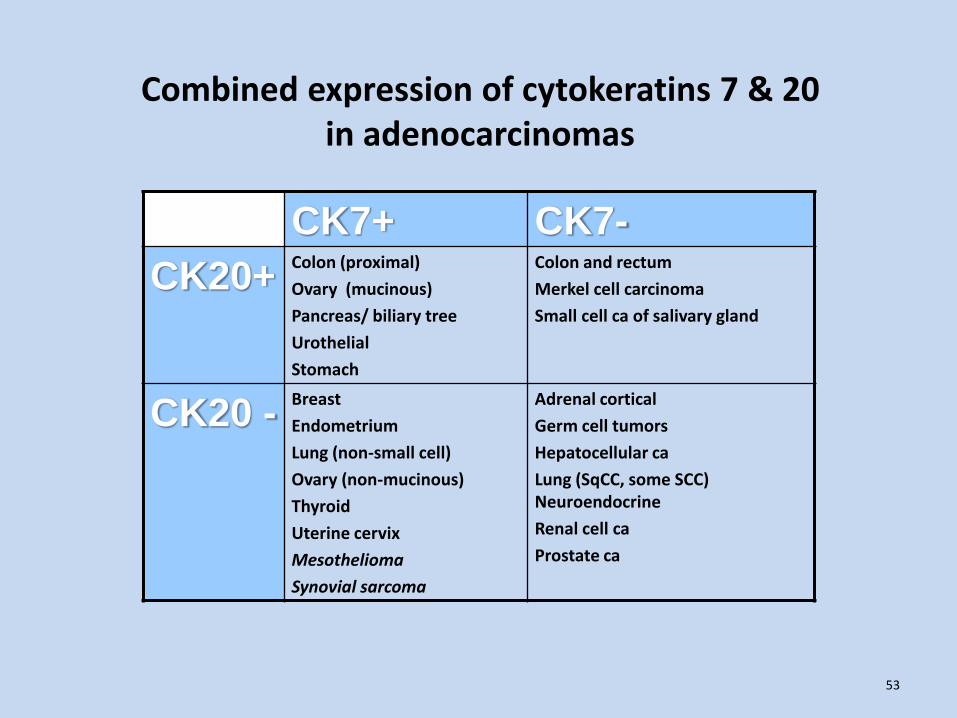
Combined expression of cytokeratins 7 & 20 in adenocarcinomas
CK7+ CK7-
CK20+Colon (proximal)
Ovary (mucinous)
Pancreas/ biliary tree
Urothelial
Stomach
Colon and rectum
Merkel cell carcinoma
Small cell ca of salivary gland
CK20 -Breast
Endometrium
Lung (non-small cell)
Ovary (non-mucinous)
Thyroid
Uterine cervix
Mesothelioma
Synovial sarcoma
Adrenal cortical
Germ cell tumors
Hepatocellular ca
Lung (SqCC, some SCC) Neuroendocrine
Renal cell ca
Prostate ca
53
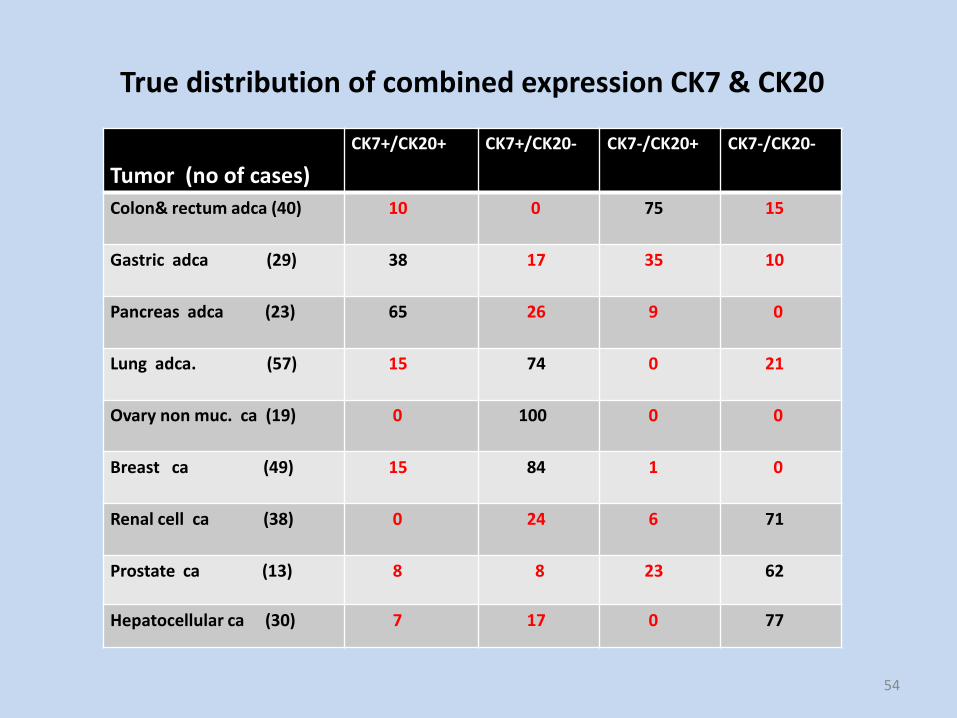
True distribution of combined expression CK7 & CK20
Tumor (no of cases)
CK7+/CK20+ CK7+/CK20- CK7-/CK20+ CK7-/CK20-
Colon& rectum adca (40) 10 0 75 15
Gastric adca (29) 38 17 35 10
Pancreas adca (23) 65 26 9 0
Lung adca. (57) 15 74 0 21
Ovary non muc. ca (19) 0 100 0 0
Breast ca (49) 15 84 1 0
Renal cell ca (38) 0 24 6 71
Prostate ca (13) 8 8 23 62
Hepatocellular ca (30) 7 17 0 77
54
Things that matter are not easy!
