University of Zurich Zurich Open ... fileP; Marincek, B; Alkadhi, H; Kaufmann, P A (2008)....
12
University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich http://www.zora.uzh.ch Year: 2008 Comparison of diagnostic accuracy of 64-slice computed tomography coronary angiography in patients with low, intermediate, and high cardiovascular risk Husmann, L; Schepis, T; Scheffel, H; Gaemperli, O; Leschka, S; Valenta, I; Koepfli, P; Desbiolles, L; Stolzmann, P; Marincek, B; Alkadhi, H; Kaufmann, P A Husmann, L; Schepis, T; Scheffel, H; Gaemperli, O; Leschka, S; Valenta, I; Koepfli, P; Desbiolles, L; Stolzmann, P; Marincek, B; Alkadhi, H; Kaufmann, P A (2008). Comparison of diagnostic accuracy of 64-slice computed tomography coronary angiography in patients with low, intermediate, and high cardiovascular risk. Academic Radiology, 15(4):452-461. Postprint available at: http://www.zora.uzh.ch Posted at the Zurich Open Repository and Archive, University of Zurich. http://www.zora.uzh.ch Originally published at: Academic Radiology 2008, 15(4):452-461.
Transcript of University of Zurich Zurich Open ... fileP; Marincek, B; Alkadhi, H; Kaufmann, P A (2008)....

University of ZurichZurich Open Repository and Archive
Winterthurerstr. 190
CH-8057 Zurich
http://www.zora.uzh.ch
Year: 2008
Comparison of diagnostic accuracy of 64-slice computedtomography coronary angiography in patients with low,
intermediate, and high cardiovascular risk
Husmann, L; Schepis, T; Scheffel, H; Gaemperli, O; Leschka, S; Valenta, I; Koepfli,P; Desbiolles, L; Stolzmann, P; Marincek, B; Alkadhi, H; Kaufmann, P A
Husmann, L; Schepis, T; Scheffel, H; Gaemperli, O; Leschka, S; Valenta, I; Koepfli, P; Desbiolles, L; Stolzmann,P; Marincek, B; Alkadhi, H; Kaufmann, P A (2008). Comparison of diagnostic accuracy of 64-slice computedtomography coronary angiography in patients with low, intermediate, and high cardiovascular risk. AcademicRadiology, 15(4):452-461.Postprint available at:http://www.zora.uzh.ch
Posted at the Zurich Open Repository and Archive, University of Zurich.http://www.zora.uzh.ch
Originally published at:Academic Radiology 2008, 15(4):452-461.
Husmann, L; Schepis, T; Scheffel, H; Gaemperli, O; Leschka, S; Valenta, I; Koepfli, P; Desbiolles, L; Stolzmann,P; Marincek, B; Alkadhi, H; Kaufmann, P A (2008). Comparison of diagnostic accuracy of 64-slice computedtomography coronary angiography in patients with low, intermediate, and high cardiovascular risk. AcademicRadiology, 15(4):452-461.Postprint available at:http://www.zora.uzh.ch
Posted at the Zurich Open Repository and Archive, University of Zurich.http://www.zora.uzh.ch
Originally published at:Academic Radiology 2008, 15(4):452-461.

Comparison of diagnostic accuracy of 64-slice computedtomography coronary angiography in patients with low,
intermediate, and high cardiovascular risk
Abstract
RATIONALE AND OBJECTIVES: The aim of this study was to compare the diagnostic accuracy of64-slice computed tomographic coronary angiography (CTCA) in groups of patients with low,intermediate, and high risk for coronary artery disease (CAD) events. MATERIALS AND METHODS:The institutional review board approved this study; written informed consent was obtained from allpatients. Eighty-eight consecutive patients with suspected CAD (40 women; mean age, 64.3 +/- 9.4years; range, 39-82) underwent CTCA, calcium scoring, and invasive coronary angiography and weregrouped according to their Framingham 10-year risk for hard coronary events into low (<10%),intermediate (10%-20%), and high (>20%) risk categories. Significant stenoses (luminal diameternarrowing > or =50%) were assessed on an intention-to-diagnose-basis; no coronary segment wasexcluded and nonevaluative segments were rated false positive. To determine differences betweengroups, Kruskal-Wallis tests were performed for individually determined values of diagnosticperformance. RESULTS: Per-patient sensitivity, specificity, negative predictive, and positive predictivevalues were 90.0%, 79.2%, 95.0%, and 64.3%, respectively, with low (n = 34), 87.5%, 92.3%, 85.7%,and 93.3%, respectively, with intermediate (n = 29), and 100%, 75.0%, 100%, and 89.5%, respectively,with high risk (n = 25), with a trend toward higher positive predictive value (P = .07). Per-segmentnegative predictive value was lower with high pretest probability (P < .01). Mean calcium-score unitswere 90, 220, and 312 (P = .23), and the prevalence of CAD was 29.4%, 55.2%, and 68.0% (P < .01)with low, intermediate, and high risk. CONCLUSION: Sensitivity and specificity of CTCA are notinfluenced by the prevalence of CAD, whereas the negative predictive value is lower and the positivepredictive value tends to be higher in patients with a high prevalence of CAD.

Original Investigations
Comparison of Diagnostic Accuracy of 64-SliceComputed Tomography Coronary Angiography
in Patients with Low, Intermediate, and HighCardiovascular Risk1
Lars Husmann, MD, Tiziano Schepis, MD, Hans Scheffel, MD, Oliver Gaemperli, MD, Sebastian Leschka, MDInes Valenta, MD, Pascal Koepfli, MD, Lotus Desbiolles, MD, Paul Stolzmann, MD, Borut Marincek, MD
Hatem Alkadhi, MD, Philipp A. Kaufmann, MD
Rationale and Objectives. The aim of this study was to compare the diagnostic accuracy of 64-slice computed tomo-graphic coronary angiography (CTCA) in groups of patients with low, intermediate, and high risk for coronary artery dis-ease (CAD) events.
