
UNIT Three Lesson 3B Positioning - RNPDCrnpdc.nshealth.ca/images/pdf/FT Unit 3 Lesson 3B...
21
Unit Three: Lesson 3B Positioning ____________________________________________________________________________________ ___________________________________________________________________________________ September 2014 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 1 UNIT Three Lesson 3B Positioning Introduction Patient positioning is an integral part of perioperative nursing. Along with infection control practices, patient positioning ranks high on the list of priorities for safe patient care. The perioperative nurse should view positioning as a specialized piece of knowledge that, when applied, can make a distinct difference in patient outcomes. Learning Outcomes 1. Describe the “optimal” surgical position. 2. Identify the positioning considerations that need to be considered with intraoperative positioning. 3. Describe the effects of each position on the musculoskeletal, neurosensory, circulatory, respiratory, and integument systems. 4. Identify the common nerves involved in positioning injuries with surgical patients. 5. List the pressure points associated with the following positions: • Supine • Lithotomy • Lateral • Prone 6. Differentiate between pressure, friction, and shear force, in terms of positioning injuries. 7. Identify some common positioning devices used in the preoperative setting. 8. Apply the nursing process to patient positioning. 9. Identify the required documentation for surgical positioning.
Transcript of UNIT Three Lesson 3B Positioning - RNPDCrnpdc.nshealth.ca/images/pdf/FT Unit 3 Lesson 3B...

Unit Three: Lesson 3B Positioning ____________________________________________________________________________________
___________________________________________________________________________________ September 2014 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 1
UNIT Three
Lesson 3B Positioning
Introduction Patient positioning is an integral part of perioperative nursing. Along with infection control practices, patient positioning ranks high on the list of priorities for safe patient care. The perioperative nurse should view positioning as a specialized piece of knowledge that, when applied, can make a distinct difference in patient outcomes. Learning Outcomes 1. Describe the “optimal” surgical position. 2. Identify the positioning considerations that need to be considered with
intraoperative positioning. 3. Describe the effects of each position on the musculoskeletal, neurosensory,
circulatory, respiratory, and integument systems.
4. Identify the common nerves involved in positioning injuries with surgical patients.
5. List the pressure points associated with the following positions: • Supine • Lithotomy • Lateral • Prone
6. Differentiate between pressure, friction, and shear force, in terms of positioning
injuries. 7. Identify some common positioning devices used in the preoperative setting. 8. Apply the nursing process to patient positioning. 9. Identify the required documentation for surgical positioning.

Unit Three: Lesson 3B Positioning ____________________________________________________________________________________
___________________________________________________________________________________ September 2014 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 2
Required Readings Operating Room Nurses Association of Canada. (2013). The ORNAC Standards for
perioperative registered nursing practice (11th ed.). Canada: Author. • Specimen, Section 3, pages 144-149
Phillips, N. (2013). Berry & Kohn’s Operating Room Technique. (12th ed.). Toronto:
Mosby, • Positioning, page 489-509.
Note: This reading (Phillips) provides the foundation for surgical positioning and should be used in conjunction with this lesson. Required Video AORN (2010). Safely positioning the surgical patient [Video 35 mins]. AORN.
Unit Three: Lesson 3B Positioning ____________________________________________________________________________________
___________________________________________________________________________________ September 2014 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 3
Intraoperative Positioning Intraoperative positioning is the art of moving and securing human anatomy into place to ensure the best surgical site exposure with the least compromise of the patient’s physiologic functions and minimal mechanical stress on the patient’s joints. Positioning patients safely for surgery to facilitate positive patient outcomes is a routine intraoperative nursing responsibility. The perioperative nurse shares responsibility and legal accountability for positioning with the surgeon and the anesthesiologist. Therefore, it is imperative that the perioperative nurse know her/his responsibilities as to assessment criteria, anatomical and physiological considerations, safety measures, and documentation of the position, devices used, and patient outcomes (Goodman & Spry, 2014). Desired Outcomes of Surgical Positioning The optimal surgical position provides optimal exposure for the surgeon while allowing access to the patient’s airway, intravenous lines, and monitoring devices. The position should not compromise integumentary, circulatory, respiratory, musculoskeletal, or neurological structures. The comfort and dignity of the patient should always be considered. Although desired outcomes are patient specific, there are desired patient outcomes relative to positioning that are applicable to all patients. At the completion of the procedure, the patient should have sustained no injury as a result of positioning. Criteria for measuring achievement of the desired outcomes include:
• Skin integrity is maintained--no signs and symptoms of:
- physical injury reported by the patient. - impaired skin integrity or breakdown.