David Levithan
Remember about expression of cytokeratins in carcinoma
• Neuroendocrine carcinomas are often CK7-/CK20-
• Squamous cell carcinomas are often CK7-/CK20-
• Lobular breast carcinoma often cross-reacts with CKHMW (clone 34β12)
• Combined positivity for CK5/6 and P63/P40 is characteristic for squamous cell carcinomas, transitional cell carcinomas, basaloid carcinomas, and many myoepithelial tumors.
56

P63 and its isoform P40 (ΔNp63)
Transcription factor, member of p53 gene family, present in several isoforms regulating growth and development of epithelial organs. Mostly used for demonstration of myoepithelial/basal cells, but also in subtyping of carcinoma. P63+ should be interpreted together with the staining for high molecular weight cytokeratin (CK5, CK5/6) when confirming the line of differentiation.
! Cytokeratin 34BE12 can not be reliably used for confirmation of HMWCK since it shows cross-reactivity with low molecular weight CK19.
P40 expression seems to be more restricted to squamous, urothelial and myoepithelial cells. Absolute majority of cases show consistent expression of P40+/P63+ with P63 being slightly more often positive.
Exceptions! Ewing sarcoma: positive for P40 as a rule, but for p63 only in 20%. Polymorphous low grade carcinoma and canalicular adenoma of salivary gland are positive for p63, but negative for p40.
57
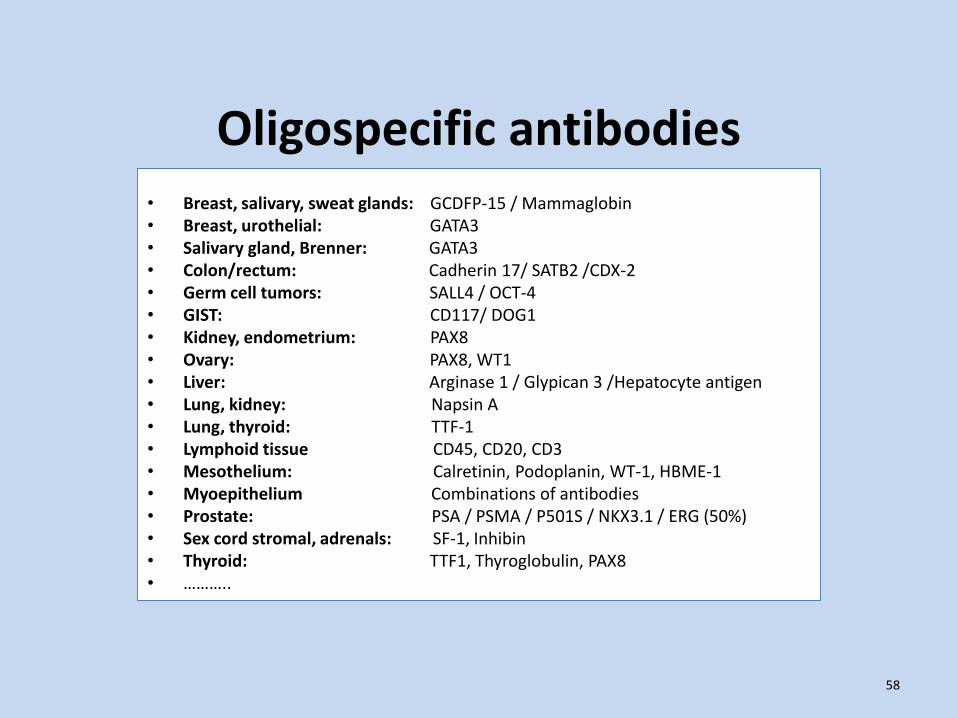
Oligospecific antibodies • Breast, salivary, sweat glands: GCDFP-15 / Mammaglobin • Breast, urothelial: GATA3• Salivary gland, Brenner: GATA3• Colon/rectum: Cadherin 17/ SATB2 /CDX-2 • Germ cell tumors: SALL4 / OCT-4• GIST: CD117/ DOG1• Kidney, endometrium: PAX8• Ovary: PAX8, WT1• Liver: Arginase 1 / Glypican 3 /Hepatocyte antigen • Lung, kidney: Napsin A • Lung, thyroid: TTF-1• Lymphoid tissue CD45, CD20, CD3• Mesothelium: Calretinin, Podoplanin, WT-1, HBME-1• Myoepithelium Combinations of antibodies• Prostate: PSA / PSMA / P501S / NKX3.1 / ERG (50%) • Sex cord stromal, adrenals: SF-1, Inhibin • Thyroid: TTF1, Thyroglobulin, PAX8• ………..
