
Unit 9 Management of Comorbidities and Other Services
64
Unit 9 Management of Comorbidities and Other Services Training for Clinicians on the Use of the Namibian Guidelines for Antiretroviral Therapy, 6 th Edition
Transcript of Unit 9 Management of Comorbidities and Other Services

Unit 9
Management of Comorbidities and
Other Services
Training for Clinicians on the Use of the
Namibian Guidelines for Antiretroviral
Therapy, 6th Edition

Unit 9: Slide 2
TB/HIV CO-INFECTION

Unit 9: Slide 3
World Top 10 Notification Rates; 2017
0
100
200
300
400
500
600
700
800
Sou
th A
fric
a
Lesot
ho
Kiri
bati
Phi
lippi
nes
Moza
mbiq
ue
DPR
Kore
a
Timor-
Leste
Gab
on
Nam
ibia
PN G
uinea
NO
TIF
ICA
TIO
N R
AT
E

Unit 9: Slide 4
Trends in case notification rates;
2007-2017
Source: ETR.net V20180222

Unit 9: Slide 5
Estimated burden of TB Disease in
Namibia; 2017
Source: WHO Global TB report 2018.

Unit 9: Slide 6
• Very high prevalence of both HIV and TB
• Most common HIV-related OI in Sub-Saharan Africa
• In 2017:
98% of TB patients knew their HIV status
36% of these patients tested HIV positive
• Intensified TB Case-finding (ICF)
Screen all PLHIV for TB at each encounter
o Symptoms
o Exposure contact
Eligible PLHIV should be offered TPT
TB/HIV Co-Infection
Source: ETR.net V20180222

Unit 9: Slide 7
TB/HIV Co-Infection (2)
• 10% lifetime risk of reactivating latent TB among HIV negative
persons
• 10% risk per year of reactivating latent TB among HIV positive
persons
HIV +
HIV -
New TB
Infection
Latent
TB
Infection
Primary
Progressive
TB Disease (children,
rare adults,
HIV+)
~ 10%
reactivate (TB disease)
each year
~ 5%
reactivate (TB disease)
2 years
till death
~5 %
reactivate (TB disease)
1-2 years

Unit 9: Slide 8
• Reduces risk of active tuberculosis by 60 - 90%
in HIV positive patients on ART
• Can be used in pregnancy
• All HIV positive patients who do not have a
contraindication should have a course of TPT
TB Preventative Therapy (TPT)

Unit 9: Slide 9
• Screen all PLHIV for TB
• If no to TB screening questions
Initiate TPT
• Assess this at every clinical visit
• Patients that have completed TB treatment
should be initiated immediately on TPT
Eligibility for TPT

Unit 9: Slide 10
• Refer to Handout 9.1 / guidelines on algorithm
for TB screening and TPT initiation.
• Symptom screening in adults
Cough (current), weight loss, night sweats, fever
• Symptom screening in children
Cough (current), poor weight gain, fever,
swellings in the neck or armpits (lymph node
enlargement), recent close contact
• If yes to any symptom screening question
Perform a bacteriological examination for TB
Algorithm for TB Screening

Unit 9: Slide 11
• Bacteriologically (preferred) Xpert MTB/RIF (GeneXpert)
o an automated molecular diagnostic test for TB .
o Detects M.tb as well as rifampicin resistance-conferring mutations
o Provides results directly from sputum in less than two hours.
o Should be the first diagnostic test for all presumptive cases including HIV + cases.
o Results can be:
− MTB Detected with Rif resistance / Rif sensitivity or Rif indeterminate (positive)
− MTB not detected (negative)
Diagnosing TB

Unit 9: Slide 12
• Bacteriologically
Line probe assays o 2nd line LPA as a follow-on test for Xpert
rifampicin resistance to screen for
resistance to fluoroquinolone and 2nd line
injectables.
o 1st line LPA to confirm resistance to
isoniazid and rifampicin, only when needed
o LPA for MOTT IDTo identify the species
when culture is positive for Mycobacterium
other than MTB.
Mycobacterial culture, when needed
Direct (smear) microscopy
o not routinely provided for diagnosis
o mainly used for confirmed TB cases, at
baseline or follow-up
Diagnosing TB (2)

