

Unit XIV & XV: Gastrointestinal System Drugs & Nutrients
79
Unit XIV & XV: Gastrointestinal System Drugs & Nutrients Clinical Pharmacology Lourdes College Amy Spangler RN MS CPNP
-
Upload
roary-mcbride -
Category
Documents
-
view
48 -
download
0
description
Unit XIV & XV: Gastrointestinal System Drugs & Nutrients. Clinical Pharmacology Lourdes College Amy Spangler RN MS CPNP. Effects of Drugs on the Digestive System. Drugs may be administered to relieve symptoms and disorders of the digestive system - PowerPoint PPT Presentation
Transcript of Unit XIV & XV: Gastrointestinal System Drugs & Nutrients

Unit XIV & XV: Gastrointestinal System Drugs &
NutrientsClinical Pharmacology
Lourdes College
Amy Spangler RN MS CPNP

Effects of Drugs on the Digestive System
• Drugs may be administered to relieve symptoms and disorders of the digestive system
• Drugs may also cause symptoms to digestive system
• Drugs used in digestive disorders primarily alter GI secretion, absorption, or motility

Drugs Used for Peptic Ulcer (PUD) and
Acid Reflux Disorders (GERD)

Drugs for Peptic Ulcer Disease
• Peptic ulcer disease– Upper GI disorders – Degrees of erosion of the gut wall
• Cause– Imbalance between mucosal and
aggressive factors

Figure 76-1 The relationship of mucosal defenses and aggressive factors to health and peptic ulcer disease.

Classes of Antiulcer Drugs
• Antibiotics• Antisecretory agents• Mucosal protectants• Antisecretory agents that enhance
mucosal defenses• Antacids

Figure 76-2 A model of the regulation of gastric acid secretion showing the actions of antisecretory drugs and antacids.
H. pylori

Helicobacter pylori• Test: breath test or serum• Treatment (two antibiotics are prescribed.)
– Bismuth compounds• Ranitidine bismuth citrate (Tritec)• Bismuth subsalicylate (Pepto)*
– Clarithromycin– Amoxicillin– Tetracycline– Metronidazole
• H2 RA and PPI

Histamine-2 Receptor Antagonists (H2RAs)
• Histamine causes strong stimulation of gastric acid secretion (PNS – Vagus Nerve)
• H2RAs inhibit both basal secretion of gastric acid and secretion stimulated by histamine, acetylcholine, and gastrin
• Decrease amount, acidity, and pepsin content of gastric juices

Histamine2-Receptor Antagonists
• Cimetidine [Tagamet]• Ranitidine [Zantac]• Ranitidine bismuth citrate [Tritec]• Famotidine [Pepcid]• Nizatidine [Axid]

H2 antagonists
• May decrease absorption of other drugs which require acidic environment
• Cimetidine: inhibits liver cytochrome P-450 of some drugs– Warfarin, theophylline, phenytoin
• Dosages should be reduced
– Alcohol metabolism is also inhibited.
Proton Pump Inhibitors (PPIs)
• Strong inhibitors of gastric acid secretion• Bind irreversibly to the gastrin proton pump to
prevent release of gastric acid from parietal cells – blocks final step
• Suppresses gastric acid secretion in response to all primary stimuli, histamine, gastrin, and acetylcholine
• example: Omeprazole (Prilosec)• Also; esomeprazole (Nexium), lansoprazole
(Prevacid)• Biotransformed in liver
– Prilosec and Nexium inhibit metabolism of anticoagulants, diazepam and phenytoin (may increase blood levels)

Sucralfate
• Used to prevent and treat peptic ulcer disease– Does not neutralize acid or decrease secretion
• Acts locally on gastric and duodenal mucosa
• Low incidence of adverse effects• Give alone 30 to 60 min before meals• Give 2 hours before or after drugs as it
may prevent other drugs absorption
Prostaglandin
• Prostaglandin E inhibits gastric acid secretion and increases mucus and bicarbonate secretion, mucosal blood flow, and perhaps mucosal repair
• PT: Misoprostol (Cytotec) – Blocks secretion of excess acid and protects stomach
mucosa in those with use of chronic NSAIDS• Use in duodenal and peptic ulcers caused by NSAID
• Added to an NSAID to decrease negative GI effect: Arthrotec (diclofenac and misoprostol)
• Contraindicated in pregnancy, induces abortion

