University of Groningen Reflections on flurbiprofen ...
153
University of Groningen Reflections on flurbiprofen eyedrops van Sorge, Adriaan Alastair IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 2002 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): van Sorge, A. A. (2002). Reflections on flurbiprofen eyedrops. s.n. Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license. More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne- amendment. Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons the number of authors shown on this cover page is limited to 10 maximum. Download date: 04-10-2021
Transcript of University of Groningen Reflections on flurbiprofen ...

University of Groningen
Reflections on flurbiprofen eyedropsvan Sorge, Adriaan Alastair
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2002
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):van Sorge, A. A. (2002). Reflections on flurbiprofen eyedrops. s.n.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license.More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne-amendment.
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 04-10-2021

REFLECTIONS ON FLURBIPROFEN EYEDROPSREFLECTIONS ON FLURBIPROFEN EYEDROPS


RIJKSUNIVERSITEIT GRONINGEN
PROEFSCHRIFT
ter verkrijging van het doctoraat in deWiskunde en Natuurwetenschappenaan de Rijksuniversiteit Groningen,
op gezag van de Rector Magnificus, dr. F. Zwarts,in het openbaar te verdedigen op
maandag 2 december 2002om 14.15 uur
door
Adriaan Alastair van Sorge
geboren op 28 oktober 1944te New Rochelle, New York, USA
REFLECTIONS ON FLURBIPROFEN EYEDROPSREFLECTIONS ON FLURBIPROFEN EYEDROPS

PROMOTORES Prof. dr. J. ZaagsmaProf. dr. W.J. QuaxProf. dr. H.W. Frijlink
CO-PROMOTOR Dr. N.J. van Haeringen
BEOORDELINGSCOMMISSIE Prof. dr. P.T.V.M. de JongProf. dr. J.R.B.J. BrouwersProf. dr. H.V. Wikström
ISBN: 90-9016364-6Verzorging proefschrift: B-Point, Karin Scheele

PARANIMFEN Dr. R.F.A. WeberDr. A.J.P.F. Lombarts
My parents, who got me started
Aty, Nina, Joline and Arlette, who let me go on
Eelco, who wouldn't let me quit


CONTENTS
Preface A historical introduction 9Scope of thesis
Chapter 1 General introduction 171.1 Flurbiprofen, an overview1.2 Cataract and caractogenesis1.3 Cystoid macular edema1.4 Prostanoids
Chapter 2 Rationale for using a phosphate buffer for S(+) flurbiprofen eyedrops. 43
Chapter 3 Flurbiprofen, S(+), eyedrops: formulation, enantiomeric assay,shelflife and pharmacology (1). 49
Chapter 4 Specificity of flurbiprofen and enantiomers for inhibition ofprostaglandin synthesis in bovine iris/ciliary body (2). 63
Chapter 5 Flurbiprofen and enantiomers in ophthalmic solution testedas inhibitors of prostanoid synthesis in human blood (3). 73
Chapter 6 Constitutive cyclooxygenase-1 and induced cyclooxygenase-2in isolated human iris inhibited by S(+) flurbiprofen (4). 83
Chapter 7 99mTc-Diflunisal and the human iris: topical applicationreveals localization (5). 95
Chapter 8 S(+) flurbiprofen and R(-) flurbiprofen. 99mTc-labelingreveals difference in stereochemistry (6). 107
Chapter 9 Alternative splicing of cyclooxygenase-1 mRNAin the human iris (7). 115
Summary/Samenvatting 123List of publications 135Dankwoord 137Curriculum Vitae 143Color pictures 147Addendum 151

REFERENCES
1. van Sorge AA, Wijnen PH, van Delft JL, Carballosa Coré-Bodelier VMW, vanHaeringen NJ. Flurbiprofen, S(+), eyedrops: formulation, enantiomeric assay,shelflife and pharmacology. Derived from Pharm World Sci 1999;21:91-5.
2. Sorge van AA, Delft van JL, Bodelier VMW, Wijnen PH, Haeringen van NJ.Specificity of flurbiprofen and enantiomers for inhibition of prostaglandin synthesisin bovine iris/ciliary body. Prostaglandins Other Lipid Mediat 1998;55:169-77.
3. Haeringen van NJ, Sorge van AA, Delft van JL, Carballosa Coré-Bodelier VMW.Flurbiprofen and enantiomers in ophthalmic solution tested as inhibitors ofprostanoid synthesis in human blood. J Ocular Pharmacol 2000;16:345-52.
4. Haeringen van NJ, Sorge van AA, Carballosa Coré-Bodelier VMW. Constitutivecyclooxygenase-1 and induced cyclooxygenase-2 in isolated human iris inhibitedby S(+) flurbiprofen. J Ocular Pharmacol 2000;16:353-61.
5. Sorge van AA, Etten van RJ, Rehmann CJ, Rijnders AJM, Haeringen van NJ. 99mTc-Diflunisal and the human iris: topical application reveals localization. J OcularPharmacol 2002;18:185-95.
6. Sorge van AA, Ruiken IWM, Janssen HWM, Haeringen NJ. S(+) flurbiprofen andR(-) flurbiprofen. 99mTc-labeling reveals difference in stereochemistry. Enantiomer2002; Accepted pending suitable revision.
7. Dröge MJ, van Sorge AA, van Haeringen NJ, Quax WJ, Zaagsma J. Alternativesplicing of cyclooxygenase-1 mRNA in the human iris. Submitted.
8

PREFACE

A HISTORICAL INTRODUCTION
A simple question put forward in 1980 by one of the ophthalmologists to the hospi-tal pharmacist led to a chain of events culminating in this thesis. The question was:"Is it possible to prepare indomethacin eyedrops?".
The principal reason for the question were reports on eye research, mainly ofJapanese origin (1, 2, 3, 4, 5), indicating that use of topically applied indomethacincould prevent cystoid macular edema after lens extraction, required e.g. when apatient had acquired a senile cataract. The incidence of this complication variedbetween 2 and 50% but reports of 70% were known as well. The complication hadbeen reported earlier as a newly defined vitreous syndrome following cataract sur-gery and was described in 1953 (6).
Just over 65 years ago it was postulated by Selye (7) that our physiological system,activated by stress, not only will try to protect and restore itself but also can derailand afflict damage. The most common responses to stress are activation of thesympathetic nervous system and of the hypothalamic-pituitary-adrenal (HPA) axis,resulting in or accompanied by immunological changes.
The immunological defense mechanisms of the ocular surface have been reviewedin detail in 1983 (8). A review ten years earlier (9) refers to the finding by Ambacheof a physiological smooth muscle stimulant as a constituent of the rabbit iris ("Irin")in 1957, and the further elucidation of its nature in 1959 (10,11).
In 1967 the synthesis of prostaglandins in the pig iris was reported (12) and in 1968their release from bovine iris (13). Subsequently, prostaglandins were related tovarious ocular functions indeed (14).
In 1971 a pivotal study was reported by Vane (15) demonstrating the inhibitingeffect on prostaglandin synthesis as the mechanism of action of non-steroidal anti-inflammatory drugs (NSAIDs).
Release of prostaglandins in the rabbit eye was shown following an acuteimmunological inflammatory reaction induced by a single intravitreal injection ofsterile crystallized bovine serum albumin (16). This report preceded a study, also inrabbits, demonstrating that an acutely traumatized eye shows an irritative responsecharacterized by hyperaemia of the conjunctiva and iris, miosis and disruption ofthe blood-aqueous barrier. One of the signs of blood-aqueous barrier disruption isan increased concentration of blood proteins in the aqueous humour. Using a rele-vant pharmacological model a significant reduction in protein concentration in theaqueous humour could be demonstrated by pretreating the animal with a rectal
Preface
10

dose of acetosal (acetylsalicylic acid; 600mg) (17). Stabilization of the blood-aque-ous barrier in the human eye with acetosal administered orally (4 doses of 650mg;3 before and one on completion of ocular surgery) was reported in 1975 (18).
Levels of prostaglandin-like activity in aqueous humour samples correlated wellwith the clinical intensity of uveitis. This in contrast to patients with cataract whoseaqueous humour was essentially devoid of activity when the eyes were uninflamed,and low in activity when treated with corticosteroids (19).
In vitro inhibition of rabbit prostaglandin synthase systems of various organs,including the eye, by indomethacin was reported in 1974 (20). Tissue homogenatesof the iris and the ciliary body (anterior uvea), the conjunctiva, the cornea and reti-na were prepared; spleen and kidney (medulla) were also investigated. Theinhibitory effect of indomethacin was clearly demonstrated and the compoundshowed differential inhibitory capacity. The retinal enzymes were least susceptibleto inhibition followed by iris and ciliary body (twofold more) and the conjunctiva (sixfold more). This also raised the possibility that prostaglandins are involved both inexternal as well as internal ocular inflammation.
The potential complication reported by our ophthalmologists that could arise aftercataract surgery, cystoid macular edema, seemed linked to the release ofprostaglandins. Thus, in the event of adequate permeation of indomethacin throughthe cornea, the edema should be prevented by topical administration of eyedrops.In 1972 it has been demonstrated by application of 100 microgram radiolabelledindomethacin to the cornea (either in aqueous suspension form or in oily solution)that the drug could be detected in the cornea, aquous humor, iris, choroids and reti-na of the rabbit eye (21). An inflamed eye gave rise to enhanced penetration. In1983 it was subsequently shown, by use of topically applied radiolabelledindomethacin (2% suspension in sesame oil, including 17% ethanol) on phakic andaphakic rabbit eyes, that penetration into the vitreous took place; the concentrationin the vitreous was higher for the aphakic eye. Concentrations in retina and choroidwere the same for both conditions, suggesting a pathway other than diffusionthrough the vitreous to reach these tissues. Aqueous humour concentrations weresufficient to inhibit prostaglandin synthesis in either situation (22).
Indomethacin, [1-(4-chlorobenzoyl)-5-methoxy-2-methylindol-3-yl]acetic acid, molec-ular weight 357.8 dalton, pKa 4.5, is practically insoluble in water. In aqueous buffersat pH 7.5 - 8.0 it can be rendered soluble (23). In basic solutions hydrolysis ofindomethacin occurs into 5-methoxy-2-methylindolyl-3-acetic acid and 4-chloroben-zoic acid (24,25,26). These substances are pharmacologically inactive. In theEuropean pharmacopea (1997) 4-chloro-benzoic acid is mentioned as an impurity.
Preface
11

Pharmacokinetics of indomethacin are as follows. The major route of elimination isby transformation in the liver and involves glucuronidation, O-demethylation and N-deacylation. The major (inactive) metabolites are desmethyl indomethacin, des-chlorobenzoyl indomethacin and their glucuronides. Protein binding is more than90%. Volume of distribution is 0.12 L/kg; clearance is 1-2 mL/min/kg with a half-lifeof 6 hours. The compound is excreted unchanged in urine for 30%.
Indomethacin was introduced into the field of ophthalmology in different types offormulations including a solution in sesame oil and an ophthalmic aqueous sus-pension (1,27). Concentrations in suspension eyedrops varied between 0.5% to 1%and in oily solutions from 0.1 to 1%. In the Dutch literature several formulations ofindomethacin eyedrops followed the first international reports (vide supra) on theprevention of cystoid macular edema after lens extraction (28,29,30). As useexpanded in the clinic, reports indicated that the prepared solutions, being a sus-pension or an aqueous solution, were irritating to the eye (burning sensation). Areduction in concentration was suggested from 1% to 0.2% or 0.1% to prevent thisundesirable effect. In 1981 it was shown that four different indomethacin suspen-sion eyedrops, all being 0.5% in concentration, differed in prostaglandin synthaseinhibiting activity, which was attributed to the differences in physicochemical prop-erties. It was concluded that the use of eyedrops as a suspension yields irrepro-ducible results from the pharmacokinetic point of view and gives rise to subjectivecomplaints of irritation in the eye (31).
In 1984 Indoptol®, an aqueous eyedrop suspension of 1% indomethacin, wasintroduced to the Dutch market and in 1986 Indocid® of comparable compositionwas introduced in France. In 1987 a second presentation of indomethacin followedin France in the form of Indocollyre® (0,1%), which was introduced in TheNetherlands in 1994. This formulation contains indomethacin as a lyophilized(freeze-dried) product which is brought into solution by addition of a sterile boratebuffer. In the international literature aqueous formulations of indomethacin eye-drops have been published (32,33,34) reflecting the need for a more suitable andreliable pharmaceutical preparation. Ongoing own research with different bases, L-Lysine, D-Lysine, L-Arginine, D-Arginine, and Tromethamol (not published), to pro-vide an indomethacin solution with an acceptable shelflife, did not provide suitablepharmaceutical alternatives. They all were aqueous solutions in order to circumventthe irritating properties of the suspension based eyedrops and the sesame oilbased solution causing blurring of vision by difference in refractive index. However,our originally introduced solution (29) without extra pharmaceutical excipients andhaving a concentration of indomethacin of 0.1% remained the mainstay of the eyeclinic. This solution was tested in a pharmacological setting in the rabbit eye usinga paracentesis model of removing the aqueous humor and measuring the influx ofprotein and fluorescein into the secondary aqueous humor (35). The results
Preface
12

showed, in a concentration of indomethacin as low as 0.05%, 90 - 100% pharma-cological efficacy in inhibiting fluorescein and protein influx (36). The indomethacin0.1% formulation was incorporated in the Dutch national formulary (FNA) in 1986.Inpracticalities with indomethacin in aqueous solution - no sterilization possible anda short shelflife - prompted us to investigate the possibility in formulating eyedropsbased on a different NSAID. In 1990 topically applied S(+) ibuprofen was reportedto be effective in a rabbit model of interleukin-1 (37) or paracentesis induced uveitis(38) at relatively elevated concentrations (0.9% and 0.8% respectively). Also withS(+) naproxen, marketed by Syntex as enantiomeric pure NSAID, an anti-inflam-matory effect of eyedrops (0,5%) was demonstrated experimentally (39).
In our quest for a pharmaceutically more acceptable solution of an NSAID, weturned to the USP in which a flurbiprofen ophthalmic solution is mentioned.
Ophthalmic solutions of flurbiprofen, diclofenac, and indomethacin (pH 7.5), havebeen subjected to research in rabbit eyes to investigate the maximal effect in pre-venting breakdown of the blood-aqueous barrier (40). Effective doses [nmol] pereye resulting in 50% inhibition (ID50) of influx of protein and of fluorescein into sec-ondary aqueous humor after paracentesis corresponded well for indomethacin andflurbiprofen (12 nmol for flurbiprofen, 11 nmol for indomethacin, and 8.0 nmol forflurbiprofen and 9.0 nmol for indomethacin, respectively).
In a comparative test of 11 nonsteroidal anti-inflammatory compounds in 0.01%solution, using the rabbit paracentesis model, flurbiprofen proved to be the mosteffective, showing a half-life of the inhibitory effect of 10 hours (41). A speciality,Ocufen®, containing 0.03% flurbiprofen sodium 2H2O (equivalent to 0.024% flur-biprofen acid), is on the market in the United States since 1987 for inhibition ofintraoperative miosis (42). Ocuflur® of comparable composition, marketed inBelgium, is also indicated for use in intraoperative inhibition of miosis, treatment ofinflammation as a result of surgical intervention or trabeculoplasty by laser treat-ment and for prevention of cystoid macular edema after cataract surgery.
We embarked on a study to manufacture flurbiprofen eyedrops by protocol of june1992. A letter of consent to aid the project (9206SO.008) was issued January 8th
1993 by the SWOR (Stichting ter bevordering van Wetenschappelijk Onderzoek inziekenhuis Rijnstate).
REFERENCES
1. Miyake K. Prevention of cystoid macular edema after lens extraction by topical indomethacin (I).Albrecht v. Graefes Arch Klin Exp Ophthal 1977;203:81-8.
2. Mochizuki M, Sawa M, Masuda K. Topical indomethacin in intracapsular extraction of senilecataract. Jpn J Ophthalmol 1977;21:215-26.
3. Miyake K. Prevention of cystoid macular edema after lens extraction by topical indomethacin(II): a control study in bilateral extractions. Jpn J Ophthalmol 1978;22:80-94.
Preface
13

4. Miyake K, Sugiyama S, Norimatsu I, Ozawa T. Prevention of cystoid macular edema after lensextraction by topical indomethacin (III): Radioimmunoassay measurement of prostaglandins inthe aqueous during and after lens extraction procedures. Albrecht v. Graefes Arch Klin ExpOphthal 1978;209:83-8.
5. Sholiton, DB, Reinhart WJ, Frank KE. Indomethacin as a means of preventing cystoid macularedema following intracapsular cataract extraction. Am Intra-ocular Implant Soc J 1979;5:137-40.
6. Irvine SR. A newly defined vitreous syndrome following cataract surgery. Interpreted according torecent concepts of the structure of the vitreous. Am J Opthalmol 1953;36:599-619.
7. Selye H. Syndrome produced by diverse nocuous agents. Nature 1936;138:32.8. Chandler JW, Gillette TE. Immunologic defense mechanisms of the ocular surface.
Ophthalmology 1983;90:585-91.9. Neufeld AH and Sears ML. Prostaglandin and eye. Prostaglandins 1973;4:157-75.10. Ambache N. Properties of irin, a physiological constituent of the rabbit’s iris. J Physiol
1957;135:114-32.11. Ambache N. Further studies on the preparation, purification and nature of irin. J Physiol
1959;146:255-94.12. van Dorp DA, Jouvenaz GH, Struijk CB. The biosynthesis of prostaglandin in pig eye iris. Biochim
Biophys Acta 1967;137:396-9.13. Posner J. The release of prostaglandin E2 from the bovine iris. Br J Pharmacol 1968;34:163P-4P.14. Waitzman MB. Possible new concepts relating prostaglandins to various ocular functions. Survey
of Ophthalmology 1970;14:301-26.15. Vane JR. Inhibition of prostaglandinsynthesis as a mechanism of action for aspirin-like drugs.
Nature 1971;231:232-5.16. Eakins KE, Whitelocke RAF, Perkins ES, Bennett A, Unger WG. Release of prostaglandins in ocular
inflammation in the rabbit. Nature New Biology 1972;239:248-9.17. Neufeld AH, Jampol LM, Sears ML. Aspirin prevents the disruption of the blood-aqueous barrier
in the rabbit eye. Nature 1972;238:168-9.18. Zimmerman TJ, Gravenstein N, Sugar A, Kaufman HE. Aspirin stabilization of the blood-aqueous
barrier in the human eye. Am J Ophthalmol 1975;79:817-9.19. Eakins KE, Whitelocke RAF, Bennett A, Martenet AC. Prostaglandin-like activity in ocular inflam-
mation. BMJ 1972;3:452-3.20. Bhattacherjee P, Eakins KE. Inhibition of the prostaglandin synthase systems in ocular tissues by
indomethacin. Br J Pharmac 1974;50:227-30.21. Hanna C, Sharp JD. Ocular absorption of indomethacin by the rabbit. Arch Ophthal 1972;88:196-8.22. Green K, Bowman K, Luxenberg MN, Friberg TR. Penetration of topical indomethacin into pha-
kic and aphakic rabbit eyes. Arch Ophthalmol 1983;101:284-8.23. Katz IM. Indomethacin. Ophthalmology 1981;88:455-8.24. Krasowska H, Krowczynski L, Bogdanik Z. The assay of indomethacin in the presence of its
hydrolytic degradation products. Pol J Pharmacol Pharm 1973;1973;25:417-21.25. Kahns, AH, Jensen, PB, Mørk N, Bundgaard H. Kinetics of hydrolysis of indomethacin and
indomethacin ester prodrugs in aqueous solution. Acta Pharm Nord 1989;1:327-36.26. Tomida H, Kuwada N, Tsuruta Y, Kohashi K, Kiryu S. Nucleophilic aminoalcohol-catalyzed degra-
dation of indomethacin in aqueous solution. Pharm Acta Helv 1989;64:312-5.27. Yanuzzi LA, Landau AN, Turtz AI. Incidence of aphakic cystoid macular edema with the use of
topical indomethacin. Ophthalmology 1981;88:947-54.28. Lute NP, Vyth A, De Keizer RJW. Indometacine oogdruppels 0,5%. Pharm Weekbl 1980;
115:1663-4.29. Van Nispen tot Pannerden EBLM, Van Sorge AA. Waterige oogdruppels met indometacine in
oplossing; “corpora agunt nisi soluta”. Pharm Weekbl 1981;116:386-7.
Preface
14

30. Cox HLM van der Graaf H. Indometacine-oogdruppels als oplossing. Pharm Weekbl1981;116:387-8.
31. Oosterhuis JA, van Haeringen NJ, Glasius E, van Delft JL, Swart-van den Berg M. The effect ofindomethacin on the anterior segment of the eye after paracentesis. DocumentaOphthalmologica 1981;50:303-13.
32. Bechetoille A, Chabanais JL, Jallet G, Saraux H. Contusion et perméabilité de la barrière héma-to-aqueuse à la fluorescéine. Influence d’ un pré-traitement par l’indométacine locale. J FrOphthalmol 1978;1:139-43.
33. Liou S-W, Yen R-J. The effect of 0.1% indomethacin eyedrops on cataract surgery. J OculPharmacol 1991;7:77-81.
34. Kahan LI, Bögi J, Farkas A, Tüdos F, Imre Gy. Az Indosol – nagy terápiás hatású nemszteroidgyulladásgátló – ismertetése. Acta Pharmaceutica Hungarica 1994; 64:125-9.
35. Van Haeringen NJ, Oosterhuis JA, van Delft JL, Glasius E and Noach EL. A comparison of theeffects of non-steroidal compounds on the disruption of the blood-aqueous barrier. Exp Eye Res1982;35:271-7.
36. Van Sorge AA, Van Nispen tot Pannerden EBLM, Janssen HWM. Oogdruppels met lage con-centratie indometacine: bereidingsvoorschrift en onderzoek naar de werkzaamheid. PharmWeekbl 1986;121:1039-46.
37. Tilden ME, Boney RS, Goldenberg MM and Rosenbaum JT. The effects of topical S[+]-ibuprofenon interleukin-1 induced ocular inflammation in a rabbit model. J Ocul Pharmacol 1990;6:131-5.
38. Tjebbes GWA, van Delft JL, Barthen ER, van Haeringen NJ. d-Ibuprofen in ocular inflammationinduced by paracentesis of the rabbit eye. Prostaglandins 1990;40:29-33.
39. Stampinato S, Marino A, Bucolo C, Canossa M, Bachetti T, Mangiafico S. Effects of sodiumnaproxen eyedrops on rabbit ocular inflammation induced by sodium arachidonate. J OculPharmacol 1991,7:125-133.
40. Van Haeringen NJ, Oosterhuis JA, van Delft JL, Glasius E and Noach EL. A comparison of theeffects of non-steroidal compounds on the disruption of the blood-aqueous barrier. Exp Eye Res1982;35:271-7.
41. Van Haeringen NJ, Glasius E, Oosterhuis JA, van Delft JL. Drug prevention of blood-aqueousbarrier disruption. Ophthalmic research 1983;15:180-4.
42. Anonymous. Flurbiprofen – an ophthalmic NSAID. The Medical Letter 1987;29:58-9.
Preface
15

SCOPE OF THE THESIS
The studies described in this thesis were performed to investigate and to evaluate(1) the pharmaceutical application of flurbiprofen in eyedrops and (2) the pharma-cology of this non-steroidal anti-inflammatory drug - both the racemic form and theindividual enantiomers -, with special reference to the constitutive and induciblecyclooxygenases, COX-1 and COX-2, respectively.
Chapters 2 and 3 cover the pharmaceutical aspects of S(+) flurbiprofen eyedrops,i.e. the formulation, the analysis (including the development of an enantiomericassay), and the chemical and enantiomeric stability under different conditions andperiods of time.
In Chapter 4 the specificity of flurbiprofen and its enantiomers for inhibition ofPGE2 production by COX-1 in the bovine iris/ciliary body was investigated includ-ing the possibility of chiral inversion during the period of incubation.The interaction with the COX-1 and COX-2 isozymes in whole human blood, anextra-ocular matrix, was addressed in Chapter 5. COX-1 activity was monitored bymeasuring TxB2 (the stable metabolite of TxA2) production from platelets whereasCOX-2 activity was determined using PGE2 production in monocytes, followinginduction of this isozyme by LPS. In Chapter 6 the interaction of S(+) flurbiprofenwith COX-1 and COX-2 in the human iris was studied. After LPS-treatment for 24h,substantial amounts of COX-2 immunoreactivity could be visualized for the first timein human iris/ciliary body preparations. Remarkably, S(+) flurbiprofen showed a3,600-fold higher potency for inhibiting COX-1 compared to COX-2. Furthermore,the susceptibility of human iris COX-1 for inhibition by S(+) flurbiprofen was 70-foldhigher than of COX-1 in human blood.
In Chapter 7 99mTc-labeled diflunisal eyedrops were applied in the human eye inan attempt to visualize the internal structures having high(est) COX-activity.Diflunisal was used for radiolabeling instead of S(+) flurbiprofen because the label-ing efficiency of the latter compound was insufficient (Chapter 8). Scintigraphicactivity surrounding the pupil indeed provided clear evidence of visualization of theiris/ciliary body.
In the final Chapter the occurrence of alternative splicing of COX-1 in RNA in thehuman iris was explored, as a possible explanation of the remarkably high affinityof S(+) flurbiprofen for COX-1 reported in Chapter 6.
Preface
16

CHAPTER 1GENERAL INTRODUCTION

1.1 FLURBIPROFEN - AN OVERVIEW
IntroductionFlurbiprofen, CAS registry number (Substance name) 5104-49-4, a member of thephenylalkanoic acids (1), a white (or almost white) crystalline powder, melting point114-117°C, practically insoluble in water, but readily soluble in most organic solvents,also known as a hydratropic acid analog (2), was already subjected for evaluation ofits platelet aggregation inhibiting action in 1973 (3). Chemically it is known as: 2-flu-oro-α-methyl-[1,1'-biphenyl]-4-acetic acid; 2-fluoro-α-methyl-4-biphenyl-acetic acid;2-(2-fluoro-4-biphenylyl)propionic acid; 3-fluoro-4-phenylhydratropic acid (4). In1993 its potent anti-platelet activity was evaluated in a double-blind, placebo-con-trolled, multi-centre study for efficacy on preventing reinfarction and reocclusion aftersuccessful thrombolysis or angioplasty in acute myocardial infarction (5).
Flurbiprofen
Flurbiprofen is described in the recent editions of the United States (USP),European (EP), British Pharmacopoeia (BP) and Japanese Pharmacopoeia (JP). Inthe USP both flurbiprofen and its sodium salt are described in the racemic form. Inthe EP the racemic form is also described; however in the EP and BP monographof flurbiprofen the existence of an enantiomer is alluded to ("and enantiomer"). TheJapanese Pharmacopoeia (JPXIII) gives no hint of the chiral nature of the flur-biprofen molecule. A solution of flurbiprofen in methanol giving no optical rotation isthe only description given thereof.
A monograph for flurbiprofen eyedrops is mentioned in the USP as "Flurbiprofensodium ophthalmic solution" and in the BP as "Flurbiprofen eyedrops". They con-tain not less than 90.0% and not more than 110.0% of the prescribed or statedamount. The sodium salt of flurbiprofen in the USP and BP is available in the dihy-drate form.
In the EP, five impurities for flurbiprofen are mentioned. Interestingly 4 are chiral(one chiral centre) and one diastereomeric in nature (two chiral centers).
18
Chapter 1
FCO2H
CH3

PharmacodynamicsThe major pharmacological properties have already been reviewed by Adam et al.in 1975 (1). Several discriminating techniques were applied to determine the lowesteffective oral dose (mg/kg) as anti-inflammatory, analgesic and antipyretic drug. Inthe anti-inflammatory tests three animal species were used: guinea pig, rat andmouse. In the guinea pig the UV-erythema test was employed in which the referencecompound (acetylsalicylic acid, 80 mg/kg) was found to correspond to 0.25 mg/kg offlurbiprofen. In the mouse model the capillary permeability of the peritoneum wasevaluated by use of a dye (Pontamine sky blue). Acetylsalicylic acid at 120 mg/kgwas equivalent to 0.47 mg/kg of flurbiprofen. In the rat three methods wereemployed: the carageenan edema test, and two adjuvant arthritis models for thedeveloping state and the established state. Reference compounds were, respec-tively, acetylsalicylic acid (81 mg/kg) in the first and indomethacin (1 mg/kg) andphenylbutazone (10 mg/kg) in the two latter models. The corresponding lowest effec-tive dose for flurbiprofen was, 0.11 mg/kg, and 0.33 mg/kg in the two latter models.
With the carageenan edema test a subgroup of rats was also tested who werebilaterally adrenalectomised to rule out any adrenocortical interference. Severalconclusions were drawn from this study. Flurbiprofen was devoid of adrenocortical-stimulating properties and was one of the most potent agents of this type reportedyet; at least 10 times more potent than ibuprofen. It was postulated that the modeof action in the mouse and rat was not identical to that of acetylsalicylic acidIn US patent 3,755,427 (August 28th 1973) (6) it was stated that flurbiprofen wasbetween 75 to over 100 times as potent as acetylsalicylic acid.
In (2) the relative potency of various hydratropic acids were tested for their relaxingability on guinea pig tracheal ring contraction after sensitization by rat SRS-A.Furthermore the paper not only provided information for flurbiprofen but also for thelevorotary (-) and dextrorotary (+) enantiomers. It became apparent that the relaxingpotency of the racemic mixure (±) was unexpectedly too low as compared to the dex-trorotary component suggesting that the dextrorotary component was hindered by thesimultaneous presence of the levorotary component. The putative interactionbetween the two enantiomers was tested by the simultaneous addition of the two sep-arate enantiomers to the muscle bath. Reversal by the dextrorotary component wasdiminished by the simultaneous presence of the (-) flurbiprofen. Taking this in consid-eration (+) flurbiprofen was approximately 80 fold more potent than (-) flurbiprofen.
PharmacokineticsPharmacokinetic properties have been assessed in different species (7). In man(8), when assessed by HPLC of the racemic molecule, a two-compartment openmodel appeared the most appropriate for flurbiprofen. Drug absorption efficiencywas found independent of the oral dose. The intact drug resides mainly in the
19
General introduction

peripheral and central compartments, disappearing with a terminal half life ofapproximately 5.5 hours. More than 99% of flurbiprofen is bound to serum proteins.The serum flurbiprofen concentrations in clinical use however show an occupancyof less than 10% of the primary binding sites. The binding site differs from that ofdrugs like oral anticoagulants and sulphonamides. Drug interactions will thereforenot automatically occur with simultaneous use.
Oxidation and conjugation are the main pathways of metabolism. More than 95%of an oral dose is excreted via the kidney within 24 hours. Forty to 47% of a dailyoral dose is excreted as 2-[2-fluoro-4'-hydroxy-4-biphenylyl]propionic acid; 5% as 2-[2-fluoro-3',4'-hydroxy-4-biphenylyl]propionic acid; 20-30% as 2-[2-fluoro-3'-hydroxy-4'-methoxy-4-biphenylyl]propionic acid and 20-25%. as the parent mole-cule flurbiprofen. Between 65 - 85% of flurbiprofen and its metabolites are presentas glucuronide and sulfate conjugates.
Stereoselective HPLC of human plasma has also been performed (9). After oraladministration of 25 mg of the R(-) enantiomer of flurbiprofen no indication wasfound that inversion to the S(+) enantiomer occurred. This was confirmed in healthyvolunteers taking either 50 mg R(-) flurbiprofen or S(+) flurbiprofen (10). Severalstudies on the pharmacokinetics of flurbiprofen in the rat have been performed allshowing that in this species a minimal amount of inversion could take place(approx. 5%), the inversion halftime being approximately half an hour (11,12,13,14).
Stereoselectieve studies have been performed following the disposition of flur-biprofen in normal volunteers after a single 50 mg racemic dose (15), in healthyfemale subjects following oral administration of the single enantiomers of flurbipro-fen, 50 mg S(+) flurbiprofen or R(-) flurbiprofen or 100 mg R(-) flurbiprofen or place-bo, in a 4-way crossover design with placebo (16); in patients with end-stage renaldisease undergoing continuous ambulatory peritoneal dialysis (CAPD) after admin-istration of a single 100 mg racemic dose (17), and stereoselective disposition ofracemic flurbiprofen in single and multiple dosing in uraemic patients (18). On thebasis of pharmacokinetics, adjustment of flurbiprofen dosing in uraemic patients isnot necessary. In CAPD patients circulating plasma levels of flurbiprofen proved 40-50% lower than in normal subjects implying that analgesia could be less thanexpected in this selected group of patients. Accumulation of the 2-[2-fluoro-4'-hydroxy-4-biphenylyl]propionic acid metabolite, which has minimal anti-inflammato-ry activity, does occur in this group of patients but the clinical significance is notestablished. In patients with liver disease with ascites and in renal failure patientswith a creatinine clearance of less than 10 ml.min-1, significant higher free fractionsof R(-)- and S(+) flurbiprofen were detected in conjunction with lower albumin con-centrations (19). An overview of the clinical pharmacokinetics of flurbiprofen and itsenantiomers is presented in (20).
20
Chapter 1
21
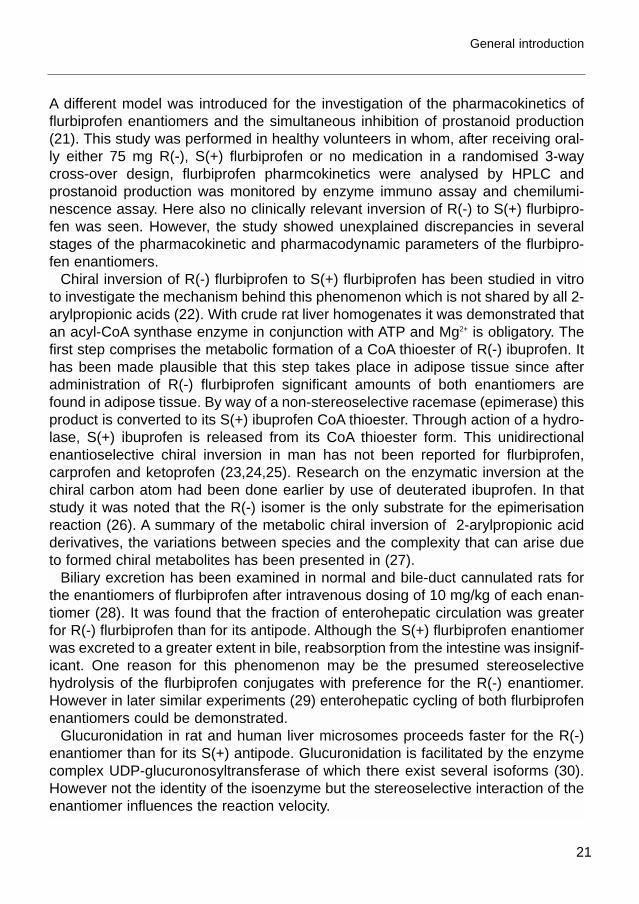
A different model was introduced for the investigation of the pharmacokinetics offlurbiprofen enantiomers and the simultaneous inhibition of prostanoid production(21). This study was performed in healthy volunteers in whom, after receiving oral-ly either 75 mg R(-), S(+) flurbiprofen or no medication in a randomised 3-waycross-over design, flurbiprofen pharmcokinetics were analysed by HPLC andprostanoid production was monitored by enzyme immuno assay and chemilumi-nescence assay. Here also no clinically relevant inversion of R(-) to S(+) flurbipro-fen was seen. However, the study showed unexplained discrepancies in severalstages of the pharmacokinetic and pharmacodynamic parameters of the flurbipro-fen enantiomers.
Chiral inversion of R(-) flurbiprofen to S(+) flurbiprofen has been studied in vitroto investigate the mechanism behind this phenomenon which is not shared by all 2-arylpropionic acids (22). With crude rat liver homogenates it was demonstrated thatan acyl-CoA synthase enzyme in conjunction with ATP and Mg2+ is obligatory. Thefirst step comprises the metabolic formation of a CoA thioester of R(-) ibuprofen. Ithas been made plausible that this step takes place in adipose tissue since afteradministration of R(-) flurbiprofen significant amounts of both enantiomers arefound in adipose tissue. By way of a non-stereoselective racemase (epimerase) thisproduct is converted to its S(+) ibuprofen CoA thioester. Through action of a hydro-lase, S(+) ibuprofen is released from its CoA thioester form. This unidirectionalenantioselective chiral inversion in man has not been reported for flurbiprofen,carprofen and ketoprofen (23,24,25). Research on the enzymatic inversion at thechiral carbon atom had been done earlier by use of deuterated ibuprofen. In thatstudy it was noted that the R(-) isomer is the only substrate for the epimerisationreaction (26). A summary of the metabolic chiral inversion of 2-arylpropionic acidderivatives, the variations between species and the complexity that can arise dueto formed chiral metabolites has been presented in (27).
Biliary excretion has been examined in normal and bile-duct cannulated rats forthe enantiomers of flurbiprofen after intravenous dosing of 10 mg/kg of each enan-tiomer (28). It was found that the fraction of enterohepatic circulation was greaterfor R(-) flurbiprofen than for its antipode. Although the S(+) flurbiprofen enantiomerwas excreted to a greater extent in bile, reabsorption from the intestine was insignif-icant. One reason for this phenomenon may be the presumed stereoselectivehydrolysis of the flurbiprofen conjugates with preference for the R(-) enantiomer.However in later similar experiments (29) enterohepatic cycling of both flurbiprofenenantiomers could be demonstrated.
Glucuronidation in rat and human liver microsomes proceeds faster for the R(-)enantiomer than for its S(+) antipode. Glucuronidation is facilitated by the enzymecomplex UDP-glucuronosyltransferase of which there exist several isoforms (30).However not the identity of the isoenzyme but the stereoselective interaction of theenantiomer influences the reaction velocity.
General introduction

In a review (31) on the binding of flurbiprofen to albumin in human plasma it wasreported that at low therapeutic concentrations the S(+) enantiomer has a higherprotein binding than its R(-) antipode. At high drug concentrations there is no meas-urable difference, however. In an ultrafiltration study done with normal volunteersthe free fraction of R(-) flurbiprofen was higher than its S(+) antipode at low druglevels but similar for both enantiomers at higher drug levels. Patients with renalimpairment and patients exhibiting hypoalbuminaemia have higher free fractions offlurbiprofen enantiomers than normal volunteers. Plasma protein binding of anenantiomer is not influenced by its own concentration or the presence of itsantipode under clinical therapeutic conditions (32).
In a model study using isolated perfused rabbit lungs it was demonstrated thatflurbiprofen does not undergo pulmonary metabolism to any extent (33).
As mentioned above (8) the main routes of biotransformation of flurbiprofen arethrough oxidation and conjugation. Oxidation has been investigated more specifi-cally (34) for the enantiomers of flurbiprofen utilizing human liver microsomes. Themost prominent oxidative metabolism route is by cytochrome P450. It was estab-lished that cytochrome P450 2C9 and its allelic variant R144C catalysed the oxida-tive reaction. Interestingly, there was no stereoselective preference of one enan-tiomer over the other.
Safety for intestinal permeability changes when using the racemate or the sepa-rate enantiomers of flurbiprofen was studied in rats for which species it was estab-lished that only a minimal inversion of the R(-) enantiomer takes place. Intestinalpermeability was measured by urinary excretion of 51Cr-EDTA (35). It was estab-lished that at both dosages used (1 mg/kg and 3 mg/kg for the racemic drug andhalf for the enantiomers) permeability was significantly different from control. R(-)flurbiprofen was safest in both dosage ranges. S(+) flurbiprofen inflicted similardamage as the racemic form.
In (36) it was shown that in rats R(-) flurbiprofen gave the same increase of intes-tinal permeability, but the difference was that the impact on mucosal prostanoid pro-duction was smaller and not accompanied by ulcerative changes in the small intes-tine.
Although it would seem attractive to develop therapeutic R(-) enantiomers of 2-arylproionic acids due to its supposedly lower toxicological profile it must be bornein mind that the presumed pharmacological action required for reducing inflamma-tion is inhibition of prostaglandin synthesis. This property resides primarily, in thecase of flurbiprofen, in the S(+) enantiomer for which a difference of 30 to 100 timescompared to the R(-) enantiomer was established depending on the model used.Only with full metabolic inversion of a R(-) enantiomer to a S(+) enantiomer wouldsuch a therapeutic drug be a possibility. For flurbiprofen this is not the case inhumans (37,38,39).
22
Chapter 1

