
University of Groningen Infection prevention in intensive care ......RIJKSUNIVERSITEITTE GRONINGEN...
154
University of Groningen Infection prevention in intensive care. Infection prevention in multiple trauma patients by selective decontamination of the digestive tract (SDD) Stoutenbeek, Christiaan Peter IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 1987 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): Stoutenbeek, C. P. (1987). Infection prevention in intensive care. Infection prevention in multiple trauma patients by selective decontamination of the digestive tract (SDD). [s.n.]. Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons the number of authors shown on this cover page is limited to 10 maximum. Download date: 22-07-2021
Transcript of University of Groningen Infection prevention in intensive care ......RIJKSUNIVERSITEITTE GRONINGEN...

University of Groningen
Infection prevention in intensive care. Infection prevention in multiple trauma patients byselective decontamination of the digestive tract (SDD)Stoutenbeek, Christiaan Peter
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:1987
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Stoutenbeek, C. P. (1987). Infection prevention in intensive care. Infection prevention in multiple traumapatients by selective decontamination of the digestive tract (SDD). [s.n.].
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 22-07-2021

INFECTION PREVENTION IN MULTIPLE TRAUMA PATIENTS BY SELECTIVE DECONTAMINATION OF THE DIGESTIVE TRACT

CIP-GEGEVENS KONINKLIJKE BIBLIOTHEEK, DEN HAAG
Stoutenbeek , Christiaan Peter
Infection prevention in multiple trauma patients by selective decontamination of the digestive tract I Christiaan Peter Stoutenbeek . - [s. I . : s .n .] (Groningen : Van Denderen) Proefschrift Groningen. - Met l i t . opg. - Met samenvatting in het Nederlands. ISBN 90-9001 736-4 SISO 605.11 U DC 616.9(043 .3) Trefw. : infectieziekten; preventie.

RIJKSUNIVERSITEITTE GRONINGEN
INFECTION PREVENTION IN MULTIPLE TRAUMA PATIENTS BY SELECTIVE DECONTAMINATION
OF THE DIGESTIVE TRACT
PROEFSCHRIFf
tcr vcrkrijging van hct doctoraat in de Gcnccskundc
aan de Rijksuniversiteit tc Groningcn
op gczag van de Rector Magnificus Dr. E. Bleumink
in het opcnbaar tc verdedigen op wocn�dag 8 juli 1 987
de' namiddag� le 2.45 uur precies
door
CHRISTI AAN PETER STOUTEN BEEK
geboren tc Utrecht
1987 DRUKKERIJ VAN DENDEREN B.V.
GRON ING EN

Promotores : Prof. Dr. G. F. Karliczek
Referent Prof. Drs. B. B innendij k Dr. H.K . F. van Saene

Aan mijn ouders Voor Margot , Astrid en Robin

ABBREVIATIONS
ACTH AIS ARDS AT III CABG CDC CI GNB GVN HTI ICU ISS MBC M IC PEEP PPM PTA RES RTI SOD SD SEM UTI
Ad reno Corti co Tropic Hormone Abbreviated Injury Scale Adult Respiratory Distress Syndrome Anti-thrombine I I I Coronary Artery Bypass Grafting Center for Disease Control Colonisation Index Gram-Negative Bacilli Gentamicin + Vancomycin + Nystatin Hospital Trauma Index Intensive Care Unit Inj ury Severity Score Minimal Bactericidal Concentration Minimal Inhibitory Concentration Positive End-Expiratory Pressure Potentially Pathogenic Microorganisms Polymyxine E + Tobramycine + Amphotericin B Reticule Endothelial System Respiratory Tract Infection Selective Decontamination of the Digestive tract Standard Deviation Standard Error of the Mean Urinary Tract Infection

TABLE OF CONTENTS
ACKNOWLEDGEMENTS
CHAPTER I AN INTRODUCTION TO THE INFECTION PROBLEM IN THE ICU
CHAPTER 2
THE EFFECT OF SELECTIVE DECONTAMINATION OF THE DIGESTIVE TRACT ON COLONISATION AND INFECTION RATE IN MULTIPLE TRAUMA PATIENTS ......................................... 1 9
I ntensive Care Med 10 : 1 85 ( 1 984)
CHAPTER3
THE PREVENTION OF SUPERINFECTION IN MULTIPLE TRAUMA PATIENTS
J Antimicrob Chemother 1 4(8) :203 ( 1 984)
CHAPTER4
THE EFFECT OF O ROPHARYNGEAL DECONTAM INATION USING TOPICAL NON-ABSORBABLE ANTIBIOTICS ON THE INCIDENCE OF NOSOCOMIAL RESPIRATORY TRACT
33
INFECTIONS IN MULTIPLE TRAUMA PATIENTS ..................... 45 J Trauma 27:357 ( 1 987)
CHAPTERS
EFFECT OF ORAL NON-ABSORBABLE ANTIB IOTICS ON THE EMERGENCE OF RESISTANCE IN AN INTESIVE CARE UNIT
J Antimicrob Chemother 1 9:5 1 3 ( 1 987)
CHAPTER6
THE I MPACT OF AN INTEGRATED TRAUMA SERVICE ON THE LATE MORTALITY FROM MULTIPLE ORGAN FAILURE
59
AND SEPSIS IN SE VE RELY INJURED PATIENTS . . . . . . . . . . . . . . . . . . . . . . 69

CHAPTER7
NOSOCOMIAL GRAM-NEGATIYE PNEUMONIA IN CRITICALLY ILL PATIENTS. A 3-year experience with a novel therapeutic regimen
Intensive Care Med 12:419 (1986)
CHAPTERS
GENERAL DISCUSSION
87
95
SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 05
SAMENV A TTING . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 111
REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 117
CURRICULUM VITAE 127
APPENDIX
PROTOCOL INFECTION PREVENTION IN THE ICU . .. . .. . ... . . . . . . .. 133

ACKNOWLEDGEMENTS/VOORWOORD
Bij het tot standkomen van dit proefschrift was de hulp van vele mensen onontbeerlijk ; met name wil ik h ierbij noemen :
Prof. Dr. G . F. Karliczek , bestc Gerhard , ik ben je zeer erkentelijk voorde wijze waarop je mij in moeilijke momenten met raad en daad terzijde hebt gestaan. Het stem! mij daarom tot grote vreugde dat je mijn promotor hebt wil len zijn .
Prof. Ors. B . Binnendijk , beste Ben , het was een voorrecht met jou en jouw afdeling te mogcn l.amenwerken . Hoewel dit af en toe niet zonder, soms flamboyante , discussies verliep, heeft het geresulteerd in een grote mate van integratie van de anesthesie en intensive care in de behandeling van de polytraumatise . Met name wil ik je ook danken voor de vrijheid en het vertrouwen die je me bij het onderzoek altijd hebt gegeven .
Dr. H . K. F . van Saene , beste Rick , jou ben ik veel verschuldigd. Jarenlang hebben wij intensief en met veel enthousiasme samengewerkt aan dit onderzoek . I k denk met veel genoegen terug aan de vele avonden , dat wij de gegevens aan het uitwerken waren en theorieen langzamerhand gestalte kregen ; we hebben vee l plezier gehad. Ik hoop dat ook in je huidige positie als senior lecturer aan de universiteit van Liverpool , we in de gelegenheid zullen zij n onze samenwerking voort te zetten . Verde r wil ik hier nog met name vermelden de buitengewone wijze waarop j ij gestalte hebt gegeven aan de klin ische bacteriologic in de Intensive Care .
Prof. Dr. D. Langrehr, het instituut voor Anesthe!.iologie en Intensive Care heeft sinds Uw komst naar Groningen een grote bloei doorgemaakt , en ik prijs mij gelukkig dat ik in die tijd mijn opleiding tot anesthesioloog heb kunnen voltooien.
Dr. D. R. Miranda , beste Dinis, acht jaar tang heb ik met jou mogen werken aan de opbouw van de Intensive Care . Deze jaren zijn voor mij van onschatbare waarde geweest voor mij n vorming tot intensivist. Ook ben ik je erkentelijk voor de wijze waarop je je hebt ingespannen om dit onderzoek mogelij k te maken .
Durk Zandstra, Hans Barns en de collega's van de Intensive Care en de ICdienstgroep (D 1 -groep ), j ull ie persoonlijke betrokkenheid en de bereidheid van ieder van j ul l ie om een groot dee I van je vrije tijd in de Intensive Care te besteden , heb ik altijd als zeer bijzonder ervaren . Alleen h ierdoor was het mogelij k de Intensive Care 24 uur per dag effectief te laten functioneren . De grote onderlinge collegialiteit en vriendschap is a ltijd bijzonder stimulerend geweest . Ook ben ik j ull ie dankbaar voor de loyale medewerking aan het onderzoek .
Gerda Manschot en verpleegkundigen van de In tensive Care , zonder jul l ie medewerking was dit onderzoek ten ene male onmogelij k geweest. De bereidheid aan steeds nieuwe onderzoekingen mee te werken, het enthousiasme en de nauw-

keurigheid waarmee j ul l ie hebben geholpen , is van doorslaggevend belang geweest voor het welslagen ervan. Henderika Hoekstra en de laboranten van de dependance microbiologie , jullie wit ik danken voor het vele werk dat jullie gedaan hebben en de grote kundigheid en precisie waarmee jul l ie het hebben uitgevoerd.
Marjan Laseur en haar collega's van de apotheek. wit ik bedanken voor hun loyale medewerking en onovertroffen accuratesse.
Annemarie de Smet , Liesbeth Jordans. Elike ten Berge , Ernst van der Poe t , Nienke ten Kate . Klaas Hoogenberg. Sigrid Schi l te. ik w i t van deze gelegenheid gebruik maken om jullie te bedanken voor het vele werk en de grote hoeveelheid tijd die j ul l ie , geheel belangeloos, in dit onderzoek geinvesteerd hebben bij het verzamelen van de k l in ische data. het invoeren in de computer en het verwerken van de gegevens. Ik hoop dat deze besteding van je wachttijd ook voor jul l ie nog zijn vruchten zal afwerpen .
Verder w i l ik bedanken . Wil Noordik voor haar secretariele hulp en voor het maken van i l lustraties, Ian Jenkins en Gee rt Kinkhorst voor de taalkundige correctie van het manuscript , Douwe Suiter voor het ontwerpen van de omslag en verder nog een ieder die heeft bijgedragen aan de tot standkoming van dit proefschrift en die hier niet bij name genoemd is.
Graag wil ik hier een woord van dank rich ten tot mij n ouders: naarmate ik ouder word , besef ik steeds meer we Ike inspanning U zich getroost heeft om vijf kinderen groot te brengen. U heeft ons geleerd dat vrij heid al leen gedragen kan worden in verantwoordelij kheid en hiervoor ben ik U nog steeds dankbaar.
Tot slot wil ik Margot , mijn echtgenote , bedanken . Dit onderzoek is steeds een gezamenlijke inspanning van ons beiden geweest. Ik bewonder je voor de wijze waarop j ij , naast je eigen werk , thuis altijd een atmosfeer van rust hebt weten te creeren , waarin a Iles moeiteloos leek te functioneren, en die de extra inspanning, die voor dit onderzoek nodig was, als vanzelfsprekend maakte . Ook wil ik je danken voor de grote interesse die je a ltijd hebt getoond i n deze studie.
Chapter 1
AN INTRODUCTION TO THE INFECTION PROBLEM IN THE ICU
THE MAGNITUDE OF THE INFECTION PROBLEM Colon isation and infection CDC-guidelines for prevention of no�ocomial infection� Conventional antibiotic policy
II M ICROORGANISMS lndigenom flora 'Community-acquired' infections 'Hospi tal-acquired' infection-;
I l l PATHOGENESIS OF CO LONISATION AND INFECTION Origin of infection : exogenous vs. endogenous Defence mechani�ms: colon isation defence and infection defence ( i ) coloni-;ation defence of the oropharyngeal cavity and gastro-intestinal
canal Altered colon isation defence of the oropharynx and gastro-intestinal tract
( i i ) colonisation defence of the respiratory. urinary tract and skin Altered colonisation defence of the respiratory and urinary tracts and the skin
( i i i ) Infection defence Altered infection defence
IV I NTESTINAL FLORA SUPPRESSION
V AIM OF THE STUDY Co-trimoxazole versus tobramycin Oral decontamination Study design Why multiple trauma patients? Control group Description of the studies

I THE MAGNITUDE OF THE INFECTION PROBLEM
The Intensive Care Unit {ICU) is intended for the treatment of patients suffering from fa ilure of one or more major vital organ systems. Many sophisticated and complex techniques have been developed for monitoring and support of re�piratory . cardiocirculatory or renal failure . However. the success of these techniques is frequently annihi lated by the desastrous occurrence of infections. The devastating effects of infection may start a downhil l spiral of multiple organ failure . which further decreases the infection defence and promotes infection, which eventually may become fatal . Infection is responsible for more than 80% of late mortality in the ICU (Fry et a l . , 1 980; Goris & Draaisma, 1 982) and the costs of added morbidity and hospital charges are overwhelming (Freeman et al . , 1 979; Haley, 1 980, 1 98 1 ). So far. relatively l i ttle progress has been made in the monitoring and treatment of failure of the complex system which provides defence against infection and which is probably the most common form of organ failure .
A nosocomial infection i s defined as an infection occurring a t least 48 h after admission to the hospital ( i . e . 'hospital-acquired infection') . In contrast to the 5% to I 0% crude nosocomial infection rate in the general ward patient (Eickhoff et al . , 1 969; Wenzel et al. . 1 976, 1 983) . infection rates in selected critical care areas may be 300% to -l00% higher (Daschner et al.. 1 982; Donowitz et al.. 1 982; Brown et al . , 1 985) . The rate of infection in the ICU is determined by several factors: ( i ) the type of patients treated. Medical patients and patients undergoing clean
elective surgery have a relatively low infection rate ( + 3% ) whereas in surgical and traumatological I CUs the overall infection rate may be as high as 38% (Caplan et al.. 1 98 1 ; Brown et al . , 1 985; Daschner, 1 985);
( i i ) the use of invasive techniques for monitoring and life support. The most common site of infection is the respiratory tract in mechanically ventilated patients: 20%-60% (Stevens et a l . , 1 974; Thorp et al . . 1 979; Cross et al . , 1 98 1 ; Dunham et a l . , 1 984; Tobin et a l . , 1 984) . The second most common site is the urinary tract: 10%-30% (Gross et al . , 1 980; MacKay. 1984) , in patients with an indwelling urinary catheter. The next most common site of infection is the bloodstream in patients with multiple intravenous and intra-arterial catheters: 1 5% (Dominguez de Villota et a l . , 1 983) followed by wound infections : 1 5% (Daschner, 1 985) ;
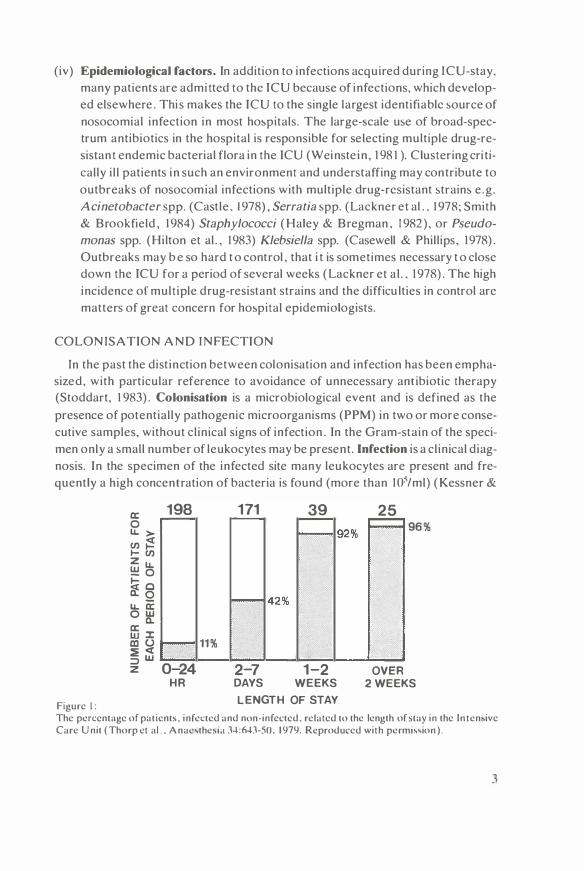
( i i i ) Length oflCU-stay. A l inear relationship exists between the duration o f stay in the ICU and the infection rate (figure 1 ). After 5 days of intensive care the infection rate is as high as 80%- 1 00% (Northey et al . , 1 974; Thorp et a l . , 1 979) . This is explained o n the one hand by the increased risk o f infection for patients requiring prolonged intensive care , and on the other hand by the prolongation of I CU-stay due to early infections.
2
(iv) Epidemiological factors. In addition to infections acquired during ICU-stay. many patients are admitted to the ICU because of infections, which developed elsewhere . This makes the ICU to the single largest identifiable source of nosocomial infection in most ho�pitals. The large-�cale use of broad-spectrum antibiotics in the hospital is responsible for selecting multiple drug-resistant endemic bacterial flora in the ICU (Weinste in , 1 98 1 ). Clustering cri tically i l l patients in such an environment and understaffing may contribute to outbreaks of nosocomial infections with multiple drug-resistant strains e .g . Acinetobacter spp. (Castle . 1978) , Serratia spp. (Lackner et al . , 1 978; Smith & Brookfield , 1 984) Staphylococci (Haley & Bregman . 1982) , or Pseudo
monas spp. (Hilton et al . , 1 983) Klebsiella spp. (Casewell & Phillips, 1 978) . Outbreaks may b e so hard t o control , that i t is sometimes necessary t o close down the ICU for a period of several weeks (Lackner et a l . . 1 978) . The high incidence of multiple drug-resistant strains and the difficu lties in control arc matters of great concern for ho�pital epidemiologists.
COLON ISATION AND INFECTION
In the past the dist inction between colonisation and infection has been emphasized, with particular reference to avoidance of unnecessary antibiotic therapy (Stoddart, 1 983) . Colonisation is a microbiological event and is defined as the presence of potentially pathogenic microorganisms (PPM) in two or more consecutive samples, without clinical signs of infection . In the Gram-stain of the specimen only a small number of leukocytes may be present . Infection is a clinical diagnosis. In the specimen of the infected site many leukocytes are present and frequently a high concentration of bacteria is found (more than 105/ml) (Kessner &
a:: 198 171 39 25 0 96% u. > en � ._ en z u. !!! 0 �o Cl: Q u.. a:: ow Q. ffi ::c 11% a:i (.) � <( ::::> w
0-24 2-7 1- 2 z OVER HR DAYS WEEKS 2WEEKS
Figure 1: LENGTH OF STAY
The percentage of patients. infected and non-infected. related to the length of stay in the Inten,ive Care Unit (Thorp et al.. Anae,the,i;i J4:MJ-50. 1 979. Reproduced with permi,,ion).
3

Lepper, 1967; Weinstein & Brown. 1977; Stoddart . 1 983) . Colonisation rates of the major organ systems are extremely high in ICU patients. In patients requiring prolonged mechanical venti lation colonisation of the lower respiratory tract occurs in more than 80% . colonisation of the urinary tract occur� in 20°,{, -60'Yo and colon isation of wound� in 30'Y.,-5()''1(, of patients (Northey et al . . 1 974 ; Ro�e & Bahcock . 1975 ; Hemming et al . , 1 976; Martinez et a l . . 1 986).
CDC-GU IDELINES FOR PREVENTION OF NOSOCOMIAL INFECTIONS
The Center for Disease Control . Atlanta , Georgia . USA recently published guidelines (CDC. 1985) that were viewed as ' . . applicable in most hospitals regardless of size . patient population or endemic nosocomial infection rates (Category I}' (Table I). Most of these measures are directed either at e l imination of exogenom (environmental) sources or at prevention of cross-infection i . e . an infection caused by a microorganism that is transferred directly or indirectly from one person to another (Stoddart , 1 983) . According to the CDC. the measures in Category I are ' . . strongly �upported by well-designed and controlled clinical studies that show their effectiveness in reducing the risk of nosocomial infections or are viewed as effective by a majority of expert reviewers . · Although some studies did show a reduction of nosocomial infections by the strict implementation of these guidelines. the reduction (less than 3%) was small in comparison to the infection rate (Daschner et al . . 1982). In other studies. however. no reduction could be achieved by a program involving improved maintenance of inhalation therapy equipment and strict hand asepsis (Rosendorf et a l . , 1 974) ; it has also been shown that isolation measures which are extremely costly and require special architectural design have very li ttle effect on the colonisation and infection rate (Preston et al.. 198 1 ) .
CONVENTIONAL ANTIBIOTIC POLICY
The control program for antibiotic therapy and prophylaxis (CDC) (Table I) restricts the use of parenteral antibiotics by ( i) not giving routine systemic prophylaxis ; ( i i ) by not treating colonisation ; ( i i i ) by giving specific systemic antibacterial
Table I CDC-GUIDELINES (Category I ) FOR PREVENTION OF NOSOCOMIAL INFECTIONS
- discipline - handwashing and hand-di>infection - adoption of CDC-guideline� for nur�ing techntque� - adoption of CDC isolation tcchni4ue' - sufficient personnel/patient relation - disinfection procedures - control program for antibiotic therapy and prophylaxi�.
4

therapy on strict clinical and bacteriological indications (Stoddart, 1 983 ). Several cl inical studies have led to this approach . Lackner et a l . ( 1 975) and Rotter ( 1 978) studied the effects of systemic antibiotic prophylaxis on pneumonia and septicaemia rate in a general ICU and found no reduction in the infection rate. Price ( 1 98 1 ) studied the effect of systemic antibiotic prophylaxis on the incidence of pneumonia in 100 patients requiring prolonged mechanical venti lation . Patients who were given prophylactic antibiotics for non-respiratory reasons had significantly more respiratory complications such as purulent sputum and infi l tration on the chest X- rays, than the group which did not receive systemic antibiotic prophylaxis. Neither can urinary tract infections be prevented with systemic antibiotic prophylaxis (Kass , 1 955) ; also in t raumatic wounds or burns. systemic antibiotic prophylaxis was not effective to prevent wound infections (Sanchez-Ubeda ct a l . , 1 958; Altemeicr et al . , 1 962; Caplan et al . , 1 979) . However, controlled cl inical trials have shown that a short course of antimicrobial prophylaxis (24 h) can lower the incidence of infection after certain operations (Hirschmann & Jnu i , 1 980; Gorbach , 1 982) .
Apart from clinica l evidence that systemic antibiotic prophylaxis is generally not effective, it is obvious that emergence of resistance is related to the extensive use of systemic antibiotics. Price ( 1 970) described an outbreak of Klebsiella infections in an ICU where prophylactic ampici l l in and cloxaci l l in were routinely prescribed . The epidemic was abruptly brought to an end when all ant ibiotic!> were withdrawn from the unit . Franco et a l . ( 1 973) found that in a neonatal ICU where kanamycin was routinely used, 80% of Enterobacteriaceae colonising the babies were kanamycin resistant . After substituting gentamicin for kanamycin there was a sharp fall in the incidence of kanamycin-resistance to 20% , while the gentamicin-resistance increased .
The aim of the conventional antibiotic policy is to avoid selection of mul tiple drug-resistant endemic flora in the ICU. However, there is increasing evidence that the premises upon which this policy is based , are merely theoretical . Firstly, the distinction between colonisation and infection : in daily practice it is often extremely difficult to distinguish between colonisation and infection , particularly of the respiratory tract (Shield et a l . , 1 979; Andrews et al . , 1 98 1 ) . Clinical symptoms of infection such as fever, leukocytosis, infi l trations on the chest X-ray or deterioration of blood gases may be present in a wide variety of non-infectious clinical conditions in critical ly i l l patients; this may result in too early administration of antibiotic therapy, which apart from not being effective, increases the risk of suprainfections; secondly , to wait with specific antibiotic therapy unti l there are clinical signs of infection is not effective either: once an infection with Enterobacteriaceae or Pseudomonadaceae has developed, antibiotic therapy often comes too late. Even with the new potent antimicrobial agents, bacteriological and clinical
5
cure rates are very disappointing and these infections are associated with a high mortality: 30'Yo -70% (Stevens et al . . 1 974; Baker et al . . 1 980: Platt et al . . 1982 ; Berger et al . , 1 985 ; Schentag et al . . 1 985) ; thirdly, not to give antibiotic prophylaxis: emergence of re�i�tance does not only occur during systemic antibiotic prophylaxis, but even more so during systemic antibiotic therapy (Goldstein et a l . , 1 983) . The incidence of colonisation and suprainfection with resistant strains during systemic antibiotic therapy ha� been reported to be as high as 38'Yo (Weinstein et a l . , 1 954; Platt et al . . 1 98 1 ; Schentag et a l . , 1 985).
In summary. in the la�t decade the coloni�ation and infection rate in the ICU ha� remained extremely high . Al though the introduction of efficient disinfection procedures has el iminated many exogenous source� of infection, the infection rate did not decrease significantly. Attempts to control cross-infections by implementation of the CDC-guidelines did not result either in the expected reduction of the infection rate. The generally accepted restrictive ant1biot1c policy has been very disappointing with respect to morbidity and mortality from infections, while the problem of emergence of multiple drug-resistant strain� in the ICU remains a major concern in many hospitals.
II MICROORGANISMS
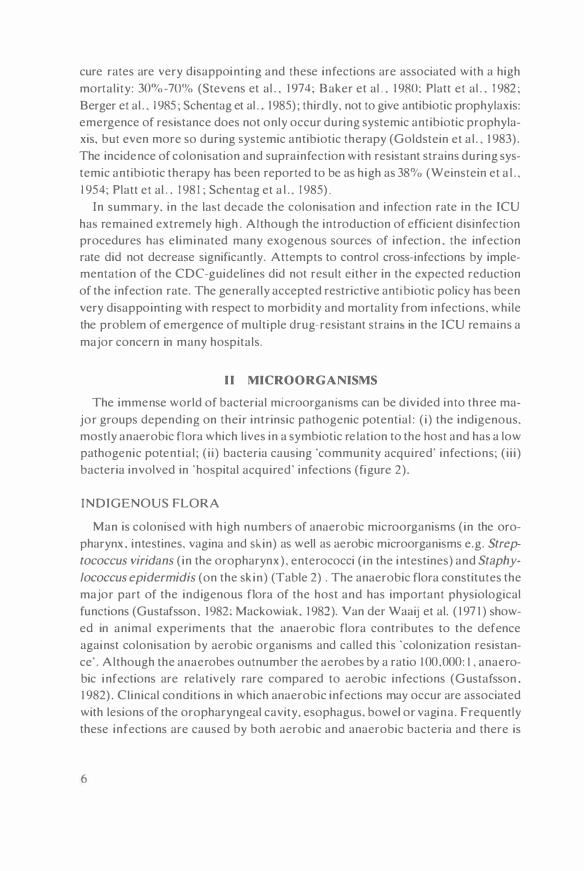
The immense world of bacterial microorgan isms can be divided into three major groups depending on their intrinsic pathogenic potential: ( i ) the indigenous, mostly anaerobic flora which lives in a symbiotic re lation to the host and has a low pathogenic potent ia l ; ( i i ) bacteria causing 'community acquired' infections; ( i i i ) bacteria involved in "hospital acquired' infections (figure 2).
INDIGENOUS FLORA
Man is colonised with h igh numbers of anaerobic microorganisms (in the oropharynx . intestines. vagina and sl..in) as well as aerobic microorganisms e.g. Strep
tococcus viridans ( in the oropharynx) , enterococci ( in the intestines) and Staphy
lococcus epidermidis (on the sk in) (Table 2) . The anaerobic flora constitutes the major part of the indigenous flora of the host and has important physiological functions (Gustafsson , 1 982: Mackowiak. 1 982). Van der Waaij et al. ( 1 97 1 ) showed in animal experiments that the anaerobic flora contributes to the defence against colonisation by aerobic organisms and called this ·colonization resistance' . Although the anaerobes outnumber the aerobes by a ratio 1 00,000: I, anaerobic infections are relatively rare compared to aerobic infections (Gustafsson . 1 982) . Clinical conditions in which anaerobic infections may occur are associated with lesions of the oropharyngeal cavity, esophagus, bowel or vagina . Frequently these infections are caused by both aerobic and anaerobic bacteria and there is
6

evidence that aerohic bacteria , by consuming oxygen , create the anaerobic circumstance!> which are nece!>!>ary for the development of anaerohic hacteria (Onderdonk et al . , 1 976; Fincgold. 1 977).
HIGH PATHOGENIC POTENTIALLY PATHOGENIC LOW TO (A) PATHOGENIC
60f'delella pertussis
Corynebacterium diphteriae
Mycobacterium tuberculosis
Streptococcus pyogenes
Salmonella species
Campyk>bacter species Enterobaclenaceae (other than
hosts. own e. c::olil
e.g. K1ebsiella spp, Proteus
and MorganeUa spp, Enlerobacter and Citro-
bacler spp, Serratia spp,
Pseudomonadaceae spp
Acinetobacter spp Streptococcus pneumoniae
Heomophilus mfluenzae
Branhamella catarrhalis
Eschenchia coli
Staphylococcus aureus
Candida alb1cans
Streptococcus vir1dans
Streptococcus faecalis
Staphylococcus eptdermidis
anaerobes
EPIDEMIC HOSPITAL COMMUNITY INDIGENOUS
host. percentage of heally carrier
Figun: 2: Microorgani'm' can he divided according to their in<rin,ic pathogenic potential and their conccn<ratiun in the normal microtlora into pathogens. potentially pathogenic microorganisms (PPM), and indigcnou' flora. The arrangement of PPM is hascd on the ohscrvationsof Kurrie ct al. ( 1981 ) .
'COMMUN ITY-ACQU IRED' INFECTIONS
Healthy people may carry PPM in the oropharyngeal cavity and gastro-intestinal canal ( Rose bury , 1 962) (Table 2). which may cause an infection when the resistance decreases. More than 90% of people carry Escherichia coli in the gut and this organism is frequently involved in urinary tract infections. Streptococcus
pneumoniae, Haemophilus influenzae and Branhamella catarrhalis are frequently present in the oropharyngeal cavity and are often involved in infections of ears, sinuses and the respiratory tract. 30%-40% of healthy people carry Staphylococ
cus au re us in the oropharyngeal cavity, gastro-intestinal canal or skin and this microorganism is frequently involved in wound infections. Before the antibiotic era these 'community-acquired' bacteria were responsible for most infections and the
7

first antibacterial agents developed, were specifical ly active against these microorganisms . Most of these microorganisms are still very sensitive to many antibiotics, and in general 'community-acquired' infections have a low morbidity and mortality.
Table ?. NORMAL FLORA
Microorgani'm�
Anaerobe' S. viridans S. pneumomae H. influenzae B. catarrhalis S. aureus Yeastspp. Enterohacteriaccac } Pseudomonadaceae
Anaerobes Enterococci E. coli Yeastspp. Enterobactenaceae} P'cudomonadaceac
Concntrat1on hact/ml
OROPHARYNGEAL I 07 '' IO' IO'·' IO'' IO'< IO'' IO' IO'
INTESTINAL IO'' II
IO' IO' IO' IO'
'HOSPITAL-ACQUI RED' INFECTIONS
Frequency 1y.J
IOO% 100%
30-80% 30-80% 30-80'X, 30-40% 30-40%
<IS'}�,
100"., IOO'X, 90"<•
20-40'¥,, <l.51111
I n the hospital . patients may become colonised by 'hospital' bacteria e.g . Enterobacteriaceae (other than the host's own E. coli) such as Klebsiella . Proteus, En
terobacter spp. , and Pseudomonas and Acinetobacter spp. This flora-shift is promoted by many factors such as the underlying disease, advanced age and the use of antibiotics (Weinstein , 1 968) . Most commonly used antibacterial agents are act ive against both the i ndigenous flora and the 'community' bacteria , which are then quickly eliminated and replaced by hospital bacteria (Florey et al . , 1 947 ; Kessner & Lepper. 1 967; Caplan et al . , 1 979) . Hospital-acqu1red infections , and in particular those of the lower respiratory tract. are difficult to treat and have a h igh morbidity and mortality (Gross et al . , 1 980; Brown et al . , 1 985) . ·
III PATHOGENESIS OF COLONISATION AND INFECTION
ORIGIN OF I NFECTION: EXOGENOUS VS. ENDOGENOUS
An exogenous infection is defined as an infection by microorganisms that are not present in the oropharyngeal or i ntestinal flora of the patient . This type of infection , which used to be an important cause of infection in the early days of in ten-
8

sive care , is associated with environmental sources e . g. venti latory equipment . humidifiers . nchul isers . contaminated infusion solutions etc.
An endogenous infection is defined as an infection by microorganisms that arc part of the patient's oropharyngcal or i ntest inal flora .
DEFENCE MECHANISMS: COLON ISATION DEFENCE AND INFECTION DEFENCE
Host defence against bacterial invasion can be divided in coloni�ation-defence and infection-defence (figure J).
Coloni�ation defence can be defined as a complex of mechanisms defending aga inst coloni�ation hy cxogcnou� PPM . Thi� defence �y�tem con:-i�ts of several
Figure J:
INT ACT DEFENCE MECHANISMS
SEVEN CLEARING FACTORS AIMING AT "CONTROL"
1. Anatomy
2. Physiology 3 Molihty
HOSPITAL
Enlerobacter1aceae
(olher than hosts'
own E coo)
Pseudomonadaceae
Acinelobacter spp.
S s -lgA
6 Mucosal cell turnover
Candida spp.
COMMUNITY'
S aureus
S pneumomae
H influenzae
B catarrhahs
E coll
RESPIRATORY URINARY TRACT
SKIN DEFENCE AGAINST
INFECTION (Ill)
RESPIRATORY URINARY TRACT
SKIN DEFENCE AGAINST
COLONISATION (II)
OROPHARYNGEAL CAVITY/
GASTRO INTESTINAL CANAL DEFENCE AGAINST
COLONISATION (I)
Schematic representation of the three harrier., con.,tituting the defence again>! haeterial i nva>ion . and the factor� contrihuting to each of the.,e hmrier ...
9

mucosa- and skin- associated mechanisms which clear PPM from the oral cavity, the gastro-intestinal canal , the respiratory and urinary tracts and the skin .
( i) colonisation defence o f the oropharyngeal cavity and gastro-intestinal canal
The major supply of bacteria is formed by food and beverages (Remington , 1 98 1 ) . A healthy individual is able to cope with a large challenge of bacteria (up to 1 09 bact) without colonisation (Buck & Cooke, 1 969; LaForce et al., 1 976). Factors contributing to the colonisation defence are (i) integrity of anatomy, ( i i) normal physiology and (i i i ) moti l i ty (swallowing, salivary flow and peristalsis) (Dixon , 1 960) , (iv) secretions such as saliva, bile and mucus, (v) secretory immunoglobulinA (S-IgA) , (vi) desquamation and shedding of mucosal cells and (vii) the indigenous (anaerobic) flora (van der Waaij , 1 97 1 ). The mechanical clearing mechanisms (swallowing, peristalsis) are essential for the colonisation defence (Dack & Petran, 1 934) . Adherence of bacteria to the mucosa is inhibited by mucus secretions, S-IgA and desquamation of cells. The indigenous flora contributes to the colonisation defence through bacterial interference via volatile fatty acids, bacteriocins, food competition and masking of receptor sites (Rolfe. 1 984). When the colonisation defence is intact (the first barrier) the oropharyngeal cavity does not harbor Enterobacteriaceae or Pseudomonadaceae and apart from the indigenous flora the bowel is only colonised by E. coli (Table 2) (Rosebury, 1 962; La· Force et al . , 1 976) .
Altered colonisation defence of the oropharynx and gastro-intestinal tract
Johanson ( 1 969) reported an increased colonisation by Enterobacteriaceae and Pseudomonadaceae in severely ill patients. He demonstrated that the severi· ty of the underlying disease was associated with an increased adherence of these microorganisms to the buccal mucosal cel ls (Johanson, 1 979) . Valenti et a l . ( 1 978) showed that advanced age decreases the colonisation defence of the oropharyngeal cavity. In critically ill patients many other factors may also play an important role: instrumentation (e.g. endotracheal tubes , nasogastric tubes etc. ) , paralytic i leus, coma, the use o f anesthetics , sedatives and muscle relaxants which interfere with swallowing and gastric motility, the suppression of gastric acidity by antacids and Hi-receptor antagonists (Atherton & White, 1 978; DuMoulin et al . , 1 982 ; Hil lman et al . , 1 982; Pingleton et al . , 1 986) which promotes the proliferation of bacteria in the stomach; the administration of antibacterial agents which af· feet the indigenous flora may further decrease the defence against colonisation and promote colonisation by Enterobacteriaceae and Pseudomonadaceae. Penici l l ins, ampici l li n , cloxaci l l in , ticarci l l in , azlocil l in, mezlocil l in , piperacil l in , erythromycin , moxalactam and many others are known to decrease the colonisation
JO
defence (flora factor) (Wiegersma et al . , 1 982; Nord et al . , 1 984; Kager et a l . , 1 984; Hentges et al . , 1 985 ; Sunakawa et al . , 1 985 ; Vogel & Oermann, 1 985)
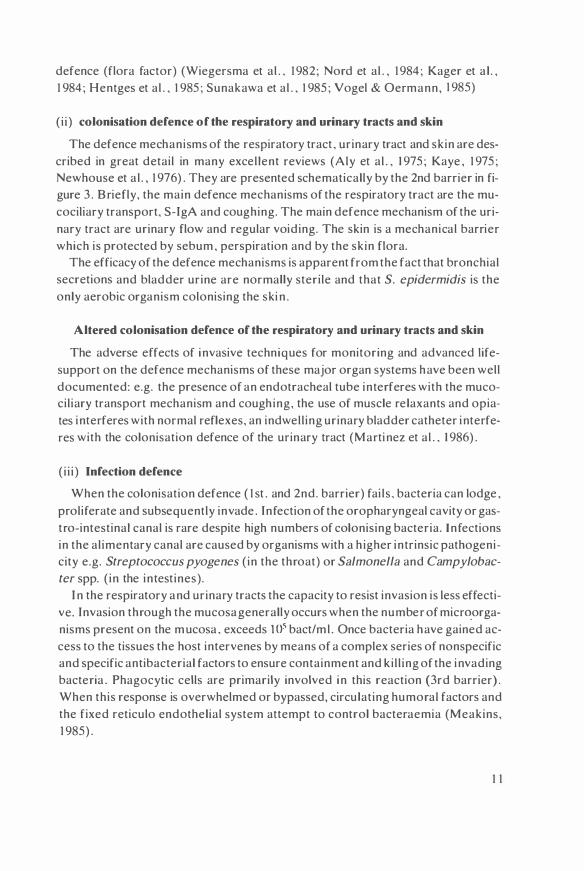
( i i) colonisation defence of the respiratory and urinary tracts and skin
The defence mechanisms of the respiratory tract , urinary tract and skin are described in great detail in many excellent reviews (Aly et al . , 1 975 ; Kaye , 1 975 ; Newhouse et a l . , 1 976 ) . They are presented schematically by the 2nd barrier in figure 3 . Briefly, the main defence mechanisms of the respiratory tract are the mucociliary transport, S-IgA and coughing. The main defence mechanism of the urinary tract are urinary flow and regular voiding. The skin is a mechanical barrier which is protected by sebum , perspiration and by the skin flora.
The efficacy of the defence mechanisms is apparent from the fact that bronchial secretions and bladder urine are normally sterile and that S. epidermidis is the only aerobic organism colonising the ski n .
Altered colonisation defence of the respiratory and urinary tracts and skin
The adverse effects of invasive techniques for monitoring and advanced lifesupport on the defence mechanisms of these major organ systems have been well documented: e.g. the presence of an endotracheal tube interferes with the mucociliary transport mechanism and coughing, the use of muscle relaxants and opiates interferes with normal reflexes, an indwell ing urinary bladder catheter interferes with the colonisation defence of the urinary tract (Martinez et al . , 1 986).
( i i i ) Infection defence
When the colonisation defence ( 1 st . and 2nd. barrier) fai ls , bacteria can lodge , proliferate and subsequently invade . Infection of the oropharyngeal cavity or gastro-intestinal canal is rare despite high numbers of colonising bacteria. Infections in the al imentary canal are caused by organisms with a h igher intrinsic pathogenicity e.g. Streptococcus pyogenes ( in the throat) or Salmonella and Campylobac
ter spp. ( in the intestines). I n the respiratory and urinary tracts the capacity to resist invasion is less effecti
ve. Invasion through the mucosa generally occurs when the number of micr�organisms present on the mucosa , exceeds 105 bact/ml . Once bacteria have gained access to the tissues the host intervenes by means of a complex series of nonspecific and specific antibacterial factors to ensure containment and ki l l ing of the invading bacteria . Phagocytic cells are primarily involved in this reaction (3rd barrier) . When this response is overwhelmed or bypassed, circulating humoral factors and the fixed reticulo endothelial system attempt to control bacteraemia (Meakins, 1 985) .
1 1

Altered infection defence
In the critica l ly ill patient there are many factors interfering with the ce llular and humoral immune -.ystem (Brun Buisson, 1 983) (Table 3)
The cri tically ill patient ha-. to be considered as an immunocompromised host with an acquired immunodeficiency. This accounts for the high infection rate and for the high mortality from infections . However, this immunodeficiency is mo-.tly reversible when the underlying disease is successfully treated .
Tahlc J I M M UNOCOM PROMISED HOST
Factor' 1.kcrca>tng infection dekncc in critocall) ill patocnh:
- cardoopulmonary in>ufficicncy (e.g. 'hod . . acido>b. hypoxia) - multiple iniuric,. 'urgical trauma. lhcrm.ol injur) - ;plcncctomy - prnlcin-caloric malnulrition. calaholi'm - mcdicatmn (cyto,talic drug,. cort1co,tcrnid,. ,111,1c,thctic') - advanced agc - cardio-pulmonary hypa"
infcction'
IV INTESTINAL FLORA SUPPRESSION
Intestinal flora suppression dates back to 1939 when Garlock and Seley suggested the use of sulphanilamide in colorectal surgery. In this type of surgery the use of oral antibacterial agents to prevent wound infections has been extensively studied. Many different antimicrobial agents such as sulphonamides, streptomycin. neomycin, kanamycin and paromomycin have been tried for intestinal flora suppression (Poth et a l . , 1 950, 1 957 ; Cohn& Longacre . 1 959;Weinstein et al . , 1 96 1 ) . Because of the gap in the antimicrobial spectrum and the development of resistance when only one oral drug was used. Poth et a l . ( 1 960) advocated a combination of neomycin and phthalylsulphathiazole . Nicols and Condon ( 1 972) stated that this combination allowed the persistence of anaerobes in approximately one half of the subjects. They proposed the use of neomycin in combination with the absorbable erythromycin to cover both the anaerobic and aerobic fractions more completely. Up to the present time this combination is widely used in colorectal surgery (Figueras-Fil ip et al . , 1 984) .
A second group of patients in which oral antibiotic programs are being used , are immunocompromised granulocytopenic patients. In order to prevent colonisation and infection of the respiratory and urinary tracts and skin, oral antibiotics are given to suppress the oropharyngeal and intestinal flora, which is known to be the endogenous source in these patients (Schimpff et al . , 1972). A well known oral regimen consisted of gentamicin, vancomycin and nystatin (GVN) to suppress both the aerobic and anaerobic intestinal flora (total flora suppression) .
12