Antacids
• Alkaline substances that neutralize acids• Inhibits conversion of pepsinogen to pepsin by raising pH• Aluminum compounds have low neutralizing capacity and
slow onset• Magnesium-based have high neutralizing capacity and
rapid onset– Example: Maalox (aluminum hydroxide and magnesium
hydroxide)• Calcium compounds have rapid onset but may cause
“acid rebound”, caldcium carbonate (Tums) – best as Ca++ supp.
• Mixtures may be used, as well as addition of other ingredients
• Al & Ca: constipation, Mg++: loose stools

Antacids…interactions
• May chelate and make insoluble• May decrease absorption of some drugs• If drug needs strong acid environment• Enteric coatings

http://hopkins-gi.nts.jhu.edu/pages/latin/templates/index.cfm?pg=disease4&organ=5&disease=16&lang_id=1
John’s Hopkins University Digestive Disease Library- Stomach and Duodenum Peptic Ulcer Disease

Laxatives and Cathartics

Laxatives
• Used to ease or stimulate defecation– Soften the stool– Increase stool volume– Hasten fecal passage through the
intestine– Facilitate evacuation from the rectum

Indications for Laxative Use
• Constipation is determined by stool consistency and frequency of defecation.
• Indications:– Diagnosis– Treatment/procedure preparation– Constipation– Poisoning

Classification of Laxatives
• Bulk-forming laxatives– Psyllium [Metamucil]
• Stimulant laxatives– Bisacodyl [Dulcolax]
• Osmotic laxatives– Milk of magnesia (MOM)
• Surfactant laxatives (stool softeners)– Docusate sodium [Colace]

Laxatives
• Bulk-forming laxatives are substances that are largely unabsorbed from intestine adding bulk to fecal mass to stimulate peristalsis. Pull water into intestinal lumen– Psyllium (Metamucil)– Methylcellulose (Citrucel)– Polycarbophil (Fiberall, Fibercon)

Laxatives
• Osmotic laxatives increase osmotic pressure in intestinal lumen and cause water to be retained. Distension of bowel promotes peristalsis.– Magnisium Citrate (Milk of Magnesia)– Fleets enema– Lactulose pulls water into intestinal lumen
• Used to treat constipation and hepatic encephalopathy d/t increased BUN, cramping is main SE.
– Polyethelene glycol (GoLytely, MiraLax) evacuant, bowel prep for surgery or treatment for chronic constipation (dose dependent/formulation).

Laxatives, cont.
• Stimulant cathartics are strongest and most abused laxative. Act on the intestinal wall of the small bowel and colon to increase the amounts of fluids and electrolytes within the intestinal lumen. PO or suppository– Bisacodyl (Dulcolax), senna (Senokot)

Laxatives, cont.
• Lubricant laxative lubricates fecal mass and slows colonic absorption of water from fecal mass.– Mineral Oil – enema or
PO
Laxatives, misc.
• Miscellaneous laxatives – Other uses– Sorbitol pulls water into intestinal
lumen. Given with Kayexalate to aid in expulsion of potassium and in Activated Charcoal to help promote elimination of toxins.

Stool Softeners
• stool softeners (surfactant laxatives) decrease the surface tension of fecal mass to allow water to penetrate stool (softer poopy).– Ducosate sodium (Colace, correctol)

Dietary and Herbal Supplements
• Many plant-based supplements such as cascara, psyllium, senna are stimulant laxatives and should only be used short term for the same reason as the prescriptive or OTC forms.
• castor oil obsolete, can cause toxicity and should not be used.
• Aloe is not recommended due to strong stimulant effect

