
UNDERSTANDING PARTICIPATION OF RACIAL AND ETHNIC GROUPS … · UNDERSTANDING PARTICIPATION OF...
199
UNDERSTANDING PARTICIPATION OF RACIAL AND ETHNIC GROUPS IN MULTIPLE SCLEROSIS CLINICAL TRIALS A Thesis Presented to The Faculty of the Department of Anthropology San José State University In Partial Fulfillment of the Requirements for the Degree Master of Arts By Angela Fuller May 2015
Transcript of UNDERSTANDING PARTICIPATION OF RACIAL AND ETHNIC GROUPS … · UNDERSTANDING PARTICIPATION OF...

UNDERSTANDING PARTICIPATION OF RACIAL AND ETHNIC GROUPS IN
MULTIPLE SCLEROSIS CLINICAL TRIALS
A Thesis
Presented to
The Faculty of the Department of Anthropology
San José State University
In Partial Fulfillment
of the Requirements for the Degree
Master of Arts
By
Angela Fuller
May 2015

© 2015
Angela Fuller
ALL RIGHTS RESERVED
The Designated Thesis Committee Approves the Thesis Titled
UNDERSTANDING PARTICIPATION OF RACIAL AND ETHNIC GROUPS IN
MULTIPLE SCLEROSIS CLINICAL TRIALS
By
Angela Fuller
APPROVED FOR THE DEPARTMENT OF ANTHROPOLOGY
SAN JOSÉ STATE UNIVERSITY
May 2015
Dr. Roberto Gonzalez Department of Anthropology Dr. Guadalupe Salazar Department of Anthropology Dr. Charlotte Sunseri Department of Anthropology

ABSTRACT
UNDERSTANDING PARTICIPATION OF RACIAL AND ETHNIC GROUPS IN MULTIPLE SCLEROSIS CLINICAL TRIALS
By Angela Fuller
Multiple sclerosis (MS) patients from different racial and ethnic groups are
equally likely to participate in clinical trials despite the significant risk that
experimental drugs pose to their health. This is in contrast to existing literature
which points to minority group distrust of medical research as a reason for low
clinical trial participation rates. Given this disparity, the purpose of this thesis is
to understand the complexities surrounding MS clinical trial participation. A
mixed methods approach was utilized, including: 1) review of archival data for
racial and ethnic group clinical trial participation rates; 2) an electronic survey to
capture MS patient exposure to and knowledge of clinical trials; and 3) semi-
structured interviews to elucidate perceptions of clinical trial participation.
Despite the predicted influence of distrust on clinical trial participation rates, this
study identified no differences in motivations to participate among racial or ethnic
groups. Focusing only on minority distrust as a reason for low clinical trial
participation may overlook true patient motivations which are mediated, not by
arbitrary categories of race and ethnicity, but by balancing the complicated
interactions of distrust, risk perception and risk acceptance, with the perceived
benefits of clinical trial participation. These motivations are situated within the
context of structural barriers that can prevent clinical trial participation, such as
health care access and clinician bias.
v
ACKNOWLEDGEMENTS
I would like to extend my deepest appreciation to my thesis committee,
Dr. Roberto Gonzalez, Dr. Guadalupe Salazar, and Dr. Charlotte Sunseri, for
their support and guidance throughout this entire thesis process. It has been
such an important learning experience for which I am eternally grateful and will
not soon forget. I wish to give a special thank you to the multiple sclerosis
patients I was able to work with every day, who taught me so much about trust,
fear, patience, and hope. It was through their endless curiosity and inspiration
that I was able to finish this work. Finally, I would like to thank my family, friends,
and fellow graduate students for their continuous support and encouragement.
And to Micah, who never doubted that it could be done.