Unit 9: Slide 13
• Clinically Radiologically
o CXR when − Xpert MTB/RIF is negative, or
− in emergency situations where sputum cannot be produced
− The patient is a symptomatic child being evaluated for TB.
Histopathologically (when required)
Tuberculin skin test (TST) o is useful in supporting the diagnosis of
active TB in young children.
• Other methods TB lateral flow LAM test
o The test may be used to assist in the diagnosis of TB in HIV positive adult in-patients with signs and symptoms of TB (pulmonary and/or extrapulmonary) and
− Who have a CD4 cell count of 100 cells/µl or less, or
− Who are seriously ill regardless of CD4 count.
Diagnosing TB (3)

Unit 9: Slide 14
Treating TB: Summary of anti-TB regimens
National Tuberculosis and Leprosy Programme
Regimen Indication
First line regimen for TB
(2HRZE/4HRE)
New TB patients without rifampicin resistance
Previously treated TB patients without rifampicin
resistance
Standardised DR-TB
regimen
Patients with uncomplicated rifampicin resistant
TB
Individualised DR-TB
regimens
Patients with complicated DR-TB, including
resistance to fluoroquinolone and/or second line
injectables
Unit 9: Slide 15
• Screen all PLHIV routinely for active TB
• Exclude active TB disease before initiating TPT
• It is safe to initiate ART and TPT on the same
day
• PLHIV who are close contacts of patients with
TB should receive TPT even if they have
completed a previous course of TPT.
TPT Considerations

Unit 9: Slide 16
•Signs and symptoms of TB present
• Cough, fever, night sweats, weight loss and loss of
appetite
• NB: TB-TPT should not be given to patients who are
unwell and where there is no explanation of the illness.
•History of:
• active liver disease, liver insufficiency, or jaundice (or);
• hypersensitivity to INH or any other agent used for
TPT, (or);
• exfoliative dermatitis
Contraindications for TPT

Unit 9: Slide 17
• Educate patients on possible side effects before
initiating TPT
• If side effects develop, the patient must stop
taking TPT and report immediately to the
nearest health facility for assessment.
• Health workers should always assess clients for
side effects when they come for refills.
Managing TPT associated side
effects

Unit 9: Slide 18
• Discontinue TPT after serious toxicity.
Isoniazid-induced hepatitis
Peripheral neuropathy
Rifapentine may cause orange/red discoloration
of body fluids.
Skin manifestations e.g. exfoliative demartitis
• Screen for signs/symptoms of active TB at each
visit
• Document adherence in TB-TPT register, ePMS,
patient booklet and stamp in patient passport
TPT Monthly Monitoring

Unit 9: Slide 19
Regimen Duration Considerations
INH Once daily for 6
months (6H)
(NEW)
• TPT is now given for 6 months instead of
9 months
• Patients previously prescribed 9 months
INH and has taken 6 months should be
stopped and considered as completed.
• HCWs should ensure that the outcome is
updated in the ePMS as “TPT Completed
INH and
Rifapentine
Weekly for a total
of 12 doses
(3HP)
INH and
Rifampicin
Daily for 3
months (RH)
• Consult with TB or HIV clinical mentor or
experienced physician
TPT regimens