Materials and Methods. The institutional review board approved this study; written informed consent was obtained from allpatients. Eighty-eight consecutive patients with suspected CAD (40 women; mean age, 64.3 � 9.4 years; range, 39–82) under-went CTCA, calcium scoring, and invasive coronary angiography and were grouped according to their Framingham 10-year riskfor hard coronary events into low (�10%), intermediate (10%–20%), and high (�20%) risk categories. Significant steno-ses (luminal diameter narrowing �50%) were assessed on an intention-to-diagnose-basis; no coronary segment was ex-cluded and nonevaluative segments were rated false positive. To determine differences between groups, Kruskal-Wallistests were performed for individually determined values of diagnostic performance.
Results. Per-patient sensitivity, specificity, negative predictive, and positive predictive values were 90.0%, 79.2%, 95.0%,and 64.3%, respectively, with low (n � 34), 87.5%, 92.3%, 85.7%, and 93.3%, respecitively, with intermediate (n � 29),and 100%, 75.0%, 100%, and 89.5%, respectively, with high risk (n � 25), with a trend toward higher positive predictivevalue (P � .07). Per-segment negative predictive value was lower with high pretest probability (P � .01). Mean calcium-score units were 90, 220, and 312 (P � .23), and the prevalence of CAD was 29.4%, 55.2%, and 68.0% (P � .01) withlow, intermediate, and high risk.
Conclusion. Sensitivity and specificity of CTCA are not influenced by the prevalence of CAD, whereas the negative pre-dictive value is lower and the positive predictive value tends to be higher in patients with a high prevalence of CAD.
Key Words. Framingham; coronary risk stratification; prevalence; diagnostic accuracy; coronary angiography; 64-slicecomputed tomography.© AUR, 2008
Acad Radiol 2008; 15:452–461
1 From the Institute of Nuclear Cardiology (L.H., T.S., O.G., I.V., P.A.K.), Institute of Diagnostic Radiology (L.H., H.S., S.L., L.D., P.S., B.M., H.A.), Cardiovas-cular Center (P.K., O.G., P.A.K.) and University Hospital Zurich, Raemistrasse 100, and Center for Integrative Human Physiology (P.A.K.), University of Zurich,CH-8091 Zurich, Switzerland. Received October 18, 2007; accepted December 10, 2007. Dr. Kaufmann was supported by a grant from the Swiss NationalScience Foundation (SNSF professorship grant PP00A-114706). Drs Alkadhi, Scheffel, Stolzmann, and Desbiolles were supported by the National Center ofCompetence in Research, Computer Aided and Image Guided Medical Interventions (NCCR CO-ME) of the Swiss National Science Foundation. Addresscorrespondence to: P.A.K. e-mail: [email protected]
©
AUR, 2008doi:10.1016/j.acra.2007.12.008452

Academic Radiology, Vol 15, No 4, April 2008 ACCURACY OF CT CORONARY ANGIOGRAPHY
Sixty-four–slice computed tomography (CT) has beenshown to be a reliable noninvasive tool to document orrule out significant coronary artery lesions (1–10). In par-ticular, the high negative predictive value (NPV) of CTcoronary angiography (CTCA), demonstrated in all stud-ies (1–10), has been suggested to obviate the need forinvasive coronary angiography (ICA) in patients whosesymptoms or abnormal stress test results require rulingout the presence of coronary artery disease (CAD) (11).Although some guidelines (12) allow consideration ofCTCA in patients with a low pretest probability, othershave suggested CTCA as an appropriate tool in patientswith an intermediate risk for CAD (11,13). In high pretestpopulations, CTCA is not considered a useful tool, be-cause the likelihood for the necessity of a subsequent ICAis high.
However, most studies that determined the diagnosticaccuracy of 64-slice CTCA have included patients withknown CAD (1,2,6–8) and patient cohorts with highprevalences of CAD (56%–85%) (1–3,5,6,8,10), not tak-ing into account the pretest probability or the risk to de-velop coronary events in those patients with suspectedCAD (1–10).
Therefore, the purpose of our study was to determineand compare the diagnostic accuracy of 64-slice CTCA ingroups of patients with low, intermediate, and high riskfor CAD events.
MATERIALS AND METHODS
PatientsEighty-eight consecutive patients suspected of having
CAD (40 women and 48 men; mean age, 64.3 � 9.4years; range, 39–82) were scheduled for CTCA and ICA,provided there were no reasons for exclusion, such asallergy to iodinated contrast agent, renal insufficiency(creatinine levels �150 �mol/L), nonsinus rhythm, orhemodynamic instability. The patients were referred be-cause of dyspnea (n � 22), typical angina pectoris (n �31), or atypical chest pain (n � 19), or to preoperativelyrule out CAD (n � 16). Framingham risk scoring wasassessed, using the factors of age, gender, low- and high-density lipoprotein cholesterol levels, systolic and dia-stolic blood pressure, diabetes, and nicotine abuse. The 10-year risk for hard coronary heart disease events was deter-mined as described in the National Cholesterol EducationProgram’s Adult Treatment Panel III report (14), and pa-
tients were categorized into groups with low (10-year risk�10%), intermediate (10-year risk 10%–19%), and high(10-year risk �20%) risk for CAD events.
The study protocol was approved by the local ethicscommittee, and written informed consent was obtainedfrom all patients.
