Unilateral Spatial Neglect. Unilateral Neglect Characterised by a failure to attend, respond or...
26
Unilateral Spatial Neglect
-
Upload
sydney-morris -
Category
Documents
-
view
235 -
download
0
Transcript of Unilateral Spatial Neglect. Unilateral Neglect Characterised by a failure to attend, respond or...

Unilateral Spatial Neglect


Unilateral Neglect Characterised by a failure to attend, respond or orient to a stimulus or side
opposite the lesion which is not referrable to a sensory or motor deficit
May extend to all sensory modalities i.e. neglect of visual, auditory and somatosensory stimuli on the side of the body and/or space opposite the lesion
When asked to draw a picture, bisect a line or read they perform as if one half of the object, line or word does not exist
Patient is often unaware of the deficit
Most commonly reported following a posterior parietal lesion of the right hemisphere
May also be seen following right frontal lesions and lesions of the cingulate gyrus or of the thalamus and basal ganglia


Clinical Presentation
Commonly seen after stroke or in association with a tumour
Often transient with the most conspicuous features in many cases lasting no more than a few weeks
Often seen in association with sensori-motor deficits including VFD’s and hemiparesis
Most cases of severe and persisting neglect involve RH lesions
Studies of unselected cases (ie including those with aphasia) consistently demonstrate that left visual neglect is more frequent and severe (RH damage) than right visual neglect (LH damage)
Incidence:
Figures vary:40-45% following RH CVA15% following LH CVA
NB. May be task specific eg., evident in reading but not drawing

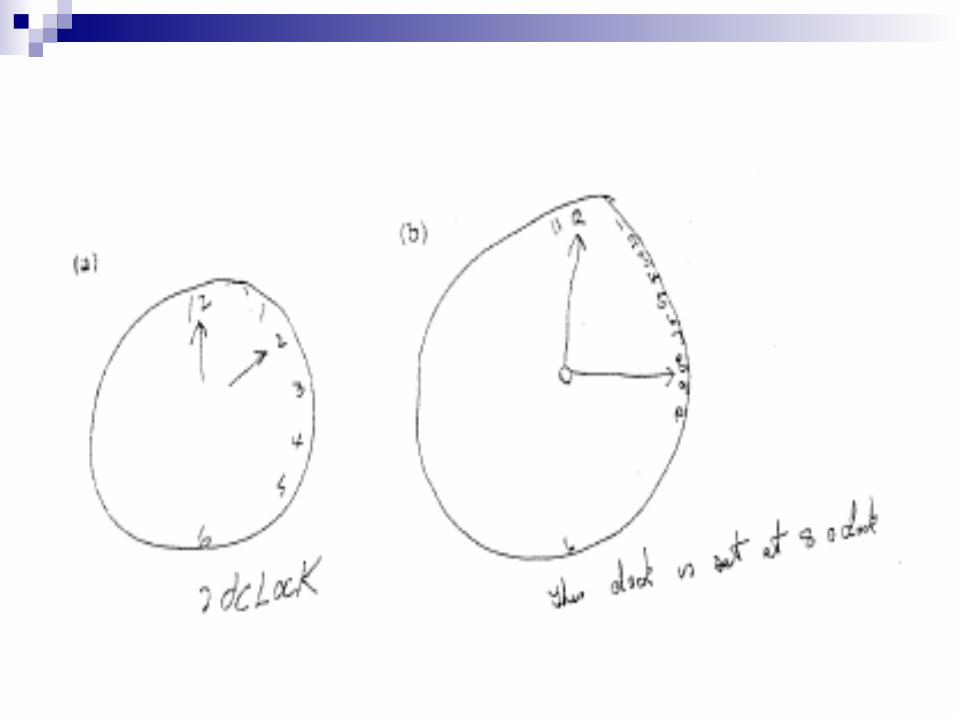
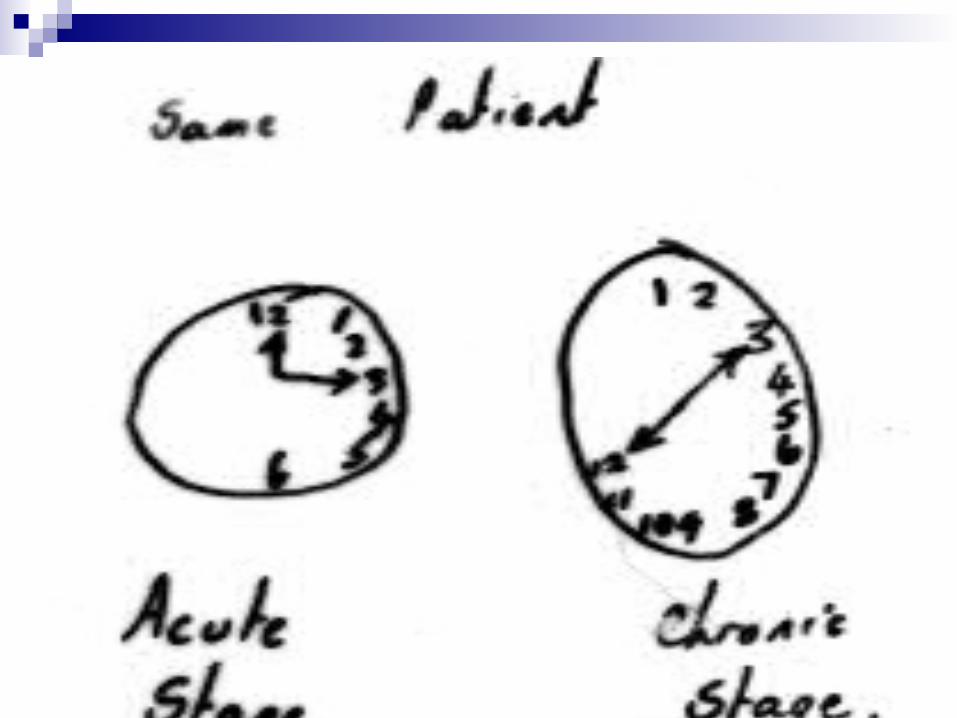
Severe forms of neglect- Asked to lift arms: will lift only one- Asked to draw a clock face: reproduce only half or
crowd all numbers into one side- Asked to read a compound word such as ice-cream or
football: read cream and ball- Dressing: May fail to put on left side of clothes- Grooming: Shave or apply makeup to only one side of
the face- Unaware that anything is wrong (anosognosia)