Unit 9: Slide 20
TPT regimens with ART
ART regimen Preferred
Regimen Alternative
On Efavirenz and Raltegravir
based regimen 6H *3HP (for adults and
children >2 years)
3HR (in children only)
On DTG based regimen and
fully VL suppressed 6H *3HP (for adults and children
>2 years)
3HR (in children only)
On DTG not fully VL
suppressed or no evidence
of suppression
6H
Pregnant women 6H
Children <2 years 6H 3HR
PI based regimen 6H
*3HP should not to be used in; pregnant women, children <2 years, patients who are
on PI containing regimen and, for patients on DTG containing regimen with high VL.
Unit 9: Slide 21
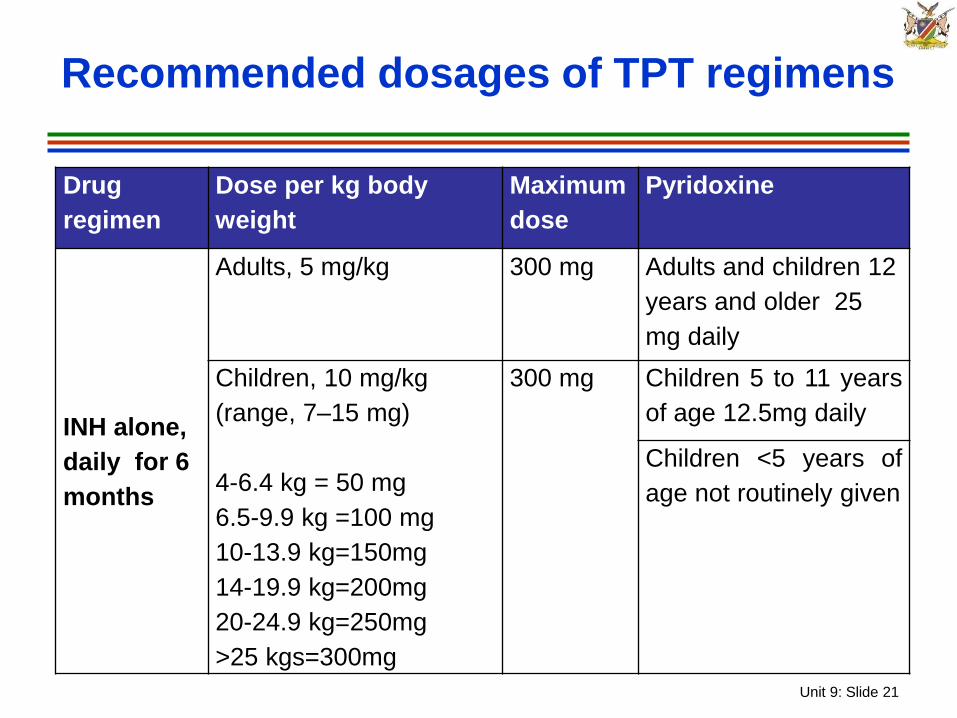
Recommended dosages of TPT regimens
Drug
regimen
Dose per kg body
weight
Maximum
dose
Pyridoxine
INH alone,
daily for 6
months
Adults, 5 mg/kg 300 mg Adults and children 12
years and older 25
mg daily
Children, 10 mg/kg
(range, 7–15 mg)
4-6.4 kg = 50 mg
6.5-9.9 kg =100 mg
10-13.9 kg=150mg
14-19.9 kg=200mg
20-24.9 kg=250mg
>25 kgs=300mg
300 mg Children 5 to 11 years
of age 12.5mg daily
Children <5 years of
age not routinely given

Unit 9: Slide 22
Recommended dosages of TPT
regimens (2)
Drug
regimen
Dose per kg body weight Maximum
dose
Pyridoxine
Weekly
rifapentine
plus INH for
3 months
(12 doses)
Individuals aged ≥ 12 years:
INH: 15 mg/kg
Individuals aged 2–11 years:
INH: 25 mg/kg
Rifapentine: 10.0–14.0 kg
= 300 mg
14.1–25.0 kg = 450 mg
25.1–32.0 kg = 600 mg
32.1–50.0 kg = 750 mg
> 50 kg = 900 mg
INH, 900
mg
Rifapentine,
900 mg
Adults and children 12
years and older 50 mg
daily
Children 5 to 11 years
of age 25mg daily
Children <5 years of
age not routinely given

Unit 9: Slide 23
Recommended dosages of TPT
regimens (3)
Drug
regimen
Dose per kg body
weight
Maximum
dose
Pyridoxine
Daily INH
plus
rifampicin
for 3
months
INH:
Adults, 5 mg/kg
Children, 10 mg/kg
(range, 7–15 mg)
Rifampicin:
Adults, 10 mg/kg
Children, 15 mg/kg
(range, 10–20 mg)
INH, 300 mg
Rifampicin,
600 mg
Adults and children
12 years and older 25
mg daily
Children 5 to 11 years
of age 12.5mg daily
Children <5 years of
age not routinely
given
Unit 9: Slide 24
• PTB is a WHO Clinical Stage 3 disease, while EPTB is Clinical Stage 4:
Individuals with either diagnosis are eligible for ART
If not already on ART, start TB treatment first, followed by ART as soon as possible
ART must be started within 2 - 8 weeks o Do not wait until after 8 weeks!
With profound immunosuppression (e.g. CD4 <50) start ART as soon as possible within first 2 weeks
When to Start ART During TB Therapy in
Adults and Children