CT Data Acquisition and PostprocessingAll CT examinations were performed on a 64-slice CT
scanner (Somatom Sensation 64; Siemens Medical Solu-tions, Forchheim, Germany). For coronary calcium scor-ing, a nonenhanced, retrospectively electrocardiographi-cally-gated scan was performed using the following scan-ning parameters: detector collimation of 32 � 0.6 mm,slice acquisition of 64 � 0.6 mm using a z-flying focalspot, pitch of 0.2, gantry rotation time of 330 msec, tubevoltage of 120 kV, and an effective tube-current timeproduct of 60 mA. Intravenous metoprolol (5 to 20 mg,Beloc; AstraZeneca, London, UK) was administered priorto the CTCA examination to achieve a target heart rate�70 beats/min, if necessary. In the presence of contrain-dications for �-adrenoceptor antagonists or when themaximum dose did not lower the heart rate satisfactorily,the scan was performed even at higher heart rates. In ad-dition, all patients received a single dose of 2.5 mgisosorbiddinitrate sublingual (Isoket; Schwarz Pharma,Monheim, Germany) 2 minutes before the scan. TheCTCA examination was started by continuously injectinga bolus of 80 ml of iodixanol (Visipaque 320, 320 mg/ml;GE Healthcare, Buckinghamshire, UK) followed by 30 mlof saline solution into an antecubital vein via an 18-gaugecatheter (injection rate, 5 ml/sec). Bolus tracking was per-formed with a region of interest placed into the ascendingaorta, and image acquisition was automatically started 5seconds after the signal density reached a predefinedthreshold of 100 Hounsfield units. Scanning was per-formed from 1 cm below the level of the tracheal bifurca-tion to the diaphragm in a craniocaudal direction usingthe following scanning parameters: detector collimation32 � 0.6 mm, slice collimation 64 � 0.6 mm using az-flying focal spot, gantry rotation time of 330 msec,pitch of 0.2, tube potential of 120 kV, and tube-currenttime product of 650 effective mA. The electrocardiogramwas digitally recorded during data acquisition and wasstored with the unprocessed CT dataset.
CT Image Reconstruction and AnalysisSynchronized to the electrocardiographic data, CT data
sets were retrospectively reconstructed throughout the
entire cardiac cycle in 5% steps of the RR interval. When453

HUSMANN ET AL Academic Radiology, Vol 15, No 4, April 2008
automatic positioning of the R-wave indicators by thesoftware failed, manual repositioning of the indicatorswas performed. In case of irregular heart rates, the tempo-ral variability in the reconstruction phase was compen-sated by manual electrocardiographic editing. In case ofpremature heartbeats, the temporal window of the follow-ing heartbeat was deleted, and the next diastolic windowwas filled with one to three temporal windows to avoiddata gaps. The adaptive cardiovolume approach was usedfor image reconstruction, which automatically switchesbetween one- and two-segment reconstruction dependingon the patient’s heart rate (15). Reconstruction of axialimages was performed with a slice thickness of 1.0 mmand an increment of 0.8 mm. All images were recon-structed using a medium-soft and a sharp tissue convolu-tion kernel (B30f and B46f) and were transferred to anexternal workstation (Leonardo; Siemens Medical Solu-tions).
For analysis of CTCA data, coronary arteries were seg-mented as suggested by the American Heart Association(16): The right coronary artery was defined to includesegments 1–4, the left main artery and the left anteriordescending artery to include segments 5–10, and the leftcircumflex artery to include segments 11–15. The inter-medial artery was designated as segment 16, if present.All segments with a diameter of at least 1.5 mm at theirorigin were included.
One reader (L.H.) semiquantitatively assessed the over-all image quality in the best reconstruction interval on a5-point scale, based on a previously published score (17)(1, no artifacts; 2, mild artifacts; 3, moderate artifacts; 4,severe artifacts; 5, nonevaluative) and determined the re-construction interval with the best image quality. Twoindependent readers (L.H., H.A.) evaluated and classifiedcoronary arteries, using axial source images, multiplanarreformations, and thin-slab maximum-intensity projectionson a per-segment basis. Both readers assessed all coro-nary artery segments for the presence of significant steno-ses, defined as narrowing of the coronary luminal diame-ter �50%. For any disagreement in data analysis betweenthe two observers, consensus agreement was achieved.Diagnostic accuracy of CTCA was determined on an “in-tention-to-diagnose” basis; no coronary segment was ex-cluded, and nonevaluative segments were rated as falsepositive.
Invasive Coronary AngiographyICA was performed according to standard techniques,
and multiple views were stored on a CD-ROM. The an-
454
giograms were evaluated by two experienced observer inconsensus (O.G., P.K.), blinded to the results fromCTCA. Coronary artery segments were defined as previ-ously mentioned (16), and analysis was performed in allvessels with a luminal diameter of at least 1.5 mm, ex-cluding those vessels distal to complete occlusions. Eachvessel segment was scored as being significantly stenosed,defined as a diameter reduction of �50%.
Statistical AnalysisQuantitative variables were expressed as mean � stan-
dard deviation, and categorical variables as frequencies,median (25th and 75th percentiles), or percentages. SPSSsoftware (version 12.0.1; SPSS, Chicago, IL) was usedfor statistical testing (L.H.). Sensitivity, specificity, posi-tive predictive value (PPV), NPV, and accuracy in theidentification of stenoses were assessed on a per-segment,per-vessel, and per-patient basis using cross tables. ICAwas considered the standard of reference.