58
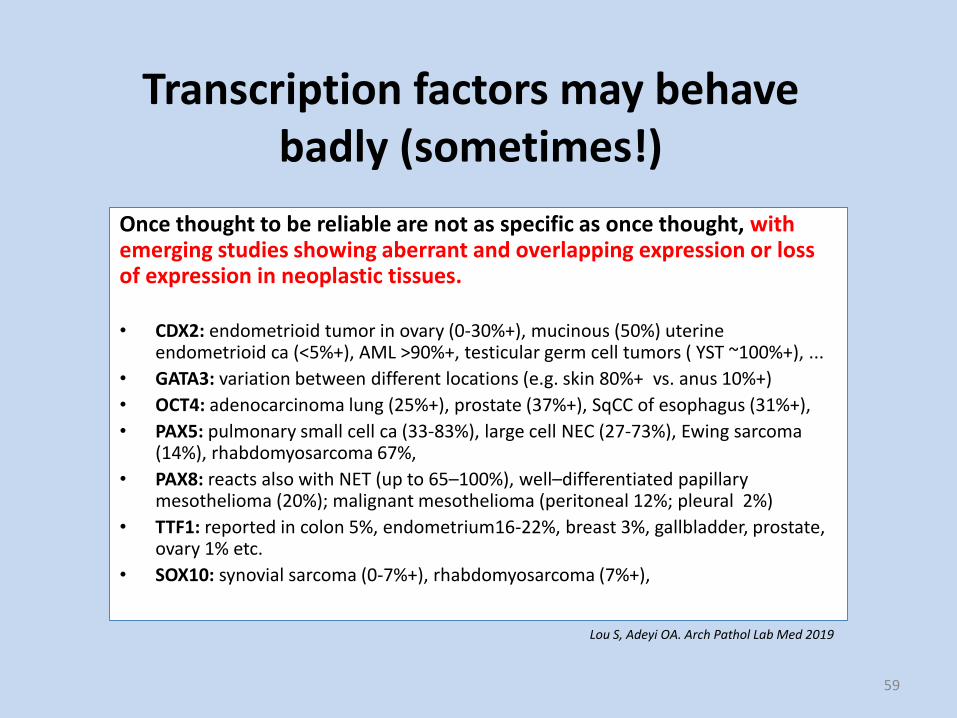
Transcription factors may behave badly (sometimes!)
Once thought to be reliable are not as specific as once thought, with emerging studies showing aberrant and overlapping expression or loss of expression in neoplastic tissues.
• CDX2: endometrioid tumor in ovary (0-30%+), mucinous (50%) uterine endometrioid ca (<5%+), AML >90%+, testicular germ cell tumors ( YST ~100%+), ...
• GATA3: variation between different locations (e.g. skin 80%+ vs. anus 10%+)
• OCT4: adenocarcinoma lung (25%+), prostate (37%+), SqCC of esophagus (31%+),
• PAX5: pulmonary small cell ca (33-83%), large cell NEC (27-73%), Ewing sarcoma (14%), rhabdomyosarcoma 67%,
• PAX8: reacts also with NET (up to 65–100%), well–differentiated papillary mesothelioma (20%); malignant mesothelioma (peritoneal 12%; pleural 2%)
• TTF1: reported in colon 5%, endometrium16-22%, breast 3%, gallbladder, prostate, ovary 1% etc.