In a comparative study (40) done in rabbits, the inhibitory effect on rise in intraocu-lar pressure and increase in aqueous humor protein after topical application ofarachidonic acid (5% in peanut oil) by 14 nonsteroidal anti-inflammatory inhibitorswas measured. For 50% inhibition of the intraocular pressure response, flurbipro-fen ranked second best with an effective concentration of approximately 0.06%.Indomethacin (suspension in water, not further specified) ranked 4th with an approx-imate concentration of 0.2%.
In a short review (41) the importance of the involvement of prostaglandins to cer-tain eye conditions is discussed. The rise in intraocular pressure and the break-down of the blood-aqueous barrier were related to these compounds. A search forthe best drug in inhibiting prostaglandin mediated diseases was called for beforetesting them in the human eye.
The comparative in vivo inhibitory effects of flurbiprofen, indomethacin and acetyl-salicylic acid, all as sodium salt solutions, have been tested in the rabbit anterioruvea and conjunctiva after topical (0.5% solutions) and intraperitoneal administra-tion (42). In both methods of administration acetylsalicylic acid almost completelyabolished prostaglandin synthesis. Flurbiprofen given intraperitoneally was morepotent than indomethacin which inhibited prostaglandin synthesis only partially,even at twice the dose of acetylsalicylic acid and flurbiprofen. Topical administrationrevealed that acetylsalicylic acid performed well even at a dose as low as 0.01%but indomethacin and flurbiprofen performed poor.
Use of flurbiprofen (0.01% and 0.1%) was evaluated in comparison to 1% pred-nisolone as an inhibitor of corneal neovascularization in New Zealand albino rab-bits (43). Flurbiprofen 0.1% and prednisolon 1% were equally effective in inhibitingvessel growth.
As an alternative possibility for the use of topical administration of corticosteroidsa nonsteroidal anti-inflammatory drug was considered (44). Flurbiprofen was test-ed in a double-blind fashion to see if intraocular pressure would change and if itsuse could block corticosteroid induced ocular hypertension. In a selected group ofpatients, with known intraocular sensitivity towards corticosteroids, flurbiprofen eye-drops (0.03%) did not alter intraocular pressure following six weeks of treatment.Also pretreatment by flurbiprofen did not block corticosteroid-induced ocular hyper-tension.
Flurbiprofen was also investigated for human use in the prevention of intraocularinflammation (45). In a randomised double-blind parallel group study, placebo orflurbiprofen (100 mg thrice daily) was given orally for 8 days starting 24 hoursbefore routine cataract extraction. Flurbiprofen was only favoured over placebo forthe resolution of corneal inflammation at day 6. Interestingly, flurbiprofen concen-trations in the aqueous were detected up to 4 hours after the last dose with a con-
23
General introduction

centration of 0.57 mg/L (2.3x10-6M). The authors conclude that flurbiprofen may beof value in the treatment of uveitis and other kinds of intraocular inflammation. In a study (46) involving female New Zealand rabbits, eyedrop disposition was stud-ied after application of 14C labeled flurbiprofen in a concentration of 0.03%. Nometabolism was detected for flurbiprofen in the eye. The total amount present inocular tissues (cornea, aqueous humor, iris, ciliary body, choroid and retina) in nor-mal rabbit eyes 30 minutes after application of 50 microliter of a 0.03% solution,was 4.25%. At 6 hours this was 1.59%. Following ocular application 77.51±8.79%was found in a 24-urine collection period. Unchanged flurbiprofen accounted for25.3±3.6%.
Ocular availability was studied in female albino rabbits (47) receiving 50 microliterof 0.3% or 0.15% solution of flurbiprofen. The ocular bioavailability of the 0.3% solu-tion was 10% and for the 0.15% solution 7%. The elimination half-life in the aque-ous humor was 93 minutes which approximates the turnover rate of aqueous humorin the rabbit and indicates that drainage is the main route of elimination.
Bioavailability was determined after a single dose and after multiple doses oflabeled flurbiprofen in rabbit eyes using topical application (48). Multiple dosing ofa flurbiprofen solution of 0.03%, every half hour three doses, gave levels in the eyehigh enough to prevent prostaglandin synthesis. It compared favourably to the useof a single drop of 0.1% solution possibly because of less irritation of the eye andthus less stimulation of tear flow. Peak tissue concentrations were reached between30 minutes and 60 minutes and were 2 to 6 times higher in all tissues than seenafter one drop of 0.1% solution.
To determine the intraocular concentration of flurbiprofen sodium in the humanaqueous humor of patients undergoing cataract surgery, samples were taken afterreceiving flurbiprofen sodium at selected times prior to surgery (49). Only singledrop instillation was done. Samples of aqueous humor were analysed by HPLC.Flurbiprofen concentrations were detectable in the aqueous between 30 minutes to7.25 hours after topical application.
To determine if and how much drug can penetrate to the posterior segment of theeye, a study was done in white New Zealand albino rabbits, by single drop methodof dosing, using paracetamol 1% in saline and bendazac lysine 0.5% in saline orother solvent (50). When comparing the data with literature data it appeared thatparacetamol behaved similar to flurbiprofen as regards penetration into the aque-ous humor, having a very poor entry into the vitreous and attaining higher concen-trations in the retina than paracetamol. In all three eye compartments bendazaclysine permeated poorly. The data suggest an alternative entry route to the poste-rior segments of the eye. It appears that the lens acts as a barrier for the entry fromthe aqueous.
24
Chapter 1

In a study done by Carabaza et al. inhibition of prostaglandin synthesis was inves-tigated using the enantiomers of three NSAIDs (ketoprofen, flurbiprofen and ketoro-lac), including stereoselective inhibition of inducible COX-2 (51). It became appar-ent that inhibition by the three enantiomer pairs is comparable for COX-1 and COX-2. With both cyclooxygenase isoenzymes inhibition resides almost exclusively inthe S(+) isomer.
One of the most frequent problems encountered during cataract surgery is invol-untary pupillary constriction. In the past, several pharmacological interventionshave been tried as a remedy, but without success. Albino rabbits have been usedto study the effect of topical administration of indomethacin (1% aqueous solutionwith no further specification of buffer and pH used) and flurbiprofen (0.03% aque-ous solution of sodium flurbiprofen) on this unwanted condition (52). In this set-upalso local anaesthetics, capsaicin, sympathomimetic agents and an anticholinergicwere involved all according to a specified protocol. Flurbiprofen demonstrated asignificant inhibitory effect on miosis while topical indomethacin failed. However nosingle agent or combination of agents blocked the miotic response completely.
Although nonsteroidal anti-inflammatory drugs are pharmacologically effectiveinhibitors of cyclooxygenase activity and prostaglandin synthesis (53), cyclooxyge-nase-independent anti-inflammatory actions of NSAIDs are also known (54). Sinceit was reported that sodium salicylate and acetylsalicylic acid inhibit the action of thetranscription factor nuclear factor kappa B (NF-κB), the enantiomers of flurbiprofenwere tested in a zymosan-induced paw inflammation model. Although R(-) flur-biprofen does not inhibit cyclooxygenase to a significant extent, it is more potentthan S(+) flurbiprofen and almost as effective as dexamethasone in this inflamma-tory model. Inhibition of NF-κB by R(-) flurbiprofen resulted in a reduced expressionof COX-2 and tumor necrosis factor a (TNF-α).
Nitric oxide formed by the inducible NO synthase (iNOS) has been implicated asa mediator of pain and tissue injury in various inflammatory and autoimmune dis-eases. In an in vitro model involving RAW 264.7 macrophages, it could be demon-strated that iNOS mRNA expression is equipotently suppressed by the enantiomersof flurbiprofen. S(+) flurbiprofen and R(-) flurbiprofen did not inhibit LPS inducedCOX-2 mRNA expression but did inhibit LPS-induced prostaglandin E2 formationenantioselectively, with the S(+) antipode being 46 times more active than the R(-)flurbiprofen (IC50 0.0061µM and 0.28 µM respectively). Collectively, these findingswould suggest that the pharmacological (i.e. anti-inflammatory) activity of the flur-biprofen enantiomers is not only related to inhibition of cyclooxygenase enzymeactivities but also to inhibition of transcription factor activition like NF-κB and AP-1,resulting in diminished formation of pro-inflammatory factors like iNOS and TNF-α(55,56).
25
General introduction

26
REFERENCES
1. Adam SS, McCullough KF, Nicholson JS. Some biological properties of flurbiprofen, an anti-inflammatory, analgesic and antipyretic agent. Arzneim Forsch (Drug Research) 1975;25:1786-91.
2. Greig ME, Griffin RL. Antagonism of slow reacting substance in anaphylaxis (SRS-A) and otherspasmogens on the guinea pig tracheal chain by hydratropic acids and their effects on anaphy-laxis. J Med Chem 1975;18:112-116.
3. Nishisawa EE, Wynalda DJ, Suydam DE Molony BA. Flurbiprofen, a new potent inhibitor ofplatelet aggregation. Thrombosis research 1973;3:577-88.
4. The Merck Index, Thirteenth Edition, 2001, Merck & Co., Inc. Whitehouse Station, N.J., USA. 5. Brochier ML. Evaluation of flurbiprofen for prevention of reinfarction and reocclusion after suc-
cessful thrombolysis or angioplasty in acute myocardial infarction. The flurbiprofen French trial.Eur Heart J 1993;14:951-7.
6. US patent 3,755,427 (August 28th, 1973).7. Risdall PC, Adams SS, Crampton EL, Marchant B. The disposition and metabolism of flurbiprofen
in several species including man. Xenobiotica 1978;8:691-704.8. Kaiser DG, Brooks CD, Lomen PL. Pharmacokinetics of flurbiprofen. Am J Med 1986;80:10-5
(suppl 3A).9. Jamali F, Berry BW, Tehrani MR, Russell AS. Stereoselective pharmacokinetics of flurbiprofen in
humans and rats. J Pharm Sci 1988;77:666-9.10. Geisslinger G, Menzel-Soglowek S. Stereoselective high-performance liquid chromatographic
determination of flurbiprofen in human plasma. J Chromatogr 1992;573:163-7.11. Knihinicki RD, Day RO, Graham GG, Williams KM. Stereoselective disposition of ibuprofen and
flurbiprofen in rats. Chirality 1990;2:134-40.12. Jamali F, Berry BW, Wright MR. Dose-dependency of flurbiprofen enantiomer pharmacokinetics
in the rat. J Pharm Sci 1994;83:1077-80.13. Peskar BM, Kluge S, Peskar BA, Soglowek SM, Brune K. Effects of pure enantiomers of flur-
biprofen in comparison to racemic flurbiprofen on eicosanoid release from various rat organs exvivo. Prostaglandins 1991;42:515-31.
14. Berry BW, Jamali F. Enantiomeric interaction of flurbiprofen in the rat. J Pharm Sci 1989;78:632-4.15. Knadler MP, Brater DC, Hall SD. Stereoselective disposition of flurbiprofen in normal volunteers.
Br J Clin Pharmacol 1992;33:369-75.16. Geisslinger G. Stereoselective disposition of flurbiprofen in healthy subjects following adminis-
tration of the single enantiomers. Br J Clin Pharmacol 1994; 37:392-4.17. Cefali EA, Poynor WJ, Sica D, Cox S. Pharmacokinetic comparison of flurbiprofen in end-stage
renal disease subjects and subjects with normal renal function. J Clin Pharmacol 1991;31:808-14.18. Knadler MP, Brater DC, Hall SD. Stereoselective disposition of flurbiprofen in uraemic patients.
Br J Clin Pharmacol 1992;33:377-83.19. Blouin R, Chaudhary I, Nishikara K, Cox S. The effects of liver and renal disease on stereoselective
serum binding of flurbiprofen. Br J Clin Pharmacol 1993;35:62-4.20. Davies NM. Clinical pharmacokinetics of flurbiprofen and its enantiomers. Clin Pharmacokinet
1995;28:100-14.21. Oelkers R, Neupert W, Williams KM, Brune K, Geisslinger G. Disposition and effects of flurbipro-
fen enantiomers in human serum and blister fluid. Br J Clin Pharmacol 1997;43:145-53.22. Knihinicki RD, Williams KM, Day RO. Chiral inversion of 2-arylpropionic acid non-steroidal anti-
inflammatory drugs-1. In vitro studies of ibuprofen and flurbiprofen. Biochem Pharmacol1989;38:4389-95.
23. Mayer JM. Stereoselective metabolism of anti-inflammatory 2-arylpropionates. Acta Pharm Nord1990;2:197-216.
Chapter 1

27
24. Knadler MP, Hall SD. Stereoselective arylpropionyl-CoA thioester formation in vitro. Chirality1990;2:67-73.
25. Wechter WJ. Drug chirality: on the mechanism of R-aryl propionic acid class NSAIDs.Epimerization in humans and the clinical implications for the use of racemates. J Clin Pharmacol.1994;34:1036-42.
26. Wechter WJ, Loughhead DG, Reischer RJ, VanGiessen GJ, Kaiser DG. Enzymatic inversion at sat-urated carbon: nature and mechanism of the inversion of R(-) p-iso-butyl hydratropic acid. BiochemBiophys Res Commun. 1974;61:833-7.
27. Caldwell J, Hutt AJ, Fournel-Gigleux S. The metabolic chiral inversion and dispositional enan-tioselectivity of the 2-arylpropionic acids and their biological consequences. Biochem Pharmacol1988;105-14.
28. Menzel S, Beck WS, Brune K, Geisslinger G. Stereoselectivity of biliary excretion of 2-arylpropi-onates in rats. Chirality 1993;5:422-7.
29. Eeckhoudt SL, Evrard PA, Verbeeck RK. Biliary excretion and enterohepatic cycling of R- and S-flurbiprofen in the rat. Drug Metab Dispos 1997;25:428-30.
30. Hamdoune M, Mounie J, Magdalou J, Masmoudi T, Goudonnet H, Escousse A. Characterizationof the in vitro glucuronidation of flurbiprofen enantiomers. Drug Metab Dispos 1995;23:34308.
31. Lapicque F, Muller N, Payan E, Dubois N, Netter P. Protein binding and stereoselectivity of non-steroidal anti-inflammatory drugs. Clin Pharmacokinet 1993; 25:115-25.
32. Knadler MP, Brater DC, Hall SD. Plasma protein binding of flurbiprofen: enantioselectivity and influ-ence of pathophysiological status. J Pharmacol Exp Ther 1989; 249:378-85.
33. Hall SD, Hassazadeh-Khayyat M, Knadler MP, Mayer PR. Pulmonary inversion of 2-arylpropionicacids: influence of protein binding. Chirality 1992;4:349-52.
34. Tracy TS, Rosenbluth BW, Wrighton SA, Gonzalez FJ, Korzekwa KR. Role of cytochrome P4502C9 and an allelic variant in the 4’-hydroxylation of (R)- and (S) flurbiprofen. Biochem Pharmacol1995;49:1269-75.
35. Davies NM, Wright MR, Russell AS, Jamali F. Effect of the enantiomers of flurbiprofen, ibuprofen,and ketoprofen on intestinal permeability. J Pharm Sci 1996;85:1170-3.
36. Mahmud T, Somasundaram S, Sigthorsson G, Simpson RJ, Rafi S, Foster R, Tavares IA, RosethA, Hutt AJ, Jacob M, Pacy J, Scott DL, Wrigglesworth JM, Bjarnason I. Enantiomers of flurbipro-fen can distinguish key pathophysiological steps of NSAID enteropathy in the rat. Gut1998;43:775-82.
37. Wright MR, Davies NM, Jamali F. Rationale for the development of stereochemically pure enan-tiomers: are the R enantiomers of chiral nonsteroidal anti-inflammatory drugs inactive? J PharmSci 1994;83:911-2.
38. Menzel-Soglowek S, Geisslinger G, Beck WS, Brune K. Variability of inversion of (R)-Flurbiprofenin different species. J Pharm Sci 1992;81:888-91.
39. Geisslinger G, Menzel-Soglowek S, Beck WS, Brune K. R-flurbiprofen: isomeric ballast or activeentity of the racemic compound? Agents Actions Suppl 1993;44:31-6.
40. Podos SM, Becker B. Comparison of ocular prostaglandin synthesis inhibitors. Invest Ophthalmol1976;15:841-4.
41. Podos SM. Prostaglandins, nonsteroidal anti-inflammatory agents and eye disease. Trans AmOphthalmol Soc 1976;74:637-60.
42. Kulkarni PS, Srinivasan D. Comparative in vivo inhibitory effects of nonsteroidal anti-inflammato-ry agents on prostaglandin synthesis in rabbit ocular tissues. Arch Ophthalmol 1985;103:103-6.
43. Cooper CA, Bergamini MVW, Leopold IH. Use of flurbiprofen to inhibit corneal neovasculariza-tion. Arch Ophthalmol 1980;1102-5.
44. Gieser DK, Hodapp E, Goldberg I, Kass MA, Becker B. Flurbiprofen and intraocular pressure.Ann Ophthalmol 1981;13:831-3.
General introduction

28
45. Hillman JS, Frank GJ, Kheskani MB. Flurbiprofen and human intraocular inflammation. InAdvances in prostaglandin and thromboxane research. Vol 8;1723-5:1980. Edited by B.Samuelsson, P.W. Ramwell, and R. Paoletti. Raven Press New York, USA.
46. Anderson JA, Chen CC, Vita JB, Shackleton M. Disposition of topical flurbiprofen in normal andaphakic rabbit eyes. Arch Ophthalmol 1982;100:642-5.
47. Tang-Liu DD-S, Liu SS, Weinkam RJ. Ocular and systemic bioavailability of ophthalmic flur-biprofen. J Pharmacokinet Biopharm 1984;12:611-26.
48. Anderson JA, Chen CC. Multiple dosing increases the ocular bioavailability of topically adminis-tered flurbiprofen. Arch Ophthalmol 1988;106:1107-9.
49. Ellis PP, Pfoff DS, Bloedow DC, Riegel M. Intraocular diclofenac and flurbiprofen concentrationsin human aqueous humor following topical application. J Ocular Pharmacol 1994;10:677-82.
50. Romanelli L, Morrone LA, Guglielmotti A, Piccinelli D, Valeri P. Distribution of topically adminis-tered drugs to the posterior segment of rabbit eye. Pharmacol Res 1992;25: 39-40 (Suppl 1).
51. Carabaza A, Cabre F, Rotlan E, Gomez M, Gutierrez M, Garcia ML, Mauleon D. Stereoselectiveinhibition of inducible cyclooxygenase by chiral nonsteroidal antiinflammatory drugs. J ClinPharmacol 1996;36:505-12.
52. Duffin RM, Camras CB, Gardner SK, Pettit TH. Inhibitors of surgically induced miosis.Ophthalmology 1982;89:966-79.
53. Versteeg HH, van Bergen en Henegouwen PMP, van Deventer SJH, Peppelenbosch MP.Cyclooxygenase-dependent signalling: molecular events and consequences. FEBS 1999;445:1-5.
54. Tegeder I, Pfeilschifter J, Geisslinger G. Cyclooxygenase-independent actions of cyclooxygenaseinhibitors. FASEB J 2001;15:2057-72.
55. Tegeder I, Niederberger E, Israr E, Gühring H, Brune K, Euchenhofer C, Grösch S, Geisslinger G.Inhibition of NF-κB and AP-1 activation by R- and S-flurbiprofen. FASEB J 2001;15:2-4; and 595-7. To read full text: http://www.fasebj.org/ cgi/doi/10.1096/fj.00-0130fje.
56. Hinz B, Brune K, Rau T, Pahl A. Flurbiprofen enantiomers inhibit inducible nitric oxide synthaseexpression in RAW 264.7 macrophages. Pharm Res 2001;18:151-6.
Chapter 1

1.2 CATARACT AND CATARACTOGENESIS
CataractAlterations in lens transparency increase with age. It seems possible that the lensstays transparent until the age of 120 years. In the fifth decade of life howeverapproximately 65% of people will have some form of lens opacity. This can varyfrom small spots to complete opacification. The patient will not immediately noticethe development of cataractogenesis as this process does not proceed with anovert inflammatory process nor is any pain experienced. Symptoms accompanyingsuch a process are difficulty in reading, in recognizing faces, watching television,seeing in bright light and during driving (1,2). A simple test is available to assessvisual function, the Snellen chart, but reliability warrants consideration (3).
On a global scale cataract is the commonest cause of visual disability and by farthe single largest cause of blindness (4). Traditional eye medicines in rural Africainflict corneal ulcers and cause blindness in children in a quarter of cases (5). Thebest known medication to cause cataracts are corticosteroids (6) with evidence thatphenothiazines, amiodarone, chloroquine and possibly acetylsalicylic acid alsomight be associated with increased risk (7). There are still limitations in the identifi-cation of the causes of cataracts, not only in developing countries but also in indus-trialised countries (8). Research is ongoing to gain a better understanding of thegenetics of human cataract. It can be envisaged that knowledge of congenitalcataract will provide more insight into the putative role of genes in age-relatedcataract (9).
There is still no effective, pharmacological, remedy for established cataractsalthough a theoretical and experimental basis is building up to address age-onsetcataractogenesis by anti-cataract agents (10).
Treatment is purely surgical with an established success rate >90%. Two basictechniques are in use for management: extracapsular cataract surgery and intra-capsular cataract surgery.
The surgical removal of an opacified lens was first reported in 1745 (April 8th,Marseille) performed by Jacques Daviel (1693-1762). In 1752 two lectures werepresented by him at the Académie Royale de Chirurgie in Paris where an accountwas given of 206 lens extractions. Of these 182 were successful: 88%. Almost twocenturies later Sir Harold Ridley performed the first successful lens implantation(London, November 29th 1949).
Innovation is still improving cataract surgery, especially by the technologicaladvancement of extracapsular extraction and posterior-chamber intraocular lensimplantation (11). These substantial improvements should become available to anincreasing group of patients on the waiting list (12,13,14). Outpatient cataract sur-
29
General introduction

gery seems very well possible without loss of quality (15). Bilateral cataract extrac-tion can be safely done within 48 hours (16).
CaractogenesisAge related, or senile cataract is the most common form and inflicts blindnessworldwide. There are two types of age-related cataract, nuclear and cortical. Oneof the possibilities that has been investigated for nuclear caractogenesis is throughhydroxyl radical-attack of lens proteins which causes cross-linking and proteinaggregation, ultimately resulting in opacity of the lens (17). In another model it isproposed that cataract is essentially a conformational disease in which non-enzy-matic modification of amino groups e.g. by sugars and steroids destabilize the lensproteins and causes conformational changes. The interaction between the aminoacid of a lens protein and a sugar, well known as the Maillard reaction, will not onlygive rise to a colored reaction product but will also cause the protein to cross-link,aggregate and eventually to become insoluble which in turn will opacify the lens(18). In another sugar-related process it was investigated whether the polyol path-way was involved in the process of cataractogenesis. By the enzyme aldose reduc-tase glucose can be converted to sorbitol. However, when a limited amount ofantioxidants is available a significant amount of hydrogen peroxide can be formed.This will give rise to the production of hydroxyl radicals and will lead to the initialstage of a "sugar" cataract (19). Another reported mechanism on the formation ofcataract was the kynurenine metabolic pathway. The tryptophan metabolite, 3-hydroxykynurenine is present at elevated concentrations in the lens and is able toabsorb UV radiation. However, an excessive amount in the lens has been report-edly associated with cataract formation. In the rabbit eye enzymes, leading to theformation of this metabolite, are present in the iris/ciliary body. The formed metabo-lite is taken up by the lens for formation of UV-filtering products. If however anexcess of 3-hydroxykynurenine is present in the lens, free radical formation mayoccur, which will ultimately lead to tissue injury like lens opacification (20,21).Oxidative damage of lens proteins seems to be a major factor in cataract formation.A threshold of protein oxidation has been identified at which opacification will takeplace (22). Radiation-induced cataractogenesis will commence above 1 Gy as hasbeen observed in survivors of the Hiroshima and Nagasaki atomic bombs (23).
The lens is not a purely passive optical element but maintains an internal circula-tion for lens transparency. Sodium-potassium pumps have been identified in thelens as well as a major intrinsic protein belonging to the aquaporin family of waterchannels. Glucose is transported from the aqueous humor to the lens for energysupport. It has been postulated that dysfunction of any of these links in this chainof events may ultimately lead to cataract formation (24).
30
Chapter 1

31
General introduction
REFERENCES
1. Elkington AR, Khaw PT. Cataracts. BMJ 1988;296:1787-90.2. Cotlier E. The Lens in: Adler's Physiology of the eye. Clinical application. Chapter 10; 6th Edition
1975. RA Moses, MD Editor. The CV Mosby Company ISBN 0-8016-3540-3.3. McGraw P, Winn B, Whitaker D. Reliability of the Snellen chart (Better charts are now available).
BMJ 1995;1481-2.4. Thylefors B, Négrel A-D, Pararajasegaram R, Dadzie KY. Global data on blindness. Bull WHO
1995;73:115-21.5. Anonymous. Traditional eye medicines: a note of concern. WHO Drug information 1995;9:152-3.6. Butcher JM, Austin M, Mc Galliard J, Bourke RD. Bilateral cataracts and glaucoma induced by
long term use of steroid eyedrops. BMJ 1994;309:43.7. Cumming RG, Mitchell P. Medications and cataract (The blue mountains eye study).
Ophthalmology 1998;105:1751-8.8. Johnson GJ. Limitations of epidemiology in understanding pathogenesis of cataracts. Lancet
1998;351:925-6,9. Francis PJ, Berry V, More AT, Bhattacharya S. Lens biology; development and human catarac-
togenesis. TIG 1999;15:1916.10. Benedek GB, Pande J, Thurston GM, Clark JI. Theoretical and experimental basis for the inhibi-
tion of cataract. Progress in retinal and eye research. 1999;18:391-402.11. Tielsch JM. Appropriate technology for cataract surgery. Lancet 1998;352:754-5.12. Gray CS, Crabtree HL, Oçonnell JE, Allen ED. Waiting in the dark: cataract surgery in older peo-
ple (We need a better means of assessing priorities for surgery). BMJ 1999;318:1367-8.13. Allan B. Intraocular lens implants (Have come a long way, but the advances are not yet available
to all). BMJ 2000;320:73-4.14. Fielder AR, Watson MP, Seward HC, Murray PI. Action on cataracts should influence surgical
training. BMJ 2000;321:639.15. Javitt JC, Street DA, Tielsch JM, Wang Q, Kolb MM, Schein O, SommerA, Bergner M, Steinberg
EP, on behalf of the Cataract Patient Outcomes Research team. Ophthalmology 1994;101:100-6.16. Booth A, Coombes A, Rostron C. Bilateral cataract extraction can be safely done within 48 hours.
BMJ 1999;319:579.17. Fu S, Dean R, Southan M, Truscott R. The hydroxyl radical in lens nuclear catractogenesis. J Biol
Chem 1998;273:28603-9.18. Crabbe MJC. Cataract as a conformational disease - the maillard reaction, alpha-crystallin and
chemotherapy. Cell Mol Biol 1998;44:1047-50.19. Kubo E, Miyoshi N, Fukuda M, Akagi Y. Cataract formation through the polyol pathway is asso-
ciated with free radical production. Exp Eye Res 1999;68:457-64.20. Chiarugi A, Rapizzi E, Moroni F, Moroni F. The kynurenine metabolic pathway in the eye: studies
on 3-hydroxykynurenine, a putative cataractogenic compound. FEBS1999;453:197-200.21. Davies MJ, Truscott RJW. Photo-oxidation of proteins and its role in cataractogenesis. J Photo
Biol 2001;63:114-25.22. Boscia F, Grattagliano I, Vendemiale G, Micelle-Ferrari T, Altomar E. Protein oxidation and lens
opacity in humans. Invest Ophthalmol Vis Sci 2000;41:2461-5.23. Belkacémi Y, Touboul E, Méric JB, Rat P, Warnet JM. Cataract radio-induit: aspects phys-
iopathologiques, radiobiologiques et cliniques. Cancer/Radiother 2001;5:397-412.24. Donaldson P, Kistler J, Mathias RT. Molecular solutions to mammalian lens transparency. News
Physiol Sci 2001;16:118-23.

1.3 CYSTOID MACULAR EDEMA
In 1942 a report was published on a toxic ocular reaction. The characteristic findingwas that the primary aqueous (aqueous humor obtained on a first paracentesis) didcoagulate in contrast to the usual finding that coagulation only takes place in sec-ondary aqueous (aqueous humor obtained on a second paracentesis). The natureof this phenomenon in the - as it was termed - plasmoidtoxic aqueous- of the primaryaqueous, was investigated in some detail. Although no exact culprit could be definedit became clear that the increased permeability of the ciliary body was a major con-tributing factor in the toxic ocular reaction and that the fibrinogen system played anessential role in the coagulation process of the plasmoidtoxic aqueous (1).
In 1953 a paper was published in which a complication was described followingcommon intracapsular cataract extraction. One of the features of this complicationwas the development of postoperative macular changes, and of ultimate reductionof vision as a result of vitreous opacities or macular degeneration. Of the 1,068cataract extractions 894 were intracapsular extractions. Of these 483 occurredintact; the remaining 222 showed complications varying from marked prolapse of thevitreous into the anterior chamber without rupture to late rupture of the anteriorhyaloid with or without adhesions. The percentage of patients encountered with poorvision as a result of vitreous opacities or macular degeneration was found to be 2%.This was similar to the postoperative detachment of the retina after cataract surgery,as found in a total of reviewed 1,200 cases (2).
In 1966 a new study was presented showing the advantage of the use of intra-venous sodium fluoresceinate to detect the lesion. It was demonstrated that resolu-tion of fluorescein leakage into the retina and optic nerve generally parallels the clin-ical resolution of edema of the macula and optic disc. The earlier reports of an inci-dence of 2% of cystoid macular edema was questioned and it was expected to behigher as experience was gained with this new staining technique (3).
A review on the complication of cystoid macular edema in 1976 showed that thiscomplication following cataract surgery was the most common and troublesome (4).The progress in surgical techniques was impressive enough to diminish the majori-ty of complications other than cystoid maculopathy. The incidence of clinically sig-nificant cystoid macular edema remained 2 - 6%. In an attempt to grasp the etiolog-ical factors the author (A.R. Irvine) put forward the possibility of "vasoactive factorsfrom inflammatory cells in the vitreous to penetrate the retina preferentially at themacula and disc". Of the possibilities to produce aphakic cystoid macular edema,inflammation and increased permeability were major steps in the reaction sequence.Medication seemed straight forward as to use steroids. However oral therapy provedof transient value just like periocular steroid injections and had unfavourable sideeffects. Topical steroid therapy was found to be ineffective. New perspectives
32
Chapter 1

appeared following the elucidation of the role of prostaglandins in inflammatory vas-cular permeability changes. However the controlled study mentioned in this reviewusing indomethacin (orally 25 mg tid for 3 weeks) failed to demonstrate any benefi-cial effect (4).
In 1985 a hypothesis was put forward for aphakic cystoid macular edema. Basedon the results of a randomised double blind trial that showed a reduction in incidenceof 50% for aphakic cystoid macular edema by use of an ultraviolet radiation-absorb-ing chromophore in a posterior chamber intraocular lens, it was postulated that post-operative exposure to near-ultraviolet radiation generates free radicals. These radi-cals would facilitate the synthesis of inflammatory mediators like prostaglandins.Prostaglandins are involved in the breakdown of blood-ocular barriers. It follows thata combination of factors like UV-A radiation and the synthesis of prostaglandins is apossibility worth testing as a contributing factor toward cystoid macular edema andtherefore amenable to medical treatment (5).
In an update of the pharmacological therapy it was mentioned that topical non-steroidal anti-inflammatory agents were still not commercially available. However,topical indomethacin was mentioned as the one agent effective in the prophylaxis ofangiographic aphakic cystoid macular edema. Other nonsteroidal anti-inflammatoryagents and corticosteroids are mentioned but no evidence was presented other thananecdotal, not detailed enough or in number too small to evaluate statistically (6).
Further studies on cystoid macular edema revealed that any disturbance of the vit-reous can lead to this syndrome. In particular three possibilities are mentioned bywhich intraocular lenses can give rise to chronic cystoid macular edema (7). Theseare iris chaffing in combination with an uveitis-glaucoma-hyphema syndrome afterposterior chamber intraocular lens implantation, movement of the intraocular lens withintermittent corneal touchings and the corneo-retinal inflammatory syndrome com-promising both the cornea and the retina. When one of these three situations occurintraocular lens removal is required to prevent permanent macular damage (7).
Cystoid macular edema has also been described in the French literature as Irvine-Gass syndrome. An extensive treatise is presented in (8).
In the German literature a report was published on the safety and efficacy of a 1%indomethacin suspension for the prevention of cystoid macular edema (also knownas Irvine-Gass-Norton syndrome or Irvine syndrome). The incidence of cystoid mac-ular edema was 1.34%. Side effects of the eyedrops, as observed in 10% of thecases, were mainly conjunctival in origin (9). Another pharmacological approach forfailing visual acuity, local application of steroids and an injection of tolazoline (α-adrenergic antagonist, having some cholinergic, H2-histaminergic, and 5HT1 recep-tor antagonistic properties as well) in Tenon's capsule, is proposed (10).
In the meantime the FDA has approved several topical NSAIDs for clinical use inophthalmology (11). The approvals are restricted to specific indications, however;
33
General introduction

flurbiprofen sodium and suprofen for the prophylaxis of surgical miosis, ketorolac forthe relief of itching due to allergic conjunctivitis and diclofenac for the treatment ofpostcataract inflammation. For intraoperative miosis no conclusive evidence hasbeen presented that an NSAID is effective. For the prevention of postcataract surgi-cal inflammation the NSAIDs are at least as effective and perhaps more effectivethan corticosteroids in preventing disruption of the blood-aqueous barrier. For cys-toid macular edema the evidence is that topical NSAIDs are better than topical cor-ticosteroids.
In a Canadian report the incidence of aphakic/pseudophakic cystoid macularedema in 90 studies from 1979 to 1991 is presented using three different techniques(12). For intracapsular and extracapsular cataract extraction and the phacoemulsifi-cation technique it varied between 2 - 10%, 0 - 7.6% and 0.6 - 6.0%, respectively.However when using fluorescein angiography the incidence varied between 40 -60%, 2.7 - 11.3% and 2.1 - 6.0%, respectively. Interestingly, aphakic cystoid macu-lar edema occurs more frequently with intracapsular than extracapsular cataractextraction, and even less with placement of an intraocular lens in an intact capsularbag. It seems that the capsular bag encompasses properties other than just for sup-port. The lens barrier protects, it seems, against access of inflammatory agents intothe vitreous. Permanent visual impairment due to cystoid macular edema will varybetween 0.5% and 2%. Treatment of clinically or angiographically proven cystoidmacular edema with indomethacin decreased the incidence of cystoid macularedema; however there was no difference in visual outcome between active andplacebo treated groups. No long-term effectiveness was shown yet with treatment bya NSAID. In the same report carbonic anhydrase inhibitors (e.g. acetazolamide) arementioned as possibly effective drugs in cystoid macular edema caused by changesin the external blood-retinal barrier (retinitis pigmentosa). However, a recent reporton gastric mucosa samples obtained by biopsy showed that NSAIDs (acetylsalicylicacid, indomethacin, naproxen, diclofenac and piroxicam) can activate the carbonicanhydrase isoenzymes I, II and IV (13).
An extensive review was published in 1998 (14) in which the view is held that theincidence, pathogenesis and treatment of cystoid macular edema following cataractsurgery are still poorly understood. Incidence of cystoid macular edema is greatestfollowing an intracapsular cataract extraction with implantation of an iris clip lens inan older population with systemic vascular disease. Clinical characteristics of cys-toid macular edema are a nonuniform distribution of the retinal intravascular fluidwithin the macula leading to accumulation of transudate and ultimately to a sympto-matic or asymptomatic decrease in visual acuity. Preferential leakage from perifovealcapillaries in eyes with cystoid macular edema cannot be explained yet and possi-bly reflects a result of an unknown capillary vitreous interaction. Inflammation, how-ever, is the mainstay in the development of cystoid macular edema. Presumably,
34
Chapter 1