Antidiarrheals

Antidiarrheal Agents
• Opioids– Diphenoxylate [Lomotil]– Activate opioid receptors in the GI tract,
decrease intestinal motility, slow intestinal transmit, more time for fluids and electrolytes to be absorbed
– Camphorated tincture of opium (Paregoric)– Loperamide (Immodium, Kaopectate)
Antidiarrheal drugs
• Bismuth salts (Pepto-Bismol)– have antibacterial and antiviral activity. ASA
component may decrease inflammation Polycarbophil (FiberCon) and psyllium (Metamucil) decrease fluidity of stools
• Specific therapy dependent on cause and may include– Antibacterial – Metroniazole/ Cipro – Enzymatic – if low level of GI enzymes– bile salt-binding - Questran– Short gut syndromes: hycosyamine (anaspaz)

• Nonspecific therapy is adequate fluid and electrolyte replacement
• Do not use antidiarrheals with simple gastroenteritis or abdominal pain (unknown diagnosis)

Antiemetics

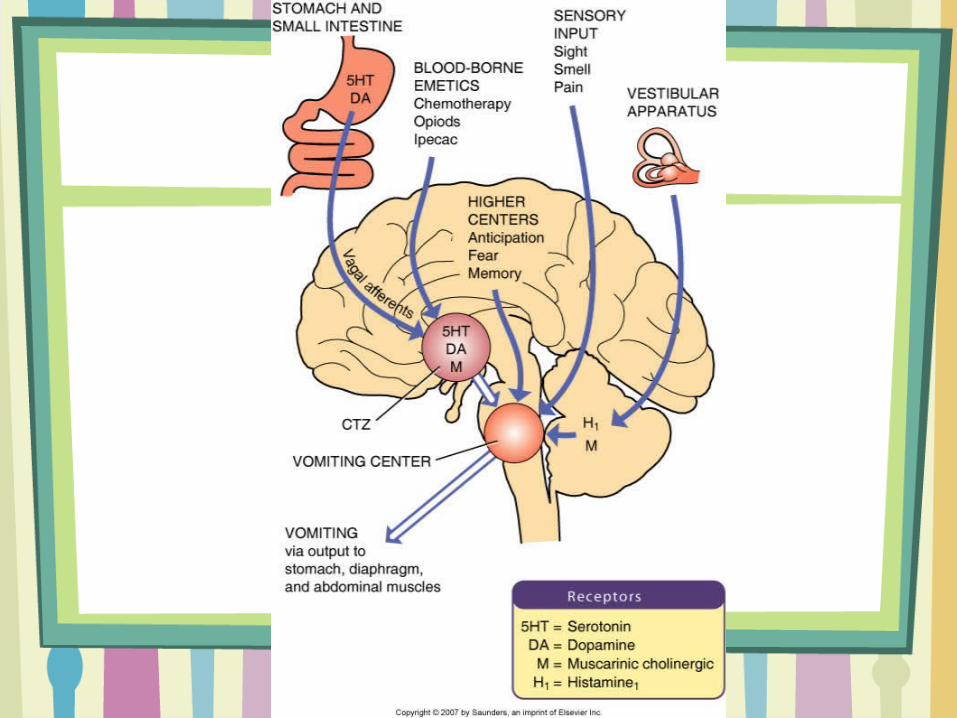

Treatment is based on cause!
• Opioid acting directly on CTZ?• Chemotherapy?• Anxiety?• NSAIDs causing irritation of gastric
mucosa?• Motion sickness?• Increased intracranial pressure?• GI obstruction?

Serotonin Receptor Antagonists
• Blocks serotonin: the major neurotransmitter for emesis
• 5-HT3 located in CTZ, vagal nerve terminals in stomach and small intestine. When these are blocked: prevents initiation of signal for nausea and vomiting.

