Understanding PP and treatment of HypoPP Biannual Meeting of the PPA Orlando, FL, 2011 Frank...
19
Understanding PP and treatment of HypoPP Biannual Meeting of the PPA Orlando, FL, 2011 Frank Lehmann-Horn, Senior Research Professor
-
Upload
reece-govier -
Category
Documents
-
view
214 -
download
0
Transcript of Understanding PP and treatment of HypoPP Biannual Meeting of the PPA Orlando, FL, 2011 Frank...
Understanding PPand
treatment of HypoPP
Biannual Meeting of the PPA Orlando, FL, 2011
Frank Lehmann-Horn, Senior Research Professor

Electrical potentials P of skeletal muscle fibers
P-values around -83 mV are most frequent (P1)
Second fraction around -60 mV (P2)
P is about 1/100 of the voltage of a car battery
K+ Battery
P1
-90 -80 -70 -60 (mV)
P2
Dis
trib
utio
n fr
eque
ncy
%

Muscle strength dependent on resting potential P
Muscle fibers
-90mV
-73 mV
-65 mV
-55 mVDepolarized fibers can´t develop force
Simple basis of PP weakness:Many fibers are episodically or permanently in the P2-state

prevalence: 1:100,000; dominant transmission
onset of disease: childhood or puberty
clinical features: weakness episodes (at younger age) and/orpermanent weakness, a progressive myopathy
weakness episodes: up to daily for several hours
Provocative factors: carbohydrates, sodium, resting periods after exercise, mental stress, cooling, fever, cortisol induce a drop in serum potassium
between episodes: blood potassium is normal
etiology: voltage sensor mutations (Na+, Ca2+ channels)
Hypokalemic Periodic Paralysis (HypoPP)
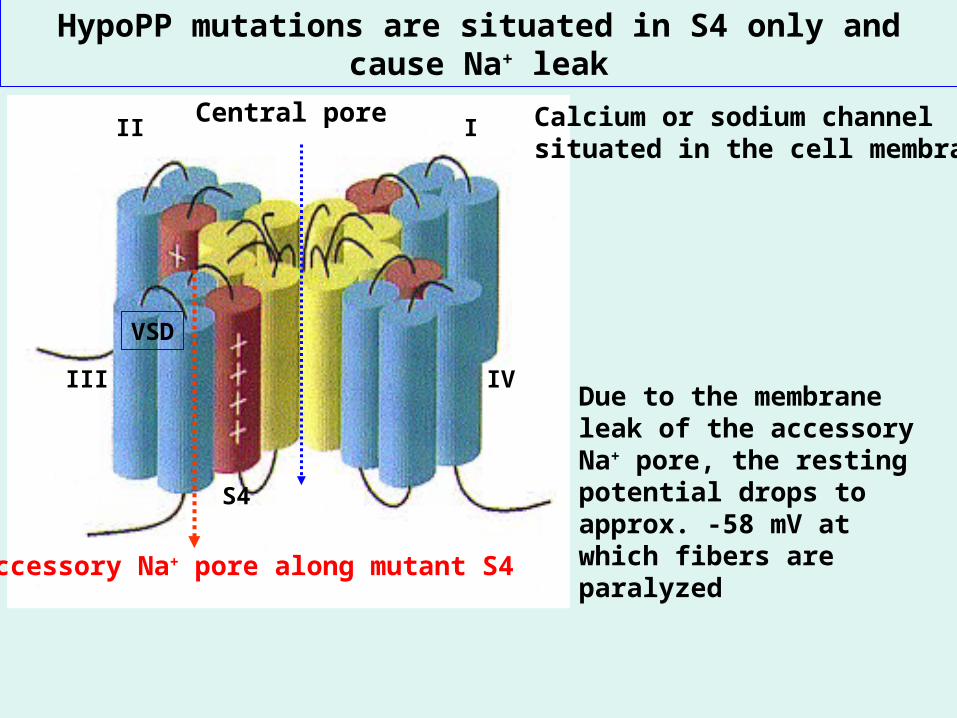
HypoPP mutations are situated in S4 only and cause Na+ leak
Due to the membrane leak of the accessory Na+ pore, the resting potential drops to approx. -58 mV at which fibers are paralyzed
VSD
III
III IV
Central pore
Accessory Na+ pore along mutant S4
S4
Calcium or sodium channelsituated in the cell membrane