vi
TABLE OF CONTENTS
Chapter 1: Introduction ......................................................................................... 1
An Introduction to the Unknown ................................................................. 1
Clinical Trials 101 ...................................................................................... 2
Clinical Research Coordinator or Ethnographer? ...................................... 6
Objectives .................................................................................................. 9
Chapter 2: The Discourse of Multiple Sclerosis .................................................. 13
Multiple Sclerosis as Medical Diagnosis .................................................. 13
Multiple Sclerosis as Identity .................................................................... 17
An Epidemiological Story ......................................................................... 20
The Causation Hypotheses ...................................................................... 26
Missing Pages of the Epidemiological Story ............................................ 29
Chapter 3: Underrepresentation in Clinical Trials ............................................... 33
Reporting Rates of Clinical Trial Participants by Race and Ethnicity ....... 33
Are There Differences By Race and Ethnicity? ........................................ 36
Barriers to Clinical Trial Participation ....................................................... 40
Facilitators to Clinical Trial Participation .................................................. 44
Precautions .............................................................................................. 47
Chapter 4: The Anthropology of Clinical Trials ................................................... 52
The Inclusion-and-Difference Paradigm................................................... 52
Biopolitical Citizenship and the Illusion of Race ....................................... 54
Recruitmentology ..................................................................................... 61

vii
Risk .......................................................................................................... 64
Chapter 5: Research Design .............................................................................. 68
Research Questions ................................................................................ 68
Research Methods ................................................................................... 68
Institutional Approvals .............................................................................. 75
Chapter 6: Results .............................................................................................. 76
Archival Data ........................................................................................... 76
Electronic Survey ..................................................................................... 83
Semi-Structured Interviews ...................................................................... 93
Chapter 7: Discussion ...................................................................................... 161
Underrepresentation Exists .................................................................... 161
Distrust is Real but Not Absolute ........................................................... 166
Risk Perception ...................................................................................... 170
Why Participate in Clinical Trials? .......................................................... 172
References Cited .............................................................................................. 175
viii
LIST OF TABLES
Table 1: Four Phases of Clinical Trials ................................................................. 3
Table 2: Estimated Prevalence Rates of MS in the United States by Race and Ethnicity ................................................................................................... 23
Table 3: MS Clinical Trial Participants in the US by Sex .................................... 77
Table 4: MS Clinical Trial Participants in the US by Race .................................. 79
Table 5: MS Clinical Trial Participants in the US by Ethnicity ............................. 80
Table 6: Demographics of MS Patients Served by BAMC MS Clinic .................. 81
Table 7: Demographics of MS Patients Participating in Clinical Trials at BAMC MS Clinic .................................................................................................. 83
Table 8: Demographics of Electronic Survey Respondents ................................ 84
Table 9: Frequency of Survey Respondents’ Primary Reasons for Accepting Participation in a Clinical Trial .................................................................. 88
Table 10: Frequency of Survey Respondents’ Primary Reasons for Declining
Participation in a Clinical Trial .................................................................. 88 Table 11: Degree of Influence on Participation in a Clinical Trial by Race or
Ethnicity ................................................................................................... 90 Table 12: Degree of Influence on Participation in a Clinical Trial by Sex ............ 91
Table 13: Degree of Influence on Participation in a Clinical Trial by Income Level ........................................................................................................ 91 Table 14: Demographics of Interview Participants .............................................. 95
Table 15: Interview Participants’ Primary Reasons for Accepting Participation in a Clinical Trial ........................................................................................... 109
Table 16: Interview Participants’ Primary Reasons for Declining Participation in a
Clinical Trial ........................................................................................... 110 Table 17: Current MS Clinical Trials Being Conducted at BAMC ..................... 141

ix
Table 18: Current FDA Approved MS Medications ........................................... 147