Antiemetics
• Ondansetron [Zofran]– Blocks type 3 serotonin receptors on
afferent vagal nerve– More effective when used with
dexamethasone• Used to prevent or treat moderate to
acute severe nausea and vomiting associated with cancer chemotherapy, radiation, and postoperatively
• IV, PO• Antagonize receptors and prevent
activation by emetogenic anticancer drugs

Dopamine Receptor AntagonistsPhenothiazines
• Used for Acute Psychosis too (Thorazine)• CNS depressants• Block dopamine from receptor sites in brain and CTZ• Effective in preventing or treating nausea and vomiting induced by drugs, radiation,
surgery and most other stimuli• Ineffective in motion sickness• Cause sedation• Prochlorperazine (Compazine) and • trimethobenzamide (Tigan)• Promethazine (Phenergan) also competitive at the H1 receptor w/ histamine

Cannibinoids
• Dronabinol (Marinol) is a cannabinoid used in management of nausea and vomiting associated with anticancer drugs and unrelieved by other drugs– Side effects include psychiatric symptoms,
high abuse potential, and withdrawal syndrome
– Schedule II narcotic– Decreased use since ondestron emerged

Drugs for Motion Sickness

Muscarinic Receptor Antagonists
• Scopalamine (Transderm –Scop) • anticholinergic drug
– Reversible inhibitor of the actions of acetylcholine at muscarinic recepetors. Prevents actions of acetylcholine in vestibular system.
– Effective in relieving motion sickness. Available in transdermal patch (decreased SE)
Histamine Receptor Antagonists (Antihistamines)
• All antihistamines used in nausea work by anticholinergic activity: H1 receptor blocking agents relieve nausea and vomiting by blocking action of acetylcholine in brain.
• May be effective in treating motion sickness• Not all antihistamines are effective as
antiemetics• Meclizine (Antivert)• PT: Dimenhydrinate (Dramamine)

Benzodiazepine Antianxiety Drugs
• Often used in multi-drug regimens to prevent nausea and vomiting associated with cancer chemotherapy
• Produce relaxation and inhibit cerebral cortex input to vomiting center
• Lorazepam (Ativan) commonly used

Other antiemetics
• Metoclopramide (Reglan) is a prokinetic agent that increases GI motility and rate of gastric emptying by increasing release of acetylcholine in GI tract. Blocks dopaminegic (D2) receptors at the CTZ and blocks at sertogonergic (HT3) receptors. Antagonizes dopamine. Contraindicated in Parkinson’s disease
• Phosphorated carbohydrate solution (Emetrol) is a hyperosmolar solution with phosphoric acid. Reduces smooth muscle contraction in GI tract (OTC)

Irritable Bowel Syndrome
• Antispasmodics (hyosyamine, dicyclomine)
• Bulk forming agents (Psyllium)*• Antidiarrheals (loperamide)*• TCA’s • Antbiotics and acid supresssants• Alosetron (Lotronex)• Tegaserod (Zelnorm)

Drugs for Inflammatory Bowel Disease (IBD)
• Crohn’s disease and ulcerative colitis – see Table 78-5
• 5-aminosalicylates (Sulfasalazine)• Glucocorticoids (dexamethasone)• Immunomodulators (azathioprine
(Imuran), mercaptopurine)
Vitamins

Intake of Vitamins
• Recommended Dietary Allowances (RDAs) for vitamins are set by the Food and Nutrition Board of the Nation Academy of Sciences and represent the average daily dietary intake sufficient to meet the nutrient requirements of nearly all (97%-98%) healthy individuals in a particular life stage or gender.
Intake of Vitamins (cont’d)
• The Tolerable Upper Intake Limit (UL) for a vitamin is the highest average daily intake that can be consumed by nearly everyone without a significant risk of adverse effects.
• The UL is an index of safety—not a recommendation to exceed the RDA.
Vitamins
• Classification of vitamins• Fat soluble
– Vitamins A, D, E, K• Water soluble
– Vitamin C– Vitamin B complex—thiamin, riboflavin,
niacin, pyridoxine, panthothenic acid, biotin, folic acid, cyanocobalamin
Vitamin A (Retinol)
• Deficiency causes– Night blindness– Xerophthalmia – Keratomalacia– Blindness– Therapeutic uses

Vitamins D and E
• Vitamin D– Regulates calcium and phosphorus– Deficiency causes rickets or osteomalacia
• Vitamin E– Antioxidant properties– Dietary sources—fresh greens, seeds, oils