Weak after carb-rich meal
-90 -80 -70 -60 -50 -400.00
0.04
0.08pr
obab
ility
den
sity
(m
V-1)
Em (mV)
P1
P2
P2
P1
-110 -100 -90 -80 -70 -60 -500.00
0.01
0.02
0.03
0.04
0.05
0.06
0.07
Em /mvUsually strongP2-fraction explains full-blown attack
hypokalemia opens Na+ pore

Periodic paralysis: permanent weakness
large P2-fraction explains perma-nent weakness
-90 -80 -70 -60 (mV)
P1
P2
Does the accessory pore really con-duct Na+? More Na+ in the fibers?

HypoPP with permanent weakness: dystrophy, edema and intracellular Na+ accumulation
1H-T1 23Na-IR1H-T2-STIR
NaCl solution
NaCl inagarose
Novel technique: 23Na-MRI IRControl: low muscle Na+
i content

P1
P2
-90 -80 -70 -60 (mV)
P1
P2
-90 -80 -70 -60
VolunteerStrength improved
by K+ and AA or CAI
(mV)-90 -80 -70 -60 (mV)
P1
P2
permanent weakness (large P2-fraction)
Therapy: shifting fibers from the P2- to the P1-state
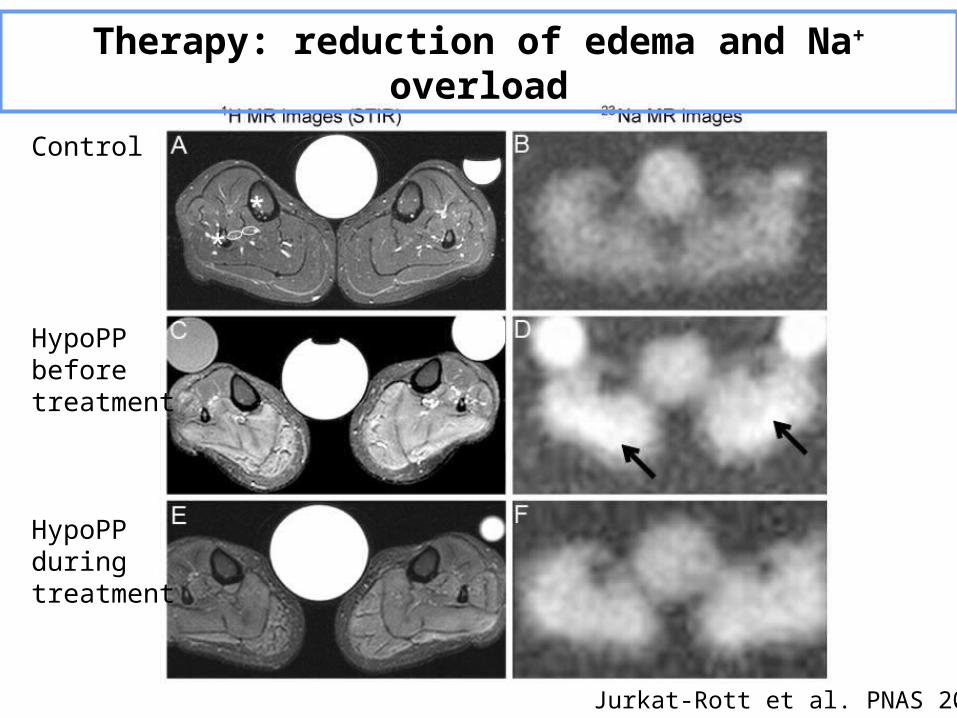
control
untreated patient
Control
HypoPP before treatment
HypoPP during treatment
Jurkat-Rott et al. PNAS 2009
Therapy: reduction of edema and Na+ overload