Unit 9: Slide 25
• No interaction with NRTI class
• Drug interactions between rifampicin and INSTIs and PIs
• INSTIs class:
Rifampicin lowers DTG levels
o Give twice daily DTG
• Protease inhibitor (PI) considerations:
Rifampicin lowers the blood levels of almost all PIs by up to 80%
Modification of PI dose required if used with rifampicin
Do not use Atazanavir with Rifampicin
TB/HIV Treatment Issues

Unit 9: Slide 26
ART for Adults with Active TB
Preferred 1st line ART
regimen
TDF + FTC (or 3TC) + DTG (at 50mg twice daily)
Alternate 1st line ART
regimen
TDF + FTC (or 3TC) + EFV (at 400mg once daily) (this is a change
from the previous guidance which recommended increasing the dose to
600mg with TB treatment).
For PLHIV on a boosted PI
regimen
Option 1: Substitute rifampicin in the TB treatment with rifabutin
Option 2: If Rifabutin is unavailable or contraindicated, maintain
rifampicin in TB treatment and use PI based regimen super boosted
with ritonavir.*
TDF or AZT + 3TC with LPV/r 400mg+ritonavir 400 mg BD (LPV/RTV)
or (LPV/r 800 +ritonavir 200mg BD)
Note: ATV/r is contraindicated in patients with TB/HIV co-infection
Preferred 1st line
ART regimen
TDF + FTC (or 3TC) + DTG (at 50mg twice daily)
Alternate 1st line
ART regimen
TDF + FTC (or 3TC) + EFV (at 400mg once
daily)
For PLHIV on a
boosted PI
regimen
Option 1: Substitute rifampicin in the TB
treatment with rifabutin
Option 2: If Rifabutin is unavailable or
contraindicated, maintain rifampicin in TB
treatment and use PI based regimen super
boosted with ritonavir.*

Unit 9: Slide 27
Child or adolescent with TB and is
not yet on ART
<4 weeks old • Seek advice
4 weeks to <3
years old or
weight <10
kg
• ABC/3TC + DTG bd
• If DTG not available:
• ABC + 3TC + RAL or
• ABC + 3TC + super-boosted
lopinavir/ritonavir (LPV/r + R)*
• NB: Switch to standard ART regimen two
weeks after competing rifampicin-based
TB treatment

Unit 9: Slide 28
3 years old and
weight 10 kg to
<20 kg
• ABC + 3TC + DTG bd
• NO previous eMTCT/PMTCT NVP exposure:
ABC+ 3TC + EFV
• if DTG not available and the child has had
previous eMTCT/PMTCT NVP exposure:
• ABC + 3TC + RAL
• or
• ABC + 3TC + super-boosted lopinavir/ritonavir
(LPV/r + R) *
• NB: two weeks after TB treatment is completed,
change to the standard ART regimens
Child or adolescent with TB and is
not yet on ART (2)

Unit 9: Slide 29
Child or adolescent with TB and is
not yet on ART (3)
Adolescents 20
to <30 kg
• ABC + 3TC + DTG bd
• if no DTG available,
• And If the child has had NO previous
eMTCT/PMTCT NVP exposure
• ABC+ 3TC + EFV
• ABC + 3TC + RAL (if RAL available)
• ABC + 3TC + super-boosted lopinavir/ritonavir
(LPV/r + R)*
≥30 kg and at
least 10 years
old:
• TDF + 3TC + DTG bd
• If DTG not available, TDF + 3TC + EFV

Unit 9: Slide 30
• Bacteriological confirmation is crucial for TB
diagnosis.
• All PLWA should be screened for TB at every
visit.
• All PLWA with no S/S of TB should receive at
least one course of TPT.
• INH for TPT is now given on the same day as
ART initiation and is only for 6 months.
• A course of TPT should be repeated after TB
treatment or after exposure to TB from a close
contact.
Key Messages

Unit 9: Slide 31
CRYPTOCOCCAL MENINGITIS

Unit 9: Slide 32
Cryptococcal Meningitis
• Clinical presentation:
Occurs most commonly when CD4 < 200
Characterized by subacute meningitis
Acute confusional state
Nausea and vomiting
Stiff neck is absent in 70% of cases
Cranial nerve abnormalities common with
increased intracranial pressure from
communicating hydrocephalus