• SOX10: synovial sarcoma (0-7%+), rhabdomyosarcoma (7%+),
59
Lou S, Adeyi OA. Arch Pathol Lab Med 2019
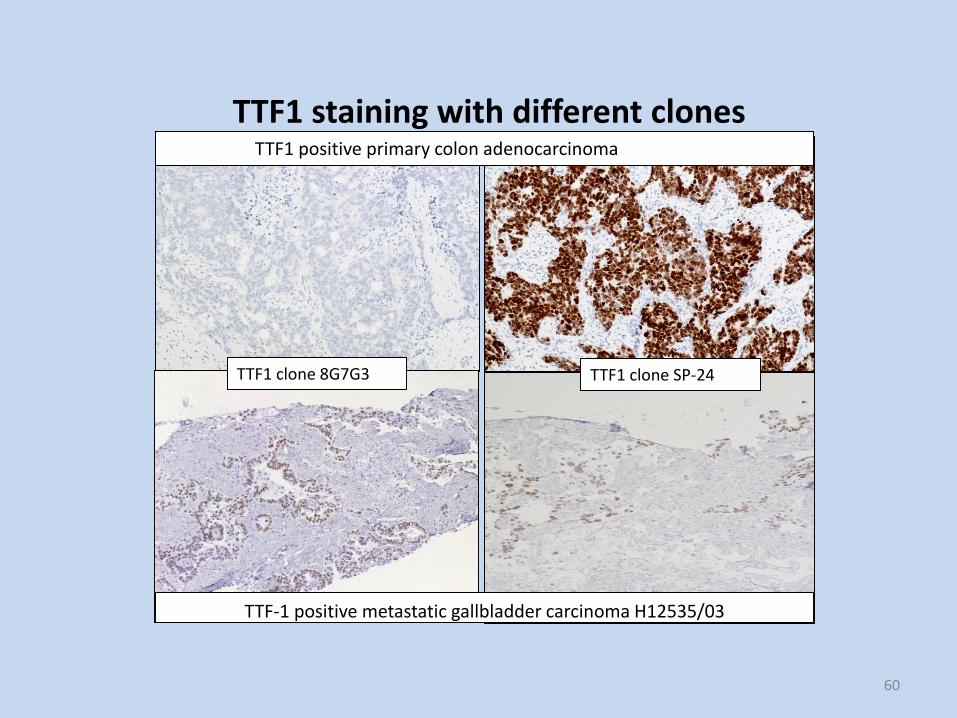
TTF1 staining with different clonesTTF1 positive primary colon adenocarcinoma
TTF1 clone 8G7G3
TTF-1 positive metastatic gallbladder carcinoma H12535/03
TTF1 clone SP-24
60
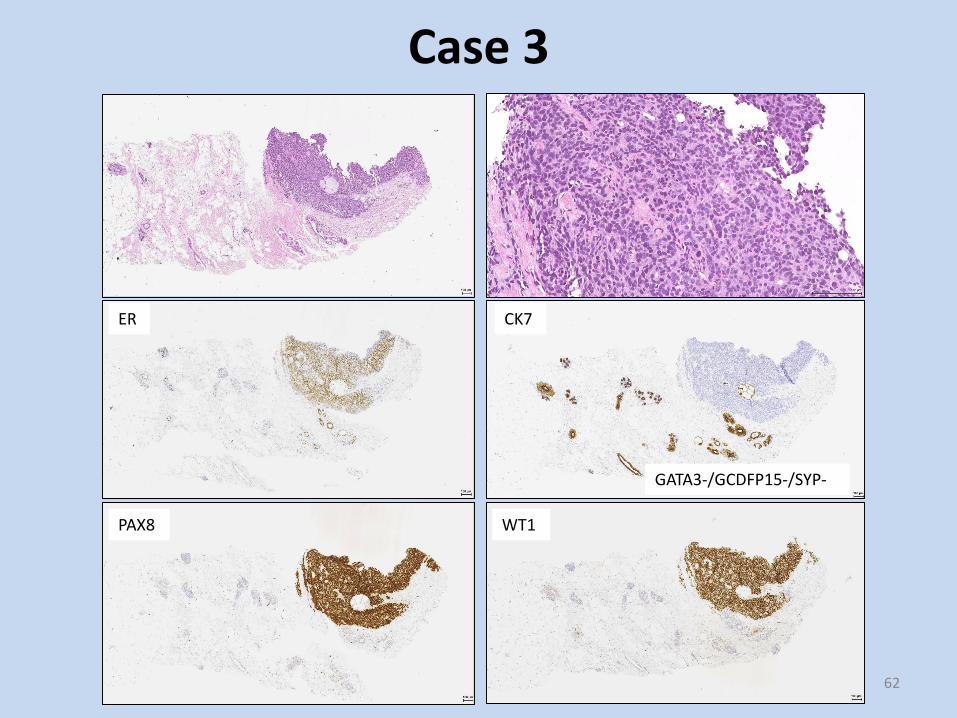
Case 3• Woman 73 years• Palpable tumor in the left breast.• Mammography: suspected for malignancy (4).• 14 years ago operated because of the tumor in
the ovary with diagnosis serous carcinoma. No signs of recurrence.