Therapy also increases muscle strength
0,9
1
1,1
1,2
1,3
1,4
1,5
1,6
17 22 27 32
Na+ / mM
rela
tive
str
eng
th in
crea
se p
ost
/pre
tre
atm
ent
after therapy (acetazolamide)
before therapy
Jurkat-Rott et al. PNAS 2009

After 6 months of therapybefore therapy
Response to an aldosterone antagonist
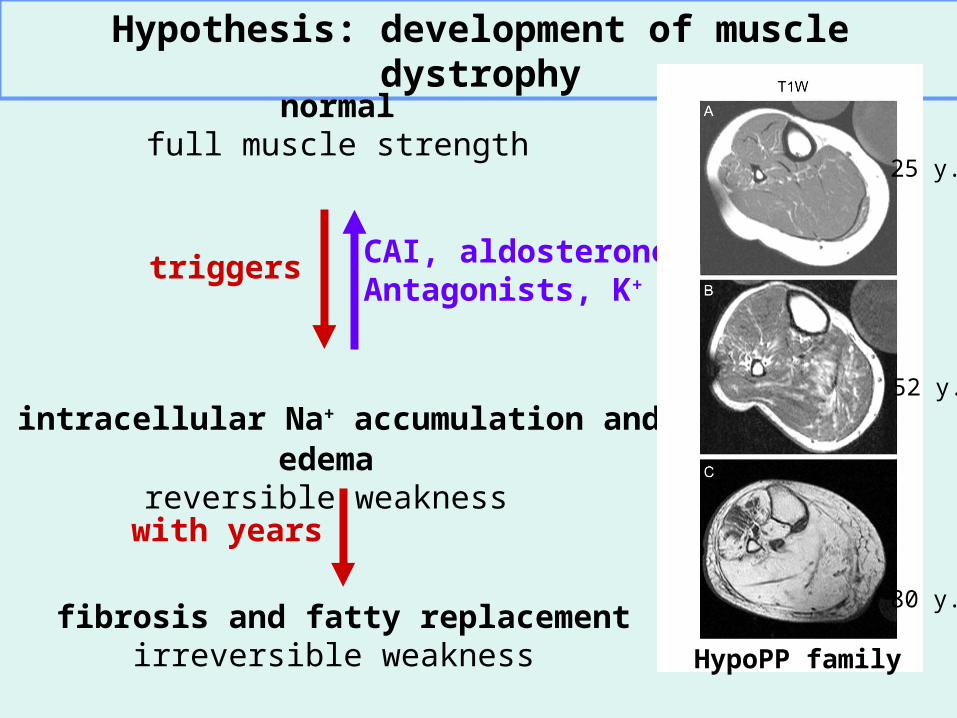
Hypothesis: development of muscle dystrophy
normalfull muscle strength
intracellular Na+ accumulation and edemareversible weakness
fibrosis and fatty replacementirreversible weakness
triggers CAI, aldosterone Antagonists, K+
25 y.
52 y.
80 y.
HypoPP family
with years
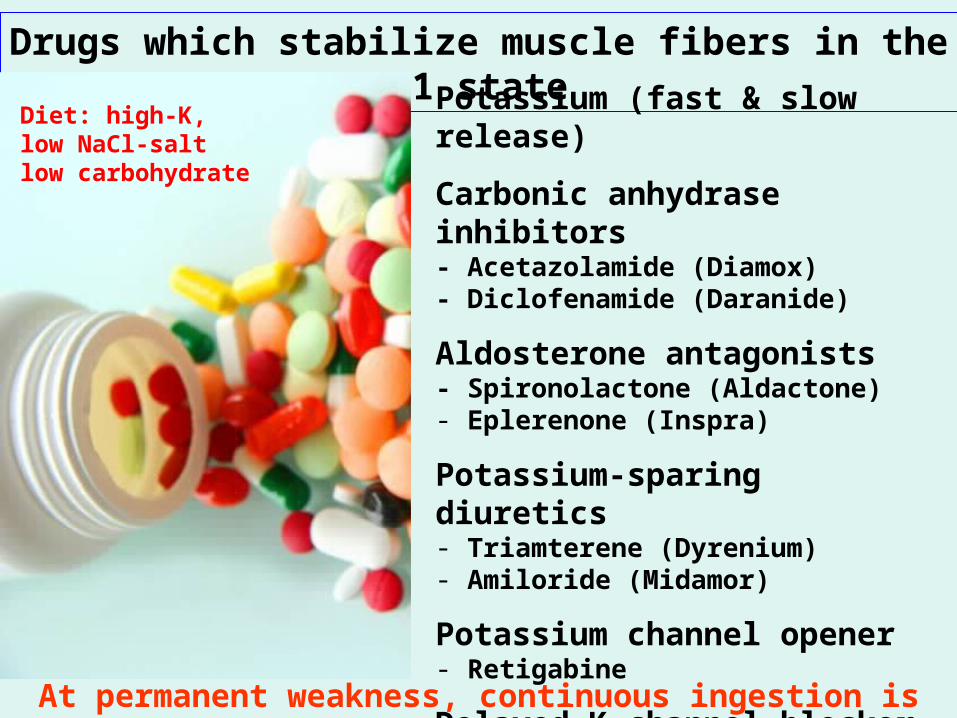
Drugs which stabilize muscle fibers in the P1 state