Acute stages of a unilateral spatial neglectMost severe signs seen in the acute stages of CVA – neglect
of the half of space contralateral to the lesion
Patients attention systematically orients towards stimuli lying on the extreme part of the non-neglected side: May eat from only one side of the plate, neglect to lock the wheelchair on the left
May be characterised by marked deviation of head, eyes and trunk away from the contralesional field.
Acute stages (con’t)
Test visual fields:The very placement of one’s hand to the patient’s right renders him unable to maintain central fixation.
Known as ‘compulsive orientation’ to the right
Scanning scacades restricted to the ipsilesional side although pt may have full ocular movement to command
In severe cases patients may fail to recognise contralateral extremities as their own
May experience difficulty in remembering left sided details of internally represented familiar scenes

Acute stages (con’t)
Thus, impaired perception, action and mental representation of the contralesional half of space
Most striking signs resolve quite rapidly
With appropriate testing may see residual signs


Unilateral Spatial Neglect – Later stages Extinction to Double Simultaneous Stimulation
Patient asked to fix gaze. Test visual fields by presentation of a single stimulus on one side. Do the same on the other. Patients fields will be ‘Full to Confrontation’ i.e., detection appears normal in both the left and the right visual fields (cf with hemianopic pt)
When two objects are presented at the same time, one in each field, only one of the stimuli is reported – ‘Extinction to Double Simultaneous Stimulation’.