However, the increased risk of overgrowth by resistant organisms necessitated reverse isolation (Bodey, 1 974; Klastcrsky ct a l . , 1 974 ) . With this regimen intestinal colonisation occurred not only with resistant organisms but also with sensitive organisms. in particular with Pseudomonas spp. Van dcr Waaij ( 1 97 1 ) showed that the effect of these oral antibiotics on the anaerobic flora might be responsible for the observed overgrowth by aerobic microorganisms. This observation and the fact that anaerobes are not frequently involved in infections, have lead to more selective flora-suppression regimens aiming at selective el imination of only the aerobic PPM, whilst preserving the indigenous anaerobic flora as much as possible. With the FRACON-regimcn, consisting of framycctin (neomycin) + col istin (polymyxin E) + nystatin, and with the combination of polymyxin B + neomycin + nalidixic acid + amphotericin B, good results were obtained (Storring et al . , 1 977; Sleyfer et a l . , 1 980; G uiot et al . , 1 98 J ) . Overgrowth by sensitive or resistant organisms was less frequent and reverse isolation did not appear to be necessary with these regimens. Another approach has been the use of co-trimoxazole to suppress Enterobacteriaceae in the intestinal flora without affecting the anaerobic flora ('selective flora suppression') . This was first shown clinical ly by Hughes et a l . ( 1 977) who gave oral co-trimoxazole as prophylaxis for Pneumocystis carinii infections in children with acute lymphocytic leukaemia , and found a substantial reduction of the frequency of bacterial infections. This has stimulated the use of oral co-trimoxazole in granulocytopenic patients. However, resistance against co-trimoxazole rapidly develops and often the addition of another agent such as colistin is necessary (Wilson & Guiney, 1 982 ; Rozenberg et al . , 1 983) . Besides, as a consequence of absorption of the high oral dose , co-trimoxazole has undesirable systemic side-effects , particularly prolonged bone marrow depression.
Other conditions in which flora suppression has been shown to be useful are prevention of necrotising enterocolitis in small infants and neonates (Egan et a l . , 1 976; Grylack & Scanlon, 1 978) and prevention of colonisation and infection of wounds in burn patients (Jarret et al . , 1 978) .
V AIM OF THE STUDY
At the time of onset of the study described in this thesis i t was generally accepted that the majority of infections in the ICU were cross-infections and that exogenous sources of PPM were most important. The role of endogenous infections in the ICU was not well defined. The experience with selective decontamination of the digestive tract in leukaemic patients (Sleyfer et al . , 1 980) suggested that, in the ICU also, at least part of the infections might be endogenous and could therefore be prevented in this way. Therefore, in 1 98 1 , a pilot study was started with selective decontamination of the digestive tract in mechanically venti lated intensive
1 3

care patients staying more than 5 days in the ICU . The oral antihiotic regimen consisted of polymyxin E 4x200 mg, co-trimoxazole : 3x(800 mg sulfamethoxazole + 1 60 mg trimethoprim) and amphotericin B 4x500mg. The oral cavity was rinsed with chlorhexidine 2% aq . Fifty-five patients were treated: 32 multiple trauma patients, 5 cardiac surgery patients and I 8 septic patients. It was found that 1 8 out of 55 patients were colonised in the oropharynx and intestines during treatment, mostly with Pseudomonas and Acinetobacter spp. , which were in-vitro sensitive to polymyxin E . but not to co-trimoxazole . Although the rate of urinary tract infection was relatively low (5/55) . pulmonary infections occurred in 12 patients (22%) (Stoutenbeek et al . . I 982) . Due to the inpredictable absorption of co-trimoxazole in intensive care patients. it was necessary to monitor co-trimoxazole plasma levels. in particular in patients with renal insufficiency. Moreover. seriom side-effects (e.g. allergy and thromhocytopenia) were noted.
Co-trimoxazole versus tobramycin:
Because of the unsatisfactory results and the side- effects. it was decided to replace cotrimoxazole with the nonabsorbable tobramycin. Tobramycin seemed to be a better choice than gentamicin . because of (i) the failure of the gentamicin + vancomycin + nystatin (GVN) regimen in leukaemic patients and (i i) the good results obtained with tobramycin in volunteers (Mulder et al . . I 984) ( i i i ) the excel lent activity of tobramycin against ICU-associated flora e .g . Pseudomonas and Acinetobacter spp.
Oral decontamination:
The next step was to improve the oropharyngeal decontamination. Rinsing the oral cavity with an 2% aqueous solution of chlorhexidine was not effective against colonisation with Gram-negative baci l l i . Attempts were made to decontaminate the oropharynx with a 2% solution of the same antibiotics as used for intestinal decontamination. Cultures taken before and after rinsing the oropharynx with this solution . showed no significant difference in colony counts. Increasing the antibiotic concentration did not improve the results. One hour after rinsing, no antibiotic levels were detectable in saliva samples. Therefore other application forms were examined. Some experience was available with Orabase® (Squibb. Rijswijk , Holland) containing amphotericin B in healthy volunteers (de Vries & van der Waaij , 1 978) . Orabase and different composi tions of carboxymethylcellulose-paste, were tested in-vitro as vehicle for polymyxin E, tobramycin and amphotericin B (2%) with respect to drug-release and duration of activity. Orabase . which is a very sticky paste adhering to the moist mucosa for many hours, had the best in-vitro characteristics (Laseur. unpublished observations) and was clinically effective .
14

Study design:
Because the character of the study was stil l experimental , it was decided to do a prospective open tria l with this new regimen, in polytrauma patients, during a period of six months and compare the results with a historical control group (vide infra) . The other patients in the ICU, staying longer than 5 days, were also treated with this regimen to e l iminate all sources of PPM in the ICU and to reduce the risk of transmission of microorganisms between patients. Th is excluded the possibi l ity of an untreated control group. At that time, the fear of emergence of resistance against the topical antibiotics prohibited a 'bl ind' study design because this implies that the clinician would not be informed about the results of the bacteriological cultures of throat and rectum . This would carry the risk that an outbreak with a mult iple-resistant strain might well go unnoticed, until serious consequences would have developed .
This study was discontinued after 5 months, due to the high incidence o f early pneumonia (Chapter 4) . It was decided to continue the study in multiple trauma patients, but now with the addition of systemic antibiotic prophylaxis, which proved to be effective . This part of the study was continued for two years. The reasons to extend this study over such a long period were: first , to ascertain that the initial good effects of this regimen on the colonisation and infection rate could be maintained and second, to be able to monitor the sensitivity patterns of al l isolated aerobic Gram-negative bacteria over a prolonged period of time to detect the possible emergence of resistance under this regimen.
Why multiple trauma patients ? ( i ) Polytrauma patients are l ikely to have a normal microflora at the time of the
accident. Therefore al l changes in the microflora have to be the result of the trauma itself, the treatment or hospitalisation.
( i i ) In accordance with a generally recommended antibiotic policy (Gaya, 1 976) , polytrauma patients did not routinely receive any systemic antibiotic prophylaxis. This permitted study of the effect of the topical nonabsorbable antibiotics on colonisation and infection rate, uninfluenced by systemic antibiotic use .
( i i i ) General ly , polytrauma patients are previously healthy individuals who suffer from a sudden severe impairment of the function of the vital organs and the infection defence mechanisms. However, in contrast to other immunocompromised patients (e .g . leukaemic patients) this fai lure is transient , provided no complications occur such as infections.
(iv) infection is responsible for 80% of late deaths and is the major cause of mult iple organ fai lure in polytrauma patients (Fry et al . , 1 980; Goris & Draaisma,
15

1 982; Watt & Ledingham, 1 984) . Thus. if it would be possible to prevent infections in the period of susceptibility for infections, it was to be expected that the prognosis would improve.
(v) the �everity of injuries can be determined with an generally accepted scoring system ( Injury Severity Score) (Baker et a l . . 1 97..J.) . which allows comparison of patient groups.
Control group:
Since 1 979 all polytrauma patients in our institution were treated with the same trauma treatment protocol. by the same team of traumatologists and intensivists. From all patients an accurate daily recording of infection was made by one of the intensivists. Bacteriological surveil lance cultures were taken from all sites ( including throat and rectum) on admission and thereafter three times a week (Ors. J . Dankert , Ziekenhuis epidemiologie ) . After inspecting the available material and confirming that no essential data were missing, a retrospective study on colonisation and infection over a two-year period was undertaken. The results of these studie� are de�cribed in the following chapter� .
Description o f the studies
Chapter 2: Firstly, the colonisation and infection rate is determined in a control group of mechanically ventilated multiple trauma patients treated without systemic antibiotic prophylaxis (conventional antibiotic policy) . Secondly, the pathogenesis of infection is studied, in order to determine whether ICU-acquired infections were exogenous or endogenous. Thirdly. the effect of selective decontamination on colon isation and infection rates is studied in a prospective open trial . in mechanically ventilated multiple trauma patients, treated with oral nonabsorbable antibiotics and systemic antibiotic prophylaxis.
Chapter 3 : It is generally accepted that a restrictive antibiotic policy decreases the risk of emergence of resistance and superinfection . This assumption was tested by studying the use of systemic antibiotics in the control group, with particular reference to the question whether the restrictive antibiotic policy had really been restrictive and whether this decreased the risk of superinfections. These data are compared with the effect of routine systemic antibiotic prophylaxis, in the group treated with selective decontamination .
Chapter 4: This study describes the pathogenesis and prevention of pulmonary infection in mechanically ventilated multiple trauma patients. In the first part of the study the incidence and the pathogenesis of pulmonary infections in the control group are analyzed . In the second part the effect of three consecutive prophylactic antibiotic regimens are compared: (i) intestinal decontamination alone , ( i i )
1 6

inte'>tinal decontamination in comhination with oral decontamination . ( i i i) intest inal + oral decontamination + sy<>temic antihiotic prophylaxis.
Chapter 5: The hypothc-;is i-; tc.'>tcd that the use of a third-generation cephalosporin for routine systemic antibiotic prophylaxis . and an aminoglycoside for selective decontaminat ion would in the long term lead to selection of mult iple-drug resistant microorganism-, which would render valuable antibiotics worthless for '-Y'>tcmic therapy. The -,tudy dcscrihes the incidence of acqui-,it ion. '>Ccondary colonisation and infection by resistant Enterobacteriaceae anti Pseudomonadaceae during 30 month-, of continuous use of the -;amc antibiotic regimen .
Chapter 6: In the l i terature . the reported overall mortality of multiple trauma paticnh is approximately 2011 11 -30110 . Many inve-.tigator-. have shown the prognostic value of the I nj ury Severity Score and age for morbidi ty and mortality. The causes of death in the intensive care unit arc either craniocercbral trauma. which is mostly fatal within the first 5 days. or sepsis. multiple-organ failure and ARDS. which arc the principal causes for late mortal i ty . This study reports the late mortality from sepsis and multiple organ failure in relation to Injury Severity Score and age in severely injured patients. admitted during a 30 month period .
Chapter 7: Nmocomial Gram-negative pneumonia in the ICU has a notoriously high mortality (33'1., -70% ). Whilst the patient is intuhated. i t is difficult to eradicate the causative microorganisms from the respiratory tract with systemic antibiotic therapy alone ; and the incidence of relapse and superinfection is high. I n this pilot-study the hypothesis i s tested that i f the endogenous source of the infection can be eliminated by -;elective decontamination. the results of the treatment may improve . The study describes a 3-year experience with selective decontamination in mechanically ventilated patients with pneumonia caused by Enterobacteriaceae or Pseudomonadaceae.
Chapter 8: New insights in the concept of 'colonisation resistance· and 'selective decontamination' are discussed. An account is given of the choice of antibiotics used for selective decontamination . The second part of this chapter summarizes the main differences between conventional infection prevention pol icies in the ICU and the novel approach described in this the<>is.
1 7


Chapter 2
The effect of selective decontamination of the digestive tract on colonisation and infection rate in multiple trauma patients
Ch. P. Stoutenbeek, H . K . F. van Saene("') , D . R. Miranda and D. F. Zandstra
Institute for Anesthesiology and lntcn�ivc Care and dept. of Cl inical Bacteriology ( ) . Univcr�ity Hospital, Groningen
Intensive Care Medicine 10 : 1 85 ( 1 984)
1 9

Abstract
1 22 multiple trauma patients staying in the ICU for 5 or more days and needing mechanical ventilation were investigated to determine the effect of selective c.lccontamination of the digestive tract on prevention of infection . The (retrospectively studied) control group of 59 patient� received no antibiotic prophylaxi�. The infection rate during ICU-�tay wa� 8 1 'X, , Mmt infection� were cau�cd by potentially pathogenic microorganism� (PPM) from the oral cavity or intc�tinc� ( i .e . endogenous infection ) . The oropharynx and intestines were rapidly colonised with ICU- associated Gram-negative bacil l i . After 2 wccb more than 80% of patient� were found colon i�cd . Thb secondary colonbat1on of the digestive tract i� a very important stage in the pathogenesis of infections. Sixty-three patient� were selectively decontaminated with non-ab�orbablc antibiotics, admin istered through the gastric tube even if pcristabis was absent . Empha�i� was laid on the selective decontamination of the oral cavity, using topical application of an antibiotic paste . With th is technique the oral cavity was free of PPM within 3 day� in most patients. No secondary colonisation wa� found . Rectal coloni�ation decreased significantly after 5 days. Secondary colonisation occurred in 9 patients with PPM sensitive to the antibiotics used. The prophylactic regimen included systemic ccfotaximc, directed against early endogenous infection . The supprc��ion and after �omc time the absence of the endogenous source of PPM resulted in a significant reduction of colonisation and infection . The total infection rate decreased to I 6'X, .
Introduction
I nfection continues to be the major cause of morbidity and mortality in severely traumatised patients (Baker ct al . , 1 980; Gori� & Draaisma , 1 982) . These patients arc very susceptible to infection due to an acquired defect in host defence mechanisms (Bradley ct al . , 1 98 1 ) . Advanced life support including invasive techniques of monitoring and treatment further increases the risk of infection (Freeman & McGowan , 1 978) . The predominating pathogens causing infection in the ICU arc aerobic Gram-negative baci l l i (Stoddart , 1 983) .
I t is generally recommended that systemic antibiotic prophylaxis should not be given in these patients because apart from being not effective 1t may give ri�c to emergence of resistant strains of nosocomial Gram-negative bacil l i (Ga ya , 1 979 ; Daschner, 1 978; Stoddart, 1 983 ) . Therefore treatment with systemic antibiotics should only be given when there is clin ical evidence of infection. However, once a serious infection has developed, the outcome will often be fatal , even with adequate antibiotic treatment (Northey ct al . , 1 974 ; Stevens ct al . , 1 974; Thorp ct al . , 1 979 ; Cross & Roup, 1 98 1 ) .
Another approach to infection prevention, used in lcukaemic patients (Schimpff, 1 980) and surgery (Altemeier e t al . , 1 968 ; Nichols , 1 98 1 ), is based on
20

the observation that many infections arc cndogcnou!> i . e . cau!>cd by potentially pathogenic microorganisms (PPM) colonising the digestive tract of a patient . Many of the techniques used aim at total gut decontamination ( i . c . suppression of both the aerobic and anaerobic bacteria) . Total gut decontamination however, carries the risk of overgrowth by resistant Gram-negative bacil l i from the hospital environment (Altcmcicr ct al . , 1 968; Schimpff ct a l . , 1 972) . The enhanced risk of overgrowth is probably due to the !>upprcssion of the anaerobic flora and hence a reduction in colonisation resistance.
The concept of colonisation resistance proposed by van dcr Waaij !>uggcst!> a beneficial effect of the anaerobic flora in resisting colon isation by acrobcs along the alimentary canal (van dcr Waaij ct a l . , 1 969) . Selective decontamination of the digestive tract (SOD) aims at selective el imination of the aerobic Gram-negative baci l l i and yeasts from the al imentary cana l , leaving the anaerobic flora unaffected . This techn ique has been successfully applied in leukaemic patients (Slcyfer et a l . , 1 980) .
The aim of the present study was to invc!>tigatc whether selective decontamination of the digestive tract could be effective in ICU-patients whose digestive tract is not functioning and to study the effect!> of this techn ique on the colon isation pattern and infection rate . In 1 98 1 we started a pilot study on infection prevention by SOD, initially without additional systemic antibiotic prophylaxis. As this appeared not optimal , a sy!>temic, colonisation resistance-indifferent, antibiotic such as cefotaxime was added to the regimen, assuming that the combination with SOD prevents emergence of resistance .
A double-blind trial seemed not to be the appropriate method for investigation because in the first place it was considered l ikely that having heavily contaminated patients next to decontaminated patients might adversely affect the potentially beneficial results. Secondly , a reduction of the number of contagious patients by applying SOD in half of them, might reduce the acquisition , colonisation and infection incidence in the not-SOD-treated control group. Therefore we have chosen for an open tria l comparing the results obtained with this technique with a retrospective study from two years without SOD ( 1 979+ 1 980) . Results of SOD treatment in 1 98 1 are not included in this investigation since in that year the study was set up as a pilot study, necessary to adapt procedures and methods of SOD developed in leukaemic patients to the requirements in a surgical ICU .
Patients and methods
Hundred and twenty-two patients who were admitted to the ICU with multiple injuries and who remained in the ICU for 5 days or longer arc included in the study. All patients were cndotracheally intubated and mechanically ventilated .
2 1
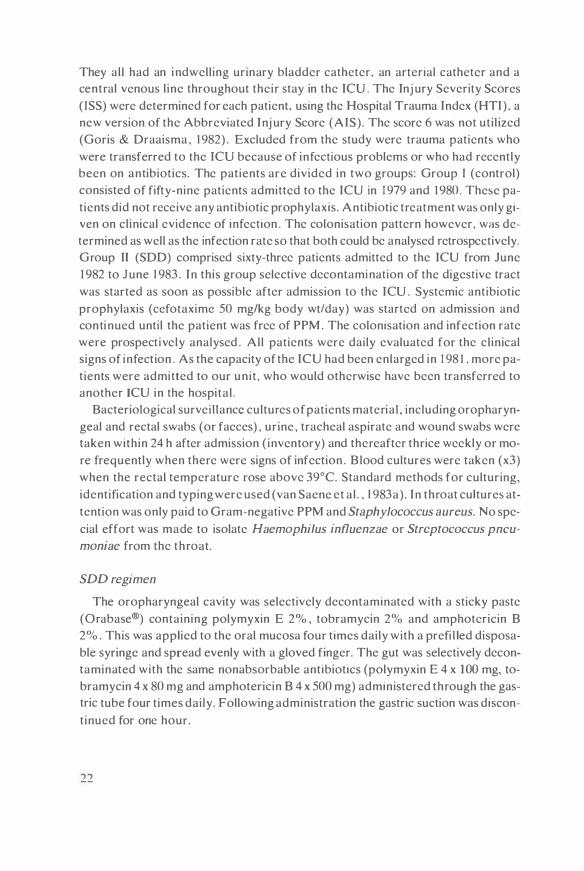
They all had an indwelling urinary bladder catheter. an arterial catheter and a central venous l ine throughout their stay in the ICU . The Inj ury Severity Scores ( ISS) were determined for each patient, using the Hospital Trauma Index (HTI) , a new version of the Abbreviated Injury Score (AIS) . The score 6 was not util ized (Goris & Draaisma , 1 982) . Excluded from the study were trauma patient� who were transferred to the ICU because of infectious problems or who had recently been on antibiotics. The patients are divided in two groups: Group I (control) consisted of fifty-nine patients admitted to the ICU in 1 979 and 1 980 . These patients did not receive any antibiotic prophylaxis. Antibiotic treatment was only given on clinical evidence of infection . The colonisation pattern however, was determined as well as the infection rate so that both could be analysed retrospectively. Group II (SOD) comprised sixty-three patients admitted to the ICU from June 1 982 to June 1 983 . In this group selective decontamination of the digestive tract was started as soon as possible after admission to the ICU . Systemic antibiotic prophylaxis (ccfotaximc 50 mg/kg body wt/day) was started on admission and continued until the patient was free of PPM. The colonisation and infection rate were prospectively analysed . All patients were daily evaluated for the clinical signs of infection . As the capacity of the ICU had been enlarged in 1 98 1 . more patients were admitted to our unit , who would otherwise have been transferred to another ICU in the hospital .
Bacteriological surveillance cultures of patients material , including oropharyngeal and rectal swabs (or faeces) , urine , tracheal aspirate and wound swabs were taken within 24 h after admission ( inventory) and thereafter thrice weekly or more frequently when there were signs of infection . B lood cultures were taken (x3) when the rectal temperature rose above 39°C. Standard methods for culturing, identification and typing were used (van Saene et a l . , l 983a) . In throat cultures attention was only paid to Gram-negative PPM and Staphylococcus aureus. No special effort was made to isolate Haemophilus influenzae or Streptococcus pncu
moniae from the throat.
SDD regimen
The oropharyngeal cavity was selectively decontaminated with a sticky paste (Orabase®) containing polymyxin E 2% , tobramycin 2% and amphotcricin 8 2% . This was applied to the oral mucosa four times daily with a prefi l led disposable syringe and spread evenly with a gloved finger. The gut was selectively decontaminated with the same nonabsorbable antibiotics (polymyxin E 4 x 1 00 mg, tobramycin 4 x 80 mg and amphotericin 8 4 x 500 mg) administered through the gastric tube four times daily. Following administration the gastric suction was discontinued for one hour.
22

In group II (SOD) the first dcfaccation after admission to the ICU was recorded .
Definitions
In this study the following definit ions arc used:
Colonisation: is the presence of the same species of PPM in an organ system for more than 3 days (>2 positive samples) , without signs of infection. Colonisation wa� assumed to begin with or to continue up to the first sample free of that PPM (extrapolation) . Endogenous infection: infection caused b y PPM that have first colonised the digestive tract . These PPM can either be part of the 'normal' resident flora (primary endogenous) or be newly acquired PPM that have colonised the digestive tract (secondary endogenous) . Many of the latter group do not belong to the normal indigenous flora . Exogenous infection: infection caused by PPM isolated from the site of infection only without previous colonisation of the digestive tract. Using standard biochemical methods for identification and typing an infection was assumed to be endogenous when the same specie� of PPM was found in the oropharynx or the intestines before or simultaneously with isolation from sputum , urine or wounds. Infection has been defined according to generally accepted criteria (Northey ct al . , 1 974; Thorp ct a l . , 1 979) . Respiratory tract infection (RTI) was diagnosed on purulent sputum (Gram-stain) and dense growth in bacteriological cultures from tracheal aspirate . The diagnosis lower RTI was made on physical and radiological signs of pulmonary infi ltration, fever and lcucocytosis . Urinary tract infection (UTI) was diagnosed on a bacteriological culture from catheter urine of more than JO� PPM/ml . The diagnosis of wound infection was based on purulent discharge from wounds on Gram-sta in, a positive culture and signs of inflammation. Only bactcriologically confirmed scpticaemias were recorded . Blood cultures yielding Staphylococcus epidermidis were considered positive if the same strain of S. epidermidis was isolated at least twice .
Statistical analysis
The data from both groups were analysed using the Chi-square test with Yates correction and the Student's t-tcst to compare means. A p-value of less than or equal to 0.05 was considered statistical ly significant .
Results
Patient characteristics of both groups are summarised in Table I . The two
23

groups were comparable with respect to sex, age, length of stay in the ICU and traumascore (Student's t-test ) .
Colonisation pattern of the oropharynx
On admission 24/59 (41 % ) of patients of group I (control) carried S. aureus and 22/59 (37%) of patients were found positive for one or more Gram-negative PPM in the throat . S. aureus gradually disappeared during stay in the ICU. whereas the
Table I . Patient� characteristics.
GROUP I GROUP I I (Control) (SOD)
Enrolled in study 59 63 n .s .
Age (yr)" 37 ± 21 35 ± 1 9 n .s . range (yr) (7 - 8 1 ) ( I 89)
Male/female 4 1 / 1 8 48/ 1 5 n . s .
Stay (days)" 1 4 ± JO I I ± 8 n .s. range (days) (5-68) (5 -46)
HTI-ISS" 33.7 ± 1 3 . I 34.4 ± 14 .9 n .s . range ( 1 4- 75) (9 75)
" Data are given a� mean ± SD
� 10�' a. � gram + PPM OAOPHAAYNX 90
;:: 80 - gran - PPM
8 70
�
60 so
u
:!' z "'
� 10 " 12 1l 14 15
(i:;J E col RECTUM
100'l' - other gram-PPM
8 � c:S u
:!' z "' � oe.
10 12 1l �vsJcu
Figure I : Number of patients in group I (control) colonised by P P M in the oropharynx and intestines. The majority of patients was rapidly colonised by I CU-a�sociated Gram-negative bacil l i in the oropharynx and later in the rectum .
24

colonisation rate with Gram-negative PPM simultaneously increased (Fig. I ) . After 1 5 days 1 21 1 4 (86% ) patients were colonised with one or more types of Gram-negative PPM (Klebsiclla and Proteus spp. etc) and none with S. aureus.
After three weeks Klcbsiclfo and Pseudomonas spp . predominated (Table 2 ) .
Tahle 2 . Oropharyngeal coloni,ation during ICU-stay.
Group I (control) Group II (SOD)
PPM day I day I S day 2 1 day I day 1 5 day 2 1 Specie' n =S<J n 1 4 n = 6 n=6:1 n 14 n = 6
S . aurcu't 24 1 5 Klehsidla spp. I l l 7 :i 2 E. coli 6 7 Entcrohactcrspp. s 2 I Proteus 'PP· 4 3 :i Citroh;Ktcr,pp. 4 I p,cudomon.1.\ 'PP· 2 2
Total coloni,ation 37/59 1 21 1 4 5/6 26/63 0/ 1 4 0/6 r.1te ofpatieni-·• (63"u) (86'Y., ) ( 8 1 'X. ) ( 4 1 % ) (0% ) (0% )
·' A� many paticnh were coloni,ed with more th.in one 'pec1c,. the tot.ti numher of coloni,ed patienh m.1y he ,m.,ller than the 'um of i'olated PPM.
In group II (SOD) 1 5/63 (24'Yo ) of patients carried S. aureus in the throat on admission and 1 3/63 (2 1 'Yc. ) of patients were found positive for one or more Gramnegative PPM. In the following days the colonisation rate decreased (Fig. 2) . The difference in colonisation rate between the first and fol lowing days was significant after two days (p<0.02) . No secondary colonisation was found in th is group (Table 2) .
Colonisation pattern of the intestines
From six patients of the control group inventory rectal cultures were not carried out . From the remaining 53 patients 28% carried aerobic Gram-negative PPM other than Escherichia coli in the rectum (Fig. I ) . The (resident) E. coli is considered separately from other Gram-negative PPM in order to facil itate determination of secondary colonisation with PPM acquired in the ICU. During ICU-stay the colonisation rate with E. coli remained the same. However, most patients became rapidly colonised by aerobic ICU-acquired PPM (Fig. 2), predominantly Pseudo
monas aeruginosa, Proteus and Acinetobacter spp. (Table 3) . In group I I (SOD) 7/63 { I I % ) of patients carried aerobic Gram-negative PPM
other than E. coli in the rectum on admission . The colonisation by E. coli gradually decreased (Fig. 2) . Secondary colonisation by Gram-negative baci l l i occurred in 9/63 ( 1 4% ) patients in the first 2 weeks. Ten strains of PPM were isolated (Pseudomonas spp. 4x , Enterobacter spp. 3x, Acinetobacter 2x, Serratia spp.
25

Figure 2:
100'!. 90
� gram · PPM - gram- PPM
OROPHARYNX
§ E co! RECTUM
- Olhergam-PPM
10 11 12 13 14 15
10 11 12 13 14 15 DAYS IN ICU
Colonisation rate of selectively decontaminated patients in group I I (SDD). PPM were effectively e l iminated from the oropharyngeal cavity. within 3 days. Secondary coloni�ation of the intestine� was largely prevented. A significant reduction of rectal nora was achieved after 7 days (p<0.01 ) .
l x) . I n al l cases these colonising PPM were sensitive to one of the antibiotics used for selective decontamination . In four patients these PPM disappeared without changing the antibiotic regimen. Five patients could not be further evaluated because they were discharged from the ICU. The difference in colonisation rate between admission and fol lowing days was significant after 7 days (p<0.01 ) . Twenty-four patients passed stools during their stay in the ICU. The median duration of stay before defaecation was 8 days (range 3-27 days , mean IO days). In 2 1 /24 patients the rectum was free of PPM after the first defaecation .
The infection rate in both groups is presented in Table 4. Since many patients had mixed Gram-positive and Gram- negative infections and/or more than one infection, the sum of i nfections exceeds the number of infected patients. I n group I (control) 48/59 (81 % ) patients suffered from 94 infectious episodes.
In group I I (SOD ) I0/63 ( 1 6% ) patients had 1 1 infections, a highly significant difference (p<0.00 1 ) . In the infected patients cefotaxime proved to be an appropriate antibiotic except for two patients with (endogenous) wound infections. They responded however, to adjustment of antibiotic therapy and to surgical treatment. The duration of cefotaxime prophylaxis in group II was 9 .3 ± 4.8 days (mean ± SD) range 3-26 days .
26

T;ihle J. Intestinal coltmis;ition with PPM (other than E. coli) during ICU-stay.
Group I (control) Group II (SDD)
PPM day I day 1 5 day 2 1 day I day I S day 2 1 Species n- 5J n - I Jh n=6 n=63 n = 1 4 n == 6
Protcus�pp. 7 4 2 2 Pseudomonas spp. J 5 Acecinobacterspp. 4 2 Entcrobactcrspp. J 2 Citrobactcr spp. J Klcbsiclla spp. 2 2 3 Scrratia spp.
Total colonisation I J/5J I 0/ 1 3 6/6 7/63 1 / 1 4 0/6 rate of patients" (28% ) (77%) ( 100%) ( 1 1 % ) (7% ) (0%)
" As many patients were colonised with more than one species, the total number of colonised patients may he smaller than the sum of isolated PPM.
h From I patient rectal culture� were not evaluable on day 1 5 .
Table 4. Infection rate during ICU-stay.
Group I Group I I (Control) (SDD)
Site N =59 N -63
Respiratory tract 35 (59%) 5 (8%) Gram + 24 3 Gram - 25 3
Urinary tract 1 9 (32% ) 1 (2% ) Gram + 9 Gram - 1 3
Blood 25 (42'}\, ) 2 (J%) Gram + 20 2 Gram - 1 3
Wounds 1 5 (25 % ) 3 (5%) G ram + 1 0 Gram 8 3
Total number of infections 94 I I
Total number of infected patients 48 ( 8 1 % ) I O ( I 6% )
X'-value P-value df= l 20
X1=34.2 P<0.00 1
x�- 1 8.7 P«H>O I
X1=24.9 P<0.00 1
X1=8.8 P<0.0 1
X1=49.8 P<0.001
A� many patient\ had more than one infection and/or mixed Gram-positive and Gram-negative infections. the �um of infections exceeds the number of infected patients.
In both groups most infections were endogenous infections ( i . e . the same species of PPM was cultured from the site of infection as well as from the digestive tract) (Table 5 ) . Exogenous PPM ( i .e . PPM found only at the site of infection and not in the digestive tract) were particularly important as cause of septicaemia in group I (30%) .
27

Table 5 . Endogenou' infections.
Site
Re,piratory tract infection' Number of PPM i'olatcd Endogenou' PPM
Urinary tract infection' Number of PPM isolated Endogenous PPM
Septicaemia Numberof PPM isolated Endogenou' PPM
Wound infection' Number of PPM i'olated Endogenous PPM
Group I (Control ) N = 59
35 68 63 (95°0 )
1 9 30 29 (97"{, )
25 50 35 (70° .. )
1 5 24 2 1 (88% )
Table 6. Bacteriological 'urveil lance cultures of tracheal aspirate.
Group I Group I I (Control) (SOD)
Site N - 59 N = 6J
Respiratory tract Total number of cultures 459 298 Number of po,itrve culture' 3 1 9 (69"0) 27 (9" .. )
Number of PPM isolated 442 32 Gram + I J 2 1 5 Gram - 264 14 C. a/bicans 46 3
Table 7. Bacteriological surveillance cultures of urine.
G roup I Group I I (Control) (SOD)
Site N - 59 N = 63
Urinary tract Total number of cultures 346 3 1 9 Number of positive cultures 1 2 1 (35 % ) 2 1 (7%)
Number of PPM isolated 1 50 25 < H r' PPM/ml 62 20 � 1 0·' PPM/ml 59 I
Gram + 46 1 6 G ram- 6 1 9 C. albicans 43 0
28
Group I I (SOD) N "' 63
s 7 4 (57% )
0 (0" .. )
2 2 0 (0° .. )
3 5 5 ( 1 00"1., )
X'-valuc p-valuc
X' = 263 . 5 P«UlOI
x�-valuc p-value
x� =78 o P<0.00 1

Tables 6 and 7 show the results of bacteriological surveillance cultures from tracheal aspirate and catheter urine specimens. The number of posi tive cultures (including both colonisation and infection) is significantly lower in de SOD group than in the control group (p<0.001 ) .
Discussion
The patients included in this study were al l at h igh risk of infection . The severity of the inj uries, the duration of stay (>5 days) and the use of invasive instrumentation e .g. endotracheal intubation, urinary catheter, central venous lines, al l enhanced the colonisation and infection risk (Freeman & McGowan , 1 978) . The h igh incidence of infections in our historical control group (8 1 % ) is in accordance with figures from other studies (Northey et a l . , 1 974; Thorp et a l . , 1 979) . The major infectious problem was colonisation and infection of the respiratory tract, a well-known phenomenon in mechanically ventilated ICU-patients (Johanson et al . , 1 972; La Force, 1 98 1 ) .
In our study we found that most infections in group I (control) were endogenous: the oropharyngeal flora being the source for RTI and wound infections and the rectal flora being the source for UTI and wound infections. Although the importance of the digestive tract flora as a major source of infection has been demonstrated in leukaemic patient� (Schimpff et al . . 1 972) and also in ICU-patients (Johanson et al . , 1 972 ; Schwartz et al . , 1 978; La Force , 1 98 1 ; van Uffelen et al . , 1 984) , this aspect has been overshadowed by the apparent importance of exogenous infections in the ICU (Gaya, 1 976; Daschner et al . . 1 982) . Endogenous infections can be subdivided into primary endogenous infections (caused by PPM from the normal resident flora) and secondary endogenous infections (caused by newly acquired PPM colonising the digestive tract) . We found that secondary colonisation of the digestive tract is an essential stage in the development of infections. During colonisation of the digestive tract PPM can rapidly increase in number which may lead to subsequent colonisation and infection of the major organ systems.
Multiple trauma patients are l ikely to have a normal flora before the accident . However, after admission to the ICU the endogenous flora of the oropharynx and intestines may change profoundly and most patients become colonised b}'. endemic ICU-strains of PPM (Fig. 1 ) in the digestive tract . Thus many apparently exogenous infections were really secondary endogenous infections.
The normal oropharyngeal flora consists predominantly of Streptococcus viri
dans ( 10 7/ml) and anaerobes ( 1 09/ml ) . Approximately 30% of healthy individuals carry S. aureus, H. influenzae or S.
pneumoniae in the t hroat . These PPM (S. aureus in particular) are responsible for a large number of early respiratory tract i nfections and pulmonary septicaemia
29

(Romano et al . , 1 979 ; Espersen & Gabrielsen, 1 98 1 ) . These primary endogenous infections cannot be prevented by SOD, since it takes a few days to eliminate PPM from the resident flora. Thus a systemic (CR-indifferent) antibiotic is necessary to prevent these infections.
Oropharyngeal colonisation with Gram-negative baci lli is rare in healthy individuals (Rose bury, 1 962) . Increased colonisation is related to the severity of the underlying disease (Johanson et al . , 1 969) , to old age and to antibiotic use (Yoshioka et al . , 1 982). The most important factor determining colonisation appears to be an increased adherence of bacil l i to the mucosa due to alteration of the epithelial surface (Johanson et al . , 1 980) . Important normal cleansing mechanisms of the oral cavity are swallowing, salivary flow, mucus, IgA (Will iams & Gibbons, 1 972 ; La Force et al . , 1 976) and bacterial interference of the normal oropharyngeal flora (Sprunt & Redman , 1 968) . In ICU-patients however, the condition of the patient and the treatment interfere with these cleansing mechanisms e.g. coma, sedatives, incapacity of swallowing, instrumentation, antibiotics , while the exposure to ICU-associated Gram- negative bacil l i is very high (Rosendorf et al . , 1 974) e .g other patients, food . The combination of an increased adherence , impaired oral defense mechanisms and a h igh exposure might explain the very rapid colonisation by Gram- negative baci l l i in the oral cavity and intestines in multiple trauma patients. The disappearance of S. a ureus from the oral cavity is probably the result of antibiotic treatment. The oropharyngeal colonisation rate on admission in both groups is greater than expected for normal healthy individuals (Rosebury, 1 962) and may reflect the rapid acquisit ion and colonisation of PPM.
The difference in colonisation rate between the two groups on admission could be explained by the fact that many inventory samples in group I (control) were ac
tually taken the morning after admission , while in Group I I (SOD) the samples were taken without delay before starting SOD. The intestinal flora showed a similar pattern of secondary colonisation by Gram-negative PPM (Fig. I ) , replacing the normal flora. In a healthy individual the stomach and small gut are free of aerobic Gram-negative bacill i . The normal colonic flora consists of large numbers of anaerobes ( 1 01 1/ml), enterococci ( 1 05/ml) and Enterobacteriaceae , predominantly E. coli ( 1 05/ml ) . A large number of different factors control the colonisation pattern of the gut by aerobic PPM. These factors include peristalsis, acidity of the stomach , bile secretion , mucus, IgA , eel desquamation and the anaerobic flora (van der Waaij , 1 979).
In ICU patients peristalsis is frequently impaired or absent, the pH of the stomach is often high (e .g . antacids) , the secretion of bile and mucus decreased and the anaerobic flora can be affected by antibiotic treatment (e.g. penicill ins such as ampici l l in) . At the same time the exposure to ICU-associated (multiple resistant) Gram-negative PPM is often h igh (Le Frock et al . , 1 979) e.g. from the oral cavity,
30

tube feeding, instrumentation . In ICU-patients it has been found (Du Moulin et a l . , 1 982; Hi l lman et a l . . 1 982) that heavy colon isation of the stomach with Gramnegative bacil l i may occur within 24 hrs and that this could be a source of infection of the respiratory tract (Du Moulin et al . , 1 982) . In our study we found that colonisation of the rectum by ICU-strains took longer. The majority of patients in the control group were colonised in the rectum with ICU-associated PPM after I 0 days (Fig. I ) . reflecting the recovery of the intestinal function .
The technique of infection prevention in this study is a combination of SOD (nonabsorbable antibiotics) with a systemic CR-indifferent antibiotic prophylaxi� (cefotaxime) . SOD is particularly directed against secondary colonisation by aerobic Gram-negative PPM. Cefotaxime prophylaxis, directed against early endogenous infections, could be discontinued as soon as the patient was free of PPM (mean 9 days) . Since respiratory tract infections arc the most frequent infections in intubated and ventilated patients, selective decontamination of the oropharyngeal cavity is essentia l . The topical application of antibiotics dissolved in a �ticky paste to the oral mucosa. resulted in a rapid el imination of PPM from the oral cavity (Fig. 2) without secondary colon isation with (resistant) PPM .
Selective decontamination of the gut was more difficult because many patients had no gastro-intestinal function for more than one week . After four days the colonisation rate decreased (Fig. 2). Secondary colonisation occurred in 9 patients in group I I . On no occasion were the PPM resistant to both antibiotics included in this decontamination regimen. As soon as the patient had normal bowel funtion the rectum became free of PPM and secondary colon isation was not observed.
This technique resulted not only in a highly significant reduction of the number of positive cultures from sputum and urine (reduction of colon isation of RT and UT) but also in a significant decrease of the infection rate . Since cultures were taken daily when there were severe infections, the total number of cultures of tracheal aspirate and of urine taken in group I I actually decreased reflecting the decrease in infection rate .
The generally accepted policy for infection control in the ICU concentrates on cross-contamination and subsequent infection . I t is based on controll ing environmental sources of infection e .g . sinks, nebulizers and on interrupting the transmission of PPM to patients by isolation measures, barrier nursing, handwashing etc. (Gaya , 1 976 ; Daschner et a l . , 1 982; Stoddart , 1 983) . However, these measures seem to be of l imited value (Preston et al . , 1 98 1 ) since the major source of PPM, being the patient's digestive tract flora, is not effectively el iminated .
Infection prevention by elimination of the endogenous source of infection not only lowers the risk of infection for the individual patient , but also has important epidemiological consequences. Each decontaminated patient no longer acts as a source of PPM for his environment and neighbouring patients. I t has been shown
3 1

(Miranda et al . . 1 983) that since the introduction of SOD in our ICU an important reduction of the contamination level of the environment was ach ieved, without special cleansing procedures. The reduction of exposure to ICU-associated PPM may have been a very important factor contributing to the efficacy of SOD in ICU-patients. Furthermore , it could be an explanation for the relatively low number of exogenous infections in the SOD-treated patients.
Conclusions
Selective decontamination of the digestive tract in critically i l l ICU patients with mul tiple injuries proved to be particularly effective against secondary colonisation of the oropharynx and intestines by ICU-associated Gram-negative PPM. Additional systemic antibiotic prophylaxis i s necessary to prevent early endogenous infections. The suppression and (later) elimination of the endogenous PPM resulted not only in a reduction of colonisation of the respiratory and urinary tract but also in a reduction of the infection rate from 81 % to 1 6% . Resistance against the antibiotics used for SOD or against the prophylactic cefotaxime was very rare. We feel that the emergence of resistance against systemic antibiotics is effectively prevented by SOD (study in progress).
Acknowledgements
We thank the nurses of the ICU and the technicians of the microbiology laboratory for their cooperation. Without their help this study would not have been possible. We thank Prof. D. van der Waaij for his help and for the many valuable comments in preparing the manuscript . We thank Douglas Newton for reviewing the manuscript , Wil Noordik for the secretarial help and Jack Duitsch for preparing the i l lustrations.
32

Chapter 3
The prevention of superinfection in multiple trauma patients
Ch. P. Stoutenbeck. H. K. F. van Saene . D. R. Miranda . D. F. Zandstra and B. Binnendij k - �
Dcp.1rtmcnt o f Anc,thc,iolog} and I ntcn\lvc C.1rc. Dcp.trlrncnt o f Clinical Bactcnolog} Department of Tr.1urnatology . Univcr�ity Ho,pit,1 1 . Groningen. The Neth.:: rland'
Journal of Antimicrobial Chemotherapy 1 4 , Suppl . B, 203 ( 1 984)
33