35
breakdown of the blood aqueous barrier is associated with the development of cys-toid macular edema. This was established in rabbits in which the topical activity ofNSAIDs in stabilizing the blood aqueous barrier following paracentesis was studiedby monitoring the integrity of the barrier using anterior ocular fluorophotometrybefore and after paracentesis. The integrity was followed by changes in fluoresceinconcentrations measured after intravenous administration of fluorescein sodium inthe anterior chamber of the eye. All NSAIDs studied (flurbiprofen 0.03%, 0.1%diclofenac, 0.5% ketorolac and 1% suprofen) stabilized the blood aqueous barrierafter paracentesis.
In a Swiss overview it was concluded that NSAIDs with potent anti-inflammatoryproperties allow good control of ocular inflammation, effective maintenance of mydri-asis during surgery and delay the onset of cystoid macular edema (15). A recentreview on topical NSAIDs for ophthalmic use concluded that the benefit-risk ratio isstill favorable when they are applied in an appropriate and judicious manner (16).
REFERENCES
1. Ayo C. A toxic ocular reaction. II On the nature of the reaction. J Immunol 1942;46:127-32.2. Irvine SR. A newly defined vitreous syndrome following cataract surgery. Am J Ophthalmol
1953;36:599-619.3. Gass JDM, Norton EWD. Cystoid macular edema and pailledema following cataract extraction.
Arch Opthalmol 1966;76:646-61.4. Irvine AR. Cystoid maculopathy. Surv Ophthalmol 1976;21:1-17.5. Jampol LM. Aphakic cystoid macular edema; a hypothesis. Arch Ophthalmol 1985;103:1134-5.6. Jampol LM. Pharmacologic therapy of aphakic and pseudophakic cystoid macular edema.
Ophthalmology 1985;92:807-10.7. Drews RC. The present understanding of cystoid macular oedema. Trans opthalmol Soc UK
1985;104:744-7.8. Sole P et al (Expertise bibliographique). Le syndrome d' Irvine Gass. J Fr Ophthalmol 1986;1:75-83.9. Dirscherl M, Straub W. Zur prophylaxe des zystoiden Makulaödems nach Katarkatoperationen
(eine anwendungsbeobachtung van Chibro-Amuno 3). Ophthalmologica 1990;200:142-9.10. Hruby K. Das Irvine-syndrom; diagnose, pathogenese und therapie. Fortschr Ophthalmol
1985;82:147-8. 11. Jampol LM, Jain S, Pudzisz B, Weinreb RN. Nonsteroidal anti-inflammatory drugs and cataract
surgery. Arch ophthalmol 1994;112:891-4.12. Rocha G, Deschenes J. Pathophysiology and treatment of cystoid macular edema. Can J
Ophthalmol 1996;31:282-8.13. Puscas C, Chis F, Pasca R, Pasca S, Mihaescu M, Puscas I. Gastric, vascular and antidiuretic
effects of indomethacin are dependent on direct activation of carbonic anhydrase (CA). Gut1999;45:S5:P0087.
14. Flach AJ. The incidence, pathogenesis and treatment of cystoid macular edema followingcataract surgery. Tr Am Ophth Soc 1998;96:557-634.
15. Guex-Crosier Y. Anti-inflammatoires non stéroïdiens (AINS) et inflammation oculaire. KlinMonatsbl Augenheilkd 2001;218:305-8.
16. Gaynes BI, Fiscella R. Topical nonsteroidal anti-inflammatory drugs for ophthalmic use. A safetyreview. Drug Saf 2002;25:233-50.
General introduction
1.4 PROSTANOIDS
In 1929 it was documented that feeding of rats not only should include essentialelements like amino acids, vitamins and minerals but also small amounts of unsat-urated fat. Analysis uncovered the essential fatty acid linoleic acid, an eighteen car-bon atom chain with two double bonds.
Screening of many types of polyunsaturated fatty acids showed arachidonic acid(20 carbon atoms and 4 double bonds) to be the most active fatty acid to preventmanifestations of nutritional deficiency.
In 1930 a factor was discovered in human semen that contracted the uterus; italso lowered blood pressure. Von Euler demonstrated this to be a fatty acid andintroduced in 1935 the name prostaglandin. In 1960 Bergström elucidated the struc-ture of some prostaglandins, one of them being prostaglandin E2. In 1964 van Dorpcarried out experiments in the Unilever Research laboratories (Vlaardingen) anddemonstrated by use of labeled arachidonic acid that it was converted intoprostaglandin E2 by the medium of homogenized sheep seminal vessels. This find-ing was published in 1964 jointly with Bergström in the same journal. In 1970 Vanepublished his discovery that the biosynthesis of prostaglandins was inhibited byaspirin-like drugs. Four years later Samuelsson discovered the bioconversion byplatelets of arachidonic acid into thromboxane A2. Two years later prostacyclin wasdiscovered by Vane.
The first comprehensive reviews were published in 1974 summarizing resultsfrom the already expanding field of prostaglandin research (1,2). All efforts werenow geared to 'visualize' the prostaglandin endoperoxide synthase enzyme(Cyclooxygenase, COX). Known features were that cyclooxygenase is a polypep-tide, homodimeric in nature (approximately 70 kDa) and in monotopic arrangementin the cell membrane. It carried two distinct functional enzyme activities, catalyzingboth the bisoxygenation of arachidonic acid to its hydroperoxy arachidonatemetabolite prostaglandin G2 and consecutively catalyzing the peroxidative reduc-tion of prostaglandin G2 to its endoperoxide H2 (3). The peroxidase activity of theenzyme complex is not affected by NSAIDs.
A major advance in the field of eicosanoid research was the discovery of a sec-ond inducible cyclooxygenase isoenzyme, COX-2 (4,5). The two isoforms, COX-1and COX-2, were believed to explain the therapeutic but also the adverse effects ofthe frequently used NSAIDs. By hypothesizing that the COX-1 enzyme was theconstitutive enzyme, designed to be available for physiological functions, the COX-2 enzyme was thought primarily to act in pathophysiological processes (COXdogma). An important aim would be to develop COX-2 specific NSAIDs that wouldaid in fighting inflammatory processes and not displaying unwanted side-effectsrelated to inhibition of the COX-1 enzyme (6,7).
36
Chapter 1

Evidence was delivered that localization of the COX-1 enzyme primarily was in thesmooth endoplasmic reticulum and the COX-2 enzyme in the nuclear envelope.Cell membrane receptors for prostanoids have been localized on several tissuesincluding the eye (8,9).
In studying the dynamics of inhibition by flurbiprofen and indomethacin of thehuman prostaglandin H synthases it became evident that these compounds influ-enced at least five processes, including the rate of catalytic activation, the rate ofsubstrate turnover, the rate of autoinactivation of the enzyme complex and theassociation and dissociation rates of the inhibitor with the complex. Overall,indomethacin and flurbiprofen behaved similarly towards the human prostaglandinendoperoxide H synthase-1 and -2 enzymes, although the individual kinetic param-eters differed (10,11). In an earlier study it was concluded that the inhibitor-enzymecomplex is more stable for the flurbiprofen-prostaglandin H synthase-1 than for flur-biprofen-prostaglandin H synthase-2 complex (12).
Each isoenzyme, prostaglandin endoperoxide H synthase-1 and prostaglandinendoperoxide H synthase-2, is encoded by a different gene. When activated andwith adequate arachidonic acid and oxygen present, a single prostaglandinendoperoxide H synthase (COX) molecule can produce 103 molecules ofprostaglandin G2, a hydroperoxide, which is catalytically reduced to its alcoholicform (PGH2) by peroxidase (13). The COX-1 and COX-2 enzymes are homodimers.Each dimer consists of three independent folding units: a membrane-bindingdomain, an enzymatic/catalytic domain and an epidermal growth factor-like domain.The enzymatic/catalytic domain consists of two separate, closely spaced, but inter-dependent areas encompassing 80% of the protein. The cyclooxygenase site is sit-uated at the apex of a long hydrophobic channel in the prostaglandin endoperoxideH synthase molecule. A marked difference between COX-2 and COX-1 is the larg-er channel and the approximately 20% larger binding site in the former. This differ-ence has been exploited to examine the possibility of designing selective COX-2inhibitors (14). Although it has been suggested that the COX-1 enzyme complex ismainly active for maintenance purposes and the COX-2 enzyme, by nature of itsrapid induction capabilities, for the contribution to prostaglandin related inflamma-tion, pain and fever, implying that selective COX-2 inhibitors would benefit thepatient, some doubt has arisen concerning this elegant theory (15,16). In a morerecent study using a COX-1 selective inhibitor as well as COX-2 selective and non-selective inhibitors in normal and monoarthritic rats and mice with paw inflamma-tion, it was concluded that inhibition of both COX-isoenzymes was needed for effec-tive analgesia in inflammation (17). In studies involving the use of cyclooxygenaseknockout mice it became apparent that deficiency of COX-2 had more pronouncedeffects on the physiological maintenance of the body than deficiency of COX-1 (18).To initiate the cyclooxygenase reaction, activation of the peroxidase active site is
37
General introduction

necessary (19). When activated, an aqueous insoluble, nonchiral, arachidonic acidmolecule, liberated by phospholipase A2 from the membrane phospholipids, will be'sucked' into the hydrophobic channel where it will be converted to theprostaglandin G2 endoperoxide. After bioconversion of arachidonic acid into theprostaglandin G2 endoperoxide it will be transported to a reservoir type enclaveformed by the dimeric cyclooxygenase enzym complex. From here transport ofprostaglandin G2 to the peroxidase catalytic site is possible, where it will be trans-formed into prostaglandin H2 endoperoxide.
Closer examination of the interaction of the NSAID flurbiprofen, a representativeof the 2-phenylpropionic acid class, with the enzyme channel, reveals that theamino acid tyrosine 355, situated near the entrance of the channel, creates a localnarrowing which in turn provides a handsome explanation why the S(+) flurbiprofenenantiomer of this molecule will have a better fit than its counterpart R(-) flurbipro-fen (20,21). The carboxylate group of flurbiprofen as well as of indomethacin willcomplex with the guanidinium group of arginine 120 just like the carboxylate groupof arachidonic acid. Preparation of neutral NSAIDs by transforming the carboxylategroup into an ester or amide function may enhance COX-2 selectivity (22).
The cyclooxygenase enzymes produce prostanoids from the polyunsaturated fattyacid, arachidonic acid. These prostaglandins, D2, E2, F2α, I2 and thromboxane A2, actvia their respective receptors to elicit various physiological reactions (23).
A number of receptors have been identified (24). Prostaglandins are involved,together with histamine and bradykinine, in the local increase in vascular perme-ability and edema in which PGE2 and PGI2 are prominently involved. It has becomeevident that they elicit these vascular changes as well as inflammatory pain via EP-and IP-type receptors, respectively.
In a study involving knock-out mice with a EP1 receptor deficient status, the pain-sensitivity responses were tested in two acute prostaglandin-dependent models (25).The animals' reaction was reduced by approximately 50%, the same amount ofreduction that could be achieved by pharmacological interventions in wild-type mice.
In determining the inhibitory effects of the flurbiprofen enantiomers on the COX-1and COX-2 isoenzymes, it is of advantage to take the biological surroundings of theNSAID in the human body, e.g. causing protein binding, into consideration. Use ofhuman whole blood, as an ex vivo method for quantification of the inhibitory effectsof an NSAID on the synthesis of prostanoids has become an established procedure(26,27). As an unequivocal example of functional COX-1 the Ca2+-ionophore stimu-lated platelet is used, measuring the metabolite of thromboxane A2. Thelipopolysaccharide stimulated monocyte can be taken as an activity indicator offunctional COX-2. Any interference by platelets is excluded by acetylation of theCOX-1 enzyme by prior administration of acetylsalicylic acid.
38
Chapter 1

Prostaglandin levels have been measured using radioimmunoassays in 41 humaneyes of patients undergoing vitrectomy (28). In 'quiet eyes' undergoing routinecataract extraction physiological prostaglandin levels of around 100 pg/ml werereported. In patients with a diagnosis of cataract and cystoid macular edema meanlevels of PGI2 varied between 49 and 360 pg/ml.
Induction of COX-2 mRNA can take place in the rabbit eye within three hoursfollowing glaucoma filtration surgery (29). Paracentesis however fails to induceCOX-2 mRNA, possibly because of the minimal disturbance by this procedure.
Prostaglandin synthase activity exists both in vascular and avascular structures ofthe eye, being most abundant in the iris-ciliary body.
Although the iris-ciliary body of the rabbit eye has a high functional capacity tosynthesize prostanoids following paracentesis, only a transient ocular inflammato-ry response follows which resolves within 3 - 4 hours (30).
Eicosanoid measurements in the aqueous obtained during paracentesis of therabbit eye showed a strong and rapid rise in PGE2 levels in the aqueous humor withpeak values at 20 minutes, followed by recovery to baseline within 48 hours (31).No prostacyclin (measured as the stable metabolite 6-keto-PGF1α) was detected inthe aqueous humor at the start but was markedly present at ten and twenty minutesafter the initial trauma. Prostaglandin synthesis was followed shortly by an increasein aqueous humor protein, with peak levels achieved within 30 minutes after para-centesis. Both PGE2 and protein levels declined gradually to near baseline levels48 hours after trauma.
Experimental evidence has shown that the inducible COX-2 mRNA is present in thefirst hours after injury and is possibly assisting in wound healing (32,33). COX-1knockout mice do not show signs of spontaneous gastrointestinal ulceration aswould have been expected when the generation of prostaglandins by the COX-1enzyme is involved in maintenance and integrity keeping purposes (34). ClassicalNSAIDs still show efficacy when the COX-2 enzyme is no longer present, as shownby Western blotting (35). Administering COX-2 inhibitors then does not seem indi-cated. Interestingly, a COX-2 enzyme complex showed up again near resolution ofinflammation and produced anti-inflammatory prostaglandins, PGD2, PGF2α and amember of the PGJ2 family (36). This is in contrast with the view hinting thatcyclooxygenase-2 inhibitors might be the new approach to therapy in ocular inflam-mation (37).
The case against the use of COX-2 inhibitors seems more compelling now that ithas become clear that in the field of rheumatology a five fold higher risk of cardiaccomplications can occur (38,39,40,41). In a well designed study using knockout
39
General introduction

mice deficient of a prostacyclin receptor or a thromboxane receptor, it was shownthat efficient cross talk exists between prostacyclin- and thromboxane- dependentsignaling pathways (42). Inhibition of one signaling pathway might induce the other.This could account for unforeseen complications with the use of cyclooxygenase-2inhibitors (43). Also the presence of mutations in cytochrome P450 isoenzymes thatmetabolize arachidonic acid could play a role in diseases involving clotting andinflammatory disorders (44). Potential drug alternatives, however, are being devel-oped (45).
Flurbiprofen is an NSAID with preferential cyclooxygenase-1 inhibiting capacitylike indomethacin. Its use as a NSAID eyedrop for combatting inflammatoryresponses following cataract surgery therefore seems appropriate.
REFERENCES
1. Flower RJ. Drugs which inhibit prostaglandin biosynthesis. Pharmacol Rev 1974;26:33-67.2. Flower RJ, Vane JR. Inhibition of prostaglandin biosynthesis. Biochem Pharmacol 1974;23:1439-50.3. Merlie JP, Fagan D, Mudd J, Needleman P. Isolation and characterization of the complementary
DNA for sheep seminal vesicle prostaglandin endoperoxide synthase (cyclooxygenase). J BiolChem 1988;263:3550-3.
4. Xie W, Chipman JG, Robertson DL, Erikson RL, Simmons DL. Expression of a mitoogen-respon-sive gene encoding prostaglandin synthase is regulated by mRNA splicing. Proc Natl Acad SciUSA 1991;88:2692-6.
5. Xie W, Robertson DL, Simmons DL. Mitogen-inducible prostaglandin G/H synthase: a new targetfor nonsteroidal anti-inflammatory drugs. Drug Dev Res 1992;25:249-65.
6. Vane J. Towards a better aspirin. Nature 1994;367:215-6.7. Allen KN. Aspirin - now we can see it. Nature Medicine 1995;1:882-3.8. Goetzl EJ, An S, Smith WL. Specificity of expression and effects of eicosanoid mediators in nor-
mal physiology and human diseases. FASEB J 1995;9:1051-8.9. Morita I, Schindler M, Regier MK, Otto JC, Hori T, DeWitt DL, Smith WL. Different intracellular
locations for prostaglandin endoperoxide H synthase-1 and -2. J Biol Chem 1995;270:10902-8.10. Callan OH, So O-Y, Swinney DC. The kinetic factors that determine the affinity and selectivity for
slow binding of human prostaglandin H synthase 1 and 2 by indomethacin and flurbiprofen. J BiolChem 1996;271:3548-54.
11. So O-Y, Scarafia LE, Mak AY, Callan OH, Swinney DC. The dynamics of prostaglandin H syn-thases. Studies with prostaglandin H synthase 2 Y355F unmask mechanisms of time-dependentinhibition and allosteric activation. J Biol Chem 1998;273:5801-7.
12. Laneuville O, Breuer DK, Dewitt DL, Hla T, Funk CD, Smith WL. Differential inhibition of humanprostaglandin endoperoxide H synthases-1 and -2 by nonsteroidal anti-inflammatory drugs. JPharmacol Exp Ther 1994;271:927-34.
13. Kulmacz RJ. Cellular regulation of prostaglandin H synthase catalysis. FEBS letters1998;430:154-7.
14. Brooks P, Emery P, Evans JF, Fenner H, Hawkey CJ, Patrono C, Smolen J, Breedveld F, Day R,Dougados M, Ehrich EW, Gijon-Baños J, Kvien TK, van Rijswijk MH, Warner T, Zeidler H.Interpreting the clinical significance of the differential inhibition of cyclooxygenase-1 andcyclooxygenase-2. Rheumatology 1999;38:779-88.
15. Wallace JL. Selective COX-2 inhibitors: is the water becoming muddy? TiPS 1999;20:4-6.
40
Chapter 1

16. Reuter BK, Asfaha S, Buret A, Sharkey KA, Wallace JL. Exacerbation of inflammation-associat-ed colonic injury in rat through inhibition of cyclooxygenase-2. J Clin Invest 1996;98:2076-85.
17. Mazario J, Gaitan G, Herrero JF. Cyclooxygenase-1 vs. cyclooxygenase-2 inhibitors in the induc-tion of antinociception in rodent withdrawal reflexes. Neuropharmacology 2001;40:937-46.
18. Langenbach R, Loftin C, Lee C, Tiano H. Cyclooxygenase knockout mice. Models for elucidatingisoform-specific functions. Biochemical Pharmacology 1999;58:1237-46.
19. Kiefer JR, Pawlitz JL, Moreland KT, Stegeman RA, Hood WF, Gierse JK, Stevens AM, GoodwinDC, Rowlinson SW, Marnett LJ, Stallings WC, Kurumbail RG. Structural insights into the stereo-chemistry of the cyclooxygenase reaction. Nature 2000;405:97-101.
20. Bhattacharyya DK, Lecomte M, Rieke CJ, Garavito RM, Smith WL. Involvement of arginine 120,glutamate 524, and tyrosine 355 in the binding of arachidonate and 2-phenylpropionic acidinhibitors to the cyclooxygenase active site of ovine prostaglandin endoperoxide H synthase-1. JBiol Chem 1996;271:2179-84.
21. Kurumbail RG, Kiefer JR, Marnett LJ. Cyclooxygenase enzymes: catalysis and inhibition. CurrOpinion Struct Biol 2001;11:752-60.
22. Rainsford KD. Profile and mechanisms of gastrointestinal and other side effects of nonsteroidalanti-inflammatory drugs (NSAIDs). Am J Med 1999;107 (6A) 27S-36S.
23. Tilley SL, Coffman, Koller BH. Mixed messages: modulation of inflammation and immuneresponses by prostaglandins and thromboxanes. J Clin Invest 2001;108:15-23.
24. Narumiya S, Sugimoto Y, Ushikubi F. Prostanoid receptors: structures, properties, and functions.Physiol Rev 1999;79:1193-226.
25. Stock JL, Shinjo K, Burkhardt J, Roach M, Taniguchi K, Ishikawa T, Kim H-S, Flannery PJ,Coffman Tm, McNeish JD, Audoly LP. The prostaglandin E2 EP1 receptor mediates pain per-ception and regulates blood pressure. J Clin Invest 2000;107:325-31.
26. Patrignani P, Panara MR, Greco A, Fusco O, Natoli C, Iacobelli S, Cipollone F, Ganci A,Créminon C, Maclouf J, Patrono C. Biochemical and pharmacological characterization of thecyclooxygenase activity of human blood prostaglandin endoperoxide synthases. J PharmacolExptl Ther 1994;271:1705-12.
27. Young JM, Panah S, Satchawatcharaphong C, Cheung PS. Human whole blood assays for inhi-bition of prostaglandin G/H synthases-1 and -2 using A23187 and lipopolysaccharide stimulationof thromboxane B2 production. Inflamm Res 1996;45:246-53.
28. Thomas MA, O'Grady GE, Swartz SL. Prostaglandin levels in human vitreous. Br J Ophthalmol1985;69:275-9.
29. Chang MS, Tsai JC, Yang R, DuBois RN, Breyer MD, O'Day DM. Induction of rabbit cyclooxyge-nase 2 in the anterior uvea following glaucoma filtration surgery. Curr Eye Res 1997;16:1147-51.
30. Kulkarni PS, Srinivasan BD. Cyclooxygenase and lipoxygenase pathways in anterior uvea andconjunctiva. In: Bito LZ, Stjernschantz J, editors. The ocular effects of prostaglandins and othereicosanoids. New York Alan R Liss 1989:39-52.
31. Graff G, Brady MT, Gamache DA, Spellman JM, Yanni JM. Transient loss of prostaglandin syn-thetic capacity in rabbit iris-ciliary body following anterior chamber paracentesis. Ocul ImmunolInflamm 1998;6:227-38.
32. Mizuno H, Sakamoto C, Matsuda K, Wada K, Uchida T, Noguchi H, Akamatsu T, Kasuga M.Induction of cyclooxygenase 2 in gastric mucosal lesions and its inhibition by the specific antag-onist delays healing in mice. Gastroenterolgy 1997;112:387-97.
33. Gilroy DW, Colville-Nash PR, Willis D, Chivers J, Paul-Clark MJ, Willoughby DA. Induciblecyclooxygenase may have anti-inflammatory properties. Nat Med 1999;5:698-701.
34. Morteau O, Morham SG, Sellon R, Dieleman LA, Langenbach R, Smithies O, Balfour Sartor R.Impaired mucosal defense to acute colonic injury in mice lacking cyclooxygenase-1 or cyclooxy-genase-2. J Clin Invest 2000;105:469-78.
41
General introduction

35. Gilroy DW, Tomlinson A, Willoughby DA. Differential effects of inhibitors of cyclooxygenase(cyclooxygenase 1 and cyclooxygenase 2) in acute inflammation. Eur J Pharmacol 1998;355:211-17.
36. Willoughby DA, Moore AR, Colville-Nash PR. COX-1, COX-2, and COX-3 and the future treat-ment of chronic inflammatory disease. Lancet 2000;355:646-8.
37. Masferrer JL, Kulkarni PS. Cyclooxygenase-2 inhibitors: a new approach to the therapy of ocu-lar inflammation. Surv Opthalomol 1997;41:S35-S40.
38. Bombardier C, Laine L, Reicin A, Shapiro D, Burgos-Vargas R, Davis B, Day R, Bosi Ferraz M,Hawkey CJ, Hochberg MC, Kvien TK, Schnitzer TJ, for the VIGOR study group. Comparison ofupper gastrointestinal toxicity of rofecoxib and naproxen in patients with rheumatoid arthritis. NEngl J Med 2000;343:1520-8.
39. Ray WA, Stein CM, Daugherty JR, Hall K, Arbogast PG, Griffin MR. COX-2 selective non-steroidal anti-inflammatory drugs and risk of serious coronary heart disease. Lancet2002;360:1071-3.
40. Jüni P, Rutjes AWS, Dieppe PA. Are selective COX 2 inhibitors superior to traditional nonsteroidal anti-inflammatory drugs? Adequate analysis of the CLASS trial indicates that this maynot be the case. BMJ 2002;324:1287-8.
41. Jones R. Efficacy and safety of COX 2 inhibitors. New data are encouraging but the risk:benefitratio remains unclear. BMJ 2002;325:607-8.
42. Cheng Y, Austin SC, Rocca B, Koller BH, Coffman TM, Grosser T, Lawson JA, FitzGerald GA. Roleof prostacyclin in the cardiovascular response to thromboxane A2. Science 2002;296:539-4.
43. Vane JR. Back to an aspirin a day? Science 2002;296:474-5.44. Nebert DW, Russell DW. Clinical importance of the cytochromes P450. Lancet 2002;360:1155-62.45. Skelly MM, Hawkey CJ. Potential alternatives to COX 2 inhibitors. New molecules may overtake
the COX 2 inhibitors debate. BMJ 2002;324:1289-90.
42
Chapter 1

CHAPTER 2RATIONALE FOR USING A PHOSPHATE BUFFER
FOR S(+) FLURBIPROFEN EYEDROPS

RATIONALE FOR USING A PHOSPHATE BUFFER FOR S(+) FLURBIPROFENEYEDROPS
Although the eye, eyelids and skin surrounding the eye are sensitive to externalstimuli, physiological reactions due to deviations outside the near normal values forosmolality or pH are not always seen.
However, in a state of ill-health or during regular use of ophthalmic preparations,this situation may be more outspoken.
The active principle in the eyedrop can provoke, when not properly dissolved, anirritating or burning sensation leading to lacrimal discharge, occasional haemor-rhage or endangering blinking reflexes during surgery. Lacrimal discharge willcause an unwanted dilution and drainage of medicine.
Individual sensitivity may vary and physiological values of tear fluid can fluctuate,which is also dependant on the health condition of the individual eye in general, thenasal corner of the eye being the most sensitive.
Even if the composition of the eyedrop approximates the ideal solution, certain(active) principles may cause discomfort to the eye.Non-irritating eyedrops should comply with: (1) sterility, (2) isotonicity and (3) pHvalue. Sterility is of paramount importance when an ophthalmic solution is appliedto the injured eye.
The character of the active ingredient will to a certain degree determine the abovementioned requirements. The osmotic value of an ophthalmic solution shouldreflect that of blood, corresponding to a 0,9% sodium chloride solution. Deviationsfrom this value have been noted from 0,6% to as high as 5% sodium chloride with-out marked discomfort. Yet it is of prime importance to adhere as close as possibleto isotonicity, as the optical integrity of the cornea can be influenced significantly bydeviations thereof. In this respect the physiological term tonicity seems more appro-priate than the physicochemical term osmolality. The cornea functioning as selec-tive permeable biomembrane is better accomodating this term. The osmotic valueis commonly expressed in (milli)osmol/liter (osmolarity). This can be transformed toosmolality (mosmol/kg) by dividing by the specific gravity of the solution.
Eye irritation must be discerned from an allergy which requires the choice of a dif-ferent pharmacological agent. Cutaneous hypersensitivity due to a particularstereoisomer has been reported (1).
There are several reasons for buffering an ophthalmic solution:· To prevent unwanted pH changes caused by hydroxyl ion release from the
glass in which the solution is stored.· In case of a pH-dependent degradation of the active principle, a buffer should
be used for stabilization.
44
Chapter 2

· In case of a pH-dependent solubility, a buffer can be used to dissolve therequired amount of drug.
On the other hand there are also limitations to the use of buffers. First of all, the lim-ited buffer capacity of the lacrimal fluid precludes the use of strong buffers outsidethe pH range of 6.8 - 7.6.
In addition, adherence to a pH as close to the physiological pH as possible isimportant for preventing local precipitations of the drug and minimizing deteriorationafter administration.
For the formulation of S(+) flurbiprofen eyedrops, a published phosphate buffer ofpH 7.4, used in an eyedrop, was chosen as a starting point (2). The specialtyOcuflur® containing racemic flurbiprofen sodium (appendix A) is produced in a cit-rate buffer of pH 6.45. However, the quantitative nature of the citrate buffer usedwas not disclosed. Analysis by HPLC revealed a citrate concentration of 5.5 gram/l(see appendix B for materials & conditions).
The buffer used by us in preparing S(+) flurbiprofen eyedrops consists of 0.022 Mdisodium phosphate dihydrate and 0.112 M potassium dihydrogen phoshate, result-ing in approximately 0.13 M total salt concentration and an ionic strength of 0.36 M.
It should be realised, that at pH=7.4 practically all dissolved flurbiprofen (pKa= 4.22)is present in the salt form; the acidic form fraction is determined by
Log [flurbiprofen acid/flurbiprofen salt] = pKa - pH; thus % [flurbiprofen acid] = 0.066%.
The importance of this value is that because only the non-protonized form of anacid (like flurbiprofen) is able to pass the different membranes in the eye, the driv-ing force for permeation is rather low (0.066%). It should be realized, however, thatthe pH of the ophthalmic solution is not the only parameter determining permeationefficacy.
The choice for a buffer applied to the ophthalmic solution is determined by the bestcompromise of the following issues:1. It is convenient for patient and surgeon to stay as close as possible to the nat-
ural pH of the tear fluid (7.4).2. As far as flurbiprofen is concerned, the solubility in aqueous solution is prob-
lematic at pH values below 7 (3), as illustrated on the next page:
45
Phosphate buffer

46
pH 3.5 4.0 4.5 5.0 5.5 6.0 6.5 7.0 7.2
3. Discomfort for the patient will not be present as long as the pH is between 6.6- 7.8. Tolerability for the cornea is in the pH range of pH 6.6 - 8.5. Changes inpermeability will occur outside the pH range of 4 and 10.
4. The permeation of flurbiprofen increases at lower pH values.
On the basis of the above considerations it follows that the optimal pH is between7.0 and 7.4. For the present formulation the physiological pH (7.4) was chosen. Theoften used citrate buffer would have been less favourable, because this buffer com-position has hardly any buffering capacity around pH 7.4, in clear contrast to aphosphate buffer.
Interestingly, no difference in pharmacological effect could be demonstratedusing ophthalmic solutions of diclofenac, indomethacin or flurbiprofen in a pH rangeof 5.0 - 7.5 in preventing disruption of the blood-aqueous barrier in a rabbit para-centesis model (4).
In addition, the use of a phosphate buffer provides stable, single stereoisomer for-mulations of the NSAID ketorelac. This was in contrast to the use of acetate or cit-rate buffers (5).
Chapter 2

REFERENCES
1. Buzo-Sanchez G, Martin-Munoz MR, Navarro-Pulido AM, and Orta-Cuevas JC. Stereoisomericcutaneous hypersensitivity. Ann Pharmacother 1997;31:1091.
2. van Nispen tot Pannerden EBLM, van Sorge AA. Waterige oogdruppels met indometacine inoplossing (Aqueous eyedrops with indomethacin in solution) Pharm Weekbl 1981;116:386-7.
3. Naaijkens MS and Van Sorge AA . Preparation of a 5% Flurbiprofen hydrogel. Pharmaceuticalaspects. 6th Internet World Congress for Biomedical Sciences. Ciudad Real, Spain February14th - 25th , 2000.
4. Van Haeringen NJ, Oosterhuis JA, Van Delft JL, Glasius E, Noach EL. A comparison of the effectsof non-steroidal compounds on the disruption of the blood-aqueous barrier. Exp Eye Res1982;35:271-7.
5. Brandl M, Conley D, Johnson D, Johnson D. Racemization of ketorolac in aqueous solution. JPharm Sci 1995;84:1045-8
APPENDIXAOcuflur®Composition according to package insert august 1995 Allergan S.A./N.V.
Flurbiprofen sodium dihydrate 0.03%, Polyvinylacohol, Thiomersal 0,005%, Sodium edeticacid, sodium chloride, sodium citrate dihydrate, sodium chloride, citric acid monohydrate,sodium hydroxide, hydrochloric acid, aqua purificata
BHPLC method of analysisMaterials & MethodsColumn: Chrompack Organic acids 300*6.5mm conventional stainless steel Catalogue No.28350Eluent: 0.005 mol/l sulphuric acidFlow: 0.8 ml/minTemperature: 35°CDetector: UV 210 nmInternal Standard: oxalic acidInjection volume: 25 µL
47
Phosphate buffer

48

CHAPTER 3FLURBIPROFEN, S(+), EYEDROPS:
FORMULATION, ENANTIOMERIC ASSAY, SHELFLIFEAND PHARMACOLOGY
Adriaan A. van Sorge, Peter H. Wijnen, Jan L. van Delft,Valérie M.W. Carballosa Coré-Bodelier and Nicolaas J. van Haeringen
Derived from Pharm World Sci 1999;21:91-5

ABSTRACT
Aphakic cystoid macula edema, occurring after cataract extraction is ascribed totrauma-induced production of intra-ocular prostaglandins. Sufficient experimentaland clinical evidence supports the use of prostaglandin synthesis inhibitors to coun-tervail this clinical condition. The active S(+) enantiomer of flurbiprofen, aprostaglandin synthesis inhibitor, has been formulated into a stereoselective, bal-last free eyedrop solution in a concentration of 0.015%. Analysis by capillary zoneelectrophoresis shows shelflife stability up to four years at room temperature of thisenantiomer. The inhibitory effect on the synthesis of prostaglandins as measuredon a homogenate of bovine iris/ciliary body, remained unaffected during a shelflifeperiod of three years.
INTRODUCTION
Following cataract surgery non-specific inflammatory responses are induced,caused by surgical trauma. In the animal model of ocular trauma it is well substan-tiated that the greater part of this inflammatory process is based on synthesis ofprostaglandins by iris tissue (1,2). The prostaglandins are released into the aque-ous humor and cause breakdown of the blood aqueous barrier, characterized byinflux of plasma proteins. Diffusion of prostaglandins through the vitreous to theposterior segment of the eye, may cause breakdown of the blood retinal barrierresulting in the development of aphakic cystoid macular edema (3).
Ophthalmic solutions of several nonsteroidal anti-inflammatory drugs (NSAIDs)are commercially available such as diclofenac (0.1%), indomethacin (0.1%), flur-biprofen (0.03%), ketorolac (0.5%) and a suspension of indomethacin (1.0%).Indomethacin 0.1% formulation was incorporated in the Dutch National Formulary(FNA) in 1986. Inpracticalities with indomethacin in aqueous solution - no sterilisa-tion possibility and only a short shelflife when in solution (4-7) - prompted us toinvestigate the possibility in formulating an eyedrop based on flurbiprofen (8). Anofficial monograph on Flurbiprofen sodium ophthalmic solution is mentioned in theUSP XXIII . The solubility of flurbiprofen (pKa 4.22) in its acid form is 100mg/L at pH5.0; its sodium salt has a solubility of 400mg/L (26°C, pH 7).
Shortly after it was recognized that inhibition of prostaglandin synthesis could bethe main mechanism of action of NSAID's (9), analysis of the category of 2-aryl pro-pionic acids (profens] revealed their nature to be racemic and their inhibitory acti-vity almost exclusively residing in the S-stereoconfiguration (10). However only in1990 the ocular effect of topically applied S(+) ibuprofen was reported in a rabbitmodel of interleukin-1 (11) and paracentesis induced uveitis (12] at relatively highconcentrations (0.9% and 0.8% respectively). Also with S(+) naproxen, marketed
50
Chapter 3

by Syntex as enantiomeric pure NSAID, the antiinflammatory effect in eyedrops(0,5%) was demonstrated experimentally (13). In a bovine iris/ciliary bodyhomogenate incorporating the cyclooxygenase -1 (COX-1) enzyme, the S(+) flur-biprofen proved to be the pharmacological active moiety, showing 100 times greaterpotency than R(-) flurbiprofen in inhibiting prostaglandin synthesis (14).
In keeping with the benefits of only using the proposedly active moiety, (S+) flur-biprofen, we investigated formulations, containing the pure enantiomers of flurbipro-fen (15). We thereby avoid isomeric ballast, providing a reduction in metabolic loadto the patient. Advantages would eventually be: less complex pharmacokinetic pro-files (16), less complex drug interactions and uncomplicated concentration-effectrelationships. The present study deals with the formulation, analysis, keeping quali-ty and pharmacology of solutions containing 0.03% flurbiprofen, 0.015% flurbiprofen(S+) or flurbiprofen (R-) 0,015%, all three based on their acid form.
MATERIALS AND METHODS
Drugs and chemicalsFlurbiprofen, (S+)flurbiprofen and (R-)flurbiprofen were purchased from DuchefaPharma BV (Haarlem, The Netherlands). Disodiumphosphate.2H2O, Potassium-dihydrogen-phosphate were purchased from Bufa (Uitgeest, The Netherlands).USP reference standard, USP 2-(4-Biphenylyl)propionic acid RS, (Flurbiprofenrelated compound A limit test; catalog number: 28576 ).
Vancomycin hydrochloride was purchased from Sigma (St Louis, Mo, USA).H3PO4, KH2PO4, TRIS and Na2HPO4 were analytical grade and obtained from JTBaker (Deventer, The Netherlands).Water for injections USPXXIII (Fresenius, 's-Hertogenbosch, The Netherlands). Water for analysis was purified in an Alpha-Qapparatus (Millipore, Bedford, MA,USA). Samples of the speciality Ocuflur® (0.03%flurbiprofen sodium, lotnumbers: 94G11 exp:01/96, 96L18 exp: 06/98 and 99K29exp: 05/2001) were a gift from Allergan (Belgium).
Formulation of eyedropsThe formulation for the 0.13M phosphate buffer, pH 7.4 and osmolality of 290mOsmols/kg is based on previous work with indomethacin (7)Composition of buffersolutionDisodiumphosphate. 2H2O 20 gramPotassiumdihydrogenphosphate 3 gramWater for injections ad 1 LiterThis solution is filtered through a 0.22 micron filter before sterilization for 15 minutesat 121°C. This buffersolution is used for preparing the eyedrops for pharmacologicaltesting and for the shelflife procedure.
51
Flurbiprofen, S(+), Eyedrops

Preparation of the racemic, (S+)- and (R-) flurbiprofen eyedrops proceeds by addi-tion of respectively 30 mg racemic flurbiprofen and 15 mg of each of the enan-tiomers to 100 ml of phosphatebuffer solution. The final pH remaining unchangedat 7.4, because the relatively low concentration of flurbiprofen (1.2mM) does notburden the buffer (130mM) significantly. All flurbiprofen preparations were stored inglass containers. No preservative is added to the final solution as the eyedrops willbe used prior to cataract surgery and eye-surgeons show preference to use eye-drops, if feasable, without unnecessary additions thereby avoiding possible allergicreactions.
For shelflife testing, preparations were either 0.22 micron filtered, heat treated at100°C for 60 minutes or sterilized at 121°C for 15 minutes.Preparations were stored for a period of up to 60 months, either at room tempera-ture in subdued light or at - 20°C. Analysis was performed by capillary zone elec-trophoresis (CZE) on samples at t=0 and samples stored for 36, 48 and 60 months.All concentrations complied with the requirement of containing between 90 - 110%of the active moiety and were set at 100% at the start of shelflife analysis.
Additional analysis was done, according to the monographs on Flurbiprofen men-tioned in the USP24-NF19, European Pharmacopea 1999 and the BritishPharmacopea 2000, on Flurbiprofen related substances of which 2-(4-Biphenylyl)propionic acid (Flurbiprofen related compound A limit test) is the maincomponent.
Analytical assayACZE is a technique which permits high separation efficiencies combined with smallsample volumes. Quantitative aspects of CZE methods for enantiomeric purity test-ing are discussed in the literature for both basic and acidic drugs. Depending on theresolution of the peaks, limits of detection of <0.1% are shown for determination ofthe minor enantiomer (17-20).
An applied Biosystems (San Jose, CA, USA) Model 270A-HT CZE system wasused, equipped with a variable-wavelength UV absorbance detector (254 nm, 0.5second rise time). The separations were performed in a fused silica capillary (70 cmx 50 µm inner diameter, Polymicro Technologies, Phoenix, AZ, USA) with a lengthof 50 cm to the detection window. The electrophoresis buffer was prepared byadjusting a 50mM KH2PO4 solution to pH=6.0 with a 50 mM Na2HPO4 solution. Theglycopeptide antibiotic Vancomycin was used as chiral selector (21-23). The selec-tor was added to the inlet buffer only, at a concentration of 0.6mM.
The separations were carried out at +15 kV, with the oven temperature set at30°C. Samples were introduced into the capillary at the anodic end via a controlledvacuum injection system of 1 or 2 seconds corresponding to a volume of approxi-
52
Chapter 3
mately 4 - 8 nanoliter, respectively. After sample injections the electrode and theouter surface of the fused silica capillary were dipped for 0.5 seconds in water forcleansing. Analytes are detected in the capillary near the cathode. Data wererecorded using a Fisons Model VG-Multichrom system.
Enantiomeric assayChiral separation occurs through selective complexation of the flurbiprofen enan-tiomers with vancomycin. From the corrected peak areas of the enantiomers, theenantiomeric ratio (E.R.) was calculated as R(-)/S(+). To determine if racemizationoccurred during storage conditions the E.R. was determined in all samples. Theracemic drug will have an enantiomeric ratio of unity. For the S(+) and R(-) samplesthe impurities are calculated as percentage relative to the main optical isomer. Theracemic samples under investigation were injected after appropriate dilution.Phosphate buffer, used in the formulation of the eyedrops, was injected as blanksolution to rule out interference.
Quantitative assayFor quantitative determination of the S(+) and R(-) samples the above describedsystem was changed for analysis of total flurbiprofen. The CZE-buffer was stabi-lized to pH 7 and consisted of 40mM TRIS/H3PO4 solution without chiral selector.S(+) and R(-) flurbiprofen migrate as one peak, thus minimizing the contribution ofintegration errors on the quantitative results. Separations were carried out at +25kV. Samples were analyzed in duplo and on two separate days. The racemic sam-ples and the S(+) and R(-) samples were appropriately diluted before injection.Standards were injected at the beginning, halfway and at the end of the samplesequence. Calibration was taken into account by insertion of standards in the sameconcentration range during the analysis. The phosphate buffer was included asblank for investigation of possible interferences.
BA test on common impurities can be performed according to the monographs onFlurbiprofen (Sodium) described in the European Pharmacopea (1999 page 859-61), the USP24-NF19 (effective january 2000) and the British Pharmacopea (2000page 718) To perform a limit test on 2-(4-Biphenylyl)propionic acid (Flurbiprofenrelated compound A), the main impurity, a liquid chromatography system wasequipped with a variable-wavelength UV absorbance detector set at 247 nm and achrompack Inertsil 5 octadecylsilyl-3 column (catalog number CP28308). As themobile phase, at a flow rate of 1.0 ml/min, a mixture of 5 volumes of glacial aceticacid, 35 volumes of acetonitrile and 60 volumes of water was used. Injection vol-ume used was 20 microliter with a relative standard deviation for replicate injections
53
Flurbiprofen, S(+), Eyedrops

of less than 1%. The resolution factor between the two principle peaks is larger than1.5 (1.94) and accords with the requirements set by the British Pharmacopoeia,European Pharmacopoeia and USP24-NF19. The relative retention time for flur-biprofen related compound A to flurbiprofen is 0.87 (figures 1a and 1b). Samplingon several batches of flurbiprofen S(+) 0.015%, flurbiprofen R(-) 0.015% and ofOcuflur® (0.03% flurbiprofen sodium) was performed.
Figure 1a. Analysis of Ocuflur® (batch 96L18) for Flurbiprofen related compound A.
Figure 1b. Analysis of Flurbiprofen S(+) 0.015% (batch 28081995) for Flurbiprofen relatedcompound A
54
Chapter 3