• Core biopsy from the breast lesion.
61
ER
PAX8 WT1
CK7
GATA3-/GCDFP15-/SYP-
62
Case 3

Case 3
Dg: Metastatic serous carcinoma of the ovary to the breast.
Antibody Ovary serous ca Breast ca NOS
PAX8 95% 0%
WT-1 85% 5%
CA125 80% 15%
GATA3 5% 80%
GCDFP15 2% 50%
Mammaglobin 10% >50%
Estrogen receptors 65% 70%
Her-2 overexpression <20% <15%
CK-7 >95% >90%
63
Case 4
• Man 57 years• No relevant medical history• 19 mm tumor in the left breast• Mammography: malignant (5)• Needle biopsy from the breast tumor
64

65
Case 4
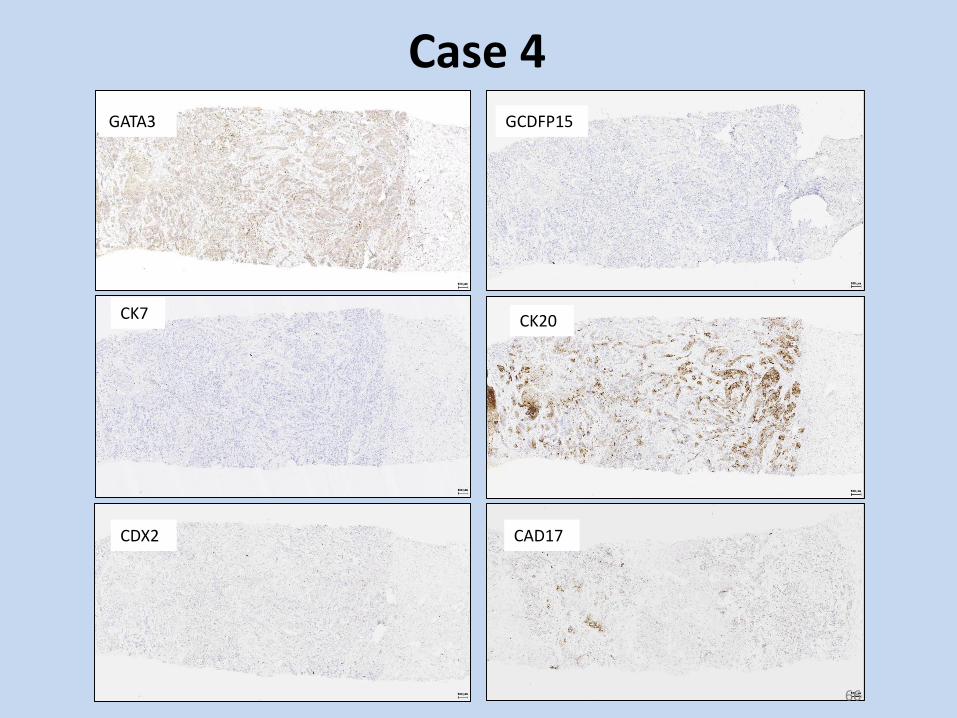
CK7
GATA3
CK20
GCDFP15
CDX2 CAD17
66
Case 4

CK17
Case 4Summary IHC: GATA3- /GCDF15- /S100- /
Vim- /TTF1- / SYP- /SALL4- /CK7- /CK20+ /
CDX2- /CAD17-/+ /CK17+.
SATB2 not available.
Dg: Metastatic adenocarcinoma in the breast -primary location in: pancreas?/biliary tract?/colon? Considered.
CAD17
CK20CK7
Biopsy from ulcerated tumor in colon ascendens
67
CDX2 / Cadherin 17/ SATB2
CAD17: membranous staining of epithelium of colon, rectum, pancreatic ducts, less often epithelium of bile ducts, but not other cell types. Positive in >90% adenocarcinoma colon and rectum, ~80% lymphoepithelioma-like carcinoma of colon and rectum, metanephric adenoma, ~60% adenocarcinoma of urinary bladder, adenocarcinoma of esophagus, ~40% adenocarcinoma of endocervix, stomach, ~15% adenocarcinoma of the pancreas, lung, <10% urothelial and hepatocellular carcinoma, endometrioid adenocarcinoma, adenocarcinoma prostate.
SATB2: involved in regulation of transcription. Nuclear diffuse staining in 80-100% tumors of colon, rectum, appendix and ~20% papillary kidney ca. Focal staining in 10-20% adenocarcinomas of stomach, esophagus, pancreatic/biliary, lung, urothelial carcinoma, prostate and breast. Constant positivity in osteosarcoma.