Summary
In a control group of 59 multiple trauma patients requiring prolonged intensive care , a conventional restrictive antibiotic policy was followed. Forty-eight patients (8 1 % ) developed 94 infections. Fifty-one patients received systemic antibiotic therapy with one or more drugs. The total quantity of systemic antibiotics used was very high ( l 8.3 ± 22. l antibiotic days per patient ) . This policy resulted in a very h igh incidence of superinfections (24'Yo ) with multiple-resistant Gramnegative bacteria , mostly emerging from the digestive tract ( i . e . secondary endogenous infection�). Five patients died with infection.
A novel technique of infection prevention , based on the maintenance of the colonisation resistance and on selective decontamination of the digestive tract in combination with systemic antibiotic prophylaxis with cefotaxime , proved to be very effective . Out of 63 multiple trauma patients, intubated and venti lated for 5 days or more in the ICU, ten patients ( 1 6%) developed 1 1 infections. Most infectiom. occurring under this regimen were primary endogenous infections which were treated by continuation of cefotaxime. Only two patients (3% ) developed a superinfection with cefotaxime-resistant Gram-negative bacteria . No patient died. This approach to i nfection prevention in the ICU shows that prophylactic administration of antibiotics significantly reduced the infection rate of critically i l l patients without the development of superinfection .
Introduction
Multiple trauma patients who require prolonged Intensive Care and mechanical ventilation , have a very high risk of infection (Schimpff et a l . , 1 974; Freeman & McGowan . l 978; Daschner et al . , 1 982) . The predominating potential ly pathogenic microorganism� causing infection in the ICU are aerobic Gram-negative bacil l i . Most infections are endogenous ( i .e . those caused by organisms from the oral or intestinal flora) . Infections due to the indigenous flora (e.g. Streptococcus
pneumoniae, Escherichia coli) are referred to as 'primary endogenous infections' . These are generally sensitive to many antimicrobial agents. However . once a patient is hospitalised the indigenous aerobic flora is replaced by hospital organisms. ICU-patients arc rapidly colonised with nosocomial Gram-negative bacteria (e.g. Pseudomonas, Acinetobacter, Klebsie/la spp. ) , not only in the oropharynx (Northey et al . , 1 974; Rose & Babcock, 1 975 : Laforce , 1 98 1 ) , but also in the stomach (Du Moulin et al . , 1982) and in the intestines (Le Frock et al . , 1 979) . I n this stage (colonisation of the digestive tract) , potentially pathogenic microorganisms may rapidly increase in number with subsequent colonisation and infection of the major organ systems (Stoutenbeek et al . , 1 984) . Infections caused by bacteria from the digestive tract , but that do not belong to the indigenous flora are defined as 'secondary endogenous' infections.
34
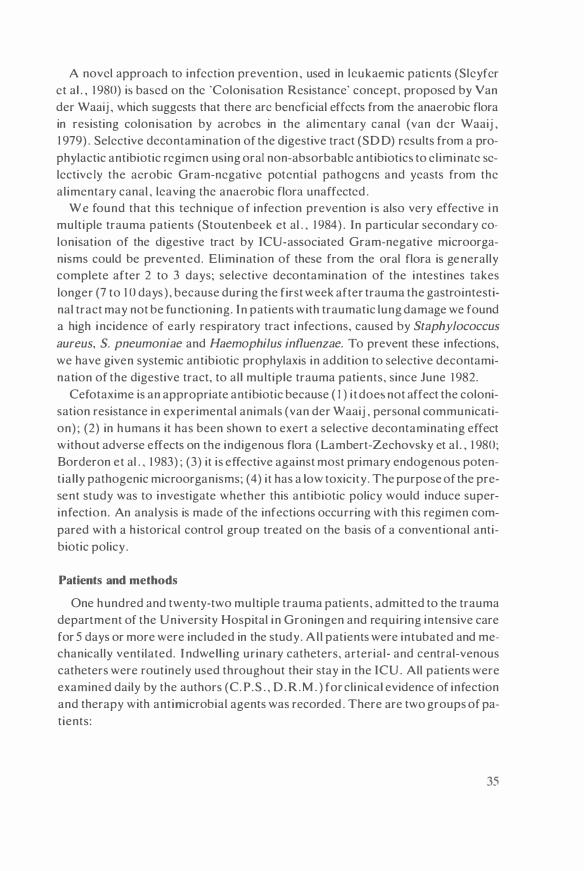
A novel approach to infection prevention , used in lcukaemic patients (Sleyfcr ct al . , 1 980) is based on the 'Colonisation Resistance' concept, proposed by Van der Waaij , which suggests that there arc beneficial effects from the anaerobic flora in resisting colon isation by acrobcs in the alimentary canal (van dcr Waaij , 1 979) . Selective decontamination of the digestive tract (SD D) results from a prophylactic antibiotic regimen u�ing oral non-absorbablc antibiotic� to el iminate selective ly the aerobic Gram-negative potential pathogens and yeasts from the alimentary canal , leaving the anaerobic flora unaffected .
We found that this technique of infection prevention i s also very effective i n multiple trauma patients (Stoutenbeek et al . , 1 984) . In particular secondary colonisation of the digestive tract by ICU-associated Gram-negative microorganisms could be prevented. Elimination of these from the oral flora is generally complete after 2 to 3 days; selective decontamination of the intestines takes longer (7 to 1 0 days) , because during the first week after trauma the gastrointestinal tract may not be functioning. In patients with traumatic lung damage we found a high incidence of early respiratory tract infections, caused by Staphylococcus
aureus, S. pneumoniae and Haemophilus influenzae. To prevent these infections, we have given systemic antibiotic prophylaxis in addition to selective decontamination of the digestive tract, to all multiple trauma patients, since June 1 982.
Cefotaxime is an appropriate antibiotic because ( I) i t doe� not affect the colonisation resistance in experimental animals (van der Waaij , personal communication) ; (2) in humans it has been shown to exert a selective decontaminating effect without adverse effects on the indigenous flora (Lambert-Zechovsky et al . , 1 980; Borderon et al . , 1 983) ; (3) it is effective against most primary endogenous potential ly pathogenic microorganisms; (4) it has a low toxicity. The purpose of the present study was to investigate whether this antibiotic policy would induce superinfection. An analysis is made of the infections occurring with this regimen compared with a h istorical control group treated on the basis of a conventional antibiotic policy .
Patients and methods
One hundred and twenty-two multiple trauma patients, admitted to the trauma department of the University Hospital in Groningen and requiring intensive care for 5 days or more were included in the study. Al l patients were intubated and mechanically ventilated. I ndwell ing urinary catheters, arterial- and central-venous catheters were routinely used throughout their stay in the ICU . All patients were examined daily by the authors (C. P.S . , D .R . M . ) for clinical evidence of infection and therapy with antimicrobial agents was recorded . There are two groups of patients:
35

Group I (control)
Fifty-nine patient� admitted to the ICU in 1979 and 1980. This group has been studied retrospectively. They did not rece ive any antibiotic prophylaxis. Therapy was given only on strict clin ical and bacteriological evidence of infection . guided by the sensitivity pattern. Serious infections were usually treated with a combination of cephalosporins and aminoglycosides. If the patient fai led to respond to therapy. metronidazol was added even if anaerobes had not been cultured.
Group II (Selective decontamination)
Sixty-three patients admitted to the ICU from June 1 982 to June 1 983. In this group selective decontamination of the digestive tract was started as soon as possible after admission to the ICU . Systemic antibiotic prophylaxis ( cefotaxime 50-60 mg/kg hw/day) was started on admission. In heavily contaminated patients tobramycin (3-4 mg/kg/day iv) was added prophylactically. Systemic antimicrobial prophylaxi!> was continued until the patient was effectively decontaminated . The colonisation and infection rates were prospectively analysed.
The Injury Severity Scores (ISS) were determined for each patient . using the Hospital Trauma Index (HT! ) (Goris & Draaisma. 1 982).
Bacteriology
Bacteriological survei l lance cultures including oropharyngeal and rectal swabs (or faeces) . urine . tracheal aspirate and wound swabs were taken on admission and thereafter thrice weekly or more frequently when there were signs of infection . Three blood cultures were taken (3x) when the rectal temperature rose above 39°C. Standard methods for culturing. identification and typing were used (van Saene et al . . I 983a) .
Selective decontamination of the digestive tract (SDD) has been described in detai l elsewhere (Stoutenbeek et al . . 1 984 ) : the oropharyngeal cavity was selectively decontaminated by an antibiotic ointment (Orabasell<l) containing 2% of polymyxin E. tobramycin and amphotericin B . The gut was selectively decontaminated with oral nonabsorbable antibiotics (polymyxin E 4x I 00 mg, tobramycin 4x80 mg and amphotericin B 4x500 mg) administered through the gastric tube . After each administration gastric suction was discontinued for one hour.
Definitions
Defin itions used for colonisation and infection have been previously described (Stoutenbeek et a l . . 1 984) . On the basis of standard biochemical methods for identification and typing, an infection was assumed to be endogenous when the same species of organisms was found in the oropharynx or the intestines before or
36
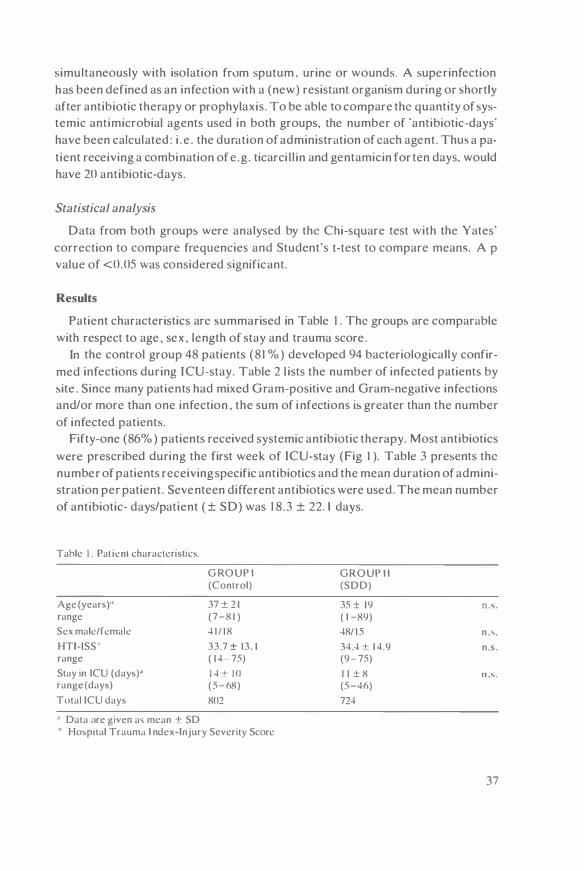
simultaneously with isolation from sputum , urine or wounds. A superinfection has been defined as an infection with a (new) resistant organism during or �hortly after antibiotic therapy or prophylaxis. To be able to compare the quantity of �ystemic antimicrobial agents used in both groups, the number of 'antibiotic-days· have been calculated : i . e . the duration of administration of each agent . Thm a patient receiving a combination of e .g . ticarci l l in and gentamicin for ten days. would have 20 antibiotic-days.
Statistical analysis
Data from both group� were analysed by the Chi-square test with the Yates' correction to compare frequencies and Student's t-test to compare means. A p value of <0.05 was considered significant.
Results
Patient characteristics arc �ummarised in Table 1 . The group� are comparable with respect to age , sex , length of stay and trauma score .
In the control group 48 patients (8 1 % ) developed 94 bacteriologically confirmed infections during ICU-stay. Table 2 l ists the number of infected patients by �ite . Since many patients had mixed Gram-positive and Gram-negative infections and/or more than one infection , the sum of i nfections is greater than the number of infected patients.
Fifty-one (86%) patients received systemic antibiotic therapy. Most antibiotics were prescribed during the first week of ICU-stay (Fig 1 ). Table 3 presents the number of patients receiving specific antibiotics and the mean duration of administration per patient . Seventeen different antibiotics were used. The mean number of antibiotic- days/patient ( ± SD) was 1 8.3 ± 22. l days.
Tahlc I . Pat ienl characlenstics.
Age (yearsr• range
Sex male/female
HTl-ISS" range
Stay in ICU (day,)" range (day>)
Total ICU days
·' Data :ire given a� mean + SD
G ROUP I (Control)
37 ± 2 1 (7-8 1 )
4 1 / 1 8
33.7 ± 13 . 1 ( 1 4- 75)
1 4 ± 10 (5-68)
802
Hospital Trauma I ndex-Injury Severity Score
GROUP I I (SOD)
35 ± 19 ( l -89)
48/ 1 5
34.4 + 1 4.9 (9- 75)
1 1 ± 8 (5-46)
724
n ... .
n ....
n .s .
37

Table 2. Infection rate during ICLJ-,tay.
Group I I Selective gut
Group I dec<mtamination X'-\ ;due (Control) ( +cefotaxime) P-value
Site n=SlJ 11=63
Infected pat1en1' .J8 ( 8 1 °o ) 1 0 ( 1 6°0 ) Respiratory tract 35 ( 'ilJ" o ) 5 (8°u ) x � 3.J.2
Gram + 2.J 3 P<O OO I Gram 25 3
Urinary tract 1 9 (32°0 ) I (2" .. ) x-- 1 8 . 7 Gram + l) P<O OO I Gram 1 3
Blood 25 { 42 " o ) 2 ( 3 ° o ) X ' 2.J .lJ Gram + 20 2 P<0.00 1 Gram 1 3
Wounds 15 ( 25 " o ) 3 ( 5 ",o ) X' = 8 . 8 Gram + 1 0 P<0.0 1 Gram 8 3
Total infection' l).J I I
As many patients had more than one infection and/or mixed Gram-po,1t1\ e and Gram-negative infection, . the �um of infection� exceed� the number of infected patienh.
Table 3 , Usage of 'Y�temic antimicrobial agenb.
Cefotaxime
Cephrad1ne/Ccfuroxime
Tobramycin/gentamicin
Metronidazol
Carben ici I Ii n/tica rci l I i n
Mi�cellaneou�
Number of patients with systemic antibiotic�
Total antibiotic day�
Total antibiotic days/ patient
data are given a' mean ± SD
No. of patient� ("<, ) and antibiotic day,/patient in
Group I (Control)
.J� ( 76 " o ) 8 . 3 ± 5 .2
32 (5.J"'o ) lJ . 3 ± 7.2
1 8 (3 1 % ) 8 . 7 + .J . lJ
1 3 ( 2 2 % ) 7 . 3 + 3 . 2
1 7 (29° 0 ) 8 . 2 ± 8.5
5 1 (86% )
1 062
1 8. 3 ± 22
• • In group I I no gentamicin has been u�ed
38
Group I I Selective gut decontamination ( +Cefotaxime)
63 ( 1 00 % ) lJ . 3 ± .J. 8·
2 ( 3 % ) 7.5 2lJ ( .J 5 ° o ) ''* 7.5 ± 5 . 2
3 ( 5 % ) 1 3 . 7 ± 1 3 . 3
2 ( 3 % ) 1 2.5
63 ( 100% )
883
1 3 .9 :f: 1 3 . 1
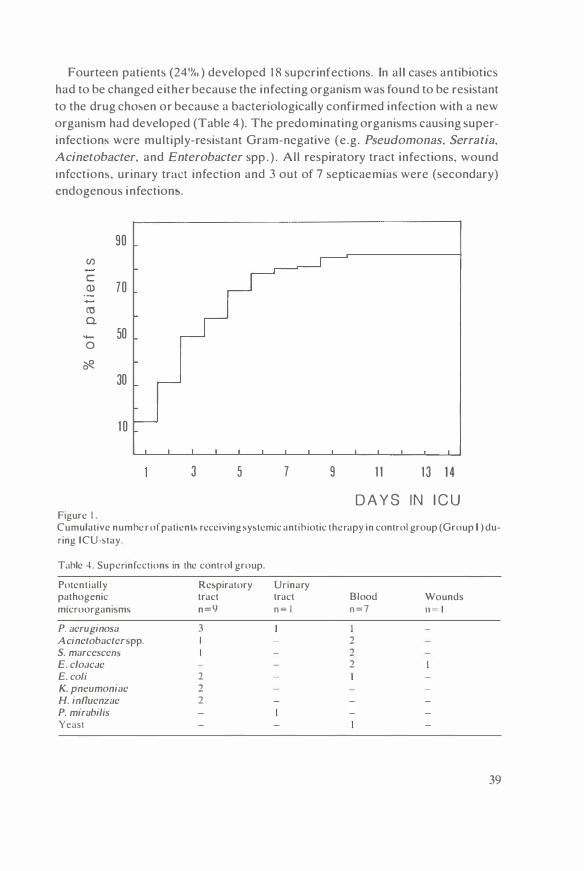
Fourteen patients (24'Yc. ) developed 1 8 superinfections. In al l cases antibiotics had to be changed either because the infecting organism was found to be resistant to the drug chmen or becau�e a bacteriologically confirmed infection with a new organism had developed (Table 4 ). The predominating organisms causing superinfection� were multiply-resistant Gram-negative (e.g. Pseudomonas. Serratia.
Acinetobacter, and Enterobacter spp . ) . All respiratory tract infections, wound infection�. urinary tract infection and 3 out of 7 septicaemia� were (secondary) endogenous infections.
90
(/) c a> 70
cu 0.
50 0 �
30
1 0
3 5 7 9 1 1 1 3 1 4
D A Y S I N I C U Figure I . Cumulative numhc r of patient' rece1ving �y�tcmic antihiotic therapy m control group (Group I ) during ICU-stay.
Tahle .i . Supennfcction' in the control group.
Potentially pathogenic m1croorgani�m'
P. acruginosa Acinctobactcnpp. S. marcesccm E. c/oacJc E. coli K. pneumoniac H. influcnzac P. mirabilis Yeast
Rc�piratory tract n = 9
3 I
2 2 2
Urinary tract n = I
Blood n =7
2 2 2
Wounds n - 1
39
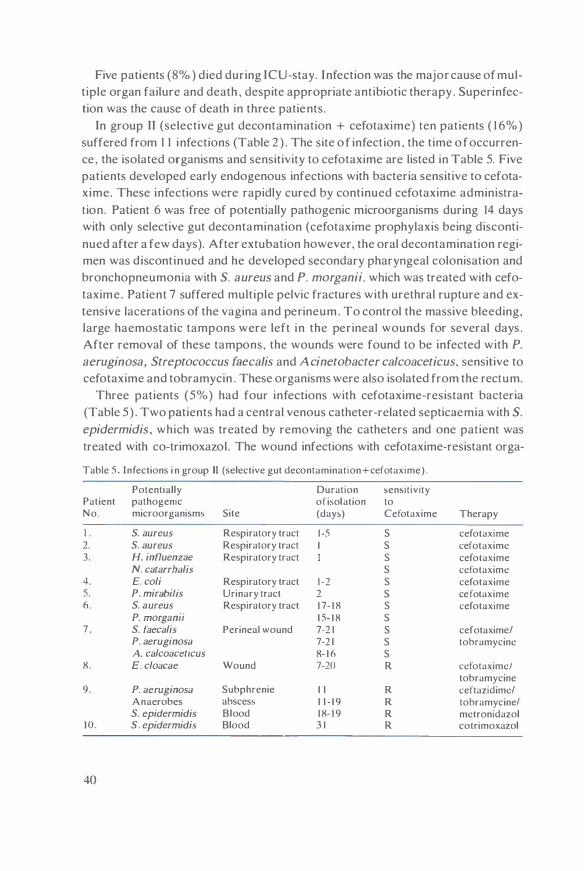
Five patients (8% ) died during ICU-stay. Infection was the major cause of multiple organ failure and death , despite appropriate antibiotic therapy. Superinfection was the cause of death in three patients.
In group II (selective gut decontamination + cefotaxime) ten patients ( 1 6%) suffered from I I infections (Table 2 ) . The site o f infection , the time o f occurrence , the isolated organisms and sensitivity to cefotaxime are listed in Table 5. Five patients developed early endogenous infections with bacteria sensitive to cefotaxime. These infections were rapidly cured by continued cefotaxime administration. Patient 6 was free of potentially pathogenic microorganisms during 14 days with only selective gut decontamination (cefotaxime prophylaxis being discontinued after a few days). After extubation however, the oral decontamination regimen was discontinued and he developed secondary pharyngeal colonisation and bronchopneumonia with S. aureus and P. morganii, which was treated with cefotaxime. Patient 7 suffered multiple pelvic fractures with urethral rupture and extensive lacerations of the vagina and perineum . To control the massive bleeding, large haemostatic tampons were left in the perinea( wounds for several days . After removal of these tampons, the wounds were found to be infected with P.
aeruginosa, Streptococcus faecalis and Acinetobacter calcoaceticus, sensitive to cefotaxime and tobramycin . These organisms were also isolated from the rectum.
Three patients (5%) had four infections with cefotaxime-resistant bacteria (Table 5 ) . Two patients had a central venous catheter-related septicaemia with S.
epidermidis, which was treated by removing the catheters and one patient was treated with co-trimoxazol. The wound infections with cefotaxime-resistant orga-
Table 5 . Infections i n group II (selective gut decontamination +cefotaxime) .
Potentially Duration �en�itivity Patient pathogenic of isolation to No. microorganisms Site (day�) Cefotaxime Therapy
I . S. aureus Respiratory tract 1 -5 s cefotaxime 2. S. aureus Respiratory tract 1 s cefotaxime 3. H. influenzae Respiratory tract s cefotaxime
N. catarrhalis s ccfotaximc 4. E. coli Respiratory tract 1 -2 s cefotaxime 5. P. mirabi/is Urinary tract 2 s cefotaxime 6. S. aureus Respiratory tract 1 7- 1 8 s cefotaxime
P. morganii 1 5- 1 8 s 7 . S. faecalis Perinea! wound 7-2 1 s cefotaxime/
P. aeruginosa 7-2 1 s tobramycinc A. calcoaceticus 8- 1 6 s
8. E. cloacae Wound 7-20 R ccfotaximcl tobramycine
9. P. aeruginosa Subphrenie 1 1 R ceftazidimcl Anaerobes abscess 1 1 - 1 9 R tobramycinel S. epidermidis Blood 1 8- 1 9 R mctronidazol
10 . S . epidermidis Blood 3 1 R cotrimoxazol
40

nisms were both endogenous. caused by bacteria that were part of the patients intestinal flora at admission and which had become cefotaxime-resistant during treatment. Patient 8, a 84-year old male suffered a severe crush-injury of the leg. Surgical treatment included osteo�ynthesis and repair of the vascular lesions. The patient developed acute renal insufficiency and was haemodialysed. His leg had to be amputated because of per�istent ischaemia and a wound infection with Enterobacter cloacae. The same organism (sensitive to cefotaxime) was isolated from the rectum on admission . but was rapidly el iminated from the intestines by selective gut decontamination . In the wound however. E. cloacae had become re�i�tant agai nq cefotaxime. The patient recovered completely . Patient 9 developed a subphrenic abscess after a traumatic bowel perforation and liver rupture. P.
aeruginosa was isolated from the rectum on admission. Eleven days later when the abscess was drained, the same P. aeruginosa together with anaerobes were isolated from the pus . This infection was successfully treated by surgical drainage and antibiotic therapy (ceftazidime. tobramycin and metronidazol) .
S ix different antimicrobial agents were used for systemic prophylaxis or therapy. The number of patients treated with metronidazol (against anaerobes) was significantly less than in the control group. No patient was treated with antipseudomonas penicil l ins ( carbenici l l in . ticarcil l in ) . The total amount of systemic antimicrobials used in this group, including the routine systemic prophylaxis. was less than in the control group (Table 3): the mean number of antibiotic days/patient ( 1 3 .9 ± 1 3 . l ) (t = l .35 ns).
No patient died in this group during ICU-stay.
Discussion
The very high infection rate in the control group (8 1 % ) is in accordance with other reports (Northey et al . , 1 974; Thorp et al . , 1 979) . Risk factors explaining the h igh incidence of infections in multiple trauma patients are : ( I ) a severe defect of the humoral and cellular immune system (Maderazo et a l . . 198 1 ) ; (2) prolonged intensive care because of severe trauma (Schimpff et al . . 1 974) ; (3) prolonged endotracheal in tubation and mechanical ventilation and other invasive monitoring and therapy (e.g. indwelling urinary catheters, central venous catheters) (Freeman & McGowan. 1 978; Daschner et a l . . 1 982) .
In the control group a generally recommended antibiotic policy (Stoddart . 1 983) has been followed, based on the restrictive usage of systemic antimicrobial agents to prevent emergence of resistance : ( I ) no routine systemic antibiotic prophylaxis was given ; (2) positive bacteriological cultures without signs of infection were considered to be 'colonisation ' ; (3) systemic antibiotic therapy was given only on strict clinical and bacteriological indications. However. most patients in the control group {86% ) received systemic antibiotic therapy within the first week of
4 1

ICU-stay. I n case of serious infections a combination of antimicrobial agents was given. This explains why the amount of systemic antibiotics used in the control group is greater than in Group II who routinely received systemic antibiotic prophylaxis, although the difference was not significant. In the control group a very h igh incidence of superinfections was found. Fourteen patients (24% ) developed one or more superinfections with multiple-resistant Gram-negative PPM (e.g. Pseudomonas, Acinetobacter. Serratia, Enterobacter spp . ) frequently accompanied by septicaemia. An important observation is that most superinfections were preceded by colonisation of the oral cavity or intestines with the same species during antibiotic therapy. Either these PPM have been selected under antibiotic pressure or had been acquired from the environment . Five patients (8% ) of the control group died from uncontrollable infection, despite seemingly appropriate antibiotic therapy.
In group II (selective gut decontamination+ cefotaxime) the total number of infected patients was 1 0 ( 1 6% ). Not only the infection rate decreased significantly, but the number of infected sites also decreased from 94 in the control group to 1 1 in group I I . No Gram-negative septicaemia occurred in this group. Seven infections occurring under this antibiotic policy were caused by organisms sensitive to cefotaxime. These infections were rapidly cured by continued cefotaxime administration .
Three patients (5%) had four superinfections with cefotaxime-resistant microorganisms. Two patients had catheter-related septicaemia with S. epidermi
dis. Only two patients had an infection with resistant Gram-negative organisms. Both patients had severe multiple inj uries heavily contaminated by their own flora. Resistance developed in the wounds. In the control group seventeen different antimicrobial agents were necessary to treat infections, while in group II only six different agents were used for prophylaxis or therapy: in only two patients was it necessary to use others than those used for prophylaxis.
No patient died in this group, although it included patients with severe multiple trauma : two patients had a trauma score of 75.
Recent studies report a high incidence of superinfections during therapy with third generation cephalosporins, in particular in immunocompromised patients. These antibiotics may induce B-lactamases that are responsible for a novel type of resistance described by Sanders ( 1 983) as 'non-hydrolytic barrier mechanisms'. Induction of resistance is primarily demonstrable when sub-inhibitory concentrations of antimicrobial agents are used. However, we feel that our antibiotic policy (systemic colonisation resistance-indifferent antibiotics in combination with oral non-absorbable antimicrobial agents) may prevent emergence of resistance . When antibiotics are given only systemically, the subinhibitory concentrations that may be found in the lumen of the digestive tract are l ikely to indu-
42

ce resistance , particularly when organisms are present which possess inducible Blactamases (e .g . Pseudomonas, Enterobacter or Serra ti a spp . ) .
If, in addition, the indigenous (anaerobic) flora i s affected by these agents, the resistant strains may proliferate and may subsequently cause superinfections. This i:,, confirmed by studie:,, reporting the emergence of resistance in the oropharyngeal cavity (Stille et al . , 1 983) or intestines (Borderon et al . , 1 983) during systemic antibiotic therapy and by our observation that most superinfections in the control group were secondary endogenous infections. With selective gut decontamination however, high levels of the decontaminating drugs are attained in the lumen of the digestive tract, el iminating the potentially pathogenic bacteria without disadvantageous effect on the indigenous anaerobic flora. Thus conditions favourable for the emergence of resistance are not created. In the two cases of wound infection , however, resistance could develop, probably because the antibiotic levels in the wound were too low for B-lactamase producing organ isms.
A conventional antibiotic pol icy resulted in a h igh infection rate , a h igh consumption of systemic antibiotics, complicated antibiotic therapy and a h igh incidence of superinfections with multiple-resistant Gram-negative potential ly pathogenic microorganisms.
An approach to infection prevention based on the maintenance of colonisation resistance and on selective decontamination of the digestive tract (SOD) resulted in ( I) a significant reduction of the number of infected patients ; (2) a reduction of the number of infections per patient ; (3) a significant reduction of the incidence of superinfections; (4) although systemic antibiotic prophylaxis was given routinely to al l patients, development of resistance was largely prevented and additional systemic antibiotic therapy was seldom necessary.
43


Chapter 4
The effect of oropharyngeal decontamination using topical nonabsorbable antibiotics on the i ncidence of nosocomial respiratory tract i nfections in multiple trauma patients
Ch. P. Stoutenbeek , H . K . F. van Saene� , D. R . Miranda , D. F. Zandstra and D. Langrehr
Department of Anc�thc�iology and lnten�ive Care. Department of Clinical Bacteriology • . University Ho�pital. Groningen. The Netherlands
Journal of Trauma 27:357 ( 1 987)
45

Abstract
The incidence of respiratory tract infections was determined in 59 multiple trauma patients requiring prolonged intensive care (>5 days) and receiving no antibiotic prophylaxis. Early pneumonia ( <48 hr�) with S. aureus, S. pncu
moniae, and/or H. influenzac was found in 44% of patients. Secondary colonisation of the oropharynx and respiratory tract with ICU-associated Gram-negative baci l l i followed by pneumonia occurred in 1 2 patients (20% ). The overall incidence of respiratory tract infections was 59% .
In a prospective open trial three prophylactic antibiotic regimen� were compared : 1 7 patients were treated with intestinal decontamination using nonabsorbable antibiotics (polymyxin E .. mo mg, tobramycin .320 mg, amphotericin B 2 ,00C mg/day) . No difference in infection rate wa� found. Twenty- five patients were treated with intestinal and oropharyngeal decontamination u�ing an ointment containing 2% of t he same antibiotics. Secondary colonisation and infection of the respiratory tract with Gram-negative baci l l i was �ignificantly reduced (p<0.00 1 ) . The incidence of early (Gram-positive) infections however, was unchanged. Another group of 63 patients was treated with systemic antibiotic prophylaxis during the first days in combination with oropharyngeal and intestinal decontamination . The incidence of early pneumonia was �ignificantly reduced (p<0.001 ). Five patients (8% ) developed an infection . Superinfections were not observed.
Introduction
Multiple trauma patients requiring prolonged mechanical ventilation are at h igh risk of infections (Schimpff et a l . , 1 974; Freeman & Mc Gowan , I 978; Allgower et al . , 1 980; Daschner et al . , 1 982 ; Dunham & LaMonica . 1 984) with an increased morbidity and mortality (Goris & Draaisma, 1982). However, we have found few detailed studies on the rate of respiratory tract infections (RTI) in this group of patients. In critically i l l surgical and medical patients the rate of pneumonia is 60% after 5 days of mechanical ventilation (Northey et al . , 1 974; Thorp ct al . , 1979; Cross & Roup, 198 1 ) . Contaminated ventilatory equipment, which used to be an important cause , is rarely the cause of infection nowadays (Comhaire & Lamy, 1981; Cross & Roup, 198 1 ) . The major determinant for the development of nosocomial respiratory tract infections is oropharyngeal colonisation (La Force , 1 98 1 ) .
The present study has two parts: the first part describes the incidence and type of RTI in long-term ventilated multiple trauma patients treated with a conventional antibiotic policy, and the purpose of the second part was to study the effectiveness of topical antibiotics in the prevention of pulmonary infect ion . In a prospective open trial three regimens using topical nonabsorbable antibiotics were
46

evaluated: i) Selective decontamination of the digestive system only; i i ) selective decontamination of both dige-.tive system and oropharynx; amt i i i ) selective decontamination of the digestive system and oropharynx in combination with systemic antibiotic prophylaxis.
Selective decontamination aims at selective elimination of aerobic Gram-negative baci lli and yeasts from the oropharyngeal cavity and digestive system (van der Waaij & Berghuis-de Vries, 1 974) . It is based on the assumption that preservation of the indigenom anaerobic flora is beneficial to the host. Data from an experimental animal model indicate that acquisition and colonisation of new aerobic organi!>ms is faci l itated by suppression of the anaerobic flora (van der Waaij et al . , 1 97 1 ) . The antimicrobial agents chosen have l ittle effect on the anaerobic flora and administration of other antibiotics which do inhibit anaerobes. such as penicillin or ampicil l in was avoided . This technique is shown to be effective in preventing secondary colonisation and infection in neutropcnic patient.. (Sleyfcr ct al . , 1 980) and i n multiple trauma patients (Stoutenbeek et al . , 1 984) .
The topical antibiotics used were polymyxin E, tobramycin, and amphotericin B. This combination was chosen because: i) Polymyxin E is bactericidal for the majority of aerobic Gram-negative bacilli except Proteu:, spp. which are intrinsically insensitive to polymyxin . Tobramycin is given to prevent colonisation by Proteus spp . ii) The combination is synergistic against Pseudomonns and Acine
tobacterspp and is least inactivated by faeces (van Saene et al . , 1 985a) . i i i ) A combination of two agents would decrease the chance of resistance developing during treatment. iv) This combination has l itt le effect on the anaerobic flora of the gut in the dosage used (van der Waaij et al . , 1 982 ; Mulder et al . . 1 984) . v) These drugs are nonabsorbable when applied topically. To prevent overgrowth of yeasts, amphotericin B was used.
For systemic antibiotic prophylaxis cefotaxime has been used because it is active against most aerobic potentially pathogenic microorganisms that may be present in the oropharynx and because it has l ittle effect on the normal (anaerobic) flora . Many studies reported that treatment with cefotaxime did not promote the emergence of resistant organisms (Lambert-Zechovsky et al . , 1 980; Guggenbichler & Kofler, 1 984) .
This study was designed a s a consecutive open trial rather than a s a blinded placebo-controlled trial because: i) patients colonised or infected with Gram-negative bacteria may serve as a source of environmental contamination and cross-infection ; ii) selective decontamination has prevented endogenous infections but not exogenous (cross-) infections; as a consequence the presence of placebotreated patients might increase the risk of infection in the treated group whereas successful decontamination in the treated group would probably decrease the risk of colonisation and i nfection in the untreated group; i i i ) a blinded study is difficult
47

because selective decontamination has marked effects on the bacterial flora so that treated patients can readily be identified from the culture results. However. the clinician must have the results to make therapeutic decisions. Finally, to exclude the possibil ity of emergence of resistance due to a new antibiotic regimen, the observation period should be long enough.
Patients and methods
Multiple trauma patients requiring prolonged mechanical ventilation and staying 5 days or more in the ICU were included in the study. Patients admitted because of infectious problems or on antibiotics before admission were excluded from the study.
Patients were divided into 3 groups: Group I (control) consisted of 59 patients admitted to the ICU in 1 979- 1 980. These patients did not routinely receive antibiotic prophylaxis. Antibiotic therapy was given on strict clinical and bacteriological evidence of infection. Because surveillance cultures were taken in all patients and signs of infection had been recorded daily by one of the authors ( including chest X-ray, blood gas analysis. and haematological examinations) , the colonisation pattern and the infection rate could be retrospectively analysed. Group II and I I I were prospectively studied. Group I I comprised 42 patients admitted to the ICU in 1 98 1 - 1 982 . They were treated with decontamination using topical nonabsorbable antibiotics. No systemic prophylaxis was given . Seventeen patients (Group I IA) were treated only with intestinal decontamination . Another 25 patients (Group I IB) were treated with decontamination of both the GI-tract and the oropharyngeal cavity. Group I I I consisted of 63 patients admitted to the ICU in 1 982- 1 983 . In this group decontamination of the GI- tract and oropharynx was combined with systemic prophylaxis. using cefotaxime (50- 1 00 mg/kg/day iv). Cefotaxime was given immediately on arrival and was discontinued when no PPM were isolated from the oropharynx or respiratory tract . The I njury Severity Score was determined for each patient using the Hospital Trauma Index (American College of Surgeons, 1 980) . The severity of injury is graded 0 (no inj ury) to 5 ( critical) in the major organ systems. The sum of the squares of the three highest grades gives the I njury Severity Score. Thus the highest possible score is 75.
Patients were generally in tubated by orotracheal route. Nasotracheal intubation or tracheostomy were not routinely used for long-term ventilation. A mucolytic agent (Mistabron®. UCB Farma Nederland, Breda) and a bronchodilator (Ventolin®, Glaxo, N ieuwegein) were nebulised four times daily. I ntensive chest physiotherapy was performed eight times daily. Ventilator circuits were sterilized daily in Groups I and II and three times per week in Group I I I . All patients were examined daily by one of the authors (CPS, ORM .DFZ) for clinical signs of infection , in eluding chest X-rays, complete blood count and blood gas analysis.
48

Selective Decontamination regimen: This ha� been dc-;cribed in detail elsewhere (Stoutenbeek et al . , 1 984) . A 1 0-ml suspension of polymyxin E 100 mg, tobramycin 80 mg and amphotericin B 500 mg was administered through the gastric tube four times daily. Gastric suction was discontinued for one hour following administration. The oropharyngeal cavity was treated with an adhe�ive paste (Orabase®, Squibb, Rijswij k) containing 2% each of polymyxin E, tobramycin , and amphotericin B . This ointment was applied to the buccal mucosa with a prefi l led syringe and evenly smeared out with a gloved finger, four times daily.
Bacteriology: Culture� of oropharynx, rectum (swabs) or faeces, urine , tracheal aspirate and wound swabs were taken on admission (baseline) and thereafter thrice weekly (survei l lance) . B lood was cultured whenever the rectal temperature was 39°C or higher. Specimens were cultured in a qualitative and semiquantitative way. Standard methods for identification and typing were used (van Saene
et al . , I 983a). Growth density was graded using the four-quadrant method: growth only in broth (bra in-heart infusion )= + I , which is comparable to 1 - 1 0 PPM/ml , growth in the first quadrant of the solid plate = + 2 ( :s; I 03) , in the second quadrant = + 3 ( :s; JO') . in the third quadrant= +4 ( :s; I07) and growth on the whole plate = +5 (> 1 07) .
Definitions:
Potentially pathogenic microorganisms (PPM) : organisms that may cause infection when the host defence is decreased, not including the indigenous anaerobic and aerobic flora.
Colonisation : the isolation of the same PPM from two or more consecutive samples from the same site , in a growth density > + I , without signs of infection . Colonisation was assumed to extend from the preceding negative culture until the first sample in which that particular PPM was no longer present .
Colonisation index (CI ) : the sum of semiquantitative growth densities of each PPM isolated, divided by the number of samples (Wade et al . , 1 982) . This index reflects both growth densities and the number of different species isolated per sample. For example, if two different PPM can be isolated from a specimen, with growth densities +2 and +3 , the colonisation index would be 5. Only the findings of the prospective part of the study were included in the index calculations.
Respiratory tract i nfection (RTI ) : the presence of purulent sputum (Gramstain ) , heavy growth (;;:,:+3) of PPM in cultures of tracheal aspirate , clinical and radiological signs of pulmonary infi l tration , and fever and leukocytosis (Tobin & Grenvik , 1 984) . A d istinction between primary and secondary RTI was made: primary RTI were infections which developed before systemic antibiotic use and secondary RTI were infections developing during or after systemic antibiotic therapy (Spencer & Phi l ip, 1 973) .
49
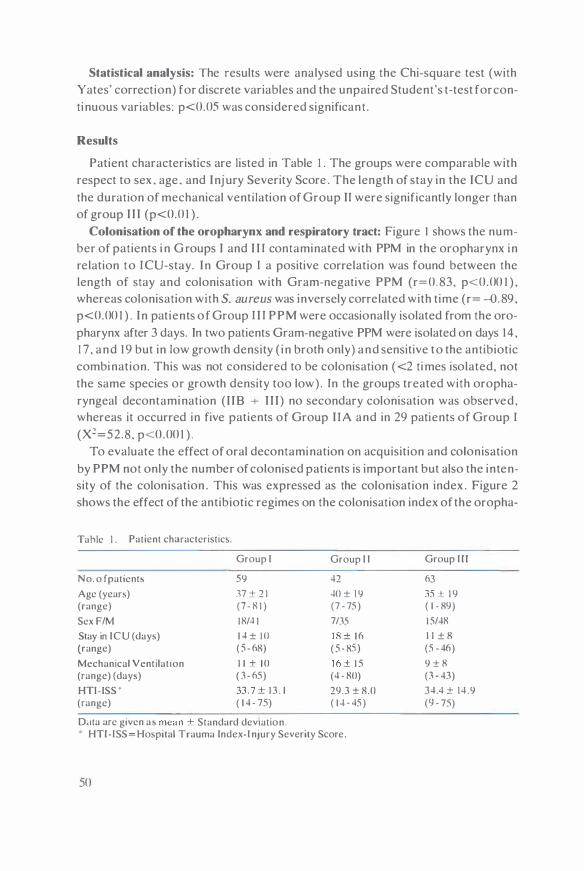
Statistical analysis: The results were analysed using the Chi-square test (with Yates' correction) for discrete variables and the unpaired Student's t-test for continuous variables: p<0.05 was considered significant .
Results
Patient characteri�tics are listed in Table 1 . The groups were comparable with respect to sex . age. and Injury Severity Score . The length of stay in the ICU and the duration of mechanical ventilation of Group II were significantly longer than of group I I I (p<0.0 1 ) .
Colonisation of the oropharynx and respiratory tract: Figure I shows the number of patients i n Groups I and I I I contaminated with PPM in the oropharynx in relation to ICU-stay. In Group I a positive correlation was found between the length of stay and colonisation with Gram-negative PPM (r=0.83, p<0.00 1 ) , whereas colonisation with S. au re us was inversely correlated with time (r= -0.89 . p<0.00 1 ) . In patients of Group I I I PPM were occasionally isolated from the oropharynx after 3 days. In two patients Gram-negative PPM were isolated on days 14 , 1 7 , and 1 9 but in low growth density ( in broth only) and sensitive to the antibiotic combination. This was not considered to be colonisation ( <2 times isolated, not the same species or growth density too low). In the groups treated with oropharyngeal decontamination ( 1 18 -r I I I ) no secondary colonisation was observed, whereas it occurred in five patients of Group I IA and in 29 patients of Group I (Xl=52.8 , p<0.00 1 ) .
To evaluate the effect of oral decontamination on acquisition and colonisation by PPM not only the number of colonised patients is important but also the intensity of the colonisation . This was expressed as the colonisation index . Figure 2 shows the effect of the antibiotic regimes on the colonisation index of the oropha-
Ta hie I . Patient characteristic�.
Group I Group I I
No. o f patient� 59 42
Age (year;) 37 + 2 1 40 ± 1 9 (range) (7- 8 1 ) (7 - 75)
Sex F/M 18/4 1 7/35
Stay rn ICU (days) 1 4 ± 10 1 8 ± 1 6 (range) ( 5 - 68) ( 5 - 85 )
Mechanical Ventilation 1 1 + 1 0 1 6 ± 1 5 (range) (day>) ( 3 - 65) (4 · 80)
HTl- ISS ' 33. 7 ± 1 3 . 1 29.3 ± 8.0 (range) ( 1 4 - 75) ( 1 4 - 45)
D<lla arc given a� mean ± Standard deviation . HTl-ISS= Hospital Trauma Index-I njury Severity Score.
50
Group I l l
63
35 ± 1 9 ( 1 - 89)
1 5/48
1 1 ± 8 (5 - 46)
9 ± 8 (3 - 43)
34.4 ± 14 .9 (9 - 75)