Pharmacological assayInhibition of prostaglandin synthesis by flurbiprofen was performed using bovineiris/cilliary body homogenate according to Van Sorge et al (14). In brief, 25 µL offlurbiprofen solution is added to 100 µL of iris/ciliary body homogenate, preparedfrom one iris/ciliary body in one ml of 0.05 M TRIS buffer pH 7.4. The enzyme reac-tion was stopped by heating for 3 minutes in boiling water. In the supernatant aftercentrifugation PGE2 was determined using an enzyme immune assay. Inhibition ofPGE2 release was calculated by the difference of PGE2 release in the absence andpresence of flurbiprofen, expressed in percent of the non-inhibited release.
RESULTS
ANALYTICAL ANALYSIS
Enantiomeric analysisOn injection of the phosphate buffer used in the formulation of the eyedrops nointerfering peaks were detected. The E.R. of the flurbiprofen standard was 0.999 ±0.006 (n=6) which corresponds to 50.0 ± 0.2%.
Stored samples of racemic flurbiprofen displayed no change in E.R. as comparedto standard. Neither a heat treated sample at 100°C and stored at roomtempera-ture for 60 months (E.R.: 0.996), nor a second sample of the same date sterilizedfor 15 minutes at 121°C and stored at room temperature (E.R.: 0.997) showed sig-nificant deviation in E.R from the standard racemic flurbiprofen (E.R. 0.999).Samples of 48 months storage at roomtemperature (E.R.: 0.996) and 24 months at-20°C (E.R.: 0.995) exhibited no change in E.R. as compared to standard. Ocuflur®(lotnumber 94G11) stored at room temperature (36 months) showed no change inE.R. (0.995).
All samples of S(+) flurbiprofen (48 months or less and stored at room tempera-ture) showed no R(-) enantiomer above limit of detection of the assay, which isapproximately 0.1%.
The racemic moiety of S(+) in R(-) flurbiprofen at t=0 was determined as 0.7% ± 0.1(n=3). In Figure 2 the electropherograms are shown for two samples of R(-) flur-biprofen, after storage at -20°C for 48 months without sterilization as well as afterstorage for 48 months at roomtemperature after sterilization. The presence of S(+)flurbiprofen in the R(-) storage samples (48 months at room temperature sterilizedat 15 minutes 120°C) increased to 0.9% (n=2).
55
Flurbiprofen, S(+), Eyedrops

Figure 2. Comparison of two superimposed electropherograms of R(-) flurbiprofen samples:(A) stored at roomtemp, sterilized; (B): not sterilized stored at -20 ºC.
Quantitative analysisS(+) flurbiprofen samples irrespective of heat treatment and storage at roomtem-perature for 48 months showed a maximum decline to 93% of declared value of theactive moiety. The R(-) flurbiprofen samples revealed the same degradation char-acteristics as those for S(+). Ocuflur® stored at roomtemperature showed a declineto 92% of the declared value after 36 months while racemic flurbiprofen samples,irrespective of heat treatment showed a maximum decline to 90% in 48 months.The type of degradation reaction involved was not investigated. In the electro-pherogram no extra signals are detected, but in the set-up used only negativecharged components with UV-absorbance at 254 nm would be visible.
Analysis of Flurbiprofen related compound A (Limit test)Impurities can be found in compendial articles. According to the EuropeanPharmacopoeia 3e Edition 2001 Flurbiprofen has five identified impurities. One ofthese is known as flurbiprofen related compound A and is used for the limit test.This substance in it self is a stereoisomer but is available as a racemic referencestandard USP 2-(4-Biphenylyl)propionic acid RS.
56
Chapter 3

57
Flurbiprofen, S(+), Eyedrops
Table 1. Flurbiprofen related compound A content in ophtalmic solutions.
Preparation Sterilized Date of manufacturing ‰ Flurbiprofen15 min 121°C related compound A
S(+)Flurbiprofen 0.015% Y 28-08-95 0,9; 1,0N 28-08-95 1,3 ; 1,3; 0,9; 0,8Y 08-10-93 0,5; 0,5; 0,6; 1,03
R(-)Flurbiprofen 0.015% Y 08-10-93 0,9; 0,8N 08-10-93 0,3; 0,4Y 28-08-95 0,2; 0,2N 28-08-95 0,2; 0,2
Ocuflur®* Y 94G11 2,5; 2,9Y 96L18 3,7; 3,6Y 99K29 2,5; 2,5; 2,6; 2,3
* Flurbiprofen Sodium. 2H2O 0.03%. Y=yes, N=No.In either case the products agreed with the Pharmacopoeial limits for the known impurity Flurbiprofenrelated compound A (5‰), being stored at room temperature and irrespective of heat treatment.
In Table 1 the results are presented not only for the batches prepared with the flur-biprofen isomers as ophthalmic solution but also for the racemic flurbiprofen spe-cialty Ocuflur®. The ophthalmic solutions of isomeric flurbiprofen have beenanalysed with the same maximum storage time as was stated under enantiomericanalysis.
PHARMACOLOGICAL ANALYSIS
Samples of flurbiprofen (R-) and flurbiprofen (S+) retained their inhibitory effect onprostaglandin synthesis during the period (36 months at room temperature) ofshelflife analysis. This appeared from identical concentration inhibition curvesusing bovine iris/ciliary body homogenate (results not shown) as compared withfreshly prepared solutions (Figure 3). The ratio of 100 in inhibitory potency for S(+)flurbiprofen vs. R(-) flurbiprofen also remained unchanged as appears from the un-changed IC50 of 10-8 M for S(+) flurbiprofen and of 10-6 M for R(-) flurbiprofen.

Figure 3. Concentration-response curves for inhibition of prostaglandin synthesis in bovineiris/ciliary body homogenate by racemic flurbiprofen (∇ ), R(-)flurbiprofen (O), and S(+)flur-biprofen (�) (derived from reference 14). Concentrations of flurbiprofen are final concen-trations in the assay mixture. For racemic flurbiprofen the concentration values are given inconcentrations of the individual enantiomers. Each point represents the average ± S.E.M.of four to six determinations from different pools of bovine iris/ciliary homogenates.
DISCUSSION
The formulation of an eyedrop, like indomethacin based on a previously publishedphosphate buffer at pH 7.4 (7), is possible for flurbiprofen. Due to the racemicnature of the molecule and the current national and supranational policies (24) torequire quality, safety and efficacy on medicinal products it was deemed necessaryto exploit every possibility to formulate an eyedrop that was free of enantiomericballast and only contained the pharmacologically active moiety, S(+) flurbiprofen.
The first reports on use of indomethacin as an effective eyedrop to combat mac-ula edema after cataract surgery were reassuring but were impractical in pharma-ceutical sense. Short shelflife of indometacin when in aqueous solution, uncertain-ty of the real available concentration when provided as a suspension and irritatingwhen applied as an oily solution. The available specialties that have arrived on theDutch market are not the satisfactory solution for this clinical entity. Indoptol® con-tains the irritating substance phenylethanol and also benzalkoniumchloride the lat-ter which can react with indomethacin to form insoluble complexes that will remainunnoticed in a suspension. Indocollyre® incorporates the for the eye unpleasantsubstance methylparahydroxybenzoate and measures a high osmolality whenbrought in to solution (approximately 1500 mOsm/kg).
58
Chapter 3

The shelflife analysis of a stereospecific ballast free flurbiprofen eyedrop formula-tion was carried out by CZE. To rule out pitfalls as in vitro racemization, analysiswas performed of the enantiomeric ratio of flurbiprofen during the shelflife period.The observed decline in flurbiprofen was not supported by observation of degrada-tion products in the electropherograms. This does not rule out any degradation, asonly UV-active negatively charged compounds within the chosen run time would bedetected. During the investigative period no evidence was found of in vitro inver-sion. The shelflife determination of S(+) flurbiprofen has shown the solution to bestable in glass containers for 48 months (Ocuflur® 36 months in durable plasticcontainer) when one adheres to the limits of maximum 10% degradation. The con-centration limit for the known impurity USP 2-(4-Biphenylyl)propionic acid RS hasnot been exceeded in any of the investigated samples. The enantiomeric inversionof R(-) flurbiprofen to the pharmacologically active S(+) flurbiprofen as observed inseveral species (25) has been ruled out in our assay using homogenates of bovineiris/ciliary body (14). In human blood no chiral inversion could be detected (26).Metabolism of flurbiprofen does not occur in ocular tissues as appeared from expe-riments in rabbits using radioactive labelled material (27).
In the pharmacological assay we investigated the potency of racemic flurbiprofenand the separate enantiomers S(+) and R(-) to inhibit the bovine iris/ciliary bodycyclooxygenase-1 enzyme in producing prostaglandin E2 (14). The S(+) moiety dis-played 50% prostaglandin synthesis inhibition at a concentration of 10-8M (IC50).Extrapolation of in vivo data on the ocular bioavailability of ophthalmic racemic flur-biprofen shows that our present data on the IC50 (10-8M) for inhibition ofprostaglandin synthesis by S(+) flurbiprofen fall well within the concentrations offlurbiprofen, available in aqueous humor and shown to be effective in the eye afterapplication to the outer eye (Table 2).
Table 2. Dose/concentration relationships of racemic flurbiprofen in rabbit and human eye.
Flurbiprofen (nmol) Flurbiprofen (M)Instilled dose in aqueous humor
400* (rabbit) 800 x 10-8*10 (ID50)** (rabbit) 20 x 10-8***50**** (human) 25 x 10-8****
*Values derived from (28), **average value for protein and fluorescein influx, derived from (8), *** extrapolated from (28), **** values derived from (29)
59
Flurbiprofen, S(+), Eyedrops

60
Investigation of the dose-response inhibition curves (8) reveals that racemic flur-biprofen with a concentration of 0.03% produces near maximal effect on the break-down of the blood-aqueous barrier and this will also pertain to our stereospecificophthalmic solution of 0.015%. In contrast to our study the flurbiprofen eyedropsused in clinical investigations or marketed specialities are composed of flurbiprofensodium 0,03%. Flurbiprofen sodium complying to pharmacopoeial standards repre-sents the dihydrate and therefore 0,03% is equivalent to only 0.024% flurbiprofenacid, or 0.012% S(+) flurbiprofen acid.
CONCLUSIONS
Analytical and pharmacological evidence is provided that eyedrops with a mere0.015% flurbiprofen S(+) should suffice for meeting the indications for ophthalmicuse and justifies its use as ballast free stereo specific drug. The shelflife of theseeyedrops can be put at four years when supplied in a glass container. For a com-mercially available eyedrop (i.e. Ocuflur®, durable plastic eye drop container) threeyears is more appropriate.
Acknowledgements: Preparation of all flurbiprofen samples by Jacqueline Loos-vander Sman is greatly appreciated Stichting Wetenschappelijk Onderzoek Rijnstate(SWOR) is indebted for financial support in acquisition of Flurbiprofen enantiomers.
REFERENCES
1. Waitzman, MB. Possible new concepts relating prostaglandins to various ocular functions.Survey of Ophthalmology 1970;14:301-26.
2. Eakins KE, Whitelocke RAF, Perkins ES, Bennett A, and Unger WG. Release of a prostaglandinin ocular inflammation. Nature 1972;239:248-9.
3. Worst JGF. Biotoxizität des Kammerwassers. Eine vereinheitlichende pathologische Theorie,begründet auf hypothetische biotoxische Kammerwasserfaktoren. Klin Mbl Augenheilk1975;167:376-84.
4. Lute NP, Vyth A, De Keizer RJW. Indometacine oogdruppels 0,5%. Pharm Weekbl1980;115:1663-4.
5. Van Nispen tot Pannerden EBLM, Van Sorge AA. Waterige oogdruppels met indometacine inoplossing. Pharm Weekbl 1981;116:386-7.
6. Cox HLM van der Graaf H. Indometacine-oogdruppels als oplossing. Pharm Weekbl1981;116:387-8.
7. Van Sorge AA, Van Nispen tot Pannerden EBLM, Janssen HWM. Oogdruppels met lage con-centratie indometacine: bereidingsvoorschrift en onderzoek naar de werkzaamheid. P h a r mWeekbl 1986;121:1039-46.
8. Van Haeringen NJ, Oosterhuis JA, van Delft JL, Glasius E and Noach EL. A comparison of theeffects of non-steroidal compounds on the disruption of the blood-aqueous barrier. Exp EyeRes 1982;35:271-7.
Chapter 3
61
9. Vane JR. Inhibition of prostaglandinsynthesis as a mechanism of action for aspirin-like drugs.Nature 1971;231:232-5.
10. Takeguchi C and Sih CJ. A rapid spectrophotometric assay for prostaglandin synthase: applica-tion to the study of non-steroidal anti-inflammatory agents. Prostaglandins 1972;2:169-84.
11. Tilden ME, Boney RS, Goldenberg MM and Rosenbaum JT. The effects of topical S(+]-ibuprofenon interleukin-1 induced ocular inflammation in a rabbit model. J Ocul Pharmacol 1990;6:131-5.
12. Tjebbes GWA, van Delft JL, Barthen ER, van Haeringen NJ. d-Flurbiprofen in ocular inflammationinduced by paracentesis of the rabbit eye. Prostaglandins 1990;40:29-33.
13. Stampinato S, Marino A, Bucolo C, Canossa M, Bachetti T, Mangiafico S. Effects of sodiumnaproxen eyedrops on rabbit ocular inflammation induced by sodium arachidonate. J Ocul.Pharmacol. 1991,7:125-133.
14. Van Sorge AA, van Delft JL, Bodelier VMW, Wijnen PH, van Haeringen NJ. Specificity of flur-biprofen and enantiomers for inhibition of prostaglandin synthesis in bovine iris/cilliary body.Prostaglandins Other Lipid Mediat 1998;55:169-77.
15. Kean WF, Lock CJL, Howard-Lock HE. Chirality in antirheumatic drugs. Lancet 1991;338:1565-8.16. Van Sorge AA, Essink AWG, van Delft JL and van Haeringen NJ. Pharmacokinetics of flurbiprofen
enantiomers in two rabbit species. Ophthalmic Research 1997;29:S1: 033.17. Altria KD, Walsh AR and Smith NW. Validation of a capillary electrophoresis method for the enan-
tiomeric purity testing of fluparoxan. J Chromatogr. 1993;645:193-6.18. Nielen MWF. Chiral separation of basic drugs using cyclodextrin-modified capillary zone elec-
trophoresis. Anal. Chem.1993;65:885-93.19. Guttman A and Cooke N. Practical aspects in chiral separation of pharmaceuticals by capillary
electrophoresis. II Quantitative separation of naproxen enantiomers. J Chromatogr A1994;685:155-9.
20. Altria KD, Goodall DM and Rogan MM. Quantitative applications and validation of the resolutionof enantiomers by capillary electrophoresi. Electrophoresis, 1994;15:824-7.
21. Gasper MP, Bethod A, Nair UB and Armstrong DW. Comparison and modeling study of van-comycin, ristocetin A, and teicoplanin for CE enantioseperations. Anal Chem 1996; 68: 2501-14.
22. Ward TJ, Dann III C, Brown AP. Separation of enantiomers using vancomycin in a countercurrentprocess by suppression of electroosmosis. Chirality 1996;8:77-83.
23. Vespalec R, Billiet HAH, Frank J, Bocek P. Vancomycin as a chiral selector in capillary elec-trophoresis: an appraisal of advantages and limitations. Electrophoresis 1996;17:1214-21.
24. Rauws AG, Groen K. Current regulatory (draft) guidance on chiral medicinal products: canada,eec, japan, united states. Chirality 1994;6:72-5.
25. Menzel-Soglowek S, Geisslinger G, Beck WS, Brune K. Variability of inversion of R(-) flurbiprofen in different species. J Pharm Sci 1992;81:888-91.
26. Geisslinger G, Menzel-Soglowek S, Schuster O, Brune K. Stereoselective high performance liq-uid chromatographic determination of flurbiprofen in plasma. J Chrom 1992;573:163-7.
27. Anderson JA, Chen CC, Vita JB, Shackleton M. Disposition of topical flurbiprofen in normal andaphakic rabbit eyes. Arch Ophthalmol 1982;100:642-5.
28. Tang-Liu DD-S, Liu SS, Weinkam RJ. Ocular and systemic bioavailability of ophthalmic flur-biprofen. J Pharmacokin Biopharm 1984;12:611-26.
29. Ellis PP, Pfoff DS, Bloedow DC, Riegel M. Intraocular diclofenac and flurbiprofen concentrationsin human aqueous humor following topical application. J Ocular Pharmacol 1994;10:677-82.
Flurbiprofen, S(+), Eyedrops

62

CHAPTER 4SPECIFITY OF FLURBIPROFEN AND ENANTIOMERSFOR INHIBITION OF PROSTAGLANDIN SYNTHESIS
IN BOVINE IRIS/CILIARY BODY
Adriaan A. van Sorge, Jan L. van Delft, Valérie M.W. Carballosa Coré-Bodelier, Peter H. Wijnen, and Nicolaas J. van Haeringen
Prostaglandins Other Lipid Mediat 1998;55:169-77

ABSTRACT
In the eye prostaglandin production, as stimulated by trauma, is caused by theactivity of the constitutive enzyme cyclooxygenase-1 (COX-1), present in the iris/cil-iary body. For flurbiprofen, a nonsteroid anti-inflammatory drug (NSAID), used ineyedrops, the specificity of racemic flurbiprofen and the enantiomers S(+) and R(-)flurbiprofen in their inhibitory effect on COX-1 was studied, using bovine iris/ciliarybody as source of the enzyme. S(+) is 100 times more potent in COX-1 inhibitionthan R(-). The measured effect of R(-) is not caused by metabolic inversion of inac-tive R(-) to active S(+) during the assay.
INTRODUCTION
Prostaglandin-like activity by vasoactive substances, termed "Irin", already wasdemonstrated in iris tissue of several species by Ambache (1,2). Eakins et al. (3)proved that prostaglandins were released in the aqueous humor in ocular inflam-mation and Miller, Eakins and Atwal (4) found that acetylsalicylate could preventthe, prostaglandin mediated, disruption of the blood-aqueous barrier after paracen-tesis of the anterior chamber in the rabbit. Using this paracentesis model VanHaeringen et al. (5) determined concentration-response curves of the clinical use-ful nonsteroid anti-inflammatory drugs (NSAIDs) indomethacin, diclofenac and flur-biprofen in eyedrops on the influx of protein and of fluorescein into the anteriorchamber of rabbits.
Various NSAIDs inhibit the cyclooxygenase (COX) activity of the enzymeprostaglandin G/H synthase (PGHS, E.C. 1:14.99.1), the rate limiting enzyme in theproduction of pro-inflammatory prostaglandins. COX exists in at least two isoforms:COX-1, the constitutive form, and COX-2 the inducible form. COX-1 was firstlycharacterized in sheep vesicular glands, is present in platelets, kidney, stomachand vascular smooth muscle (6,7) and in the iris/ciliary body (8). COX-2, is inducedin macrophages and other migratory cells, when these are exposed to proinflam-matory agents (7,9); however COX-1 also appears to be involved in prostaglandinsynthesis in both control and stimulated rat macrophages (10).
Both COX-1 and COX-2 isoforms are expressed under physiological conditions inrat (11) and human (12) tissues and constitutive fetal prostaglandin synthesis isprobably mediated by COX-1, whereas COX-2 is upregulated during labour infetal membranes (13). Although COX-1 is recognized to mediate "housekeeping"functions as in the stomach and kidney, from studies using "knockout" mice, thatis mice with no gene function for COX-1 or COX-2, appeared that in COX-2 defi-cient mice COX-1 could contribute to normal inflammatory responses (14) and
64
Chapter 4

that COX-1 deficient mice have a lack of gastric ulceration (15), possibly due toas yet unknown compensatory mechanisms.
The concept of the therapeutic use of NSAIDs as antiinflammatory drugs in gen-eral is based on the ability of NSAIDs to inhibit the COX-2 activity, whereas inhibi-tion of COX-1 may explain the undesired side effects such as gastric and renal tox-icity and bleeding disorders. However the inhibition of COX-1 activity even is adesired effect in the prevention of heart attacks and strokes by aspirin (16), basedon the reduction of thromboxane production in platelets and in the prevention of ocu-lar irritation during cataract extraction (17) and after therapeutic laser treatment ofthe anterior eye (18,19). Flurbiprofen is a racemic mixture of two isoforms: S(+) andR(-) flurbiprofen. The availability of the pure enantiomers of flurbiprofen allows theinvestigation of the anti-inflammatory effects of the optical isomers of this NSAID.Therefore, also with respect to the demands for ballast free stereo specific drugs, weembarked to study the effect of the enantiomers S(+) and R(-) flurbiprofen in com-parison with racemic flurbiprofen on the prostaglandin E2 (PGE2) activity of bovineiris.
MATERIALS AND METHODS
Flurbiprofen and enantiomers were obtained from Duchefa Pharma (Haarlem, TheNetherlands), Fresh bovine eyes were obtained in a slaughterhouse and within twohours post mortem the iris/ciliary body was removed from the eye with tweezersafter resection of the cornea. The iris/ciliary body was homogenized in Tris HCl 0.05M, pH 7.4, containing 1 mM phenylmethylsulfonylfluoride (PMSF), in a ratio of 1iris/ciliary body per mL buffer solution, using a Potter-Elvehjem glass in glasshomogeniser in melting ice.
For determination of PGE2 100 µl of homogenate was incubated with 25 µl ofphosphate buffered saline (PBS) in an 1-ml eppendorf tube at 37°C during 60 min.The effect of flurbiprofen was studied by addition of 25 µL of a solution of appro-priate concentrations, prepared in PBS, reaching final concentrations of 10-4 M to10-10M. The enzyme reaction was stopped by heating for 3 min in boiling water.Blanks were prepared by heating the tubes in boiling water, without incubation at37°C. In the supernatant of centrifugation (30 min at 16,000 g) released PGE2 wasdetermined using a commercially available kit for PGE2 enzyme immune analysis(Cayman Chemical Co., Ann Arbor MI, U.S.A.).
Inhibition of PGE2 release was calculated by the difference of PGE2 release in theabsence and the presence of flurbiprofen expressed in percent of the non-inhibitedrelease. In concentration-response curves the concentrations of flurbiprofen arepresented as final concentrations in the test. For racemic flurbiprofen the concen-trations are given in concentrations of the individual enantiomers.
65
Bovine, iris/ciliary body

For the determination of chiral inversion by iris/ciliary body homogenate, 1 mL ofhomogenate was incubated with 250 µL of 10-4M R(-) or S(+) flurbiprofen in PBS at37°C during 60 min. For the isolation of flurbiprofen enantiomers the procedure wasfollowed as described by Geisslinger et al (20). The incubate was acidified byadding 0.1 mL of 4M hydrochloric acid, followed by extraction into 6.00 mL of ice-cooled hexane-diethylether (8:2, v/v). After centrifugation (5 min. at 1500 g), 5.00mL of the organic layer were removed and evaporated to dryness under a gentlestream of dry nitrogen. The residue was dissolved in 1 mL PBS, acidified with phos-phoric acid and extracted again with 1 mL heptane. The residue after evaporationof the organic layer was dissolved in 75 µL of buffer for capillary zone elec-trophoresis (CZE) and an aliquot was injected into the capillary to determine therelative concentrations of R(-) and S(+) flurbiprofen.
For the analysis an Applied Biosystems (San Jose, CA, U.S.A) Model 270A-HTCZE system was used, equipped with a variable-wavelength UV absorbance detec-tor, operated at 254 nm and a 0.5 s rise time. CZE was performed in a 70-cm x 50-µm-i.d. fused silica capillary (Polymicro Technologies, Phoenix, AZ, U.S.A.) having alength of 50-cm to the detection window. The electrophoresis buffer was prepared byadjusting a 50 mM KH2PO4 solution to pH=6.0 with a solution of 50 mM Na2HPO4.The macrocyclic antibiotic Vancomycin was used as chiral selector (21,22). Theselector was added to the inlet buffer only, at a concentration of 0.6 mM.
The separations were carried out at +15 kV, with the oven temperature set at30°C. Samples were introduced into the capillary via a controlled vacuum injectionof 1 or 2 s corresponding to a volume of approximately 4-8 nL. Sample injectionswere followed by a 0.5-s dip in water in order to wash the electrode and the outsideof the fused silica capillary. Data were recorded using a Fisons Model VG-Multichrom system. The ratio of the enantiomers, which are each others internalstandard, were calculated as the relative peak areas (corrected by migration time).
RESULTS
The concentrations of PGE2 after non-inhibited release from iris/ciliary bodyhomogenate varied from 10-20 ng/mL of assay mixture. The pharmacodynamiceffects of racemic flurbiprofen, S(+) and R(-) flurbiprofen are presented in figure 1.S(+) flurbiprofen (IC50 = 8.0 (-log M)) is equipotent in comparison to racemic flur-biprofen (IC50 = 8.0) but is 100 times more potent than R(-) flurbiprofen (IC50 = 6.0).
In figure 2, the separation of racemic flurbiprofen is presented, showing a baselineresolution with an analysis time of 22 min. In the measurements of possible meta-bolic inversion of the flurbiprofen enantiomers, the optical impurity measured in theR(-) standard for S(+) was 0.7 ± 0.1% (mean ± SEM)(n=3).
66
Chapter 4

Figure 1. Concentration-response curves for inhibition of the COX-1 activity of bovine iris/cil-iary body racemic flurbiprofen (∇ ), R(-) flurbiprofen (�) and S(+) flurbiprofen (�).Concentrations of flurbiprofen are final concentrations in the assay mixture. Each point rep-resents the average ± S.E.M. of four to six determinations from different pools of bovineiris/ciliary body homogenates.
Figure 2. Analysis of racemic flurbiprofen by capillary zone electrophoresis, showing sepa-ration in R(-) and S(+) flurbiprofen.
67
Bovine, iris/ciliary body

Figure 3. Electropherograms of extracted bovine iris/ciliary body homogenate after incuba-tion for 60 min with (A) R(-) flurbiprofen 10-4 M and (B) S(+) flurbiprofen 10-4 M, showing noincrease of optical antipode after incubation. Controls of standard solution of R(-) flurbipro-fen already contain an impurity of 0.7% of the S(+) enantiomer.
For the S(+) standard the optical impurity of R(-) was below the detection limit ofthe assay (approximately 0.1%). The precision and the reproducibility of the enan-tiomer ratios are merely determined by integration errors (influence of noise) for theminor isomer. The measured optical enantiomer concentration of S(+) in the R(-)containing fraction isolated from the incubate was 0.69 ± 0.07% (n=6) (figure 3A)and the concentration of R(-) in the S(+) containing fraction was below the detec-tion limit of 0.1% (n=3) (figure 3B).
DISCUSSION
The enzyme responsible for the prostaglandin production by the porcine iris/ciliarybody has been characterized as COX-1, by an immunocytochemical method, usingsections of tissue which were incubated with rabbit anti COX-1 polyclonal antibodyand treated with goat anti-rabbit IgG, conjugated with 15-nm gold particles (8). Thesame authors also demonstrated that ω/ω-1 hydroxylase activity in porcine ciliarybody can inactivate accumulated prostaglandins (23). In our test we obviouslymeasure the net result of production of PGE2 by COX-1 from arachidonate mobi-lized from endogenous lipids and of inactivation by ω/ω-1 hydroxylase.
The pharmacodynamic profiles of inhibition by S(+) flurbiprofen and racemic flur-biprofen of PGE2 synthesis by the iris/ciliary body are rather similar, but the curve
68
Chapter 4

69
for R(-) flurbiprofen shows a shift of about 2 log units to the right, which means thatthe R(-) enantiomer possesses about 1% of the potency of the S(+) enantiomer.Kulmacz and Lands (24) found R(-) flurbiprofen not inhibitory on COX-1, purifiedfrom sheep seminal vesicles, at concentrations where S(+) flurbiprofen inhibited theenzyme for 94%.
These distinctions between the two enantiomers of flurbiprofen follow the patternobserved with many other enantiomeric pairs of NSAIDs that the (+) isomer is morepotent in COX-1 inhibitory action. With human recombinant PGHS-1 activity fromhuman monocytes the inhibitory action of the (-) enantiomer of pemodolac wasabout 0.07% of that of the (+) enantiomer and the (-) enantiomer of etodolac wasessentially inactive at concentrations up to 10-4 M (25). Also on PGHS-1 purifiedfrom sheep seminal vesicle (-) etodolac was inactive up to 3X10-4 M (26) and (-)ibuprofen was inactive up to 20 times the IC50 of the (+) enantiomer on COX-1activity of blood platelets (27). Metabolic chiral inversion of the R(-) flurbiprofen intothe S(+) enantiomer and the variation between different species has been report-ed, however no reports are available on the chiral inversion in bovine tissue (28).In human plasma no chiral inversion could be detected (20). We could not demon-strate any chiral inversion of the enantiomers by the bovine iris/ciliary body underthe experimental conditions, using a final concentration of 10-4 M of the flurbiprofenenantiomers. Therefore the observed 1% relative inhibitory activity of the R(-) enan-tiomer cannot be explained by inversion to the S(+) enantiomer during the test, butmust be ascribed to intrinsic inhibitory action of the R(-) enantiomer or to the smallamount of S(+) flurbiprofen, present as impurity (0.7%) in the R(-) enantiomer (29).In the resolution methods used in the pharmaceutical industry to separate enan-tiomers from a racemate it is very difficult to remove completely the chiral impuri-ties (30).
Our results suggest that S(+) flurbiprofen might be the therapeutically relevantanti-inflammatory agent in eyedrops intended for use against conditions initiallycaused by activity of COX-1, including intraoperative miosis and postoperative ocu-lar inflammation after surgery or laser treatment. R(-) flurbiprofen can be designat-ed as unnecessary ballast with even no indication of a pro-drug property, whichcould be based on inversion of the less active (-) enantiomer into the far more active(+) enantiomer, as observed in other species as man.
Bovine, iris/ciliary body

REFERENCES
1. Ambache, N. Properties of irin, a physiological constituent of the rabbit's iris. J. Physiol. 135:114-132, 1957.
2. Ambache, N. Further studies on the preparation, purification and nature of irin. J. Physiol.146:255-294, 1959.
3. Eakins, K.E., Whitelocke, R.A.F., Perkins, E.S., et al. Release of prostaglandins in ocular inflam-mation in the rabbit. Nature New Biol. 239:248-249, 1972.
4. Miller, J.D., Eakins,K,E. and Atwal, M. The release of PGE2-like activity into the aqueous humorafter paracentesis and its prevention by aspirin. Inv. Ophthalmol. Vis. Sci. 12:939-942, 1973.
5. van Haeringen, N.J., Oosterhuis J.A., van Delft, J.L., Glasius E. and Noach, E.L. A comparisonof the effects of non-steroidal compounds on the disruption of the blood-aqueous barrier. Exp.Eye Res. 35:271-277, 1982.
6. DeWitt, D.L., Meade E.A., Zeilhofer H.U. PGH Synthase isoenzyme selectivity: the potential forsafer nonsteroidal antiinflammatory drugs. Am. J. Med. 95:40S-46S, 1993.
7. Mitchell, J.A., Akarasereenont, P., Thiemermann, C., Flower, R.J., Vane, J.R. Selectivity of non-steroidal antiinflammatory drugs as inhibitors of constitutive and inducible cyclooxygenase. Proc.Natl. Acad. Sci. USA 90:11693-11697, 1994.
8. Asakura, T., Sano, N., Stichi, H. Prostaglandin synthesis and accumulation by porcine ciliaryepithelium. J. Ocular Pharmacol. 8:333-341, 1992.
9. Xie, W., Robertson, D.L., Simmons DL. Mitogen-inducible prostaglandin G/H synthase: A new tar-get for nonsteroidal anti-inflammatory drugs. Drug Dev. Res. 25:249-265, 1992.
10. Wilborn, J., De Witt, D.L., Peters-Golden, M. Expression and role of cyclooxygenase isoforms inalveolar and peritoneal macrophages. Am. J. Physiol. 268:L294-301, 1995.
11. Feng, L., Sun, W., Xia, Y., Tang, W.W., Chanmugam, P., Soyoola, E., Wilson, C.B., Hwang, D.Cloning two isoforms of rat cyclooxygenase: differential regulation of their expression. Arch.Biochem. Biophys. 307:361-368, 1993.
12. O'Neill, G.P., Ford-Hutchinson, A.W. Expression of mRNA for cyclooxygenase-1 and cyclooxyge-nase-2 in human tissues. FEBS Lett. 330:156-160, 1993.
13. Slater, D.M., Berger, L., Newton, R., Moore, G.E., Bennett, P.R. Expression of cyclooxygenasetypes1 and 2 in human fetal membranes at term. Am. J. Obstet. Gynecol. 172:77-82, 1995.
14. Morham, S.G., Langenbach R., Loftin, C.D., Tiano, H.F., Vouloumanos, N., Jennette, J.C.,Mahler, J.L., Kluckman, K.D., Lee, C.A., Smithies, O. Prostaglandin synthase 2 gene disruptioncauses severe renal pathology in the mouse. Cell 83:473-482, 1995.
15. Langenbach, R., Morham, S.G.,Tiano,H.F., Loftin,C.D.,Ghanayem,B.I.,Chulada,P.C., MahlerJ.F., Lee,C.A., Goulding, E.H., Kluckman, K.D., Kim,H.S., Smithies, O. Prostaglandin synthase 1gene disruption in mice reduces arachidonic acid-induced inflammation and indomethacin-induced gastric ulceration. Cell 83:483-492, 1995.
16. Smith, J.B.., Willis, A.L. Aspirin selectively inhibits prostaglandin production in human platelets.Nature New Biol. 231:235-237, 1971.
17. Flach, A.J. Cyclo-oxygenase inhibitors in ophthalmology. Therapeutic Review. SurveyOphthalmol. 36:259-284, 1992.
18. Hotchkiss, M.L., Robin, A.L., Pollack, I.P., Quigley, H.A. Nonsteroidal anti-inflammatory agentsafter argon laser trabeculoplasty. A trial with flurbiprofen and indomethacin. Ophthalmology91:969-976, 1984.
19. Pillunat, L.E., Wagner, P., Stodtmeister, R. Comparison of topically applied prostaglandin synthesisinhibitors in Nd:Yag-laser surgery. Preliminary results. Fortschr. Ophthalmol. 84:583-586, 1987.
20. Geisslinger, G., Menzel-Soglowek, S., Schuster, O., Brune, K. Stereoselective high-performanceliquid chromatographic determination of flurbiprofen in plasma. J.Chrom. 573: 163-167, 1992.
70
Chapter 4

21. Gasper, M.P., Berthod, A., Nair, U.B., Armstrong, D.W. Comparison and modelling study of van-comycin, ristocetin A, and teicoplanin for CE enantioseparations. Anal. Chem. 68: 2501-2514, 1996.
22. Vespalec, R., Billiet, H.A.H., Frank, J., Bocek, P. Vancomycin as a chiral selector in capillary elec-trophoresis: an appraisal of advantages and limitations. Electrophoresis 17:1214-21, 1996.
23. Asakura, T., Shichi, H. Cytochrome P450-mediated prostaglandin ω/ω-1 hydroxylase activities inporcine ciliary epithelial cells. Exp. Eye Res. 55:377-84, 1992.
24. Kulmacz, R.J., Lands, W.E.M. Stoichiometry and kinetics of the interaction of prostaglandin Hsynthase with anti-inflammatory agents. J. Biol. Chem. 260: 12572-8, 1985.
25. Glaser, K., Sung, M., O'Neill, K., Belfast, M., Hartman, D., Carlson, R., Kreft, A., Kubrak, D.,Hsiao, C.-L., Weichman, B. Etodolac selectively inhibits human prostaglandin G/H synthase 2(PGHS-2) versus human PGHS-1. Eur. J. Pharmacol.281:107-11, 1995.
26. Markey, C.M., Alward, A., Weller, P.E., Marnett, L.J. Quantitative studies of hydroperoxidereduction by prostaglandin H synthase. J. Biol. Chem. 262: 6266-79, 1987.
27. Evans, A.M., Nation, R.L., Sansom L.N., Bochner, F., Somogyi, A.A.: Effect of racemic ibupro-fen dose on the magnitude and duration of platelet cyclo-oxygenase inhibition: relationshipbetween inhibition of thromboxane production and the plasma unbound concentration of S(+)ibuprofen. Br. J. Clin. Pharmacol. 31:131-8, 1991.
28. Menzel-Soglowek, S., Geisslinger, G., Beck,W.S., Brune, K. Variability of inversion of (R) flur-biprofen in different species. J. Pharm. Sci. 81:888-91, 1992.
29. Carabaza, A., Cabre, F., Rotlan, E., Gomez, M., Gutierrez, M., Garcia, M.L., Mauleon, D.Stereoslective inhibition of inducible cyclooxygenase by chiral nonsteroidal antiinflammatorydrugs. J. Clin. Pharmacol. 36:505-12, 1996.
30. Li,Z. J. And Grant, D.J.W. Relationship between physical properties and crystal structures ofchiral drugs. J. Pharm. Sci. 86:1073-8, 1997.
71
Bovine, iris/ciliary body