x
LIST OF FIGURES
Figure 1: Four Clinical Courses of Multiple Sclerosis ......................................... 16 Figure 2: Percentage of Caucasian and non-Caucasian Respondents who have
Discussed Clinical Trial Participation with their Doctor, Nurse, or Research Personnel ................................................................................................. 87
1
Chapter 1 - Introduction
An Introduction to the Unknown
I was at home with my legs paralyzed. That's how bad it got. I couldn't even move these legs. It got really, really bad and I didn't even know if I was having a flare up or not. I was just accepting my condition. And so, I mean, I would say, it's just sheer survival. I think we all have it, whether you're Mexican, Black or whatever race you're in. That might be the common answer. People want to survive. That’s what motivated me. It’s just plain survival. I was willing to risk my life even if it was to kill me because I really felt like I didn't have anything to live for anymore. [Isabelle Carbajal]
This sentiment was shared with me by one of my clinical trial patients,
Isabelle,1 during our semi-structured interview for this project. Even though I had
known her for four years as a participant in a multiple sclerosis (MS) clinical trial,
it was still a surprise to hear the dire circumstances she found herself in before
she decided to enter the clinical trial she is still participating in today. Because I
was working as a clinical research coordinator (CRC) for a San Francisco Bay
Area medical center (referred to throughout this document as Bay Area Medical
Center or BAMC),2 I was able to get to know Isabelle, as well as all the other MS
patients who were participating in various MS clinical trials at BAMC. Many of
the other MS patients had also been participating in their respective clinical trials
for at least four years, and some of the newest patients I had already known for
at least a year and a half. What always struck me about these patients was the
courage and strength it took to not only face a chronic, debilitating, neurologic
1 All names have been changed to protect the identities of the study participants.
2 Name of medical center has been changed to further protect the identities of the study participants and
medical center staff.
2
disease, but to also jump head first into a clinical trial in which there were so
many unknowns. As she candidly explained, Isabelle was willing to participate in
a clinical trial, even if it was going to kill her. “I felt like I was almost using
[BAMC] to end things for me if I wasn’t going to get any better. I was willing to
just give my life for that” (Isabelle Carbajal).
Clinical Trials 101
MS is a complex disease with unknown etiology, equivocal incidence and
prevalence rates, unpredictable symptoms and symptom severity, and mildly
effective treatments. There is currently no cure for MS. Given all of these
unknowns, what motivates patients to participate in clinical trials? On the
surface, clinical trials would not seem to provide the bastion of stability MS
patients might pursue. Clinical trials are prospective biomedical or behavioral
human research studies designed to answer questions about a proposed
intervention, medication or therapy. The central focus is to understand whether a
new medication is safe and effective. If data from a clinical trial can show that a
medication is both safe and effective as it progresses through the requisite three
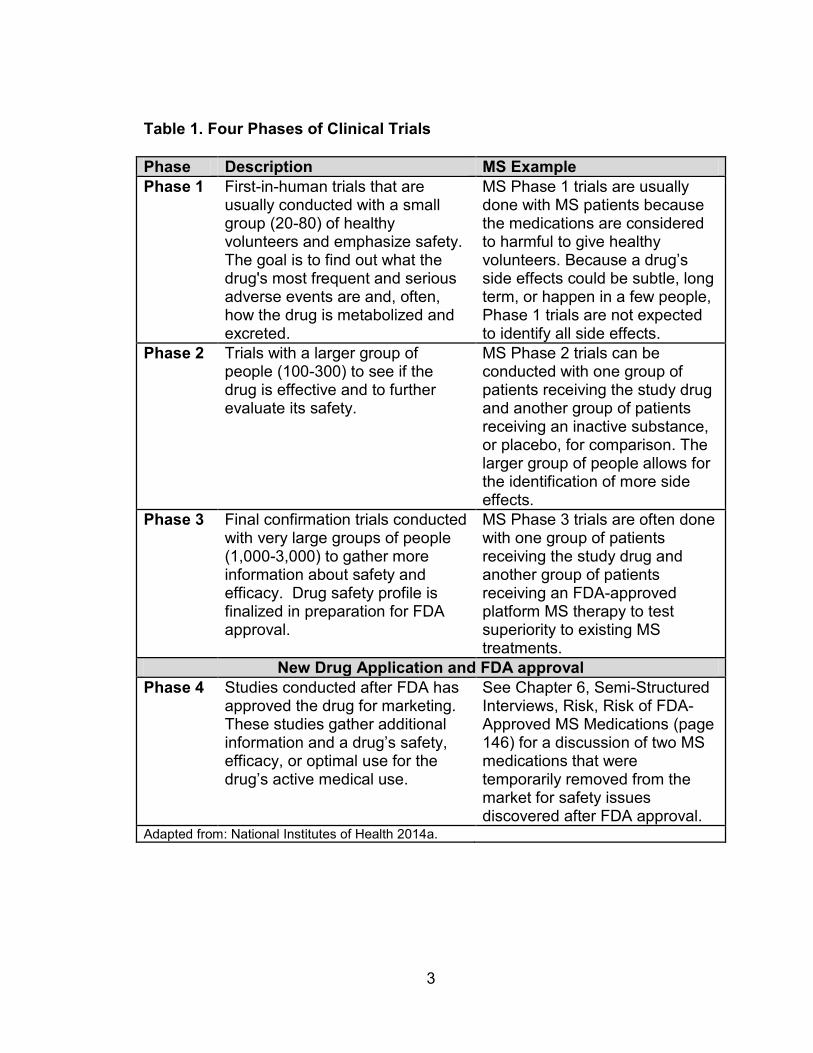
phases of clinical trials, not including the fourth after-market phase (see Table 1),
then the US Food and Drug Administration (FDA), after significant review, can
approve the medication for use in a larger population (National Institutes of
Health 2014a). Conducting a clinical trial is not possible until initial review and
approval by an Institutional Review Board (IRB) which is tasked with protection of
human subjects in research per Title 21 Code of Federal Regulations (CFR) Part
3
Table 1. Four Phases of Clinical Trials
Phase Description MS Example
Phase 1 First-in-human trials that are usually conducted with a small group (20-80) of healthy volunteers and emphasize safety. The goal is to find out what the drug's most frequent and serious adverse events are and, often, how the drug is metabolized and excreted.
MS Phase 1 trials are usually done with MS patients because the medications are considered to harmful to give healthy volunteers. Because a drug’s side effects could be subtle, long term, or happen in a few people, Phase 1 trials are not expected to identify all side effects.
Phase 2 Trials with a larger group of people (100-300) to see if the drug is effective and to further evaluate its safety.
MS Phase 2 trials can be conducted with one group of patients receiving the study drug and another group of patients receiving an inactive substance, or placebo, for comparison. The larger group of people allows for the identification of more side effects.
Phase 3 Final confirmation trials conducted with very large groups of people (1,000-3,000) to gather more information about safety and efficacy. Drug safety profile is finalized in preparation for FDA approval.
MS Phase 3 trials are often done with one group of patients receiving the study drug and another group of patients receiving an FDA-approved platform MS therapy to test superiority to existing MS treatments.
New Drug Application and FDA approval
Phase 4 Studies conducted after FDA has approved the drug for marketing. These studies gather additional information and a drug’s safety, efficacy, or optimal use for the drug’s active medical use.
See Chapter 6, Semi-Structured Interviews, Risk, Risk of FDA-Approved MS Medications (page 146) for a discussion of two MS medications that were temporarily removed from the market for safety issues discovered after FDA approval.
Adapted from: National Institutes of Health 2014a.
4
56 (Food and Drug Administration 2014). This body helps determine whether the
benefits of the proposed trial outweigh the risks, and that any potential risks are
appropriately mitigated and disclosed.
When assessing the legitimacy of clinical trial data, the gold standard
according to the evidence-based medicine movement is the randomized
controlled trial. Randomized controlled trials are often employed during Phase 2
and Phase 3 trials, when the efficacy of a drug is tested through comparison to a
placebo, an inactive product that looks indistinguishable from the study drug but
without its treatment value, or other drug comparator. However, in MS clinical
trials, the use of placebos is somewhat limited because of the ethical and safety
concerns of MS patients going untreated for extended periods of time.
Sometimes MS trials are designed to have a short window of randomization to
the study drug or placebo, after which all trial participants, even participants who
were in the placebo group, are re-randomized to different doses of the study drug
for the remainder of the trial. Randomization ensures that participants are
assigned to a treatment group by chance rather than choice, which helps
eliminate any treatment bias. Blinding of the treatment assignment prevents the
research staff or trial participants from knowing which treatment they have been
assigned to so they cannot influence the results. In a single-blind study, only the
trial participant lacks knowledge of his or her treatment assignment; in a double-
blind study, the trial participant and research staff, including the investigators,