CDX2: transcription factor for intestinal epithelial cells. Nuclear positivity in adenocarcinomas with intestinal differentiation in different organs: colon, small intestine, appendix but also majority of cases of gastric, pulmonary mucinous, sino-nasal, ovarian mucinous, ampullary, bladder, mucinous urothelial-type carcinoma of prostatic urethra, urachal mucinous, intestinal type cervical adenocarcinoma, pseudomyxoma peritonei, midgut carcinoids). Used in combination with other antibodies incl. CK7 and CK20 to predict origin.
68
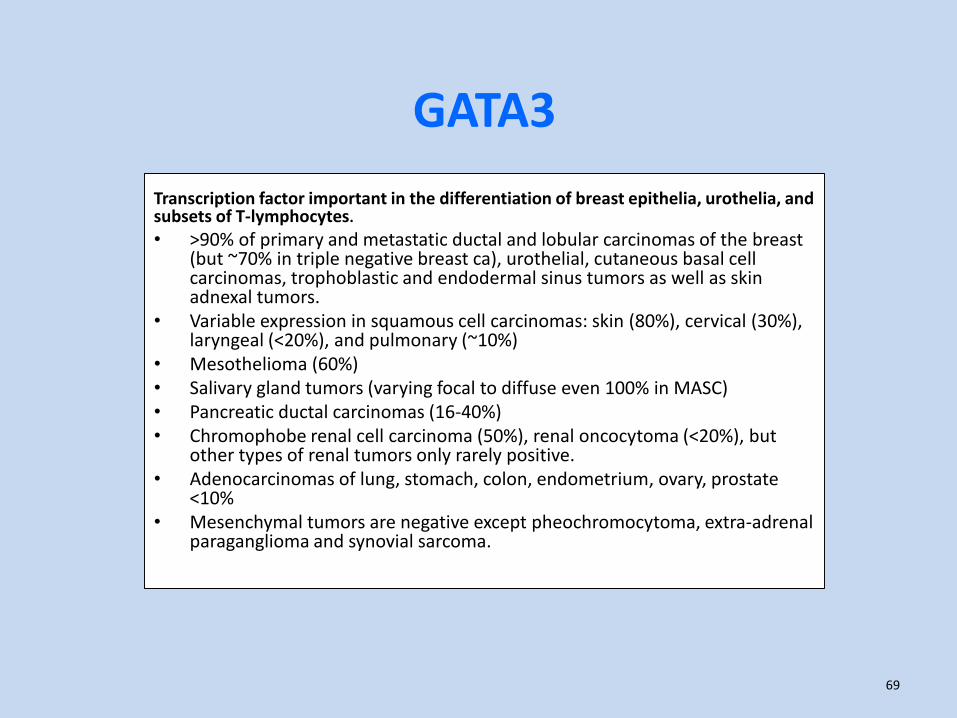
GATA3
Transcription factor important in the differentiation of breast epithelia, urothelia, and subsets of T-lymphocytes.
• >90% of primary and metastatic ductal and lobular carcinomas of the breast (but ~70% in triple negative breast ca), urothelial, cutaneous basal cell carcinomas, trophoblastic and endodermal sinus tumors as well as skin adnexal tumors.
• Variable expression in squamous cell carcinomas: skin (80%), cervical (30%), laryngeal (<20%), and pulmonary (~10%)
• Mesothelioma (60%) • Salivary gland tumors (varying focal to diffuse even 100% in MASC)• Pancreatic ductal carcinomas (16-40%) • Chromophobe renal cell carcinoma (50%), renal oncocytoma (<20%), but
other types of renal tumors only rarely positive.• Adenocarcinomas of lung, stomach, colon, endometrium, ovary, prostate
<10%• Mesenchymal tumors are negative except pheochromocytoma, extra-adrenal
paraganglioma and synovial sarcoma.