• Breathing pattern is unaltered--no signs and symptoms of:
- ineffective breathing. - impaired gas exchange.
• Tissue perfusion is unaltered--no signs and symptoms of: - edema. - cold or discolored extremities. - diminished arterial pulses.

Unit Three: Lesson 3B Positioning ____________________________________________________________________________________
___________________________________________________________________________________ September 2014 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 4
• There is no injury to musculosketetal or nervous system--no signs and symptoms of: - postoperative cramping or pain in joints or muscles (excluding the surgical
site) - inability to resume preoperative range of motion without pain or discomfort - weakness, tingling, or numbness in extremities sensory deficit (Goodman &
Spry, 2014). Patient dignity should also be a desired outcome during positioning. The patient should not be exposed unnecessarily, and once positioning is complete, a final check should be made to ensure that the patient is appropriately covered. Patients should be comfortable with the idea that, even when they are anesthetized and most vulnerable, they will be appropriately covered. Traffic in the room should be limited, and the doors kept closed. Provide privacy for the patient to speak openly to the perioperative staff while awake (AORN, 2013). For some patients, the response to entering the operating room is to relinquish control to their caregivers. Even an awake patient who feels a loss of dignity when exposed during positioning may not feel confident enough to cover an area inadvertently left exposed. The perioperative nurse, as patient advocate, must preserve the patient’s dignity whether the patient is awake or asleep. Considerations for Surgical Positioning Perioperative nurses need specific knowledge surrounding anatomy (musculoskeletal, vascular, nervous systems), range of motion, risks of pulmonary/cardiovasuclar compromise, and pressure injuries when regards to positioning surgical patients safely. We will discuss a few of these in detail. 1. Range of Motion: Pressure on or stretching of nerves can lead to paralysis and
wasting (Phillips, 2013). The body should be kept in proper alignment and all extremities need to be supported during surgical positioning. The joints of the human body allow a specific range of movement or range of motion (Fuller, 2013). During surgical positioning, it is critical not to exceed the limits of a joint. For example, when positioning a patient’s arm on an armboard, it is critical to restrict abduction to less than 90º (Fuller, 2013).
2. Physiologic Compromises: Ineffective breathing patterns and impaired gas