5
lack knowledge of patient treatment assignments (National Institutes of Health
2014b).
Despite the potential risks of an experimental drug and the unknowns
inherent in clinical trial design, the drive for patients to participate in clinical trials,
at least from a CRC perspective, is strong. In addition to working on MS clinical
trials, I have also had the opportunity to work on clinical trials for stroke,
Parkinson’s disease, and Alzheimer’s disease. For our stroke trial, which was a
Phase I clinical trial requiring stereotactic implantation3 of adult stem cells into the
brain, I was contacted by hundreds of patients from across the US and abroad
for the chance to qualify and participate. Because of the stringent inclusion
criteria, a high percentage of patients were ineligible, and much time was spent
delivering this news and consoling sobbing patients. For the Parkinson’s disease
trial, patients were required to undergo stereotactic implantation of a gene
therapy product into the area of the brain thought to cause the disease. Because
this was a Phase II efficacy trial, a control group was required for comparison;
thus, half of patients participating in the trial received the actual surgery, while
the other half received a “sham surgery”4 and neither patient group could tell
which they had received. Again, many patients were interested but few qualified.
The interest in an Alzheimer’s disease trial was similar since there are currently
3 A metal frame is secured to the patient’s skull at four points to allow for trajectory planning of stem cell
implementation into the brain. 4 A sham surgery is part of an ethically contentious trial design that provides a truly blinded control group
in a surgical clinical trial. In this case, the sham surgery consisted of completely shaving the patient’s head, applying the metal frame to the patient’s skull, administering anesthesia, drilling a partial burr hole into the skull, sitting in the operating room for at least 4 hours to simulate the length of time an actual surgery would take, screwing a titanium plate over the partial burr hole, and stitching up the scalp.