69
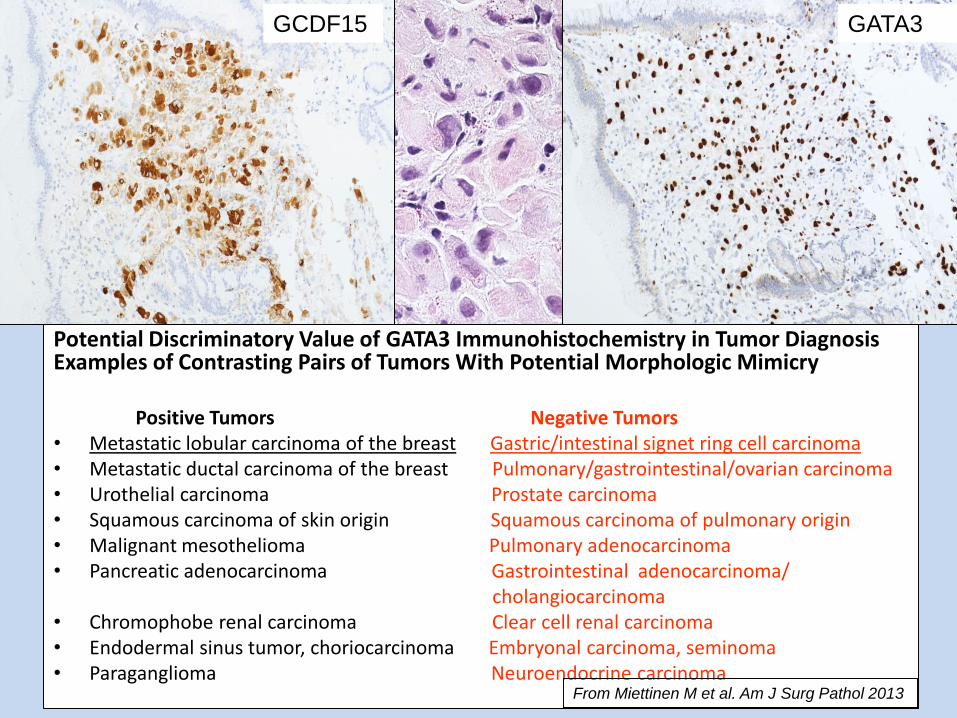
Potential Discriminatory Value of GATA3 Immunohistochemistry in Tumor Diagnosis Examples of Contrasting Pairs of Tumors With Potential Morphologic Mimicry
Positive Tumors Negative Tumors• Metastatic lobular carcinoma of the breast Gastric/intestinal signet ring cell carcinoma• Metastatic ductal carcinoma of the breast Pulmonary/gastrointestinal/ovarian carcinoma• Urothelial carcinoma Prostate carcinoma• Squamous carcinoma of skin origin Squamous carcinoma of pulmonary origin• Malignant mesothelioma Pulmonary adenocarcinoma• Pancreatic adenocarcinoma Gastrointestinal adenocarcinoma/
cholangiocarcinoma• Chromophobe renal carcinoma Clear cell renal carcinoma• Endodermal sinus tumor, choriocarcinoma Embryonal carcinoma, seminoma• Paraganglioma Neuroendocrine carcinoma
From Miettinen M et al. Am J Surg Pathol 2013
GCDF15 GATA3

Panel for metastatic adenocarcinoma of the pancreas
DPC4 (SMAD4) - deleted in ~50% pancreatic ca, but also other cancers in the region -negative staining supports pancreatobiliary origin.
MUC1+/CK17+ positive markers for pancreatic ductal carcinomas, the ampullary carcinoma of pancreatobiliary origin and cholangiocarcinomas with positive predictive values of 76%, 83% and 58% respectively.
MUC2+/CDX2+ positive markers for the intestinal-type adenocarcinoma of duodenal papillary origin with a positive predictive value of 82%.
GATA3+ more common in pancreas adca than other gastrointestinal locations including cholangiocellular adenocarcinoma.
CK19 alone should not be used to confirm pancreatic origin. It is not enough specific -reported in almost 100% of pancreatic ductal carcinoma and at least 150 other tumors including adenocarcinomas, squamous cell carcinomas, sarcomas.
Cytokeratin 17 - basal type, complex epithelia, squamous and basaloid differentiation. Positive in ~80% of ductal pancreatic adenocarcinoma and ~60% of cholangiocellular ca, but not in gastric or colorectal carcinomas. Positive also in squamous cell ca, transitional cell ca, epithelial-myoepithelial ca.