Differences between the three groups regarding diag-nostic performance were tested for significance using �2
tests for comparison of cross tables. For further compari-son, univariate analyses of variances (ANOVAs) wereperformed for the following variables: age, body massindex, low- and high-density lipoprotein, diastolic andsystolic blood pressure, heart rate, and heart rate variabil-ity. Kruskal-Wallis tests were performed for calciumscore, Framingham risk score and 10%-year risk, imagequality, and best reconstruction interval. and �2-tests wereperformed for gender, diabetes, nicotine abuse, and preva-lence of CAD. A P-value of � .05 was considered statis-tically signficant. Interobserver agreements for assessmentof significant coronary artery (patient, vessel, and segmentbased) stenoses were interpreted according to the guide-lines of Landis and Koch (18).
RESULTS
CTCA and ICA were successfully performed within 7 �15 days in all 88 patients. In 13 patients (14.8%), CTCAwas performed prior to ICA. Forty-one patients (47%) wereon oral �-adrenoceptor antagonist medication as part oftheir baseline medication. Additional intravenous meto-prolol was administered in seven patients prior to the CTexamination. Baseline characteristics of the entire studygroup and the three subgroups are presented in Table 1.
A total of 351 vessels (1 missing because of an ana-
tomic variant) and 1191 coronary artery segments with a
Table 1Patient Demographics
All Patients Low Risk for CAD EventsIntermediate Risk for
CAD Events High Risk for CAD EventsSignificance
P-Value
No. of patients 88 34 29 25Female/male (n) 40/48 24/10 10/19 6/19 �2: �.001Diabetes (n) 16 1 5 10 �2: �.001Nicotine abuse (n) 36 6 17 13 �2: �.01Age (y) 64.3 � 9.4 (39–82) 62.7 � 11.3 (39–81) 64.4 � 7.8 (47–79) 66.5 � 7.9 (49–82) ANOVA: .30BMI (kg/m2) 23.2 � 3.9 (13.3–35.8) 22.2 � 4.7 (13.3–35.8) 23.3 � 2.9 (18.2–29.7) 24.2 � 3.9 (18.7–34.0) ANOVA: .17LDL (mmol/L) 2.9 � 1.1 (1.4–7.4) 2.4 � 0.8 (1.5–4.5) 2.9 � 0.9 (1.4–5.0) 3.7 � 1.4 (1.5–7.4) ANOVA: .001HDL (mmol/L) 1.4 � 0.4 (0.3–2.4) 1.7 � 0.4 (0.7–2.4) 1.3 � 0.3 (0.8–2.0) 1.2 � 0.3 (0.3–1.8) ANOVA: �.001Diastolic BP (mm Hg) 79 � 12 (45–110) 77 � 10 (55–96) 77 � 12 (45–99) 83 � 12 (60–110) ANOVA: .16Systolic BP (mm Hg) 135 � 20 (70–190) 129 � 18 (70–160) 132 � 18 (100–167) 147 � 20 (120–190) ANOVA: �.01Framingham risk score 7 (6, 17) 6 (3, 9) 7 (6, 12) 11 (9, 17) K-W: �.00110-Year risk (%) 11 (7, 40) 6 (5, 9) 11 (11, 18) 24 (22, 40) K-W: �.001At CTCA scanning
HR (beats/min) 63.0 � 9.2 (46–90) 63.2 � 8.6 (48–76) 62.2 � 9.0 (46–78) 63.8 � 10.4 (47–90) ANOVA: 1.0HR variability (beats/min) 4.5 � 4.4 (0.5–22.2) 4.9 � 4.7 (0.8–22.2) 3.9 � 4.1 (0.8–16.1) 4.6 � 4.7 (0.5–18.9) ANOVA: 1.0Calcium score 173 (5, 635) 90 (1,589) 220 (37, 635) 312 (95, 1196) K-W: .23Overall image quality
score 1, 2, 3, 4, 52 (1, 4)
33, 30, 17, 8, 02 (1, 4)
15, 11, 6, 2, 02 (1, 4)
13, 7, 6, 3, 02 (2, 4)
5, 12, 5, 3, 0K-W: .25
Best recon. interval30%, 35%, 40%,55%, 60%, 65%, 70%
60 (60, 70)5, 7, 3, 3, 42, 16, 8
60 (60, 70)2, 3, 0, 1, 19, 5, 4
60 (60, 70)1, 2, 0, 2, 12, 8, 3
60 (40, 70)2, 2, 3, 0, 11, 3, 3
K-W: .36
Quantitative variables are expressed as mean � standard deviation (range); categorical variables are expressed as frequencies, or median (25th, 75th percentiles).BMI, body mass index; LDL, low-density lipoprotein; HDL, high-density lipoprotein; BP, blood pressure; CTCA, computed tomography coronary angiography; HR, heart
rate; recon., reconstruction; K-W, Kruskal-Wallis.
Academ
icR
adiology,V
ol15,
No
4,A
pril2008
AC
CU
RA
CY
OF
CT
CO
RO
NA
RY
AN
GIO
GR
AP
HY455

HUSMANN ET AL Academic Radiology, Vol 15, No 4, April 2008
diameter �1.5 mm were evaluated (of 1408 segments, 88patients, each with coronary 16 segments, 137 segmentswere missing because of anatomic variants; 76 segmentshad a diameter less than 1.5 mm at their origin). Thirteensegments (1.1%) were rated not evaluative in CTCA andwere subsequently scored as “false positive” on an inten-tion-to-diagnose basis.
Diagnostic Accuracy of CTCA: Overall and inGroups With Low, Intermediate, and High PretestProbability for CAD
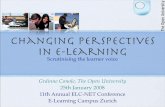
A total of 114 coronary artery stenoses with a luminal
Figure 1. Demonstration of significant stenosisin a 62-year-old male patient.