1 00 x z >-a:: < BO ::i:: Q._ CJ a:: CJ UJ 60 I-< a:: z •o CJ -I-< N - 20 z CJ -' CJ u
5 1 0 1 5 20
DAYS in I CU
Group /: Group ///: • S. aureus e S. oureus D Grom-Negative PPM 0 Grom-Negati ve PPM
Figure I : Coloni�ation of the oropharynx. I n the control group a hnear correlation w.i\ found between the length of �tay and colom�ation with Gram-negative PPM (�olid l ine). Gr.im-po�itive PPM were gradually el iminated. In Group I l l both Gram-negative ,ind Gr,1m-positive PPM were el iminated within 2-3 day�; thereafter Gram-negative PPM were occ11s1on.illy isolated and in low growth dcn,ity.
2 u � ,, <lJ I . b -0 c
c I . 2 � r:: N 0 . 8 -c 0 0 0 . 4 u
'\J o c u l t u r e s 1 4 2
Figure 2 : C r o u p s Ilt\
O R O P H A R Y N X
*** n s
� * ***
C::l.:.:. 1 6 5 2 7 6
IIB m
D G r a m n eg . P P M l2Z3 G r a m p a s . P P M
R E S P I R A T O R Y T R 1\ C l
� *** n s
� n s ***
"1 3 1 ! J S 2 9 8
Ilt\ IIB III Effect of oropharyngeal decontamination on the Colonisation I ndex of the oropharynx and respiratory tract. The mean Colonisation I ndex ( ± S . E . M ) is shown for both Gram-positive and Gramnegative PPM. Baseline cultures were not included . ( * • p<0.00 1 ; =p<lJ.05). Selective decontamination of both the oropharynx and digestive system (Group l lB) significantly reduced the Colonisation I ndex of Gram-negative PPM compared to Group l l A . which was treated without oropharyngeal decontamination. The index of Gram- positive PPM was significantly reduced only in Group I I I . using �ystemic antibiotic prophylaxis in addition to selective decontamination.
5 1

rynx and respiratory tract . Baseline cultures were not considered . In Group I IB . treated with both intestinal and oral decontamination . a significant reduction (p<ll .00 1 ) was found in the Gram-negative colon isation index of the oropharynx
Tahl.: 2 . Rc,p1ratory tract infr:cl1on,.
Group I Group l l A Group l l B
SD of intc,tinc' + SD of oropharynx + ccfotaxime iv
No. of patient' 59 1 7 2.'i Primary RTI 26 (44"u ) J 0 (59"u ) J J (52"o ) (pncumo-septicacmia) 9 3 2
Secondary RTI 1 2 ( 20% ) J ( 1 8 "',, ) ( pneumo-,epticacm1a) J I Total RTI Yi ( .'ilJ"u ) J 0 (5lJ"u ) J J ( 52 " u )
Died 5 (8°o ) 2 ( 1 2 % ) 1 (-l"u )
SD = 'elective decontamination.
T;thlc J. PPM cau,mg pneumonia and pncumona-,epticaemi,1.
Group I l l
+ + +
63
.5 (H11 u )
()
PRIMARY RTI SECONDARY RTI
Group'
I nfected patient' 26 Number of PPM 49 S. pneumoniJc 1 7 S. aureus IH H. mfluenwe 9 8. catarrhali' I H+-streptococ G Klebsielhl 'PP· 2 E coli Proteus spp. P. aeruginosa Acinetobactcr spp . E. cloacae S. mJrcescen�
Pneumo-scpticaemiae 9 Number of PPM IO S. ;iureus 7 S. pneumoniae 2 K pneumonwc E. coli E. c/o;ic;ie S. marcescens P. aeruginosa
R TI = Respiratory tract infection.
l lA 1 1 8 JO n 1 7 1 6 8 6 5 4 J I
2
J 2 3 2 2
PPM = Potcnt1ally pathogenic microorgani,m.
1 2 1 7
J J 2 5 I 2
3 3
• l patient had septicaemia with K. pneumoniae and S. aurcus
52
l l A 1 1 8 I l l
J s 4 7
J l I
2

and lower airways compared to Group I IA, treated with intestinal decontamination only. No significant difference could be found in Gram-positive colonisation index between these groups. In Group I I I , which received systemic prophylaxis during the first days in addition to the decontamination regimen, a h ighly significant reduction (p<0.001 ) of the Gram-positive colonisation index was found , compared to both Groups I IA and I IB . Although the Gram-negative colon isation index of the oral cavity was slightly lower than in Group I IB (p<0.05 ) , no difference was found for the respiratory tract .
Infection rate: From the patients who did not receive systemic antibiotic prophylaxis (Groups I + I IA + I IB ; n= 1 0 1 ), 49 patients developed lower respiratory tract infections before any systemic antibiotic had been given (Table 2) . In 78% of patients this infection developed within 48 hr after admission . The predominating pathogens causing infection were S. pneumoniae, S. aureus and H. influenzae
(Table 3) . In 29% of patients septicaemia occurred during the infection , most frequently by S. aureus (Table 3) . The median time of occurrence was the third day (range , 1 -9 days) . Secondary RTI , developing during or after systemic antibiotics had been given , were found in 1 2 patients of Group I and in three patients of Group l lA (20%) . No secondary RTI were observed in Group l lB (X1=4.4. p<0.05 ) . Secondary pneumonias were caused predominantly by Gram-negative ICU-acquired PPM (e .g. , P. aeruginosa. Acinetobacter)(Table 3). The mean time of occurrence was 8 ± 6 days (3- 1 8 days). In 1 3/ 1 5 patients (87%) the infections were preceded by oropharyngeal colonisation . Four patients developed septicaemia during secondary pneumonia and all four died as a consequence of the infection . One other patient died during secondary infection .
In Group I I I five patients (8%) developed RTI , a highly significant reduction (X2=38. I ; p<0.001 ) compared to Groups I and I I . Most infections occurred in the first days after admission and were cured with the systemically given cefotaxime. One patient developed a bronchopneumonia with S. aureus and P. morganii
on the fourteenth day, after detubation and after discontinuing the decontamination antibiotics. The infection was treated with cefotaxime.
Discussion
The first part of this study was a retrospective analysis of the influence of a conventional antibiotic policy on the incidence and type of respiratory tract infections in mechanical ly ventilated multiple trauma patients. In this group 59% of patients had one or more RTI during ICU stay. This h igh infection rate reflects the severity of the underlying disease : only patients with multiple injuries , requiring prolonged mechanical ventilation, were included in the study. A similar high infection rate has been reported by others (Freeman & McGowan , 1 978; Dunham & LaMonica, 1 984) . The clinical diagnosis of bacterial pneumonia may be very difficult
53

in the presence of other pathologic processe!> (e.g . . lung contusion, ARDS. or pulmonary haemorrhage)(Andrews et al . , 1 980). Probably the true infection rate is even underestimated (Andrews et a l . , 1 980; Bell et al . , 1 983) . The clinical significance of the recorded RTI was apparent from the rapid deterioration of the lung function and the h igh incidence of septicaemia. The influence of the antibiotic policy on the type of PPM causing infections has been demonstrated by dividing the infections into primary- (without antibiotics) and secondary infections (with antibiotics) . I n the control group 26 patients (44% ) developed a primary infection and 1 2 patient!> (20%) a !>econdary infection . Primary RTI: Primary infections were caused predominantly by S. aure11s, S.
pneumoniae and H. influenzae. A striking phenomenon was the early onset (within 48 hr) and the fulminant course of these infections. To our knowledge , the importance of early pneumonia in multiple trauma patients if no systemic antibiotic prophylaxis is given, has not been described. I t is well known that 30%-40% of healthy persons carry S. aureus in the nasopharynx (Rose bury , 1 962) and that the carriership of S. pneumoniae and H. influenzae is even h igher (30%-80%) ( Hir!>chmann & Everett , 1 979) . These PPM are readily introduced into the lower airways by aspiration and/or by endotracheal intubation (Espersen & Gabrielsen , 1 98 1 ) at the time of accident . Pulmonary antibacterial defence mechanisms are known to be compromised by shock , acidosis, oedema . hypoxia, and corticosteroid therapy (Green et al . . 1 977) , all of which are common in trauma patients. The presence of traumatic lung damage may further promote the rapid onset of infection .
Secondary RTI: Secondary pulmonary infections were invariably caused by nosocomial Gram-negative PPM (e.g. , Pseudomonas spp . ) which were often resistant to the antibiotics used. The first pathogenetic step is acquisition of Gramnegative bacil l i in the oral cavity followed by colonisation (LaForce , 1 98 1 ) . The rapid oropharyngeal colonisation observed in the control group (figure I ) may be explained by a h igh exposure to Gram-negative PPM in the ICU (Teres et al . , 1 973; Rose & Babcock , 1 975) and by the impairment of oral defence mechanisms. I n critical ly i l l patients these defence-mechanisms are fail ing due to: i ) increased adherence of Gram-negative PPM to buccal epithelial cells (Johanson et a l . , 1 980) : i i ) impairment of the normal clearing mechanisms (e .g. salivary flow, swallowing) ( LaForce et al . , 1 976) ; or i i i ) disturbance of the indigenous oropharyn geal flora (Sprunt & Redman , 1 968; Murray & Rosenblatt, 1 976; Yoshioka et al . , 1 982) . Not only the oral cavity but also the gastric contents may become heavily colonised with Gram-negative baci l l i (Atherton & White , 1 978; Du Moul in et a l . , 1 982; Hillman et al . , 1 982) and these may act as reservoirs of PPM. The second pathogenetic step is colonisation of the lower airways with Gram-negative bacilli from the oropharynx (van Uffelen et al . , 1 984) , which is a common finding in intu-
54
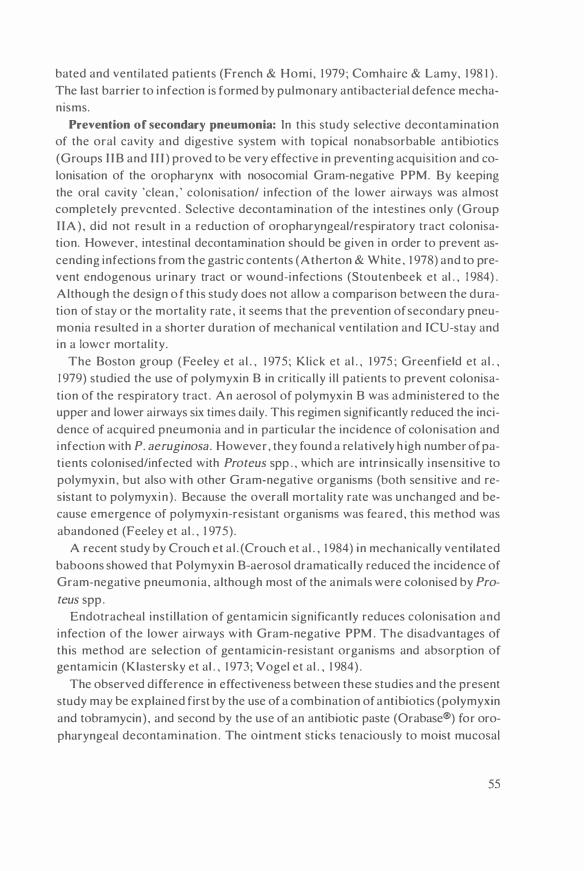
bated and ventilated patients (French & Homi, 1 979 ; Comhaire & Lamy, 1 98 1 ) . The last barrier to infection is formed by pulmonary antibacterial defence mechanisms.
Prevention of secondary pneumonia: In this study selective decontamination of the oral cavity and digestive system with topical nonabsorbable antibiotics (Groups I IB and I I I ) proved to be very effective in preventing acquisition and colonisation of the oropharynx with nosocomial Gram-negative PPM. By keeping the oral cavity 'clean , ' colonisation/ infection of the lower airways was almost completely prevented . Selective decontamination of the intestines only (Group I IA) , did not result in a reduction of oropharyngeal/respiratory tract colonisation. However, intestinal decontamination should be given in order to prevent ascending infections from the gastric contents (Atherton & White , 1 978) and to prevent endogenous urinary tract or wound-infections (Stoutenbeek et al . , 1 984 ) . Although the design o f this study does not al low a comparison between the duration of stay or the mortality rate , it seems that the prevention of secondary pneumonia resulted in a shorter duration of mechanical ventilation and ICU-stay and in a lower mortality.
The Boston group (Feeley et al . , 1 975; Klick et al . , 1 975 ; Greenfield et al . . 1 979) studied the use of polymyxin B in critical ly i l l patients to prevent colonisation of the respiratory tract . An aerosol of polymyxin B was administered to the upper and lower airways six times daily. This regimen significantly reduced the incidence of acquired pneumonia and in particular the incidence of colonisation and infection with P. aeruginosa. However, they found a relatively h igh number of patients colonised/infected with Proteus spp . , which are intrinsically insensitive to polymyxin , but also with other Gram-negative organisms (both sensit ive and resistant to polymyxin) . Because the overall mortality rate was unchanged and because emergence of polymyxin-resistant organisms was feared, this method was abandoned (Feeley et al . , 1 975) .
A recent study by Crouch et a l . (Crouch et al . , 1 984) in mechanically ventilated baboons showed that Polymyxin B-aerosol dramatical ly reduced the incidence of Gram-negative pneumonia, a lthough most of the animals were colonised by Pro
teus spp . Endotracheal insti l lation of gentamicin significantly reduces colonisation and
infection of the lower airways with Gram-negative PPM. The disadvantages of this method are selection of gentamicin-resistant organisms and absorption of gentamicin (Klastersky et al . , 1 973; Vogel et al . , 1 984) .
The observed difference in effectiveness between these studies and the present study may be explained first by the use of a combination of antibiotics (polymyxin and tobramycin) , and second by the use of an antibiotic paste (Orabase®) for oropharyngeal decontamination . The ointment sticks tenaciously to moist mucosa!
55

surfaces and slowly releases the drugs (de Vries-Hospers & van der Waaij , 1 978). This appears to be important, because in a preliminary study an aqueous solution of the same antibiotics proved to be minimally effective for decontamination of the oral cavity.
Finally , the fundamental difference between our approach and other studies using either parenteral or topical antibiotics seems to be elimination of the endogenous source of PPM from both the oropharynx and the gut. I f antibiotics are given parenterally, emergence of resistance is most likely to occur in the oropharynx and the gut where large numbers of aerobic Gram-negative bacilli are present and where only peri-inhibitory antibiotic concentrations are reached, thus promoting the selection of resistant strains. With selective decontamination of the digestive tract the bulk of Gram-negative PPM is eliminated by nonabsorbable antibiotics reaching high concentrations in the lumen of the gut. So far, no secondary colonisation with resistant PPM has been observed with this technique .
Prevention of primary pneumonia: The early respiratory tract infections were not prevented by the antibiotics used for selective decontamination ; first, because these antibiotics are not active against Gram-positive PPM, and, second , because selective decontamination is started after the resuscitation phase , when aspiration in an injured lung has already taken place. Thus systemic antibiotic prophylaxis ( c.q . , early treatment) should be instituted as soon as possible in mechanically ventilated multiple trauma patients to prevent early pneumonia. Early infections are generally caused by community flora sensitive to penicillin- G or penicillin-derivatives (e.g. , ampicillin and cloxacill in) . However, these are not first-choice drugs because they are associated with a high incidence of superinfections (Sabath et al . , 1 962; Tillotson & Finland, 1 969; Price & Sleigh, 1 970; van Saene et al . , I 983b) . This has been attributed to the deleterious effects of these antibiotics on the indigenous (anaerobic) flora (van der Waaij , 1 979) . Group I I I patients received cefotaxime iv during several days in addition to selective decontamination of the oral cavity and intestines. This proved to be very effective in reducing both the incidence and the severity of early pneumonia. Neither colonisation with resistant organisms nor superinfections were observed in this group.
In summary, multiple trauma patients requiring prolonged intubation and mechanical ventilation are at high risk of early ( <48 hr) pneumonia with S. aureus,
S. pneumoniae and/or H. influenzae, if no systemic antibiotic prophylaxis is given. Late RTI are invariably caused by nosocomial Gram-negative PPM and are associated with a high mortality. Secondary colonisation of the oropharynx and the digestive system with Gram-negative PPM acquired from the hospital environment plays a key role in the pathogenesis of RTL Selective decontamination of the oropharynx and intestines with topical nonabsorbable antibiotics proved to be very effective in preventing colonisation of both oropharynx and respiratory
56

tract and it reduced the incidence of secondary infections. Systemic antibiotic prophylaxis is indicated in mechanically venti lated patients to prevent early pneumonia.
Acknowledgements:
The constructive criticisms of John A . Washington, I I , M .D . and Waldemar G . Johanson M .D . are gratefully acknowledged. It i s a pleasure to acknowledge the dedicated work and the invaluable help given by the nursing staff of the ICU. We thank Henderika J. Hoekstra for the technical assistance , Wit Noordik for preparing the i l lustrations.
57

Chapter 5
The effect of oral nonabsorbable antibiotics on the emergence of resistant bacteria in patients in an intensive care unit
Christiaan P. Stoutenbeek MD, Hendrik K . F. van Saene MD* and Durk F. Zandstra MD
Department o f Ane�the�iology and l nten�ive Care. Department o f Clinical Bacteriology . University Ho�pital , Gron ingcn . The Netherland.,
Journal of Antimicrobial Chemotherapy 1 9 :5 1 3 ( 1 987)
59

A bstract
Critically i l l patients admitted to the surgical intensive care unit since 1 982 have been treated prophylactically with oral nonabsorbablc antibiotic� combined with parenteral cefotaxime . A mixture of polymyxin E, tobramycin and amphotcricin B has been administered via a na�ogastric tube and also applied topically to the buccal mucosa. This regimen has proven to be highly effective in reducing the infection rate . The present study evaluated the occurrence of rc�istant bacteria with this regimen during a 30-month period , in 1 64 patients with multiple trauma . No increase in the percentage of patients with acquired drug-resistant Gram-negative bacilli was found during this period. Colonisation of the oral cavity and/or gastro-intcstinal canal by polymyxin E-resistant strains (invariably Proteus �pp . ) occurred in 8% of patients, and by tobramycin-resistant bacil l i (Escherichia coli.
Acinetobacter or Pscudomonas spp . ) in 4% . Intestinal colonisation with cefotaxime-resistant strains (e .g . Pseudomonas. Acinctobactcr or Entcrobacter spp . ) was observed in 1 7 patients ( 1 0% ) . Of these strains 82'Yo were eliminated within one week by the oral nonabsorbablc antibiotics. Colonisation of the respiratory tract , urinary tract or wounds with cefotaxime-resistant Gram-negative bacil l i occurred in only 3 patients (2% ) .
Introduction:
Colonisation and infection with multi-resistant Gram- negative bacil l i (GNB) are matters of great concern in most surgical intensive care units (ICU). Traditional control measures have relied on efforts to decrease transmission between patients, to eliminate environmental sources and to restrict antibiotic use (Weinstein & Kabins, 1 98 1 ) . However, these strategies have not resulted in any significant decrease in colonisation or infection rates in critically ill patients (Donowitz et a l . , 1982) .
The surgical ICU of the Groningen University Hospital has adopted a prophylactic antibiotic regimen which consists of topical application of nonabsorbable antibiotics to the oral cavity and gastro-intestinal tract, combined with a parenteral third-generation cephalosporin . Polymyxin E and tobramycin are given oral ly to prevent acquisition and colonisation with ICU-associated pathogens (e .g . Pseudomonas or A cinetobacter spp . ) and to suppress the endogenous aerobic Gram-negative flora. Amphotericin B is also given to prevent overgrowth with yeasts . Parenteral prophylaxis with cefotaxime is used to prevent early respiratory tract infections by Staphylococcus aureus, Streptococcus pneumoniae or Haemophilus influenzae (Stoutenbeek et al . , 1 987) . This regimen has resulted in a dramatic reduction in colonisation and infection in multiple trauma patients (Stoutenbeek et a l . , 1 984a,b ) .
60

However, the major concern of using tobramycin and a third-generation cephalosporin for prophylaxis, was the possible emergence of resistance to these agents. The present study was designed to evaluate the incidence of acquisition , colon isation and infection with GNB, resistant to the prophylactic antibiotics used, during a 30-month period.
Methods:
Antibiotic regimens
Patients with multiple trauma who required prolonged mechanical ventilation and stayed 5 days or longer in the ICU were included in the study . Patients referred from other centres with infectious problems, or who had received antibiotics prior to admission were also included. All patients had an endotracheal tube , an urinary catheter and several indwell ing intravascular l ines. Patients were divided into five consecutive groups detailed in table I . All groups were treated with topical nonabsorbable antibiotics. A JO ml suspension of polymyxin E J OO mg (colist in , Dumex, Copenhagen) , tobramycin 80 mg (Eli Lil ly) and amphotericin B 500 mg (Squibb) was administered through the naso-gastric tube four times a day. Gastric suction was discontinued for one hour after administration . A sticky paste (Ora base®, Squibb) containing 2% polymyxin E, 2% tobramycin and 2% amphotericin B was applied to the buccal mucosa four times a day. Parenteral prophylaxis with cefotaxime (50- I 00 mg/kg/day iv . ) , was started immediately on admission and continued for at least four days , in all groups except group I . This group did not routinely receive prophylactic parenteral antibiotics. Cefotaxime was discon-
Table I . Patient characteristics.
Groups I I I l l IV v 1 982 1 982 1 983 1 983 1 984 Jan-Jun Jul-Jan Jan-Jul Jul-Jan Jan-Jul
No.patient� 2 1 39 35 33 36
Sex ( M/F) 1 7/4 3 1 /8 25/ 1 0 27/6 25/ 1 1
Age (years) • 35 ± 1 9 32 ± 1 8 38 ± 2 1 36 ± 20 36 ± 22 range (9-72) (2-76) (0-89) (6-84) (4,82)
ICU-stay (days) ' 1 7 ± 1 7 1 2 ± 7 1 6 ± 1 7 1 3 ± 9 1 3 ±9 range (6-86) (5-3 1 ) (5-82) (5-4 1 ) (5-36)
Mechanical ventilation (days)' 1 4 ± 1 6 8 ± 6 1 2 ± 1 4 1 0 ± 8 I I + 8 range (4-80) ( 1 -26) ( 1 -69) (2-34) (2-34)
Died I (5%) 0 I (3%) 2 (6%) 2 (6%)
• mean ± S .D.
61

tinued when subsequent cultures of all sampled sites were free of aerobic potentially pathogenic microorganisms. and yielded only indigenou!. flora . such a!> coagulase-negative staphylococci . viridans streptococci and enterococci .
Bacterial surveillance
Specimens- oropharyngeal swab. rectal swab or faeces, urine . tracheal aspirate and wound swabs - were cultured on admis!>ion and then three time� a week. All specimens were cultured in a qualitative and semi-quantitative manner (van Saene et al . . I 983a) . Enterobacteriaceae were identified by the API 20E system (Washington et al . . 1 97 1 ) . The sensitivity of individual strains to polymyxin E, tobramycin and cefotaxime was te!>ted by the agar diffusion method (Kirby-Bauer) (Bauer et a l . . 1 966) . Cefotaxime sensitivity was determined routinely only in groups II-IV. The break- points for resistance to cefotaxime and tobramycin were an inh ibition-zone <24 mm. For polymyxin 1 9 mm was taken as break-point because of the poor diffusibility of polymyxin in agar. Not all i�olates of Pseudo
monas spp. were tested for cefotaxime sensitivity; tho!>e that were not tested were considered to be resistant .
Definitions
Acquisition was defined as isolation of a new strain not present in any of the samples taken in the first three days (baseline) . Colonisation was defined as isolation of the same species from two or more consecutive cultures from the same site without clinical signs of infection . Colonisation was called 'primary' if the colonising bacteria were present in the baseline samples and 'secondary' if colonisation occurred later by acquired bacteria. Secondary infection was the term used for clinical diagnosis (by standard criteria) of infection by acquired bacteria .
Statistical analysis
The incidence of resistance was evaluated statistically by the Chi-square test (with Yates' correction) . A level of p<0.05 was considered significant .
Results
One hundred and sixty four patients were treated with the antibiotic regimen for a mean duration of 14 days. The total number of cultures evaluated was 525 1 (mean of 32 cultures/patient) and 1 1 9 1 cultures (23%) yielded strains of Enterobacteriaceae or Pseudomonadaceae . Excluding strains repeatedly isolated from the same site in the same patient , 374 isolates were identified; 76% of GNB were cultured from rectum/faeces, 1 0% from throat, 5% from sputum, 7% from wounds and 2% from urine .
62

Resistant strains
Figure I shows the resistance pattern of the different strains isolated. Four percent of strains were resistant to tobramycin . All strains but Proteus spp . ( I 2'X, ) were sensitive to polymyxin E . Escherichia coli. Klebsiel/a spp. and Proteus spp . were invariably sensitive to cefotaxime. Although the number of isolates wa'> smal l , a considerable percentage of Pseudomonas spp . . Acinetobacter spp. , En
terobacter cloacae and Citrobacter �pp . were found to be cefotaxime re�istant . Investigation of the flora present on admission showed 96% sensitivity to cefotaxime . The majority of cefotaxime-resistant GNB were i�olated more than three days after admission and were considered to be newly acquired from the hospital environment.
Acquisition
Figure 2 shows the incidence of acquisition . secondary colonisation and infection of the major organ systems. Thirty-five percent of patients acquired one or more different strains during their stay on the ICU (94 acquisitions) . Most strains were isolated from the rectum and had a low growth density ( < I 03 CFU/gm faeces or equivalent growth from a swab). The GNB isolated most frequently were Pseudo
monas spp . (2 1 times) , Enterobacter spp . (2 1 times) , Acinetobacter spp. ( 1 8 times) and Proteus spp. ( 1 3 times) . Forty percent of these �trains were cefotaximeresistant but none was resistant to the combination of ora l . nonabsorbable antibiotics .
<I) z � 1 00% ,_ <I) ,_ z .. ,_ <I) ;;; w 0: � 0 w "' .. ,_ z w u 0: w a.
Figure 1 :
B O
6 0
4 0
2 0
� E.tc• 0 3 6
'J17l ! CEFOT AXIM
lL.-. P�s spp Ent,roNcter spp Prot� spp
• 64 ' 4 6 ""'43
liiiiil:J TOBRAMYCINE
Klebloeb spp Acn1t;b1ctet" spp C.1/llC.lctl9' � Tou•
n:Z4 n:Z4 MEI 5 n,.J 7 4
[::::jJ POL YMYXIN E
Sensitivity pattern of Gram-negative bacilli for cefotaximc. tobramycin , and polymyxin E. A total of 374 different strains were isolated in a 30-month period. The different species are presented in descending order of frequency of isolation. Sen,itivity of Proteus 'PP· to polymyxin E was not determined ( intrinsically insensitive) . Results with Pseudomonus spp. may over-c,t1matc cefotaximc rc�istancc (sec Method�).
63
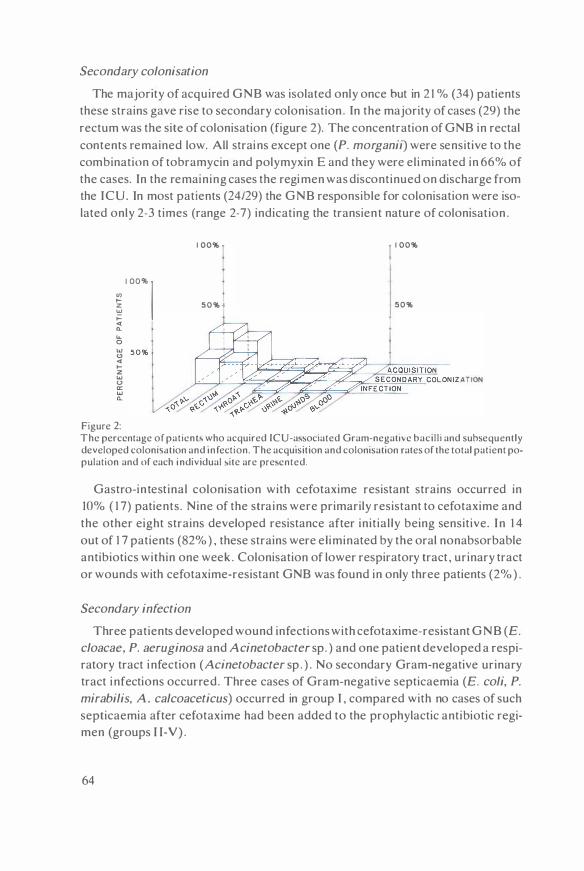
Secondary colonisation
The majority of acquired GNB was isolated only once but in 2 1 % (34) patients these strains gave rise to secondary colonisation . In the majority of cases (29) the rectum was the site of colonisation (figure 2). The concentration of GNB in rectal contents remained low. All strains except one (P. morganii) were sensitive to the combination of tobramycin and polymyxin E and they were eliminated in 66% of the cases. In the remaining cases the regimen was discontinued on discharge from the ICU. In most patients (24/29) the GNB responsible for colonisation were isolated only 2-3 times (range 2-7) indicating the transient nature of colonisation .
� ' °" I <t "-... 0 w (.!) <t .... z w () a: w "-
Figure 2:
1 00% 1 1 00%
50% t 50%
The percentage of patient\ who acquired ICU-a,sociated Gram-negative bacill i and subsequently developed colonisation and mfection. The acquisition and colonisation rates of the total patient population and of each individual 'itc are prc>cnted.
Gastro-in testinal colonisation with cefotaxime resistant strains occurred in 10% ( 1 7) patients. Nine of the strains were primarily resistant to cefotaxime and the other eight strains developed resistance after init ial ly being sensitive. In 1 4 out of 1 7 patients (82% ) , these strains were el iminated by the oral nonabsorbable antibiotics within one week . Colonisation of lower respiratory tract , urinary tract or wounds with cefotaxime-resistant GNB was found in only three patients (2% ) .
Secondary infection
Three patients developed wound infections with cefotaxime-resistant GNB (E.
cloacae, P. aeruginosa and Acinetobacter sp. ) and one patient developed a respiratory tract infection (Acinetobacter sp . ) . No secondary Gram-negative urinary tract infections occurred. Three cases of Gram-negative septicaemia (E. coli, P.
mirabilis, A . calcoaceticus) occurred in group I , compared with no cases of such septicaemia after cefotaxime had been added to the prophylactic antibiotic regimen (groups 1 1-V) .
64

Figure 3 shows the overall percentage of patients colonised with G NB resistant to tobramycin , polymyxin E or cefotaxime, in each study period . Both primary and secondary colonisation of any site are presented. Colonisation by polymyxin E-resistant GNB (Proteus spp . ) occurred in 8% ( 13) patients and by tobramycinresistant strains in 4% (7 patients) . The site of colonisation was the GI-tract or oral cavity in 1 9/20 cases . No significant differences were found between the inci· dence of resistance in any of the study periods.
Discussion
It is well known that more than 80% of critically i l l patients are colonised by hospital-acquired GNB within I 0 days of treatment (Northey et al . , 1 974; Shield et al . , 1 979; Thorp et a l . , 1 979) and that these (often multiple resistant) organisms are responsible for the majority of late infections (Rose & Babcock, 1 975 ; Weinstein & Kabins, 1 98 1 ) .
In earlier studies (Stoutenbeek et al . , I 984a,b ) , we showed that topical application of non-absorbable antibiotics in the oropharynx and GI-tract is h ighly effective in preventing secondary colonisation and infection with hospital-acquired GNB. This study, extending the experience over a 30 month period, confirms these findings. In leukaemic patients similar results were obtained with oral gentamicin therapy (in combination with vancomycin and nystatin ) . However, a h igh inci-
Figure 3 :
(/) fz w f-� 4 0 % 0 w N z 3 0 % 0 .J 0 (.) u... 0 w (!) <{ fz w (.) a: w Q.
2 0 %
1 0 %
1 9 8 2 1 1 9 0 2 II
--=C E F O T A X I M o- - -o = P O L Y M Y X I N E E •- - -• = T O B R A M Y C I N E
1 9 8 3 1 1 9 8 3 n 1 9 8 4 1
The percentage of patients who developed (transient) colonisation with cefotaxime, polymyxin E or tobramycin resistant strains, during their stay in the ICU . No increase in antibiotic resistant strains was found during the 30-month �tudy period. In the first period ( 1 982 1 ) cefotaxime was not included in the antibiotic regimen and sensitivity to cefotaxime was not routinely determined. Polymyxin-re�istant strains were invariably Proteus spp.
65

dcnce of resistance has been reported (Klastersky et a l , 1 974; Hahn et al . , 1 978) . Besides, overgrowth with gentamicin-sensitive strains often occurred (Klastersky et al, 1 974) .
During 30 months o f continuous topical use of tobramycin and polymyxin E there has been no increase in the incidence of resistance . Polymyxin E-resistant strains were invariably Proteus spp. which are intrinsically insensitive to this drug. It is well known that development of polymyxin- resistance is extremely rare (Sogaard, 1 982) .
Tobramycin-resistant strains. assessed by standard criteri a . were not common . In one patient the GI-tract was colonised with tobramycin-resistant P. morganii
( inhibition-zone 1 6 mm) ; nevertheless the organisms later disappeared . probably because tobramycin levels in faeces are very high with this regimen (Mulder et al . . 1 984) .
Secondary colonisation of the GI-tract with GNB sensitive to the combination of tobramycin and polymyxin E was found in 29 patients ( 1 8% ). However, the effectiveness of the topical antibiotics was apparent from the low growth densities of the organisms and the transient nature of colonisation . The fact that sensitive organisms were able to persist for a while may reflect the impaired colonisation defence of the G I-tract as long as peristalsis is absent .
The discrepancy between the incidences of aminoglycoside-resistance in this study and the studies using gentamicin en vancomycin might be explained by the fact that gentamicin is largely inactivated by faeces whereas tobramycin is not (van Saene et al . , I 985a) . by our use of a synergistic combination of tobramycin with polymyxin E (van Saene et al . . 1 985a) . by the preservation of the indigenous (anaerobic) flora which might contribute to the colonisation resistance (van der Waaij et al . , 1 97 1 ) .
Recent studies reported a very h igh incidence of colonisation of the major organ systems with resistant GNB and suprainfection (up to 25%) during therapy with third- generation cephalosporins (Platt et al . , 1 98 1 ; Schentag et a l . , 1 985) . None of these studies reported data on changes in the oral or intestinal flora , which would probably show an even higher rate of emergence of resistant strains.
In this study no i ncrease in the incidence of cefotaxime-resistant strains was observed. Development of resistance of E. coli, Klebsiella spp. and P. mirabilis was not common . The majority of cefotaxime-resistant strains (e.g. E. cloacae,
Pseudomonas spp . and P. morganii) were first found in the GI-tract . Because these GNB were not present in the flora on admission they were considered to be hospital-acquired. Acquisition of resistant strains seems to be an important mechanism of emergence of resistance. However, it is possible that some of the strains were already present in the admission flora in a growth-density too low to be detected by routine bacteriological methods. Only 8 strains of GNB (e .g . E.
66

cloacae) in the intestinal flora, which were previously sensitive to cefotaxime , developed resistance . The sub-inhibitory concentration of cefotaxime in faeces (Stille et al . , 1 983) probably induced resistance in organisms with inducible B-lactamases (Sanders, 1 983) . None of the cefotaxime-resistant GNB colonising the GItract were resistant to the combination of tobramycin with polymyxin E and the majority of the organisms was eliminated before they could cause clinical problems.
In conclusion it can be said that the combined regimen was h ighly effective in preventing acquisit ion, secondary colonisation and infection by hospital-associated GNB while no increase was observed in resistance to the antibiotics used. Most resistant strains were found in the intestinal flora . Surveil lance of oropharyngeal and intestinal flora should become part of the routine monitoring of critically i l l patients in the intensive care unit .
Acknowledgements:
We thank the nurses of the ICU and Henderika J . Hoekstra of the microbiology laboratory for their cooperation . We gratefully acknowledge for the valuable help of Dr. Kevin West in the preparation of the manuscript. We thank Jack Duitsch for preparing the i llustrations.
67


Chapter 6
The impact of an integrated trauma service on the late mortality from multiple organ failure and sepsis in severely inj ured patients
Ch. P. Stoutenbeek , D. F. Zandstra , H . K . F. van Saene* and 8. Binnendij k * *
Department o f Ane,the�iology and l nten,ive Care. Department o f Clinical Bacteriology and Department of Traumatology · • , Univcr,ity Ho,pita l . Groningcn. The Netherland'
69

Abstract
The impact of an integrated strategy for the management of the multiple trauma patient, on the mortality. i!> dc!>cribcd. The treatment include� aggrcs�ivc rc�uscitation . prophylactic mechanical ventilation, early ostcosynthcsis and infection prevention with oral nonabsorbablc and �y�tcmic antibiotic!> . In a 30-month period 1 67 patients with an Injury Severity Score of 1 8 or more were treated according to these principles. Twenty-three patients ( 1 4'X, ) died. The main cause of death was cranioccrcbral trauma (22 patients), which was mostly fatal within the first five days of treatment. No patient died from multiple organ failure , scp�is or ARDS. No correlation was found between the Inj ury Severity Score and mortality, or age and mortality. It i� po�tulatcd that infcctiou� complication!> arc �olcly responsible for the high correlation which is normally found between age or Inj ury Severity Score and late mortality and that thc�c complication!> can almo!>t completely be prevented by an integrated trauma treatment protocol, including an effective infection prevention �tratcgy.
Introduction
Trauma i!> the principal cause of death in pcr�ons under the age of 37 year� in our society. The mortality at the scene of injury and in the first 24 hours of emergency care i!> cau!>cd primarily by i rreversible cerebral damage or massive haemorrhage . The mortality in the next 72 hours ('early mortality') is mainly due to the development of ma!>!>ivc cerebral oedema m severe cerebral inj uric!>, whereas late mortality (after 4 days) is generally caused by sepsis and multiple organ failure (Baker ct al . , 1 980) .
To describe and quantify the severity of injuries, a scoring system , the 'Abbreviated Injury Scale (AIS) ' , has been published by the Committee on Medical Aspects of Automotive Safety ( 1 97 1 ). Based on the AIS, Baker ct al. developed the ' Inj ury Severity Score ( ISS) ' , a method rating the overall severity of injury in persons who have sustained inj ury to more than one area of the body and which was designed to compare death rates of groups (Baker et al . , 1 974) . The 'Hospital Trauma Index (HTI)' is a new version of the AIS, which has an additional score for the cardiovascular system (American College of Surgeon�, 1 980) . The ISS can be calculated with both the AIS or the HTI , and although the HTI-ISS is generally somewhat higher than the AIS-ISS, both score!> correlate very well (Goris & Draaisma, 1982) . Since the introduction of the ISS, several studies have shown the prognostic value of this index for morbidity and mortality (Baker ct al . , 1 974; Gerritsen et a l , 1 982; Lauwers et al . , 1 986) .
Age is another major determinant of outcome. Bull introduced the LD50, which he defined as a severity of injury that is lethal for 50% of the patients so injured . He found an age-dependent relationship, and determined that the LD,11
70

was an ISS of 40 for ages 1 5-44, 29 for ages 45-64, and 20 for ages 65 years and older (Bull, 1975) . The main cause of mortality is sepsis and multiple organ failure (Baker ct al . , 1 980; Goris & Draaisma, 1 982; Lauwers et a l . , 1 986) and elderly patients seem to be particularly at risk (Horst ct al . , 1 986) .
This �tudy describes the effect of an infection prevention regimen as part of an in tegrated trauma service , on mortality, in relation to ISS and age .
Patients and methods
All trauma patients admitted to the intensive care unit between January 1 982 and July 1 984, were retrospectively analysed for age, Injury Severity Score and outcome. The ISS was determined using the Hospital Trauma Index . The HTI grades the severity of inj ury from 0 (no inj ury) to 5 (cri tical) in six organ systems: central nervous system , respi ratory , cardiovascular, abdominal , extremities, skin and subcutaneous tissues. Only patients with blunt trauma and an ISS ;;. 1 8 were included in the study. This definition includes patients sustaining at least: either major injury to two organ systems, or one severely and one moderately injured organ system , or one critical inj ury . All patients dead on admission or dying within 1 hour after admission were excluded from the study. All other patients who died in the intensive care following blunt trauma, were included in the study, irrespective of the ISS. Thus no intensive care mortality was excluded from the �tudy.
RESUSCITATION
By 1 982 the pattern of care of the multiple trauma patient had become well established. Initial resuscitation measures included prophylactic mechanical ventilation of each patient with a HTl-ISS ;;. J S , independent of actual gas exchange, or chest X-ray. Oral endotracheal intubation was performed under general anaesthesia . At the same time intra- arteria l , central and peripheral venous and urinary catheters were introduced to a llow monitoring, as well as providing access to arterial blood for analysis of blood gases and biochemistry. Upon admission the patients received crystal loid and colloid solutions to restore intravascular volume. Blood was given to maintain a hematocrit of 30-35% . A Swan Ganz catheter was introduced if indicated . All patients received a bolus of dexamethasone 1 mg/kg iv and cefotaxime 1 00 mg/kg iv . Emergency operations were performed with the shortest possible delay . If the condition of the patient permitted, extensive radiological diagnostic procedures were performed according to a fixed protocol including series of chest X-rays , intravenous pyelography, ultrasound scan and, if indicated , arteriography or CT-scan (Kingma, 1 98 1 ) . After completion of the diagnostic procedures the patient was transferred to the operating room for operative fixation of fractures and/or diagnostic laparotomy .
7 1

I NTENSIVE CARE MANAGEMENT
Mechanical ventilation
I n all patients mechanical ventilation was continued for at least 24 hours . Patients were ventilated with a minimum of 4 cm of positive end-expiratory pressure (PEEP) ; to avoid barotrauma the mean airway pressure was kept as low as possible by using small tidal volumes (5- 1 0 ml/kg) and a h igh frequency (20/min) . The PEEP was adjusted to achieve an optimal functional residual capacity and gas exchange , guided by the chest X-ray, blood gas analysis and the arterial to endtidal C02 gradient (Murray et a l . , 1 984) . Patients were routinely intubated by orotracheal route , nasal intubation or tracheostomy were performed only where strictly indicated (e.g. mandibular fractures). Extubation was considered only if (i) patients were awake, cooperative and no longer required large amounts of analgesics or sedatives, and (ii) if adequate oxygenation was achieved on spontaneous respiration with a normal breathing frequency and a normal P.,C02 and (i i i ) if the chest X-ray showed no signs of infiltrations or atelectasis, suggestive of reduced functional residual capacity.
Sedation and analgesia
Patients received incremental doses of either morphine and/or benzodiazepines, or a continuous infusion of etomidate, for alleviation of pain and anxiety. Heavy sedation or deep anaesthesia with the use of muscle relaxants, was used only when strict ly indicated, e .g. cerebral edema , h igh PEEP, or differential lung ventilation .
Cardiotonics!vasodilators
All mechanically venti lated patients received low dose dopamine infusion ( 1 -5 mcg/kg/min) to counteract the negative inotropic effect and sodium retention caused by mechanical ventilation. The h igh pulmonary vascular resistance found in multiple trauma patients (Sturm et al . , 1979) was treated with a vasodilator (e.g. 5HT-antagonist, ketanseri n ) . The vasodilator, dopamine and crystalloid solutions were titrated to achieve an optimal peripheral circulation and a diuresis of at least 2 ml/kg/hour. For each patient the fluid balance was totalled every three hours, and so fluid therapy could be more accurately reassessed.
Infection prevention
Upon admission to the ICU baseline cultures were taken and the oral nonabsorbable antibiotics were started (see chapter 2) . These were continued through-
72
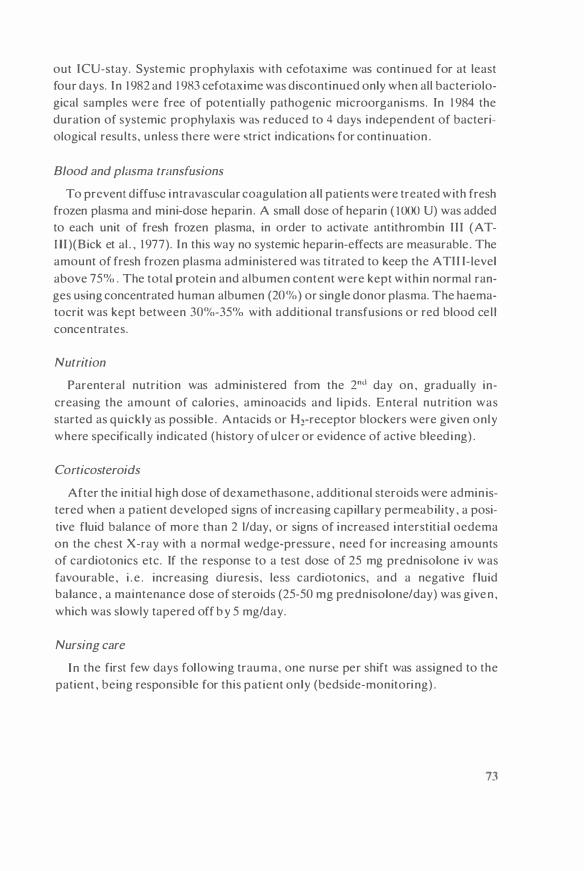
out ICU-stay. Systemic prophylaxis with cefotaxime was continued for at least four days. In 1 982 and 1 983 cefotaxime was di�continued only when all bacteriological samples were free of potentially pathogenic microorganisms. In 1 984 the duration of systemic prophylaxis wa� reduced to 4 day� independent of bacteriological results, unless there were �trict indications for continuation .
Blood and pfasma transfusions
To prevent diffu�e intravascular coagulation al l patients were treated with fresh frozen plasma and mini-dose heparin . A small dose of heparin ( 1000 U) was added to each unit of fre�h frozen plasma, in order to activate antithrombin I l l (ATl l l )(Bick et al . , 1 977). In this way no systemic heparin-effects are measurable . The amount of fresh frozen plasma administered was titrated to keep the ATII I-level above 75% . The total protein and albumen content were kept within normal ranges u�ing concentrated human albumen (20%) or single donor plasma. The haematocrit was kept between 30%-35% with additional transfusions or red blood cell concentrates.
Nutrition
Parenteral nutrition was administered from the 2"" day on , gradually increasing the amount of calories, aminoacids and l ipids. Enteral nutrition was started as quickly as possible . Antacids or H1-receptor blockers were given only where specifically indicated (h istory of ulcer or evidence of active bleeding) .
Corticosteroids
After the init ial high dose of dexamethasone, additional steroids were admin istered when a patient developed signs of increasing capillary permeability , a positive fluid balance of more than 2 I/day, or signs of increased interstit ial oedema on the chest X-ray with a normal wedge-pressure , need for increasing amounts of cardiotonics etc. If the response to a test dose of 25 mg prednisolone iv was favourable , i . e . increasing diuresis, less cardiotonics, and a negative fluid balance , a maintenance dose of steroids (25-50 mg prednisolone/day) was given , which was slowly tapered off by 5 mg/day.
Nursing care
In the first few days fol lowing trauma, one nurse per shift was assigned to the patient , being responsible for this patient only (bedside-monitoring) .
73