71
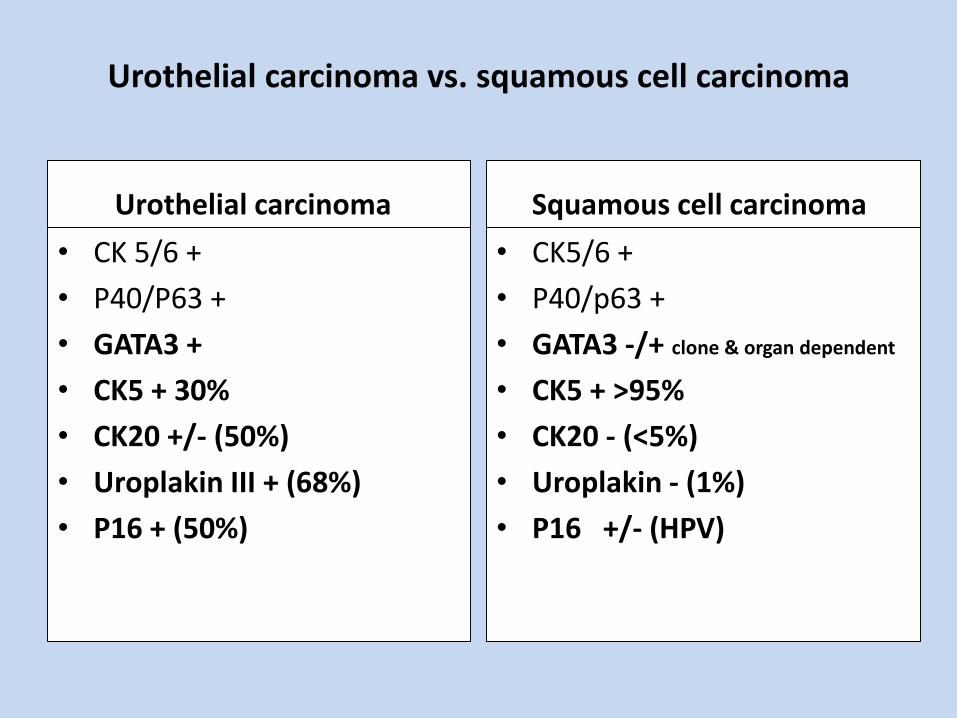
Urothelial carcinoma vs. squamous cell carcinoma
Urothelial carcinoma
• CK 5/6 +
• P40/P63 +
• GATA3 +
• CK5 + 30%
• CK20 +/- (50%)
• Uroplakin III + (68%)
• P16 + (50%)
Squamous cell carcinoma
• CK5/6 +
• P40/p63 +
• GATA3 -/+ clone & organ dependent
• CK5 + >95%
• CK20 - (<5%)
• Uroplakin - (1%)
• P16 +/- (HPV)

INSM1Emerging neuroendocrine marker
• Insulinoma-associated 1 (INSM1) - a protein containing both a zincfinger DNA-binding domain and a putative prohormone domain.
• Most sensitive and highly specific marker of neuroendocrinedifferentiation in normal and neoplastic cells so far.
• !Parathyroid adenoma and adrenal cortical carcinoma are consistently negative for INSM1.
73

PRAMEEmerging melanoma marker
PReferentially expressed Antigen in MElanoma - recognized by cytolytic T lymphocytes.
Inhibits retinoic acid-induced differentiation, growth arrest, and apoptosis through interaction with the EZH2 polycomb group proteins
It is not expressed in normal tissues, except testis, ovary, placenta, adrenals, and endometrium.
Nuclear staining positive in ~95% malignant melanoma and ~10% melanocytic nevi.
More sensitive than Melan A and HMB45 especially in metastatic lesions.
74

Mimics of metastatic carcinoma • Hemangioblastoma, glioblastoma and meningioma with epithelial metaplasia, • Choroid plexus carcinomas, • Primary neuroendocrine carcinomas in unusual locations,• Special forms of sinonasal and salivary glandular adenocarcinoma, clear-cell thyroid
carcinomas, • Unusual microscopic subtypes of pulmonary adenocarcinoma, epithelioid
myomelanocytomas (“sugar tumors”), mesotheliomas,• Primary thymic carcinomas, • Endodermal choristomas of the interatrial myocardium, • Peripheral cholangiocarcinoma,• Adrenocortical carcinoma, • Adenocarcinomas of the urinary bladder, mucinous and “rhabdoid”• Tumors of the ovaries, • Adenocarcinomas of rete testis, • Interdigitating dendritic-cell sarcoma of lymph nodes, • Some sweat gland carcinomas, • Cutaneous Merkel cell carcinoma, • Primary dermal and subcutaneous melanoma,• Mucosal and visceral melanomas, • Epithelioid sarcoma, clear-cell sarcoma, • Adamantinoma of long bones.
75Modified from Mark R. Wick 2018
Molecular profiling of CUP An adjunct to immunohistochemistry or a competitor?
• RT-PCR based commercially available tests• Promising results from preliminary studies• Expected value for choice of precision therapy (NGS)• Prospective validating studies going on
76

Molecular tests in CUP• Molecular methods applied to tumor tissue are able to predict the
Tissue Of Origin, using gene expression profiling, gene microarrays, microRNA and DNA methylation analysis.
• Several studies indicate that gene expression assays have high diagnostic accuracy for predicting tissue of origin in cancers of unknown primary.
• The impact of these assays on patient management and patient survival remains uncertain and there is insufficient data to support its routine use at the moment. Further studies are going on.
Medical Policy Statement on Molecular Profiling for Cancers of Unknown Primary Origin AHS- M2065 – updated 9/8/20

Immunohistochemistry is a complex multistep diagnostic laboratory procedure, where each step is important for final results and interpretation.
Be aware of possible pitfalls and pay attention to correct interpretation.
Apply individual approach to each case considering step by step procedure.
The interpretation of IHC should always correlate to morphology and clinical data.
CUP summary
78
Thank you for your attention!
79


