Table 2Prevalence of CAD in Groups with Low, Intermediate, and High
AnalysisLow Risk for CAD
EventsI
Patient based (n � 88) 29.4% (10/34)Vessel based (n � 351) 13.2% (18/136)Segment based (n � 1191) 4.7% (22/466)
CAD, coronary artery disease.
narrowing of more than 50% in diameter were identified
456
with ICA in 43 of 88 patients (49%) (Fig. 1). Single-ves-sel disease was present in 16 of 88 (18%), 2-vessel dis-ease in 14 of 88 (16%), and 3-vessel disease in 13 of 88(15%) patients. Significant coronary artery stenosis wasexcluded in 45 of 88 patients (51%). In groups with low,intermediate, and high risk for CAD events, the overallprevalence of CAD was 10 of 34 (29%), 16 of 29 (55%),and 17 of 25 (68%) patients, respectively; the patient-,vessel-, and segment-based prevalence of CAD within thegroups is given in Table 2.
Kappa values for interobserver agreement for coronaryartery stenosis detection with CTCA were 0.92, 0.70, and0.59 (patient, vessel, and segment based), indicating a
wheads) with CTCA (a, b, d, f) and ICA (c, e)
for CAD Events
ediate Risk forAD Events
High Risk for CADEvents
SignificanceP-Value
2% (16/29) 68.0% (17/25) �2: �.011% (30/115) 36.0% (36/100) �2: �.0016% (37/386) 16.2% (55/339) �2: �.001
(arro
Risk
ntermC
55.26.9.
moderate to excellent agreement.

Academic Radiology, Vol 15, No 4, April 2008 ACCURACY OF CT CORONARY ANGIOGRAPHY
CTCA correctly detected 92 of the 114 significantstenoses (81%), with 41 of 1191 false-positive (3%)and 22 of 1191 false-negative (2%) ratings on a seg-ment-based analysis. The vessel-based analysis re-vealed 19 of 351 false-positive (5%) and 8 of 351false-negative (2%) ratings. On a patient-based analy-sis, 8 of 88 false-positive (9%) and 3 of 88 false-nega-tive (3%) ratings occurred with CTCA overall; in thegroups with low, intermediate, and risk for CADevents, false-positive ratings were 5 of 34 (15%), 1 of29 (3%), and 2 of 25 (8%), respectively (P � not sig-nificant). With regard to the true-negative ratings, CADwas correctly ruled out with CTCA in 37 of 88 (34%)patients overall, whereas in the groups with low, inter-mediate, and high risk for CAD events, the respectivevalues differed significantly: 19 of 34 (56%), 12 of 29(41%), and 6 of 25 (24%) (P � .05; Fig. 2).
A detailed overview of the patient-, vessel-, and seg-ment-based analysis of the diagnostic accuracy of CTCAoverall, and within the three groups with low, intermedi-ate, and high risk for CAD events, is presented in Table 3.
Figure 2. The proportion (in percent) of true-negative ratingswithin each group (ie, the percentage of patients in whom unnec-essary invasive procedures would have been avoided in a clinicalsetting) was highest in the group with low risk for CAD eventsand progressively decreased low risk for CAD events.
Briefly, sensitivity and specificity of CTCA are not influ-
enced by the risk for CAD events, whereas the NPV islower (segment based) and the PPV displays a trend to behigher in patients with a high risk (patient based). Figure3 demonstrates the PPV and NPV of CTCA with respectto the risk for CAD events on a per-patient, per-vessel,and per-segment analysis.
DISCUSSION
According to the Bayesian theorem, diagnostic testperformances depend on the prevalence of the disease.Although sensitivity and specificity are not affected, thePPV increases and the NPV decreases when the preva-lence increases. Therefore, to avoid overestimation of di-agnostic accuracy in clinical practice, tests should be ap-plied in settings, comparable to the study conditions.CTCA is suggested to be used for ruling out CAD pri-marily in patients with a low and intermediate pretestprobability for CAD (11–13). Nonetheless, diagnostic ac-curacy of CTCA has mainly been studied in patient popu-lations with high prevalences of CAD (1–3,5,6,8,10), be-cause ICA as the reference standard is only justifiable inpopulations with high risk for CAD. Only little data havebeen published on the topic (19), and our study is the firstto use the recently suggested intention-to-diagnose strat-egy for evaluation (20), where nonevaluative segments inCTCA are rated as false-positive findings.
We found that the sensitivity and specificity of CTCAare not influenced by the risk for CAD events and theprevalence of CAD, whereas the NPV is lower and thePPV tends to be higher in patients with a high risk forCAD events and high prevalence of CAD.
Prevalence of CADWe stratified the patients using the Framingham score,
resulting in groups with low, intermediate, and high riskfor cardiovascular events. The findings from ICA con-firmed that this translated into low, intermediate, and highprevalence of CAD.