Unit 9: Slide 33
Cryptococcal Meningitis (2)
• CSF findings:
Clear or turbid appearance
Pressure commonly raised
CSF cell count may be normal or slightly elevated
Protein may be raised
Glucose may be low
CSF India ink yield (75%)
Ask lab to do CSF CrAg if India ink negative
CSF culture is diagnostic (95 – 100%)
• Blood culture may be positive

Unit 9: Slide 34
CSF of Patient with Cryptococcal
Meningitis
CSF India Ink
Source: https://i.pinimg.com/originals/4d/50/3b/4d503b74a7b026f2e9a3a0464c12aa12.jpg

Unit 9: Slide 35
Treatment of Cryptococcal
Meningitis: Induction
• Amphotericin B 1 mg/kg/day (given with pre-
emptive hydration and electrolyte
supplementation)
plus
• Fluconazole 1,200mg daily for adults and
12mg/kg daily (up to maximum of 800mg daily)
for children and adolescents 2 weeks in hospital
Source: WHO Rapid Advice, Diagnosis, Prevention and Management of Cryotococcal
Diseases in Adults, Adolescents and Children, December 2011.

Unit 9: Slide 36
Treatment of Cryptococcal
Meningitis (2)
• Consolidation:
Fluconazole 800 mg daily for adults and 6-12mg/kg daily (maximum 800mg daily) for children and adolescents 2 months
• Maintenance (secondary prophylaxis):
Then 200 mg daily for adults and 6mg/kg daily for children and adolescents.
• Continue Fluconazole for minimum 1 year in total and discontinue when patient has had 2 CD4 counts > 200 cells/mm3 taken at least 6 months apart

Unit 9: Slide 37
RENAL INSUFFICIENCY

Unit 9: Slide 38
• Causes of renal insufficiency among HIV positive patients, e.g.:
Acute:
o Dehydration
o Malaria
o Heart failure
Chronic:
o HIV-associated nephropathy
o Hypertension
o Diabetes
o Renal Artery Stenosis
Renal Insufficiency and HIV

Unit 9: Slide 39
• Prior to starting ART
Calculate estimated creatinine clearance (CrCl)
Adjust ART dosage as needed if alternatives are
not available
• For patients on TDF, monitor:
CrCl at week 6, month 6 and12 then every 12
months thereafter
o Monitor at least once every month in patients with
chronic renal insufficiency
Renal Insufficiency and ART

Unit 9: Slide 40
• Formula for calculation of CrCl in adults uses the
patient’s age, weight and serum creatinine:
(140-age) x weight (kg) x 1,22 serum creatinine (μmol/l)
For women, multiply above result by 0.85
Calculation of CrCl in adults

Unit 9: Slide 41
• CrCl calculation for adults is not applicable to
children < 18 years old, use Schwartz equation
• It uses child’s length/height and serum
creatinine:
length (cm) x k x 88.4 serum creatinine (μmol/l)
k = 0.45 for infants 1 - 52 weeks
k = 0.55 for children 1 - 13 years old
k = 0.55 for adolescent females 13 - 18 years
k = 0.7 for adolescent males 13 – 18 years
SCHWARTZ Equation for Children
Source: Schwartz, GL et. al. A simple estimate of glomerular filtration rate in children
derived from body length and plasma creatinine. Pediatrics 1976, 58:259-263

Unit 9: Slide 42
• NRTIs (except Abacavir)
Excreted through the kidneys
Require dosage reduction in renal impairment
TAF given in CrCl 30 -50 without dose adjustments
• NNRTIs and PIs are
Excreted through the liver
No dosage adjustment needed
• Cotrimoxazole:
Can also cause nephrotoxicity
Require Dosage Adjustment
o CrCl is 15-30 ml/minute decrease CTX dose by 50%
o < 15ml/min do not give CTX
Dosage Adjustment of Meds in Renal
Insufficiency

Unit 9: Slide 43
Dosage Adjustment of TDF/TAF in Renal
Insufficiency
Creatinine
Clearance
(ml/min)
Recommended Dosing of
TDF 300 mg
Dosing of
TAF/FTC/DTG
≥50 Every 24 hours Every 24 hours
30-49 Every 48 hours Every 24 hours
10-29 Twice a week Not recommended
< 10 No recommendation available
owing to a lack of
pharmacokinetic data in this
population
Haemodialysis
patients
Every 7 days or after a total of 12
hours of dialysis (administer
following completion of dialysis)