Vitamin K
• Action required for synthesis of prothrombin and other clotting factors
• Deficiency produces bleeding• Adverse effects
– Hypersensitivity reaction– Hyperbilirubinemia
• Therapeutic use– Warfarin overdose

Vitamin C
• Action required for production of collagen and other compounds that bind cells together.
• Has antioxidant properties• Facilitates iron absorption• Deficiency can lead to scurvy
Vitamin B Complex
• Niacin (nicotinic acid)
• Riboflavin (vitamin B2)
• Thiamin (vitamin B1)
• Pyridoxine (vitamin B6)
• Cyanocobalamin (vitamin B12)
• Folic acid

Vitamin Supplements
• Use should be for prevention and treatment of vitamin deficiencies
• Often self-prescribed, over-the-counter preparations
• Megavitamins may be harmful• No difference in use of synthetic versus
natural preparations

Effects of Vitamins
• Folic acid decreases effects of phenytoin and may decrease absorption of zinc – adequate intake reduces risk of neural tube
defects in very early pregnancy
• Niacin may increase risk of rhabdomyolysis with statin cholesterol-lowering drugs– OTC dose 15mg, Lipid lowering dose – 1.5 –
6 gms (SE: hot flashes, take ASA 1hr prior)

Effects of Vitamins – con’t
• Vitamin C- 1g daily may decrease metabolism and increase the effects of estrogens and oral contraceptives
• Vitamin E – Antioxidative effects – Cardio protective
• Vitamin A in large doses and possibly Vitamin E may increase anticoagulant effect of warfarin
• Vitamin K – Anticoagulant, antidote for warfarin (coumadin)

Enteral and Parenteral Nutrition

Enteral and Parenteral Nutrition
• Enteral nutrition is defined as provision of nutrients by way of the GI tract.
• Criteria– Patients with a healthy digestive tract but are
unable or unwilling to eat sufficient food– Patients who have a digestive or absorptive
disorder that cannot be overcome by diet modification

Enteral Nutrition
• Oral feedings safest and most effective• high protein, high-calorie meals with
snacks– commercial supplements, serve cold
• Tube Feedings– functioning GI tract– preferred over IV for long-term use

Enteral Modes of Delivery
• Tube placement– Nasogastric– Nasoduodenal– Nasojejunal– PEG tube
• Schedule of administration– Continuous– Cyclic– Intermittent– Bolus
Components of Enteral Nutrition
• Amino acids• Carbohydrates• Fats• Electrolytes• Vitamins• Trace elements
Complications of Enteral Nutrition
• Aspiration• Pneumonitis• Diarrhea• Vomiting• Insufficient gastric emptying• GI bleeding• Hyperglycemia• Electrolyte imbalances• Fatty acid deficiency
Parenteral Nutrition
• IV feedings are necessary when GI tract is nonfunctioning or needs to rest
• Short-term use provide fluids and electrolytes• Long-term use must provide all nutrients
required for body functioning– given via central vein– fat emulsions provide calories and essential
fatty acids
Parenteral Nutritional Therapy
Components– Amino acids, dextrose, fats, carbohydrates,
vitamins, electrolytes, and trace elements• Complications
– Increased blood urea nitrogen (BUN)– Glucose intolerance– Hyperlipidemia– Allergy– Infection– Catheter-related complications
• Pneumothorax• Venous thrombosis

Nutritional Products
• Supplement or substitute for dietary intake
• Example - Ensure• Most have 1 kcal/mL (up to 2 kcal/ml)• May be formulated for particular organ
impairments (Renal impairment – low Sodium,
• IV available but most are nutritionally incomplete

Pancreatic Enzymes
• Pancreatin and pancrelipase, Pancrease are commercial preparations of pancreatic enzymes
• Must be taken just before or with meals and all food
• Aid digestion and absorption of dietary carbohydrate, protein, and fat
• Cystic fibrosis, chronic pancreatitis, pancreatectomy, and pancreatic obstruction
Drugs for Obesity