exchange can either be caused by, or exacerbated by, surgical positioning which restricts chest movement, limits movement of the diaphragm, reduces lung compliance, and changes ventilation/perfusion matching. Also, the cardiovascular system’s response is affected by surgical positioning through the effects of
Unit Three: Lesson 3B Positioning ____________________________________________________________________________________
___________________________________________________________________________________ September 2014 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 5
anesthetic agents, inhibition of normal compensatory mechanisms, cardiac reserve, venous return, and vascular resistance (Rothrock, 2015).
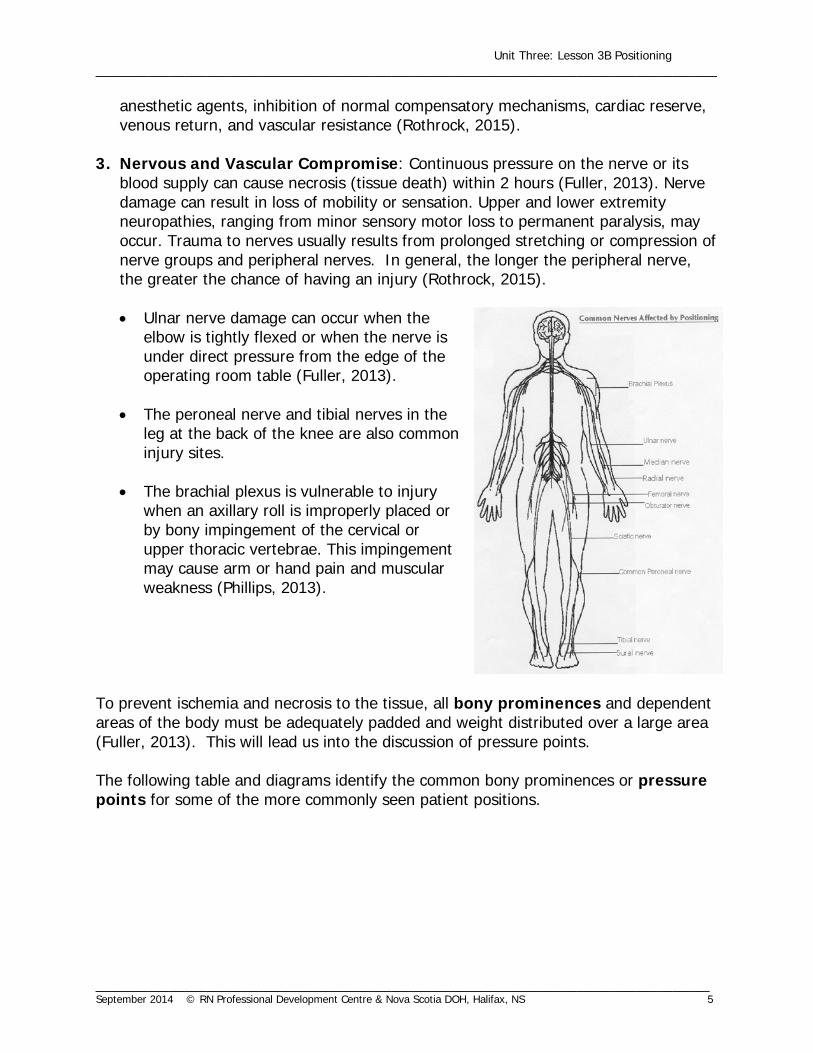
3. Nervous and Vascular Compromise: Continuous pressure on the nerve or its
blood supply can cause necrosis (tissue death) within 2 hours (Fuller, 2013). Nerve damage can result in loss of mobility or sensation. Upper and lower extremity neuropathies, ranging from minor sensory motor loss to permanent paralysis, may occur. Trauma to nerves usually results from prolonged stretching or compression of nerve groups and peripheral nerves. In general, the longer the peripheral nerve, the greater the chance of having an injury (Rothrock, 2015).
• Ulnar nerve damage can occur when the
elbow is tightly flexed or when the nerve is under direct pressure from the edge of the operating room table (Fuller, 2013).
• The peroneal nerve and tibial nerves in the leg at the back of the knee are also common injury sites.
• The brachial plexus is vulnerable to injury
when an axillary roll is improperly placed or by bony impingement of the cervical or upper thoracic vertebrae. This impingement may cause arm or hand pain and muscular weakness (Phillips, 2013).
To prevent ischemia and necrosis to the tissue, all bony prominences and dependent areas of the body must be adequately padded and weight distributed over a large area (Fuller, 2013). This will lead us into the discussion of pressure points. The following table and diagrams identify the common bony prominences or pressure points for some of the more commonly seen patient positions.

Unit Three: Lesson 3B Positioning ____________________________________________________________________________________
___________________________________________________________________________________ September 2014 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 6
Surgical Positions and Their Pressure Points 1. Supine
2. Lithotomy
Calcaneous Sacrum and Coccyx
Thoracic vertebrae Olecranon Scapulae
Occiput
Occiput
Scapulae
Olecranon
Thoracic vertebrae
Sacrum and Coccyx Calcaneous and Metatarsals
Unit Three: Lesson 3B Positioning ____________________________________________________________________________________
___________________________________________________________________________________ September 2014 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 7
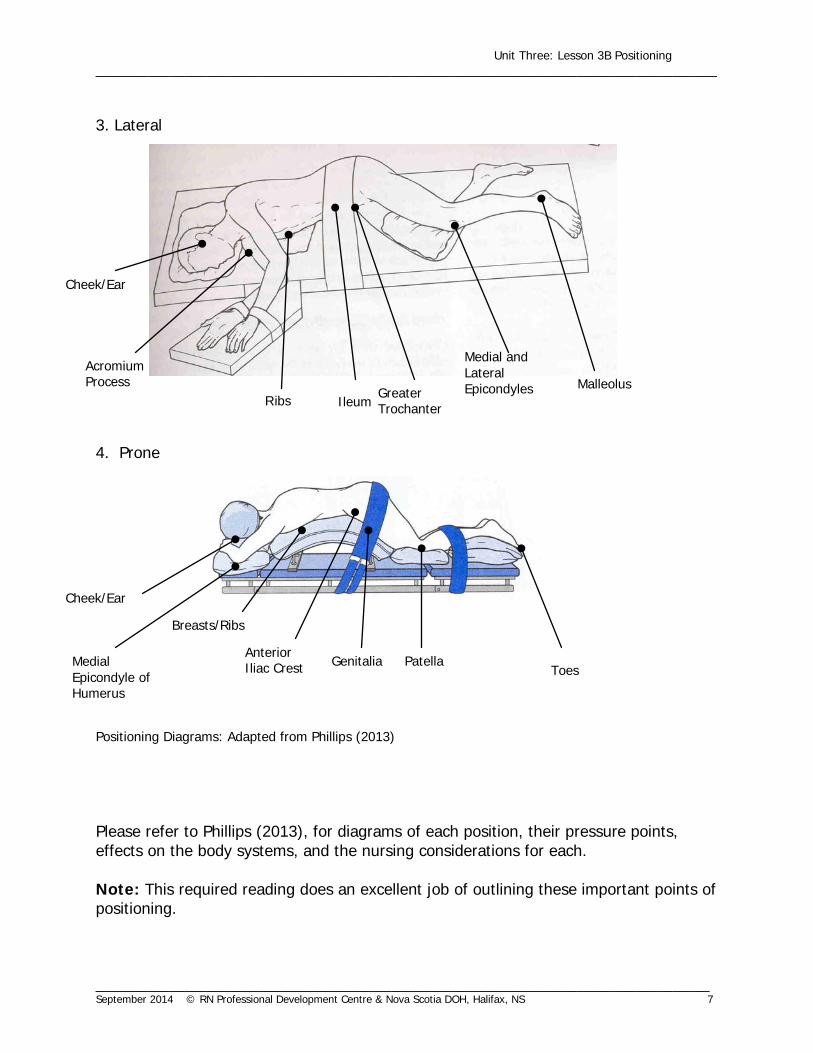