6
no treatments for the disease. Many family members were desperate to try
anything to help their loved one who was slowly losing touch with reality.
I was in awe at the courage it took for all of these patients to participate in
these clinical trials. For the MS patients I worked with, participation in their
respective clinical trials was often a calculated decision based on considerations
of the currently available FDA approved MS medications, the experimental
medications being offered in clinical trials, and the unpredictability of their
disease. I wanted to understand the motivations of these clinical trial participants
to see if there were commonalities that existed among trial participants that
enticed them to seek out clinical trials. I often wondered, if I were in the same
position, would I make the same choice?
Clinical Research Coordinator (CRC) or Ethnographer?
As a CRC, I was officially responsible for coordinating the conduct of
clinical drug trials for a variety of neurologic conditions, including MS, but it is
through my unofficial role as mediator between doctor and patient, liaison
between drug company and patient, disability claim consultant, pharmacy aid,
patient counselor, family counselor, and friend, that I became privy to the
nuanced experience of the MS patient. For the MS patients I had the privilege of
getting to know, I became their personal gateway to the world of medical
research. Together, we navigated the rigorous protocol requirements of
participating in clinical research, made more difficult by the complexities inherent
in managing the unpredictable nature of their medical condition. Many of these

7
patients came to trust me with their most difficult and complex concerns about
what it is like to be a person diagnosed with a chronic, disabling disease like MS.
I came to learn intimately how much participating in clinical trials meant to these
patients, how much it changed their lives, and how it provided them with the
agency to take control of an unpredictable disease in an ever-changing
landscape of MS medications and therapies.
Thus, when first thinking about conducting this project, I thought that my
position as a CRC with such intimate knowledge of the clinical trial patients and
being embedded in the BAMC MS clinic every day, provided me with entry to a
world few can access. Being a CRC is like being at the central hub of the entire
clinical trial enterprise, where responsibilities include dealing with a wide array of
social actors including pharmaceutical companies, contract research
organizations, IRBs, hospital administrators, research personnel (including
neurologists, neuroradiologists, neuro-ophthalmologists, psychiatrists,
pharmacists, physical and occupational therapists, nurses, medical assistants,
laboratory technicians, etc.), patients, and patients’ families. I was part of the
team that helped identify potential clinical trial patients and worked to retain those
patients in our trials for the length of the study. My experience as a CRC
provided an insider’s perspective on how clinical trials are conducted and provide
access to the MS patients who chose to participate in a clinical trial. As an
ethnographer, the benefits of this kind of access could be extremely valuable in
developing a nuanced understanding of clinical research at BAMC.
8
However, because of my role as a CRC, I was afraid that being part of the
clinical research team in charge of conducting the clinical trials would hinder my
ability to find patients willing to speak openly with me about their experience
participating in a clinical trial. There was a possibility that my role as a
researcher would place me in a position of power relative to the trial participants,
and that it would be a significant barrier to discovering true motivations for
participating in clinical trials. Participants might have felt coerced to participate
because I was part of the research team, thus affecting “voluntary consent.”
Fortunately, I felt that the potential power differential between myself and the
patient was minimized as I was considered one of the front line staff instead of a
higher level researcher. I was the one helping the MS patient navigate the
complexities of the clinical trial on a daily basis and the first one they called with
any questions they had, big or small. In fact, all of them had access to my cell
phone number in case anything came up at any time.
Although it is unclear whether my role as a researcher affected the
responses of the MS patients, I did my best to make each patient feel as
comfortable as possible by ensuring confidentiality and assurance that their
responses would not affect their normal medical or research care. Offering to do
the interviews away from BAMC was an important part of this attempt to separate
my formal relationship with patients when interacting inside BAMC from the
informal relationship I hoped to foster away from BAMC. Removing myself from
this environment was an attempt to alleviate any notion that a patient could not