In addition, when looking at the diagnostic perfor-mance of CTCA on a per-patient, per-vessel, and per-segment basis (Table 3), the numerical interdependence ofpatients, vessels, and segments needs to be taken into ac-count, as the prevalence of disease is highest in the pa-tient-based analysis and lowest in the segment-based anal-ysis (Table 2) (i.e., a patient with a single segment steno-sis will have a patient-based prevalence of disease of100%, a vessel-based prevalence of 25%, and a segment-
based prevalence of 6%).457

Table 3Diagnostic Accuracy in Groups with Low, Intermediate, and High Pretest Probability for CAD
All Patients(absolute values; 95% CI)
Low Risk for CAD Events(absolute values; 95% CI)
Intermediate Risk for CAD Events(absolute values; 95% CI)
High Risk for CAD Events(absolute values; 95% CI)
SignificanceP-Value
Patient based:Sensitivity 93.0% (40/43; 80.9–98.5) 90.0% (9/10; 55.5–98.8) 87.5% (14/16; 61.7–98.5) 100% (17/17; NA) .33Specificity 82.2% (37/45; 67.9–92.0) 79.2% (19/24; 57.9–92.9) 92.3% (12/13; 63.9–99.8) 75.0% (6/8; 34.9–96.8) .51NPV 92.5% (37/40; 79.6–98.4) 95.0% (19/20; 75.1–99.9) 85.7% (12/14; 57.2–98.2) 100% (6/6; NA) .45PPV 83.3% (40/48; 69.8–92.5) 64.3% (9/14; 35.1–87.2) 93.3% (14/15; 68.1–99.8) 89.5% (17/19; 66.9–98.7) .07Accuracy 87.5% (77/88; 78.7–93.6) 82.4% (28/34; 65.5–93.2) 89.7% (26/29; 72.7–97.8) 92.0% (23/25; 73.9–99.0) .44
Vessel based:Sensitivity 90.5% (76/84; 82.1–95.8) 94.4% (17/18; 72.7–99.9) 86.7% (26/30; 69.3–96.2) 91.7% (33/36; 77.5–98.3) .64Specificity 92.9% (248/267; 89.1–95.7) 93.2% (110/118; 87.1–97.0) 95.3% (81/85; 88.4–98.7) 89.1% (57/64; 78.8–95.5) .34NPV 96.9% (248/256; 93.9–98.6) 99.1% (110/111; 95.1–99.9) 95.3% (81/85; 88.4–98.7) 95.0% (57/60; 86.1–98.9) .20PPV 80.0% (76/95; 70.5–87.5) 68.0% (17/25; 46.5–85.1) 86.7% (26/30; 69.3–96.2) 82.5% (33/40; 67.2–92.7) .19Accuracy 92.3% (324/351; 89.0–94.9) 93.4% (127/136; 87.8–96.9) 93.0% (107/115; 86.8–96.9) 90.0% (90/100; 82.4–95.1) .59
Segment based:Sensitivity 80.7% (92/114; 72.3–87.5) 86.4% (19/22; 65.1–97.1) 83.8% (31/37; 67.9–93.8) 76.4% (42/55; 62.9–86.8) .51Specificity 96.2% (1036/1077; 94.9–97.3) 96.4% (428/444; 94.2–97.9) 96.6% (337/349; 94.1–98.2) 95.4% (271/284; 92.3–97.5) .73NPV 97.9% (1036/1058; 96.9–98.7) 99.3% (428/431; 97.9–99.9) 98.3% (337/343; 96.2–99.4) 95.4% (271/284; 92.3–97.5) �.01PPV 69.2% (92/133; 60.6–76.9) 54.3% (19/35; 36.7–71.2) 72.1% (31/43; 56.3–84.7) 76.4% (42/55; 62.9–86.8) .88Accuracy 94.7% (1128/1191; 93.3–95.9) 95.9% (447/466; 93.7–97.5) 95.3% (368/386; 92.7–97.2) 92.3% (313/339; 88.9–94.9) .06
CAD, coronary artery disease; CI, confidence interval; NA, not available; NS, not significant; NPV, negative predictive value; PPV, positive predictive value.
HU
SM
AN
NE
TA
LA
cademic
Radiology,
Vol15,
No
4,A
pril2008
458

Academic Radiology, Vol 15, No 4, April 2008 ACCURACY OF CT CORONARY ANGIOGRAPHY
Sensitivity and Specificity of CTCASeveral parameters such as body mass index (3), image
quality (17), coronary calcium score (21), heart rate (21),and heart rate variability (17) have been suggested to af-fect sensitivity and specificity of CTCA, whereas it is ageneral rule that the prevalence of a disease has no suchimpact (22). Nevertheless, in our study, an increasingprevalence appears to be paradoxically associated with anonsignificant trend toward lower specificity. This is inline with a large body of literature on CTCA (1–3,5,6,8–10) (Table 4); for example, Meijboom and colleagues(10) reported a specificity of 75% in a population with aprevalence of 85%, whereas Ropers and colleagues (9)found a specificity of 91% in a study with a prevalence of31% of CAD. Our results support the notion that highercalcium scores may account for the decreased specificityin groups with a higher prevalence. In particular, high
Figure 3. (a) PPV of CTCA in comparison to the reference stan-dard ICA, in groups with low, intermediate, and high risk for CADevents on a per-patient, per-vessel, and per-segment analysis.(b) NPV of CTCA in comparison to the reference standard ICA, ingroups with low, intermediate, and high risk for CAD events on aper-patient, per-vessel, and per-segment analysis.
calcium scores, which are generally associated with a
high prevalence of CAD (23), can often cause bloomingartefacts with subsequent overestimations of the degree ofcalcified lesions, leading to false-positive ratings andlower specificities (24). To improve specificity of CTCA,in our study, we used a sharp tissue-convolution kernelfor the assessment of calcified coronary lesions, to mini-mize this overestimating effect (25). However, we evalu-ated our patients on an intention-to-diagnose basis, ratingall nonevaluative segments as false positive, which, incontrast, has decreased the overall specificity of CTCA.The balance of these two opposite effects resulted in aspecificity ranging well within the results reported in theliterature (Table 4) (1–3,5,6,8–10).
Sensitivity of CTCA is generally high and was notinfluenced by either the risk for CAD events in our studyor the prevalence as shown in previous 64-slice CTCAstudies (1–3,5,6,8–10) (Table 4).
