Unilateral pleural effusion in liver cirrhosis, congestive heart failure and nephrotic syndrome
22
-
Upload
gamal-agmy -
Category
Health & Medicine
-
view
709 -
download
0
Transcript of Unilateral pleural effusion in liver cirrhosis, congestive heart failure and nephrotic syndrome


Unilateral Left Pleural Effusion among Patients
with Liver Cirrhosis ,Congestive Heart Failure and
Nephrotic Syndrome
Gamal Rabie Agmy, MD, FCCP
Professor of Chest Diseases, Assiut University

Distinguishing an exudate from a
transudate is the first step in the
diagnostic approach of a patient
with pleural effusion.
Introduction

This study included 320 patient with
congestive heart failure, 214 with liver
cirrhosis and 94 with nephrotic
syndrome. All patients had pleural
effusion. Out of these, 35 patients with
congestive heart failure, 38 with liver
cirrhosis and 24 with nephrotic
syndrome had unilateral left sided
pleural effusion. .
Patients and Methods

All patients were subjected to:
1-Detailed history taking.
2-Complete clinical examination.
3-Chest X-ray both posteroanterior and
lateral views.
4-Chest and abdominal sonography.
Patients and Methods

5-Diagnostic thoracentesis
6-Serum sample:
7-All investigations for detection of aetiology of pleural effusions among cases suspected to have exudative effusion.
Patients and Methods

The criteria analyzed for discrimination
between transudates and exudates were: 1-Classical, Abbreviated and modified Light’s
criteria.
2-Pleural fluid cholesterol.
3-P/S cholesterol ratio.
4-Pleural cholinesterase.
5-P/S cholinesterase ratio.
6-P/S bilirubin ratio.
7-Serum-pleural albumin gradient (SPAG).

Table1:Type and side of pleural effusion among patients with
congestive heart failure during the period of this study
Type of effusion
Congestive heart failure No of %
patients Right Left Bilateral
Transudative 130 (40.6%) 3 (0.9%) 82(25.6%) 215 67.1%
Exudative 56 (17.5%) 32 (10%) 17(5.4%) 105 32.9%
Total no of %
patients
186 (58%) 35 (11%) 99(31%) 320 100%

Table2:Type and side of pleural effusion among patients with
liver cirrhosis during the course of this study
Type of effusion
Liver cirrhosis No of %
patients
Right Left Bilateral
Transudative 110(51.4%) 4(1.9%) 35(16.4%) 149 69.6%
Exudative 17(7.9%) 34(15.9%) 14(6.5%) 65 30.4%
Total no of
patients (%)
127(59.3%) 38(17.8) 49(22.9%) 214 100%

Table3:Type and side of pleural effusion among cases with
nephrotic syndrome during the period of this work
Type of effusion
Nephrotic syndrome No of %
Patients
Right Left Bilateral
Transudative 22 (23.4%) 2 (2.1%) 40 (42.6%) 64 68.1%
Exudative 8 (8.5%) 22 (23.4%) 0 (0%) 30 31.9%
Total no of %
patients
30 (31.9%) 24 (25.5) 40 (42.6%) 94 100%

Aims of the Work and Results
The first objective was:
1-to assess the diagnostic value of
the new biochemical criteria
proposed to discriminate pleural
transudates from exudates.

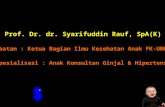
Figure1:Sensitivity, specificity and accuracy of different
biochemical parameters in identifying exudates:
0 20 40 60 80 100 120
Light criteria
SPAG
Clolesterol ratio
Cholinesterase ratio
Bilirubin ratio
Sensitivity Specificty Accuracy

2-to evaluate the effect of diuretic
therapy on different biochemical
parameters among transudative
pleural effusion.
The second Aim

Diuretics had a significant action on
light’s criteria that leaded to
misclassification of trasudates into
pseudoexudates in 50 cases of congestive
heart failure,44 cases of liver cirrhosis and
30 cases of nephrotic syndrome. On the
other hand, diuretics had insignificant
action on other parameters.

The Third Aim
3- to identify the aetiology of left
exudative pleural effusion among
patients with liver cirrhosis, heart
failure and nephrotic syndrome.

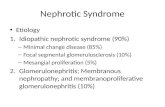
Figure2:Etiology of unilateral left pleural effusion
among cases of congestive heart failure:
0 10 20 30 40 50 60 70
Transudative effusion
Pulmonary embolism
Pneumonia
Malignancy
Collagen disease

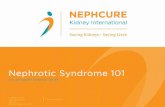
Figure3:Etiology of unilateral left pleural
effusion among patients with liver cirrhosis:
0 10 20 30 40 50 60
Transudative effusion
Tuberculosis
Malignancy
Pneumonia
Collagen disease

Figure 4:Etiology of unilateral left pleural
effusion among patients with nephrotic
syndrome:
0 10 20 30 40
Transudative effusion
pulmonary embolism
Pneumonia
Malignancy
Tuberculosis

Conclusions 1-SPAG is the most sensitive and
specific parameter in separation
between exudates and transudates.
2-Light’s criteria should not be used
for differentiation between exudates
and transudates in patients under
diuretic therapy.

3-Classical , abbreviated and modified Light’s
criteria have the same sensitivity and
specificity in segregating exudates from
transudates.
4-Cholinesterase had a poor diagnostic yield
in detection of transudates in liver cirrhosis.
5-Unilateral left trasudative pleural effusion is
rare among cases of congestive heart failure,
liver cirrhosis and nephrotic syndrome.

6-The most common cause for unilateral left
exudative pleural effusion is pulmonary
embolism among cases of congestive heart failure
and nephrotic syndrome, while, TB is the major
contributory disease in liver cirrhosis.
7-Ultrasonography is more sensitive in detection of
pleural effusion than plain chest radiograph
especially in small sized and subpulmonic
effusions.