Unit 9: Slide 44
IMMUNE RECONSTITUTION
INFLAMMATORY SYNDROME (IRIS)

Unit 9: Slide 45
• A dramatic increase in the inflammatory
response to antigens from previous, partially
treated or latent infections in HIV patients shortly
after initiating ART
• It usually occurs in the first few weeks after a
patient starts therapy
Immune Reconstitution
Inflammatory Syndrome (IRIS)

Unit 9: Slide 46
• Common risk factors for IRIS;
Rapid decline in viral load (especially in the first
three months after ART initiation)
Low baseline CD4 count (especially <50
cells/mm3) and rapid increase after initiating ART
Initiation of ART soon after initiation of treatment
for opportunistic infection (OI)
Disseminated versus localized OI
ART-naïve patient
IRIS (2)

Unit 9: Slide 47
• Although patients with IRIS appear as though ART is failing (clinical deterioration), these patients are actually undergoing robust improvements in their immune systems
• Examples of infections or conditions which have been associated with IRIS:
Tuberculosis
MAC
Cryptococcal meningitis
Herpes zoster
Kaposi Sarcoma
IRIS (3)

Unit 9: Slide 48
NON-COMMUNICABLE
DISEASES

Unit 9: Slide 49
• These diseases include hypertension, diabetes
mellitus, and ischaemic and rheumatic valvular
heart disease.
• Cardiovascular conditions particularly
pericarditis and dilated cardiomyopathies may
be HIV, OI, or medication-related.
• Some ARVs, especially PIs, may cause
hypercholesterolemia and in the long term could
result in premature onset of coronary artery
disease or stroke.
Cardiovascular Diseases
Unit 9: Slide 50
• Increased vasculitic events have been noted
in HIV patients leading to strokes, peripheral
arterial occlusions and other vaso-occlusive
events.
• Risk reduction for cardiovascular diseases by:
Weight measurements and BMI
Blood pressure
Blood glucose levels every 6 months for those at
risk
Blood cholesterol every year
Cardiovascular Diseases (2)

Unit 9: Slide 51
• PLHIV are at high risk of mental, neurological
and substance-use disorders
• Depression is one of the commonest mental
health problems among PLHIV including
adolescents LHIV
• Screen for all patients with poor adherence and
high viral load for depression
• Use the PHQ – 9 – Refer to Handout 9.2
Depression

Unit 9: Slide 52
FAMILY PLANNING

Unit 9: Slide 53
WHO medical eligibility criteria
categories for contraceptives .
Medical eligibility Description criteria category Use of medical eligibility criteria categories in clinical practice
With clinical judgement With limited clinical judgement
1 A condition for which there is no
restriction for the use of the
contraceptive method
Use method in any circumstances Yes
(use the method)
2 A condition in which the advantages
for using the method generally
outweigh the theoretical or proven
risks
Generally use the method; some follow-
up may be needed
3 A condition in which the theoretical or
proven risks usually outweigh the
advantages of using the method
Use of the method not usually
recommended unless other more
appropriate methods are not available
or not acceptable; clinical judgement
and continuing access to clinical
services are required for use
No
(do not use the method)
4 A condition that represents an
unacceptable health risk if the
contraceptive method is used
The method should not be used

Unit 9: Slide 54
WHO MEDICAL ELIGIBILITY CRITERIA CATEGORY SUMMARY TABLE FOR
CONTRACEPTION, ARV DRUGS AND TB MEDICATIONS.
CHC a POP DMPA/ NET-
EN LNG/ETG
implants
LNG-IUD
initiation
LNG-IUD
continuation
NRTIs
ABC, TDF, AZT, 3TC, ddI, FTC, d4T 1 1 1 1 2/3b 2
NNRTIs
EFV, NVP 2 2 1 2 2/3b 2
EFV, rilpivirine 1 1 1 1 2/3b 2
Protease inhibitors (PIs)
ATV/r, LPV/r, DRV/r, RTV 2 2 1 2 2/3b 2
Integrase inhibitors
Raltegravir 1 1 1 1 2/3b 2
TB medications
Rifampicin or rifabutin c 3d 3 DMPA=1
NET-EN=2 2 1 1
a. CHC: Combined Hormonal contraceptive includes the combined oral contraceptive pill, the combined
contraceptive vaginal ring, the combined contraceptive patch and the CIC.
b. No drug–drug interactions but depends on clinical disease status.
c. 3HP and 1HP used for TB preventive therapy contain rifapentine.
d. CIC is WHO medical eligibility criterion 2 for concomitant rifampicin or rifabutin therapy