Unilateral Spatial Neglect – Testing
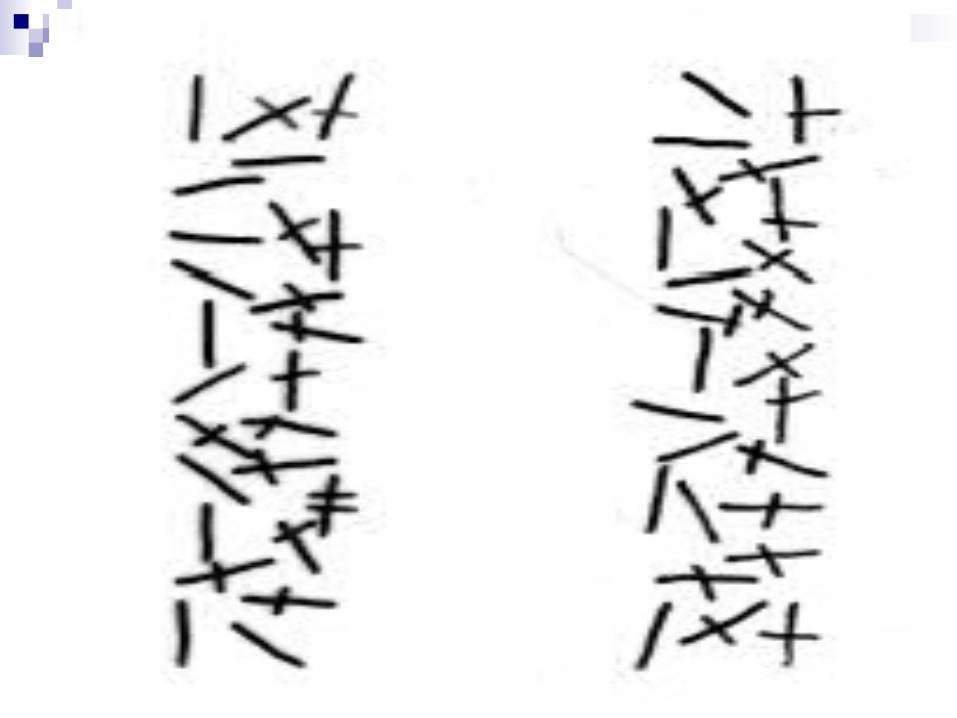
Spatial and exploratory tasks (eg. pattern crossing, line bisection)
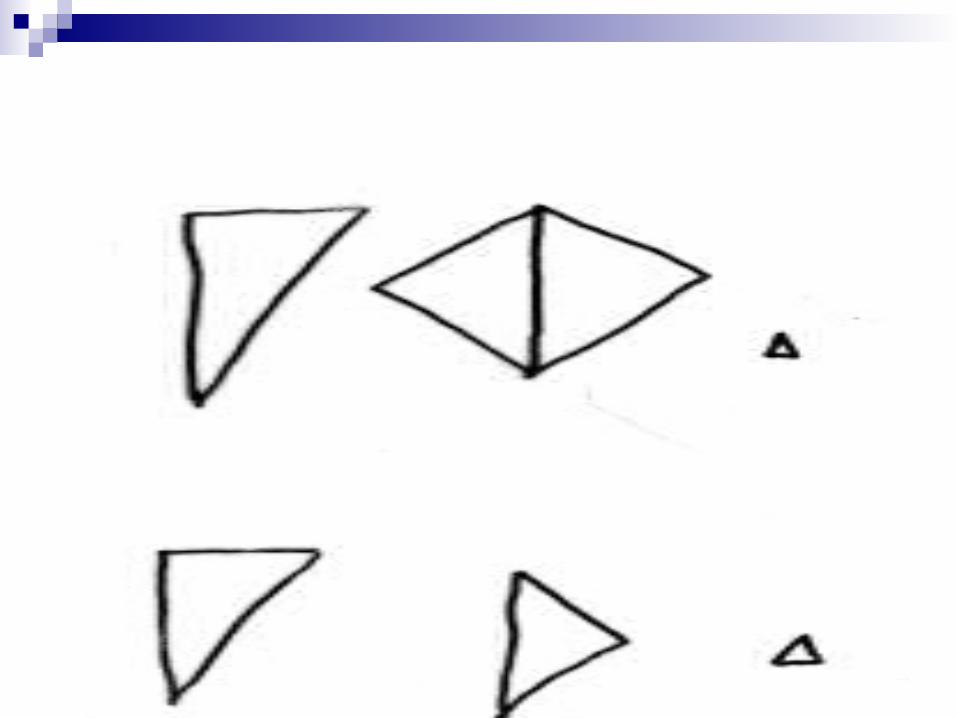
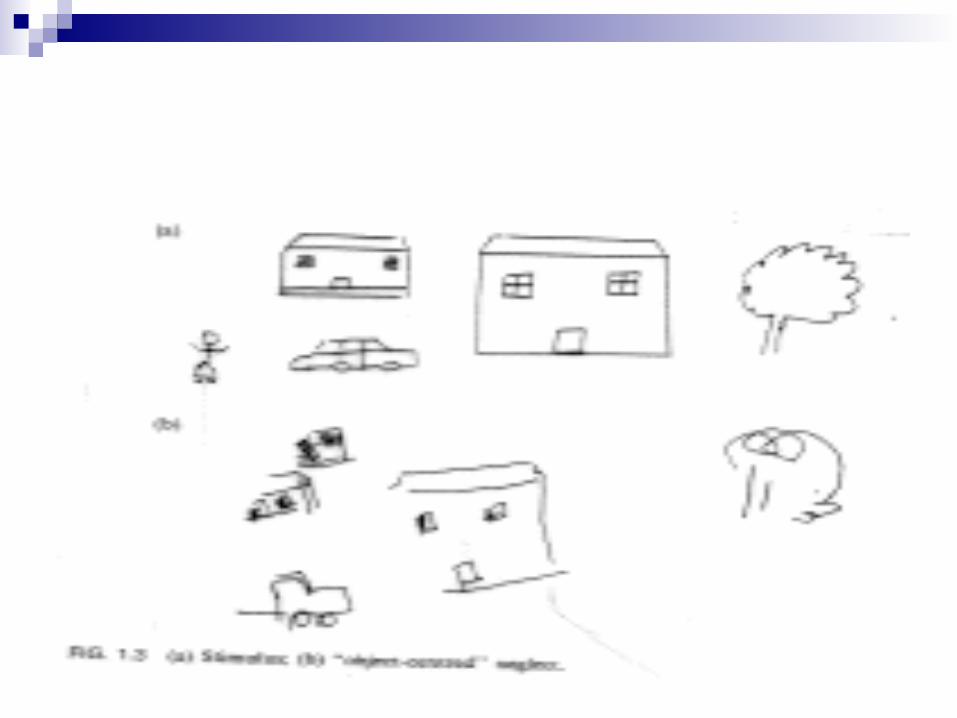
Copying tasks Drawing from memory even of objects with will known
symmetrical configuration Object centred neglect – neglect left side of the figure
although then reproduce the right side of a figure that is further to the left
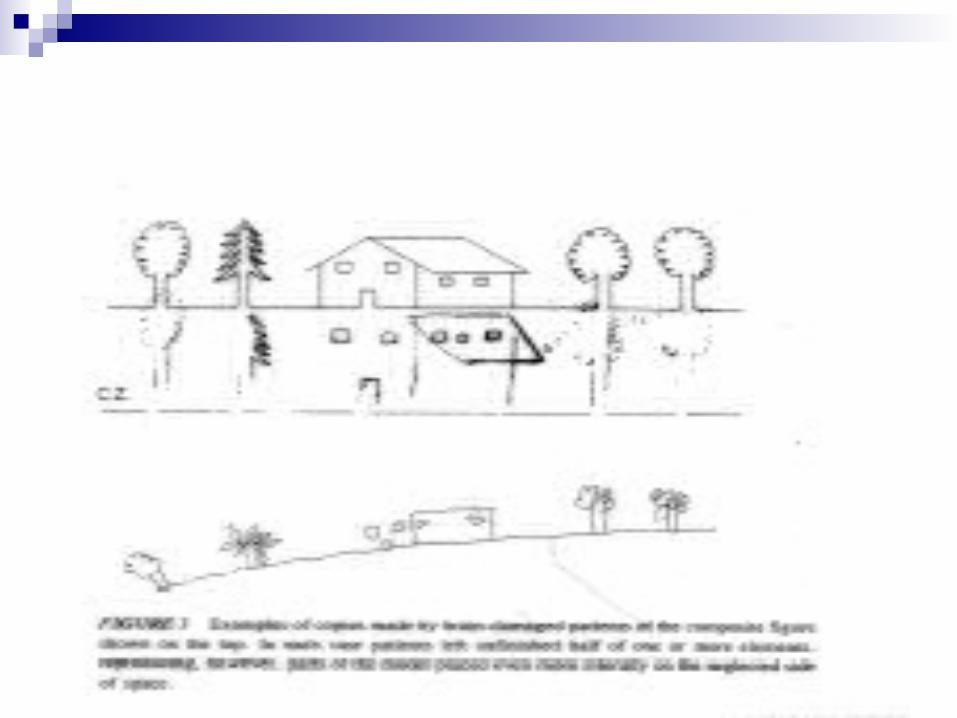
Reading Multiple-choice tasks Description of a scene