NPV and PPV of CTCAA decrease in prevalence was associated with a non-
significant trend toward a low PPV. This holds true forthe prevalence in the three groups as well as for compari-son of patient-based over vessel-based toward segment-based analysis due to a decrease in prevalence for numer-ical reasons. The contrary effect (ie, an increase in theNPV with falling prevalence) could be substantiated, al-though the NPV is excellent even with high prevalence ofdisease (Fig. 3). Similarly, Hausleiter and colleagues (21)demonstrated PPV values of CTCA of 65% versus 79%in two patient populations with Framingham risk scoresbelow and above an arbitrary cutoff of 12%, stating thatthese values did not differ. They also found NPVs not todiffer in both populations, which is in line with our re-sults on a patient-based analysis. However, on a segment-based analysis, we demonstrated a significant decrease inNPVs with an increase of prevalence. Most probably, thisis due to the increased statistical power resulting fromsubdividing all vessels of each single patient into 16 seg-ments.
Clinical ImplicationsCTCA has been proposed as a “gatekeeper” for ICA
(21). This study shows for the first time that due to itshigh NPV, CTCA can be used safely to rule out CAD inpatients with low or intermediate risk as well as thosewith high risk for CAD events. Our data suggest that in aclinical setting, CTCA would have avoided unnecessaryICA in 56%, 41%, and 24% of patients in the groups
with low, intermediate, and high risk for CAD events459

ive p
HUSMANN ET AL Academic Radiology, Vol 15, No 4, April 2008
(Fig. 2). This would not be achieved at the cost of falselysending many patients to ICA, as the high number ofavoided ICA by far outweighs the few false-positive val-ues. The present study underlines that this balance is par-ticularly favorable in low- and intermediate-risk popula-tions. Furthermore, we support the suggestion that theaddition of myocardial perfusion imaging should comple-ment CTCA (26,27) according to best clinical practice(28) to provide a basis on which a decision to revascular-ize can be based.
Study LimitationsWe acknowledge the following limitations to our
study. First, the Framingham risk score does not take intoaccount all risk factors for CAD. Nonetheless, the Fra-mingham risk score is easily assessable and a widely es-tablished method in clinical routine.
Second, �2-tests for comparison of diagnostic perfor-mance on a per-vessel and per-segment-basis must beregarded as an approximation because of data clustering.However, adequate statistical testing could not be appliedbecause of small group sizes.
Third, our study was performed using 64-slice CT andnot using most recent dual-source CT scanner technology
Table 4Diagnostic Accuracy of 64-Slice CTCA
Authors Prevalence (%) Patients (n)
Patient basedMeijboom et al. (10) 85 104Ehara et al. (8) 88 67Pugliese et al. (5) 71 35Leschka et al. (1) 70 67Nikolaou et al. (6) 57 72Raff et al. (3) 57 70Present study 49 88Leber et al. (2) 42 59Ropers et al. (9) 31 84
Segment basedEhara et al. (8) 34 884Leschka et al. (1) 18 1005Pugliese et al. (5) 14 494Nikolaou et al. (6) 13 923Meijboom et al. (10) 13 1525Present study 10 1191Raff et al. (3) 10 935Leber et al. (2) 8 798Ropers et al. (9) 4 1083
CTCA, computed tomography coronary angiography; PPV, posit
(29). However, if necessary we administered �-adreno-
460
ceptor antagonists to compensate for the lower temporalresolution of 64-slice CT.
CONCLUSIONS
The sensitivity and specificity of CTCA are not influ-enced by risk for CAD events or the prevalence of dis-ease, whereas the NPV is lower and the PPV tends to behigher when the risk for CAD events and the prevalenceof disease is high.
REFERENCES
1. Leschka S, Alkadhi H, Plass A, et al. Accuracy of MSCT coronary an-giography with 64-slice technology: First experience. Eur Heart J 2005;26:1482–1487.
2. Leber AW, Knez A, von Ziegler F, et al. Quantification of obstructiveand nonobstructive coronary lesions by 64-slice computed tomography: Acomparative study with quantitative coronary angiography and intravascu-lar ultrasound. J Am Coll Cardiol 2005; 46:147–154.
3. Raff GL, Gallagher MJ, O’Neill WW, et al. Diagnostic accuracy of non-invasive coronary angiography using 64-slice spiral computed tomogra-phy. J Am Coll Cardiol 2005; 46:552–557.
4. Mollet NR, Cademartiri F, van Mieghem CA, et al. High-resolution spiralcomputed tomography coronary angiography in patients referred fordiagnostic conventional coronary angiography. Circulation 2005; 112:2318–2323.
5. Pugliese F, Mollet NR, Runza G, et al. Diagnostic accuracy of non-inva-
ccuracy Sensitivity Specificity NPV PPV
96 100 75 100 9697 98 86 86 9897 100 90 100 96NA 100 NA 100 NA90 97 79 96 8693 95 90 93 9388 93 82 93 83NA 88 NA NA NA89 96 91 98 83
93 91 94 95 8997 94 97 99 8796 99 96 100 7894 82 95 97 6991 92 91 99 6095 81 96 98 6994 86 95 98 6696 79 97 98 7296 93 97 100 56
redictive value; NPV, negative predictive value; NA, not available.
A
sive 64-slice CT coronary angiography in patients with stable anginapectoris. Eur Radiol 2006; 16:575–582.

Academic Radiology, Vol 15, No 4, April 2008 ACCURACY OF CT CORONARY ANGIOGRAPHY
6. Nikolaou K, Knez A, Rist C, et al. Accuracy of 64-MDCT in the diagno-sis of ischemic heart disease. AJR Am J Roentgenol 2006; 187:111–117.
7. Ong TK, Chin SP, Liew CK, et al. Accuracy of 64-row multidetectorcomputed tomography in detecting coronary artery disease in 134symptomatic patients: Influence of calcification. Am Heart J 2006;151:1321–1326.