Results
In this 30-month period a total of 3435 patients were admitted to the ICU , with a global mortality of 3 . 1 per cent . Of these, 265 patients were admitted following trauma and 1 67 fulfi l led the criteria for entering the study. All patients were mechanically ventilated with a mean duration of 1 0.0 days and a maximum of 80 days. In four patients (2 .4%) a tracheostomy was performed. Twenty-three patients died ( 1 3 .8% ) . Table I shows the age , stay, and HTI-ISS of survivors, nonsurvivors and of the total group. The mean age and HTI-ISS of the non-survivors did not statistically differ from those of the survivors. Early death ( 4 days or less)
Table I . Population characterbtlcs.
Survivor� Nonsurvivors Total group
Number of patients 1 44 23 1 67 male 1 1 2 1 7 1 19 female 31 6 38
Mean Age (years) 33.7 + 1 9.6 3 1 . 7 ± 1.u 33 . .f ± 20.3 range 0 - 89 0 - 80 0 - 89
Mean �lay in ICU (day�) l.f . I ± 1 2 9 3. 6 ± 3. .f 1 1. 7 ± 1 2. 6 range 2 - 86 1 - 1 4 1 - 86
Mean HTI-ISS 35 .9 + 1 2 .7 38.� ± 1 2 .6 36 2 ± 1 2 . 7 range 1 8 - 75 J 0 - 59 JO - 75
DISTRIBUTION OF MORTALITY AND ICU-STAY
� z "' � 0. 0 a: "' ID � :J z
Figure 1 .
60 1 67 Trauma Patients
1 3 -4 7 8-14 1 5-2 1 22-29 29-35 36-42 >42 Coys in ICU
� NON-SURVIVORS [SZJ SURVIVORS
Distribution of moriality in relation to the duration of stay in the ICU in 1 67 trauma patients with an HTI-ISS score of 18 or more. The highest mortality occurred in the first 5 days as a consequence of head injuries. From the patients with a prolonged ICU-stay (up to 86 days) only six patient� died
74

occurred in I 7 cases ( I 0.2%) and late death (5 days or more) in 6 (3.6% ) . Figure I presents the relation between mortal ity and duration of stay in the ICU. No patient died after 2 week� of intensive care , although 42 patients (25%) stayed more than 2 weeks in the ICU (up to 86 days) . Head- inj uries were the cause of death in a l l except one patient ; one patient died from acute liver failure of unknown origin , after a relatively small trauma (HTI-ISS- 1 0) . Sepsis and multiple organ failure were not found to be a cause of death .
The age distribution and mortality is presented in Figure 2 . The relationship between age and ISS is shown in a scattergram in Figure 3 . To detect the influence of advanced age on mortality, patients were divided into two groups: patients over 60 year<; ( n=25) , and patients 60 years or younger (n= 142)(Table 2). The difference in mortality was statistically not significant . However, the elderly patients had a significant longer ICU-stay compared to the younger age group (p<O.O I ) .
The relationship between the ISS and mortal ity is presented in Figure 4. Six patients with an ISS of 66 or 75 survived (figure 3 .4) .
Sedation
Thirty-eight patients received a continuous etomidate infusion , with a mean daily dose of 1 1 26 mg (maximum of 2400 mg/day) and for a mean duration of 4 .5
60
50
r 40 z .., ;: � .. 0 JO a: .., m "' :i z 20
1 0
Figure 2 .
DISTRIBUTION OF MORTALITY AND AGE
1 67 Trauma Potienb
0 1 - 10 1 1 -20 2 1-JO 31 -40 41 -50 51 -60 6 1 -70 71 -80 >80Ago Groups
� NON-SURVIVORS 122'.] SURVIVORS
Distribution of mortality in relation to the age of the patient. No significant increase in mortality was found for the advanced age group�.
75

AGE vers u s HTl- ISS
... 0: 0 u Ill >.... i ... > ... Ill >-0: ; z T ;: J:
70
60
50
•O
30
20
1 0 0
D D ••
a.
: D
000 CDCD
• a
D
0 [JJ
D
D D O D DD D ma D
[JJ D �[JJD D ••
D D D D aJDDD<fb
D D
D D CD db c:P D [JJ D
D
D D � • D [JJ
aa.S.8 c£jJ • CD D D aJD 0 D D CD D CD D
20 •O
D
D D D CD D D D D D D
Figure J . 0 SURVIVORS • NON-SURVIVORS
D
D D •
Q[JJ D • D
o o • a [JJ D
� D
D
60
D
D •
D 0 D
80 AGE(yr)
Scattergram !>howing the rel.Ilion hetwecn mortality Wf'• U\ age and HTl- ISS for 1 67 trauma patient,. Six patient' with the h1ghe't HTI-ISS (66 and 75) �urviH!d. Five p.itient' of more than 60 year!> of age died.
I N JURY SEVERITY SCORE AND MORTALITY
t 67 Trauma Patients 1 00ll
90ll
BOii
10-2• 25-29 30-3• 35-39 •0-•4 45-'9 50-5• 55-59 60-75 HTl-ISS
� Pruent Study � lauwu11• flguru Figure 4. Mortality in relation to HTI-ISS. In contrast to other studies 'uch as a recent study of Lauwer!> et al ( 1 986) . no correlation was found between the severity of injury and mortality. The figure� on top of the bars represent the absolute number of patients.
76

days (range I - 1 2 days) . No patient died . These patients had a significantly higher mean-ISS, a longer mean stay in the ICU and received more corticosteroids than the patients receiving sedation with morphine/benzodiazepine (Table 3) .
Fresh frozen plasma
The mean volume of plasma transfused amounted 25 units per patient (standard deviation=27; range 2-205 units). A significant correlation was found between the use of plasma and the HTI-score for abdominal trauma (r=0.57) , the HTI-score for chest trauma (r=0.47) and with the injury severity score (r=0.49) .
Corticosteroids
Apart from the ini tial pharmacological dose of dexamethasone , 59 patients (35% ) received additional corticosteroids during I CU-stay. I n 1 6 patients dexamethasone was given for cerebral oedema while in 43 patients (26% ) prednisolone was given for suspected relative adrenocortical insufficiency. The mean dose of prednisolone was 33.7 ± 2 1 .9 mg/day (± standard deviation ; maximum 100 mg/ day) .
Tahlc 2. Mortality of elderly patients.
0-60 years >60 years
Numhcrof patients 1 42 25
Died 1 8 ( 1 2.6"'0 ) 5 (20"1o ) NS
Mean Age (years) 26.7 ± 1 3 .0 7 1 .8 + 6.92 range 0 - 59 6 1 - 89
Mean �lay in ICU (days) 1 1 .5 ± 9.7 1 9 .6 ± 2 1 .9 p<0.0 1 rc.1ngc 1 - 66 1 - 86
Mean HTl-ISS 36.6 ± 1 3 .2 34.3 ± 9.38 NS range JO - 75 1 9 - 50
Ta hie 3. Comparison of patients surviving 5 <lays or more and receiving two forms of sedation .
Morphine{ benzodiazepincs Etomidate
Number of patients 1 02 38
Mortality 5 (4.9% ) 0
Mean Age (years) 36. J ± 20.5 30.9 ± 1 7 .7 NS
Mean �tay in ICU (days) 1 3 . 1 ± 1 1 .6 18 .4 ± 1 5 .5 p=0.03
Mean HTl-ISS 33.7 ± JO. I 4 1 .4 ± 17 .0 p=0.001
Numher of patients reccivi ng corticosteroids 34 (33%) 25 (66% ) p<0.00 1
Total dose prednisolone 93.8 -t 205. 1 292.8 ± 2 1 8. 1 p<O.!Xl l
77

Discussion
It is generally accepted that the Injury Severity Score is a valuable prognostic index for mortality in multiple injured patients and is useful to evaluate the quality of care and to compare death rates of groups (Bul l . 1 982 ; Greenspan et al . . 1 985) . Table 4 summarizes the mortality reported for different groups of trauma patients. The mortal ity varies between 0% (Seibel et al . . 1 985) and more than 50% for an ISS greater than 45 (Lauwers et al . . 1 986) . with an average mortality of about 25-33% . Although these studies varied widely in inclusion criteria and thus in patient population , they had in common that most of the mortal i ty was caused by multiple organ failure and sepsis.
Table 4. Mortality rate' reported h} other invc,tigator,.
lnve,tigator Year
Sturm ct a l . 1 979
Gori' et a l . 1 982
Pini l la 1 982
Watt & 1 984 Ledingham
Pepe et a l . 1 984
Seibel et a l . 1 985
G linzct a l . 1 985
Baker et al. 1 985
Moore et al 1 985
Lauwers et a l . 1 986
Johnson et al. 1 986
Horst et a l . 1 986
No. of patient'
50
62 1 86 44 83 14
144
54 90 65
20 20
9 7
76 74
1 93 1 70
328
1 30
86
25
!SS Study population
41 Sewn: pol} trauma. excl. brain damage and children .
4 1 Major fracture\. cxcl. children and died < 1 hr
3- 1 � Multiple trauma patient' 1 6-30 .idmittcd to the ICU 3 1 -35 36-50 5 1 -75
Blunt che't trauma
26 Multiple traum,1 patient' 24 admitted to the I CU
32 Pulmonary contusion mult iple major fractures
36.3 Fractured femur or 37.3 acetahulum. ISS >22 29.3 excl. curly deuth
.n and age >65 and < 16
30.2 Exel . early death and 3 1 . 2 preexisting infection
22.5 Mult iple trauma patient' 26.3 admitted to the ICU
Che't inJuric;
36.8 Multiple trauma patienN admitted to the ICU. !SS >25
26 Pulmonary contusion
25 Age over60 years and blunt trauma
Mortality " "
44
IO
8 1 5 18 33 43
8 .3
28 47
26
() () 0 0
30 20
16 1 2
14
33
13
36
• High mortality in multiple trauma patients treated with continuou; etomidate infu;ion.
78

Our study shows that the reduction of mortality is due primarily to the prevention of sepsis and multiple organ failure . particularly in patients with a high ISS and elderly patients. However, the very low late mortality in this study should not be attributed solely to the infection prevention strategy. Infection prevention is part of a complex intensive care treatment, aiming to support not only the respiratory and cardiovascular system, but also the specific and nonspecific defence capacities against trauma and infection of the critically ill patient . However, many therapeutic strategies are still largely empirical and are the �ubject of as many controversies. In the following �ection the contribution of different aspects of treatment are reviewed.
Enrly osteosynthesis
In the past 10 years compell ing evidence has accumulated suggesting that immediate internal fixation of fractures and prophylactic mechanical ventilation reduces the risk of posttraumatic pulmonary insufficiency and �epsis, and decreases mortality (Riidi & Wolff, 1 975 ; Wolff et a l . , 1 978; Riska et al . , 1 977; Goris et al . , 1 982) . The posttraumatic pulmonary insufficiency includes syndromes such as 'fat embolism' or ' ARDS', which probably have the same pathogenesis (Pollak & Myers. 1 978; Amundsen , 1 980) . Johnson et a l . found a significant increase in the incidence of ARDS associated with a delay in operative stabil ization of major fracture�. particularly in patients with �evere injuries (Johnson et al . , 1 985). Seibel et al . studied the effect of prophylactic mechanical ventilation and immediate versus delayed internal fixation of a femur or acetabulum fracture on posttraumatic pulmonary insufficiency in 56 multiple trauma patients. They found that I 0 days of femur traction doubled the duration of pulmonary insufficiency and increased the risk of sepsis. Patients who were treated with femur traction and who were extubated after surgery had the highest incidence of pulmonary insufficiency and sepsis increasing the duration of the intensive care period by a factor 3 to 5 (Seibel et al . , 1 985). Other studies demonstrated that early osteosynthesis without prophylactic mechanical ventilation did not prevent ARDS and that prophylactic mechanical ventilation with positive endexpiratory pressure is only effective in combination with early osteosynthesis (Riidi & Wolff, 1 975 ; Wolff et a l , 1 978; Goris e t a l . , 1 982) . One of the possible mechanisms explaining the favourable effect of mechanical ventilation on the infection rate is the fact that tissue oxygenation is extremely important for local infection defence. It has been shown that systemic antibiotics are effective in preventing wound infections only in the presence of high tissue oxygen- tension (Knighton et al . , 1 986). Therefore appropriate measures should be taken to increase the tissue oxygenation (e.g. mechanical ventilation , cardiovascular support, vasodilators and reduction of interstitial oedema etc) .
79

Steroids
Corticosteroids are of paramount importance in the metabolic response to injury. After severe injury the cortisol levels may increase up to 5 times the normal values i .e . the 'stress-response' . After two weeks the plasma cortisol levels are still twice normal and the diurnal rhythmicity in cortisol is lost (Alberti et a l . , 1 980) . Apart from the well known metabolic effects, corticosteroids have many complex functions including stimulation of the synthesis of acute phase proteins, potentiation of the effect of catecholamines, preservation of the integrity of small vessels, reduction of platelet adhesiveness , inhibition of prostaglandin synthesis and bradykinin formation . inh ibition of aggregation of leukocytes and stabilisation of l iver lysosomal membranes (Gann & Lilly , 1 983). Little is known of the optimal plasma cortisol levels in intensive care patients nor is i t possible to adequately monitor corticosteroid functions.
Steroid therapy remains a controversial area. The reluctance in prescribing corticosteroids in intensive care patients is based on fear of infections and the catabolic effects and the delay of wound healing by h igh doses of corticosteroids. However, occult and untreated adrenocortical insufficiency in the intensive care patient is described in association with sepsis (Sibbald et a l . , I 977) , following general or cardiac surgery (Hubay et a l . 1 975 : Alford et al . , 1 979) . or due to posttraumatic adrenal haemorrhage (Sevitt et a l . , I 955) , or by medication such as etomidate (Wagner et al . , I 984; Watt & Ledingham. 1 984) : it is reported to have a h igh mortality. Occult or relative adrenocortical insufficiency is characterized by plasma cortisol levels that may be stil l within the normal l imits but which fail to respond to synthetic ACTH (Sibbald et al . , I 977) . The presenting symptoms are hypotension , despite maximal inotropic support and volume loading, fever, tachycardia, 'capillary leak', and increased susceptibility to infections. The classical picture of
an Addisonian crisis is seldom seen in these patients. since many signs are masked by symptomatic therapy such as control of fluid and electrolyte balance . The diagnosis is confirmed by an adequate clinical response to intravenous corticosteroid administration (two to three times normal maintenance dose) . In the present study relative adrenocortical insufficiency was observed in 43 patients, part of which were probably caused by the use of continuous infusion of etomidate. The administration of the socalled 'pharmacological dose' of corticosteroids is shown to be effective in the prevention of adult respiratory distress syndrome (ARDS) or 'fat embolism' or posttraumatic pulmonary insufficiency following severe trauma (Rokkanen et a l . , I 974; van der Merwe et al . , I 985) . In a prospective controlled study in patients with severe blunt injury of the chest and pulmonary contusion, Svennevig et a l . ( 1 984) have shown that the administration of a bolus of methylprednisolone (30 mg/kg iv) produced a significant reduction of the pulmonary vascular resistance and the right ventricular work load, compared to a non-treated
80

control group. This effect was noticeable up to the fifth day after trauma. The non-treated patients had to be mechanically ventilated more often, had significantly more respiratory tract infection-., and developed hypercoagulability and ' fat embolism' more often than the treated group. Apparently, the benefits of corticosteroids outweigh the potential adver-.e effects in the!>e circum�tances. The choice of corticosteroids seems to be important with reference to the effect on the phagocytic and bactericidal capabilitie� of normal human granulocytcs; in a recent study it was found that hydrocortisone and methylprednisolone had a deleterious effect on phagocyto�is of granulocyte-.. wherea� dexamethasone with a con�iderably greater anti inflammatory effect than the other two steroids, had no adverse effects on phagocytosis (Baltch et al . , 1 986) . This is in agreement with the clinical observation that dexametahasone treatment did not increase the incidence of pneumonia in mechanically ventilated headtrauma patients (Braun et al . , 1 986) . I n the present study a pharmacological dose o f dexamethasone was admin i�tered on arrival in the hospital , but due also to the infection prevention regimen. no infectious complications of corticosteroids were observed.
Plasma substitution
Following trauma. the cascade-systems e .g . the coagulation . fibrinolytic, kall ikrein-kinin and complement systems, are al l activated (Risberg et a l . , 1 986). These �ystems. that are al l in timately related in a very complex way, play a specific role in the development of posttraumatic pulmonary insufficiency (Risberg & Heideman. 1 980) . The natural inhibitor� of the�e �y�tems are the acute phase proteins: antithrombin-1 1 I, oc2-macroglobul in , oc 1 -antitrypsin and fibronect in . Most of these proteins are concentrated in strategic positions such as alveolar macrophages, or in the luminal surface of endothelial cells of arteries, veins, and lymphatics. Immediately after trauma the prekall ikrein , ATi l l . fibronectin and complement levels are significantly decreased during 4-5 days (Wilson et al . , 1 986; Kapur et a l . , 1 986; Stahl et al . , 1 985) .
Antithrombin-Ill
Antithrombin-I I I (ATI I I ) is the major inhibitor of thrombin and other serine proteases in the blood coagulation system. ATII I is activated by heparin and forms an irreversible complex with activated clotting factors (e .g . thrombin , factor x .. , and plasmin) which is in turn cleared by the reticulo-endothelial system (RES) (Bick et al . , 1 977) . ATII I is also a potent inhibitor of plasma kallikrein (Burrowes et al . , 1 975) and of the first component of complement but only in the presence of heparin (Ogston et al . , 1 976) . By a specific immunofluorescent techn ique ATll I was found to be localised predominantly in the microvasculature of the lung and kidney, and in the walls of the large vessels , but also in the l iver and
8 1
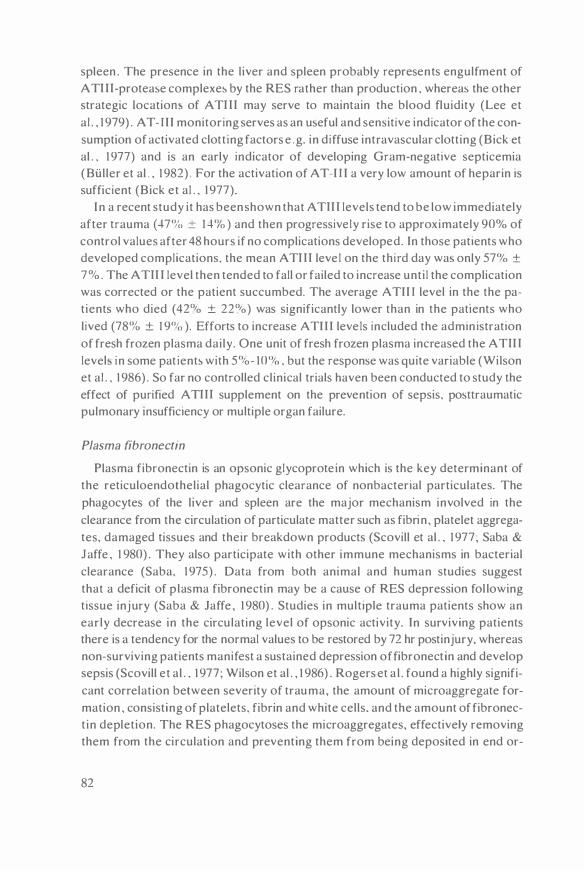
spleen . The presence in the liver and spleen probably represents engulfment of A Ti i i-protease complexes by the RES rather than production , whereas the other strategic locatiom of A Ti i i may serve to maintain the blood fluidity (Lee et al . , 1 979) . AT- I I I monitoring serves as an useful and sensitive indicator of the consumption of activated clott ing factors e .g. in diffuse intravascular clotting (Bick et al . , 1 977) and is an early indicator of developing Gram-negative septicemia (Buller et al . , 1 982) . For the activation of AT-I I I a very low amount of heparin is sufficient (Bick et al . , 1 977).
I n a recent study it has been shown that A Tii i levels tend to be low immediately after trauma (-t7'Yc, ± 1 -t'Yo ) and then progressively rise to approximately 90% of control values after 48 hours if no complications developed. In those patients who developed complications, the mean A Ti i i leve l on the third day wa� only 57% ± 7%. The A Tii i level then tended to fall or failed to increase unti l the complication was corrected or the patient succumbed. The average ATII I level in the the patients who died ( 42% ± 22%) was significantly lower than in the patients who lived (78'Yo ± 1 9% ). Efforts to increase ATI I I leve ls included the admin istration of fresh frozen plasma daily. One unit of fresh frozen plasma increased the A Tii i leveb in some pat ient� with 5%- 10% , but the response was quite variable (Wilson et al . , 1 986) . So far no controlled clinical trials haven been conducted to study the effect of punfied A Tii i supplement on the prevention of sepsis, posttraumatic pulmonary insufficiency or multiple organ failure.
Plasma fibronectin
Plasma fibronectin is an opsonic glycoprote in which is the key determinant of the reticuloendothelial phagocytic clearance of nonbacterial particulates. The phagocytes of the liver and spleen are the major mechanism involved in the clearance from the circulation of particulate matter such as fibrin , platelet aggregates, damaged tissues and their breakdown products (Scovill et al . , 1 977; Saba & Jaffe , 1 980) . They also participate with other immune mechanisms in bacterial clearance (Saba, 1 975) . Data from both animal and human studies suggest that a deficit of plasma fibronectin may be a cause of RES depression fol lowing tissue injury (Saba & Jaffe , 1 980) . Studies in multiple trauma patients show an early decrease in the circulating level of opsonic activity. In surviving patients there is a tendency for the normal values to be restored by 72 hr postinjury, whereas non-surviving patients manifest a sustained depression offibronectin and develop sepsis (Scovill et al . , 1 977; Wilson et al . , 1 986) . Rogers et a l . found a highly significant correlation between severity of trauma, the amount of microaggregate formation , consisting of platelets. fibrin and white cells. and the amount of fibronect in depletion. The RES phagocytoses the microaggregates, effectively removing them from the circulation and preventing them from being deposited in end or-
82

gans. The depletion of fibronectin and the associated RES depression might be responsible for the development of diffuse intravascular coagulation , posttraumatic pulmonary insufficiency. and multiple organ failure (Rogers et a l . , 1 986) . Infusion of cryoprecipitate . which is rich in fibronectin, reversed the opsonic activity and the RES-failure (Saba et a l . , 1 978 . 1 984) , improved pulmonary function, renal function and the microcirculation (Scovi l l et al . , 1 979; Annest et a l . . 1 980) . I n the study of Scovill e t a l . a mean of 329 m g of fibronectin was administered . Cryoprecipitate contains approximately 2 mg/ml fibronectin, fresh frozen plasma 0.33 mg/ml , and cryoprecipitate-extracted plasma ('single donor plasma') 0. 1 mg/ml .
Immunoglobulins
Glinz et a l . reported a marked deficit of immunoglobulins, complement factors and acute-phase proteins, during the first 1 2 days following trauma. In a prospective , placebo-controlled double blind trial in multiple trauma patients who required longterm mechanical ventilation, they were able to demonstrate the prophylactic effect of intravenous immunoglobulins on the incidence of pneumonia. However, no effect on the mortality rate was found compared to the untreated control group. The amount of immunoglobulin administered in this study (3 times 1 2 g purified immunoglobul in) appeared to be an insufficient quantity to produce a significant change in plasma IgG-levels. Since the halflife of infused immunoglobulins in healthy individuals is about three weeks, this may indicate a large extravascular deficit of immunoglobulins or a pathological consumption or loss of administered IgG (Glinz et al . , 1 985) . Apart from low immunoglobulin levels there is evidence that complement is also depleted in the postinjury period following moderate to severe injury (Kapur et a l . , 1 986; Stahl et al . , 1 985) . To reverse the immunosuppressive effect of trauma both immunoglobulins and complement should be substituted.
In the controversy over the use of crystal loid versus that of colloid in resuscitation , the depletion of acute-phase proteins, in particular ATI I I and fibronectin , and of immunoglobulins and clotting factors, in the first week following trauma, has received very l ittle attention . The main subject of discussion has been the reduction of the plasma oncotic pressure by crystalloid fluid and the subsequent development of interstitial oedema and pulmonary insufficiency (Lowe et al . , 1 979) . Considering the accumulating clinical evidence of the beneficial effects of substituting these plasma proteins by the administration of special preparations such as cryoprecipitate, purified immunoglobulins, or ATII I -concentrate, substitution therapy using fresh frozen plasma should begin immediately upon admission to the hospital , rather than waiting unti l the advent of multiple organ fai lure, before
83

commencing treatment . Due to the increased capillary permeabi l ity in the first days fol lowing severe trauma , plasma proteins leak into the extravascular space (Sturm et al . . 1 986) , and often a large amount of colloid solution is necessary to maintain an adequate circulation; this should be given partly as fresh frozen plasma to compemate for the loss of essential plasma proteins. To augment the effect of administered ATI I I 'mini ' amounts of heparin are added to the fresh frozen plasma ( 10 00 E heparin/unit fresh frozen plasma) . In the present study. the amount of fresh frozen plasma uti l ised . represents 6 t imes the amount of fibronectin used by Scovi l l ct a l . ( 1 979) and 2 times the amount of 1mmunoglobulins used by Glinz et al . ( 1 985) . The question whether in our study the use of fresh frozen plasma and heparin has contributed to the overal l favourable outcome . should be answered in a separate clinical investigation .
Analgesia and sedation
As yet li ttle attention has been paid to the effect of sedatives. analgesics and muscle relaxants on the colonisation defence of the oropharynx and intestines. However. anaesthesia, heavy sedation or analgesia and especially muscle relaxants do depress salivary flow . swallowing and peristalsis and may thus adversely affect the colonisation defence. This might be the explanation for the high incidence of pneumonia in comatose patients particularly when treated with barbiturates (Espersen & Gabrielsen. 1 98 1 ; Braun et al , 1 986) or in patients treated with continuous etomidate (Watt & Ledingham. 1 984) . Often a vicious circle develops starting with agita tion , then sedation . followed by colonisation and infection with impairment of vital functions. leading to more agitation and more sedation and so forth . The high mortal ity (77%) with continuous infusion of etomidate , reported by Watt & Ledingham. was due to infection and multiple organ failure (Watt & Ledingham , 1 984) . In the present study no patient using etomidate died, probably due to the use of corticosteroid suppletion and adequate infection prevention . Where continuous sedation or muscle relaxation is deemed necessary. e .g . in patients with head injuries. or in patients having h igh PEEP or being treated with differential lung ventilation. infection prevention as described in the previous chapters, is essential . Besides, infection prevention reduces the need for heavy sedation after the first few days following trauma . provided the vital organ functions are stabilised.
Organisation
The effect of organisation . and the staff to patient ratio on the outcome of intensive care in trauma patients has not been extensively studied so far. Baker et al . reported that the institution of a trauma service and reorganisation of a surgi-
8-l

cal intensive care , decreased the mortality rate from 1 6 to 6% and he i.uggested that the aggressive preventive management led to a reduction in the mortality from multiple organ failure and sepsis (Baker et al . , 1 985) . In our institution the use of an established treatment protocol , the high nuri.e :patient ratio, the good quality of nursing care , the round the clock presence of a qualified anesthetist-intensivist in the ICU , and the availability of a traumatological staff, may all have contributed to the low mortality.
Conclusion
The favourable results reported in this study are achieved by an aggressive and integrated strategy of management of the multiple trauma patient by a team of trauma surgeons, anesthetists and intensivists. The emphasis is laid on prevention, which implies aggressive resuscitation, prophylactic mechanical ventilation, early internal fixation of fractures, prevention of diffuse intravascular coagulation, and prevention of infections. The nonspecific infection defence should be supported by substitution of essential plasma proteins, metabolic care and optimal tissue oxygenation .
85


Chapter 7
Nosocomial gram-negative pneumonia in critically i l l patients A 3-year experience with a novel therapeutic regimen
Christiaan P . Stoutenbeek , H . K . F. van Saene" , 0 . R. Miranda, 0 . F. Zandstra and 0. Langrehr
Dcpartmcnt of Anc,thc,iology and l ntcn\iVO.: Carc. Dcpartmcnt of Clinical Bactcriology ' . Univcrsity Hospita l , G roningcn . The Ncthcrlamh
Intensive Care Medicine 1 2:4 19 ( 1986)
87
Abstract
The efficacy of selective decontamination of the oral cavity and GI-tract i n the treatment of established Gram-negative pneumonia in critically i l l patients was evaluated in a prospective open trial . Twenty-five patients with pneumonia caused by Enterobacteriaceae or Pseudomonadaceac were studied. All patient� were mechanically ventilated (range 2- 60 days) . Non-absorbable antibiotics (polymyxin E 100 mg, tobramycin 80 mg. amphotericin B 500 mg) were administered through the nasogastric tube four times a day. The oral cavity was decontaminated with an ointment containing 2% of the �ame antibiotics, applied to the buccal mucosa four times a day. For systemic therapy a combination of tobramycin (3-6 mg/kg) with either cefotaxime (50- 1 00 mg/kg) or ceftazidime ( 100 mg/kg) was given both intravenously and by aerosol (50% intravenous dose/5 ml saline) four times a day . Eradication of pathogens from the respiratory tract was achieved in 24 patients within 9 days (median 5 days). The cure rate was 96% . Two patients had a relapse . Neither recolonisation with resistant organisms nor supra-infections were found for the remaining period of mechanical venti lation (up to 60 days) , also after systemic/aerosol therapy had been discontinued . Only 3 patients died ( 12%) .
Introduction
Nosocomial Gram-negative pneumonia in the ICU has a notoriously high mortality (33%-70%) and can be exceedingly difficult to treat (Stevens et al . , 1974; Cross & Roup. 198 1 ; Martin et a l . , 1 984; Bryan & Reynolds, 1 984; Tobin & Grenvik , 1984; Schentag et a l . , 1 985) . Whilst the patient remains intubated it is difficult to eradicate Gram-Negative Bacilli (GNB) from the respiratory tract with systemic antibiotic therapy alone , even when using potent new antibiotics (Reitberg et a l . , 1984; Schentag et a l . , 1985) . The incidence of relapse and superinfection is h igh (Tillotson & Finland 1969 ; Reitberg et al . , 1 984; Stoutenbeek et a l . , I 984b; Weinstein & Reller, 1984) .
I n the pathogenesis of Respiratory Tract Infections (RTI) contaminated ventilatory equipment no longer plays an important role (Comhaire & Lamy, 1 98 1 ; Cross & Roup, 1 98 1 ) , the major source of pulmonary pathogens being the oropharynx (Johanson et a l . , 1972 ; La Force , 198 1 ; Crouch et a l . , 1 984) . In healthy individuals oropharyngeal colonisation by GNB is uncommon (La Force et al . , 1 976). Critically i l l patients, however, are quickly colonised by nosocomial GNB . The most important determinants of colonisation are host characteristics e .g. the underlying disease (Cross & Roup, 1 981 ; Johanson et a l . , 1972) , advancing age (Valenti , 1978) and antimicrobial therapy (Yoshioka et al . , 1 982) . Once heavy colonisation of the oropharynx with GNB is established (> 105 bacteria/ml) lower respiratory tract colonisation i nvariably follows, particularly in intubated pa-
88

ticnts (van Uffclcn ct a l . , 1 984) and this may lead to the deve lopment of a Gramncgativc pneumonia .
A previous study has shown that selective decontamination of the oropharynx and G I-tract i::. effective in the prevention of nosocomial infections (Stoutcnbcck ct a l . , 1 984) . This regimen depended on the administration of oral nonabsorbablc antibiotic::. known to preserve the indigenous flora, thus reducing the ri::.k of overgrowth by rc�istant organisms (van dcr Waaij , 1 979) . Since 1 982 it has been routinely u.,cd in all patient� requiring prolonged intensive care . This study was designed to evaluate the use of the same regimen in combination with ncbuliscd antibiotic� in the treatment of c::.tablishcd Gram-negative pneumonia .
An open, prospective trial was performed in patients with pneumonia caused by Entcrobactcriaccac or P�cudomonadaccac to observe the effect of thi� regimen on mortal i ty and clinical and bacteriological cure rates.
Patients and methods
Patient� admitted to the surgical Intensive Care Unit ( ICU) of the University Hospital Groningen between January 1 982 and December 1 984 were studied. Criteria for entering in to the trial were pneumonia caused by Enterobacteriaceae or Pseudomonadaceae, respiratory insufficiency requiring endotracheal intubation and mechanical ventilation (for at least 2 days) and prolonged intensive care (5 days or more) . Twenty-five patient� were included in the study. Characteristics of the study population are listed in Table I . Except for five multiple trauma patients. most patients were elderly patients (median age 63 years) . All patients had severe underlying disease and were orotracheally intubated and mechanically venti lated . The duration of stay in ICU varied from 5 to 79 days (mean 1 8.2 ± 1 7 .4) and the length of mechanical ventilation from 2-60 days.
Diagnosis of pneumonia was made on a clin ical picture of pyrexia, leukocyto!.is, respiratory insufficiency and new infi l trations on the chest roentgenogram. Purulent sputum on Gram-stain (>25 leukocytes per microscopic field) and heavy growth of GNB from tracheal aspirate confirmed the diagnosis (Stevens et a l . , 1 974 ; Tobin & grenvik , 1 984) .
Antibiotic regimen
(i) Intravenous antibiotics
A combination of two synergistic antibiotics was used: for Enterobacteriaceae infections: cefotaxime (50- 1 00 mg/kg/day) + tobramycin (3-6 mg/kg/day) and for Pseudomonadaceae infections: ceftazidime ( 1 00 mg/kg/day) en tobramycin (3-6 mg/kg/day) .
89
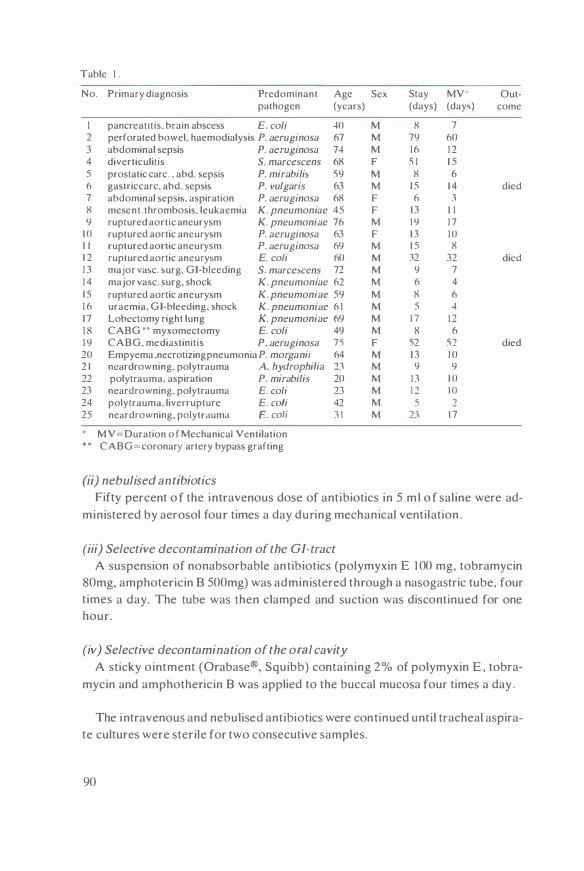
Table I .
No.
I 2 3 4 5 6 7 8 9
1 0 1 1 1 2 1 3 1 4 1 5 1 6 1 7 1 8 1 9 20 2 1 22 23 24 25
.
Primary diagnosis Predominant Age pathogen (years)
pancrealltis. brain abscess E. coli 40 perforated bowel. haemodialysis P. aeruginosa 67 abdominal sepsis P. aeruginosa 74 diverticulitis S. marcescens 68 prostatic carc . . abd. sepsis P. mirabilis 59 gastriccarc, abd. sepsis P. vulgaris 63 abdominal sepsi�. aspiration P. aerugmosa 68 mesent . thrombosis. leukaemia K. pneumoniae 45 ruptured aortic aneurysm K. pneumoniae 76 ruptured aortic aneurysm P. aeruginosa 63 ruptured aortic aneurysm P. aeruginosa 69 ruptured aortic aneurysm E. coli 60 major va�c. �urg. GI-bleeding S. marce�cens 72 major vasc. surg, shock K. pneumoniae 62 ruptured aortic aneurysm K. pneumoniae 59 uraemia, G I-bleeding. shock K. pneumoniae 6 1 Lobectomy right lung K. pneumoniae 69 CABG •• myxomectomy E. coli 49 CABG, mediastinitis P. aeruginosa 75 Empyema .necrotizing pneumonia P. morganii 64 ncardrowning. polytrauma A. hydrophi/ia 23 polytrauma. aspiration P. mirabilis 20 neardrowning, polytrauma E. coli 23 polytrauma. liverrupture E. coli 42 neardrowning, polytrauma E. coli 3 1
M V=Duration o f Mechanical Ventilation CABG=coronary artery bypass grafting
(ii) nebulised antibiotics
Sex Stay MY Out-(days) (day�) come
M 8 7 M 79 60 M 16 1 2 F 5 1 1 5 M 8 6 M 1 5 1 4 died F 6 3 F 13 I I M 1 9 1 7 F 13 10 M 1 5 8 M 32 32 died M 9 7 M 6 4 M 8 6 M 5 4 M 1 7 1 2 M 8 6 F 52 52 died M 1 3 1 0 M 9 9 M 1 3 1 0 M 1 2 to M 5 2 M 23 1 7
Fifty percent o f the intravenous dose of antibiotics in 5 m l o f saline were ad-ministered by aerosol four times a day during mechanical ventilation .
(iii) Selective decontamination of the GI-tract
A suspension of nonabsorbable antibiotics (polymyxin E 1 00 mg, tobramycin 80mg, amphotericin B 500mg) was administered through a nasogastric tube, four times a day. The tube was then clamped and suction was discontinued for one hour.
(iv) Selective decontamination of the oral cavity
A sticky ointment (Orabase®, Squibb) containing 2% of polymyxin E , tobramycin and amphothericin B was applied to the buccal mucosa four times a day .
The intravenous and nebulised antibiotics were continued until tracheal aspirate cultures were sterile for two consecutive samples.
90
Bacteriological surveillance
Tracheal aspirate and oral swabs were collected on admission and three times a week thereafter. Al l samples were cultured semi-quantitatively on agar plates and in broth (brain heart infusion) . Growth density was graded according to the four quadrant method ( + 1 to +5 ) . Bacterial identification, typing and sensitivity patterns were performed using standard methods (van Saene et al . , 1983a) .
Definitions
Selective Decontamination: el imination of potentially pathogenic microorganisms (aerobic GNB and yeasts) whi lst preserving the indigenous flora (anaerobes, streptococcus vi ridans etc) . Colonisation: the isolation of the same bacterial species from two or more consecutive samples from the same site in a growth density > + 1 , without cl inical signs of infection . Colonisation was assumed to extend from the preceding negative culture until the first sample in which that particular GNB was no longer present . Suprainfection: an infection at any s i te with organisms resistant to the antibiotics used (Weinstein & B rown , 1977) .
Results
Infection rate
In the 3-year study period 4 1 44 patients were admitted to the ICU . 701 of these patients required prolonged mechanical ventilation and stayed 5 days or more in the ICU . Twenty-five patients (3 . 5%) had a pneumonia caused by Enterobacteriaceae or Pseudomonadaceae .
Clinical and bacteriological cure rate
The predominant pathogens were E. coli, P. aeruginosa, and K. pneumonia
(Table 1 ) . Eradication of pathogens from tracheal aspirate was achieved i n 24 patients (96% ) within 9 days after starting treatment (median 5 days)(figure 1 ) .
The clinical cure rate was 96% (24/25) . Two patients had a relapse (Nos.2 and 19). No suprainfections with resistant organisms occurred. Also after discontinuing the systemic and aerosol antibiotics, no secondary colonisation of the respiratory tract by GNB was demonstrated in the remaining period of mechanical ventilation (up to 60 days) .
9 1
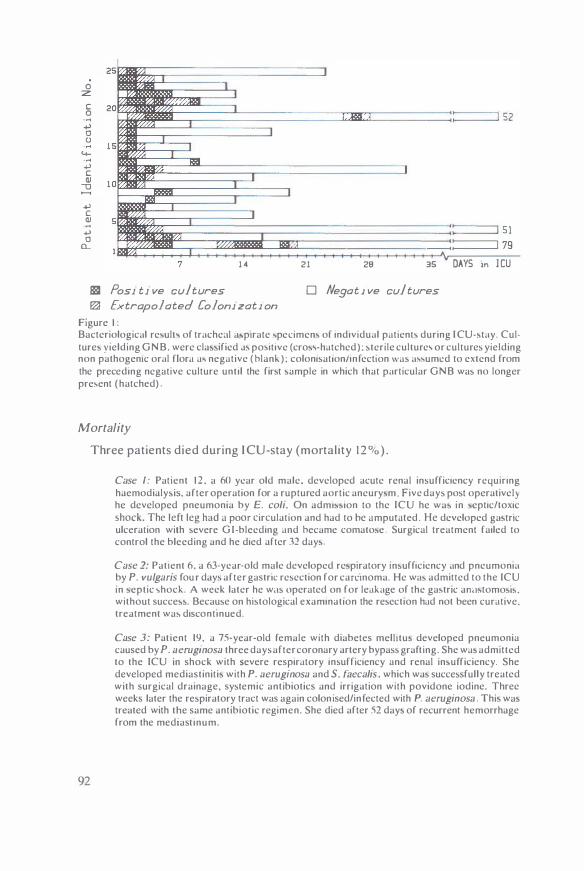
0 :z
c 0 ..... .., 0 (J
4-..... .., c QJ
-0
.., c QJ .... .., 0
CL
7 1 4 21 28 35 DAYS in J CU
881 Pos1 t1 ve cultures D Negat i ve cultures � Extrapolated Coloni zati on
Figure I : Bacteriological re,ulh of trache,11 a'p1rate 'pecimen' of individual patienh during I CU-,tay. Culture' yielding GNB. were cla,,ificd J' positive (cro,\·hatched) : 'terile culture\ or cultures yielding non pathogenic oral flora a' negative ( hlank ) : colonisat1on/infect1on was a"umcd to extend from the preceding negative culture unti l the fir't •ample in which that particular GNB was no longer pre;ent (hatched)
Mortality
92
Three patients died during I CU-stay (mortality 1 2 % ) .
Case I: Patient 1 2 . a 60 year old male. developed acute renal insufficiency requiring haemodialy,is. after operation for a ruptured aortic aneury'm Five days post operative I) he developed pneumonia by E. coli. On admb•ion to the ICU he wa' in 'eptic/toxic shock. The left leg had a poor circulation and had to he amputated . He developed ga>tric ulceration with severe G I-bleeding and hecame comato,e . Surgical treatment failed to control the bleeding and he died after 31 day•.
Case 2: Patient 6, a 63-year-o ld male developed rc,p1ratory in,ufficicncy and pneumonia by P. vulgaris fou r ddys after gastric resection for camnoma. He wa' admitted to the ICU in •eptic 'hock A week later he w<1s operated on for leakage of the ga,tric ami>tomo''' · without succe>>. Because on histological examination the resection had not been curative. treatment was discontinued.
Case 3: Patient 19. a 75-year-old female with diabetes melhtu> developed pneumonia caused by P. aeruginosa three days after coronary artery bypass grafting. She wa> admitted to the ICU in shock with severe respiratory in>ufficiency and renal in>ufficiency. She developed mediastiniti' with P. aeruginosa and S. faecal is . which wa' successfully treated with surgical drainage, systemic antibiotics and irrigation with povidone iodine. Three weeks later the respiratory tract was again colonised/infected with P aeruginosa . Thi' wa> treated with the same antibiotic regimen. She died after 52 day> of recurrent hemorrhage from the mediast inum.
Oropharyngea/ colonisation
In 84% of patients the oropharynx was colonised by the same pathogen that caused pneumonia (APl-number, sensitivity pattern ) . The growth density was high (mean 2 .9 ± 1 .2 ) , corresponding to 1 05 bacteria/ml saliva. To evaluate the effect of selective decontamination on colonisation by GNB , baseline cultures were compared with cultures taken 3 days after starting treatment. In the first 3 days 72% of oropharyngeal cultures yielded GNB, compared to 1 6% after 3 days (p<0.00 1 ). Eradication of GNB was complete in 92% of patients (23/25) within 3 days . Secondary colonisation with GNB occurred in 3 patients ( 1 2% ) . I n two cases transient colonisation developed with organisms (Pseudomonas spp. ) sensitive to the oral nonabsorbable antibiotics.
Discussion
In ventilated patients the diagnosis of pneumonia can be very difficult as many signs are nonspecific. Bell et al. ( 1 983) compared post-mortem findings with the clinical diagnosis of pneumonia and found a false negative diagnosis rate of 62% . They also found that cl in ical signs apppeared at a late stage, when it is often too late for adequate chemotherapy. However, attempts to treat colonisation or infection with systemic antibiotics before clinical symptoms are present, is unsatisfactory and increases the risk of suprainfections (La Force, 1 98 1 ) . The new generation of potent broad-spectrum antibiotics did not solve this problem. Schentag et al. ( 1 985) found that during aztreonam therapy, resistance of the original pathogen emerged in 7% of cases and suprainfection with a different pathogen in 38% of patients. Similar results were reported using tobramycin (Schentag et al . , 1 985) or cefmenoxim (Reitberg et al . , 1 984) .
The high incidence of emergence of resistant organisms may be explained by the peri- inhibitory concentrations of the antibiotics in the lumen of the oral cavity and bowel . Resistant organisms may then replace the normal flora , result ing in suprainfection. This is confirmed by a previous study (Stoutenbeek et al . , I 984b) demonstrating that suprainfections were invariably preceded by colonisation of the oropharynx or G I-tract by resistant organisms.
In this study, only 25 cases of pneumonia caused by Enterobacteriace&e or Pseudomonadaceae were diagnosed during a 3-year period. Although the infection rate may be underestimated by using strict criteria for diagnosis of pneumonia, only severe cases of G ram-negative pneumonia were included in this study. Most patients had established pneumonia on admission to the ICU . Few patients developed Gram-negative pneumonia during ICU-stay as a result of an effective infection prevention policy using selective decontamination (Stoutenbeek et al . , 1 984a) . I n the treatment of Gram-negative pneumonia i n intubated patients i t is
93

crucial to el iminate the aerobic GNB from the oral cavity and GI-tract. This can be achieved by the administration of high doses of nonabsorbable antibiotics in the oropharynx and GI-tract. Selective decontamination of the GI-tract is necessary in order to prevent (i) ascending respiratory tract infections from contaminated gastric content (Atherton & White , 1 978; Hillman et al , 1 982) , and ( i i ) to prevent infections of the urinary tract and/or of wounds (Stoutenbeek et al . , I 984a) , and ( i i i ) to prevent selection of resistant organisms in the oral or intestinal flora. Once the source of pathogens ( i .e . the oral cavity or GI-tract) has been eliminated , the focus can be effectively treated. In this study this was achieved by a combination of drugs given both systemically and by nebulisation . The resulting high antibiotic concentration within the bronchial tree eradicated the causative GNB with in 9 days. Only two patients had a relapse after withdrawal of specific therapy. Because colonisation of the respiratory tract with GNB is considered to be a premonitory sign of infection this was treated with the same regimen. The remainder of the patients �tayed free of GNB for the duration of mechanical ventilation (up to 60 days) .
The major factors determining outcome of nosocomial Gram- negative pneumonia are age and the underlying pathology (Cross & Roup, 1981 ; Bell et al . , 1 983 ; Bryan & Reynolds . 1 984; Martin et al . , 1 984) . However, this study has shown that with aggressive therapy it is possible to achieve a high clinical and bacteriological cure rate even with severe underlying disease . The prevention of �econdary colonisation and suprainfection by selective decontamination might have been essential in the final outcome. Although the design of this study does not allow a comment on the contribution of the antibiotic regimen on the low overall mortal ity ( 1 2% ) , the difference with conventional antibiotic therapy is striking. Confirmation of these results by a randomised comparative trial is required.
Acknowledgements:
We thank the nurses of the ICU and the technicians of the microbiology laboratory for their cooperation. Dr. Kevin West MD is gratefully acknowledged for the many valuable comments in preparing the manuscript.
94