72

CHAPTER 5FLURBIPROFEN AND ENTIOMERS
IN OPHTHALMIC SOLUTION TESTED AS INHIBITORSOF PROSTANOID SYNTHESIS IN HUMAN BLOOD
Nicolaas J. van Haeringen, Adriaan A. van Sorge, Jan L. van Delft,and Valérie M.W. Carballosa Coré-Bodelier
J Ocular Pharmacol 2000;16:345-52

ABSTRACT
The purpose of this study was to assess the selectivity and potency of the nons-teroidal anti-inflammatory drug (NSAID), flurbiprofen, and its enantiomers in theirinhibition of cyclooxygenase-1 (COX-1) and cyclooxygenase-2 (COX-2). An assaywas used with freshly drawn heparinized human whole blood, incubated with 25mM calcium ionophore A 23187 during 60 min to produce thromboxane B2 (TXB2)by activity of COX-1 in platelets. Incubation with E.Coli lipopolysaccharide (LPS)during 24 hours produced prostaglandin E2 (PGE2) by induction of COX-2 in mono-cytes, suppressing any possible contribution of COX-1 activity by addition of acetyl-salicylic acid. Concentration inhibition curves were determined with racemic, S(+),and R(-) flurbiprofen in final concentrations ranging from 10-3 to 10-10 M. The stere-oselectivity of S(+) flurbiprofen vs. R(-) flurbiprofen, expressed as the reciprocal ofthe ratio of the concentrations giving 50% inhibition (IC50), is 340 for COX-1 and 56for COX-2. The selectivity for COX-1 vs. COX-2, expressed as the reciprocal ratioof the IC50, was 16 for racemic, 32 for S(+), and 5.3 for R(-) flurbiprofen. Meloxicamin the same assay showed COX-2 selectivity with a ratio of 0.19.
INTRODUCTION
Cyclooxygenase (COX; prostaglandin-endoperoxide synthase, E.C.1:14.99.1), therate limiting enzyme in the production of proinflammatory prostaglandins, exists in twoisoforms: COX-1, the constitutive form, and COX-2 the inducible form. COX-1 hasclear physiological functions such as in the protection of the stomach, kidney, andvessel walls, whereas COX-2 is induced by inflammatory stimuli and by cytokines inmigratory and other cells, leading to inflammatory conditions. The therapeutic use ofnon-steroidal anti-inflammatory drugs (NSAIDs), in general, is based on their ability toinhibit the COX-2 activity, while inhibition of COX-1 might explain the undesired sideeffects such as gastric and renal toxicity and hematological disorders.
On the basis of their inhibitory activity on COX-1 and COX-2 at least three majoraspects of NSAIDs are distinguished: 1) preferential COX-1 inhibition, 2) preferen-tial COX-2 inhibition, and 3) nonpreferential inhibition. Selectivities, varyingbetween COX-1 preferential (1-3) and nonpreferential (1,4,5), have been reportedfor flurbiprofen, possibly because of methodological variations .The assay systemsto investigate the potency and selectivity of NSAIDs include intact cells, brokencells, purified enzymes and microsomal preparations of recombinantly expressedenzymes. Some of the reasons for variation have been identified such as the useof animal or human cells, microsomal preparations, incubation time of the assay orprotein binding of the NSAID.
74
Chapter 5

Whole blood, using COX-1 in platelets and induced COX-2 in monocytes repre-sents an in vitro system as close to physiological conditions as possible. It has beenshown to be a satisfactory system for testing the inhibitory action of NSAIDs onCOX-1 and COX-2 activity (3,6-11) accounting for differences in plasma proteinbinding (12) and cellular accumulation. Platelets are known to contain COX-1 andthe concentration of the enzyme remains largely stable, but two- to four-foldincreases can occur in response to stimulation by hormones or growth factors(13,14). COX-2, however, cannot be brought to expression in platelets in responseto lipopolysaccharide (LPS) (15). Therefore, platelets stimulated by calciumionophore represent a useful assay system for COX-1 activity, measuring throm-boxane production as the most distinguished prostanoid. Normal peripheral bloodmonocytes express COX-1 but can be induced to express COX-2 by LPS to 10 -20-fold after 6-24 hours (15,16). This represents a useful assay system for COX-2activity, measuring PGE2 or thromboxane as metabolite, when suppressing anypossible contribution of COX-1 activity by addition of aspirin (acetylsalicylic acid).Aspirin acetylates platelet COX-1, thereby causing irreversible loss of its cyclooxy-genase activity (17). The inactivation of COX-1 is complete by 20 min (18) andexcess of aspirin itself is hydrolyzed in blood with a half-life time of 30 min (10)before expression of COX-2 by LPS is fully developed.
The NSAID flurbiprofen, as used in eyedrops, is on the one hand effective againstinflammatory responses of the eye (19-21) caused by activity of the COX-1 of theiris (22); on the other hand in systemic use, it is effective in arthritis (23) caused byinduction of COX-2 (24,25).
Flurbiprofen is a racemic mixture of S(+) and R(-) enantiomers, and its effect islargely attributed to the inhibitory action of the S(+) enantiomer, reportedly beingabout 100 - 10,000 times more effective than the R(-) enantiomer when measuredon COX-1 or COX-2 (10,26-28). There are sufficient differences between theenzymes from different species, such that selectivity and potency established withanimal enzymes is not always predictive of effects on human enzymes and no dataare available on the potency or selectivity of the flurbiprofen enantiomers on COX-1 and COX-2 in human blood. In this study, we report dose effect inhibition curvesfor racemic, S(+) and R(-) flurbiprofen using the human whole blood assay. In com-parison the preferential COX-2 inhibitor, meloxicam, was also investigated inrespect of its enzyme selectivity.
MATERIALS AND METHODS
MaterialsFlurbiprofen and the enantiomers were obtained from Duchefa Pharma bv,Haarlem, The Netherlands. The enantiomeric impurity of S(+) flurbiprofen was
75
Human blood

<0.1% and of R(-) flurbiprofen 0.7% (29). Stock solutions of flurbiprofen were pre-pared in a phosphate buffer pH 7.4 with a concentration of 0.03% for racemic flur-biprofen and 0.015% for the enantiomers (for details see 29). Meloxicam was a giftfrom Boehringer Ingelheim, Germany. Calcium ionophore A 23187, dimethylsulfox-ide (DMSO) and LPS, derived from E.Coli 0.111;B4, were obtained from Sigma (StLouis, MO, USA). Assay kits for enzyme immune analysis of Thromboxane B2
(TXB2) and of prostaglandin E2 (PGE2) were purchased from Cayman ChemicalCo. (Ann Arbor, MI, U.S.A.).
Measurement of COX-1 ActivityFor the determination of COX-1 activity 900 µl of freshly drawn heparinized humanblood was incubated at 37°C with 2 µl of calcium ionophore A23187 (12.5 mM inDMSO) and 100 µl of phosphate buffered saline (PBS) for 30 min. Controls wereprepared by incubation of 900 µl of blood with 2 µl of DMSO and 100 µl of PBS.The reaction was terminated by chilling quickly on ice. Plasma was separated bycentrifuging, stored at -20°C, and TXB2 levels were determined.
Measurement of COX-2 ActivityFor the determination of COX-2 activity, 900 µl of heparinized human blood wasincubated at 37°C with 10 µl of acetylsalicylic acid (1 mg/ml in PBS), 2 µl of LPS(E.Coli 0111:B4, 5 mg/ml in DMSO), and 100 µl PBS for 24 hr. Controls were pre-pared by incubation of 900 µl of blood with 10 µl of acetylsalicylic acid, 2 µl ofDMSO, and 100 µl PBS. The reaction was terminated by quickly chilling on ice.Plasma was separated by centrifuging, stored at -20°C, and PGE2 levels weredetermined.
Enzyme Inhibition by Flurbiprofen and by MeloxicamThe effect of flurbiprofen was studied by substitution of 100 µl of PBS in the assays,by 100 µl of an appropriate dilution in PBS of the ophthalmic solution, reaching finalconcentrations of 10-3 to 10-10 M. Meloxicam was studied using appropriate solu-tions in PBS. Inhibition of enzyme activity was calculated by the difference of TXB2-or PGE2 - release in the absence and the presence of flurbiprofen or meloxicam,expressed in percent of the noninhibited release. From concentration-responseinhibition curves the concentration giving 50% inhibition was extrapolated and pre-sented as IC50 .
RESULTS
Addition of calcium ionophore A23187 to human blood resulted in the generation oflarge amounts of TXB2 in the plasma (128±16 ng/ml/30 min) caused by COX-1
76
Chapter 5
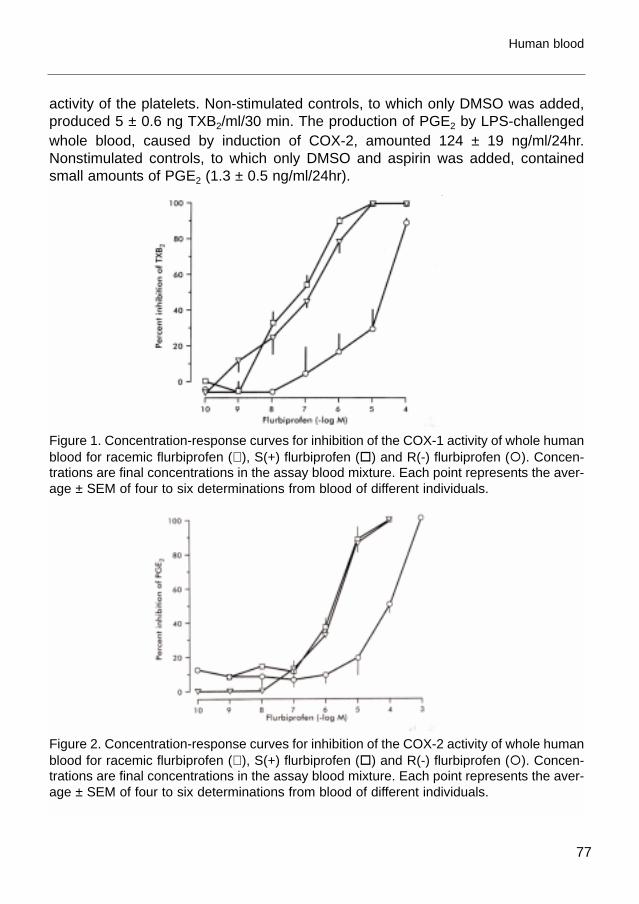
activity of the platelets. Non-stimulated controls, to which only DMSO was added,produced 5 ± 0.6 ng TXB2/ml/30 min. The production of PGE2 by LPS-challengedwhole blood, caused by induction of COX-2, amounted 124 ± 19 ng/ml/24hr.Nonstimulated controls, to which only DMSO and aspirin was added, containedsmall amounts of PGE2 (1.3 ± 0.5 ng/ml/24hr).
Figure 1. Concentration-response curves for inhibition of the COX-1 activity of whole humanblood for racemic flurbiprofen (∇ ), S(+) flurbiprofen (�) and R(-) flurbiprofen (�). Concen-trations are final concentrations in the assay blood mixture. Each point represents the aver-age ± SEM of four to six determinations from blood of different individuals.
Figure 2. Concentration-response curves for inhibition of the COX-2 activity of whole humanblood for racemic flurbiprofen (∇ ), S(+) flurbiprofen (�) and R(-) flurbiprofen (�). Concen-trations are final concentrations in the assay blood mixture. Each point represents the aver-age ± SEM of four to six determinations from blood of different individuals.
77
Human blood

Dose response inhibition curves of racemic flurbiprofen and its S(+) and R(-) enan-tiomers on the activity of COX-1 and COX-2 isoenzymes in the whole blood modelare presented in figures 1 and 2. Results of meloxicam in the same assay are pre-sented in figure 3. In table 1 the IC50 values are presented together with the enzymeselectivity, expressed as the COX-2/COX-1 ratio, for racemic flurbiprofen, its R(-)and S(+) enantiomers and for meloxicam.
Figure 3. Concentration-response curves for inhibition of COX-1 (� ) and COX-2 (�) activ-ity of whole human blood for meloxicam. Concentrations are final concentrations in theassay blood mixture. Each point represents the average ± SEM of four to six determina-tions from blood of different individuals.
Table 1. Selectivities of NSAIDs for COX-1 and COX-2 in Human Blood.
COX-1 COX-2 COX-2/COX-1IC50 µM IC50 µM
racemic flurbiprofen 0.14 ± 0.04 2.2 ± 0.2 16 ± 5S(+) flurbiprofen 0.056 ± 0.030 1.8 ± 0.4 32 ± 24R(-) flurbiprofen 19 ± 6 100 ± 32 5.3 ± 3.4meloxicam 3.0 ± 1.1 0.56 ± 0.26 0.19 ± 0.16
IC50 are mean values derived from the concentration response inhibition curves.
78
Chapter 5
DISCUSSION
This is the first report to establish in the human whole blood assay the stereoselec-tive inhibition of COX-1 and COX-2. The assays used were adapted from (3,8) andseveral authors of different research groups reported their results using this method,testing many NSAIDs, including racemic flurbiprofen (3,30) and meloxicam (31).
The whole blood system is very useful in that in vitro it may reflect better the invivo effectiveness of NSAIDs with contributing factors as protein-binding. Theprostanoid production in this assay is measured under conditions in which arachi-donic acid is generated from endogenous lipid pools rather than added in artificial-ly high (10 µM) exogenous concentrations as in other assays (28).
S(+) flurbiprofen, as in general for racemic mixtures of NSAIDs, is the more potentinhibitor of both COX isoenzymes than the R(-) isomer (9,10,32,33). The enan-tioselectivity of S(+) flurbiprofen, expressed as the ratio of the IC50 of the R(-) andthe S(+) isomer (R/S), amounts to 340 for COX-1 and 56 for COX-2. The differencein selectivity found in this study may be explained by a possible greater steric hin-drance of the binding of R(-) flurbiprofen to COX-1 than to the COX-2 enzyme. Theaccessibility of the binding site for flurbiprofen, competing with arachidonate bin-ding at the catalytic domain of the COX-1 structure, has been found to be morerestricted than in the COX-2 structure (34-36).
On the other hand the inhibitory effect measured with the R(-) isomer has beenascribed to the small amount of S(+) present as impurity in the ineffective R(-) isomer(13) Theoretically the 0.7% impurity should give a R/S ratio of about 140 and a small-er ratio might be due to metabolic inversion of the R(-) into the S(+) isomer. Metabolicinversion, however, has been demonstrated to be absent in human blood (37).
Within the errors of the methods used, the inhibition curves of the various concen-trations of flurbiprofen racemate and the S(+) isomer were found to run closely par-allel, reflecting the two-fold (0.3 log-unit) greater concentration of the pure S(+) iso-mer as compared to the racemate (figures 1 and 2). These results correspond wellwith data obtained from eicosanoid production in ex vivo experiments in rats (26).
We confirmed the selectivity of flurbiprofen towards COX-1 as found by Young etal. (3), who also used the human blood assay. The ratio COX-2/COX-1 was 16 forracemic flurbiprofen, although the IC50 values for both enzymes were about 4 timeslower in the present study. The ratio COX-2/COX-1 was 32 for S(+) flurbiprofen and5.3 for R(-) flurbiprofen, which is higher than found with guinea pig whole blood,where for S(+) flurbiprofen was found 1.0 and for R(-) flurbiprofen 0.48 (10). Geneticdifferences of human and guinea pig COX-2 are most likely responsible for thesedifferences, as has also been suggested for human and murine COX-2 (38).
Meloxicam has been found in a number of other assay systems to be selectivetowards COX-2 (6,7,39,40). Figure 3 shows that meloxicam inhibits COX-2 in
79
Human blood

human whole blood at concentrations that are at least 5 times lower than thoserequired to inhibit COX-1. It was also observed that meloxicam (IC50 0.56 x 10-6M)displayed more potency towards COX-2 than S(+) flurbiprofen (IC50 1.8 x 10-6M).
REFERENCES
1. Barnett, J., Chow, J., Ives, D., Chiou, M., Mackenzie, R., Osen, E., Nguyen, B., Tsing, S., Bach,C., Freire, J., Chan, H., Sigal, E., and Ramesha, C. Purification, characterization and selectiveinhibition of human prostaglandin G/H synthase 1 and 2 expressed in the baculovirus system.Biochem. Biophys. Acta 1209:130-139, 1994.
2. DeWitt, D.L., Meade, E.A., and Smith, W.L. PGH Synthase isoenzyme selectivity: The potentialfor safer nonsteroidal anti-inflammatory drugs. Am. J. Med. 95 (Suppl2A):40S-46S, 1993.
3. Young, J.M., Panah, S., Satchawatcharaphong, C., and Cheung, P.S. Human whole bloodassays for inhibition of prostaglandin G/H synthases-1 and-2 using A 23187 and lipopoly-sac-charide stimulation of thromboxane B2 production. Inflamm. Res. 45:246-253, 1996.
4. Mitchell, J.A., Akarasereenont, P., Thiemermann, C., Flower, R.J., and Vane, J.R. Selectivity ofnonsteroidal antiinflammatory drugs as inhibitors of constitutive and inducible cyclooxygenase.Proc. Natl. Acad. Sc.USA 90:11693-11697, 1993.
5. Riendeau, D., Percival, M.D., Boyce, S., Brideau, C., Charleson, S., Cromlish, W., Ethier, D., Evans,J., Falgueyret, J.P., Mancini, J.A., O'Neill, G., Ouellet, M., Rodger, I.W., Therien, M., Wang, Z., Webb,J.K., Wong, E., Xu,L., Young, R.N., Zamboni, R., Prasit, P., and Chan, C.C. Biochemical and phar-macological profile of a tetrasubstituted furanone as a highly selective COX-2 inhibitor. Brit. J.Pharmacol. 121:105-117, 1997.
6. Fenner, H. Differentiating among nonsteroidal anti-inflammatory drugs by pharmacokinetic andpharmacodynamic profiles. Semin. Arthritis Rheum. 26(Suppl 1):28-33, 1997.
7. Pairet, M. Selective COX-2 inhibitors: a pharmacological profile. Curr. Opinion Rheumatol.8;(Suppl 1):S15-S19, 1996.
8. Patrignani, P., Panara, M.R., Greco, A., Fusco, O., Natoli, C., Iacobelli, S., Cipollone, F., Ganci, A.,Créminon, C., Maclouf, J., and Patrono, C. Biochemical and pharmacological characterization ofthe cyclooxygenase activity of human blood prostaglandin endoperoxide synthases. J. Pharmacol.Exp. Therap. 271:1705-1712, 1994.
9. Glaser, K., Sung, M.L., O'Neill, K., Belfast, M., Hartman, D., Carlson, R., Kreft, A., Kubrak, D.,Hsiao, C.L., and Weichman, B. Etodolac selectivity inhibits human prostaglandins G/H synthase2 (PGHS-2) versus human PGHS-1. Eur. J. Pharmacol. 281:107-111, 1995.
10. Carabaza, A., Cabré, F., Rotlan, E., Gómez,M., Gutiérrez, M., García, L., and Mauleón, D.Stereoselective inhibition of inducible cyclooxygenase by chiral nonsteroidal anti-inflammatorydrugs. J. Clin. Pharmacol. 36:505-512, 1996.
11. Brideau, C., Kargman, S., Liu, S., Dallob, A.L., Ehrich, E.W., Rodger, I.W., and Chan, C.C. Ahuman whole blood assay for clinical evaluation of biochemical efficacy of cyclooxygenaseinhibitors. Inflamm. Res. 45:68-74, 1996.
12. Knadler, M.P.,Brater, D.C., and Hall, S.D. Plasma protein binding of flurbiprofen: enantioselectiv-ity and influence of pathophysiological status. J. Pharmacol. Exp.Ther. 249:378-385, 1989.
13. DeWitt, D.L. Prostaglandin endoperoxide synthase: regulation of enzyme expression. Bioch.Biophys. Acta 1083:121-134, 1991.
14. Wu, K.K., Sanduja, R., Tsai, A., Ferhanoglu, B., and Loose-Mitchell, D.S. Aspirin inhibits inter-leukin 1-induced prostaglandin H synthase expression in cultured endothelial cells. Proc. Natl.Acad. Sci. USA 88:2384-2387, 1991.
80
Chapter 5

15. Hla, T., and Neilson, K. Human cyclooxygenase-2 cDNA. Proc. Natl. Acad. Sci. USA 89:7384-7388, 1992.
16. Hla, T., Ristimäki, A., Appleby, S., and Barriocanal, J.G. Cyclooxygenase gene expression ininflammation and angiogenesis. Ann. NY. Acad. Sci. 696:197-204, 1993.
17. Roth, G.J., Stanford, N., and Majerus, P.W. Acetylation of prostaglandin synthase by aspirin.Proc. Natl. Acad. Sci. USA 72:3073-3076, 1975.
18. Meade, E.A., Smith, W.L., and DeWitt, D.L. Differential inhibition of prostaglandin peroxide syn-thase (cyclooxygenase) isoenzymes by aspirin and other nonsteroidal anti-inflammatory drugs.J. Biol. Chem. 268:6610-6614, 1993.
19. Flach, A.J. Cyclo-oxygenase inhibitors in ophthalmology. Therapeutic Review. Surv. Ophthalmol.36:259-284, 1992.
20. Hotchkiss, M.L., Robin, A.L., Pollack, I.P., and Quigley, H.A. Nonsteroidal anti-inflammatoryagents after argon laser trabeculoplasty. A trial with flurbiprofen and indomethacin.Ophthalmology 91:969-976, 1984.
21. Pillunat, L.E., Wagner, P., and Stodtmeister, R. Comparison of topically applied prostaglandinsynthesis inhibitors in Nd:Yag-laser surgery. Preliminary results. Fortschr. Ophthalmol. 84:583-586, 1987.
22. Asakura, T., Sano, N., and Stichi, H., Prostaglandin synthesis and accumulation by porcine cil-iary epithelium. J. Ocul. Pharmacol. 8:333-341, 1992.
23. Benvenuti, C., Guidoni, G., Longoni, A., and Mordini, M. Controlled study on flurbiprofen anddiclofenac in the treatment of rheumatic disorders. Int. J. Tissue React. 5:61-65, 1983.
24. Xie, W., Robertson, D.L., and Simmons, D.L. Mitogen-inducible prostaglandin G/H synthase: anew target for nonsteroidal anti-inflammatory drugs. Drug Dev. Res. 25:249-265, 1992.
25. Brune, K., Menzel-Soglowek, S., and Zeilhofer, H.U. Differential analgesic effects of aspirin-likedrugs. Drugs 44(Suppl. 5): 52-59, 1992.
26. Peskar, B.M., Kluge, S., Peskar, B.A., Soglowek, S.M., and Brune, K. Effects of pure enan-tiomers of flurbiprofen in comparison to racemic flurbiprofen on eicosanoid release from variousrat organs ex vivo. Prostaglandins 42:515-531, 1991.
27. Van Sorge, A.A., van Delft, J.L., Bodelier, V.M.W., Wijnen, P.H., and van Haeringen, N.J.,Specificity of flurbiprofen and enantiomers inhibition of prostaglandin synthesis in bovine iris/cil-iary body. Prostaglandins OtherLip.Mediat. 55:169-177, 1998.
28. Laneuville, O., Breuer, D.K., Dewitt, D.L., Hla, T., Funk, C.D., and Smith,W.L. Differential inhibi-tion of human prostaglandin endoperoxide H synthases-1 and -2 by nonsteroidal anti-inflamma-tory drugs. J. Pharmacol. Exp. Ther. 271:927-934, 1994.
29. Van Sorge, A.A., Wijnen, P.H., Van Delft, J.L., Carballosa Coré-Bodelier, V.M.W., and VanHaeringen, N.J. Flurbiprofen, S(+), eyedrops; formulation, enantiomeric assay, shelf-life andpharmacology. Pharm. World Sci. 21:91-95, 1999.
30. Santini, G., Sciulli, M.G., Panara, M.R., Padovano,R., Giamberardino, M., Rotondo, M.T., DelSoldato, P., and Patrignani, P. Effects of flurbiprofen and flurbinitroxybutylester on prostaglandinendoperoxide synthases. Eur. J. Pharmacol. 316: 65-72, 1996.
31. Patrignani, P., Panara, M.R., Sciulli, M.G., Santini, G., Renda, R., and Patrono, C. Differential inhi-bition of human prostaglandin endoperoxide synthase-1 and -2 by nonsteroidal anti-inflammato-ry drugs. J. Physiol Pharmacol. 48:4623-4663, 1997.
32. Kulmacs, R.J., and Lands, W.E.M. Stoichiometry and kinetics of the interaction of prostaglandinH synthase with anti-inflammatory agents. J Biol Chem. 260:12572-12578, 1985.
33. Evans, A.M., Nation,R.L., Sansom, L.N., Bochner, F., and Somogyi, A.A. Effect of racemic ibupro-fen dose on the magnitude and duration of platelet cyclooxygenase inhibition: Relationshipbetween inhibition of thromboxane production and the plasma unbound concentration of S(+)-ibuprofen. Br. J. Clin. Pharmacol. 31:131-138, 1991.
81
Human blood

34. Picot, D., Loll, P.J., and Garavito, R.M. The X-ray crystal structure of the membrane proteinprostaglandin H2 synthase-1. Nature 367:243-249, 1994.
35. Luong, C., Miller, A., Barnett, J., Chow, J., Ramesha, C., and Browner, M.F. Flexibility of the NSAIDbinding site in the structure of human cyclooxygenase-2. Nature Struct. Biol. 3:927-933, 1996.
36. Hawkey, C. J. COX-2 Inhibitors. Lancet 353:307-314, 1999.37. Geisslinger, G., Menzel-Soglowek, S., Schuster, O., and Brune, K. Stereoselective high-perform-
ance liquid chromatographic determination of flurbiprofen in human plasma. J. Chromatogr.573:163-167, 1992.
38. Berg, J., Fellier, H., Hartmann, M., Kremminger, P., Blaschke, H., Christoph,T., Bodenteich, A.,Rovensky, F., Stimmeder, D., and Towart, R. Novel selective cyclooxygenase-(COX)-2 inhibitorsof the diarylethersulfonamide type show greater inhibition on human COX-2 than on murineCOX-2. Naunyn Schmiedeberg Arch. Pharmacol. 358(Suppl. 2): R716, 1998.
39. Frölich, J.C. A classification of NSAIDs according to the relative inhibition of cyclooxygenaseisoenzymes. TIPS 18:30-34, 1997.
40. Engelhardt, G., Bögel, R., Schnitzler, C., and Utzmann, R. Meloxicam: influence on arachidonicacid metabolism. In vitro findings-part 1. Biochem Pharmacol 51:21-28, 1996.
82
Chapter 5

CHAPTER 6CONSTITUTIVE CYCLOOXYGENASE-1 AND
INDUCED CYCLOOXYGENASE-2 IN ISOLATED HUMAN IRISINHIBITED BY S(+) FLURBIPROFEN
Nicolaas J. van Haeringen, Adriaan A. van Sorge, and Valérie M.W. Carballosa Coré-Bodelier
J Ocular Pharmacol 2000;16:535-61

ABSTRACT
The purpose of the present study was to characterize the isoforms of cyclooxyge-nase (COX) in the human iris before and after stimulation withlipopolysaccharide(LPS) and to determine the selectivity of the nonsteroidal anti-inflammatory drug(NSAID,) S(+) flurbiprofen, for inhibition of COX-1 and COX-2 in homogenates ofthis tissue. Spotblots were made of extracts of human iris in the absence and pres-ence of LPS plus acetylsalicylic acid (aspirin). After reacting with anti-COX-1 andanti-COX-2 immunoglobulin G, the presence of both immunoreactive COXenzymes was substantiated using an indirect immunoperoxidase method. AuthenticCOX-1 and COX-2 were used as controls. Using an enzyme immune assay (EIA),the production of prostaglandin E2 (PGE2) was quantified in tissue homogenates ofhuman iris under the same conditions as described above. S(+) flurbiprofen wasadded to tissue homogenates in order to determine the inhibitory effect on PGE2
production. Half maximal inhibitory concentrations (IC50) of S(+) flurbiprofen for thePGE2 production in the tissue homogenates were determined from concentrationinhibition curves.
The selectivity of S(+) flurbiprofen for inhibition of COX-1 was expressed as theratio of IC50 for COX-2 / COX-1. Spotblots of non-stimulated iris-extracts showedpositive staining for COX-1 immunoreactivity (-ir) only. After incubation with LPS plusacetylsalicylic acid, positive staining was observed for both COX-1-ir and COX-2-ir.Concentrations of PGE2, released from homogenates of untreated iris varied from1.5-4 ng/ml and of LPS-stimulated tissue from 10-20 ng/ml of assay mixture.
S(+) flurbiprofen inhibited PGE2 production of untreated tissue homogenates atan IC50 of 8x10-10 M, whereas in the stimulated tissue IC50 was found to be 3x10-6M.The selectivity of S(+) flurbiprofen for inhibition of constitutively present COX-1, rel-ative to the inhibition of induced COX-2, was 3,600.
Our results indicate that specific expression of COX isoforms in normal human iriswas substantiated at the protein level by immunoreaction on spotblots. COX-1 re-presents the constitutively present enzyme, and COX-2 appears after stimulation withLPS. At the functional level, S(+) flurbiprofen possesses a specificity for COX-1 ininhibiting PGE2 production.
INTRODUCTION
The iris is the major site for prostaglandin (PG) formation in the eye. Theseprostanoids act through prostanoid receptors (1) to regulate smooth muscle con-traction, blood-aqueous-barrier penetration and intraocular pressure. PGs are syn-thesized by a multistep pathway from arachidonic acid, which is either released
84
Chapter 6

from membrane phospholipids by phospholipase A2 (phosphatide 2-acylhydrolase,EC 3.1.1.4) (2) or from intracellular triacylglycerols by triacylglycerol acylhydrolase(EC 3.1.1.3) (3). Their formation is catalyzed by the cyclooxygenase (COX) and glu-tathione-dependent peroxidase activities of PG endoperoxide synthase (EC1.14.99.1). Two isoforms of COX have been characterized. COX-1 was initially iso-lated from sheep seminal vesicles (4) and is constitutively expressed in a varietyof normal tissues (5) such as stomach, kidney, platelets, and in iris/ciliary body (6).However, it has been reported, that also COX-1 can make an important contribu-tion to inflammatory responses (7). COX-2 is essentially expressed only followingcell activation (8); however one exception to the low constitutive expression ofCOX-2-ir is the brain (9). Expression is time dependent and induced by variousmediators of inflammation and bioactive agents such as lipopolysaccharides (10),cytokines (11), tumor necrosis factor (TNF) (11) and platelet activating factor (PAF)(12). COX-2 induction has been described in a variety of cells including migratorycells such as monocytes and macrophages. Also in ocular rabbit models of inflam-mation, COX-2 activity is found in endothelium (13) and epithelium (14) of thecornea and in iris/ciliary body (15).
The elicited, immediate, production of PGs by the non-inflamed iris in vivo hasbeen described following several experimental manipulations including paracente-sis (16), mechanical stimulation (17), alkali burns (18), arachidonic acid adminis-tration (19), laser photocoagulation (20), and homogenization in vitro (21). Timerelated PG production has been observed after induction of uveitis with bovineserum albumin (22) or endotoxin (23). The PG synthesis in the normal iris/ciliarybody has been suggested to be due to COX-1 (24) activity, being dependent sole-ly on the availability of arachidonic acid.
Induction of COX-2 may be an explanation for increased prostaglandin formationby the inflamed iris/ciliary body during long term consequences of eye injury, infec-tion or intra-vitreal injection of endotoxin. Microsomes of rabbit iris/ciliary body syn-thesize increased amounts of cyclooxygenase products after intravitreal injection ofendotoxin (25). The induction of COX-2 mRNA in the rabbit iris has been demon-strated within three hours following surgery of the iris (15). In contrast paracentesisfailed to induce COX-2 mRNA (15). This suggests that, at least, trauma or resectionof the iris is required for the appearance of COX-2 mRNA.
The therapeutic use of non steroidal anti-inflammatory drugs (NSAIDs) is, in ge-neral, thought to be based on their ability to inhibit the induced COX-2 activity, beingresponsible for the signs of inflammation. Inhibition of COX-1 may explain the unde-sired side-effects, such as gastric and renal toxicity and bleeding disorders.However, in ophthalmology, during cataract extraction and laser treatment of theanterior eye, inhibition of constitutively present COX-1 accounts for the therapeuticeffect of NSAIDs as prophylactic treatment to prevent miosis and ocular irritation.
85
Human iris

Although data are available on the potency and/or selectivity of several NSAIDs onCOX-1 and COX-2 in human blood (26) , of bromfenac and nimesulide on the rabitiris/ciliary body (27), and of flurbiprofen on the bovine iris/ciliary body (24), no studyhas been performed on human ocular tissue. In the present study, we report theinduction of COX-2 by stimulation with LPS in the human iris and dose effect inhibi-tion curves of S(+) flurbiprofen on COX-1 and COX-2 in homogenates of human iris.
MATERIALS AND METHODS
MaterialsHuman iris tissue with a post mortem time varying from 24-30 hrs was provided bythe Cornea Bank Amsterdam. Lipopolysaccharide (LPS), derived from E.Coli0.111;B4, was purchased from Sigma (St Louis, MO, USA). COX-1 peptide (sc-1752 P), COX-2 peptide (sc-1745 P), goat anti-COX-1 immunoglobulin G (sc-1752), goat anti-COX-2 immunoglobulin G (sc-1745), and horseradish peroxydase-labeled polyclonal anti-goat immunoglobulin G (anti-goat IgGHRP; sc 2020) werepurchased from Santa Cruz Biotechnology Inc.(Santa Cruz, USA). S(+) flurbiprofenwas obtained from Duchefa Pharma bv (Haarlem, The Netherlands). Assay kits forenzyme immune analysis of PGE2 and enzyme activity of phospholipase A2 werefrom Cayman Chemical Co. (Ann Arbor MI, U.S.A.). A solution, containing3,3'diaminobenzidine (DAB) tetrahydrochloride and H2O2 was purchased from ICNBiomedicals Inc. (Amsterdam, The Netherlands).
Stimulation of Iris Tissue with LPSFor the induction of COX-2 the isolated iris, in a ratio of one tissue per 300 µl PBS,was incubated with 1 µl of a solution of LPS containing 5 mg/ml in DMSO and with10 µl of acetylsalicylic acid (10 mg/ml in PBS) during 24 hrs at 37ºC.
Immunoprecipitation and Identification of COX-immunoreactivity Isoforms Human iris tissue was homogenized in sodium dodecyl sulfate sample buffer (125mM Tris HCl, 4% sodium dodecyl sulfate, 20% glycerol, 1% dithiothreitol, pH6.8),boiled for 5 min and centrifuged for 5 min at 16,000 g. Nitrocellulose membrane wasspotblotted with 15 µl of the supernatant and 3 µl of the control COX-1- and COX-2 peptide, treated with blocking buffer (50 mM Tris, 0.15 M NaCl, 0.5% Tween-20,2% non-fat dry milk, 0.02% sodium azide, pH 10) for 90 min and probed using goatanti-COX-1 or anti-COX-2 at a 1:500 dilution in blocking buffer during 90 min.
After three washings of 5 min in washing buffer (10 mM Tris, 0.15 M NaCl, 0.05%Tween-20, pH 8) the blot was treated with anti-goat IgGHRP at a 1:1000 dilution inblocking buffer during 30 min.
86
Chapter 6

After three washings of 5 min in washing buffer and one washing in buffer contain-ing 10 mM Tris and 0.15 M NaCl staining was developed with a solution, contain-ing DAB tetrahydrochloride and H2O2.
Measurement of Prostaglandin E2 ProductionThe assay was performed in a modified form according to Van Sorge (24). Humaniris tissue was homogenized in Tris HCl 0.05 M, pH 7.4, containing 1 mM phenyl-methylsulfonylfluoride (PMSF), in a ratio of 1 iris per 400 µl buffer solution, using aPotter-Elvehjem glass in glass homogeniser in melting ice. For determination ofCOX activity 100 µl of homogenate was incubated with 25 µl of phosphate bufferedsaline (PBS) in a 1-ml Eppendorf tube at 37°C during 60 min. The effect of S(+) flur-biprofen was studied by addition of 25 µl of an appropriate dilution of the stock solu-tion in PBS. The enzyme reaction was stopped by heating for 3 min in boiling water.Blanks were prepared by heating the tubes in boiling water, without previous incu-bation. In the supernatant of centrifugation (30 min at 16,000 g) released PGE2 wasdetermined. The assay proved linear for the incubation time used and proportionalto the amount of tissue-homogenate with, on average, 96% recovery. Inhibition ofPGE2 synthesis by S(+) flurbiprofen was calculated as a percentage of the activityin the presence versus the activity in the absence of the drug.
The potency of the drug for COX was assessed by calculating the concentrationof the drug causing 50% inhibition (IC50) of the maximal activity. The selectivity ofS(+) flurbiprofen for the two COX isoforms is expressed as the ratio of the IC50 forCOX-2 versus COX-1. The higher the ratio, the more potently S(+) flurbiprofeninhibits COX-1 relative to COX-2.
Measurement of Phospholipase A2 ActivityPhospholipase A2 activity was measured in human iris tissue homogenate, pre-pared as described above. In a kinetic assay using diheptanoyl-thio-phosphatidyl-choline as substrate and 5,5"-dithiobis(2-nitrobenzoic acid) (DTNB) as colorreagent the enzyme activity was measured at 414 nm and calculated inµmol/min/ml of homogenate, using the DTNB extinction coefficient of 10.66 mM-1.
RESULTS
The presence of COX-1 immunoreactivity (-ir) and COX-2-ir was substantiated inextracts of human iris, either untreated or following stimulation with LPS, using invitro incubation experiments. Acetylsalicylate was added together with LPS to elim-inate any COX-1 activity in the iris by irreversible binding to the enzyme. To detectthe two isoforms of COX in the homogenates of the differently treated tissues, spot-blots were treated with anti-COX-1 antibody on the blotting paper, followed by
87
Human iris

immunoperoxidase labeling. Representative immunoblots with positive staining forCOX-1-ir or COX-2-ir in both untreated and LPS-incubated iris ciliary body tissueare shown in figure 1. Controls of authentic COX-1 peptide but not COX-2 peptideshowed positive staining. Treatment with anti-COX-2 produced staining of COX-2-ir only with LPS-incubated tissue and not with untreated iris tissue extract. Positivestaining was detected using control COX-2 peptide but not COX-1 peptide.
Figure 1. Detection of cyclooxygenase in human iris extracts. Authentic COX-1 and COX-2peptide and 15 µl of tissue extract were spotblotted on nitrocellulose membrane.Cyclooxygenase was detected using immunoglobulin G specific for COX-1 or for COX-2.With anti-COX-1, spots were observed in untreated iris, LPS-treated iris and with COX-1 pep-tide. With anti-COX-2, spots were observed in LPS-treated iris only and with COX-2 peptide.
To quantitate the functional activity of the COX isoenzymes, PGE2 production wasmeasured. The concentration of PGE2 produced by homogenates of normal iris tis-sue varied from 1.5-4 ng/ml assay mixture/hr and of iris treated with LPS from 10-20 ng/ml of assay mixture/hr. The synthesis of PGE2, produced under these cir-cumstances was inhibited differentially by S(+) flurbiprofen as shown in figure 2.S(+) flurbiprofen inhibits the PGE2 production of untreated iris tissue at an IC50 of8 x 10-10 M, whereas the IC50 after LPS stimulation was found to be 3 x 10-6M.
The phospholipase activity in iris homogenate (43 ± 5 µmol/min/ml) was not sig-nificantly influenced in the presence of S(+) flurbiprofen in a final concentration of10-5M.
88
Chapter 6