3. Lateral 4. Prone
Positioning Diagrams: Adapted from Phillips (2013) Please refer to Phillips (2013), for diagrams of each position, their pressure points, effects on the body systems, and the nursing considerations for each. Note: This required reading does an excellent job of outlining these important points of positioning.
Cheek/Ear
Acromium Process
Ribs Ileum Greater Trochanter
Medial and Lateral Epicondyles Malleolus
Toes Patella Genitalia
Anterior Iliac Crest
Breasts/Ribs
Cheek/Ear
Medial Epicondyle of Humerus

Unit Three: Lesson 3B Positioning ____________________________________________________________________________________
___________________________________________________________________________________ September 2014 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 8
4. Pressure Injuries: Pressure, friction, and shear forces can combine to produce pressure injuries.
Pressure forces the patient downward against the surface of the OR table, compressing skin, muscle, and bone, and adversely affecting capillary interface pressures. External pressures that exceed normal capillary interface pressures of 32 mm Hg can result in altered tissue perfusion and cause tissue ischemia (Rothrock, 2015).
Friction injuries develop when the patient’s skin rubs against rough, stationary surfaces such as linens, positioning devices, anesthesia equipment, or other surgical equipment. The injuries may be superficial (abrasions or blisters), or they may extend further into body tissues (Rothrock, 2015).
Shear force injuries occur when the patient’s skin remains stationary while underlying tissues shift or move. Patients under general or regional anesthesia can sustain shear injuries if they are repositioned without proper support to their skeletal system (Rothrock, 2015).
Types of Positioning Devices
Positioning devices are designed to fit the different anatomic structures of patients and thereby, facilitate physiologic functions and prevent any of the above outlined compromises (Rothrock, 2015). Each operating room has its own supplies and devices for positioning. These should be clean, in good repair, and used only by staff that is knowledgeable in the mechanics of the equipment (Goodman & Spry, 2014). All positioning devices should perform three functions: absorb compressive forces, redistribute pressure, and prevent excessive stretching. Positioning devices may include, but are not limited to, the following:
• Head rest • Arm boards, padded • Shoulder braces • Kidney braces • Table strap • Leg stirrups
o Yellofins Stirrups: The following is a sample video for the proper use of Yellofins Stirrups commonly used for the lithotomy position in a variety of surgical procedures. http://www.allenmedical.com/product/O-YFES.html
• Table extensions • Table attachment holders (Goodman & Spry, 2014).