Potassium (fast & slow release)
Carbonic anhydrase inhibitors- Acetazolamide (Diamox)- Diclofenamide (Daranide)
Aldosterone antagonists- Spironolactone (Aldactone)- Eplerenone (Inspra)
Potassium-sparing diuretics- Triamterene (Dyrenium)- Amiloride (Midamor)
Potassium channel opener- Retigabine
Delayed K-channel blocker- 3,4-diaminopyridine; 3,4-DAP
At permanent weakness, continuous ingestion is required
Diet: high-K, low NaCl-saltlow carbohydrate
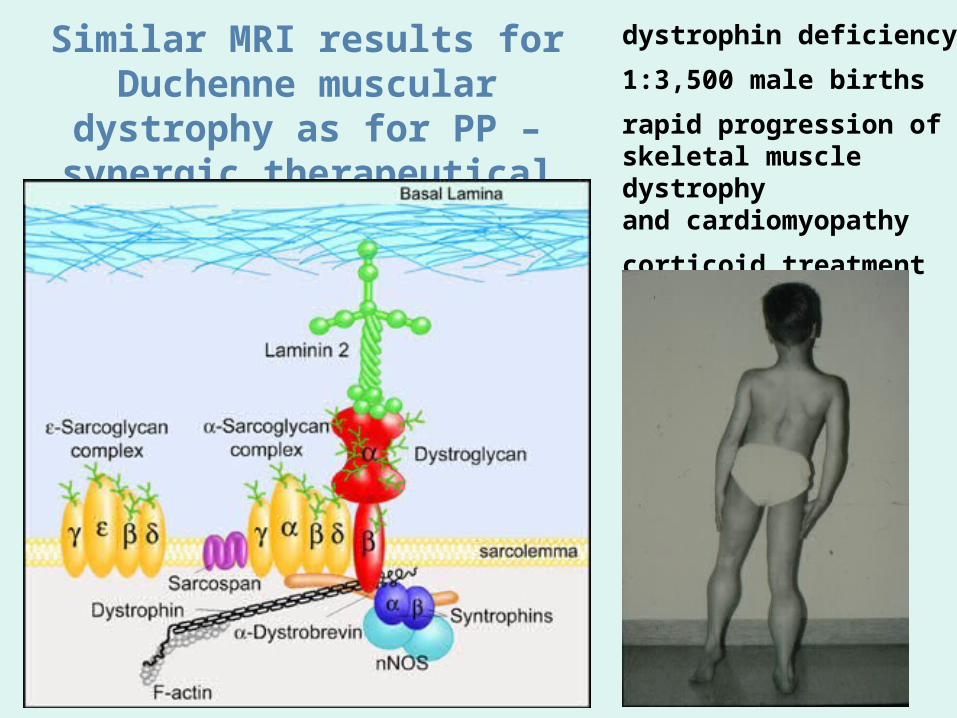
Similar MRI results for Duchenne muscular dystrophy as for PP – synergic therapeutical efforts
dystrophin deficiency
1:3,500 male births
rapid progression of skeletal muscle dystrophyand cardiomyopathy
corticoid treatment