Chapter 8
General discussion
95
What's in a name?
Selective elimination of Enterobacteriaceae from the digestive tract was described for the first time by Yan der Waaij , who treated mice and monkeys with oral nalidixic acid (van der Waaij & Berghuis, 1 974 ) . In later clinical studies it was named 'Partial antibiotic decontamination' (Guiot & van Furth , 1 977) . 'Selective
decontamination of the digestive tract' (Sleyfer et al . . 1 980) or 'Selective antimi
crobial modulation' (Guiot et al . . 198 1 ) . The latter term has also been adopted by others ( Kurrie et a l . , 1 98 1 ; Wade et al . , 1 983) . At the start of the studies described in this thesis. the Groningen nomenclature was used. However, the term 'selective decontamination of the digestive tract' is open to question . The term decontamination is used mostly in conjunction with disinfection of inanimate objects and not for flora-modulation . Moreover, the term 'decontamination of the digestive tract' suggests that only the intestinal flora is treated and although this may be the case in leukaemic patients, in intensive care patients the oropharyngeal flora is of utmost importance . In this thesis, selective decontamination is defined as selective elimination of potentially pathogenic microorganisms from both the oral and intestinal flora by topical nonabsorbable antibiotics. Therefore in the later studies (Chapter 5 ,6) the terms ' infection prevention by topical nonabsorbable antibiotics· or ·selective flora suppression ' have been used.
How 'selective' are the topical nonabsorbable antibiotics?
The studies described in this thesis were designed to evaluate the clinical effects of selective elimination of aerobic potentially pathogenic microorganisms from the microflora by topical nonabsorbable antibiotics, using polymyxin E , tobramycin and amphotericin B . No attempt has been made to measure the influence of the antibiotic regimen on the indigenous anaerobic flora , since most intensive care patients do not produce faeces and recovery of anaerobes from rectal swabs is highly unreliable. Indirectly, a disturbance of the indigenous flora can be measured by the concentration of Streptococcus viridans, enterococci and Staphylo
coccus epidermidis. However, a flora-shift may result not only from the antibiotic regimen, but from many factors which decrease the colonisation-defence. Therefore . the 'selectivity' of this antibiotic combination has been investigated under controlled circumstances in healthy volunteers. The preliminary results of this study with a combination of polymyxin E and tobramycin , show that there are no signs of disturbance of the indigenous flora (Thiilig, personal communication) .
I s the anaerobic Dora important i n ICU patients?
( i) ls the preservation of the anaerobic flora in intensive care patients essential
for the efficacy of topical nonabsorbable antibiotics ?
96

Van der Waaij has shown in mice, that the indigenous anaerobic flora is respon'iible for the capacity to resist against colon isation by exogenous microorganisms and he has named this phenomenon 'Colonisation Resistance' (van der Waaij et al . , 1 97 1 ). The observation that antibiotic regimens aiming at 'total gut steril isation' using oral gentamicin , vancomycin or neomycin , were associated with coloni�ation or even ma�sive overgrowth by both sensitive and resistant microorganisms (Bodey & Rosenbaum , 1 974; Klastersky et a l . , 1 974; Bodey & Rodriguez, 1 976; Schimpff et al . , 1 980) has been explained by the loss of 'colonisation resistance' due to the �uppressive effects of the antibiotics on the anaerobic flora. However, this might not be the only reason for this fai lure , 'iince in-vitro tests have shown that gentamicin and neomycin are almost completely inactivated by faeces (van Saene et al . , 1 985a)(vide infra) . In our experience with patients receiving high doses of antibiotics known to affect the anaerobic flora e .g . cloxaci l l in , clindamycin or ampici l l in and who were treated simultaneously with the topical antibiotic regimen , no overgrowth by �en'iit ive or resistant microorgan isms occurred. This observation , that the topical antibiotics are also effective in the presence of a severely affected anaerobic flora , �uggests that the effectiveness of the oral antibiotics may be independent of the anaerobic flora . (ii) ls the preservation of the anaerobic flora important for the colonisation defence ?
The anaerobic flora i� not the only factor, and certainly not the most important factor constituting the colon isation-defence . The most important mechanisms are those that mechanically clear microorganisms from the oral cavity or gastro-intestinal tract e .g. swallowing, salivary flow , chewing and peristalsis (LaForce et al . , 1 976; Dack & Petran , 1 934 ; Dixon , 1 960) and those that influence the bacterial adherence to the mucosa e .g. mucus, secretory-IgA and changes in the mucosa) surfaces (Johanson et a l . , 1 979) (See chapter I ) . In intensive care patients many of these mechanisms are severely impaired: patients may be comatose or anaesthetised or receiving muscle relaxants and may not be able to swallow, to eat or to drink . Often patients have no peristalsis for a considerable length of time and may receive prophylaxis against stress-ulcers with antacids or Hrantagonists, defeating the gastric acid barrier. The minor importance of the anaerobic flora in intensive care patients is i l lustrated by the rapid colonisation by exogenous microorganisms in patients not receiving any antibiotic and with a normal anaerobic flora e .g polytrauma patients. Probably the role of the anaerobic flora gains importance when the other factors constituting the colonisation defence are recovering. The impaired colonisation-defence in the critically i l l patient is crucial in the pathogenesis of nosocomial infections and should be the subject of future investigations.
97

Which antibiotics affect the anaerobic flora?
The classification of antibiotics into those which decrease the 'colonisation resistance· and those which are indifferent . is based on oral administration of the drugs in mice (van der WaaiJ . 1 979: Wiegersma et al . . 1 982) . This classification should be interpreted with caution. An antibiotic such as ampici l l in , severely affecting the anaerobic flora when given orally. may have only a slight effect when given parenterally. The spectrum , route of administration and pharmacokinetic properties of the antibiotic determine the influence on the indigenous flora . Parenteral antibiotics may affect the anaerobic flora if (i) the spectrum includes Gram-positive cocci and anaerobes and if ( i i ) it has a high bil iary excretion and if ( i i i ) it is not reabsorbed in the small intestines ( entero-hepatic cycle) and final ly if (iv) it is not inactivated by faecal contents (or B-lactamases) . It is necessary to design a standard human-model to test antibiotics on their effect on the indigenous flora . taking in to account the dosage . the mode and the duration of administration .
Which antibiotics may be used for selective flora suppression?
The choice of antibiotics is essential for the efficacy of selective flora suppression . Therefore, antimicrobial agents used for flora suppression in ICU patients should satisfy the following criteria: Nonabsorbable; (i) to achieve constant high intraluminal antibiotic levels, which are not gradually decreasing by absorption. This is particularly important to prevent selection of resistant strains; ( i i ) systemic effects of absorbed antibiotics are unnecessary and unwanted for most part of the treatment . Besides, if systemic antibiotics are indicated, the often poor absorption of oral antibiotics in ICU patients gives such unreliable plasma levels that additional parenteral administration is necessary. 'Small' spectrum; the antibiotic spectrum should cover all ICU-associated flora e .g . Enterobacteriaceae ( including Serratia spp . ) Pseudomonas and Acinetobac
ter spp. , but not the indigenous (anaerobic) flora . Bactericidal; the antibiotic should have low Minimal Bactericidal Concentrations for ICU-flora. I n the intestinal lumen no leukocytes are present to assist the action of antibiotics, therefore bacteriostatic antibiotics are of l ittle use . Minimal inactivation by food or faecal compounds and no inactivation by faecal B-lactamases. Van Saene et al . . ( I 985a) investigated the complex interaction between microorganisms, faeces and antibiotics, in-vitro. The Minimal Bactericidal Concentration (MBC) was determined for six different microorganisms (Pseudomonas aeruginosa , Acinetobacter calcoaceticus, Escherichia coli, Kleb
siel/a oxytoca , Proteus mirabilis, Enterobacter cloacae) in the presence of 0 (control) , 1 0, 20 and 30 per cent faeces. The results showed that many antibiotics were
98

largely inactivated in the presence of faeces , but that the MBC's for P. e1eruginos<1
and A . calcoaceticus generally increased much more than those of the other microorganisms. Apparently faeces has a variable 'protective effect' for different microorganisms. The results for polymyxin E, tobramycin and gentamicin are shown in figure I .
(frl �
-=-.,,,-----, .. "'� n ,.. . .... -'---�"'-----"' � :�;. . ! ·'
JI II •••
P .icr A c.1I E c011 K o•v E ck> Pm1r
P a c • A c a l E col1 K o•v E c10 P m11
Figure I :
POl Yt.tYXIU F
GENTAMICIN
Inactivation of antibiotic' by faece\.
P ,1cH A cat E coll K oxy E clo P m1r NEOMYCIN
P tc1 A cal E coll K oxy E clo P m1r TOBRAMYCIN
M inimal Bactericidal Conccntr.1t1on� ( MBC) of polymyxmc E. tobramycin . gcntamicin . and neomycin for six different Gram-negative bacil l i . in the pre�encc of 0, 10. 20 and 30% faece�. The M BC v.1lue' arc cxprc,�cd a� mg/I. in a non- l inear \cale. on top of the column' (van Sacnc ct a l . . 1 985) .
PTA-regimen
The selected antimicrobial agents used in this thesis were Polymyxin E, Tobramycin and Amphotericin B (PTA- regimen): Polymyxin E (Dumex. H ilversum , Holland) dosage 4x I 00 mg/day. Polymyxin E is nonabsorbable ; it has a small-spectrum of activity covering Pseudomonadaceae and Enterobacteriaceae except Proteus spp. (Sud and Feingold , 1 970), but it is not active against the indigenous flora (Hazen berg et a l . , 1 983) . The mode of action is disruption of the bacterial cel l wal l , making the cell permeable and causing cel l death (Nord and Hoeprich, 1 964) . This mechanism is independent of enzymatic systems. Acquired resistance against polymyxin E is very rare (Sogaard , 1 982) . Polymyxin E is inactivated to a great extent by proteins, food and faecal com-
99

pound� (Gotoff & Lepper, 1 965 ; van Saene et al . , I 985a) and should therefore be given in a large dose . Because of the gap in the spectrum (Proteus spp . ) and the in�ufficient activity in the pre�ence of faeces against Pseudomonas. Acinetobacter
and Serratia spp. , which are the most common ICU-associated potentially pa tho· genie microorganisms. it should be given in combination with an aminoglycoside .
Tobramycin (Eli Li l ly, Utrecht , Holland) . dosage 4x80 mg/day. Tobramycin is nonab�orbable . although in severe gastroenterifo ( mucositis) some ab�orption may take place (Rohrbaugh et a l . , 1 984) . Tobramycin in combination with polymyxin E has a synergistic action against Pseudomonas. Acinetobacter and Serrn
tia spp. Hazen berg et a l . ( 1 985) showed that tobramycin has a selective action on the aerobic Gram-negative microorganism� of the human faecal flora in- vitro. The selectivity was expressed as SD-factor, being the ratio of the antibiotic concentrations giving 50'Yo inhib1t1on of obligate anaerobic bacteria and of Enterobacteriaceae. The SD-factor for tobramycin varied between 1 3 .5 and 1 222 and for gentamicin between I. 94 and 1 5 . 5 (Hazen berg et al . . 1 985) . These finding� confirm animal experiment� showing that tobramycin had l ittle effect on the anaerobic flora (measured by the indirect parameters , 13-aspartylglycine and coecal weight) in doses that were still adequate to completely suppres� the endogenous Enterobacteriaceae (van der Waaij et al . , 1 982) . Another study, in volunteers. showed that the administration of tobramycin (300 mg/day orally) was effective in el iminating Enterobacteriaceae from the intestinal flora , without adverse effect� on the anaerobic flora (Mulder et a l . , 1 984) . Compared to the other aminoglycosides tobramycin is least inactivated by faecal compounds and food (figure I ) . Hazenberg et al . ( 1 985) showed that gentamicin and tobramycin are reversibly bound to the solid part of faeces and that more tobramycin is recoverable than gentamicin . These findings may explain the climcal experience that with oral gentamicin and/or polymyxin E, intestinal colon isation with sensitive strains occurred , in particular with Pseudomonas and Acinetobacter spp . (Klastersky et al . , 1 974; Bodey & Rosenbaum. 1 974) . Furthermore , intestinal colonisation by Pseudomonas or Acinetobacterspp . , is easily treated with the combination of polymyxin E and tobramycin , but not with polymyxm E- monotherapy. Amphotericin B (Squibb , Rijswijk , Holland) , dosage 4x500 mg/day. Amphotericin B is the most potent of antimycotic agents. It is added to prevent overgrowth by yeasts. Amphotericin B is nonabsorbable . but it is readily inactivated by faeces (Bodey, 1 969 ; van Saene et al . , 1 985a) and should therefore be given in a large dose.
Which antibiotic should be used for systemic prophylaxis?
The use of systemic antibiotics can be divided into prophylaxis and treatment.
J OO

However, this distinction is often not clear because many of the indications for 'prophylaxis' are in fact early treatment .
In Chapter 4 it is shown that a multiple trauma patient admitted to the ICU . should receive systemic antibiotic prophylaxis (or 'early treatment') to prevent pulmonary infections by 'community-flora· (e.g. Staphylococcus aureus, Strepto
coccus pneumoniae, Branhame/la catarrhalis, Haemophilus influenzae and E.
coli) . Most other surgical patients admitted to the ICU , receive �y�tcmic antibiotic prophylaxis during operation . In many surgical procedures a short perioperative prophylaxis is �hown to be effective in preventing postoperative wound infections (Nichols, 1 98 1 ; Gorbach , 1 982) . The spectrum of antibiotics used for perioperative prophylaxis often includes Staphylococcus and Streptococcus spp. , being the most frequent pathogens causing wound infections. This implies that these antibiotics are l ikely to disturb the indigenous flora and promote overgrowth by resistant organisms (Kager. 1 984) . When the postoperative course is uncomplicated this effect on the flora does not cause any harm. However, when per/postoperative surgical complications necessitate a prolonged stay in the ICU , then this systemic prophylaxis is not adequate to prevent infections of the respiratory or urinary tracts by hospital-acquired Enterobacteriaceae or Pseudomonadaceae . In this case an extended course of systemic antibiotic prophylaxis ( ± 4 days) should be given using a cephalosporin with l ittle effect on the indigenous flora. During the systemic prophylaxis, most potentially pathogenic microorganisms colonising the patient are el iminated by the topical antibiotics . For most indications for systemic prophylaxis, cefotaxime (Roussel Laboratories. Hoevelaken, Holland) is a suitable antibiotic. I ts spectrum covers both 'community flora' as well as 'hospital flora' (many Pseudomonas and Acinetobacter spp. excluded) and it has l ittle effect on the indigenous flora (Lambert-Zechovsky et al . , 1 980) ; it has a broad therapeutic range with few side effects. Other parenteral cephalosporins that are safe to the indigenous flora (e.g. cephradine, cefuroxime , ceftazidime , aztreonam) have either an incomplete cover of the Enterobacteriaceae (e .g . cephradine , cefuroxime) or of the Gram-positive cocci (e .g . ceftazidime, aztreonam).
What are the differences between the conventional infection prevention policy
and selective flora suppression?
The essential difference between the conventional infection prevention policy and the approach described in this thesis, is the concept of the pathogenesis of nosocomial infections in the ICU .
The conventional approach is based on the hypothesis ( i) that the difference in intrinsic pathogenicity of microorganisms is not important; ( i i ) that most infections are exogenous; many of the measures for infection prevention attempt to
1 0 1
avert the transmission of microorganisms between patients ( i .e . prevention of cross-infections) ; ( i i i ) that colonisation of the oropharynx and intestines by hospital- acquired microorganisms is harmless; besides. in most institutions no surve illance culture� of these �ites are done ; (iv) that colonisation of the respiratory and urinary tracts and wounds should not be treated with systemic antibiotics; (v) that antibiotic therapy is effective in established infections.
The novel approach described here , is based on the finding that ( i) the indigenou� flora (anaerobes. S. viridans, Streptococcus faecalis. S. epidermidis) has a much lower intrinsic pathogenicity than 'community-· or "hospital-acquired' microorganisms (Kurrie et al . . 1 98 1 ) ; (1i) that more than 80% of ICU-acquired infections are endogenous. Either potentially pathogenic microorganisms are present in the oropharyngeal or intestinal flora on admission ('primary endogenous') or ICU-acquired microorganisms have colonised the oropharynx or intestines after admission ('secondary endogenous') . The proliferation of 'exogenous' organisms in the oropharynx or intestines is essential in the pathogenesis of nosocomial infections; (iii) the recognition that colonisation of the oropharynx or intestines is the first step in the pathogenesis implies that intensive bacteriological monitoring of these sites is indispensable and that prevention of this stage is crucial ; (iv) colonisation of the respiratory and urinary tracts and wounds have to be treated before infection develops because (v) in intensive care patients, systemic antibiotic treatment in established infections has a low cure rate and a high mortality. Therefore it is essential to stop the sequence of events before it is too late .
Why has the conventional approach failed?
The conventional infection prevention measures have been very important for the elimination of inanimate sources of infections. Respiratory equipment , intravenous lines or urinary bladder drainage systems used to be important sources of infection in the early days of intensive care. However, when these sources were el iminated, the infection rate did not decrease. This is explained by the fact that the individual patient is heavily exposed to contamination from his environment , particularly from other colonised patients. Colonised patients carry h igh number� of potentially pathogenic microorganisms in oropharyngeal and intestinal flora and represent an important, continuous source of microorganisms in the ICU . As yet, the conventional isolation criteria did not take into account the oropharyngeal or intestinal flora as source of potentially pathogenic microorganisms. Secondly. measures to prevent transmission of microorganisms between patients may not be sufficiently effective to prevent transfer of very small amounts of bacteria . I n an intensive care patient with a severely decreased colonisation-defence , even a small number of bacteria may be sufficient to start colonisation of the oropharynx or intestines.
1 02
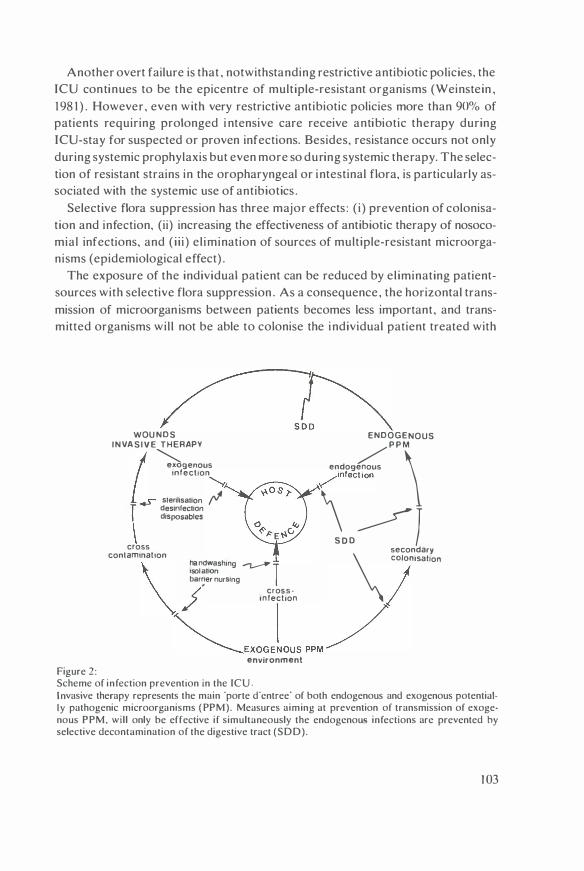
Another overt failure is that , notwithstanding restrictive antibiotic policies, the ICU continues to be the epicentre of multiple-resistant organisms (Weinstein , 1 98 1 ) . However, even with very restrictive antibiotic policies more than 90% of patients requiring prolonged i ntensive care receive antibiotic therapy during ICU-stay for suspected or proven infections. Besides, resistance occurs not only during systemic prophylaxis but even more so during systemic therapy. The selection of resistant strains in the oropharyngeal or intestinal flora, is particularly associated with the systemic use of antibiotics .
Selective flora suppression has three major effects : ( i) prevention of colonisation and infection, (ii) increasing the effectiveness of antibiotic therapy of nosocomial infections, and ( i i i ) el imination of sources of multiple-resistant microorganisms (epidemiological effect) .
The exposure of the individual patient can be reduced by eliminating patientsources with selective flora suppression . As a consequence, the horizontal transmission of microorganisms between patients becomes less important, and transmitted organisms wil l not be able to colonise the individual patient treated with
Figure 2:
s� WOU NDS INVA S I V E THERAPY
I �genous infection
"¥. ..,r stenllsat1on F
r des1nfec11on \ disposables
cross contamination
bar�er nursing
(' cros s -
ENDOGENOUS / P P M endogenous \ �infection
\.�l secondary \ ''''"�••oo \ ���
.':,�shmg �T
/ i n fection
�'>OG,lOUS OOM environment
Scheme of infection prevention an the ICU . Invasive therapy represents the main 'porte d'cntree· of both endogenous and exogenous potentially pathogenic microorganisms ( PPM). Measures aiming at prevention of transmission of exogenous PPM. will only be effective if simultaneously the endogcnou� infections arc prevented by selective decontamination of the digestive tract (SDD).
1 03

selective flora suppression. This explains the reduction in both endogenous and exogenous infections. This is schematically depicted in figure 2 . In contrast to the conventional antibiotic policy . emergence of resistance under selective flora suppression is largely prevented , because organisms, resistant to the antibiotics used for systemic prophylaxis or therapy , are eliminated by the topical nonabsorbable agents. Systemic antibiotic therapy is more effective in combination with selective flora suppression , because the source of infection i .e . the PPM in the oropharyngeal or intestinal flora is eliminated by the topical nonabsorbable antibiotics. This results in a h igher bacteriological and clinical cure rate and les� suprainfections. The epidemiological effect is a reduction of resistant strains in the ICU and prevention of outbreaks. This might offer an approach to control outbreaks with multiple-drug resistant microorganisms in hospitals . Each patient colonised with the particular microorganism in oral or intestinal flora. should be identified and treated with selective flora suppression , as we ll as all new patients, to prevent acquisition and colon isation .
However, selective flora suppression should not replace the conventional infection prevention measures. Many of the guidelines directed at the el imination of exogenous sources and prevention of transmission remain valuable or even become more effective, in combination with selective flora suppression (e .g. hand wash ing) . Isolation procedures and barrier nursing may be used now on more strict indications.
Conclusion
In the last decade anaesthesia and intensive care have made tremendous progress in l ife supporting techniques. As a consequence new frontiers have opened up for advanced medical care . However. infection control has not kept equal pace with these new developments so that much of the great efforts and costs that are successfully invested in the early phase of treatment are annihilated by infections occurring in a later phase of the i l lness . Although the here described technique for infection prevention awaits further confirmation , it may well prove to be a major step forward in intensive care . At present several clinical studies are being conducted or already completed in different centers and the results can be expected in the near future.
1 04

Summary
Chapter I, the introduction, reviews the current knowledge about infections in the critical care area, the generally accepted methods for infection prevention and the conventional antibiotic policy. The next part describes the different microorganisms involved in infections, with emphasis on the importance of preserving the indigenou!.. most anaerobic flora. In the discussion on host defence mechanisms, the role of a decreased colonisation defence of the oropharyngeal cavity and gastrointestinal tract in the pathogenesi!. of nosocomial infections. is stressed. Finally, a review is given of the h istory of flora suppression . the indications, the antimicrobials used and the effects .
The aim of this thesis was to gain a better insight in the pathogenesis of infections in intensive care patients. Secondly. to investigate whether endogenous infections could be prevented by selective decontamination with oral nonabsorbable antibiotics in intensive care patients without a functioning gastrointestinal tract. Thirdly. to determine the long term effect of selective decontamination on selection of resistant Enterobacteriaceae or Pseudomonadaceae in the ICU . Finally. to study the clinical effects of this regimen on morbidity and mortality .
Chapter 2, describes the colon isation and infection rate in a h istorical control group of 59 multiple trauma patients, who required mechanical venti lation and stayed five days or more in the ICU . No routine antibiotic prophylaxis was given in this group. After 1 5 days of ICU- stay, 86% of patients were colonised with one or more strains of potentially pathogenic microorganisms (PPM) in the oropharynx and in 77% of patients in the rectum. Colonisation of the respiratory and urinary tracts occurred in 69'Yo resp. 35 'X, of patient!.. Forty-eight patients (8 1 % ) developed 94 infections during ICU-stay, predominantly respiratory tract infections (59%) . urinary tract infections (32% ) . septicaemia (42%) and wound infections (25% ). Most infections were endogenous (95% ), except 30% of cases of septicaemia, that were apparently exogenous infections. A distinction was made between 'primary endogenous' and 'secondary endogenous' infections. The former are caused by PPM present in the admission flora whereas the latter are caused by newly acquired PPM colonising the oropharynx or intestines. The insight that 'exogenous' PPM. first multiply in the oropharynx or intestines and from there cause infection ( i . e . secondary endogenous infection ) , is essential for the prevention : primary endogenous infections will not be prevented by selective decontamination started in the ICU , and therefore systemic antibiotic prophylaxis should be given . In a prospective open tria l , the effect of selective decontamination of the digestive tract (SOD) and systemic cefotaxime prophylaxis was studied in 63 mechanically ventilated multiple trauma patients. In this group secondary colonisa-
1 05

tion of the oropharynx was completely prevented, while secondary colonisation of the intestinal tract occurred in 1 4% of patients. In 21 out of 24 patients the rectum was free of PPM after the first passage of stools (median 8 days) . The colonisation rate of the respiratory and urinary tracts were 9% and 7% respectively. Ten patients developed eleven infections: respiratory tract infections (8% ) , urinary tract infections (2% ) , septicaemia (3%) and wound infections (5% ) . No case of Gram-negative septicaemia was observed.
In Chapter 3, the conventional antibiotic policy in the control group is analysed . The assumption that emergence of resistance can be reduced by restricting the use of antibiotics. is tested. Therefore the use of systemic antibiotics in the control group was compared with the SOD- group. which was treated with systemic antibiotic prophylaxis and SOD. Although in the control group no routine systemic antibiotic prophylaxis was given. 51 patients (86%) received systemic antibiotics for suspected or proven infections, within the first week of stay in the ICU. The ineffect iveness of this policy is shown by the fact that (i) in the control group not only the amount of antibiotics administered, but also the number of different antibiotics exceeded that of the SOD-group; nevertheless, the infection rate was much higher than in the SOD-group (see chapter 2); (ii) in the control group 1 4 patients (24% ) developed 1 8 superinfections with often multiple resistant PPM. Five patients (8% ) died with infection . In the SOD-group only two patients (3%) developed a superinfection and no patient died ; ( i i i ) the preservation of the anaerobic flora in the SOD-group did apparently not give rise to more anaerobic infections, since in the control group anti-anaerobic drugs were given in 18 patients (3 1 % ) whereas in the SOD-group only 3 patients (5% ) received metronidazol .
The main objective of this antibiotic policy , to prevent induction of resistance , is not realized by a restrictive use of antibiotics. This is explained by the fact that emergence of resistance occurs predominantly during systemic antibiotic therapy, in the oral and intestinal flora, where high numbers of bacteria are present and low concentrations of antibiotics are reached.
Chapter 4, describes the pathogenesis and prevention of pulmonary infections. First an analysis is made of the type of infection in the control group. In 26 patients (44%) a pulmonary infection occurred before any systemic antibiotics were given . These infections developed very early, often within the first 48 h of treatment and were caused predominantly by Staphylococcus aureus, Streptococcus
pneumoniae and Haemophilus influenzae. I n 1 2 patients (20%) infection occurred after systemic antibiotics were given. These infections developed after a week and were invariably caused by Enterobacteriaceae or Pseudomonadaceae, which had first colonised the oral cavity or gastrointestinal tract . In the second part of this study three different regimens for prevention of pulmonary i nfection were
1 06

compared. Seventeen patients were treated only with intestinal decontamination. without oral decontamination and without systemic antibiotic prophylaxis. They had the same rate of pulmonary infection as the control group. The next group of 25 patients were treated with intestinal decontamination in combination with oral decontamination with Oraba!>c. but without cefotaxime . The rate of early pneumonia was unchanged, but secondary pulmonary infections disappeared. The third group was treated with oral and intestinal decontamination and in addition with sy!>temic ant ibiotic prophylaxis with cefotaxime . In this group both early and late infections were largely prevented.
By this �cries of �tudies we concluded that early infections can be prevented by systemic antibiotic prophylaxis and late Gram-negative infections by selective decontamination of the oral cavity and gastrointestinal tract .
Chapter 5 . describes the incidence of resistant Enterobacteriaceae and Pseudomonadaccac during 30 months of continuous use of selective decontamination . in 1 64 multiple trauma patients. The total number of cultures amounted 525 1 . Only 23 percent of all cultures yielded PPM and most of these PPM were isolated from the rectum. The study period was divided into five periods of approximately six months. No increase in the incidence of resistant strains was observed. Polymyxin E and tobramycin-resistance was rare : except Proteus spp . . no polymyxin E resistance was found and only four percent of Gram-negative strains were tobramycin resistant . Resistance against the combination of polymyxin E and tobramycin was found only once (Proteus morganii) . During this study 98 strains of cefotaxime-resistant Enterobacteriaccae or Pseudomonadaceae were found. The hypothesis that emergence of resistance against systemic antibiotics occurs primarily in the oral or gastrointest inal flora, was tested. Therefore, the origin of the resistant strains was analysed. We found that the admission flora was very sensit ive to cefotaxime (96% ) . In eight patients PPM became cefotaxime-resistant , before they were el iminated by the SOD. The majority of cefotaxime-resistant strains were found later. and were considered to be newly acquired in the ICU . In 29 out of 35 cases the site of isolation was the rectum. Therefore surveil lance cultures of the oral and i ntestinal flora are essential for the monitoring of emergence of resistance . Al though SOD does not completely prevent acquisition of cefotaxime-resistant PPM in the intestines, it prevents outgrowth and secondary colonisation, thereby preventing superinfection . We concluded that resistance against the antibiotics used for selective decontamination (polymyxin E and tobramycin) was rare , probably because ( i) the levels of these antibiotics in the lumen of the oropharynx and intestines are much h igher than the required minimal bactericidal concentration for most PPM, due to the dosage and low inactivation by faeces ; ( i i ) in contrast to cephalosporins, there are no inducible bacterial enzymes which mediate resistance against polymyxin E or tobramycin; ( i i i ) the use of a synergistic combination .
1 07

Chapter 6, describes the impact of an integrated trauma service on the late mortality following multiple trauma. The trauma treatment is based on aggressive resuscitation , prophylactic mechanical ventilation, early osteosynthesis and infection prevention with oral nonabsorbable antibiotics. In a 30-month period, 1 67 patients with an Injury Severity Score of 1 8 or more were treated according to these principles. Twenty-three patients ( 1 4 % ) died . The cause of death was craniocerebral trauma in 22 patients, which was mostly fatal within the first five days . No patient died of multiple organ failure , sepsis or ARDS. Many investigators found a close correlation between the Injury Severity Score and mortality, the second determinant of outcome being the age of the vict im. This relationship is explained by the occurrence of sepsis and the associated complications, which are responsible for more than 50% of the overall mortality. Because in this study the infectious complications and multiple organ failure were almost completely prevented , no correlation was found between the I njury Severity Score and mortality, or age and mortality.
Chapter 7 , describes the resul ts of treatment of pneumonia caused by Enterobacteriaceae or Pseudomonadaceae, with selective decontamination in combination with systemic antibiotic therapy and nebuhsed antibiotics. Nosocomial Gram-negative pneumonia has a notoriously h igh mortality (33%-70%) . The treatment with systemic antibiotics has a low cure rate and is associated with a high incidence of 'supercolonisation' and suprainfection. In a prospective open study in 25 patients with pneumonia caused by Enterobacteriaceae or Pseudomonadaceae, it was shown that by elimination of the endogenous PPM from the oral and intestinal flora with SOD, a h igh bacteriological and clinical cure rate was achieved, while superinfections were almost completely prevented. Three ( 1 2% ) of these seriously ill patients died from other causes than infection . This study shows that also in an already established infection , this antibiotic regimen is useful to increase the therapeutic effects of systemic antibiotics and to prevent superinfections.
Chapter 8, the general discussion, deals with new insights in 'colonisation resistance' and 'selective decontamination " . The concept of 'colonisation resistance' is based on the observation that the indigenous anaerobic flora is important for the defence against colonisation by exogenous PPM. Antibiotics were divided i nto 'safe' and 'unsafe' , according to their effect on the anaerobic flora and colonisation resistance. However, the anaerobic flora is just one of the factors constituting the colonisation defence. In the intensive care patient, the role of the anaerobic flora in the colonisation defence may be overestimated. This has implications for the choice of which antibiotics can be used for selective flora suppression . The effectiveness of oral antibiotics to eliminate PPM from the oral and intestinal flora, might be more important than potentially adverse effects on the indigenous an-
1 08

aerobic flora . The criteria, which an antibiotic should satisfy to be useful for selective flora suppression, include not only the effect on the anaerobic flora, but also the spectrum against ICU-associated PPM, the mode of action. absorption , and inactivation. An account is given of the choice of antibiotics used in this thesis. In the second part of this chapter, an analysis is made of the differences between the conventional infection prevention policy and the novel approach using prophylactic flora suppression, and the reasons why the conventional approach has failed. Selective flora suppression will augment the effect of some measures, used in the conventional policy. and makes other measures superfluous. However, selective flora suppression should not be considered as a substitute for the conventional methods, but rather as the missing l ink in infection prevention .
At present several clinical studies in different centers are being conducted and the results can be expected in the near future. If the results of the above described novel approach to infection prevention are confirmed by these studies. it may well prove to he a major step forward in intensive care .
1 09