Unit Three: Lesson 3B Positioning ____________________________________________________________________________________
___________________________________________________________________________________ September 2014 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 9
Other accessories may include:
• Blankets and sheets to form rolls and bolsters. A draw sheet under the patient’s body can serve as a lift/draw sheet or to secure the patient’s arms at the sides;
• Donuts made of foam, gel, or towels can be used as a head rest and to protect
the ears and nerves of the head, face, knees, and heels;
• Pillows may support various body parts, such as the lower back;
• Sandbags are used for immobilization;
• Padding (foam, cotton, gel) can protect bony prominences and pressure areas;
• Tape may be used to secure the patient or an extremity in a certain position; and
• Elastic bandages, anti-embolectomy stockings, and sequential compression devices help reduce venous pooling in certain positions and for certain conditions (Goodman & Spry, 2014).
Note: Each facility may vary in their surgical positioning devices; therefore, a proper orientation to each device may be required. Always refer to manufacturer’s instructions. Applying the Nursing Process to Surgical Positioning The perioperative nurse must possess the knowledge and demonstrate the skills associated with safe patient positioning required for surgical procedures performed in the operating room. The perioperative nurse must apply the principles of the nursing process to patient positioning to ensure a safe, comfortable position for the patient. 1. Assessment A review of the patient’s assessment information and consultation with the remaining surgical team (nurses, anesthetist, and surgeon) determines the best position for the patient and their surgery (Phillips, 2013). Special attention to disease processes, the presence of implanted devices, and patient risk factors that could impact on the ability to position the patient for surgery should be considered. Positioning of the patient depends on the:
• surgical procedure; • degree of exposure required in the operative field;
Unit Three: Lesson 3B Positioning ____________________________________________________________________________________
___________________________________________________________________________________ September 2014 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 10
• surgeon’s preference; • patient’s condition (e.g., skin condition, age, nutrition, mobility, weight/height,
etc.); and • anesthetist’s need to access the patient (e.g., airway, IVs, lines, warming device,
etc).
2. Diagnosis The ultimate goal of patient positioning according to AORN (2013) is to have the patient free from signs and symptoms of injury related to positioning. Some examples of positioning nursing diagnoses are:
• risk of injury related to intraoperative positioning; • risk of impaired skin integrity related to sustained pressure on certain body parts
intraoperatively; and • risk for ineffective breathing patterns related to intraoperative positioning
(AORN, 2013). 3. Planning After reviewing the patient’s information and considering the risk factors for each patient, the perioperative nurse, in conjunction with the entire surgical team, will plan for the appropriate surgical position. This will include identifying the appropriate mode of transportation and transfer, the positioning supplies and equipment required, and the appropriate amount of surgical staff required to safely position the patient in the correct surgical position (Rothrock, 2015). 4. Implementation Communication is key when positioning the patient in the correct surgical position. Movement or positioning of the patient should be coordinated with the entire surgical team (AORN, 2013). The anesthetist will take the lead during any movements, as it is of the upmost importance that the patient’s airway be protected at all times (AORN, 2013).

Unit Three: Lesson 3B Positioning ____________________________________________________________________________________
___________________________________________________________________________________ September 2014 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 11
The perioperative nurse must also be aware that muscle relaxants are also typically given and therefore precautions must be taken to maintain normal range of motion of any body part during any movements of the patient. The patient’s body must remain in physiologic alignment throughout the process of transfer and positioning. In most cases, the patient is anesthetized following transfer to the OR bed. Once the patient is anesthetized (and permission is given by the anesthetist for positioning/movement), then the surgeon and/or nurse(s) can properly place the patient in the correct anatomical position. When a patient is to be placed in the prone position, they are anesthetized on the stretcher prior to transfer to the OR bed. At least four OR personnel must be available during prone positioning to prevent injury to the patient and personnel.
Safe
ty A
lert
!
Regardless of the surgical procedure, an adequate number of OR staff must be available to assist with patient positioning. The number of staff required is dependent on the size of the patient, their overall condition, the surgical procedure, the required position and the safety of the staff and the patient.
Positioning devices must also be organized and conveniently located (beside or under OR table) to ensure a smooth and safe process. Positioning devices should only be used by staff that is knowledgeable in the mechanics of the positioning equipment. 5. Evaluation Once the patient is in the intraoperative position, the perioperative team should do a “head-to-toe check”. The purpose of the check is to ensure that the patient’s body is in alignment, extremities are not extended beyond their natural range of motion, bony prominences are padded, there is no pressure on nerves, respiratory and circulatory
Safe
ty A
lert
! In terms of surgical positioning, the needs of the anesthesiologist are driven by the need to maintain the patient’s airway. Patient repositioning should not be undertaken after induction without the consent of the anesthetist, since any sudden movement could displace the patient’s airway and affect hemodynamic stability.