Unit 9: Slide 55
Woman centered approach !!!!
• Comprehensive counselling and informed choice should
be provided to women and adolescent girls in making
decisions about a contraceptive method that suits their life
stage and fertility intentions.
• At all times, the decision must be based on: the client’s
values, needs and preferences and the medical eligibility
for the contraceptive options for that particular client
Unit 9: Slide 56
Contraception Recommendations for
PLHIV
• Dual protection should be encouraged:
Correct and consistent use of condoms with another
contraceptive method
ARTs be can safely used COCs, progestin-only pills,
injectables and IUCD
o Minimum of 30mcg ethinyl estradiol when COC is
chosen
• PLHIV who are clinically well, can safely undergo
voluntary male vasectomy or female sterilization

Unit 9: Slide 57
Contraception Recommendations for
PLHIV
Hormonal methods
Intrauterine Device
(IUD)
Intrauterine Contraceptive Device
(IUCDs)
Progestin only
Methods
Progesterone Only Injectables (POIs)
Contraceptive Implants
Progestin Only Pills (POPs)
Combined hormonal
contraceptives
Combined Oral Contraceptives
Combined Contraceptive Patch

Unit 9: Slide 58
Contraception Recommendations
for PLHIV (2)
Non hormonal methods
Intrauterine Device (IUD) Copper IUD
Sterilization (Voluntary
Surgical Contraception)
Vasectomy (Male Sterilization)
Bilateral Tubal Ligation (Femalesterilization)
Non-hormonal methods
(barrier methods)
Male Condom
Female Condom
Natural Family Planning
(NFP) Methods
Abstinence
Coitus Interruptus/ Withdrawal
Lactational Amenorrhea Method (LAM)
Fertility Awareness Methods (FAM)

Unit 9: Slide 59
• NNRTIs and PIs decrease the therapeutic levels
of estrogen:
However, no clinical outcomes of increased
pregnancy rates have been documented
• Depo medoxyprogesterone has no known drug
interactions with ARVs:
Counsel patients about amenorrhea
• Note: Estrogen levels decreased by rifampicin
for TB patients
Contraceptives: Drug-Drug Interactions

Unit 9: Slide 60
DTG and hormonal contraceptive
• No reported or expected drug–drug interactions that would reduce the effectiveness of the hormonal contraceptive methods,
• Pharmacokinetic and other data are limited.
• DTG can likely be used with the full range of contraceptive methods without compromising their effectiveness.
• The WHO medical eligibility criteria do not provide specific recommendations for DTG and hormonal contraception.
• USA, The United States medical eligibility criterion 1 (medical eligibility criteria for the United States from 2016).
Unit 9: Slide 61
NUTRITION

Unit 9: Slide 62
• Always promote and encourage optimal nutrition intake with a variety of foods every day.
• Discuss ART and food interactions with the client before they begin treatment.
• Use the Food and Medication Intake Form to assist in counselling the client on the importance of food intake with ART.
• Identify medications that have special food interactions
• Identify potential nutrition-related side-effects with ART and provide counselling on management of side-effects.
• Promote and encourage optimal nutrition as part of HIV care.
Nutrition

Unit 9: Slide 63
• Traditional therapies and remedies for PLHIV should
be discouraged.
• Considerations when discussing supplements with
clients should include:
Multi-vitamins should be used as prescribed by a
health worker.
• Other supplements including traditional herbs and
remedies that claim to boost the immune system or
cure disease should be discouraged as they have
potential adverse medicine interactions with ARVs.
Nutrition (2)

Unit 9: Slide 64
• HIV positive patients are susceptible to
developing OIs such as TB, cryptococcol
meningitis, Hep B and PJP.
• PLHIV must be assessed and prophylaxis and
treatment be given appropriately
• Several ARVs are affected when renal function
is impaired
Dose adjustment may be required
• Family planning should be considered and
integrated in HIV care and management
Key Points


