9
be honest with me. Interestingly, I think that some patients enjoyed my dual role
as researcher and ethnographer. They were all familiar and comfortable with my
role as a researcher, but when I was an ethnographer, it allowed the patients to
step back and consider what trial participation meant to them on a personal level.
Many admitted during the interviews that they had never thought about some of
the questions I was asking and that it was nice to stop and reflect. For myself,
my role as a researcher was enhanced by my role as an ethnographer. As a
researcher, one can get bogged down with regulations and data and paperwork.
Conducting this project and connecting with my MS clinical trial patients was an
extremely enlightening, unique, and personally rewarding experience.
Objectives
Given my professional and personal connection to MS clinical trial patients
at BAMC, I set out to explore the reasons MS patients chose to participate in
clinical trials. When I started this research, there were no studies investigating
MS patients’ reasons for participating in research. However, there was an
abundance of studies looking at why other types of patients (e.g., cancer,
cardiac, HIV/AIDS, asthma, diabetes and pain disorder) participated in clinical
research. Unexpectedly, most of these studies revolved around understanding
underrepresentation of racial and ethnic minorities in clinical trials. Results
indicated that the biggest contributing factor was systematically identified as
distrust of research. I wondered if this was the case for MS patients. Thinking
about Isabelle who self identifies as a Latina, it was highly unlikely that she had
10
distrust of research if she was willing to risk her life over her participation in a
clinical trial. Perhaps her desperation to find some kind of treatment to alleviate
or halt the progression of MS outweighed her fear and distrust. The biggest
factor for her seemed to be a medical need that outweighed any potential risks
presented by the clinical trial and perhaps even the risk of not participating in a
clinical trial. If her race and ethnicity and distrust of research were not factors in
her clinical trial participation, what helped her justify doing something so risky to
help meet her medical need?
This thesis set out to answer the following questions regarding
participation in MS clinical trials:
1. Is there underrepresentation of racial and ethnic minority groups in MS
clinical trials? If so, why?
2. In what ways do preconceptions about medical research, altruistic
motivations, and daily experience with disease contribute to MS
patients’ participation in clinical trials?
3. What are the salient MS patient attitudes towards clinical trials?
If underrepresentation is a factor in MS clinical trials, it would be
detrimental to developing a comprehensive understanding of MS treatments that
respond to the disease course variety seen in different individuals. It is important
to note that underrepresentation in this thesis will focus on minority racial and
ethnic groups and not other underrepresented groups, such as older adults, rural
populations, and those of low socioeconomic status. Underrepresentation of

11
racial and ethnic groups leads to clinical trial results that are not generalizable to
the public. For trial results to be meaningful to the general public, clinical
research participants should approximate the variety of individuals that exist in a
given population. Otherwise, a trial conducted with mostly Caucasian, middle-
aged men would have results that may not be applicable to other populations,
such as women, younger or older adults, and non-Caucasian racial and ethnic
groups. MS is already a difficult disease to study given the unpredictability of
natural history and patient prognosis. Underrepresentation of racial and minority
groups in MS clinical trials would only make the search for an effective treatment
more elusive.
Independent of finding underrepresentation of racial and ethnic minorities
in MS trials, it is also important to understand whether there are additional factors
that determine whether an MS patient decides to participate in a clinical trial.
Distrust is often cited as the main barrier to minority group participation in clinical
trials for cancer, cardiac, HIV/AIDS, asthma, diabetes and pain disorder. Given
that MS patients of different racial and ethnic groups may be equally likely to
participate in clinical trials, distrust may not be the most applicable reason for a
finding of low participation rates in clinical trials for MS. Instead, other factors like
preconceptions about medical research, altruistic motivations, and daily
experience with disease may contribute to MS patients’ participation in clinical
trials. This thesis attempts to elucidate these other factors to determine whether
distrust has the biggest influence on participation rates, or some other factor.
12
Also, illuminating salient MS patient attitudes towards clinical trials will aid in
identifying any unknown factors that may contribute to participation rates.
Thus far, much of the anthropological research on minority group
underrepresentation in medical research focuses on international ethical
concerns, improper informed consent, and misunderstandings of the Western
model of medicine and research, which are often incompatible with non-Western
environments (Adams, et al. 2007; Petryna 2005; Petryna 2007; Van der Geest,
et al. 1996). In the US, there is a great opportunity for anthropologists to
contribute to the medical community’s understanding of underrepresentation of
minority groups in clinical trials. Because anthropologists utilize methods such
as participant observation, patient narratives, and analysis of political economic
structures, contributions to safer clinical trial design, more culturally competent
care, and increased protection and participation of research participants can be
made (Azevedo and Payne 2006; Barnett 1985). Ethnographic research
methods can be used in this case to elucidate local understandings of clinical
research for MS patients and to evaluate patient motivations for participating in
clinical trials.