Unit Three: Lesson 3B Positioning ____________________________________________________________________________________
___________________________________________________________________________________ September 2014 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 12
efforts are unrestricted, and positioning devices are appropriately positioned and padded. Head-to-Toe Positioning Checklist Positioning Key Checkpoints
1. Head, neck, and cervical spine supported in a
straight line.
Head/neck
2. Scalp, head, and face protected from hairpins, beads, tight anesthesia straps, etc.
Head/face
3. Eyes and ears protected from traumatic pressure/objects and solutions.
Eyes/ears
4. Chest and torso kept in physiological position to allow full, bilateral respiratory expansion.
Chest/torso
5. Breasts protected from excessive pressure.
Breasts
6. Arms in physiological position, adequately supported: • At 90° or less • In flexion, or slight extension • Upper arm on table, not hanging or
touching metal • Elbows protected • Hands free with fingers in slight flexion
or neutral • Wrist restraints loose or padded (use
only as needed) • Palms up on arm board whenever
possible • Palms toward body when arms at sides
Arms Elbows Hands Palms
7. Genitals free of pressure. Ensure solutions do not pool. Ensure any indwelling devices (e.g. urinary catheters) are free from obstruction and there is no tension on the device.
Genitals
Unit Three: Lesson 3B Positioning ____________________________________________________________________________________
___________________________________________________________________________________ September 2014 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 13
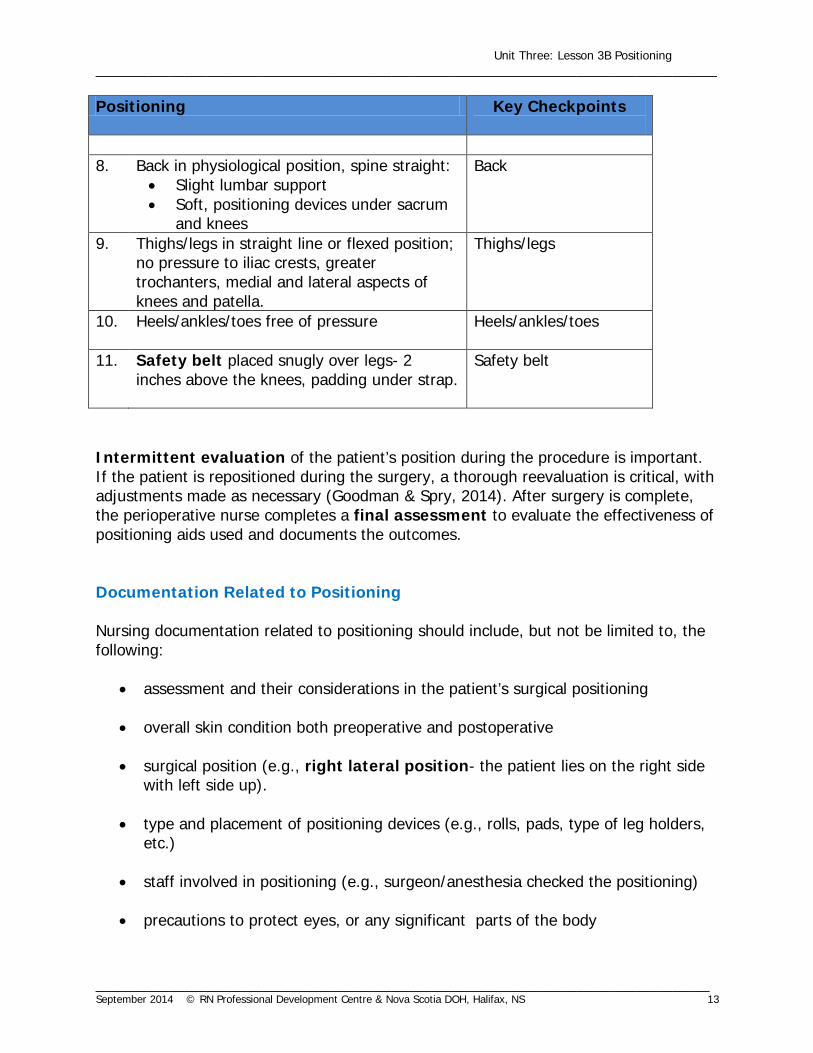
Positioning Key Checkpoints
8. Back in physiological position, spine straight:
• Slight lumbar support • Soft, positioning devices under sacrum
and knees
Back
9. Thighs/legs in straight line or flexed position; no pressure to iliac crests, greater trochanters, medial and lateral aspects of knees and patella.