Figure 2. Concentration-response curves for inhibition of the COX-1 (�) activity inhomogenate of untreated human iris and of COX-2 (�) activity in homogenate of humaniris treated with LPS. Concentrations of S(+) flurbiprofen are final concentrations in theassay mixture. Each point represents the average ± SEM of four to six determinations fromdifferent pools of tissue homogenates.
DISCUSSION
The iris is the major site for prostaglandin (PG) formation in the eye. These PGs areproduced after experimental manipulations but also following induction of uveitis.Whereas PG synthesis in the iris/ciliary body has been ascribed to COX-1 activity,induction of COX-2 may be an explanation for increased prostaglandin formation bythe inflamed human iris such as in uveitis. In this study, not only were the involvedCOX-isoforms detected at the protein level, but also their functional activity wascharacterized using the NSAID S(+) flurbiprofen. With homogenates of untreatedtissue, positive spotblot-staining for COX-1 and substantial production of PGE2
could be demonstrated. Next to the usual positive staining for COX-1-ir additionalpositive staining for COX-2-ir was achieved after stimulation with LPS, concomitantwith greater production of PGE2.
In porcine ciliary body it has been demonstrated that cytochrome P450 dependentω/ω-1 hydroxylase activity can inactivate accumulated prostaglandins (28). In poly-morphonuclear leukocytes hydrolysis of triacylglycerols by triacylglycerol hydrolasemay also provide arachidonate as a source of fatty acid for COX. In our assay weobviously measured the net result of production of PGE2 by COX-1 or COX-2 fromendogenous arachidonate mobilized by activation of specific hydrolases.
89
Human iris

The selectivity of S(+) flurbiprofen for inhibition of COX-1 with a COX-2/COX-1 ratioof 3,600 is greater than the value of 32 found using human blood as assay system(29). This discrepancy between COX-2 inhibition for S(+) flurbiprofen in ocular tis-sue and blood was unexpected and not readily explained. Carabaza et al. (30)found a similar great ratio for S(+) flurbiprofen, using ram seminal vesicles assource for COX-1, reporting an IC50 of 2X10-9 M, as compared to 0.47X10-6 M onCOX-2, using the whole blood assay. Considering the complexity of the dynamicsinvolved in inhibition of COX-1 and COX-2 by flurbiprofen, it is conceivable thatintra-species differences are possibly due to differences in tissue, protein bindingand assay protocols (31).
Inhibition of PG production for some NSAIDs, like indomethacin and sulindac,may also be caused by inhibition of phospholipase A2 (32,33), but not of triacygly-cerolhydrolases (32). However, flurbiprofen has been shown not to inhibit humansynovial or rat peritoneal phospholipase A2 (33) and our results show the same forthe enzyme in the iris. Therefore the observed inhibition of PGE2 production in thisstudy might be ascribed solely to inhibitory effects on COX-1 and COX-2 and notto inhibition of phospholipase A2.
The clinical use of flurbiprofen in the inhibition of intraoperative miosis, of disrup-tion of the blood-aqueous barrier and of cystoid macular edema is based on inhibi-tion of the "housekeeping" enzyme, COX-1, present in the iris/ciliary body.Flurbiprofen's activity directed against inflammatory signs generated by inducedCOX-2, present hours after surgery or laser treatment is minor in degree (15,27).The relative contribution of other eicosanoid or non-eicosanoid pathways inmechanical blood-aqueous barrier disruption has been estimated from experimentsusing flurbiprofen to be less than 5% (34).
We used the S(+) enantiomer of flurbiprofen, because it is the most potent isomer,like in many other enantiomeric pairs of NSAIDs. In experiments using bovine iris/cil-iary body the R(-) enantiomer of flurbiprofen showed 1% of the inhibitory activity of theS(+) enantiomer (24) and in the human whole blood assay 0.3 and 2% on COX-1 andCOX-2 respectively (29). With respect to the demands for ballastfree stereo specificdrugs providing a reduction in metabolic load to the patient, S(+) flurbiprofen in theracemic mixture can be designated as the active agent and R(-) flurbiprofen asunnecessary ballast. Outside the field of ophthalmology, a report is available on theclinical use of S(+) flurbiprofen in dentistry (35). The NSAID S(+) ibuprofen provedpharmacologically active in the prevention of leakage of protein over the blood aque-ous barrier in rabbits (36). There is no indication (37) of a pro-drug property whichcould be based on metabolic inversion of the less active R(-) isomer into the moreactive S(+) isomer, as has been observed in other species than man (38).The S(+)flurbiprofen has been formulated into a stereoselective ballast-free eyedrop solutionin a concentration of 0.015% (free acid form), which is approximately half the usual
90
Chapter 6

91
concentration of commercial available specialties containing racemic flurbiprofen inthe sodium salt form (39) .
After systemic administration, R(-) flurbiprofen shows about one third of theantinociceptive activity of the S(+) form, indicating a central site of action inde-pendent of prostaglandin synthesis inhibition and in this respect the use of racemicflurbiprofen may be reserved for analgesic applications (40). In eye conditionsresulting from prostaglandin production caused by induced COX-2, such as chron-ic uveitis, the concentration of S(+) flurbiprofen as selective COX-1 inhibitor in theregular eyedrops may be too low to give sufficient inhibition. The concentration offlurbiprofen in human aqueous humor has been measured as 60 ng/ml two hoursafter instillation of a single drop (41), which corresponds to 0.25 µM, being muchlower than the IC50 of 3 µM for COX-2 as measured in our study.
The use of selective topical COX-2 inhibitors, such as meloxicam for the treat-ment of all forms of ocular inflammation, as advocated by Masferrer and Kulkarni(42) seems not always justified. Only the management of inflammation caused byinduced COX-2 activity (15,27) may be reserved for selective COX-2 inhibitors.Meloxicam appears to be suitable for administration as eyedrops (43). The IC50 ofabout 0.5 µM (26,29) for COX-2 as measured in human blood might suffice forintraocular inhibition, depending on the concentration of meloxicam reached in theaqueous humor.
Acknowledgements: The authors thank the foundation BIS (Leiden, theNetherlands) and the Cornea Bank (Amsterdam, the Netherlands) for providinghuman iris tissue.
REFERENCES
1. Matsuo, T., and Cynader, M.S. The EP2 receptor is the predominant prostanoidreceptor in thehuman ciliary muscle. Br. J. Ophthalmol. 77:110-114, 1993.
2. Flower, R.J., and Blackwell, G.J. The importance of phospholipase-A2 in prostaglandin biosyn-thesis. Biochem. Pharmacol. 25:285-291, 1976.
3. Elsbach, P., and Farrow, S. Cellular triglyceride as a source of fatty acid for lecithin synthesis dur-ing phagocytosis. Biochim. Biophys. Acta. 176:438-441, 1969.
4. Hemler, M., Lands, W.E.M., and Smith, W.L. Purification of cyclooxygenase that formsprostaglandins: Demonstration of two forms of iron in the holoenzyme. J. Biol. Chem. 251:5575-5579, 1976
5. Simmons, D.L., Xie, W., Chipman, J.G., and Evett, G.E. Multiple cyclooxygenases: Cloning of amitogen inducible form. In Prostaglandins, Leukotrienes, Lipoxins, and PAF. Bailey, J.M. ed.,Plenum Press, New York, 1991, pp 67-78.
6. Asakura, T., Sano, N., and Stichi, H. Prostaglandin synthesis and accumulation by porcine ciliaryepithelium. J. Ocul. Pharmacol. 8:333-341, 1992.
7. Wallace, J. L., Bak, A., McKnight, W., Asfaha, S., Sharkey, K. A., and MacNaughton, W. K.Cyclooxygenase 1 contributes to inflammatory responses in rats and mice: Implications for gas-
Human iris

trointestinal toxicity. Gastroenterology 115:101-109, 1998.8. Xie, W., Chipman, J.G., Robertson, D.L., Erikson, R.L., and Simmons, D.L. Expression of mito-
gen responsive gene encoding prostaglandin synthase is regulated by mRNA splicing. Proc.Natl. Acad. Sci. USA. 88:2692-2696, 1991.
9. Yamagata, K., Andreasson, K., Kaufmann, W.E., Barnes, C.A., and Worley, P.F. Expression of amitogen-inducible cyclooxygenase in brain neurons: regulation by synaptic activity and gluco-corticoids. Neuron 11:371 - 386, 1993.
10. Akarasereenont, P., Bakhle, Y.S., Thiemermann, C., and Vane, J.R. Cytokine-mediated inductionof cyclooxygenase-2 by activation of tyrosine kinase in bovine endothelial cells stimulated bybacterial lipopolysaccharide. Br. J. Pharmacol. 115:401-408, 1995.
11. Arias-Negrete, S., Keller, K., and Chadee, K. Proinflammatory cytokines regulate cyclooxyge-nase-2 mRNA expression in human macrophages. Biochim. Biophys. Res. Commun. 208:582-589, 1995.
12. Bazan, N.G., Fletcher, B.S., Herschmann, H.R., and Mukherjee, P.K. Platelet-activating factorand retinoic acid synergistically activate the inducible prostaglandin synthase gene. Proc. Natl.Acad. Sci. USA 91:5252-5256, 1994.
13. Jumblatt, M.M., and Willer, S.S. Corneal endothelial repair. Regulation of prostaglandin E2 syn-thesis. Invest. Ophthalmol. Vis. Sci. 37:1294-1301, 1996.
14. Bazan, H.E., Tao, Y., DeCoster, M.A., and Bazan, N.G. Platelet-activating factor inducescyclooxygenase-2 gene expression in corneal epithelium. Requirement of calcium in the signaltransduction pathway. Invest. Ophthalmol. Vis. Sci. 38:2492-2501, 1997.
15. Chang, M.S., Tsai, J.C., Yang, R., DuBois, R.N., Breyer, M.D., and O'Day, D.M. Induction of rab-bit cyclooxygenase 2 in the anterior uvea following glaucoma filtration surgery. Curr.Eye. Res.16:1147-1151, 1997.
16. Miller, J.D., Eakins, K.E., and Atwal, M. The release of PGE2-like activity into aqueous humorafter paracentesis and its prevention by aspirin. Invest. Opthalmol. Vis. Sci. 12:939-942, 1973.
17. Cole, D.F., and Unger, W.G. Prostaglandins as mediators of the responses of the eye to trauma.Exp. Eye. Res. 17:357-368, 1973.
18. Paterson, C.A., and Pfister, R.R. Prostaglandin-like activity in the aqueous humor following alka-li burns. Invest. Ophthalmol. Vis. Sci. 14:177-183, 1975.
19. Bhattacherjee, P., and Eakins, K.E. Inhibition of the ocular effects of sodium arachidonate by anti-inflammatory compounds. Prostaglandins 9:175-182, 1975.
20. Unger, W.G., Perkins, E.S., and Bass, M.S. The response of the rabbit eye to laser irradiation ofthe iris. Exp. Eye Res. 19:367-377, 1974.
21. Kulkarni, P.S., Fleisher, L., and Srinivasan, B.D. The synthesis of cyclooxygenase products inocular tissues of various species. Curr. Eye Res. 3:447-452, 1984.
22. Eakins, E.K., Whitelocke, R.A.F., Perkins, E.S., Bennet, A. and Unger, W.G. Release of aprostaglandin in ocular inflammation. Nature 239:248-249, 1972.
23. Bhattacherjee, P. Release of prostaglandin-like substances by Shigella endotoxin and its inhibi-tion by nonsteroidal anti-inflammatory compounds. Br. J. Pharmacol. 54:489-494, 1975.
24. Van Sorge, A.A., Van Delft, J.L., Bodelier, V.M.W., Wijnen, P.H., and Van Haeringen, N.J.Specificity of flurbiprofen and enantiomers for inhibition of prostaglandin synthesis in bovineiris/ciliary body. Prostag. Other Lipid Mediat. 55:169-177, 1998.
25. Kass, M.A., Holmberg, N.J., and Smith, M.E. Prostaglandin and thromboxane synthesis bymicrosomes of inflamed rabbit ciliary body-iris. Invest. Ophthalmol. Vis. Sci. 20:442-449, 1981.
26. Patrignani, P., Panara ,M.R., Sciulli, M.G., Santini, G., Renda, G., and Patrono, C. Differential inhi-bition of human prostaglandin endoperoxidase synthase-1 and -2 by nonsteroidal anti-inflamma-tory drugs. J. Physiol. Pharmacol. 48:623-631, 1997.
92
Chapter 6

27. Ogawa, T., Watanabe, N., and Waki, M. Role of cyclooxygenase isozyme in inflammation andpain in rabbit eye. Exp. Eye Res. 67 (Suppl. 1);S 242, 1998.
28. Asakura, T., and Shichi, H. Cytochrome P450-mediated prostaglandin w/w-1 hydroxylase activ-ities in porcine ciliary epithelial cells. Exp. Eye Res. 55:377-384, 1992.
29. Van Haeringen, N.J., Van Sorge, A.A., Van Delft, J.L., and Carballosa Coré-Bodelier, V.M.W.Flurbiprofen and enantiomers in opthalmic solution tested as inhibitors of prostanoid synthesis inhuman blood. J. Ocular Pharmacol. Therap 16:345-352, 2000.
30. Carabaza, A., Cabré, F., Rotllan, E., Gómez, M., Gutiérrez, M., García, L., and Mauleón, D.Stereoselective inhibition of inducible cyclooxygenase by chiral nonsteroidal antiinflammatorydrugs. J. Clin. Pharmacol. 36:505-512, 1996.
31. Callan, O.H., So, O-Y., and Swinney, D.C. The kinetic factors that determine the affinity andselectivity for slow binding inhibition of human prostaglandin H synthase 1 and 2 by indomethacinand flurbiprofen. J. Biol. Chem. 271:3548-3554, 1996.
32. Kaplan-Harris, L., and Elsbach, P. The anti-inflammatory activity of analogs of indomethacin cor-relates with their inhibitory effects on phospholipase A2 of rabbit polymorphonuclear leukocytes.Biochim. Biophys. Acta 618:318-326, 1980.
33. Lobo, I.B., and Hoult, J.R. Groups I, II and III extracellular phospholipases A2: Selective inhibitionof group II enzymes by indomethacin but not other NSAIDs. Agents Actions 41:111-113, 1994.
34. van Haeringen, N.J., Oosterhuis, J.A., van Delft, J.L., Glasius, E., and Noach, E.L. A compari-son of the effects of non-steroidal compounds on the disruption of the blood-aquoeus barrier.Exp. Eye Res. 35:271-277, 1982.
35. Roszkowski, M.T., Swift, J.Q., and Hargreaves, K.M. Effect of NSAID administration on tissuelevels of immunoreactive prostaglandin E2, Leukotriene B4, and (S) flurbiprofen following exy-taction of impacted third molars. Pain. 73:339-345, 1997.
36. Tjebbes, G.W.A., van Delft, J.L., Barthen, E.R., and van Haeringen, N.J. d-ibuprofen in ocularinflammation induced by paracentesis of the rabbit eye. Prostaglandins 40:29-33, 1990.
37. Geisslinger, G., Menzel-Soglowek, S., Schuster, O., and Brune, K. Stereoselective high perform-ance liquid chromatographic determination of flurbiprofen in plasma. J. Chrom. 573:163-167, 1992.
38. Menzel-Soglowek, S., Geisslinger, G., Beck, W.S., and Brune, K. Variability of inversion of R(-)flurbiprofen in different species. J. Pharm Sci. 81:888-891, 1992.
39. Van Sorge, A.A., Wijnen, P.H., Van Delft, J.L., Carballosa Coré-Bodelier, V.M.W., and VanHaeringen, N.J. Flurbiprofen, S(+), eyedrops; Formulation, enantiomeric assay, shelflife andpharmacology. Pharm. World. Sci. 21:91-95, 1999.
40. Geisslinger, G., Ferreira, S.H., Menzel, S., Schlott, D., and Brune, K. Antinociceptive actions ofR(-) flurbiprofen - a non-cyclooxygenase inhibiting 2-arylpropionic acid - in rats. Life Sci. 54:173-177, 1994.
41. Ellis, P.P., Pfoff, D.S., Bloedow, D.C., and Riegel, M. Intraocular diclofenac and flurbiprofen con-centrations in human aqueous humor following topical application. J. Ocul. Pharmacol. 10:677-682, 1994.
42. Masferrer, J.L., and Kulkarni, P.S. Cyclooxygenase-2 inhibitors: a new approach to the therapyof ocular inflammation. Surv. Ophthalmol. 41(Suppl.20):S35-S40, 1997.
43. Stei, P., Kruss, B., Wiegleb, J., and Trach, V. Local tissue tolerability of meloxicam, a new NSAID:Indications for parenteral, dermal and mucosal administration. Br. J. Rheumatol. 35(Suppl. 1):44-50, 1996.
93
Human iris

94

CHAPTER 799mTc-DIFLUNISAL AND THE HUMAN IRIS
TOPICAL APPLICATION REVEALS LOCALISATION
Adriaan A. van Sorge, Robert Jan van Etten, Coen J. Rehmann,Ton J. Rijnders, and Nicolaas J. van Haeringen
J Ocular Pharmacol 2002;18:185-95

ABSTRACT
Following the instillation of a drug into the eye, drainage mechanisms will com-mence at once. In this report, an attempt was made to assess the dynamics of aninstilled nonsteroidal anti-inflammatory drug (NSAID), diflunisal, labeled with 1 MBq99mTc followed by twenty minutes of scintigraphy. The results obtained with thislabeled drug were compared with instillation of the same volume and activity of99mTcO4
-. Although the pertechnetate anion is an excellent and innocuous indicatorfor detecting the external lacrimal drainage system of the eye, it cannot visualizethe internal structures. A clear scintigraphic difference was noted between labeleddiflunisal and the pertechnetate anion. Scintigraphic activity surrounding the pupilof the eye provides evidence of visualization of the iris/ciliary body. This seems rea-sonable as the cyclooxygenase enzyme is located in this structure and NSAIDsexert their mechanism of action via this complex. With this technology, visualizationof some internal structures of the eye may be facilitated.
INTRODUCTION
In 1972, Rossomondo (1) published the first report on the use of sodium pertech-netate 99mTc for evaluating the lacrimal drainage system. The dose administeredwas 1.85MBq to 3.7 MBq (50 to 100 µCi) with a scintigraphic procedure of 25 min-utes duration and excellent visualization of the external lacrimal system.Applications in other medical fields were suggested, the main point being that theanatomy of the structures involved were not altered, and important physiologicalparameters could possibly be solved in an elegant, non-irritating manner. Before,radiopaque dyes had been utilized for imaging the lacrimal drainage system (dacry-ocystogram) which is uncomfortable, time consuming and deforming on anatomicalstructures. Blanksma et al. have communicated a similar experiment with use of99mTcO4
- (2).Gamma scintigraphy can be of benefit in providing data (3): · on rate and extent of drug absorption· for "proof of concept"· for explaining drug and/or formulation effects· by use of sequential scintigraphic images ("time-lapse photography")· that in vivo performance is in agreement with the intended application· concerning delivery of the right amount of drug in the right place at the right time· that may overcome the poor predictability of in vitro studiesEssential to the design of a radiopharmaceutical agent is the chemistry of thedesired radiometaled chelate. The introduction of 99mTc as a labelling agent bychelation has changed the practice of nuclear medicine. The practice of chelation
Chapter 7
96

in medicine is not new (4). In 1951, it was suggested that "salicylates" are capableof chelation and might, therefore, possess therapeutic properties. Aspirin aluminumis a known drug entity and incorporated in the Japanese Pharmacopoeia XIII. Avery known reaction in the field of biochemistry and pharmacy is the appearance ofa purple color in a weakly acid solution in the presence of a salicylate ion when fer-ric salts are added (5). In this manner, a quantitative estimate in a biological sam-ple can be given in a relatively short time. Chelating ability of the ferric and ferrouscation with salicylic acid has been reported in favor of the ferric cation in a ratio of400 to 1 (6).
Spectroscopic studies have been performed on salicylic acid, salicylamide andacetylsalicylic acid as to which spatial configuration favors these drugs most.Calculations have made it plausible that the ß-form is the preferred configuration.In this orientation, the carboxylic hydroxyl group is directed towards the enolichydroxyl group (7). Further research (8) has deepened the mechanism of com-plexation of 99mTc with "aspirin-like" molecules.
Diflunisal (5-(2',4'-difluorophenyl)salicylic acid) inhibits the COX-1 enzyme in thesame degree as sodium salicylate and approximately 20% less than flurbiprofenwith the same level (80%) of COX-2 inhibition (9,10). The authors used this welldefined pharmacological assay to assess the potential of S(+) flurbiprofen as acyclooxygenase (COX) inhibitor formulated as an eyedrop (11). Acetylsalicylic acidshowed the same degree of inhibition for COX-1 and COX-2 as flurbiprofen. Thedisadvantage of using acetylsalicylic acid, however, is its instability in solution (12).
In our study, we chose the drug, diflunisal, as a representative for the mechanismof complexation as described above and sharing pharmacologic resemblance withthe drug, flurbiprofen, as an NSAID in being fluorinated and possessing a biphenylring.
MATERIALS and METHODS
Gamma camera and computer systemGamma camera: Sopha DS7 single head, round fieldEnergy: 99mTc, 140 keVWindow: 20%Collimator: pinhole-collimator 5 mm ApertureMatrix: 128x128Session duration: 20 minutes; dynamic images taken every 10 seconds (10 secondduration)Data processing system: SMV NXT computer
99mTc-Diflunisal
97

Drugs and Chemicals99mTcO4
- activity (sodium pertechnetate eluate) was obtained from a commerciallyavailable 99Mo/99mTc generator (Mallinckrodt). Diflunisal (product number: D-3281;lotnr:95H0528) was purchased from Sigma (St Louis, Mo, USA), Stannous Tartrate500 microgram (BN040701; lyophilized) was purchased from IV DIRECT LTD(London, UK). The ophthalmic solution was dispensed by a Hamilton microlitersyringe (50 microliter; art.nr.:3038015). Thin-layer chromatography material con-sisted of Whatman paper No17 (Tamson no 194K01) and ITLC-SG (Gelman no61886); scanning was performed with a Raytest chromatogram scanner equippedwith miniGITA software.
Formulation of Diflunisal EyedropsPreparation of the diflunisal eyedrops proceeds by addition of 50 mg diflunisal to apart of the available 0.3 M sodium chloride solution. By addition of approximately1 ml of 1M sodium hydroxide, a clear solution is obtained. The pH was adjustedbetween 7.0 -7.5 before adding up to 100.0 ml. The final solution was filteredthrough a 0.22 micron filter. All diflunisal preparations were stored in glass contai-ners. No preservative was added.
Analytical AssayBy use of HPLC combined with Diode Array Detection as described by Uges et al.(13) quality of the ophthalmic solution was assayed. In short, a reversed phase RP-18 endcapped 5µm. 125x4mm column is used (Merck Darmstadt/Amsterdam,Catalog number: 21568); mobile phase: acetonitrile 470 ml(Lichrosolve) phosphor-ic acid/triëthylamine 530 ml buffer pH 3.3 is used.Content was analysed by spectrophotometric assay (Varian CARY 3) at 255 nm.
Patient SettingIn this representative study, investigations were carried out in one subject (vS,1944). Comfortably seated upright in a chair, a drop of ophthalmic solution (50microliter) was placed into the conjunctival sac at the lateral canthus. The head waspositioned with the inner canthus less than 5 mm from the pinhole collimator.Sufficient resolution could be obtained for the eye, canaliculi and lacrimal sac.Scintigraphic images were made over a 20-minute period. In two separate sessions(spaced by 1 month), the ophthalmic 99mTc-diflunisal solution and a pertechnetatesodium solution were investigated. In both instances, the left eye was used. Freepassage of the lacrimonasal duct had been assured beforehand by the test of Anel.Application of the eyedrop was experienced as a transient prickling sensation.
Chapter 7
98

Preparation of 99mTc-Diflunisal and Pertechnetate Sodium Eyedrops
99mTc-Diflunisal EyedropsSodium chloride 0,9% (low in oxygen content) is added to the vial containing 500micrograms stannous tartrate. The contents of the vial are swirled cautiously. Next,the calculated amount of sodium pertechnetate activity is added (1ml=60 MBq) fol-lowed by the addition of 1ml of 0.05% diflunisal ophthalmic solution. The total con-tents (3 ml) is boiled for 10 minutes followed by radiochemical quality control of99mTc-diflunisal. Labeling is set at 75 - 80% or more.
Sodium Pertechnetate EyedropsPreparation of the sodium pertechnetate eyedrop was analogues to the 99mTc-diflu-nisal preparation differing in substitution by sodium chloride 0.9%. of the diflunisalsolution. This solution contained 60 MBq in 3 ml solution (1 MBq in 50 microliters).Radiochemical quality control of pertechnetate was performed with purity set at95% or more.
Analytical quality control for radiochemical purityRadiochemical purity of a radiopharmaceutical is defined as the proportion of totalradioactivity in the desired compound.Analysis is performed by the two-strip mini-chromatography method as describedin (14). In figure 1, the basic outline of the procedure is presented.
Figure 1. Two-strip Mini-chromatography System. On the left the Whatman no 17 andMethylethylketone solvent is used for pertechnetate separation; on the right, ITLC-SG andPBS pH 7.4 or sodium chloride 0.9% as solvent is used for quantification of bound 99mTc.Numbers 1,2,3 and 4 denote the following: 1: bound 99mTc and hydrolyzed reduced technetium;2: free TcO4-; 3: hydrolyzed reduced technetium; 4: bound 99mTc and free TcO4
-, respectively.
99mTc-Diflunisal
99

A spot (10 microliter) of solution is deposited on Whatman paper No 17 and devel-oped in methylethylketone. Pure pertechnetate will show up in the solvent front.
Likewise, a spot of the same solution is deposited on the ITLC-SG strip and devel-oped in phosphate buffered salt (PBS; pH 7.4) or 0.9% sodium chloride. The chro-matography strip is developed in the chosen solvent and analyzed by a chro-matography scanner recording radioactivity along the length of the strip. The per-centage of radiochemical impurity is calculated from the ratio of radioactivity asso-ciated with the impurity compared with the radioactivity of the total strip.
RESULTS
ANALYTICAL ASSAY
HPLC and UV SpectrophotometryQuality control by HPLC of the ophthalmic diflunisal 0.05% solution displayed nodegradation peaks (figure 2) with a content of 99.6% diflunisal measured by quan-titative spectrophotometric analysis.
Figure 2. HPLC Chromatogram of a 0.05% Ophthalmic Solution of Diflunisal.
Radiopharmaceutical Quality Control
In figures 3, 4 and 5, examples of radiopharmaceutical quality control by thin-layerchromatography are depicted.
Chapter 7
100

Figure 3. Thin-layer Chromatography of 99mTc Diflunisal on Whatman No 17 in MEK.
Figure 4. Thin-layer Chromatography of 99mTc Diflunisal on ITLC-SG in PBS pH 7.4.For legend, see Figure 1.
Figure 5. Thin-layer Chromatography of Pertechnetate on Whatman No 17 in MEK.For legend, see Figure 1.
99mTc-Diflunisal
101

Labeling efficiency for diflunisal, measured by the thin-layer chromatography sys-tem as described, resulted in 77% when sodium chloride 0,9% was used and 83%when PBS pH7.4 was the solvent. Purity of pertechnetate, used in the ophthalmicsolution, was 96%.
Scintigraphic AssayFigure 6 demonstrates the activity seen in frame 16 and the graphic illustration ofcounts versus time (whole session). Frame 16 signals the end of the eyes-closedsequence. Some activity is still left at the point of instillation of the eye drop. At theend of the sequence, all activity seems present in the lacrimonasal ductus.
Figure 6. Scintigraphic Image of the Eye Surface and the Lacrimal Sac 160 seconds afterApplication of 99mTc Diflunisal (frame 16). Graph represents counts versus time for wholesession.
When one analyzes frame 117, residual activity (figure 7) distinct from baselineactivity is present in the area of pupil and iris. This is displayed in the accompany-ing graph.
Comparing the frames, taken at the same time sequence, obtained with 99mTc-diflu-nisal and pertechnetate, a difference in scintigraphic exposure can be seen (figure 8).
Chapter 7
102

Figure 7. Scintigraphic Image of the Area of the Iris and the Lacrimal Sac 1170 secondsafter Application of 99mTc-Diflunisal (frame 117). Graph represents counts versus time forwhole session.
Figure 8. Difference in Scintigraphic Exposure between Pertechnetate (left) and 99mTc-Diflunisal
Calculation of the activity as counts per pixel for the area designated as pupil, irisand conjunctiva (excluding the lacrimonasal ductus), leads to a graph (figure 9) dis-tinguishing a higher level of activity in the iris than the pupil. Correction for naturaldecay of 99mTc has been taken into account.
99mTc-Diflunisal
103

Figure 9. Display of Counts Per Pixel for 99mTc-Diflunisal in the Area of Pupil, Iris andConjunctiva
DISCUSSION
In this study, an eye drop volume in every day practice of 50 microliters is used toillustrate the fate of the labeled NSAID diflunisal. Under the physiological conditionsdescribed, a dose of approximately 1 MBq of labeled 99mTc-diflunisal or pertechne-tate generates a radiation absorbed dose to the epithelium of the lens of maximal-ly 4 x 10-11 Gy per Bq or 0.04 mGy (15). This is far below the dose known to pro-duce radiation cataract (16). Scintigraphic evidence in the nasal cavity can be seenwithin one minute. As reported in the literature, closing of the eye will slow theprocess of drainage. After opening the eye, the tear flow will proceed at a normalphysiological value of approximately 1 microliter per minute. After instillation of aneye drop, the extra volume will be rapidly eliminated in the first two minutes. Thiswill be followed by a bi-exponential decay (initial phase of 2 - 5 minutes; basalphase from 7 minutes onward) where the tear flow will be 1.4 and approximately 1microliter per minute, respectively. Any variation from these principles could indi-cate a disturbance in the delicate balance of the lacrimal system (17,18,19).
In figure 9, a display of counts per pixel is given for the structures of pupil, iris andconjunctiva. The amount of labeled diflunisal that has entered the eye and is visi-ble on the iris in frame 117 can be estimated by calculating the amount instilled,8.35 microgram in 50 microliters, equivalent to 2900 counts. The pupil is repre-sented by 0.15 counts per pixel (total pixel count: 79) and the iris by 0.30 (total pixelcount: 589). The estimated amount that has entered the eye through the corneaand is visibly attached to the iris will have to be corrected for the amount per pixel
Chapter 7
104
99mTc-Diflunisal scintigraphyin selected eye structures
0,00
0,50
1,00
1,50
2,00
2,50
3,00
0 200 400 600 800 1000 1200
time (seconds)
coun
ts p
er p
ixel
pupil
iris
conjunctiva

that is attached to the cornea in the iris area. The latter is derived from the amountper pixel in the pupil area. The estimated amount on the iris, thus, is 0.30 - 0.15=0.15 count per pixel. The amount of permeated labeled diflunisal is (0.15*589/2900)* 8.35µg = 0.254 microgram. This corresponds to 3% of the total amount of instilleddiflunisal.
Tissue concentration-time profiles for the iris-ciliary body closely resembles thosefor stroma-endothelium and aqueous humor. Peak concentration time for instilledpilocarpine was reached at 20 minutes (20). The initial total volume of distributionafter application of an eye drop is reported to be 350 microliters. This encompass-es the aqueous humor volume and the cornea (21). In this case 254 nanograms willbe in 350 a microliter solution. This equates to 3x10-6M for diflunisal. For flurbipro-fen, it was found that the COX-1 enzyme in the human iris is inhibited 100% by a10-7M flurbiprofen solution (11). This will also suffice for inhibition of the COX-1enzyme by diflunisal (9).
CONCLUSION
In vitro experiments (22,23), using a corneal perfusion device with simulated phys-iologic tear turnover as in vivo, or a three-dimensional tissue constructed to inves-tigate drug penetration across the cornea, have been published but lack the real-time complex interplay in dynamics of tear fluid, tear turnover, aqueous humor andmechanical stress of the eyelids. This report provides scintigraphic evidence of theiris/ciliary body with use of a 99mTc-labelled NSAID, diflunisal.
Acknowledgements: The authors express their thanks to Irma Ruiken and HermanJanssen for their conscientious preparation and quality control of the radiopharma-ceuticals. The staff of the Nuclear medicine department of Rijnstate is thanked fortheir cooperation in the scintigraphy sessions.
REFERENCES
1. Rossomondo, R.M., Carlton, W.H., Trueblood, J.H., and Thomas, R.P. A new method of evaluat-ing lacrimal drainage. Arch. Ophthal. 88:523-525, 1972.
2. Blanksma, L.J., Schweitzer, N.M.J., Beekhuis, H., and Piers, D.A. Testing of lacrimal drainagewith the aid of a gamma-ray emitting radiopharmaceutical (99mTcO4-). Doc. Ophthalmol. 42:381-384, 1977.
3. Wilding, I., and Newman, S. Saving time in the drug development process using gamma scintig-raphy. Pharm. Techno. Eur. February:26-31, 1998.
4. Schubert, J. Chelation in medicine. Sci. Am. 214:40-50, 1966.5. Trinder, P. Rapid determination of salicylate in biological fluids. Biochem. J. 57:301-303, 1954.6. Perrin, D.D. Stability of metal complexes with salicylic acid and related substances. Nature
182:741-742, 1958.
99mTc-Diflunisal
105

7. El-Shahawy, A.S. Spectroscopic structural studies of salicylic acid, salicylamide and aspirin.Spectrochim. Acta. 44A:903-907, 1988.
8. El-Shahawy, A.S., Mahfouz, R.Z., Aly, A.A.M., and El-Zohry, M. Technetium-aspirin moleculecomplexes. J. Chem. Tech. Biotechnol. 56:227-231, 1993.
9. Warner, T.D., Giuliano, F., Vojnovic, I., Bukasa, A., Mitchell, J.A., and Vane, J.R. Nonsteroid drugselectivities for cyclooxygenase-1 rather than cyclooxygenase-2 are associated with human gas-trointestinal toxicity: a full in vitro analysis. Proc. Natl. Acad. Sci. USA. 96:7563-7568, 1999.
10. Patrignani, P., Panara, M.R., Sciulli, M.G., Santini, G., Renda, G., and Patrono, C. Differential inhi-bition of human prostaglandin endoperoxide synthase-1 and -2 by nonsteroidal anti-inflammato-ry drugs. J. Physiol. Pharmacol. 48:623-631, 1997.
11. Van Haeringen, N.J., Van Sorge, A.A., and Carballosa Coré-Bodelier, V.M.W. Constitutivecyclooxygenase-1 and induced cyclooxygenase-2 in isolated human iris inhibited by S(+) flur-biprofen. J. Ocul. Pharmacol. Ther. 16:353-361, 2000.
12. Garrett, E.R. The kinetics of solvolysis of acyl esters of salicylic acid. J. Am. Chem. Soc. 79:3401-3408, 1957.
13. Uges, D.R.A., and Conemans, J.M.H. Antidepressants and antipsychotics. In Forensic Science.Handbook of Analytical Separations, Vol. 2, Bogusz, M.J., ed., 229-257 (with special referenceto pp 247-248, 2000). ISBN 0-444-82998-9.
14. Robbins, P.J. Chromatography of Technetium-99m radiopharmaceuticals: a practical guide. TheSociety of Nuclear Medicine, Inc., New York, USA. ISBN: 0-932004-18-0.
15. Robertson, J.S., Brown, M.L., and Colvard, D.M. Radiation absorbed dose to the lens indacryoscintigraphy with 99mTcO4-. Radiology. 133:747-750, 1979.
16. Wilde, G., and Sjöstrand, J. A clinical study of radiation cataract formation in adult life following irra-diation of the lens in early childhood. Br. J. Ophthalmol. 81:261-266, 1997.
17. Sørensen, T., and Taagehøj Jensen, F. Tear flow in normal human eyes. Determination by meansof radioisotope and gammacamera. Acta Ophthalmol. 57:564-581, 1979.
18. Sørensen, T., and Taagehøj Jensen ,F. Methodological aspects of tear flow determination bymeans of a radioactive tracer. Acta Ophthalmol. 55:726-738, 1977.
19. Sørensen, T., and Taagehøj Jensen, F. Lacrimal pathology evaluated by dynamic lacrimal scintig-raphy. Acta Ophthalmol. 58:597-607, 1980.
20. Sieg, J.E., and Robinson, J.R. Mechanistic studies on transcorneal permeation of pilocarpine. J.Pharm. Sci. 65:1816-1822, 1976.
21. Reim, M. Augenheilkunde. Ferdinand Enke Verlag, Stuttgart 1985. ISBN 3 432 94 5019.22. Richman, J.B., Tang-Liu, D,D-S. A corneal perfusion device for estimating ocular bioavailability in
vitro. J. Pharm. Sci. 79:153-157, 1990.23. Tegtmeyer, S., Papantoniou, I., and Müller-Goymann, C.C. Reconstruction of an in vitro cornea
and its use for drug permeation studies from different formulations containing pilocarpinehydrochloride. Eur. J. Pharm. Biopharm. 51:119-125, 2001.
Chapter 7
106

CHAPTER 8
S(+) FLURBIPROFEN AND R(-) FLURBIPROFEN99mTc-LABELING REVEALS DIFFERENCE
IN STEREOCHEMISTRY
Adriaan A. van Sorge, Irma W.M. Ruiken, Herman W.M. Janssen,and Nicolaas J. van Haeringen
Accepted pending suitable revision