Left Brain Damage
Stimuli ResponseLate LaterTruth TruckArm ArmyStop SteamSouth SoupForest ForgiveHealth HeavenModern ModestUnless UncleanFarmhouse Farmyard

Right Brain Damage
Stimuli ResponseBoat CoatCage AgeBook LookFarm HarmWeed NeedChair HairBelief GriefTheory GloryTreason ReasonClimb Limb


PS a 49 yo woman sustained a subarachnoid haemorrhage, confirmed by CT scan and angiography, from an aneurism at the bifurcation of the basilar artery. On neuropsychological testing the only finding of note was florid left neglect. Presented in free vision with arrays of simple figures to cancel, PS crossed out the stimuli on the right-hand side of the page, neglecting all those on the left. Requested to bisect horizontally-oriented lines, she typically placed her transections over 50% to the right of true centre. When copying simple line drawings and when drawing from memory, PS made accurate representations of the right side of the object but omitted the left side without any ‘conscious’ awareness that the drawing was inadequate.
On reading individual words PS would frequently omit or substitute the leftmost letters (simile read as mile; façade as arcade). On traditional criteria PS manifested prototypical left visuospatial neglect.

Of particular interest, when PS was presented simultaneously with two line drawings of a house (one having the left side on fire) she judged the houses were identical.
When asked to select which house she would prefer to live in, she reliably chose the house that was not burning.