8. Ehara M, Surmely JF, Kawai M, et al. Diagnostic accuracy of 64-slicecomputed tomography for detecting angiographically significant coro-nary artery stenosis in an unselected consecutive patient population:Comparison with conventional invasive angiography. Circ J 2006;70:564–571.
9. Ropers D, Rixe J, Anders K, et al. Usefulness of multidetector row spi-ral computed tomography with 64- � 0.6-mm collimation and 330-msrotation for the noninvasive detection of significant coronary artery ste-noses. Am J Cardiol 2006; 97:343–348.
10. Meijboom WB, Mollet NR, van Mieghem CA, et al. 64-slice Computedtomography coronary angiography in patients with non-ST elevationacute coronary syndrome. Heart 2007; 93:1386–1392.
11. Budoff MJ, Achenbach S, Blumenthal RS, et al. Assessment of coro-nary artery disease by cardiac computed tomography: A scientificstatement from the American Heart Association Committee on Cardio-vascular Imaging and Intervention, Council on Cardiovascular Radiol-ogy and Intervention, and Committee on Cardiac Imaging, Council onClinical Cardiology. Circulation 2006; 114:1761–1791.
12. Fox K, Garcia MA, Ardissino D, et al. Guidelines on the management ofstable angina pectoris: executive summary: The Task Force on theManagement of Stable Angina Pectoris of the European Society ofCardiology. Eur Heart J 2006; 27:1341–1381.
13. ACCF/ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR 2006 Appropriate-ness criteria for cardiac computed tomography and cardiac magneticresonance imaging. A report of the American College of CardiologyFoundation Quality Strategic Directions Committee AppropriatenessCriteria Working Group. J Am Coll Radiol 2006; 3:751–771.
14. Expert Panel on Detection, Evaluation and Treatment of High BloodCholesterol in Adults. Executive summary of the Third Report of theNational Cholesterol Education Program (NCEP) Expert Panel on De-tection, Evaluation and Treatment of High Blood Cholesterol in Adults(Adult Treatment Panel III). JAMA 2001; 285:2486–2497.
15. Flohr T, Ohnesorge B. Heart rate adaptive optimization of spatial andtemporal resolution for electrocardiogram-gated multislice spiral CT ofthe heart. J Comput Assist Tomogr 2001; 25:907–923.
16. Austen WG, Edwards JE, Frye RL, et al. A reporting system on patientsevaluated for coronary artery disease. Report of the Ad Hoc Committee
for Grading of Coronary Artery Disease, Council on Cardiovascular Sur-gery, American Heart Association. Circulation 1975; 51:5–40.17. Leschka S, Wildermuth S, Boehm T, et al. Noninvasive coronary an-giography with 64-section CT: Effect of average heart rate and heartrate variability on image quality. Radiology 2006; 241:378–385.
18. Landis JR, Koch GG. The measurement of observer agreement for cat-egorical data. Biometrics 1977; 33:159–174.
19. Meijboom WB, van Mieghem CA, Mollet NR, et al. 64-Slice computedtomography coronary angiography in patients with high, intermediate,or low pretest probability of significant coronary artery disease. J AmColl Cardiol 2007; 50:1469–1475.
20. Garcia MJ, Lessick J, Hoffmann MH. Accuracy of 16-row multidetectorcomputed tomography for the assessment of coronary artery stenosis.JAMA 2006; 296:403–411.
21. Hausleiter J, Meyer T, Hadamitzky M, et al. Non-invasive coronarycomputed tomographic angiography for patients with suspected coro-nary artery disease: The Coronary Angiography by Computed Tomog-raphy with the Use of a Submillimeter resolution (CACTUS) trial. EurHeart J 2007; 28:3034–3041.
22. Diamond GA, Forrester JS. Analysis of probability as an aid in the clini-cal diagnosis of coronary-artery disease. N Engl J Med 1979;300:1350–1358.
23. Arad Y, Goodman KJ, Roth M, et al. Coronary calcification, coronarydisease risk factors, C-reactive protein, and atherosclerotic cardiovas-cular disease events: The St. Francis Heart Study. J Am Coll Cardiol2005; 46:158–165.
24. Kuettner A, Trabold T, Schroeder S, et al. Noninvasive detection ofcoronary lesions using 16-detector multislice spiral computed tomogra-phy technology: Initial clinical results. J Am Coll Cardiol 2004;44:1230–1237.
25. Cademartiri F, La Grutta L, Runza G, et al. Influence of convolution fil-tering on coronary plaque attenuation values: Observations in an exvivo model of multislice computed tomography coronary angiography.Eur Radiol 2007; 17:1842–1849.
26. Gaemperli O, Schepis T, Valenta I, et al. Cardiac image fusion fromstand-alone SPECT and CT: Clinical experience. J Nucl Med 2007;48:696–703.
27. Namdar M, Hany TF, Koepfli P, et al. Integrated PET/CT for the as-sessment of coronary artery disease: A feasibility study. J Nucl Med2005; 46:930–935.
28. Kern MJ, Lerman A, Bech JW, et al. Physiological assessment of coro-nary artery disease in the cardiac catheterization laboratory: A scientificstatement from the American Heart Association Committee on Diag-nostic and Interventional Cardiac Catheterization, Council on ClinicalCardiology. Circulation 2006; 114:1321–1341.
29. Scheffel H, Alkadhi H, Plass A, et al. Accuracy of dual-source CT coro-
nary angiography: First experience in a high pre-test probability popu-lation without heart rate control. Eur Radiol 2006; 16:2739–2747.461


