ABSTRACT
The separate enantiomers of flurbiprofen, RS-(±)-2-(2-fluoro-4-biphenylyl))-propi-onic acid, have been investigated for their potential in chelating with 99mTc providedby a 99Mo/99mTc generator. The used labeling procedure of a 0.05% flurbiprofen solu-tion of the two enantiomers resulted in 1 MBq of activity in 50 microliter solution.Radiochemical quality control of the labeled compounds revealed that R(-) flur-biprofen has better chelating ability. This may indicate less steric hindrance causedby the presence of the fluorine atom in the R(-) flurbiprofen molecule.
INTRODUCTION
Flurbiprofen, belongs to the frequently prescribed and used drugs called nons-teroidal anti-inflammatory drugs (NSAIDs), often being chiral in nature (1). In the lit-erature it has been reported that the anti-inflammatory and analgesic propertiesmainly reside in the dextrorotary component (2) of these drugs. This pharmacolog-ical effect is attained through inhibition of prostanoid synthesis, by the enzymecyclooxygenase (COX) (3). As a consequence, active prostanoids cannot beformed thus giving reduction in inflammation and relief of pain. In previous studieswe have established not only a marked stereoselectivity of flurbiprofen enantiomersfor inhibition of COX-activity, but also preferential affinity for the constitutive COX-1isoenzyme compared to inducible COX-2 (4,5).
99mTc-labeling of the achiral NSAID, diflunisal, (2',4'-difluor-4-hydroxy-[1,1'-biphenyl]-3-carbonic acid), gives a probe that is useful for the visualization of COXin the iris tissue of the living human eye (6).
A further innovation is the labeling of ciprofloxacin, (1-cyclopropyl-6-fluoro-1,4-dihydro-4-oxo-7-(1-piperzynyl)-3-quinoline carbonic acid) with 99mTc, useful for theimaging of bacterial infections (7,8).
Technetium labeling of the very potent NSAID S(+) flurbiprofen might also be use-ful as a probe for the localisation of COX in living tissue. In the following report label-ing of the two individual enantiomers of flurbiprofen with 99mTc was undertaken.
MATERIALS AND METHODS
Drugs and Chemicals99mTcO4
- activity (sodium pertechnetate eluate) was obtained from a commerciallyavailable 99Mo/99mTc generator (Mallinckrodt). S(+) flurbiprofen (lotnr.: 16759) andR(-) flurbiprofen (lotnr.: 16754) were purchased from Duchefa (Haarlem, TheNetherlands); the amount of S(+) flurbiprofen in R(-) flurbiprofen is 0.7% ± 0.1%whereas the R(-) flurbiprofen content in S(+) flurbiprofen is 0.1% (9). Stannous tar-
Chapter 8
108

trate 500 microgram (BN040701; lyophilised) was purchased from IV DIRECT LTD(London, UK); Thin-layer chromatography materials consisted of Whatman No17paper (Tamson no.194K01) and ITLC-SG (Gelman no. 61886); scanning was per-formed with a Raytest chromatogram scanner equipped with miniGITA software.
Formulation of S(+) flurbiprofen and R(-) flurbiprofen SolutionPreparation of the flurbiprofen enantiomeric solutions proceeds by addition of 50mg S(+) flurbiprofen or R(-) flurbiprofen to a part of the available 0.3 M sodium chlo-ride solution. By addition of approximately 1 ml of 1M sodium hydroxide a clearsolution is obtained. The pH was adjusted between 7.0 -7.5 with hydrochloric acid0.2M before adding up to 100.0 ml. The final solution was filtered through a 0.22-micron filter. All flurbiprofen preparations were stored in glass containers. No pre-servative was added.
Analytical AssayBy use of HPLC combined with Diode Array Detection as described by Uges et al.(10) quality of the flurbiprofen enantiomeric solutions were assayed. In short, areversed phase RP-18 endcapped 5µm, 125x4mm column is used (MerckDarmstadt/Amsterdam, catalogue number: 21568); mobile phase: acetonitrile 470ml (Lichrosolve) phosphoric acid/triëthylamine 530 ml buffer pH 3.3. Injection vol-ume: 20 microliter of the enantiomeric solutions (diluted to 1:40 in the mobilephase). Content was analyzed by spectrophotometric assay (Varian CARY 3) at247 nm.
Preparation of 99mTc-S(+) flurbiprofen and 99mTc- R(-) flurbiprofen SolutionSodium chloride 0,9% (low in oxygen content) is added to a vial containing 500micrograms stannous tartrate. The contents of the vial are swirled cautiously. Nextthe calculated amount of sodium pertechnetate activity is added (1ml=60 MBq) fol-lowed by the addition of 1ml of 0.05% S(+) flurbiprofen or R(-) flurbiprofen solution.The total content (3 ml) is boiled for 10 minutes and assayed for radiochemical puri-ty of 99mTc-labeled flurbiprofen. Labeling is set at 85% or more.
Analytical Quality Control for Radiochemical PurityRadiochemical purity of a radiopharmaceutical is defined as the proportion of totalradioactivity in the desired compound.Analysis is performed by the two-strip mini-chromatography method as described(11). In figure 1 the basic outline of the procedure is presented.
99mTc-S(+) flurbiprofen
109

Figure 1. Two-strip Mini-chromatography System. On the left the Whatman no 17 andmethylethylketone solvent is used for pertechnetate separation, on the right ITLC-SG and PBSpH 7.4 or sodium chloride 0.9% as solvent is used for quantification of bound 99mTc. Numbers1,2,3 and 4 denote the following, 1: bound 99mTc and hydrolysed reduced technetium; 2: freeTcO4
-; 3: hydrolysed reduced technetium; 4: bound 99mTc and free TcO4-, respectively.
A spot (10 microliter) of solution is deposited on Whatman paper No 17 and devel-oped in methylethylketone. Pure pertechnetate will show up in the solvent front.
Likewise, a spot of the same solution is deposited on the ITLC-SG strip and devel-oped in phosphate buffered saline (PBS; pH 7.4) or 0.9% sodium chloride.
The chromatography strip is developed in the chosen solvent and analyzed by achromatographyscanner recording radioactivity along the length of the strip. Thepercentage of radiochemical impurity is calculated from the ratio of radioactivityassociated with the impurity compared with the radioactivity of the total strip.
RESULTS
Figure 2. HPLC Chromatogram of a 0.05% solution of R(-) flurbiprofen
Chapter 8
110

Analytical AssayHPLC and UV SpectrophotometryQuality control by HPLC of the 0.05% S(+) flurbiprofen or 0.05% R(-) flurbiprofensolution displayed no degradation peaks (figure 2) with a content of 102.2% for S(+)flurbiprofen and 99.9% for R(-) flurbiprofen measured by quantitative spectrophoto-metric analysis.
Radiopharmaceutical Quality ControlIn figures 3, 4 and 5 examples of radiopharmaceutical quality control by thin-layerchromatography are depicted.
Figure 3. Thin-layer Chromatogram of 99mTc-R(-) flurbiprofen developed in PBS pH7.4 assolvent on ITLC-SG. Peak 3 corresponds to hydrolysed reduced technetium, peak 4 tobound 99mTc and free TcO4
-
Figure 4. Thin-layer chromatography of 99mTc-S(+) flurbiprofen developed in PBS pH7.4 assolvent on ITLC-SG. Peak 3 corresponds to hydrolysed reduced technetium, peak 4 tobound 99mTc and free TcO4
-.
99mTc-S(+) flurbiprofen
111

Figure 5. Thin-layer chromatography of 99mTc-R(-) flurbiprofen developed in methylethyl-ketone as solvent on Whatman No 17. Peak 1 corresponds to bound 99mTc and hydrolysedreduced technetium, peak 2 to free TcO4
-.
Labeling efficiency for 99mTc-S(+) flurbiprofen solution, measured by the thin-layerchromatography system as described, resulted in 65% when sodium chloride 0,9%and 57% when PBS pH7.4 was used as the solvent. For 99mTc-R(-) flurbiprofen solu-tion, the efficiency accounted for 88% when sodium chloride 0,9% and 86% whenPBS pH7.4 was used as the solvent.
DISCUSSION
A better chelating ability (average: 87%) was found for the chiral ligand R(-) flur-biprofen with the achiral central ion 99mTc as compared to the chelation of S(+) flur-biprofen (61%). In these experiments other chiral compounds are absent. An arte-fact in chromatographic separation of bound 99mTc and free TcO4
- is excluded by thechoice of the materials used for the analysis.
The absolute configuration of S(+) flurbiprofen has been established utilising β-cyclodextrin complexation (12). Crystal structures of these complexes with R(-) flur-biprofen and S(+) flurbiprofen did reveal differences in binding to the host molecule(13). Although not directly conceivable, our result may derive from steric hindranceby the small fluorine atom present in the flurbiprofen molecule for binding of 99mTc,when one assumes that 99mTc will chelate with the carboxyl moiety of flurbiprofen
However, addition of sodium pertechnetate to a stannous tartrate solution at roomtemperature will produce, depending on pH and the amount of Sn2+ available, a99mTc5+-tartrate complex in quantitative yield. Tartrate is used in radiopharmaceuticalformulations as a transfer ligand, to prevent the Tc5+ from reducing further to loweroxidation states, mainly to avoid the formation of 99mTcO2-hydrate, which is thermo-
Chapter 8
112

dynamically stable and will compete even in the presence of a ligand with the 99mTc-complex formation. This ligand exchange method, also termed transchelation, thusinvolves first the formation of a 99mTc-complex with a weak ligand and then allowingthe complex to react with a second ligand that is relatively more stable. In this casea difference is seen between the S(+) isomer and the R(-) isomer in the formationof a more stable complex in favor of R(-) flurbiprofen.
The 99mTc flurbiprofen complex obtained presumably is a Tc5+ complex, in whichseveral possible structures, containing e.g. either the (Tc=O)3+ core (14), or the lin-ear trans-oxo group (O=Tc=O)+ (15), or the bridging (O=Tc-O-Tc=O)4+ unit (16),could be present, in which either one or more flurbiprofen molecules are coordina-ted to the 99mTc-core.
Hence it is both difficult and risky to make any definitive statements concerningsteric hindrance of the ligands unless some structural data are available. Yet, theexperimental fact showing that one isomer R(-), gives a significantly better labelingyield than the other one, S(+), under identical circumstances, points in that direction.
To gain more fundamental insight in the given experimental result we intend to fol-low a different approach namely the labeling of flurbiprofen with the 99mTc(CO)3-coreaccording to a newly available technique (17). Some advantages thereof are thehigh stability expected for the resulting 99mTc1+-complex as well as the ease of prepa-ration and high specific activity that can be achieved.
In conclusion, the low labeling efficiency of S(+) flurbiprofen make this complex lessattractive as a probe for imaging COX. Despite the greater labeling efficiency foundfor R(-) flurbiprofen it is unsuitable for use as a probe because the affinity of R(-) flur-biprofen for COX-1 and COX-2 is much lower (4, 5,18) than of its S(+) isomer.
REFERENCES
1. W.F. Kean, C.J.L. Lock, and H.E.Howard-Lock, Chirality in antirheumatic drugs, Lancet,1991,338,1565.
2. J.N. Cashman, The mechanisms of action of NSAIDs in analgesia, Drugs, 1996, 52, suppl., 5,13.3. J.R. Vane, Inhibition of prostaglandin synthesis as a mechanism of action for aspirin-like drugs,
Nature 1971, 231, 232.4. N.J. Van Haeringen, A.A. Van Sorge, J.L. Van Delft, and V.M.W. Carballosa Coré-Bodelier,
Flurbiprofen and enantiomers in ophthalmic solution tested as inhibitors of prostanoid synthesisin human blood, J. Ocul. Pharmacol. Ther., 2000, 16, 345.
5. N.J. Van Haeringen, A.A. Van Sorge, and V.M.W. Carballosa Coré-Bodelier, Constitutivecyclooxygenase-1 and induced cyclooxygenase-2 in isolated human iris inhibited by S(+) flur-biprofen, J. Ocul. Pharmacol. Ther. 2000, 16, 353.
6. A.A. van Sorge, R.J. van Etten, C.J. Rehmann, A.J.M. Rijnders, and N.J. van Haeringen,Diflunisal and the human iris Topical application reveals localisation, J. Ocul. Pharmacol. Ther.2002, 18,185.
99mTc-S(+) flurbiprofen
113

7. K.E. Britton, S. Vinjamuri, A.V. Hall, K. Solanki, Q.H. Siraj, J. Bomaji, and S. Das, Clinical evalu-ation of technetium-99m Infecton for the localisation of bacterial infection. Eur. J. Nucl. Med., 1997,24, 553.
8. F.X. Sundram, W.Y. Wong, E.S. Ang, A.S. Goh, D.C. Ng and S. Yu. Evaluation of technetium-99m
ciprofloxacin (Infecon) in the imaging of infection, Ann Acad Med Singapore 2000,29,699.9. A.A. van Sorge, P.H. Wijnen, J.L. van Delft, V.M.W. Carballosa Coré-Bodelier, and N.J. van
Haeringen, Flurbiprofen, S(+), eyedrops: formulation, enenatiomeric assay, shelflife and phar-macology, Pharm. World. Sci., 1999, 21, 91.
10. D.R.A. Uges, and J.M.H Conemans, Antidepressants and antipsychotics. In Forensic Science.Handbook of Analytical Separations, Vol. 2, Bogusz, M.J., (ed., pp. 229-257 (with special refer-ence to pp. 247-248, 2000), ISBN 0-444-82998-9.
11. P.J. Robbins, Chromatography of Technetium-99m radiopharmaceuticals: a practical guide. TheSociety of Nuclear Medicine, Inc., New York, USA, ISBN: 0-932004-18-0.
12. K. Uekama, T. Imai, F. Hirayama, M. Otagiri, and K. Harata, X-ray crystallographic determinationof the absolute configuration of (+)flurbiprofen utilizing b-cyclodextrin complexation, Chem.Pharm. Bull. 1984, 32, 1662.
13. K. Harata, F. Hirayama, T. Imai, K. Uekama, and M. Osagiri, Crystal structures of permethylatedb-cyclodextrin complexes with R-(-)- and S-(+)-flurbiprofen, Chem. Lett. 1984, 1549.
14. A.M. Verbruggen, D.L. Nosco, C.G. van Nerom, G.M. Bormans, P.J. Adriaens and M.J. de Roo,Technetium-99m-L,L-ethylenedicysteine: a renal imaging agent. I. Labeling and evaluation in ani-mals, J Nucl Med 1992, 33, 551-7.
15. P.H. Fackler, M.J. Lindsay, and M.J. Clarke ,Synthesis and structure of trans-[O2(Im)4Tc]Cl 2h2O,trans-[O2(1-meIm)4Tc]Cl 3H2O and related compounds, Inorg Chim Acta 1985, 109, 39-49.
16. F. Tisato, F Fiorenzo, U Mazzi, G Bandoli, and A Dolmella, Synthesis, characterization and elec-trochemical studies on technetium(V) and rhenium(V) oxo-complexes with N,N'-2-hydrox-ypropane-1,3-bis(salicylideneimine), Inorg Chim Acta 1989, 164, 127-35.
17. R. Alberto, R. Schibli, R. Waibel, U. Abram, A.P. Schubiger, Basic aqueous chemistry of[M(OH)2)3(CO)3]+ (M=Re, Tc) directed towards radiopharmaceutical application, Coord ChemRev 1999, 190, 901-19.
18. A.A. van Sorge, J.L. van Delft, V.M.W. Bodelier, P.H. Wijnen, and N.J. van Haeringen, Specificityof Flurbiprofen and enantiomers for inhibition of prostaglandin synthesis in bovine iris/ciliarybody, Prostaglandins Other Lipid Mediat 1998, 55, 169.
114

CHAPTER 9ALTERNATIVE SPLICING OFCYCLOOXYGENASE-1 MRNA
IN THE HUMAN IRIS
Melloney J. Dröge, Adriaan A. van Sorge, Nicolaas J. van Haeringen,Wim J. Quax and Johan Zaagsma
submitted for publication

ABSTRACT
In homogenates of the human iris, the non-steroidal anti-inflammatory drug (NSAID)S(+) flurbiprofen has been reported to inhibit cyclooxygenase-1 (COX-1) 70-foldmore potently than in human whole blood. We hypothesized that this difference maybe due to alternative splicing of COX-1 mRNA in the human iris or in whole blood. Inthis study, we have identified a similar COX-1 splice variant (COX-1SV) in both tis-sues with comparable COX-1/COX-1SV expression ratios. Therefore, we concludethat the difference in IC50 values of S(+) flurbiprofen towards COX-1 in the humaniris and human whole blood is not related to differences in the occurrence of splicedCOX-1.
INTRODUCTION
Prostaglandin G/H synthase (PGHS), cyclooxygenase (COX) (EC 1.14.99.1) is amembrane bound homodimer of two 70 kDa polypeptides, catalyzing the first twosteps in prostaglandin, thromboxane and prostacyclin synthesis (1). Two PGHS iso-forms, referred to as COX-1 and COX-2, have now been identified and cloned, andcharacterized as hemoproteins possessing both cyclooxygenase and hydroperoxi-dase activity (2-4). Inhibition of the cyclooxygenase activity of PGHS is responsiblefor the anti-inflammatory activity of non-steroidal anti-inflammatory drugs (NSAIDs).The peroxidase activity of PGHS catalyzes oxidation of a broad range of substrates.
COX-1 is constitutively expressed in various tissues (5), such as kidney, stomach,platelets, and the iris/ciliary body (6), whereas COX-2 is induced after cell activa-tion by various mediators of inflammation and bioactive agents (7). In the humaneye, the iris is the major site for producing prostaglandins, which regulate smoothmuscle contraction, blood-aqueous-barrier penetration and intra-ocular pressure(8). We have previously shown in human iris homogenates that COX-1 is indeedconstitutively expressed whereas COX-2 could be detected after stimulating withlipopolysaccharide (LPS) (9).
Inhibition of the COX activity towards prostaglandin E2 production could beachieved with the NSAID S(+) flurbiprofen in human iris homogenates. Remarkably,a 3600 fold stronger inhibition of COX-1 over COX-2 was observed (9). On theother hand, in separate experiments with human whole blood, S(+) flurbiprofeninhibited COX-1 and COX-2 rather similarly with a ratio of 32 (10). We hypothesizedthat the differential effects of S(+) flurbiprofen could be due to the presence of analternative splice variant of the COX-1 enzyme in the iris as compared to wholeblood. This seems reasonable since Diaz and coworkers reported that a splice vari-ant of COX-1 is present in human lung fibroblasts (11). Indeed, comparison of theIC50 values (half maximal inhibitory concentrations) for the inhibition of COX-1 by
Chapter 9
116

S(+) flurbiprofen in human iris tissue and whole blood revealed a 70-fold higherpotency towards COX-1 present in human iris tissue (9-10).
MATERIALS AND METHODS
Tissue collectionTissue of human irides was obtained immediately after surgery from eyes sched-uled for enucleation due to melanoma formation. After enucleation, the dissectediris tissue was snap-frozen in liquid nitrogen and stored at -80°C for subsequentRNA isolation. Human whole blood was collected in the presence of ethylenedi-aminetetraacetic acid (EDTA) and RNA extraction was performed subsequently.
RNA isolationTotal RNA was isolated from iris and whole blood samples using the RNeasy mini kitand QIAamp RNA blood mini kit, respectively (Qiagen) (12). Small amounts of iristissue (<50 mg) were homogenized in 1 ml of lysis solution using a motorized rotor-stator homogenizer. The homogenates were repeatedly centrifuged to remove tissuedebris before proceeding to filtration. Further extraction steps were performedaccording to the manufacturer's protocol. RNA derived from this procedure wastreated with DNAseI (Ambion) to remove contaminating DNA. RNA was quantifiedby measuring the optical density at 260 nm in triplicate.
OligonucleotidesPrimers were designed as described by Diaz and coworkers (11). In short, a set ofprimers was designed to specifically span the COX-1SV junction: COX-1SVREV1:5'-TTC ATG CCA AAC CTC TTG-3'; COX-1SVFOR1: 5'-GGA GAC CAT CAA GATTGT-3' (Life Technologies). The primers amplified 405 (COX-1 mRNA) or 294(COX-1SV mRNA) base pairs, respectively.
Reverse transcriptionTotal RNA (1.0 µg) was reverse transcribed in a volume of 75 µl containing: 1 xReverse transcription buffer, 10 mM MgCl2, 1 mM dNTPs, 60 units RNasin ribonu-clease inhibitor, 30 units AMV reverse transcriptase and 1.25 µg random hexamerprimers (all from Promega). Control reactions, containing neither reverse transcrip-tase nor RNA were run in parallel. Each subsequent PCR contained 3 µl cDNA tem-plate. Therefore, the amount of amplified PCR product was relative to a constantamount of starting RNA. To evaluate RNA quality, we performed a RT-PCR with 18Sprimers (18Suni1: 5'-CTA TTG CGC CGC TAG AGG TG-3'; 18Suni2: 5'-CTG AACGCC ACT TGT CCC TC-3'; Eurogentec)
COX-1 splice variant
117

PCRThe COX-1 gene fragment was amplified using the primers COX-1SVFOR andCOX-SVREV. All PCRs were performed using Pfu DNA polymerase (Stratagene, LaJolla, CA, U.S.A.). Amplification of the cDNA was performed by 40 cycles of PCRin 50 µl of Pfu DNA polymerase mixture, containing 25 pm of the COX-1SVREV1and COX-1SVFOR1 primers. The PCR protocol had low annealing and extensiontemperatures: 4 min. at 94°C, followed by 10 cycles of 30 s at 94°C, 1 min 37°Cand 10 min at 50°C, followed by 30 cycles in which the extension time was at first8 min, but increased by 15 s in each cycle (first cycle: 30 s 94°C, 1 min 55°C andthen 8 min 72°C). At the end, DNA production was finished with 10 min at 72°C. ThePCR products were analyzed by 1.5% agarose gel electrophoresis stained withethidium bromide. DNA size markers were from Fermentas (GeneRuler™ 100bpDNA Ladder). Restriction analysis using NcoI verified the sequence of the con-structs.
RESULTS AND DISCUSSION
The COX-1 gene is localized on the human chromosome 9q32-q33.3. The COX-1protein is expressed constitutively in almost all mammalian tissues and is describedas a housekeeping enzyme, responsible for cell-to-cell signaling, tissue homeosta-sis, and cytoprotection.
More recently, Diaz et al have reported the expression of two COX-1 isoforms inhuman lung fibroblasts. By cloning of the cDNA, they demonstrated that the corre-sponding mRNA can be spliced in such a way that 111 base pairs are eliminatedfrom exon 9, resulting in a COX-1 isoform that lacks residues 396-432 (11). Sincethis splicing occurs in-frame, it is expected that it will be translated into an identicalprotein. However, the alternative splicing results in the elimination of one of the fourfunctionally required N-glycosylation sites at residue 409, providing a possiblemechanism for differential regulation of enzymatic activity under physiological orpathological conditions (11,13).
In this respect, we hypothesized that different expression levels of COX-1 and itsshorter isoform could account for the difference in IC50 values of S(+) flurbiprofenobserved with human iris and human whole blood. Therefore, three human iris sam-ples were analysed for the presence of the two transcripts variants. In addition,human whole blood (corresponding to iris 1) was screened for the presence of bothtranscripts as well as human blood samples from four healthy volunteers. TotalmRNA was extracted from the human iris and blood samples and RT-PCR was per-formed subsequently. To assess whether the transcripts corresponded to COX-1 orthe alternatively spliced COX-1, the cDNA was PCR amplified using a set of primersthat specifically spanned the COX-1SV junction: a fragment of 405 base pairs
Chapter 9
118

should be obtained from transcripts with an intact exon 9, and a fragment of 294base pairs if exon 9 was lacking. PCR amplification revealed that both transcriptswere present in the human iris tissues as well as in the whole blood samples (fig-ure 1 (A)) as judged by the appearance of two major bands of approximately 400and 300 base pairs, respectively.
The gene fragments were further characterized by restriction analysis using NcoI.Restriction analysis would yield fragments of 285 and 120 base pairs (from the tran-script of 405 base pairs corresponding to an intact exon 9) and 174 and 120 basepairs (from the transcript of 294 base pairs corresponding to the spliced variant).Figure 1 (B) illustrates that all fragments were indeed obtained, thereby confirmingthe correct identity of both transcripts. No significant dissimilarities were observedbetween the various iris and whole blood samples. Furthermore, the majority of thetotal COX-1 mRNA is expressed as the fully intact COX-1, whereas only a minoramount is present as the alternatively spliced variant COX-1SV. In addition, relativeexpression levels of COX-1 and COX-1SV in the human iris and plasma are similar.
Figure 1: (A) Analysis of mRNA from human iris tissue and whole human whole blood. 1 µgof total RNA was reverse-transcribed and amplified by PCR as described in the material andmethods. The PCR product were analysed on a 1.5% agarose gel stained with ethidiumbromide. Lane 1 - 3: human iris tissue; lane 4 human whole blood (corresponding to iris 1);lane 5 - 7: human whole blood references.
COX-1 splice variant
119

Figure 1: (B) Restriction analysis of the PCR product from a human iris tissue sample (iris3) and a human whole blood sample (whole blood reference 7). Restriction analysis wasperformed using NcoI. Lane 1: PCR product from human iris 3; lane 2: PCR product fromhuman iris 3 after NcoI digestion; lane 3: PCR product from human whole blood 7; lane 4:PCR product from human whole blood 7 after NcoI digestion.
In conclusion, we have detected a splice variant of COX-1 in human irides andwhole blood for the first time. Comparison of the expression levels of COX-1 andCOX-1SV in the human iris and blood showed no striking differences. These find-ings indicate that the observed difference in IC50 values of S(+) flurbiprofen towardsthe human iris and human whole blood does not result from an alternatively splicedCOX-1 transcript. An alternative explanation may be that the iris COX-1 recognitionsite of S(+) flurbiprofen is able to adopt a different conformation than the bloodenzyme.
Acknowledgement: Provision of tissue samples of human irides by Prof. Dr. J.E.E.Keunen (Department of Ophthalmology, Academic Medical Center Leiden, TheNetherlands), Dr. P. Saeed & Prof. Dr. M.D. de Smet (Department of Ophthal-mology, Academic Medical Center Amsterdam, The Netherlands), Prof. Dr. J.M.M.Hooymans (Department of Ophthalmology, University Hospital Groningen, The
Chapter 9
120

Netherlands) and Prof. Dr. W. Timens (Department of Pathology, University HospitalGroningen, The Netherlands) is greatly acknowledged. We would like to thank MrsA. Brugman and Prof. Dr. F Muskiet (Department of Pathology and LaboratoryMedicine, Groningen University Hospital, The Netherlands) for the RNA isolationfrom whole human blood. Dr. M. Elferink (Department of Pharmacokinetics andDrug Delivery, University of Groningen, The Netherlands) is acknowledged for hervaluable advise concerning the RNA procedures of the iris samples.
REFERENCES
1. Needleman, P., Turk, J., Jakshick, B.A., Morrison, A.R., Lefkowith, J.B. (1986). Arachidonic acidmetabolism. Annu Rev Biochem., 55, 69-102.
2. Hla, T., Neilson, K. (1992). Human cyclooxygenase-2 cDNA. Proc. Natl. Acad. Sci. USA, 89,7384-8.
3. Yokoyama, C., Tanabe, T. (1989). Cloning of the human gene encoding prostaglandin endoper-oxide synthase and primary structure of the enzyme. Biochem. Biophys. Res. Commun., 165,888-94.
4. Hla, T. (1996). Molecular characterization of the 5.2 KB isoforms of the human cyclooxygenase-1 transcript. Prostaglandins, 51, 81-5.
5. Simmons, D.L., Xie, W., Chipman, J.G., Evett, G.E. (1991). Multiple cyclooxygenases: cloning ofa mitogen inducible form. In: Prostaglandins, Leukotrienes, Lipoxins, and PAF. Bailey J.M. ed.,Plenum Press, New York, 67-78.
6. Asakura, T., Sano, N., Shichi, H. (1992). Prostaglandin synthesis and accumulation by porcin cil-iary epithelium. J. Ocul. Pharmacol., 8, 333-41.
7. Xie, W., Chipman, J.G., Robertson, D.L., Erikson, R.L., Simmons, D.L. (1991). Expression of amitogen responsive gene encoding prostaglandin synthase is regulated by mRNA splicing. Proc.Natl. Acad. Sci. USA, 88, 2692-6.
8. Matsuo, T., Cynader, M.S. (1993). The EP2 receptor is the predominant prostanoid receptor inthe human ciliary muscle. Br. J. Ophtalmol., 77, 110-4.
9. Van Haeringen, H.J., van Sorge, A.A., van Delft, J.L., Carbalossa Coré-Bodelier, V.M.W. (2000).Flurbiprofen and enantiomers in ophthalmic solution tested as inhibitors of prostanoid synthesis inhuman blood. J. Ocular Pharm. Ther., 16, 345-52.
10. Van Haeringen, N.J., van Sorge, A.A., Carbalossa Coré-Bodelier, V.M.W. (2000). Constitutivecyclooxygenase-1 and induced cyclooxygenase-2 in isolated human iris inhibited by S(+) flur-biprofen. J. Ocular Pharm. Ther., 16, 353-61.
11. Diaz, A., Reginato, A.M., Jiminez, S.A. (1992). Alternative splicing of human prostaglandin g/hsynthase mRNA and evidence of differential regulation of the resulting transcripts by transform-ing growth factor ß1, interleukin 1ß, and tumor necrosis factor a. J. Biol. Chem., 267, 10816-22.
12. Kyveris, A., Maruscak E., Senchyna, M. (2002). Optimization of RNA isolation from human oculartissues and analysis of prostanoid receptor mRNA expression using RT-PCR. Mol. Vis., 8, 51-8.
13. Cáceres, J.F., Kornblihtt, A.R. (2002). Alternative splicing: multiple control mechanisms andinvolvement in human disease. Trends Genet., 18, 186-93.
COX-1 splice variant
121

122

SUMMARY

SUMMARY AND OUTLINE OF THIS THESIS
Surgery of the eye lens has become the treatment of choice for senile cataract. Asfrom the first description of this therapy, there have been reports on a serious com-plication in the macula of the retina (macula retinae) affecting the vision of thepatient. This complication, first described in 1953, has become known as cystoidmacular oedema. The incidence varies between 2 and 50%, but can incidentally goup to 70%. Publications on eye research mainly of Japanese origin have describedthe use of topically applied indomethacin to prevent cystoid macular oedema afterlens extraction. In response to these reports, in the clinics of Arnhem a questionabout the feasibility of preparing indomethacin eyedrops was put forward in 1980by one the ophthalmologists to the hospital pharmacist. This question has triggeredthe research described in this thesis.
Following these reports on the prevention of cystoid macular edema after lensextraction, several formulations of indomethacin eyedrops have been described inthe Dutch and international literature. Indomethacin acts by inhibition of the syn-thesis of prostaglandins, mediators involved in the inflammatory reaction, that is atthe basis of this complication. Indomethacin was introduced into the field of oph-thalmology in different types of formulations, including solutions in sesame oil,aqueous suspensions and aqueous solutions. Concentrations in oily solutions var-ied from 0.1 to 1%, in suspensions from 0.5% to 1% and in aqueous solutions from0.35 to 1%.
Unfortunately, the sesame oil based solutions turned out to be less suitable, sincethey caused blurring of vision as a result of difference in refractive index. The aque-ous solutions on the other hand, being either a suspension or a solution, were irri-tating to the eye (burning sensation). In order to alleviate this undesirable side effecta reduction in concentration was suggested from 1% to 0.2 or 0.1% indomethacin.In 1981 it was shown that four different indomethacin suspension eyedrops, all0.5% in concentration, gave different prostaglandin synthesis inhibiting activities,which was attributed to differences in physicochemical properties. It was conclud-ed that, apart from the subjective complaints of irritation of the eye, the use of eye-drops as a suspension gives rise to non-reproducible pharmacokinetic and phar-macodynamic behaviour.
As a result of the afore-mentioned question, a phosphate buffered (pH 7.4) aque-ous solution of indomethacin was prepared by means of the organic base meglu-mine, in a concentration of 0.1%. These eyedrops were introduced in clinical prac-tice in 1981 and produced no burning sensation when applied to the patient's eye.In 1984 Indoptol ®, an aqueous suspension eyedrop of 1% indomethacin, wasintroduced in the Dutch market and in 1986 Indocid® of comparable compositionwas introduced in France. In 1987 a new presentation of indomethacin followed in
Summary
124

France as Indocollyre® 0,1%, which was introduced in The Netherlands in 1994.This formulation contains indomethacin as a lyophilized (freeze-dried) product,which is brought into solution by addition of a sterile borate buffer. Ongoing ownresearch on our in-house developed eyedrops with different bases, L-lysine, D-lysine, L-arginine, D-arginine and tromethamol (not published), did not provide suit-able pharmaceutical alternatives.
In the meantime our first introduced (1981) solution of indomethacin 0.1%, withoutthe need of extra pharmaceutical excipients, remained the mainstay of the eye clinic.
This solution was tested in a pharmacological setting in the rabbit eye using aparacentesis model of removing aqueous humor and measuring the influx of pro-tein and fluorescein into the secondary aqueous humor which reflects the break-down of the blood-aqueous barrier. The results showed that in a concentration ofindomethacin as low as 0.05%, already 90 - 100% of the pharmacological activityis obtained, as demonstrated by the inhibition of fluorescein and protein influx.Following these results our indomethacin 0.1% formulation was incorporated in theDutch National Formulary (FNA) in 1986. Impracticalities with indomethacin inaqueous solution - no sterilisation possibility and only a relatively short shelf-lifewhen in solution - prompted us to explore the possibility of formulating eyedropsbased on a different NSAID.
In 1990, topically applied S(+)ibuprofen was reported to be effective in a rabbitmodel of interleukin-1 or paracentesis induced uveitis at relatively elevated con-centrations (0.9% and 0.8% respectively). Also with S(+) naproxen, marketed bySyntex as an enantiomeric pure NSAID, the anti-inflammatory effect of eyedrops(0,5%) was demonstrated experimentally. In our search for a pharmaceuticallymore acceptable solution of an NSAID - the introduction to the Dutch market of adiclofenac ophthalmic 0.1% solution (Naclof®) being imminent - we turned to theUSP in which a flurbiprofen sodium ophthalmic solution is mentioned. Weembarked on a study to manufacture flurbiprofen eyedrops by the protocol of June1992. A letter of consent, with restricted financial aid, for the project (9206SO.008)was issued January 8th 1993 by the SWOR (Stichting ter bevordering vanWetenschappelijk Onderzoek in ziekenhuis Rijnstate).
The aim of this thesis was to investigate and to evaluate the pharmaceutical appli-cation of flurbiprofen in eyedrops as well as the pharmacology of this nonsteroidalanti-inflammatory drug. Flurbiprofen is a chiral molecule implying that the racemateis presumably not the preferred pharmacological form to prepare such eyedrops.Therefore it was deemed necessary to characterize the contribution of each enan-tiomer. At the start of the investigations, the pharmacological action of flurbiprofenwas attributed to the inhibition of the cyclooxygenase enzyme (COX), which isknown to be responsible for prostaglandin synthesis. In 1991 it became apparent
Summary
125

that not one but two isoenzymes are capable of synthesising prostaglandins (COX-1 and COX-2). Our investigations became more challenging as it was postulatedthat this second isoenzyme would be the more relevant target for nonsteroidal anti-inflammatory drugs as its activity would be related more closely to inflammation. Itwas decided to study both the racemic form and the individual enantiomers of flur-biprofen for prostaglandin synthesis inhibiting activity. S(+) flurbiprofen showed amarked selectivity for inhibition of COX-1 compared to COX-2, both in an extra-ocu-lar matrix (human whole blood) and in human iris/ciliary body preparations. Sincethe susceptibility of iris COX-1 for S(+)flurbiprofen was 70-fold higher than for bloodCOX-1 the hypothesis was raised that a splice variant of COX-1 in the human iriscould be responsible for this observation.
In chapter 2 the rationale for the chosen buffer in the S(+) flurbiprofen eyedroppreparation is described. Although the eye, especially the nasal corner, the eyelidsand skin surrounding the eye are sensitive to external stimuli, physiological reac-tions due to deviations outside the normal values for osmolarity or pH are notalways seen. In a state of ill-health or during regular use of ophthalmic preparations,this situation may be more outspoken, however. The active component in the eye-drop can provoke, when not properly dissolved, a prickling or burning sensationleading to lacrimal discharge, occasional haemorrhage or endangering blinkingreflexes during surgery. Lacrimal discharge will cause an unwanted dilution anddrainage of medicine. Individual sensitivity may vary and physiological values oftear fluid can fluctuate, dependant on the health condition of the individual eye. Eyeirritation must be discerned from an allergy, which requires the choice of a differentpharmacological agent.
Non-irritating eyedrops should in principle comply with: (1) sterility, (2) isotonicityand (3) pH value. Sterility is of paramount importance when the ophthalmic solutionis applied to the injured eye. Isotonicity with respect to the tear fluid will reduce irri-tation and adverse reactions of the eye. The pH value of the formulation is of utmostimportance both for stability during storage and for keeping the formulation withinphysiological limits. During storage hydroxyl ions, released from the glass contain-ers, can raise the pH which may endanger the stability of the active principle. Onthe other hand, the lacrimal fluid has only limited buffering capacity. Therefore thechoice for a buffer applied to the ophthalmic solution of flurbiprofen is governed bythe following issues: (1) flurbiprofen is unstable at high pH, (2) the solubility of flur-biprofen in aqueous solution is problematic at pH values below 7, (3) the natural pHof the tear fluid is 7.4 and (4) the tolerability for the patient is in the pH range of pH6.6 - 7.8.
Based on practical experience with the indomethacin eyedrops a choice wasmade for the phosphate buffer (pH 7.4) in the preparation of the S(+) flurbiprofeneyedrops. A citrate buffer of pH 6.45, as is employed in Ocuflur® (racemic flur-
Summary
126

biprofen sodium), was not considered favourable as it has an extreme in its buffer-ing capacity at pH 6.5. The same choice was made later on, in a United Statespatent 4,996,209, describing the preparation of a single enantiomer in a phosphatebuffer. Although additional components were also present in that composition, theeyedrops described in this thesis are free of other components.
In chapter 3 the stability of the formulation is addressed. The active S(+) enan-tiomer of flurbiprofen was formulated into a stereoselective, ballast free ophthalmicsolution in a concentration of 0.015%. Analysis by capillary zone electrophoresisshows shelflife stability of up to four years at room temperature of this enantiomer.The inhibitory effect of S(+) flurbiprofen on the synthesis of prostaglandins, asmeasured in a homogenate of bovine iris/ciliary body, remained unaffected duringa shelflife period of three years after manufacture.
Chapter 4 describes the pharmacological activity of different flurbiprofen prepara-tions in isolated bovine iris/ciliary body homogenates. Concentration-responsecurves have been determined for S(+) flurbiprofen, R(-) flurbiprofen as well as theracemate, to inhibit PGE2 production mediated by COX-1. A significant differencebetween the enantiomers was established. S(+) flurbiprofen proved one hundredtimes more potent than R(-) flurbiprofen. It was concluded that S(+) flurbiprofen isthe active component that should be incorporated in the ophthalmic solution.
Using the human whole blood assay as described by Patrignani et al. (1994), inchapter 5 differences were detected between S(+) flurbiprofen, R(-) flurbiprofen andracemic flurbiprofen for inhibition of COX-1 and COX-2. COX-1 activity was moni-tored by measuring TxB2 (the stable metabolite of TxA2) production from theplatelets, whereas COX-2 activity was determined using PGE2 production in mono-cytes, following induction of this enzyme by LPS. The stereoselectivity of S(+) flur-biprofen compared to R(-) flurbiprofen, expressed as the reciprocal of the ratio of theconcentrations giving 50% inhibition (IC50), amounted to 340 for COX-1 and 56 forCOX-2. The selectivity of racemic flurbiprofen for COX-1 versus COX-2, was 16-fold.
In chapter 6 the interaction of S(+) flurbiprofen with COX-1 and COX-2 in the humaniris was studied. After LPS-treatment for 24h, substantial amounts of COX-2immunoreactivity could be visualized for the first time in human iris/ciliary body prepa-rations. Remarkably, S(+) flurbiprofen showed a 3,600-fold higher potency for inhibit-ing COX-1 compared to COX-2. Furthermore, the susceptibility of human iris COX-1for inhibition by S(+) flurbiprofen was 70-fold higher than of COX-1 in human blood.
In chapter 7 the distribution of a flurbiprofen analogue in the human eye has beenvisualised. Technetium labelled diflunisal, sharing pharmacological and chemicalresemblance with flurbiprofen as an NSAID being fluorinated and possessing abiphenyl ring, was used in an attempt to visualize COX-activity in the internal struc-tures of the eye. The scintigraphic results obtained with this labelled drug werecompared with instillation of the same volume and activity of pertechnetate. An
Summary
127

amount of 3% of instilled technetium labelled diflunisal could be localized in the eye.Activity could be visualized in the area of the iris indeed. Diflunisal was usedbecause the labelling efficiency of S(+) flurbiprofen proved not appropriate (Chapter8). R(-) flurbiprofen would chemically be a good labelling agent, but not pharmaco-logically, for obvious reasons (Chapters 5 and 6).
In the final Chapter the occurrence of alternative splicing of COX-1 in RNA in thehuman iris was explored, as a possible explanation of the remarkably high affinityof S(+) flurbiprofen reported in Chapter 6. Indeed an alternatively spliced mRNACOX-1 splice variant (SV) could be detected in the human iris tissue from 3patients. However, the same splice variant was also found in blood cells derivedfrom four individuals. The amount of COX-1SV present in the human iris was notsignificantly different from the amount present in blood cells, implying that theoccurrence of the COX-1 splice variant in the iris can not explain the observed dif-ference in IC50 by S(+) flurbiprofen between human iris (0.8 nM) and human blood(56 nM) for COX-1 inhibition.
Summary
128