Samenvatting
Hoofdstuk I , de inleiding, geeft een overzicht van de huidige kennis van infecties in intensive care . I nfectie is nog steeds de belangrijkste doodsoorzaak in de intensive care . Het falen van de huidige methoden voor infectie- preventie en van het conventionele antibiotica-beleid , wordt op krit ische wijze geanalyseerd. Vervolgens worden de versch il lende micro-organismen die een rot spelen bij infecties en de afweermechanismen van de gastheer besproken . Centraal in het ontstaan van ziekenhuis-infecties staat de snelle verandering van de microflora van de patient, als gevolg van de verminderde kolonisatie-afweer van de mondkeelholte en het maag-darmkanaal . Reeds tang heeft men getracht infecties te voorkomen door de flora te onderdrukken met antibiot ika. Er wordt een kort overzicht gegeven van de geschiedenis van flora-onderdrukking, de indikaties, de daarvoor gebruikte antibiotika en de effecten hiervan .
Het doe I van dit proefschrift was: ( i) een beter inzicht te krijgen in de ontstaanswijze van infecties in intensive care-patienten ; ( i i ) te onderzoeken of infecties voorkomen kunnen worden door selectieve darm-decontaminatie (SOD) met orate niet-resorbeerbare antibiotica in intensive care- patienten met een nietfunctionerend maag-darmkanaal ; (ii i) te bepalen of SOD op de lange-termijn zou leiden tot selectie van resistente micro-organismen.
Hoofdstuk 2 beschrij ft de kolonisatie en infectiepercentages in een groep van 59 beademde polytrauma patienten , die vijf dagen of (anger in de intensive care unit (ICU) behandeld werden. De patienten kregen geen antibiotische prophylaxe (controle groep) . Na een verblijf van 1 5 dagen op de intensive care was 86% van de patienten gekoloniseerd in de mond-keelholte met een of meer Gram-negatieve bacterien en 77% werd gekoloniseerd in het rectum met n ieuwe stammen Enterobacteriaceae of Pseudomonadaceae. Achtenveertig patienten (8 1 % ) ontwikkelden 94 infecties gedurende hun verbl ij f op de ICU , met name luchtweginfecties (59%) , urineweginfecties (32% ) , bloedbaaninfecties (42%) en wondinfecties (25% ) . De meeste infecties werden veroorzaakt door bacterien µit de mond- of darmflora ( =endogeen) (95% ) , met uitzondering van 30% van de bloedbaaninfecties, die duidelij k een u itwendige bacteriele oorsprong hadden ( =exogeen). Een tweede groep van 63 polytrauma-patienten , werden behandeld met selectieve decontaminatie van de mondholte en het maag-darmkanaal met orate , niet resorbeerbare antibiotica (polymyxine E, tobramycine , amphotericine B) en met cefotaxime-prophylaxe in de bloedbaan . In deze groep kon secundaire kolonisatie van de mondholte volledig voorkomen warden ; secundaire
I I I

kolonisatie van de darmen trad op bij 14 % van de patienten. Bij 2 1 van de 24 patienten was de darm vrij van potentiele ziektekiemen, na de eerste defaecatie (mediaan 8 dagen) . Tien patienten ontwikkelden elf infecties: luchtweginfecties (8% ) , urineweginfecties ( 2 % ) , e n wondinfecties (5% ) . Gram- negatieve bloedbaaninfecties kwamen niet voor in deze groep.
In hoofdstuk 3 wordt het conventionele antibiotica-beleid geanalyseerd . De veronderste l l ing, dat het ontstaan van resistentie verminderd kan worden door een restrictief antibiotica-beleid, werd getoetst. Hiertoe werd het gebruik van systemische antibiotica in de beide groepen vergeleken . Hoewel in de controlegroep een restrictief antibiotica- beleid werd gevoerd , werd reeds in de eerste week van hun IC-verblijf aan 5 1 patienten (86% ) systemische antibiotica toegediend, in verband met bewezen of vermoede infecties. De inefficientie van dit beleid blij kt hieruit, dat ( i) in de controle groep de hoeveelheid toegediende systemische antibiotica groter was dan in de SDD-groep, zowel wat betreft de totale hoeveelheid als ook het aantal verschi l lende antibiot ika: ( i i ) desondanks, het infectie- percentage veel hoger was dan in de SDD-groep: (iii) dit gepaard ging met een groot aantal superinfecties (24%) met vaak zeer resistente Gram-negatieve bacterien (bv Pseudomonas aeruginosa . Acinetobacter en Serratia spp . ) . Mede ten gevolge hiervan stierven vijf patienten (8% ) . De voornaamste doelstell ing van het antibiotica- beleid, n l . het voorkomen van resistentie . werd dus niet bereikt met een restrictief antibiotica-beleid .
Hoofdstuk 4 beschrijft de ontstaanswijze en de preventie van luchtweginfecties. Ten eerste werd een analyse gemaakt van de luchtweginfekties in de controlegroep. Zesentwintig patienten (44%) kregen een longontsteking, voordat een antibioticum gegeven was. Deze infecties ontwikkelden zich zeer snel , meestal binnen de eerste 48 uur van de behandeling, en werden hoofdzakelij k veroorzaakt door Staphylococcus aureus, Streptococcus pneumoniae, en Haemophi/us
influenzae, welke deel uitmaken van de 'normale' flora. Twaalf patienten (20%) kregen een longontsteking nadat systemische antibiotica gegeven waren . Deze infecties ontwikkelden zich meestal pas na een week , en werden vrijwel altijd veroorzaakt door Enterobacteriaceae en Pseudomonadaceae, die eerst de mondholte of maag-darmkanaal gekoloniseerd hadden .
I n h e t tweede dee) van de studie werden drie verschillende regimes voor de preventie van luchtweginfecties onderzocht . Zeventien patienten werden a Ileen met selectieve decontaminatie van het maag-darmkanaal behandeld (niet van de mondholte en geen prophylaxe met systemische antibiotica) . Zij hadden hetzelfde infectie-percentage als de controle-groep. Een tweede groep van 25 patienten werd behandeld met selectieve decontaminatie van zowel het maag- darmkanaal als de mondholte ; deze groep kreeg echter geen cefotaxime. Het percentage vroege longontstekingen bleef onveranderd, maar de secundaire luchtweginfec-
1 1 2
ties verdwenen. Een derde groep kreeg zowel selectieve decontaminatie van de darm en mondholte , als ook systemische prophylaxe met cefotaxime. In deze groep konden zowel de vroege als de late infecties grotendeels voorkomen worden.
De conclusie is dat primaire infecties voorkomen kunnen worden door systemische antibiotische prophylaxe , dat secundaire Gram-negatieve infecties voorkomen kunnen warden door SOD en dat de selectieve decontaminatie van de mondholte van zeer groat belang is in de beademde patient.
Hoofdstuk 5 beschrij ft het optreden van resistentie gedurende 30 maanden continu gebruik van SOD, in 1 64 polytrauma patienten . In het totaal werden 525 1 kweken afgenomen . Slechts uit 23% van de kweken konden ziektekiemen geisoleerd warden. Om een eventuele geleidelijke toename van resistentie te kunnen ontdekken we rd de studieperiode verdeeld in 5 perioden van 6 maanden. Er we rd geen aanwijzing gevonden voor toename van het aantal resistente stammen. Polymyxin E- en tobramycine-resistentie was zeer zeldzaam: behalve Proteus spp. werd geen polymyxin E- resistentie gevonden en slechts vier procent van de Gram-negatieve stammen was tobramycine-resistent . Gedurende deze 30 maanden werden 98 cefotaxime-resistente Enterobacteriaceae en Pseudomonadaceae stammen gelsoleerd . De hypothese , dat resistentie tegen systemische antibiotica voornamelij k ontstaat in de orale en intestinale flora, werd getest door de oorsprong van de resistente stammen na te gaan. Het grootste deel van de cefotaxime-resistente stammen werd pas na een aantal dagen gevonden en werd beschouwd als nieuw verkregen stammen . In 29 van de 35 gevallen werd deze stam uit het rectum gei·soleerd . De belangrij kste bevinding was echter dat het overgrote dee I van de resistente stammen verdween onder invloed van de SOD, en daardoor niet in staat was het maag-darmkanaal of enig andere plek te koloniseren .
Hoofdstuk 6 beschrijft de invloed van een gei'ntegreerde trauma-behandeling op de sterfte en de doodsoorzaken van polytrauma-patienten . Het behandelingsschema is gebaseerd op een agressieve behandeling van stoornissen van de vi tale functies, prophylactische beademing, vroege osteosynthese en infectie preventie met SOD. Gedurende een periode van 30 maanden werden 1 67 trauma patienten met een ' Inj ury Severity Score 1 ' van 18 of meer, volgens deze principes behandeld . Orie en twintig patienten ( 14% ) overleden . De belangrijkste doodsoorzaak was het schedel-hersenletse l , dat vaak al binnen vijf dagen fataal verliep. Geen patient stierf ten gevolge van sepsis, 'multiple organ failure2' , of ARDS3, onafhankelij k van de I nju ry Severity Score . Deze resultaten zijn aanzienl ijk gunstiger dan in andere studies. Vele onderzoekers vonden een l ineair verband tussen de I nj ury Severity Score en de sterfte , terwijl ook de leeftijd van grote invloed op de sterfte bleek te zijn . Dit verband wordt vrijwel volledig verklaard door het optreden van i nfectieuze complicaties en het hiermee verband houdende ARDS en
1 1 3

'multiple organ-failure ' , vooral bij de oudere patient, we Ike verantwoordelij k zij n voor meer dan de he I ft van de tot ale sterfte . In deze studie kon . doordat de late infectieuze compl icaties voorkomen werden, geen verband meer gevonden warden tussen de Injury Severity Score of leeftijd en de sterfte.
Hoofdstuk 7 beschrij ft de resultaten van de behandeling van longontsteking bij beademde patienten . Longontsteking met in het ziekenhuis verkregen ziektek iemen heeft een berucht hoge mortal iteit ; de behandeling met systemische anti biotica heeft een laag genezings-percentage en gaat gepaard met een zeer frekwent optreden van superinfectie. Vijfentwintig ernstig zieke , beademde patienten met een longontsteking veroorzaakt door Enterobacteriaceae of Pseudomonadaceae. werden behandeld met SOD. systemische antibiotica en een aerosol met ant ibiotica . Door het elimineren van de ziektekiemen uit de kee l- en darmflora met behulp van SOD. was het mogelij k een hoog bacteriologisch en kl inisch genezings-percentage te bereiken, terwij l superinfectie vrijwel volledig voorkomen kon warden. Orie ( 1 2%) van deze ernstig z1eke patienten stierven ten gevolge van andere oorzaken dan infectie. Deze studie toont aan dat. ook bij een reeds bestaande infectie , dit antibiotische regime van grote waarde is om het therapeutisch effect van de behandeling met system1sche antibiotica te vergroten en het ontstaan van resistentie en superinfecties te voorkomen .
Hoofdstuk 8, de algemene discussie , bespreekt nieuwe inzichten in 'colonisatie resistentie' en 'selectieve darm- decontaminatie ·. Het concept 'coloni�atie resistentie' is gebaseerd op de waarneming. dat de lichaamseigen anaerobe flora van groot belang is voor de afweer tegen kolonisatie met vreemde bakterien Op basis van hun invloed op de anaerobe flora, zij n de antibiotica ingedeeld in 'veilige' en 'niet-veilige' middelen . De anaerobe flora is echter maar een van de factoren die de kolonisatie-afweer bepalen . Bij de intensive care patient speelt de anaerobe flora misschien niet zo'n grote rol in de kolonisatie-afweer als aanvankelijk werd aangenomen. Dit heeft implicaties voor de keuze van de antibiotica die men voor selectieve flora-onderdrukking kan gebruiken. De effect1viteit van de orale antibiotica in het elimineren van potentiele ziektek1emen uit de mond- en darmflora is waarschij nl i jk belangrijker dan eventuele bijwerkingen op de anaerobe flora. De eisen waaraan een antibioticum moet voldoen om gebruikt te kunnen warden voor selectieve flora-onderdrukking, zij n niet al leen het effect op de anaerobe flora , maar oak het spectrum . het werkingsmechanisme . de resorptie , en de inactivatie. De keuze van antibiotica , die in dit onderzoek gebruikt zij n , wordt verantwoord . Het tweede deel van dit hoofdstuk geeft een beschouwing van de voornaamste verschillen tussen het conventionele infectiepreventie-beleid en de nieuwe benadering door middel van selectieve flora-onderdrukking, en de oorzaken voor het falen van het conventionele beleid . Selectieve flora onderdrukking kan het effect van sommige maatregelen, we Ike gebru1kelij k zijn in het conventionele
I 1 4

beleid, versterken en maakt andere maatregelen overbodig. Selectieve flora onderdrukking moet echter niet beschouwd warden als een vervanging van de bestaandc infcctic- prcventie methoden , maar eerder als een nog ontbrekende schakel in de infectie preventie .
Op het ogenblik zij n diverse kl inische studies met deze methode gaande in verschil lende centra en de resultaten h iervan mogen in de nabije toekomst verwacht worden . Indien, zoals het zich laat aanzien, de rcsultaten van de hier beschreven methode voor infectie-preventie bevestigd warden , zou dit een grote stap voorwaarts in intensive care kunnen zij n .
' I njury Severity Score = een 'core voor d e ernst van het letsel. Aan zes orgaansystemen worden punten toegd.end, varierend van 0 (geen letsel) tot 5 ( levensbedreigend letse l ) . De drie hoog;te waarden worden gd.wadrateerd en opgeteld. De maximale score is dus 75 .
' Multiple organ failure = het gelijktijdig falen van diverse orgaansystemen. met name longen. meren en lever.
' A RDS = Adult re,piratory di,tre'� ;yndrome ; ecn aspccifid. longheeld. dat gekenmcrkt wordt door het optreden v,111 longoedeem . hogc beademing;drukken en een 'lechtc ga,wi"eling.
1 1 5


References Alberti KG M M . Batstone GF. Foster KJ . Johnston DG ( 1 980) Relative role of various hormones
in medi<1ting the metabolic response to injury. J Parenter Enter Nutr 4: 1 4 1 Alford WC. Meador C K . Mihalcvich J . Burrus G R . Glassford O M . Stoney WS. Thomas CS ( 1 979)
Acute adrenal in�ufficicncy following cardiac surgical procedures. J Thorne Cardiovasc Surg 78:489
Allgtiwcr M. Diirig M. Wolff G ( 1 980) Infection and trauma. Surg Clin North Am 60: 133 Altemeicr WA. MacMillan BG . Hil l EO ( 1 962) The rationale of specific antibiotic therapy in the
management of major burn�. Surgery 52:240 Altcmeicr WA. Culbcrhon WR. Hummel RP ( 1 968) Surgical con�ideration� of endogcnou� infec
tion; 'ourcc,. type� a nd method' of control. Surg Cl in North Am 48:227 Aly R. Maib.icb H I . Rahm.in R. Shincfield HR. Mandel AD ( 1 975) Correl.1t1on of human in vivo
and in vitro cutaneous antimicrobial factors. J Infect Dis 1 3 1 :579 AMA. Committee on Medical Aspects of Automotive Safety ( 1 97 1 ) Rating the severity of tissue
damage. I the abbreviated scale. JAMA 2 1 5 :277 American College of Surgeons ( 1 980) Hmpital Trauma I ndex. Bull Am Coll Surg 65: 32 Ammundsen E ( 1 980) post-traumatic pulmonary in�ufficicncy I n : Lewb DH (ed�) Symposium on
post traumatic lung insufficiency: etiology. pathophy�iology and treatment. Acta Chir Scand (suppl) 499:3
Andrews CP. Coalson J J . Smith J D . Jolwn,on WG ( 1 98 1 ) Dtagno'i' of nmocomial bacterial pneumonia in acute. diffuse lung injury. Che;t 80:254
An nest SJ . Scovill WA. Blumenstock FA . Stratton H I-I . Newell JC. Palo,i.. 1 ct al. ( 1 980) I ncreased creatinine clearance following cryoprecip1tate infu;ion in trauma and �urgical patients with decreased renal function. J Trauma 20:726
Atherton ST. White DJ ( 1978) Stomach a' �ourcc of bacteria coloni�ing re,piratory tract during artificial ventilation. Lancet i i :968
Baker CC. Oppenheimer L. Stephan� B . Lewb FR. Trunkey DD ( 1 980) Epidemiology of trauma deaths. Am J Surg 1 40: 144
Baker CC. Degutis LC. DeSantis J Baue AE ( 1 985) I mpact of a trauma �ervice on trauma care in a university hospital . Am J Surg 149:453
Baker SP. O'Neill B. Haddon W. Long WB ( 1 974) The I njury �cvcrity ;core: a method for describing patients with multiple injuries and evaluating emergency care. J Trauma 14 : 1 87
Baltch AL. Hammer MC. Smith RP. Bishop M B . Sutphen NT. Egy MA et a l . ( 1 986) Comparbon of the effect of three adrenal corticosteroids on human granulocyte function again�! pseudomonas acruginosa. J Trauma 26:525
Bauer AW. Kirby WMM . Sherris JC. Turck M ( 1 966). Antibiotic suscept ibility testing by a �tandardized single disk method. American Journal of Clinical Pathology. 45:493
Bell RC. Coalson JJ . Smith J D . Johanson WG j r ( 1 983) Multiple organ fa ilure and infection in adult respiratory distress syndrome. Ann I ntern Med 99:293
Berger R. Arango L ( 1 985) Etiologic diagnosis of bacterial nosocomial pneumonia in senou,ly i l l patients. Crit Care Med 13 :833
Bick RL. Dukes ML, Wilson WL. Fekete LF ( 1 977) Antithrombin I l l ( AT- I I I ) as a diagno,tic aid in disseminated intra vascular coagulation. Thromb Res 10 :72 1
Bodey G P ( 1 969) The effect o f amphotericin B on the fungal flora i n feces. Clin Pharmacol Ther 1 0:675
Bodey GP. Rosenbaum B ( 1 974) Effect of prophylactic measures on the microbial flora on patient> in protected environment units. Medicine (Baltimore) 53:209
Bodey GP. Rodriguez V ( 1 976) Protected environment- prophylactic antibiotic programs; microbiological studies. Cl in Haematol 5 :395
Borderon IC. Laugics I . Gold F, Viarme F ( 1 983) Effect of cefotaxime therapy on fecal flora in children (Abstract) Proceedings of the 1 3th In ternational Congrc�s Chemotherapy Vienna. 4.21 1 0-2
Bradley J A . Ledingham Mc A I. Hami lton DNI-1 ( 1 98 1 ) Assessment of host resistance of critically ill surgical patients by the response to recall ,kin antigen>. I nten�ive Care Med 7: !05
1 1 7
Braun SR. Levin AB. Clark KL ( 1 986) Role of corticosteroids in the development of pneumonia i n mechanically ventilated head-tr.iuma victims. Crit Care Med 14 : 1 98
Brown R B . Hosmer D . Chen HC. Te res D . Sand� M. Bradley S et a l . ( 1 985) A comparison of infec· tion; in different ICU; within the same ho�pital . Crit Care Med 13A72
Browne M K . Leslie G B . Pf1rrmann RW ( 1 976) Taurol in . a new chemotherapeutic agent . J Appl Bactcriol 41 :363
Brun Bui��on C. Meakin� JL ( 1 983) Ho't defcn�e mechanbm; in the acutely ill patient. l n : McA Ledingham I. Hanning CD (ed') Recent Advance' in critical care medicine. Churchill Livingstone. Edinburgh. p97
Bry,in CS . Reynold' KL Y ( 1 984) B.icteremic nmocomial pneumonia. Analys" of 1 72 epi,ode' from a 'ingle metropolitan area. Am Rev Resp1r Dis 1 29:668
Buck AC. Cooke EM ( I 969) The fate of inge�ted p,eudomona' acrugino,a. J Med Microbial 2:52 1 Bue l ier HR. Bolwcrk C. ten Cate J . Roo, J . Kahle LH. ten Cate JW ( 1 982) Postoperative hemo�ta-
t1c profile in relation to Gram-negative 'epticemia Crit Care Med 1 0 : 3 1 1 Bull J P ( 1 975) Measure; of 'everity of injury. Injury 9: 1 84 Bull JP ( 1 982) Injury 'everity 'coring 'ystems. I njury 14 :2 Burrowe� CE. Habal FM . Mova! HZ ( 1 975) The inhibition of human plasma kallikrein by anti
thrombin 1 1 1 . Thromb Re' 7 : 1 75 Caplan ES. Hoyt N . Cowley RA ( 1 979) Changing patterns of nosocomial infections in severely
traumatized patient,. Am Surg 45:204 Caplan ES. Hoyt N ( 1 98 1 ) I nfection ;urve1 l lance and control in the severely traumatized patient .
Am J Med 70:638 Casewell M. Phil lips I ( 1 978) Epidemiological pattern' of klebsiella colonisation and infection in an
intensive care ward. J Hyg ( Lond) 80:295 Castle MRN. Tenney J H . Wein�tein MP. Eickhoff TC ( 1 978) Outbreak of a multiple resistant
acinetobacter in a 'urg1cal l n ten,ive care unit: epidemiology and control . Heart Lung 7:641 CDC ( 1 985) Guideline' for 'urveil lance and control of nosocomial infections US Department of
Health and Human 'ervice,. Public Health Service. Center' for Di,eae'e Control , Atlanta . Georgia , p l
Cohn I . Longacre A B ( 1 959) Kanamycin for inte,tinal anti,eps1>. Surg Gynccol Ob�tet 108: 100 Comhaire A. Limy M ( 1 98 1 ) Contamination rate of sterilized ventilator in an ICU. Crit Care Med
9:546 Cross AS. Roup B ( I 98 1 ) Role of re;piratory assistance device; in endemic nosocomial pneu
monia. Am J Med 70:681 Crouch TW. H iguchi J H . Coalson JJ. Johan;on WG ( 1 984) Pathogenesis and prevention of noso
comial pneumonia in a nonhuman primate model of acute respiratory failure. Am Rev Respir Dis 1 30:502
Dack G M . Pet ran E ( 1 914) Bacterial activity in different levels of the intest ine. J Infect Dis 54:204 Daschner FD ( 1 978) Ant ibiotika prophylaxis in der l ntensivmedizin Helv Chir Acta 45 :475 Da,chni:r FD. Frey P. Wolff G. Baumann PC. Suter P ( 1 982) No,ocomial infections in inten,ive
care '' ard': a mult icenter pro,pective 'tudy. l nten>ive Care Med 8:5 Daschner FD ( 1 985) Nosocomial infections in intensive care units . I ntensive Care Med 1 1 :284 Dixon JMS ( 1 960) The fate of bacteria in the small intestine. J Pathol Bae! 70: 1 3 1 Dominguez de Villata E . Algora A. Rubio J J . Roig M . Mosquera J M , Galdos P et a l . ( 1 983)
Septicaemia in a medical I ntensive Care Unit. Clinical. biochemical and microbiological data of 109 cases. I ntensive Care Med 9: 1 09
Donowitz LG . Wenzel RP. Hoyt JW ( 1 982) High mk of hosp1tal-..1cquired infection in the ICU patient . Crit Care Med !0:355
Du Moulin GC. Hedley-Whyte J . Paterson DG. L1�bon A ( 1 982) Aspiration of gastric bactena in antacid-treated patients: a frequent cause of post-operative colonisation of the airway. Lancet i i :227
Dunham CM, La Monica C ( 1 984) Prolonged tracheal intubation in the trauma patient . J Trauma 24: 1 20
Egan EA. Manti l la G. Nelson EM. Eitzman DV ( 1 976) A prospective controlled trial of oral kanamycin in the prevention of neonatal necrotizing enterocolitis. J Pediatr 89:467
1 1 8

Eickhoff TC. Brachmann PS. Bennet JV. Brown J F ( 1 969) Surveil lance of nosocomial info.:ctions in community hospitals. I . Surveillance methods. effectiveness and initial results. J Infect Dis 1 20:305
Espcrsen F. Gahrielsen J ( 1 98 1 ) Pneumonia due to staphylococcus au re us during mechanical ventilation. J I nfect Dis 1 44 : 1 9
Feeley TW, du Moulin G C , Hedley-Whyte J . Bushnell LS. Gi lhert JP. Feingold D S ( 1 975) Aerosol polymyxin and pneumonia in seriously ill pats. N Engl J Med 293:47 1
Figueras-Felip J . Ba,ilio-Bonet E. Lara-Eisman F. Caride- Garcia P. l samat-Baro E. Fava-Bargallo P ( 1 984) Oral b 'uperior to 'Y'temic antibiotic prophylaxis in operations upon the colon and rectum. Surg Gynecol Oh,tet 1 58:359
Finegold SM ( 1 977) Anaerobic bacteria in human disease. Academic press. New York. Florey M E , Rm' RWNL. Turtan EC ( 1 947) Infection of wounds with gram-negative organi'm�.
Clinical manife,tation' and treatment. Lancet i :855 Franco JA, Eitzman DY. Baer D ( 1 973) Ant ihiotic u'age and microhial re,l'tance in an intensive
care nur,ery. Am J D is Child 1 26:3 1 8 Freeman J . McGowan J E ( 1 978) Ri'k factor' for nmocomi,il infection. J Infect Di' 1 38 :8 1 1 Freeman J . Rosher BA, Mcgowan J E ( 1 979) Adverse effcch of nosocomial m fection. J I n fect Dis
1 40:732 French GL. Homi J ( 1 979) l n,ignificancc of colonic bacteria in the 'Pulum of patient' 111 a new ICU.
Crit Care Med 7:487 Fry D E , Pearlstein L, Fulton RL. Polk HC ( 1 980) Multiple system organ failure (the role of uncon
trolled infection) . Arch Surg 1 1 5 : 136 Gann DS, Lilly MP ( 1 983) The neuroendocrine response to multiple trauma. World J Surg 7: 1 0 I Garlock J H , Seley GP ( 1 939) Use of sulfanilamidc in surgery of the colon and rectum. Preliminary
report. Surgery 5 :787 Gaya H ( 1 976) Infection control in intensive care. Br J Anaesth 48:9 Gerritsen SM, Loenhout van T, Gimbrere JSF ( 1 982) Prognostic sign' and mortality in mult iply in
jured patients. I nj ury 14 :89 Glinz W , Grob PJ , Nydegger U E . Rickhn T. Stamm F. Stoffel D . La,ance A ( 1 985) Polyvalent
immunoglohulin' for prophylaxi' of haeterial infections 111 patients follow mg multiple trauma. In tensive Care Med 1 1 :288
Goldstein FW. Gutmann L. Williamson R, Collatz E, Acar JF ( 1 983) In vitro and in vivo emergence ofsirnultaneou' re'i'tance to both 13-lactarn and arninoglycoside antibiot ics in a strain ofSerratia rnarce,cen,. Ann Microhiol 1 34A:329
Gorbach SL ( 1 982) Prophylactic antibiotics. I ndications in surgical patients. Scand J I n fect Dis 36: 1 34
Goris RJA , Draaisrna J ( 1 982) Causes of death after blunt trauma. J Trauma 22: 1 4 1 Gori' R , Girnbrere J . van N1ekerk J . Sc hoots FJ. Booy L H D ( 1 982) Early osteosynthesis and pro
phylactic mechanical ventilation in the multiple trauma patient. J Trauma 22:895 Goto ff SP. Lepper M H ( 1 965) Treatment of Salmonella carriers with colistin sulphate. Arn J Med
Sci 63:399 Green G M , Jakob GJ . Low RB . Davis GS ( 1 977) Defence mechanisms of the respiratory mem
brane. Arn Rev Re,pir Dis 1 1 5 :475 Greenfield S . Tere' D, Bushnell LS. Hedley-Whyte J. Feingold DS ( 1 973) Prevention of grarn
negative bacillary pneumonia using aerosol polyrnyxin as prophylaxis I. the effect on the colonization pattern of the upper respiratory tract of seriously ill patients. J Clin I nvest 52:2935
Greenspan L, Mclellan A , Greig H ( 1 985) Abbreviated I nj ury Scale and I njury Severity Score: A scoring Chart. J Trauma 25:60
Gross PA. Neu HC. Aswapokee P. van Antwerpen C, Aswapokee N ( 1 980) Death from nosocornial infections: experience in a university hospital and a community hospital . Arn J Med 68: 2 1 9
Grylack LJ , Scanlon JW ( 1 978) Oral gentarnicin therapy i n the prevention o f neonatal necrotizing enterocolitis. Arn J Dis Child 1 32: 1 1 92
Guggenbichler JP, Kofler J ( 1984) Influence of third- generation cephalosporins on aerobic intestinal flora. J Antirnicrob Chernother 14 Suppl B :67
Guiot HFL, van Furth R ( 1 977) Partial antibiotic decontamination. Br Med J I :798
1 1 9

GulOt HFC. van der Meer JWM. van Furth R ( 198 1 ) Selective antimicrotiial modulation of human microtiial flora: infection prevention i n pat ient\ with <lecrea-.e<l ho-.t dekn-.e mechani'm' tiy selective el imination of potentially pathogenic tiacteria. 1 Infect D1-. I ·H 644
Gu\tafsson BE ( 1 982) The phriological importance of the colonic m1croflora . Scand J Gastroenterol 77: 1 1 7
Hahn DM. Schimpff SC. Fortner CL. Smyth AC. Young VM. W1crn1 J.. PH ( 1 978) I n fection in acut" lcuJ..cmia patient\ n:ce1vmg oral nonati,orti.ible .mt1ti1ot1cs Ant1m1crob Agent\ Chemoth 1 3 :958
Haley RW. Schaberg DR. van Allmen SD ( 1 980) fat1matmg extra charge' and prolongJtion of hospitalization due to nosocomial infections a compari-.on of metho<l-.. J l n fcct Dis 1 4 1 :248
Haley RW. Schaberg D R . Crossley KB ( 1 98 1 ) Extra charges and prolongation of -.tJy attributable to nosocomial infections: a perspective m our ho-.p1tal comp.1ri-.on Am J Med 70: 5 1
Haley R W. Bregman D A ( 1 982) The role o f understaffing and overcrowding in recurrent outbreak� of staphylococrnl infection in .1 neonatal -.peci•il-can: unit. 1 In fect Di-. 14� ·875
Hazenberg MP. Boom van de M . Bakker M . Merwc van der JP ( 1 983) Effect of antibiotics on the human inte�tinal flora in mice. Antonie V,m Leeuwenhoek 49:97
Hazenberg MP. Pennock-Schroder AM . Merwe van der JP ( 1 985) Binding to and antibacterial effect of aztreonam. temoc1 l l in . gcntamicin and tobramycin on hum.in faece-. . J Hyg Camb 95 :255
Hemming VG. Overall JC j r. Britt MR ( 1 976) Nmocomial infection' in .t newborn intensive care uni t . Results of 4 1 months of surveillance. N Engl 1 Med 294: 1 3 1 0
Hentges DJ . Stein AJ . Casey SW. Que JU ( 1 985) Protective role of inh:stmal flora against infection with Pseudomonas aeruginosa in mice: influence of ant1b101lcs on colonization resistance. Infect l mmun 47: 1 1 8
Hil lman K M , Riordan T. O'Farrcll SM. Tabaqchali S ( 1 982) Colornzallon of the gaMric content> in critically i l l patient� . Cnt Care Med I 0:444
H ilton E. Ulin A . Samueb S. Adams AA. Lc,scr ML. Lowy FD ( 1 983) Nosocomial bacterial eye infections in mtensiv.:- care unit-. Lmcet i: 1 3 1 8
Hirschmann JV. Everett E D ( 1 979) Haemophilus influenzac infectmns in adults: Report o f nine case-. and a review of the literature Medicine 58: 80
H irschmann JV. lnui I S ( 1 980) Antimicrobial prnphylJxis. a critique of recent trials. Rev I n fect Dis 2 : 1
Horst H M . Obeid FN . Sorensen VJ . Bivins BA ( 1 986) Factor' influencing survival of elderly trduma patients. Crit Care Med 14:681
Hubay CA. Weckesser EC. Levy RP ( 1 975) Occult adrenal insufficiency in 'urgical patients. Ann Surg 181 : 325
Hughes WT. Kuhn S. ChaudhJry S. Feldman S. Verzosa M . Aur RJA. Pratt C. George SL ( 1 977) Successful chcmoprophylaxis for pneumocystis carinii pneumonitis . N Engl J Med 297: 1 4 1 9
Jarret F. Balish E . Moylan J A . Ellerbe S ( 1 978) Clinical experience with prophylactic antibiotic bowel suppre"1on in burn patients. Surgery 83:523
Johanson WG . Pierce AK. Sanford JP ( 1 969) Changing bacterial pharyngeal flora of hospitalized patients. Emergence of gram-negative bacil l i . N Engl 1 Med 28 1 : 1 1 38
Johanson WG. Pierce A K . Sanford JP. Thomas GD ( 1 972) Nosocomial respiratory infections with Gram-negative baci l l i . The significance of colonization of the respiratory tract. Ann In tern Med 77:701
Johanson WG . Woods DE. Chaudhuri T ( 1 979) Association of rc�p1ratory tract colonization with adherence of gram- negative bacilli to epithelial cells. 1 Infect Dis 1 39:667
Johanson WG . Higuchi J H . Chaudhuri TR. Woods DE ( 1 980) Bacterial adherence to epithelial cells in bacillary colonization of the respiratory tract. Am Rev Respir Dis 1 2 1 :55
Johnson KD. Cadambi A . Seibert B ( 1 985) I ncidence of adult respiratory di-.tress syndrome m patients with multiple musculoskeletal injuries: effect of early operative stabilization of fractures. J Trauma 25:375
Kager L. Malmborg AS. Nord CE. Sjostedt S ( 1 984) Impact of single dose as compared to three dose prophylaxis with latamoxef (moxalactam) on the colonic microflora in patients undergoing colorectal surgery. J Antimicrob Chemother 1 4: 1 7 1
Kapur M M . J ain P , Gidh M ( 1986) The effect o f trauma o n serum C1 activation and its correlation with inju ry severity score in man. J Trauma 26:464
1 20

Kass EG ( 1955) Chemotherapeutic and antihiotic drugs in management of infections of the urinary tract. Am J Med 1 8: 764
Kaye D ( 1 975) Host defense mechanisms in the urinary tract. Urol Clin North Am 2:407 Ke�sncr D M , Lepper MH ( 1967) Epidemiologic studies of gram- negative bacilli in the hospital and
community. Am J Epidcmiol 85:45 Kingma LM ( 1 98 1 ) Gc�ehemati;eerdc r()ntgcndiagnostiek in het acute stadium bij ecn stomp
bor,t- en/of buiklchel. Thc�i� Groningen. Kla;ter>ky J. Cappel R. Noterman J. Mouawad E ( 1973) Endotracheal gentamicin for the preven
tion of bronchial infections in patients with trachcostomy. Int J Cl in Pharmacol 7 :279 Kla,ter;ky J . Debus,cher L. Wcert> D. Daneau D ( 1974) Use of oral antibiotics in protected units
environment: clmical effectiveness and role in the emergence of antibiotic-resist<mt 'train�. Pathol Biol 22:5
Klick J M . Du Moulin GC. Hedley-Whyte J. Te res D. Bushnel LS. Feingold OS ( 1975) Prevention of gram-negative bacillary pneumonia u'ing polymyxin aerosol a' prophylaxb 1 1 . Effect on the incidence of pneumonia in ;eriou;Jy i l l patients. J Clin I nvest 55 : 5 1 4
Knighton D R . Hall iday B , Hunt T K ( 1 986) Oxygen a � a n antibiotic. A compari,on o f t he cffcct"if in;pired oxygen concentration and antibiotic admini,tration on in vivo bacterial clearance. Arch Surg 1 2 1 : 1 9 1
Kurrie E, Bhaduri S , Krieger D . Gau' W, Heimpel H , Pflieger 1-1 ct a l . ( 198 1 ) Risk factor' for infectmn� of the oropharynx and the respiratory tract in patients with acute leukemia. J Infect Di' 1 44: 1 28
La Force FM . Hopkin' J . Trow R. Wang WU ( 1976) Human oral defense� against gram-negative rod>. Am Rev Re>pir Di> 1 1 4 :929
Laforce FM ( 198 1 ) Hosp1tal-ac4uired Gram-neg rod pneumonia': an overview.Am J Med 70:664 Lackner F. Haide r W . Orbes S. Pichler H. Rotter M . Werner HP ( 1975) Septicaemia in critical care
patient' treated with high dme' of ant 1biot1cs. Re'u'citation 3 :205 Lackner F. Coraim F. Benzer H . Koller W. Pichler H , Rotter M ct al ( 1978) Bcobachtungen von
gchiiuftcr Serr.Il ia Marce;cen' Baktcriamic bei lntcn,ivpatienten. Anaesthcsist 27:434 Lambert-Zcchovsky N , Aufrant C, Bingen E, Blum C, Proux MC. Mathieu H ( 1 980) Ccfotaximc
m children: cffic.icy. tolerance and effect on the intc�tinal bacterial flora. J Antimicrob Chcmothcr 6:235
Lauwer' LF. Ro"eel P. Roelanb A . Beeckman C. Baute L ( 1 986) A retro,pective study of 1 30 con;ecutive multiple trauma patient; in an i nten;ive care unit . l nten,ive Care Med 1 2 :296
Lee AKY. Cham V, Chan TK ( 1979) The identification and localization of antithrombin I l l in human tissues. Thromb Res 14 :209
Le Frock JL. El l is CA. Weinstein L ( 1979) The impact of ho,pitalization on the aerohic fecal microflora. Am J Med Sci 277:269
Lowe RJ . Moss . Ji lek J . Levine H D ( 1979) Cry,ta lloid versus colloid m the etiology of pulmonary failure after trauma - a randomized trial in man. Crit Care Med 7: I07
MacKay E. Lackner F. Pauser G. Rotter M. Wewalka G ( 1984) l nfektionsuherwachung an ciner vorwiegend chirurgischen lntensivbchandlungsstation . Anacsthesist 33:564
Mackowiak PhA ( 1982) The normal microbial flora. N Engl J Med 307:83 Maderazo EG . Albano SD. Woronick CL, Drezner A, Overcia R ( 1 983) Polymorphonuclear leu
kocyte migration abnormalities and their 'ignificance in 'eriou,ly traumatized patients. Ann Surg 1 98:736
Martin LF, Asher EF. Casey J M . Fry DE ( 1984) Po,topcrat1vc pneumoniJ. Determinants of mortality. Arch Surg 1 1 9: 379
Martinez OV. Civetta J M . Anderson K. Roger S. Murtha M . Malmi Tl ( 1986) Bacteriuria in the catheterized surgical intensive care patient. Crit Care Med 14 : 1 88
Meakins J L ( 1 985) Surgical infection in critical care medicine. Churchi l l Living>tone. Edinhurgh. van der Merwe CJ . Louw AF. Welthagen D. Schoeman HS ( 1985) Adult respiratory distress syn
drome in case; of >evere trauma - the prophylactic value of methylprednbolone ;odium 'uccinate . S Afr Med J 67:279
Miranda DR. van Saene H KF, Stoutenbeek CP. Zandstra OF ( 1983) Environment and costs in J surgical ICU. The implication of selective decontamination of the digestive tract (SOD). Acta Anacsthesiol Belg 34:223
1 2 1
Moore PG . J11me' OF. Byth PL. Simpson IJ ( 1 985) Factor' affecting outcome after che;t injury. Anae,th l nten,ivc Care 1 3:362
Mulder J G . W1er�ma WE. Welling GW. WaaiJ van dcr D ( 1 98-1) Lm\ do>e or.ii tobramyc:in treatment for ,elccllvc dcconlam1 nation of t he dige,tive tract: .i 'tudy in human volunteers. J Antim1crob Chcmothcr 13 : -195
Murra) I P . Modbcll J H . Gall.igher TJ . Banner MJ ( 1 98-1) Titration of PEEP b) the arterial minu' end-tidal carbon dioxide gradient . Che't 85 · IOO
Murray PR. Rmcnblatt J E ( 1976) Bacteri.il interference by ornpharyngeal and climcal i>olat<.:' of anaerobic bacteria. J Infect Di' 1 3-1:28 1
Newhou'e M. Sanchi' J. Biencn,tocl. J ( 1 976) Lung dcfen'e mechan"m' N Engl J Med 295:990 . 1 0-15
Nichol' RL. Condon RE. Gorbach SL. Nyhu' LM ( 1972) Efficac) of prepoper,1tive antimicrobial preparation of the bowel. Ann Surg 1 76:227
Nichol' RL ( 198 1 ) LJ,e of prnphylactl<: ant1b1ot1cs tn 'urg1cal practice. Am J Med 70:686 Nord CE. Heimdahl A. Kager L. Malmborg AS ( 198-1) The impact of different antimicrobial
agent' on the normal ga,t rn-inte>t inal micrnflora of human>. Re\ l nkct Di> 6:271l Nord NM. Hoeprich PD ( 1 96-1) Polymyxin B and coli>t in . a critical compari>on. N Engl J Med
270: 1 831l Northey D. Ade>> M L. Hartsucl. J M . Rhoade> ER ( 1 97-1) Microbial >urve11lance in a 'urgical in
ten,ive care unit . Surg Gynecol Obstet 1 19:32 1 Og>ton D . Murr.iy J . Crawford G PM ( 1 976) I nhibiton of the activated Cb >ubuntt of the fir>t com
ponent of complement by ant 1thrombin I l l in the pn.:>ence of heparin . Thromb Re> 9 :2 1 7 Onderdonk AB. Bartlett J G . Louie Th . Sullivan-Seigler N . Gorb.tch S L ( 1 976) Microbial >ynergy
in experimental intra-abdominal ab,cc'' · Infect l mmun 1 3 :22 Pepe PE. Hudson LD. Carrico CJ ( 1 98-1) Early application of po>1t l\e end-expiratory pre»urc in
patients at ri'I. for the adult re,piratory-di>tre» >yndrome. N Engl J Med 3 1 1 :281 Pingleton SK. Htnthorn DR. Liu C ( 1986) Entcral nutrition in patienb receiving mechantcal venti
lation. Multiple 'ource' of tracheal colonization tnclude the >tomach. Am J Med 80:827 Pinilla JC ( 1 982) Acute rc,ptratory failure in 't:vcre blunt che>t trauma . J Traum.i 22:22 1 Platt R. Ehrlich SL. Af.inan J . O'brien ThF. Pennington JE. Ka» EH ( 1 98 1 ) Moxalactam therapy
of infection> cau>ed by cephalothin resistant bactcri.i : influcncc of >Crum tnhibitory activity on clin ical rc,pon'e and acgui,ition of antibiotic rc'i'tance during therap) . An1 1m1crob Agents Chcmoth 20:35 1
Platt R. Polk BF. Murdoch B. Ro>ner B ( 1 982) Mortality a>,ociated with ntNKomial urinary tract infection. N Engl J Med 307:637
Poll,1k R. Myers RAM ( 1 978) Earl) diagno>i' of the fat cmboli'm 'yndrnme Crit Care Med 1 8: 1 2 1 Poth EJ . Fromm SM . Wisc RI . H>iang C M ( 1 950) Neomycin a new inte;tinal antbcpt1c. Tcxa>
Rcpt Btol Med 8 :Vi3 Poth EJ ( 1 957) Critical analy>i> of inte>tinal anti>ep>1>. J Am Med A;soc 163: 1 3 1 7 Poth EJ ( 1 960) The practical application o f intestinal ant isepsis t o surgery o f the colon .ind rectum.
Dis Colon Rectum 6:491 Pre;ton GA. Lar,on EL. Stamm WE ( 1 98 1 ) The effect of private i>olation room> on patient care
practices. colonisation and infection in an in tcn;ivc care unit. Am J Med 70:6-1 1 Price DJE. Sleigh J D ( 1 970) Control of infection due to Kleb;iclla aerogencs in .in ncuro,urg1cal
unit by withdrawal of ant1b1otics. Lancet i i : 1 2 1 3 . Price DJ . Ghonheim A T ( 1 98 1 ) Dangers o f antibiotic therapy in ventilated patients (Ab�tract) I l l
World Congress o n intensive and critical care medicine Crit Care Med 9 :260 Reitberg DP. Cumbo TJ, Schcntag JJ ( 1 98-1) Ccfmenoximc in the treatment nf nosocomial pneu
monias in critical care patients. J Antimicrob Chemothcr 13 :8 1 Remington JS . Schimpff SC ( 1 98 I ) Please don't cat the salads. N Engl J Med 30:-133 Risberg B. Heideman M ( 1 980) The cascade systems in post- traumatic pulmonary insufficiency.
I n : Lewb DH (eds) Sympo>ium on po;! traumatic lung in,ufficicncy: etiology. pathophy;iolo· gy and treatment . Acta Chir Scand ('uppl) 499: 107
Risberg B. Medegaerd A. Heideman M . Gyzander E. Bund>en P. Oden M ct al ( 1986) Early activation of humoral proteolytic systems in patients with multiple trauma. Crit Care Med 1 4:9 1 7
Riska E . van Bonsdorff H . Hakkinen S ( 1 977) Primary operative fixation of long bone fracture; in patient> with mult iple injurie' J Trauma I 7· 1 1 1
1 22

Rohrbaugh TM , Anolik R . August C, Serota Ff, Koch P ( 1984) Ah,orption of oral aminoglycosides following hone marrow tran�plantation. Cancer 53: 1 502
Rogers FB. Sheaff CM. Nolan PJ , Robin AP, Merlotti G. Barrett JA ( 1986) Fihronectin depletion and microaggregate clearance following trauma. J Trauma 26:339
Rokkanen P. Alho A. Avikainen V, Karaharju E, Kataja H. Lahdensuu M , Lepbtoe P, Tervo T ( 1 974) The efficacy of corticosteroids in severe trauma. Surg Gynecol Obstet 1 38:69
Rolfe RD ( 1984) I nteractions among microorganims of the indigenou� intestinal flora and their in· fluence on the host. Rev Infect Dis 6:573
Romano P . Margene! A. Sou��y C. Meltzheim B ( 1980) Bilan bacteriologique du service de reanimation chirurgicale et traumatologique de l 'Hopital Henri Mondor. Ann Anesthesiol 20:655
Rose H D , Bahcod. JB ( 1975) Colonization ofinten�ive care unit patients with gram-negative bacill i . Am J Epidemiol 1 0 1 :495
Rosehury Th ( 1 962) Microorgani�ms indigenous to man Mc Graw- Hi l l . New York . Rosendorf LL. Daicoff G, Baer H ( 1974) Sources of gram- negative infection after open heart sur
gery. J Thorne Cardiovasc Surg 67: 195 Rotter M ( 1 978) Chemoprophylaxis in I ntensive Care. l n :Siegenthaler W. Luthy R (eds) Current
Chemotherapy. Am Soc for Microbiology. Washington DC. p50 Rozenberg-Arska M , Dekker AW, Verhocf J ( 1 983) Colistin and Trimetoprim-sulfamethoxazole
for the prevention of infection in patients with acute non-lymphocytic leukaemia. Decrease in the emergence of resistant bacteria. Infection 1 1 : 1 67
Rudi T, Wolff G ( 1 975) Vermeidung posttraumatischer Komplikationen durch fruhe definitive Versorgung von polytraumatisierten mit Frakturen des Bewegung�apparat�. Helv Chir Acta 42:507
Saba TM ( 1 975) Reticuloendothelial systemic host-defense after surgery and tr.iumatic shock . Circ Shock 2 :9 1
Saba TM , Blumenstock FA, Scovil l WA, Bernard H ( 1 978) Cryoprecipitate reversal of opsonic Alpha2-surface binding glycoprotein deficiency in septic surgical and trauma patients. Science 20 1 :622
Saba TM . Jaffe E ( 1 980) Pla,ma fibronectin (opsonic glycoprotein) : its synthesis by vascular endothelial cells and role in cardiopulmonary integrity after trauma as related to reticuloendothelial function. Am J Med 68:577
Saba TM , Blumen�tock FA, Shah DM. Kaplan JE. Cho E. Scovi l l W et al ( 1 984) Reversal offibronectin and opsonic deficiency in patients. Ann Surg 1 99:87
Sabath LD, Postic B, Finland M ( 1 962) Methicillin treatment of severe staphylococcal disease. Observations in 1 46 cases. N Engl J Med 267: 1 049
Saene van H KF, Stoutenbeek CP, Miranda D R , Zandstra DF ( 1 983) A novel approach to infection control in the intensive care unit . Acta Anaesthesiol Belg 34: 193
Saene van HKF, Wil lems FfC, Zweens J ( 1 983) Influence of amoxyci l l in and cefaclor on the colonization resistance of the oropharynx . Scand J Infect Dis 39:97
Saene van JJM. Saene van H KF, Stoutenbeek CP. Lerk CF. I nfluence of faeces on the activity of antimicrobial agents used for decontamination of the alimentary canal Scand J Infect Dis 1 985 ; 1 7 :295
Saene van JJM, Veringa S I . Saene van H KF. Verhoef J , Lerk CF ( 1985) Effect of chlorhexidine and acetic acid on phagocytosis by polymorphonuclear leukocytes. Eur J Clin Microbiol 4 :493
Sanchez-Ubeda R, Fernand E. Rou,selot LM ( 1 958) Complication rate in general surgical cases. N Engl J Med 259: 1 045
Sanders CC ( 1 983) Novel re�i�tance selected by the new expanded-spectrum cephalosporins: A concern. J Infect Dis 1 47:585
Schentag JJ , Vari AJ . Win�lade N E . Swanson DJ. Smith IL . Simons GW et al ( 1 985) Treatment of aztreonam or tobramycin in critical care patients with nosocomial gram-negative pneumonia. A m J Med (suppl 2A) 78:34
Schimpff SC, Young VM , Green W H . Vermeulen GD, Moody M R . Wiernik PH ( 1 972) Origin of infection in acute nonlymphocytic leukemia. Significance of hospital acquisition of potential pathogens. Ann Intern Med 77:707
Schimpff SC, Mi l ler R M , Polakavetz RN, Hornick RB ( 1 974) Infection in the �eve rely traumatized patient. Ann Surg 1 79:352
1 23