Thighs/legs
10. Heels/ankles/toes free of pressure
Heels/ankles/toes
11. Safety belt placed snugly over legs- 2 inches above the knees, padding under strap.
Safety belt
Intermittent evaluation of the patient’s position during the procedure is important. If the patient is repositioned during the surgery, a thorough reevaluation is critical, with adjustments made as necessary (Goodman & Spry, 2014). After surgery is complete, the perioperative nurse completes a final assessment to evaluate the effectiveness of positioning aids used and documents the outcomes. Documentation Related to Positioning Nursing documentation related to positioning should include, but not be limited to, the following:
• assessment and their considerations in the patient’s surgical positioning • overall skin condition both preoperative and postoperative • surgical position (e.g., right lateral position- the patient lies on the right side
with left side up). • type and placement of positioning devices (e.g., rolls, pads, type of leg holders,
etc.) • staff involved in positioning (e.g., surgeon/anesthesia checked the positioning) • precautions to protect eyes, or any significant parts of the body

Unit Three: Lesson 3B Positioning ____________________________________________________________________________________
___________________________________________________________________________________ September 2014 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 14
• any changes made to position during the procedure • presence and position of safety strap (Goodman & Spry, 2014).
Summary Positioning the surgical patient is a vital component of perioperative nursing practice and must be completed with knowledge and forethought (Watson, 2011). Patient positioning ranks high on the list of priorities for safety because intraoperative positioning injuries are devastating for patients. Therefore, the perioperative nurse must work with the surgical team to focus on safety of the patient and do everything to promote positive surgical outcomes (Watson, 2011).
Unit Three: Lesson 3B Positioning ____________________________________________________________________________________
___________________________________________________________________________________ September 2014 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 15
Learning Check
1. Which positions compromise respiratory function in the surgical patient?
(a) lithotomy (b) lateral (c) prone (d) reverse trendelenburg
1. a, b, c 3. a, c, d 2. b, c, d 4. a, b, d
2. Which peripheral nerve is most often injured by improper positioning?
1. Ulnar 2. Sciatic 3. Obturator 4. Brachial Plexus
3. Injury resulting from prolonged pressure and stretching due to improper positioning of the anesthetized patient can occur in which of the following peripheral nerves?
(a) brachial plexus (b) frontal (c) cervical (d) peroneal
1. a, b 3. b, c 2. a, d 4. c, d

Unit Three: Lesson 3B Positioning ____________________________________________________________________________________
___________________________________________________________________________________ September 2014 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 16
4. Which of the following factors are pertinent to the perioperative team’s decision regarding surgical positioning of a patient? (a) Checks the OR schedule for the surgical procedure, surgeon, and type of
anesthesia. (b) Checks the surgeon’s preference card. (c) Assesses the patient. (d) Consults with the surgeon and anesthesia personnel when the patient’s
condition precludes the use of the surgeon’s preferred position.
1. a, b 3. c, d 2. a, d 4. all of the above
5. When formulating the positioning plan, which of the following should be considered?
(a) Must know how to use all equipment needed in patient positioning or seek
assistance from someone who does. (b) Notifies anesthesia who will determine the surgical position. (c) Collects equipment and notifies personnel who will be needed for the
positioning. (d) Bases the plan on the patient’s desires and equipment available.
1. a, c 3. b, c 2. a, d 4. b, d
6. Which of the following are additional safety rules to consider in patient
positioning?
(a) No body part should extend off the OR table. (b) The patient’s legs may be crossed during surgery. (c) The patient’s arms must never be abducted more than 30°. (d) Once the patient is on the OR table, a safety belt should be attached over
the patient’s legs 2 inches above the knees.
1. a, b 3. b, c 2. a, d 4. c, d
Unit Three: Lesson 3B Positioning ____________________________________________________________________________________
___________________________________________________________________________________ September 2014 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 17
7. Case Study
M.C. is a 22-year-old college student who is scheduled for a Dilation & Curettage of the Cervix. For the past 2 years, she has been closely followed by her physician with pap smears performed every 6 months, because of results which suggested dysplasia. Results of her last pap smear (1 month ago) suggested that the moderate dysplasia has progressed to severe with questionable carcinoma in situ.