SAMENVATTING

SAMENVATTING
De operatieve verwijdering van de ooglens, tegenwoordig gevolgd door implantatievan een kunstlens, is vandaag de dag de voorkeurstherapie voor de behandelingvan ouderdomscataract (staar). Vanaf de eerste toepassingen van deze therapiezijn ernstige bijwerkingen in de macula van het netvlies gerapporteerd, welke hetgezichtsvermogen van de patiënt ernstig kunnen aantasten. Deze complicatie werdvoor het eerst beschreven in 1953 en staat bekend onder de naam cystoid maculaoedeem. De incidentie van deze aandoening varieert van 2 tot 50%, maar spo-radisch worden percentages van 70% gemeld. Eind jaren zeventig werd in een aan-tal Japanse publicaties het gebruik van indomethacine oogdruppels ter preventievan het cystoid macula oedeem beschreven. Op grond hiervan werd in 1980 in deklinieken van Arnhem door een van de oogartsen aan de ziekenhuisapothekergevraagd of deze een indomethacine oogdruppel kon samenstellen, omdat deze(nog) niet in de handel was. Deze vraag was uiteindelijk de aanleiding tot hetontstaan van dit proefschrift.
Na deze eerste publicaties over de preventie van cystoid macula oedeem, zijn erdiverse formuleringen van indomethacine oogdruppels beschreven in deNederlandse en internationale literatuur. Indomethacine is een remmer van de syn-these van prostaglandines, een belangrijke klasse van ontstekingsmediatoren, ookbij deze aandoening. Indomethacine oogdruppels werden geïntroduceerd in ver-schillende formuleringen waaronder oplossingen in sesamolie, waterige suspen-sies en waterige oplossingen. Concentraties van oplossingen in olie varieerden van0,1 tot 1,0%, in suspensie oogdruppels van 0,5% tot 1% en in waterige oplossin-gen van 0,35 tot 1,0%.
Helaas leidde het gebruik van olieachtige oogdruppels tot klachten over wazig zien,veroorzaakt door het verschil in brekingsindex. De waterige oplossingen daarente-gen - hetzij als suspensie, hetzij als oplossing - veroorzaakten vaak irritatie van hetoog. Om van deze, hinderlijke bijwerking af te komen werd een verlaging van deindomethacine concentratie voorgesteld van 1% naar 0,2% of 0,1%.
In 1981 werd aan de hand van vergelijkend onderzoek van vier indomethacinesuspensie-oogdruppels (0,5%) geconstateerd, dat de mate van prostaglandinesyn-these remming nogal varieerde, waarschijnlijk als gevolg van verschillen in fysischchemische eigenschappen. Geconcludeerd werd dat het gebruik van suspensie-oogdruppels niet reproduceerbare farmacokinetische en farmacodynamischeuitkomsten gaf.
In antwoord op bovengenoemde vraag werd door ons met succes een waterigefosfaat-gebufferde indomethacine oplossing (pH 7,4) ontwikkeld in een concen-tratie van 0,1%, waarbij de indomethacine in oplossing werd gebracht met behulp
Samenvatting
130

van de organische base meglumine. Deze oogdruppel werd in 1981 in de kliniekgeïntroduceerd en had geen irriterende bijwerkingen in het oog.
In 1984 werd Indoptol®, een 1% indomethacine suspensie oogdruppel, op deNederlandse markt geïntroduceerd en 1986 werd Indocid®, met een vergelijkbaresamenstelling, in Frankrijk op de markt gebracht. In 1987 volgde een nieuwontwikkelde vorm van de indomethacine oogdruppel, Indocollyre®, in een sterktevan 0,1%. Introductie van dit product op de Nederlandse markt geschiedde in 1994.Deze formulering bevat indomethacine als gevriesdroogd product, hetgeen inoplossing gebracht kan worden door additie van een steriele boraatbuffer.
Nader onderzoek van de eigen indomethacine oogdruppel met verschillendeorganische basen zoals L-lysine, D-lysine, L-arginine, D-arginine en trometamolleverde geen verbeterde oplossing op. De in 1981 geïntroduceerde, aseptischbereide, gebufferde indomethacine oplossing (pH 7,4) in een concentratie van0,1%, zonder verdere farmaceutische toevoegingen bleef dientengevolge déoplossing in onze kliniek.
Deze oplossing werd farmacologisch onderzocht middels het paracentese model,waarbij vocht aan de voorste oogkamer van het konijnenoog wordt onttrokken ende influx van eiwit en fluoresceïne in het secundair gevormde oogkamerwater (alsmaat voor de verbreking van de bloed-kamerwater barrière) gemeten wordt. Uit deresultaten bleek dat een concentratie van slechts 0,05% indomethacine al resul-teerde in 90 - 100% remming van eiwit- en fluoresceïne- instroom. Op grond vandeze resultaten werd de door ons ontwikkelde indomethacine formulering in 1986opgenomen in het FNA.
Nadeel van deze formulering is echter, dat het hier een aseptische bereiding vaneen oogdruppeloplossing betreft met een beperkte houdbaarheid. Hierdoorontstond het idee om te onderzoeken of er ook oogdruppels te formuleren warenop basis van een andere NSAID.
In 1990 werd gerapporteerd dat S(+) ibuprofen in een concentratie van respec-tievelijk 0,9% en 0,8% effectief was in de bestrijding van door interleukine-1 of doorparacentese geïnduceerde uveitis. Ook van S(+) naproxen, op de markt gebrachtdoor de firma Syntex als een zuiver enantiomeer, werd het anti-inflammatoir effectals oogdruppel (0,5%) experimenteel aangetoond. Op zoek naar een farmaceutischmeer compatibele oplossing voor een andere NSAID werd in de United StatesPharmacopeia (USP) de monografie van flurbiprofen sodium ophthalmic solutionaangetroffen , terwijl in Nederland de introductie van een diclofenac oogdruppel(Naclof®) op handen was.
In 1992 werd het plan opgevat om flurbiprofen oogdruppels te gaan bereiden. Hetproject werd ter beoordeling aangeboden aan de Stichting Wetenschappelijk
Samenvatting
131

Onderzoek Rijnstate (9206SO.008) en in een brief van 8 januari 1993 werd beperk-te financiële steun toegezegd.
De scope van dit proefschrift betreft een onderzoek naar de farmaceutische berei-ding en -eigenschappen van flurbiprofen oogdruppels en de farmacologie van ditNSAID. Flurbiprofen is een chiraal molecuul, wat inhoudt dat de racemische vormmogelijk niet de gewenste farmacologische entiteit is voor de bereiding van oog-druppels. Derhalve werd het noodzakelijk geacht de bijdrage van elk enantiomeerafzonderlijk te onderzoeken, zodat een gefundeerde keuze gedaan kon wordenvoor de bereiding van een oogdruppel met de meest actieve chirale entiteit. Bij deaanvang van dit onderzoek werd aangenomen dat de farmacologische werking vanflurbiprofen gebaseerd is op remming van het enzym cyclooxygenase (COX), datverantwoordelijk is voor de synthese van prostaglandines. In 1991 werd duidelijk,dat niet één maar twee isoenzymen (COX-1 en COX-2) betrokken zijn bij de syn-these van prostaglandines. Het onderzoek kreeg hierdoor een nieuwe uitdagingwant er was ook geconstateerd, dat dit tweede isoenzym sterker aan ontstekinggerelateerd zou zijn - en derhalve een beter doelwit voor NSAIDs - dan COX-1. Erwerd besloten het racemisch mengsel alsmede de individuele enantiomeren vanflurbiprofen te onderzoeken op hun prostaglandinesynthese remmende activiteitzowel intra- als extra-oculair, en zowel op COX-1 als op COX-2.
In hoofdstuk 2 wordt het gekozen buffer-systeem beargumenteerd. Ofschoon hetoog, speciaal de neushoek, de oogleden en de huid rondom het oog gevoelig zijnvoor externe stimuli, zijn fysiologische reacties ten gevolge van afwijkingen buitende normaalwaarden van osmolaliteit of pH niet altijd duidelijk. Bij ziekte of bij chro-nisch gebruik van oogheelkundige preparaten kan dit echter meer op de voorgrondtreden. Het farmacologische agens in een oogdruppel kan, wanneer niet goedopgelost, een prikkelende of branderige sensatie veroorzaken, hetgeen weer kanleiden tot traanproductie, soms zelfs tot bloedingen of tot gevaarlijke knipperreflex-en gedurende een operatieve ingreep. Overmatige traanproductie leidt totongewenste verdunning van de oogdruppel en zelfs tot het uitspoelen van hetgeneesmiddel. De individuele gevoeligheid kan variëren en de fysiologische waar-den van het traanvocht kunnen fluctueren afhankelijk van de gezondheidsstatusvan het betreffende oog. Irritatie van het oog moet echter onderscheiden wordenvan een allergische reactie. In het laatste geval dient een ander farmacologischagens gekozen worden.
Niet-irriterende oogdruppels moeten in principe voldoen aan eisen betreffende:(1) steriliteit (2) isotoniciteit en (3) pH waarde. Steriliteit is van eminent belang bijtoepassing van oogdruppels in een beschadigd oog. Wanneer de oplossing isotoonis met het traanvocht, zullen irritaties en reacties van het oog tot een minimumbeperkt blijven. De pH waarde van de formulering is van groot belang, zowel voorde stabiliteit gedurende opslag als voor het handhaven van fysiologische condities
Samenvatting
132

in het oog. Gedurende opslag kunnen hydroxyl ionen, afkomstig uit het glas van deoogdruppeldispenser, de pH omhoog brengen hetgeen de stabiliteit van het farma-cologisch agens in gevaar kan brengen. Aan de andere kant heeft traanvochtslechts een beperkte buffercapaciteit.
Bij de keuze voor een buffer ten behoeve van de bereiding van een flurbiprofenoogdruppel moest met de volgende gegevens rekening gehouden worden: (1) flur-biprofen is instabiel bij hoge pH, (2) de oplosbaarheid in waterige oplossingen isslecht bij pH waarden lager dan 7, (3) de normale pH waarde van traanvocht is 7,4en (4) de tolerantie van de patiënt ligt tussen pH 6,6 tot 7,8.
Op basis van de ervaring met de indomethacine oogdruppel werd voor het berei-den van de S(+) flurbiprofen oogdruppels gekozen voor een fosfaatbuffer (pH 7,4).Het specialité Ocuflur® (racemisch flurbiprofen natrium) is bereid in een citraat-buffer van pH 6,45. Dit werd door ons echter als een ongeschikt buffersysteembeschouwd, omdat voor een citraatbuffer een bovenste grens in buffercapaciteitvan pH 6,5 bekend is. Een zelfde conclusie wordt overigens ook getrokken in hetUnited States patent 4.996.209, waar een fosfaatbuffer wordt gemeld voor desamenstelling van een anti-inflammatoire S(+) flurbiprofen oogdruppel. In dezeoogdruppel komen echter ook andere componenten voor. De samenstelling van deoogdruppel toegepast in dit proefschrift is vrij van die andere componenten.
In hoofdstuk 3 wordt de stabiliteit van de formulering onderzocht. Van het actieveS(+) enantiomeer van flurbiprofen, is een stereoselectieve, ballastvrije oogdruppelgeformuleerd in een concentratie van 0,015%. Analyse per capillaire zone electro-forese techniek toonde een houdbaarheid aan van 4 jaar bij kamertemperatuur. Deprostaglandine-synthese remmende activiteit van S(+) flurbiprofen, gemeten in eenhomogenaat van runder iris/corpus ciliare weefsel, bleek drie jaar na bereidingonveranderd.
Hoofdstuk 4 beschrijft de farmacologische activiteit van verschillende flurbiprofenbereidingen in runder iris/corpus ciliare homogenaten. Concentratie-respons cur-ven zijn gemeten voor S(+) flurbiprofen, R(-) flurbiprofen en het racemisch mengselbetreffende remming van PGE2 productie door COX-1. Een significant onderscheidin remmende werking werd vastgesteld tussen de enantiomeren, waarbij S(+) flur-biprofen honderd maal actiever bleek te zijn dan R(-) flurbiprofen. Geconcludeerdkon worden dat S(+) flurbiprofen het actieve farmacologische agens is datonderdeel zou moeten uitmaken van een oogdruppel oplossing ten einde deprostaglandinesynthese te remmen.
In hoofdstuk 5 wordt beschreven hoe, met toepassing van de methode vanPatrignani et al., in humaan bloed, verschillen aangetoond werden in de remmendeactiviteiten van S(+) flurbiprofen, R(-) flurbiprofen en racemisch flurbiprofen op deisoenzymen cyclooxygenase-1 en cyclooxygenase-2. COX-1 activiteit werd geme-ten aan de hand van TxB2 (de stabiele metaboliet van TxA2) geproduceerd door
Samenvatting
133

bloedplaatjes. COX-2 activiteit werd gemeten met behulp van PGE2 productie doormonocyten na inductie van dit enzym door lipopolysaccharide (LPS). De stereose-lectiviteit van S(+) flurbiprofen ten opzichte van R(-) flurbiprofen, uitgedrukt als dereciproke waarde van de ratio van de concentraties die 50% remming geven (IC50),liepen uiteen van 340 voor COX-1 tot 56 voor COX-2. De selectiviteit vanracemisch flurbiprofen voor COX-1 versus COX-2 was 16-voudig.
In hoofdstuk 6 is de interactie van S(+) flurbiprofen met COX-1 versus COX-2 inde humane iris bestudeerd. Na voorbehandeling met LPS kwam een aanzienlijkehoeveelheid COX-2 immunoreactiviteit naar voren. Verrassenderwijs toonde S(+)flurbiprofen een 3600-voudig hogere potentie tot remming van COX-1 versus COX-2. Verder bleek de gevoeligheid van humaan iris COX-1 voor S(+) flurbiprofen 70maal hoger dan de gevoeligheid van COX-1 in menselijk bloed.
In hoofstuk 7 wordt de verdeling van een flurbiprofen analogon over het menselijkoog onderzocht. Technetium gelabeled diflunisal, een chemisch op flurbiprofengelijkend NSAID - gefluorineerd met eveneens een bifenyl ring - werd toegepast omde COX-activiteit in de interne structuren van het oog te kunnen visualiseren. Descintigrafische resultaten van dit gelabelde farmacon werden vergeleken met dievan de instillatie van eenzelfde volume en activiteit pertechnetaat anion.
Een hoeveelheid van 3% van het geinstilleerde technetium gelabelde diflunisal konin het oog worden getraceerd. COX-activiteit werd duidelijk gevisualiseerd in deregio van de iris. In dit onderzoek werd diflunisal toegepast omdat de labelingsef-ficiency van S(+) flurbiprofen aan de (te) lage kant was (hoofdstuk 8). R(-) flurbipro-fen leverde weliswaar een betere labeling op, maar farmacologisch is dit het inac-tieve enantiomeer (hoofdstukken 5 en 6).
In het laatste hoofdstuk is het voorkomen van een splice variant van COX-1mRNA in de menselijke iris onderzocht als een mogelijke verklaring voor de hogeaffiniteit van S(+) flurbiprofen gerapporteerd in hoofdstuk 6. Inderdaad werd eenalternatieve splice variant (SV) van COX-1 aangetroffen in iris weefsel afkomstigvan 3 patiënten. Echter, dezelfde splice variant werd ook gevonden in bloedcellenafkomstig van 4 vrijwilligers. De hoeveelheid COX-1SV aanwezig in de iris was nietsignificant verschillend van de hoeveelheid aanwezig in bloed cellen, hetgeenimpliceert dat daarmee het verschil in IC50 van S(+) flurbiprofen tussen humane iris(0,8 nM) en humaan bloed (56 nM) niet kan worden verklaard.
Samenvatting
134

LIST OF PUBLICATIONS

1. van Sorge AA, Wijnen PH, van Delft JL, Carballosa Coré-Bodelier VMW, vanHaeringen NJ. Flurbiprofen, S(+), eyedrops: formulation, enantiomeric assay,shelflife and pharmacology. Derived from Pharm World Sci 1999;21:91-5.
2. Sorge van AA, Delft van JL, Bodelier VMW, Wijnen PH, Haeringen van NJ.Specificity of flurbiprofen and enantiomers for inhibition of prostaglandin syn-thesis in bovine iris/ciliary body. Prostaglandins Other Lipid Mediat1998;55:169-77.
3. Haeringen van NJ, Sorge van AA, Delft van JL, Carballosa Coré-BodelierVMW. Flurbiprofen and enantiomers in ophthalmic solution tested as inhibitorsof prostanoid synthesis in human blood. J Ocular Pharmacol 2000;16:345-52.
4. Haeringen van NJ, Sorge van AA, Carballosa Coré-Bodelier VMW. Constitutivecyclooxygenase-1 and induced cyclooxygenase-2 in isolated human iris inhib-ited by S(+) flurbiprofen. J Ocular Pharmacol 2000;16:353-61.
5. Sorge van AA, Etten van RJ, Rehmann CJ, Rijnders AJM, Haeringen van NJ.99mTc-Diflunisal and the human iris: topical application reveals localization. JOcular Pharmacol 2002;18:185-195.
6. Sorge van AA, Ruiken I, Janssen HWM, Haeringen NJ. S(+) flurbiprofen andR(-) flurbiprofen. 99mTc-labeling reveals difference in stereochemistry.Enantiomer; accepted pending suitable revision.
7. Dröge MJ, van Sorge AA, van Haeringen NJ, Quax WJ, Zaagsma J. Alternativesplicing of cyclooxygenase-1 mRNA in the human iris. Submitted.
List of publications
136

DANKWOORD

DANKWOORD
De wijze waar op dit proefschrift tot stand is gekomen is voor menigeen onbegrij-pelijk. Met slechts ƒ 1800,- aan "venture capital", verkregen via de SWOR vanziekenhuis Rijnstate, lijkt dit een onmogelijke zaak. Het kon alleen maar lukkendoor de enthousiaste, belangeloze medewerking van velen. Hierdoor loop ik hetrisico, dat ik in dit dankwoord iemand kan vergeten en daar bied ik bij voorbaat almijn welgemeende excuses voor aan.
Door mijn komst naar Arnhem kwam ik samen te werken met mijn collega's JhrE.B.L.M. van Nispen tot Pannerden (St Elisabeth's Gasthuis; EG) en J.C. KutschLojenga (Gemeente ziekenhuis). Beiden waren gedreven ziekenhuisapotheker metname door de directe lijnen tussen de kliniek en de apotheek. Hier bouwde ikverder aan mijn kennis en leerde ik nog meer in te spelen op vragen uit de kliniek,zowel verpleegkundig, organisatorisch als medisch-farmaceutisch. Het contact metde medici was zeer veelvuldig en vaak informeel, vooral in het EG waar een geza-menlijk koffiedrinken de onderlinge contacten bevorderde. Tijdens één van dezecontacten kwam dr J.P. (Paul) de Haas, oogarts, met de vraag of wij een preparaatkonden bereiden, dat nog niet commercieel beschikbaar was, maar volgens de li-teratuur wel van groot nut zou zijn bij de nabehandeling van patiënten, die eenstaaroperatie hadden ondergaan. Een kolfje naar de hand des ziekenhuisapothe-kers! Dit leidde tot de ontwikkeling van de indomethacine oogdruppels.
Het was evenwel zaak, dat een en ander ook onderbouwd werd en al spoedig vielde naam van collega Nico van Haeringen, traanspecialist van wereldfaam en ver-bonden aan het IOI (Interuniversitair Oogheelkundig Instituut) gelokaliseerd "onder"het AMC, te Amsterdam alsmede thuis aan het LUMC te Leiden. Na diens farma-cologische onderbouwing van de indomethacine oogdruppels, volgde een publi-catie en werd deze oogdruppel uiteindelijk standaard opgenomen in hetFormularium der Nederlandse Apothekers (FNA).
Na afloop van dit projekt verklaarde Nico zich bereid om in de toekomst mee tewerken aan het farmacologisch onderbouwen/onderzoeken van eventueel nieuw teontwikkelen oogdruppels. Het zou evenwel tot 1991 duren alvorens wij weer con-tact zouden hebben.
Naar aanleiding van vragen en opmerkingen uit het farmaceutische en medischeveld was inmiddels gebroed op een nieuwe NSAID oogdruppel. Het "oog viel" opflurbiprofen en de eerste proefnemingen volgden spoedig. Onze apothekers-assi-stenten en niet minder de vele bijna-apotheker stagiaires, wil ik hierbij hartelijkdanken voor alle inspanningen die zij leverden om steeds weer een en ander tebereiden, te steriliseren enzovoort. Het was niet altijd even makkelijk, zeker niet ineen tijd van fusieperikelen. Ook de analisten van ons farmaceutisch-toxicologischlaboratorium wil ik dank zeggen voor het oneindige geduld dat opgebracht werd om
138
Dankwoord

toch weer een en ander te analyseren. Het noemen van namen gaat hierbijmogelijk te ver, zo veel zijn het er geweest; een ieder heeft er zonder twijfel "lastvan gehad".
Voor het farmacologisch onderzoek volgden wederom vele paracenteses in dekonijnenstallen van het LUMC nu met flurbiprofen en diens enantiomeren als far-macologisch agens. Veel dank ben ik hierbij verschuldigd aan Jan van Delft, eenexpert op dit gebied. Ook Ed Barthen wil ik danken. Steeds stond hij klaar om onste helpen, ook bij het verkrijgen en behandelen van humaan irismateriaal.
Door renovatie van de dierenstallen van het LUMC werd het werkterrein ver-plaatst naar het IOI te Amsterdam alwaar nog enige experimenten met konijnen vol-gden. Dank zij toestemming van de direkteur van het IOI, Prof Paulus de Jong,mocht ik als gast-medewerker aldaar verder gaan. Hiervoor ben ik jou, Paulus, zeererkentelijk. Spoedig evenwel werd overgestapt op de human whole blood assay.Deze techniek werd opgedaan tijdens een internationaal congres te Cannes en hetwas weer aan het eminent biochemisch inzicht en jouw praktische ervaring, Nico,dat wij hiermee aan de slag konden gaan. Uiteraard mijn hartelijk dank hiervoor.
Door deze veranderde werkwijze verplaatsten de proefnemingen zich naar hetbiochemisch laboratorium, alwaar Valérie Bodelier als voortreffelijk analiste devoortgang van het onderzoek waarborgde. Ik dank haar bij deze voor het vele werkdat met toewijding en expertise is verricht.
Naarmate de proefnemingen vorderden werd ook gedacht de rundermatrix te ver-vangen door die van de mens. Hierin heeft Dr Liesbeth Pels ons bijgestaan en daarben ik haar zeer erkentelijk voor.
Voorafgaand en parallel aan deze ontwikkelingen werd ook de farmaceutischekwaliteit van de flurbiprofen oogdruppels onderzocht. Toen er in de wetenschap-pelijke bijlage van het NRC Handelsblad een artikel over "Spiegelbeelden scheidenmet een membraan" verscheen van de hand van onderzoekers verbonden aan hetlaboratorium van AKZO NOBEL Central Research, Dr Ir J.T.F. Keurentjes en Ir E.van Andel, waarin een nieuwe methode werd besproken om zuivere stereoiso-meren te bereiden, werd besloten contact met hen op te nemen om te bezien ofdeze methode voor de ziekenhuisapotheek bruikbaar kon zijn en dan in het bijzon-der voor de bereiding van flurbiprofen enantiomeren. Andere enantiomeren van far-maceutisch belang, zoals bupivacaine en ketamine, werden ook tot de mogelijkhe-den gerekend. Uit dit contact volgde een afspraak met collega Mw Dr M. Lelouxvoor verdere bespreking. Ten leste werd contact gelegd met het laboratorium voorCentral Research waar Peter Wijnen toestemming verleende de houdbaarheid-sproeven van de flurbiprofen isomeren aldaar te verrichten. Voor deze medewerk-ing zijn wij AKZO NOBEL, en Peter Wijnen in het bijzonder, zeer erkentelijk. Het bij-zondere is natuurlijk dat dit heeft kunnen plaatsvinden bij een multinational en ooknog in de stad Arnhem.
139
Dankwoord

Tijdens deze periode zijn eveneens congressen bezocht en voordrachtengehouden over de vorderingen, die gemaakt waren. Dit leidde tot het contact metDr Johan Bours, eiwitexpert op oogheelkundig gebied, die veel van zijn kennishierover heeft overgebracht. Voor deze stimulerende gesprekken, Johan, ben ik jeveel dank verschuldigd.
Al dit werk was zeker niet mogelijk geweest als mijn (computer)vriend van deeerste uren, Lex Dreves, mij niet geholpen had bij het leren omgaan met de nieuwgeintroduceerde techniek van de computer. Ondanks zijn handicap van de ziektecystic fibrosis, kon hij het opbrengen om mij hierbij met raad en daad bij te staan.Het was dan ook een enorme set-back hem op 30 jarige leeftijd te moeten ver-liezen. Via zijn ouders wil ik Lex alsnog hartelijk danken voor zijn ondersteuning.Ook mijn andere (computer)vrienden, Max Wolff en Carla Hulsewé, wil ik hartelijkdanken voor de vele fijne gesprekken over het vorderen van het werk en het uit-zoeken van de juiste computer-configuratie, zodat dit proefschrift tot een goedeinde kon worden gebracht.
Vermeldenswaard en zeker een compliment, verdient de staf van onze biblio-theek. De dames Mieke Noordegraaf, Erna Altena, Anje van den Berg en Tanja vanBon zijn van grote klasse in het opzoeken en opvragen van de gezochte literatuur.Piet Huggers van het laboratorium voor pathologie dank ik voor het professioneelbewaren van de iris monsters alvorens deze te toe te passen voor onderzoek.
Voorts wil ik ook de directie van ons ziekenhuis bedanken voor de mogelijkhedendie onze kliniek heeft voor het doen van wetenschappelijk onderzoek. De staf encollegae ziekenhuisapothekers en Guus Essink in het bijzonder, wil ik danken voorde direkte dan wel indirekte steun bij het werk zodat ik een en ander tot een goedeinde kon brengen.
De oogartsen van ziekenhuis Rijnstate wil ik hartelijk danken, dat zij steeds open-stonden voor nieuwe ideeën op het gebied van de farmaceutische oogheelkunde.Aan Maarten Jonkers kan ik nu eindelijk de prachtige bijbels van de ophthalmolo-gie teruggeven! Maarten, hartelijk dank voor je geduld in deze.
Ook de paranimfen, Rob Weber en Arnold Lombarts wil ik hartelijk danken, voorhun spontane toezegging te helpen daar waar mogelijk. Door deze promotie is ein-delijk de cirkel rond en kunnen we alledrie terugzien op een optreden als paranimfbij elkaars promotie.
Dr J.C. Verhoef, beste Hans, jou zou ik willen bedanken voor de vele uren die wijsamen hebben besteed aan het hoofdstuk over de achtergronden van de gebruik-te buffer. Jouw kennis over de electrochemie nodigt uit om samen nog een hoofd-stuk te schrijven over een andere benadering van de cyclooxygenase gemedieerdereactie. Hartelijk dank voor de door jou geleverde inspanning en je toezegging tewillen opponeren. Bovendien bracht je mij in 2001 in kontakt met Willy H.J.Boesten, corporate scientist (scheikundige èn uitvinder) bij DSM Research, die
140
Dankwoord

bereid was een search te doen naar artikelen over de synthese van enantiomerenen die van flurbiprofen in het bijzonder. Spoedig volgde een dikke stapel literatuur,alwaar tot mijn verbazing ook een patent in terug te vinden was over het gebruikvan S(+)flurbiprofen, en wel opgelost in fosfaatbuffer. Bij deze wil ik hem hiervoorhartelijk danken.
Ook wil ik een woord van dank uitbrengen aan Dr Hector Knight van de firmaMallinckrodt. De bespreking van de resultaten van hoofdstuk 8 aangaande de label-ing van de flurbiprofen enantiomeren heb ik bijzonder gewaardeerd. Een opzetnaar een volgend onderzoek maar dan met labeling middels de IsoLink® technieklijkt veelbelovend.
Tot slot van deze historisch getinte opbouw van mijn dankwoord wil ik nogmaalsNico van Haeringen hartelijk danken voor de wetenschappelijke begeleiding. Jeimmer rustige maar trefzekere inschatting van het werk hebben bijgedragen aan devoltooiing van dit opus. Ook Eelco van Nispen wil ik nogmaals bedanken:reikhalzend zag hij uit naar de afronding van dit project.
De Hoogleraren Prof Dr J.E.E. Keunen (LUMC), Prof Dr M.D. DeSmet (AMC),Prof. Dr. J.M.M. Hooymans (Academisch ziekenhuis Groningen), Prof. Dr. W.Timens (Academisch ziekenhuis Groningen) en Prof. Dr. F Muskiet (Academischziekenhuis Groningen) alsmede Mw A. Brugman (Academisch ziekenhuisGroningen) en Dr. M. Elferink (Rijks Universiteit Groningen) wil ik hartelijk dankenvoor hun medewerking bij het tot stand komen van het laatste hoofdstuk. In het bij-zonder wil ik nog bedanken Drs Melloney Dröge wier conscientieus werk het laat-ste hoofdstuk praktisch mogelijk heeft gemaakt.
De leden van de beoordelingscommissie, Prof Dr P.T.V.M. de Jong, Prof DrJ.R.B.J. Brouwers, en Prof Dr H.V. Wikström wil ik bedanken voor hun bereidheidhet manuscript te beoordelen.
De laatsten in de lange rij van personen, die ik wil bedanken voor hun bijdrageaan de tot standkoming van dit proefschrift, zijn de hoogleraren, Prof Dr H.W.Frijlink, Prof Dr W.J. Quax en Prof Dr J. Zaagsma. Zij kwamen bij mijn eerstebezoek in de zomer van 1999 tot de conclusie dat dit werk vatbaar was voor eenpromotie.
In het bijzonder wil ik hier de unieke begeleiding van Prof Dr J. Zaagsma ver-melden. Beste Hans, waar op (niet-academische, perifere) afstand een en andertoch wel moeilijk kan zijn is het je gelukt een bijzondere band op te bouwen. Alsziekenhuisapotheker, onkundig van de gang van zaken op het academisch pro-motievlak, heb ik het bijzonder gewaardeerd een zo plezierige ondersteuning enbejegening te mogen ontvangen. De vele doorhalingen, correcties en voorstellenmiddels het "ouderwetse" correctiepotlood waren altijd bestemd om tot een betereformulering te komen. Ook de meer moderne middelen als fax en e-mail zijn inten-
141
Dankwoord

sief gebruikt. Je organisatietalent heeft het mogelijk gemaakt, dat deze promotienog dit jaar heeft kunnen plaats vinden. Hiervoor mijn oprechte dank.
Ter afsluiting wil ik natuurlijk mijn ouders bedanken, die mij de mogelijkheidhebben geboden een universitaire scholing te doorlopen, hetgeen in die tijd nietaltijd vanzelfsprekend was.
En last but not least gaat mijn grote dankbaarheid uit naar Aty en de kinderen diezich afvroegen of dit allemaal wel de moeite waard was en het desondanks tochmet groot enthousiasme hebben gesteund. Een historisch analogon is hier op zijnplaats:
"Quosque tandem A3aan abutere patientiam nostram"?s. Cicero
142
Dankwoord

CURRICULUM VITAE

CURRICULUM VITAE
Adriaan Alastair van Sorge (geboren 28 oktober 1944) doorliep het GereformeerdGymnasium (ß) gelegen aan de Keizersgracht te Amsterdam. Na de vervulling vanzijn dienstplicht startte hij in 1965 met de studie Farmacie aan de Universiteit vanAmsterdam. Na voltooiing van deze studie met het doctoraal examen werd in 1972het apothekers examen met goed gevolg afgelegd. Een korte periode was hijwerkzaam in de officiene apotheek maar al snel werd gekozen voor een baan in defarmaceutische industrie (R&D; Philips Duphar).
Aangestoken door enthousiaste artikelen over de klinische farmacie in deVerenigde Staten van de hand van collega Armbrust, diende hij een aanvraag in bijde University of California, School of Pharmacy, te San Francisco voor het doorlopenvan een Postdoctoral Pharm D residency programme in Clinical Pharmacy (1973-1974). Deze aanvraag werd gehonoreerd. Tijdens deze studie werd eveneens ken-nisgemaakt met de klinische farmacologie onder leiding van Dr. K.L. Melmon en Dr.H.F. Morrelli. Het geheel werd afgesloten met het predikaat Pharm D.
Na terugkeer uit de Verenigde Staten volgde hij de opleiding tot ziekenhuis-apotheker in de Apotheek Haagse Ziekenhuizen. Tijdens deze opleiding maakte hijkennis met de interne school van Dr F. Kalsbeek (Leyenburg ziekenhuis) en werk-te onder diens leiding mee aan de tweede druk van Materia Medica Selecta ("Eenpraktische handleiding voor het rationeel kiezen en voorschrijven van geneesmid-delen"). Tevens werd de farmacotherapeutische zorg ten behoeve van hetWesteinde Ziekenhuis aan de auteur toevertrouwd.
In 1976 werd de opleiding tot ziekenhuisapotheker afgesloten met een registratieonderwerp betreffende de remming van prostaglandinesynthese door niet steroideanti-inflammatoire middelen. Het werkzame leven als ziekenhuisapotheker inArnhem werd aangevangen met een full-time functie verdeeld over het StElisabeth's Gasthuis (hoofd Jhr E.B.L.M. van Nispen tot Pannerden) en hetGemeente Ziekenhuis (hoofd J.C. Kutsch Lojenga). Het diploma "Bevoegdheidbeheer C-laboratorium" niveau 3 werd in 1979 behaald.
Vanaf 1981 tot de dies finalis maakte van Sorge deel uit van de Geneesmiddelen-commissie van het Ministerie van WVC, eerst als lid en vervolgens als plaatsver-vangend voorzitter.
De auteur is lid geweest van verscheidene ziekenhuisgebonden commissies.Vanaf 1987 fungeerde de auteur, met een kleine onderbreking, als opleider vanapothekers in opleiding tot ziekenhuisapotheker.
Inmiddels waren beide ziekenhuizen gefuseerd tot ziekenhuis De Malberg, in eentwee-lokatiemodel. Met de "echte" fusie tot ziekenhuis Rijnstate in 1990, door hetsamengaan van De Malberg met het Diaconessenhuis, werd het team versterkt metcollega dr. J.S. Meulenhoff.
144
Curriculum Vitae
146

COLOR PICTURES

pH 3.5 4.0 4.5 5.0 5.5 6.0 6.5 7.0 7.2
Chapter 2. As far as flurbiprofen is concerned, the solubility in aqueous solution is proble-matic at pH values below 7.
Chapter 6, figure 1. Detection of cyclooxygenase in human iris extracts. Authentic COX-1and COX-2 peptide and 15 ml of tissue extract were spotblotted on nitrocellulose mem-brane. Cyclooxygenase was detected using immunoglobulin G specific for COX-1 or forCOX-2. With anti-COX-1, spots were observed in untreated iris, LPS-treated iris and withCOX-1 peptide. With anti-COX-2, spots were observed in LPS-treated iris only and withCOX-2 peptide.
148
Color pictures

Chapter 7, figure 6. Scintigraphic Image of the Eye Surface and the Lacrimal Sac 160 sec-onds after Application of 99mTc Diflunisal (frame 16). Graph represents counts versus timefor whole session.
Chapter 7, figure 7. Scintigraphic Image of the Area of the Iris and the Lacrimal Sac 1170seconds after Application of 99mTc-Diflunisal (frame 117). Graph represents counts versustime for whole session.
149
Color pictures

Chapter 7, figure 8. Difference in Scintigraphic Exposure between Pertechnetate (left) and99mTc-Diflunisal
Chapter 7, figure 9. Display of Counts Per Pixel for 99mTc-Diflunisal in the Area of Pupil, Irisand Conjunctiva
150
Color pictures
99mTc-Diflunisal scintigraphyin selected eye structures
0,00
0,50
1,00
1,50
2,00
2,50
3,00
0 200 400 600 800 1000 1200
time (seconds)
coun
ts p
er p
ixel
pupil
iris
conjunctiva

ADDENDUM

In deze tijd werd, ondanks de hectiek van die jaren, de grondslag gelegd voorverder onderzoek met oogdruppels. Ook het kontakt met collega Dr Nico vanHaeringen, zo behulpzaam geweest bij de farmacologische onderbouwing van deinmiddels landelijk bekende indometacine oogdruppels FNA, (samen met collegaVan Nispen in 1981 ontwikkeld) werd weer aangehaald. Er werd begonnen metfarmacologisch onderzoek in konijnen, maar dan met flurbiprofen oogdruppels.Het onderzoek heeft zich in de beginjaren afgespeeld in het Leids UniversitairMedisch Centrum. Door vernieuwing van de konijnenstallen werd het onderzoekverplaatst naar het Interuniversitair Oogheelkundig Instituut, IOI, alwaar de auteurmet toestemming van Professor Paulus de Jong, direkteur van het IOI, als gast-medewerker werkte.
De farmaceutische analyses van de S(+) flurbiprofen oogdruppels werden ver-richt in het laboratorium van de apotheek van ziekenhuis Rijnstate alsmede in delaboratoria van AKZO-NOBEL te Arnhem (P.H. Wijnen).
Voor het nucleaire onderdeel werd enthousiaste medewerking verleend door deafdeling Nucleaire Geneeskunde van Ziekenhuis Rijnstate (nucleair geneeskundi-gen A.J.M. Rijnders en C.J. Rehmann).
In de zomer van 1999 werd contact gezocht met de huidige promotores, de pro-fessoren W.J. Quax, J. Zaagsma en H.W. Frijlink, om te bezien of een promotie totde mogelijkheden behoorde. Dit contact leidde tot het laatste deel van het onder-zoek dat te Groningen werd verricht, alwaar de professoren Zaagsma en Quaxalsmede collega Drs Melloney Dröge de aanzet gaven tot de uitwerking van hetlaatste hoofdstuk.
145
Curriculum Vitae