Drugs for Obesity
• Many potential serious side effects, recommended for short-term use, rapid regain of weight when use terminated
• Amphetamines – 1960’s Abused d/t physical dependence – adrenergic agonist – increased metabolism, decrease gastric secretions. Moved to Schedule II and d/c of weight loss indication for this group. ADHD use only
• Fenfluramine/ Dexfenfuramine: 1997 Fen-Fen combo – black box warning to d/c combined use – Death of patients d/t pulmonary hypertension
• Phentermine – Mild prescription form for weight loss– Anorexiant/ adrenergic similar to amphetamines
Drugs for Obesity• Assessment—obesity
– Degree of obesity• Body mass index (BMI)
– Pattern of fat distribution• Waist circumference
– Presence of risk factors• Coronary heart disease, diabetes,
hypertension• Other atherosclerotic diseases, sleep
apnea

Weight Loss Therapy Guidelines
• Who should be treated?– BMI of 30 or more– BMI of 25 to 25.9 with two risk factors– Waist circumference with two risk
factors
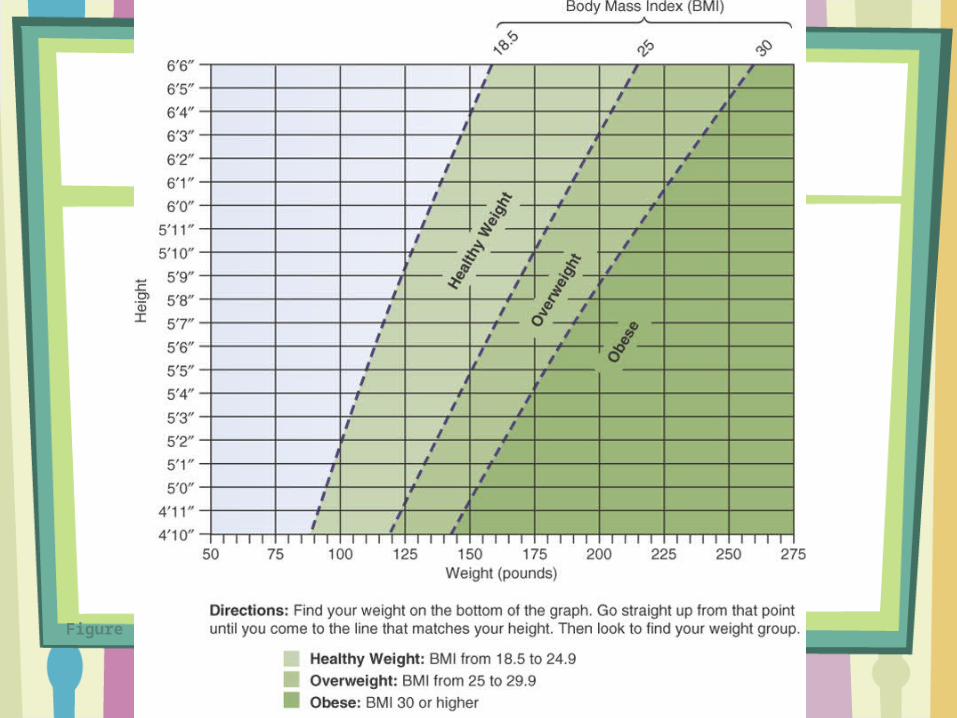
Figure 81-1 Weight classification based on body mass index (BMI).

Treatment Modalities
• Diet therapy• Exercise• Behavior modification• Drug therapy• Bariatric therapy

Sibutramine [Meridia]
• most commonly prescribed• inhibits reuptake of serotonin and norepinephrine, so inc.
saiety and inc. metabolism• Activated with 1st pass then inactivated with 2nd pass• Suppresses appetite and decreases absorption of fat• Drug interactions• Adverse effects
– Headache– – Dry mouth– Constipation– – Elevated heart rate– Insomnia– – Elevated blood pressure– – Nervousness– – Anxiety
Orlistat [Xenical]
• Acts in the GI tract to reduce absorption of fat
• Adverse effects– GI effects
• Flatus, diarrhea, abdominal pain
– Reduced absorption of fat-soluble vitamins• Caution
– Warfarin (enhances effect)


