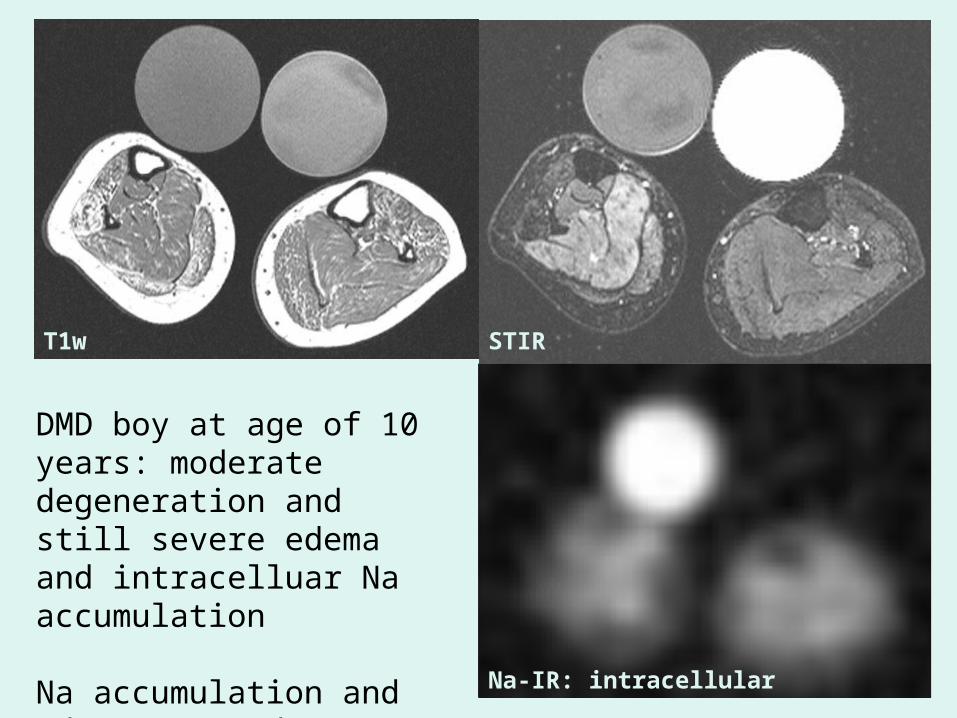
T1w STIR
Na-IR: intracellular Na+
DMD boy at age of 7 years: minor degeneration, however: already severe edema and intracelluar Na accumulation
!
T1w STIR
[Na+]
DMD boy at age of 10 years: moderate degeneration and still severe edema and intracelluar Na accumulation
Na accumulation and edema preceed/cause degeneration
Na-IR: intracellular Na+

Thanks to Karin Jurkat-Rott (Ulm), Marc-André Weber (Heidelberg), & Eva Luise Köhler

View from Ulm University of Ulm Munster and the Alpes