A colposcopy was performed in her physician’s office which confirmed these findings. Surgery (D & C) was booked to establish the degree of carcinoma infiltration. Question: Based on the case study presented, indicate the surgical position required and the potential for injury to the patient related to the surgical position.
• Position:
• Potential for injury of this position:

Unit Three: Lesson 3B Positioning ____________________________________________________________________________________
___________________________________________________________________________________ September 2014 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 18
8. Case Study
B.H. is a 32-year-old male who has been scheduled for an incision and drainage of a pilonidal cyst (cyst at bottom of coccyx) through day surgery. He is 5 feet 10 inches tall and weighs 280 pounds.
B.H. does not smoke, but does drink two to four glasses of beer per week. B.H. is a teacher and he spends most of his day standing, sitting occasionally. He is an avid runner and cyclist.
Question:
Based on the case study presented, indicate the surgical position required and the potential for injury to the patient related to the surgical position.
• Position
• Potential for injury of this position:

Unit Three: Lesson 3B Positioning ____________________________________________________________________________________
___________________________________________________________________________________ September 2014 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 19
Learning Check Answers 1. 1 2. 4 3. 2 4. 4 5. 1 6. 2 7. Position: Lithotomy
Potential for injury related to lithotomy position:
• Hands – should not extend beyond the break in the table. If the arms are to be placed at the patient’s sides, they should be crossed over the patient’s chest prior to raising the end of the table.
• Elbows – to prevent pressure place armboards parallel against the table.
• Ulnar nerve – extend arms at the elbows.
• Bracheal Plexus – if in Trendelenburg, do not extend arms beyond 90°.
• Femoral/obturator nerve -
• buttock cannot extend beyond break in the table, have the patient position himself just above the break in the table.
• Pad sacrum to prevent pressure. • two staff should simultaneously raise the legs and place feet in
stirrups. • hip should be symmetrical. • calves parallel to the table. • do not allow instruments to rest on the groin area. • pad all stirrups.
• Peroneal nerve damage -
• stirrup holders should be placed well on the outside of the leg allowing no contact between the leg and the holder.
• extra padding around knee.

Unit Three: Lesson 3B Positioning ____________________________________________________________________________________
___________________________________________________________________________________ September 2014 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 20
8. Position: prone (Jack knife)
Potential for injury related to prone position:
• Position patient prone with a minimum of four persons. Ensure stretcher and bed are locked prior to transfer;
• Check pedal pulses before positioning and after positioning;
• Pad the head and face, feet, arms (including elbows and wrists), knees, and other bony prominences. Eyes should be taped shut and clear of all pressure.
• Place bolster on each side of chest (to reach from iliac crest to acromium
process);
• Check to ensure genitals are free of pressure;
• Position patient’s arms on armboards with palms down (arms at right angles or flexed at the elbows);
• Place padded safety strap 2 inches above the knees.
Evaluation:
• Assess the patient’s skin integrity for color changes, breaks in the skin; check temperature of feet and color of toes;
• Assess peripheral pulses as to perfusion compared with preop; • Document the skin condition preoperatively and postoperatively. Also
document pre-existing conditions, position, positioning devices, and patient outcomes.
Unit Three: Lesson 3B Positioning ____________________________________________________________________________________
___________________________________________________________________________________ September 2014 © RN Professional Development Centre & Nova Scotia DOH, Halifax, NS 21
References AORN (2013). Perioperative standards and recommended practices. Colorado: Author. Fuller, J. (2013). Surgical technology. (6th ed.). Toronto: Mosby. Goodman, T. & Spry, C. (2014). Essentials of Perioperative Nursing (5th ed.) Toronto:
Jones and Bartlett Publishing. Operating Room Nurses Association of Canada. (2013). ORNAC Standards for
Perioperative Registered Nurses (11th ed.). Canada: Author. Phillips, N. (2013). Berry & Kohn’s Operating Room Technique. (12th ed.). Toronto:
Mosby. Rothrock, J.C. (2015). Alexander’s Care of the Patient in Surgery
(15th ed.). Toronto: Mosby.
Watson, D. (2011). Perioperative safety. Toronto: Mosby.


