Schimpff SC ( 1 980) I n fection prevcnt10n during profound granulrn:ytopcnia. Ann Intern Med 93-.358
Schwarll: SN . Dowling JN. Bcn kovic C. De Ou1ttncr-Buchanan M. Po>tko T. Yee RB ( 1 978) Sources of gram-ncgativc hac1lli colonizing the tr.ichea of intuhatcd Patient>. J Infect Dis 1 38:227
Scovill WA. Saha TM . Kapl,m J E . Bcrn,1rd HP. P<mcr> SP ( 1977) D1>turhancc> in circulating op�onic activity in man after opera ti\ e and hlunt trauma. J Surg Re; 22:709
Scovill WA. Anne�! SJ . Saha TM . Blumcn>tod. FA . Newell JC. Stratton H H ct al ( 1 979) Card1ova�cular hemodynamic> after op>imic alpha-2-;urface binding glycoprotem therapy in inj ured patients. Surgery 86:284
Seibel R . L1Duca J. Has�ctt J M . Bah1k1an G. Milb B. Border DO ct al. ( 1985) Blunt mult iple trauma ( I SS 36). femur tract ion . and the pulmon,tr} f.ii lure-><:ptic >late . Ann Surg 202:283
Scv1t t S ( 1 955) Po;t traumatic adrenal .ipoplcxy. J Clin Pat ho I 8: 1 85 Shield MJ . Hammill HJ . Neale DA ( 1979) Sy>tematic hacterio logic.t l monitoring of intcn;ive care
unit patient;. The rc;ult; of ,1 twel\ e month ;tudy. l ntcn;ive Care Med 5: 17 1 Sibhald WJ . Short A . Cohen MP. Wibon RF ( 1977) Variation; m adrenornrtical re,pon,ivene''
during 'evere bacterial i nfect ion,. Unrecognized adrenocort1cal 111,ulf1cienc} in 'evere bacte rial mfcct1ons. Ann Surg 186· 29
Slcvfcr DT. M ulder N H . Yne' Ho,per' de H G . Fidler V. N ie\\ eg 0. Waai.1 ' an der D ( 1980) I n fection prevention in granul1K} topcnic patieni- by ;elective decontamination of the dige;tive trac t . Eur J Cancer 16 :8.:W
Smith P J . Brookfield DSK ( 1 984) An outbreak of ;erratia marcc•ccn; 111fcct1on in a neonatal un i t . Lancet i : 1 5 1
Sogaard H ( 1 982) The pharmacod\ namic' o f polymyxm antibiotic; with •pccial reference t o drug rcsi;tancc l iahility. J Yet Pharmarnl Thcr 5.2 1 9
Spencer R C . Philip J R ( I 97J) Effect> of prev1ou' antimicrobial therapy o n bacteriological finding' in patient� with primar} pneumonia Lancet 1 1 : 349
Sprunt K. Redman W ( I %8) Evidence 'uggest ing importance of role of intcrbacterial mhihition in maint. i ining halam:c of normal flora. Ann I n tern Med 68:579
Stahl W. Singh A. Marcu; M ( 1 985 ) Re;pon;e; of op>onic ;uh;tancc; to major trauma and ;cpsb. Cnt Care Med 1 3 :779
Steven� R M . Tac; D. Skillman JJ . Feingold DS ( 1 974) Pneumonia in an ICU. A 30-month experience. Arch Intern Med 1 34: !06
Stil le W. Dih el M. Shah PM ( 1 982) Microbial ;election 1 11 the ornl cavity under treatment with ccfot .ix imc. (Ah;tr.ict) Proceeding' of the 1 3th I nternational Congrc" on Chemotherapy. Vienna. p, 4.2/ 1 0-4
Stil le W. Rah me I-Pitzer A. Shah PM ( 1 983) Oral ah;orption and fecal level' of parenteral ccphalo'porin,. Proceeding' 1 3th In ternational Cong re" of Chemotherapy. Vienna. 85 SE8.3/ l - 1 3 . 56
Stoddart JC ( 1 983) Hospital-acquired i nfect ion,. I n : Tinker J. Ra pm M (ed;) Care of the Critically ill patient Springer Verlag. Berl in . p 87J
Stomng RA. Jame;on B. McElwain TJ . Wilt-.ha\\ E. Spiers ASD . Gay a H ( 1 977) Oral non-absorbed antihiot1e> prevent infection in acute non-lymphohla;tic leukaemia . Lancet i i :837
Stoutenbeek CP. Miranda DR. Sa enc van HKF ( 1 982) A new technique for infection prevention in the 111ten;1ve care unit. Ab;tract. Proceeding; 'ixth european congrc'' of anaesthesiology. Anaesthe•ia:56
Sturm J A . Lewis FR. Trentz 0. OeMern HJ . Hempelm,m G. T'chcrne H ( 1 979) Cardiopulmonary parameter> and prognosis after severe muluple trauma. J Trauma 1 9 :305
Sturm J A . Wi•ner D H . OeMern HJ. Kant CJ . T"hernc H . CrcutLig H ( 1 986) Increased lung capillary permeability after trauma: a prospective clinical •tudy. J Trauma 26:409
Sud IJ . Feingold DS ( 1 970) Mechant'm' of polymyxin B re,1;tanec 111 Proteus mirabili;. J Bacteriol 1 04 :289
Sundkdwa K. Akita H . Iwata S. Sato Y ( 1 985) Clirncal superinfcction and it' ;1ttendant ;ymptoma· tic changes in pediatric,, I nfection (suppl I ) 13: 1 03
Svennevig JL, Bugge-Asperhei m B. Vaage J . Gerran 0. Birkeland S ( 1 984) Corticosteroids 1 11 the treatment of blunt injury of the chest. I nj ury 1 6:80
1 24

Tcre' D. Schweer' P. Bu,l111cll LS . I lcdley-Whyte .I ( 1 973) Sources of Pseudomonas aeruginosa infection in a re,piratory/,urgery intensive therapy unit . Lancet i : 4 1 5
Thorp J M . Richard' W C . Telfer AB ( 1 979) A survey of infection in a n intensive c.irc u11 1 t . "Forwarncd i' forarmcd· . Anac,thc,ia 34:643
T1l loh1m J R . Finland M ( 1 969) Bacterial colonization and clinical supcrinfcction of the Respiratory tract complicating antibiotic treatment of pneumonia. J Infect Dis 1 1 9 :597
Tobin MJ . Grcnvik A ( 1 984) Nosocomial lung infection and its di.ignosis . Crit Care Med 1 2 : 1 9 1 Uffelen van R. Sacne van H KF. Fidler V. L6wenberg A ( 1 984) Oropharyngeal nora: source of
colonization of the rc,piratory t ract in patients on art ificial ventilation. Intensive Care Med !0:233
Valenti WM. Trudell RG . Bentley DW ( 1 978) Factors predisposing to oropharyngcal colonization with gram- negative baci ll i in the aged. N Engl J Med 298: l I08
Vogel F. Krau,g1ll P. Rommcl,hc1m K. Exner M. Werner H ( 1 984) Prophylaxc von Pncumonien wiihrend der Bcatmung durch intratracheale Aminoglyl.o,ide Applil..ition Umwcltmedizin 4:57
Vogel F. Oermann R ( 1 985) Veranderungen der Darmnora unter Ant ibiotikatherapie bei 'chwer krankcn Paticntcn. Umweltmedizin 4:63
Vries de-Hospers H G . Waaij van der D ( 1 978) Amphotericin B concentrations in saliva after .ipphcation of 2'X, amphotericin B in orabasc. Infection 6:3
Waaij van der D. Berghub-de Vne, J M . Lekkcrkerk-van der Wees J EC ( 1 97 1 ) Colonization re"'tance of the digestive t ract in conventional and antibiotic-treated mice . J Hyg Camb 69 :405
Waaij van der D. Berghuis-de Vries J M . ( 1 974) Selective elimination of Enterobacteriace,1e 'pecies from the digestive tract in mice and monkeys . .I Hyg Camb 72:205
Waaij van der D ( 1 979) Colonization resistance of the digestive tract as a major lead in the 'election of ant ibiotics for therapy. In : van der Waaij D. Verhocf J (eds) New criteria for antin111:rob1,d therapy. Excerpta Medica. Amsterdam p27 1
Waaij van der D. Aberson .I . Thijm H A . Welling GW ( 1 982) The -..:reening of four aminogl)LOside' in the selective decontamination of the digeMive tract in mice. Infection 10 :35
Wade JC. Schimpff SC. Newman KA. Wiern1k PH ( 1 982) Staphyloccu' ep1dermid1s: an 111cre.i,1 11g cause of infection in patients with granulocytopcnia. Ann I ntern Med 97:503
Wadc JC. de Jongh CA. Newman KA. Crowley J. Wiernik PH. SchimpffSC ( 1 983 ) Selective ,11111 microbial modulation as prophylaxb again't infection during granulocytopenia: Trimethoprim-sulfamethoxazole. J Infect Di' 1 47 :624
Wagner RL. White PF. Kan. Rosenthal M l-I . Feldman D ( 1 984) Inhibition of adrenal �tcroidogcne,is by the anc,thetic etomidate. N Engl J Med 3 1 0: 1 4 1 5
Washington JA I I . Y u PKW. Martin WJ ( 1 97 1 ) Evaluation o f accuracy o f mult1test micromethod 'yMcm for identification of Enterobacteriaceae. Applied Microbiology 24·449
Watt I . Ledingham I Mc A ( 1 984) Mortality amongst multiple trauma patients <1dm1tted to ,in inten'ive therapy unit. Anae,the�ia 39:973
WeinMein L. Goldfield M . Chang TW ( 1 954) Infection� occurring during chemotherapy. N Engl J Med 25 1 :247
Wein,tcin L. Samet CLA . Meade RH ( 1 96 1 ) Effect of paromomycin on the bacterial nor.i of the human intestine. JAMA 1 78:89 1
Weinstein L. Dalton AC ( 1 968) Host determinants of re,ponse to ant1m1crob1al agent,. N Engl J Med 279:467 .524.580
Weinstein L. Brown RB ( 1 977) Colonization. supra111fection and superinfection: major m1crobiologic and clinical problem,. Mt Sinai J Med 44: l (Xl
Wein�tein MP. Reller LB ( 1 984) Clinical importance of "breakthrough· bacteremia. Am J Med 76: 1 75
Weinstein RA. Kabin' SA ( 1 98 1 ) Strategics for prevention and control of multiple drug-re�1�t.int no�ocomial infection. Am J Med 70:449
Wenzel RP. Osterman CA. Hunting KJ ct al . ( 1 976) Hospital-acquired infection�. I Infection �urvcillancc in a university hospital . Am J Epidemiol 1 03 :25 1
Wenzel RP, Thompson RL. Landry SM, Russell BS. M iller PJ . Ponce de Leon S ct al. ( 1 983) Hospital-acquired infections in intensive care unit patients: an overview with cmpha'i' on epidemics. Infect Control 4:37 1
1 25

W1egersma N . Jansen G . van der Waaij D ( 1 982) Effect of twelve antimicrobial drugs on the colonization resistance of the digestive tract of mice and on endogenous potentially pathogenic microorganisms J Hyg (Camb) 88:22 1
Will iams KC. Gibbons RJ ( 1 972) I nhibition of bacterial adherence by secretory immunoglobulin A: a mechanism of antigen disposal . Science 1 77:697
Wilson J M . Guiney DG ( 1 982) Failure of oral tnmethoprim- sulfamethoxazole prophylaxis in acute leukaemia holation of resi�tant plasmids from strmns of Enterobacteriaceae causing bacteremia. N Engl J Med 306: 1 6
Wilson R F . Mammen E F . Robson M C . Heggers JP. Soullier G . D e Poli P A ( 1 986) Antitrombin . prekall ikrein. and f1bronectin levels in surgical patients. Arch Surg 1 2 1 :635
Wolff G. Dittmann M . Riidi Th ( 1 978) Koordination von Chirurg1e und lntensivmedizin zur Vermeidung der posttraumatischen respiratorbche lnsuffiz1enz . Unfallheilkunde 81 :425
Yoshiol..a H . Fujita K. Maruyama S. 01..a R ( 1 982) Change., in aerobic pharyngeal flora related to antibiotic use and the emergence of gram-negative baci l l i . Cl in Pcdiatr ( Phila) 2 1 :460
1 26
Curriculum Vitae
Date of birth
Place of birth
Marital status
Christiaan Peter Stoutenbeek
Augu�t 1 2 , 1 947
Utrecht , the Netherlands
Married in 1 970 to Margot Liesbeth Nijboer Daughter, Astrid Catharina, born in 1 977 Son , Robin Christiaan , born in 1 98 1
Education 1 960- 1 966, Stedel ij k Gymnasium Utrecht 1 966- 1 973 , Medical School University of Utrecht
Postgraduate training 1 973- 1 974, Resident in Surgery, I nternal Medicine , Gynecology and Obstetrics, Bleuland Hospital , Gouda , the Netherlands. 1 974 , Course in Tropical Medicine at the Royal Institute for the Tropics, Amsterdam 1 975- 1 976, Tropical doctor in the Albert Schweitzer Hospital , Lambarene, Gabon. 1 976- 1 979, Resident in Anesthesiology and I ntensive Care (Prof. Dr. D. Langrehr) , University Hospital , University of Groningen , the Netherlands 1 979- 1 987, Staff-member Dept. I ntensive Care (Director: D . R. Miranda) , University Hospital Groningen , the Netherlands 1 987-, Director Intensive Care , Onze Lieve Vrouwe Gasthuis, 1 c Oosterparkstraat 1 79, 1 09 1 HA Amsterdam , the Netherlands.
Specialty Certification November 1 979 (Dutch Board of Anaesthesia)
127

Publications of the author
Papers:
M iranda DR, Stoutenbeek CP , Kingma L. Differential lung ventilation with HFPPV. Intensive Care Med 1 98 1 ;7: 1 39
Krom RAF, Gips CH, Sikkens H , Slooff HJH, Weits J , Stoutenbeek CP. Two years experience with liver transplantation in Groningen . Neth J Med 1 98 1 ;45 : 1 852
Stoutenbeek CP, Miranda DR, Zandstra DF. A new hygroscopic condenser humidifier. Intensive Care Med 1 982;8:23 1
Miranda DR, Stoutenbeek CP, Karliczek G , Rating W. Effects of dexamethasone on the early post-operative course after coronary artery bypass surgery. J Thorac Cardiovasc surg 1 982;30:2 1
Miranda DR, Stoutenbeek CP, Zandstra DF, Alexander JP The effects of serotonine-receptor blockade after cardiopulmonary bypass. A pilot study. Acta Anaesth Belg 1 982;33 ,63
Newton DEF, Wesenhagen H, Stoutenbeek CP. Livertransplants facing the facts of massive blood loss. In : Developments in haematology and immunology vol 5. (eds. Smit Sibinga C. ) Mart in us Nyhoff publishers, Den Haag 1 982.
Miranda DR, Stoutenbeek CP. Etomidate in the ICU Lancet 1 983; 1 7 :684 (letter) Stoutenbeek CP, Saene van HKF, Miranda DR, Waaij van der D. Acinetobacter
mediastinitis and pneumonia in a thorotrastoma patient . The oropharyngeal flora as source of infection. In tensive Care Med 1 983;9: 1 39
Zandstra DF, Stoutenbeek CP, Alexander JP . Antipyretic effect of diclofenac sodium. In tensive Care Med 1 983 :9 :2 1
Stoutenbeek CP, Saene van HKF, Miranda DR, Zandstra DF. The effect of Selective Decontamination of the Digestive Tract on colonization and infection rate in multiple trauma patients. Intensive Care Med 1 984; 1 0: 1 85
Stoutenbeek CP, Saene van HKF, Miranda DR, Zandstra DF, Binnendij k 8 . The prevention o f superinfections in multiple trauma patients. J Antimicrob Chemotherapy 1 984; 14,suppl . B ,203
Stoutenbeek ChP, van Saene HKF, Miranda DR. l nfektie preventie op een chirurgische I ntensive Care . ZIP 1 984;3:34
Saene van JJM, Saene van HKF, Stoutenbeek CP, Lerk CF. I nfluence of faeces on the activity of antimicrobial agents used for decontamination of the alimentary canal . Scand J Infect Dis 1 985 ; 1 7 :295
Zandstra DF, Stoutenbeek ChP, Miranda DR. Effect of mucolytic and bronchodilator aerosol therapy on airway resistance in mechanically ventilated patients. In tensive Care Med 1 985 ; 1 l :3 1 6
1 28
Stoutenbeek CP, Saene van HKF, Miranda DR, Zandstra OF, Binnendij k 8 . A novel approach to antibiotic prophylaxis in multiple trauma patients. I n : Infections en mil ieu chirurgicale . (eds. Viar P.) Librairie Arnette , Paris. 1 986.38 1
Stoutenbeek CP, Saene van HKF. Zandstra OF. Langrehr D . Prevention of no�ocomial Gram-negative pneumonia in critically i l l patients by topical non-absorbable antibiotics. Fortschri tte der Antimikrobielle , antineoplastischen Chemotherapie. Paul Ehrlich Gesellschaft fiir Chemotherapy, Futuramed Verlag, Munchen. I 986
Stoutenbeck CP, Saene van HKF, Miranda DR, Zandstra OF, Langrehr D . Nosocomial Gram-negative pneumonia in critically i l l patients. A 3-year experience with a novel therapeutic regimen. Intensive Care Med 1 986 : 1 2: 4 1 9
Saene van JJM, Lerk CF, Stoutenbeek CP, Saene van HKF. Faecal inactivation of quinolones. J Infect Dis 1 986; 1 53 :999
Stoutenbeek CP, Saene van HKF, Zandstra OF. Effect of oral non-absorbable antibiotics on the emergence of resistance ICU patients. J Antimicrob Chemotherapy I 987; I 9 :5 I 3
Stoutenbeek CP. Saene van HKF. Miranda DR. Zandstra OF. The effect of oropharyngeal decontamination using topical non-absorbable antibiotics on the incidence of nosocomial respiratory tract infections in multiple trauma patients. J Trauma 1 987;27:357
Stoutenbeek CP, Saene van HKF. Zandstra OF. Infection prevention in the ICU by selective flora suppression . (Editorial ) . Intensive & Critical Care Digest (in press) .
Zandstra OF, Stoutenbeek CP. Monitoring treatment of massive unilateral pulmonary embolisms by differential lung ventilation . I ntensive Care Med (in press) .
Sacne van JJM, Lerk CF. Stoutenbeek CP, Saene van H KF. Faecal endotoxin in human volunteers : normal values (submitted) .
Saene van JJM, Keyzer JJ . Lerk CF, Stoutenbeek CP, Saene van H KF. Reduction of intestinal endotoxin pool by oral polymyxin E in volunteers. (submitted) .
Saene van JJM, Lerk CF, Stoutenbeek CP, Saene van H KF. Reduction of intestinal endotoxin pool by oral pefloxacine in volunteers. (submitted) .
Abstracts:
Stoutenbeek CP, Miranda DR. Saene van HKF. A new techn ique for infection prevention in the ICU. Sixth European Congress of Anaesthesiology (Abstract) . Anaesthesia ( 1 982) ; vol summaries:56
1 29

Saene van HKF, Stoutenbeek CP, Miranda DR, Zandstra OF. A novel approach to infection control in the Intensive Care Unit . Proceedings of a symposium on prevention and control of infection in intensive care . Acta Belg Anaest 1 983;34: 1 93
Stoutenbeek CP, Saene van H KF, Miranda DR, Zandstra OF. A new techn ique of infection prevention in the I ntensive Care Unit by Selective Decontamina· tion of the Digestive Tract (SOD). Proceedings of a symposium on prevention and control of infection in intensive care. Acta Belg Anaest 1 983 ;34:209
Miranda DR, van Saene HKF, Stoutenbeek CP, Zandstra OF. Environment and costs in a surgical ICU. The impl ication of selective decontamination of the digestive tract (SOD). Proceedings of a symposium on prevention and control of infection in intensive care . Acta Belg Anaest 1 983 ;34 :223
Zandstra OF, Stoutenbeek CP, Miranda DR. Antipyretic therapy with diclofenac sodium in ICU patients. Effects and side effects of 1 00 mg suppository versus 0,2 mg/kg im . In tensive Care Med 1 983 :9 :206
Saene van HKF, Stoutenbeek CP, Miranda DR. Zandstra OF, Langrehr D , Binnendij k B. Nieuwere inzichten in infectiepreventie bij traumapatienten . De trauma patient . Proceedings nascholingscurus NA V. Utrecht , 1 984.
Zandstra OF, Miranda DR, Stoutenbeek ChP. Clinical approach to differential lung ventilation . Proceedings 2e symposium 'nieuwe perspectieven in beademing en Anesthesiologie . Rotterdam, 1 984.
Saene van HKF, Stoutenbeek CP, Miranda DR, Zandstra OF. Homan vd Heide JN. A new strategy for infection control in Intensive care unit: a prospective two-year study in cardiac surgery babies. Proceedings Second International Symposium on pediatric, surgical and neonatal Intensive Care in Rotterdam. Eds. JC Molenaar, AM Holschneider. Hippokrates Verlag Stuttgart 1 984; 1 68
Stoutenbeek CP, Saene van HKF, Miranda DR, Zandstra OF, Langrehr D. Therapy of Gram-negative pneumonia in in tensive care patients by a combination of selective decontamination of the oral cavity and antibiotics given both intravenously and by aerosol . Proceedings 1 4th International Congress of chemotherapy, Kyoto, 1 985. In : Recent advances in chemotherapy. Tokyo press, 1 985 . p2026
Stoutenbeek CP, Saene van HKF, Miranda DR, Zandstra OF. Langrehr D. The emergence of resistance against prophylactically used antibiotics is preven ted by selective decontamination of the digestive tract . Proceedings 1 4th I nternational Congress of chemotherapy, Kyoto, 1 985. In : Recent advances in che· motherapy. Tokyo press, 1 985 . p2470
1 30
Zandstra DF, Stoutenbeek CP, Miranda DR. Selective monitoring of VC02 during differential lung ventilation in multiple trauma patients with asymmetric lung contusion . Clinical impl ications. Proceedings 3rd Annual Meeting Dutch Society Traumatology Utrecht, november 1 985
Saene van H KF, Stoutenbeek CP, Miranda DR, Zandstra DF, Langrehr D. A new strategy for infection control in multiple trauma patients. Proceedings 3rd Annual meeting Dutch Society Traumatology U trect , 1 985 . I nj ury 1 986; 1 7 :332
Stoutenbeek CP, Saene van H KF, Zandstra DF. The effect of topical non-absorbable antibiotics on the incidence of nosocomial respiratory tract infections in multiple trauma patients. Proceedings Post-graduate Update course in Respiratory Intensive Care , Pavia, 1 986. p 1 67
Langrehr D , Miranda DR, Stoutenbeek CP, Zandstra DF, Saene van H KF. Langzeitsedierung des I ntensivpatienten. 2c Hamburger Anaesthesiologisch/ ln tensivmedizinisches Symposium. Schulte am Esch J (ed). W .Zuckschwerdt Verlag Munchen . 1 986. p46
Saene van H KF, Stoutenbeek CP, Zandstra DF. A new way for prophylaxis and therapy of infections in ICU patients. Proceedings 8 . lnternationales Symposium uber aktuelle Probleme der Notfallmedizin und lntensivtherapie, Munster 1 987. In: l ntensivmedizin 1 987. Lawin P , Peter K, van Aken H, Prien Th. (eds) . I ntensivmedizin Notfal lmedizin Anasthesiologie . Thieme Verlag Stuttgart . 1 987. p92
Stoutenbeek CP, Saene van H KF, Zandstra DF. Effects of selective flora suppression on colonisation and infection rate in intensive care patients. Proceedings 8. ln ternationales Symposium uber aktuelle Probleme der Notfal lmedizin und lntensivtherapie , Munster 1 987. I n : ln tensivmedizin 1 987. Lawin P , Peter K , van Aken H , Prien Th . (eds) . lntensivmedizin Notfallmedizin Anasthesiologie . Thieme Verlag Stuttgart . 1 987. p l 0 1
B leichrodt RP, Stoutenbeek CP. Relaparotomies i n diffuse peritonitis: the surgeon's point of view. Proceedings 8. l ntemationales Symposium uber aktuelle Probleme der Notfallmedizin und Intensivtherapie , Munster 1 987. I n : I ntensivmedizin 1 987. Lawin P, Peter K , van Aken H , Prien Th . (eds) . lntensivmedizin Notfallmedizin Anasthesiologie . Thieme Ver1ag Stuttgart . 1 987 . p 1 1 7
1 3 1


Appendix
Protocol infection prevention in the ICU
133
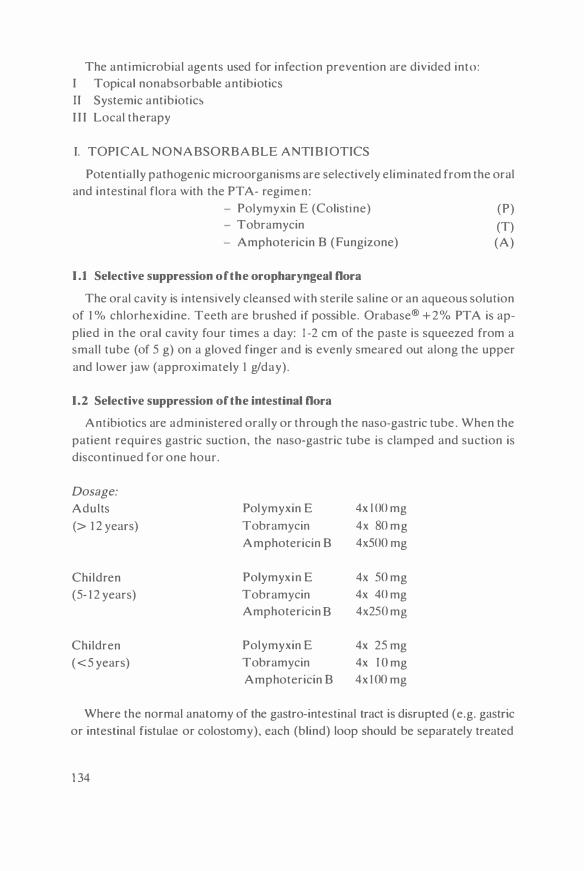
The antimicrobial agents used for infection prevention are divided into: I Topical nonabsorbable antibiotics II Systemic antibiotic� I I I Local therapy
I. TOPICAL NONABSORBABLE ANTIBIOTICS
Potential ly pathogenic microorganisms are selectively eliminated from the oral and in testinal flora with the PT A- regimen :
- Polymyxin E (Colistine) (P) - Tobramycin (T) - Amphotericin B (Fungizone) (A)
1 .1 Selective suppression of the oropharyngeal Dora
The oral cavity is intensively cleansed with sterile saline or an aqueous solution of 1 % chlorhexidine. Teeth are brushed if possible. Ora base® + 2% PT A is applied in the oral cavity four times a day: 1 -2 cm of the paste is squeezed from a small tube (of 5 g) on a gloved finger and is evenly smeared out along the upper and lower jaw (approximately I g/day).
1.2 Selective suppression of the intestinal Dora
Antibiotics are admin istered orally or through the naso-gastric tube . When the patient requires gastric suction, the naso-gastric tube is clamped and suction is discontinued for one hour.
Dosage:
Adults Polymyxin E 4x l 00 mg
(> 1 2 years) Tobramycin 4x 80 mg Amphotericin B 4x500 mg
Children Polymyxin E 4x 50 mg (5- 1 2 years) Tobramycin 4x 40 mg
Amphotericin B 4x250 mg
Children Polymyxin E 4x 25 mg ( <5 years) Tobramycin 4x J O mg
Amphotericin B 4x 1 00 mg
Where the normal anatomy of the gastro-intestinal tract is disrupted (e.g. gastric or intestinal fistulae or colostomy), each (blind) loop should be separately treated
1 34

with approximately half the oral PTA-dosis in an adequate amount of volume. N . B . I n specific circumstances some resorption of the antimicrobial agents may
occur: e .g . neonates, patients with severe gastro-intestinal resorption disturbances after irradiation (Rohrbaugh et al. . 1984 ) ; reduction of the dosage l>hould then be considered .
1.3 Selective suppression of the rectal flora
A patient who does not have peristalsis or produce faeces. and who i� heavily colonised with potentially pathogenic microorganisms in the rectum (more than I 05/g faeces) , should be treated with an enema containing half the oral PTAdosis in 100-200 ml sal ine . two times a day .
I I . SYSTEMIC ANTIBIOTICS
Antibiotics . that disturb the normal indigenous flora as little as possible , are preferred: I . Ccfotaxime 2. Tobramycin 3 . Metronidazol 4. Aztreonam 5 . Flucytosine 6. Amphotericin B
11 .1 Prophylaxis
Gram-positive PPM/Enterobacteriaceae Enterobacteriaceae/Pseudomonadaceae Anaerobes Pseudomonadaceae Yeast/fungi Yeast/fungi
The routine systemic antibiotic prophylaxis for an intensive care patient who has not been hospital ized prior to admission and who probably has a 'normal' flora , consist of cefotaxime 50- 1 00 mg/kg/day iv in 4 daily doses (standard dosis for adults: 4x I g iv). The prophylaxis is discontinued after 4 days unless there are clinical indications to continue .
If a patient receives antibiotics for peri-operative prophylaxis e .g . prophylaxis of endocarditis after implantation of prosthetic material in heart- or vascular-surgery, this prophylaxis may be continued . but additional covering of nosocomial Gram-negative microorganisms with a cephalosporin (e.g. cefotaxime) should be considered.
A patient admitted to the ICU with a recent history of antibiotic usage and hospitalization, is likely to be colonised with nosocomial microorganisms; in this case a broader systemic prophylaxis should be considered (e.g. cefotaxime in combination with tobramycin , or a third- generation quinolone) ; this prophylaxis should be continued until the results of all cultures are free of potentially pathogenic microorganisms .
1 35

When colonisation or infection of the body cavities or of the major organsystems with Enterobacteriaceae or Pseudomonadaceae is to be expected (e.g. intestinal perforations. near-drowning) . cefotaxime is combined with tobramycin (3-6 mg/kg/day iv divided over 3 doses; standard dosis for adults: 3x80 mg iv. guided by plasma levels) . In case of established colonisation by Acinetobacter or Pseudo
monas spp . . cefotaxime should be replaced by ceftazidime or aztreonam . When an increased risk for anaerobic infections exists (e.g. surgery or trauma
of the oropharynx. bowel or vagina). additional anti-anaerobic prophylaxis should be given : Metronidazol 20-25 mg/kg/day iv in 3 doses (standard dosis for adults: 3x500 mg iv) . In contrast to other anti - anaerobic agents, parenteral metronidazol has no perceptible effect on the anaerobic bowel flora.
11.2 Therapy
The criteria for selecting a suitable antibiotic for systemic treatment are : ( i) the spectrum (ii) the pharmocokinetic propertie� (iii) the effect on the indigenous flora. Infections by 'community flora' e .g . Staphylococcus aureus. Streptococcus
pneumoniae. Branhamella catarrhalis. Haemophilus influenzae and Escherichia
coli may be treated with only one antibiotic (monotherapy) . Infections by 'hospital flora· should be treated with a (synergistic) combination of two antibiotics to increase efficacy and to decrease the risk of selection of resistant strains.
Recommendations for different therapeutic antibiotic combinations are given below. including the daily dosage per kg body weight per day and the standard dosis per day.
ll. 2. 1 Enterobacteriaceae
For blind systemic antibiotic treatment and for bacteriologically confirmed infections with Enterobacteriaceae: * Cefotaxime (50- 1 00 mg/kg/day iv)(standard 4x l g) ., Tobramycin (3-6 mg/kg/day iv)(standard 3x80 mg)
ll.2.2 Pseudomonadaceae
* Ceftazidime ( 1 00 mg/kg/day iv) (standard 3x2 g) * Aztreonam ( 1 00 mg/kg/day iv) (standard 3x2 g) * Tobramycin (3-6 mg/kg/day iv) (standard 3x80 mg)
ll.2.3 Yeast and fungi
Yeast and fungi infections (e.g. Candida albicans or Aspergillus spp . ) should be treated with a combination :
1 36

* 5-flucytosine ( J OO- I 50 mg/kg/day iv) in continuous infusion; (standard dosis adults: 1 0 g= 1000 ml iv) * Amphotericin B (0.3-0.6 mg/kg/day iv) in continuous infusion; (standard dosis adults: 20-40 mg iv)
11. 2. 4 Anaerobic infections
* Metronidazol (20-25 mg/kg/day iv)(standard 3x500 mg).
11. 2.5 Enterococcus
�· Co-trimoxazol (trimethoprim 6 mg en sulfamethoxazole 30 mg /kg/day iv) (standard dosis 2x IO ml iv) or
" Ampicil l in (50- 100 mg/kg/day iv)(standard dosis 4x I g) Sometimes treatment with antibiotic agents that disturb the indigenous flora is inevitable , as in severe Streptococcus faecalis or Staphylococcus epidermidis infections.
11. 2. 6 Staphylococcus
Staphylococcus epidermidis septicaemia is a frequent compl ication of indwelling intravascular lines. A line should be removed, if two out of three bloodcultures taken from that l ine , yield the same strain of S. epidermidis (same sensitivitypattern ) . It is often sufficient to replace the l ine at another site ; antibiotic treatment is seldom necessary. Severe infections with S. au re us or S. epidermidis (e.g. endocarditis) should be treated with: ... Ya neomycin (20-50 mg/kg/day iv)(standard do�is 3x750 mg iv) in slow infusion.
III LOCAL ANTIMICROBIAL TREATMENT
111.t Respiratory tract
In the treatment of respiratory tract infections, the same antibiotics that are given parenterally, are administered into the airways by aerosol , in order to obtain h igh antibiotic levels in the bronchial secretions. Because less than 5% of the aerosol is delivered into the terminal bronchiol i , a high antibiotic concentration is necessary. Nebulisation of antibiotics should continue unti l two consecutive cultures of tracheal aspirate are steri le. Aerosol dosis:
Cefotaxime Tobramycin Aztreonam Flucytosine(5-FC) Amphotericin B
500 mg/5ml 40 mg/5ml
500 mg/5ml 5 mg=5ml 5 mg/5ml
4 times a day 4 times a day 4 times a day 4 times a day 4 times a day
1 37

111.2 Wounds, sump-drains, body cavities
Colonised or infected wounds should be treated with local disinfecting agents. These agents should meet the fol lowing cri teria : ( i) no adverse effect on leukocyte function or wound healing ( i i) no toxic side effects ( i i i ) l i ttle protein binding (iv) quick-acting and bactericidal . Silversulfadiazine , nitrofurans, acetic acid , H202 and betadine-iodine interfere with leukocyte function and can produce a local inflam matory response (van Saene et al . I 985b) Taurol in (Geistl ich . Wolhusen . Switzerland) , a re latively new disinfecting agent , does not interfere with leukocyte function. it inactivates endotoxin and can be given intravenously with l ittle side-effect!> (Browne et al . . 1 976) .
Colonisation or infection of the peritoneal , pleural or mediastinal cavities is treated with Taurolin (0 .5% ) . Drains are rinsed with Taurolin (500 ml Taurolin 0.5%/drain/day) on indication.
Colon isation by Pseudomonas spp. can be treated effectively with a 2% aqueous solution of acetic acid. It should be used only for local disinfection as it is not suitable for internal use or wounds. Colonised superficial wounds can be treated with Orabase paste 4 times a day.
III .3 Vagina
Colonisation of the vagina with C. albicans, which may give rise to colonisation of the urinary tract, can be treated with vaginal application of miconazol. two times a day. Colonisation by Gram-negative bacteria should be treated with tampons with Orabase +2%PTA . two times a day.
ISOLATION MEASURES
When a patient is admitted to the ICU , colonised or infected with potentially pathogenic microorganisms insensit ive to the routinely used prophylactic antibiotics, standard isolation measures are taken. The patient is isolated in a single room, and treated with topical nonabsorbable antibiotics unti l the causative microorganisms are no longer isolated from any site. Usually isolation procedures can be discontinued within one week.
D ISPOSABLES
Most disposables used in the ICU will be contaminated with microorganisms from the patienfs flora and may then function as a source of infection . Disposables, used at the bedside of a colonised patient, should be changed more frequently than when a patient is free of PPM. The guidelines given below, should be individually adjusted, depending upon the site and the extent of colonisation.
1 38

Device
Intra vascular devices
Infusion sets Pressure domes venous catheter Arterial catheter Central venous l ine Ventilatoryequipment:
Ventilatory tubing Watersets Humidification system Nebulizers Endotracheal tube Urinary drainage systems:
Urinary volume-meter Urinary catheter Miscellaneous:
Thoracic-drain-sets Sumpdrain-sets
Interval of replacing
:48 hour� :48 hour� :48 hours :on indication :on indication
: I week :48 hours : I month :24 hours :on indication
: I month :on indication
: I week :48-72 hours
BACTERIOLOGICAL MONITORING
Critically i l l patients do not only require intensive monitoring of the haemodynamic and pulmonary function, but also intensive bacteriological monitoring of the microflora of the host .
Sampling: frequency, sites and techniques
Inventory samples from throat, rectum , trachea, urine , wounds, sumps etc are taken upon admission ; survei l lance- cultures from the same sites are taken on Monday, Wednesday and Friday (7 .00 am) . When a patient passes stools, a portion of faeces is collected for quantitative culture. Specimens of the respiratory tract are collected by tracheal-aspiration, via the endotracheal tube. A fresh portion of urine is collected from the indwell ing urinary catheter. Generally, samples consisting of a few ml of fluid, al lowing microscopic examination and quantitative culturing, are preferred to swabs. Some sites, however, have to be sampled by swabs. If the surface to be cultured is too dry, the swabs should be moistened with sterile water.
Blood cultures are taken when the body-temperature quickly rises, accompan ied by chills, or when temperature rises above 39°C. Depending on the site of
1 39

the suspected infection . the blood culture may be taken from an arterial or central-venous line. When endocarditis is suspected, blood-cultures should not be taken from indwel l ing catheters but by arterial puncture .
The bacteriological samples should be processed immediately or else be kept i n a frigidaire (with the exception of blood culture!.) .
Bacteriological examination
All fluid specimens (tracheal aspirate. urine etc) are microscopically examined both in a 'wet' (um.tained) film and in a 'dry' Gram-stained fi lm . noting the cytological and bacteriological content in a semi-quantitative way. Then they are cultured in a quantitative way. One ml or gram of a specimen is suspended in a sterile culture tube containing 9 ml of brain heart infusion (BHI broth . Oxoid) and a dilution series ( I : I 0 steps) is made . After 18 hours of incubation at 37°C all turbid dilution steps are subcultured on four solid media: MacConkey agar plates (Oxoid) for Enterobacteriaceae and Pseudomonadaceae, Yeast Isolation agar plates ( Merck) for yeast and fungi . aesculine azide agar plates (Merck) for S.
faecalis and blood agar plates (Oxoid) for S. aureus. S. viridans and S. epidermidis.
Bacterial concentrations are expressed as logarithmic concentration per ml or gram. Swabs (oropharynx . wounds, rectum) are cultured in a semi-quantitative
way . The same media are inoculated using the four-quadrant method and the tip of the swab is cultured in BHI broth . Agar plates and the BHI broth are incubated for 1 8 hrs at 37°C. If the BHI broth is turbid, inoculation on solid media is performed _ Semi-quantitative estimation of the bacterial concentration is made on a scale of + 1 to +5 . Growth in broth only is reported as + 1 . corresponding to 10 1 bacteria/ml , growth in the first quadrant of the plate as + 2 ( � 103) , in the second quadrant as + 3 ( � 1 O') , m the third quadrant as +4 ( � 1 07) or in the whole plate a�
+5 (> 1 07) . Morphologically distinct colonies are isolated in pure culture and identified by standard techniques (API 20E). Sensitivity tests are determined with the Kirby-Bauer method for all different strains and for all antibiotics used. both for flora suppression and for systemic prophylaxis or treatment (van Saene et al, 1 983) .
Recording
All bacteriological results are stored in a database using a Personal Computer. An application-program has been developed in a general-purpose database (dBasell or I I I , Ashton-Tate , Amsterdam) . This system enables the monitoring of sensitivity patterns in order to disclose emergence of resistance as well as the detection of outbreaks. The final results per patient are presented as a bacteriological chart plotted by the computer. This way of representation of bacteriological
1 40

data visualizes not only the relation between the oral/intestinal flora and the site of infection but also the effect of �elective flora suppre�sion (figure I ) .
Figure I :
Ps . A E R . Fl Ps. A E R .
K L . OX Y.
C. FR E U N D l l
Ps . A E R .
PS . A E R 10
S T R . F A E C . 10
3 6
C. ALB. 3 10
K L . O X Y .
EN T E R OCOC.
Ps . A E R.
C . A L B .
T H R O A T
IBHI I+ 1 j R E C T U M
� S P U T U M
El U R I N E
3 2 10 10
� P. E.S. 69 YR
A B O . W O U N D + S U M P D R A I N S
2 10 4 10
2 3 4 5 6 7 8 9 10
DAY S I C
Bacteriological chart of a patient with a pancreatic p�cudocy�t . infected with multiple intestinal microorganisms. Each square rcprcscnb an i�olatcd stra in . the growth dcn�ity is indicated in�idc the square. Negative cultures arc represented by a da�h.
1 4 1



