13
Chapter 2 – The Discourse of Multiple Sclerosis
Multiple Sclerosis as Medical Diagnosis
Multiple Sclerosis (MS) is an autoimmune, inflammatory disease in which
the body’s own immune cells attack the nerves in the central nervous system
(CNS), which is made up of the brain, spinal cord and optic nerve (Vollmer 2007).
Inflammation, which is triggered by the immune response, causes damage to
myelin, the protective covering surrounding nerve cells. Myelin is like the rubber
insulation on a wire: if the rubber on the wire is missing or damaged, electrical
conduction is slowed down or obstructed. The same occurs with a patient
diagnosed with MS: if the myelin is missing or damaged due to the body’s own
immune response, nerve impulses to various parts of the body are slowed down
or stopped. In 1868, the French neurologist, Jean Martin Charcot, first clarified
the clinical and pathological features of MS as being distinct from other
neurologic diseases. He named the disease “sclérose en plaques” which
described the damage (lesions or plaques) in the brain, spinal cord, and optic
nerves characteristic of MS. The name multiple sclerosis describes the
“sclerosed” or hardened plaques of tissue lesions located at “multiple” sites
throughout the CNS (Holland, et al. 2007). Symptoms for MS patients are
extremely variable because they depend on the location and severity of each
inflammation attack. Symptoms can include, but are not limited to, numbness,
pain, tingling, loss of balance, difficulty walking, vision loss, bowel and bladder

14
incontinence, decreased attention span and memory loss, slurred speech,
fatigue, and depression.
There is no one laboratory test or physical exam finding that can
determine whether or not an individual has MS. In order to make a diagnosis, a
physician must 1) find evidence of damage or lesions in at least two separate
locations in the CNS, 2) find evidence that the damage or lesions occurred at
least one month apart, and 3) rule out all other possible diagnoses. These long-
established criteria are based on the principle of finding CNS lesions
disseminated in both space and time; however, there have been several
revisions to the criteria which account for advancements in medical technology
and diagnostic thresholds (Milo and Miller 2014). The Schumacher and Poser
criteria allow diagnosis with demonstration of two separate MS attacks, or
relapses, which involve at least two different areas of the CNS. The 2001
McDonald Criteria, and the 2005 and 2010 Revised McDonald Criteria, allowed
for earlier diagnosis and to account for evidence provided to physicians by
magnetic resonance imaging (MRI) of the brain and spinal cord.
The natural history of MS is widely variable and largely unpredictable on
an individual basis, thus rendering any predication for patient outcome or
prognosis tenuous at best. The disease can lie dormant for any brief or extended
amount of time with periodic relapses of MS symptoms. Relapses are also called
attacks or flares. Alternately, the disease can present as progressive worsening
over time without any recognizable relapses or attacks of MS symptoms. With

15
such variability, physicians have found it helpful to classify the disease under four
distinct categories to assist with medical care, rehabilitation, and treatment
options. Relapsing-remitting MS is characterized as having unpredictable
attacks followed by periods of symptom remissions lasting months or even years.
Secondary-progressive MS is characterized as the stage of continuous and
progressive neurologic decline which follows the initial stage of relapsing-
remitting MS; thus the term “secondary” is used to denote the progressive phase
as secondary to the initial relapsing phase. Primary-progressive MS is
characterized by continuous and progressive neurologic decline from the outset
of the disease without any identifiable relapses or attacks; thus, the term
“primary” is used to denote the progressive phase as being the first phase of the
disease. Finally, progressive-relapsing MS is characterized by a continuous and
progressive neurologic decline from the outset but with relapses and attacks in
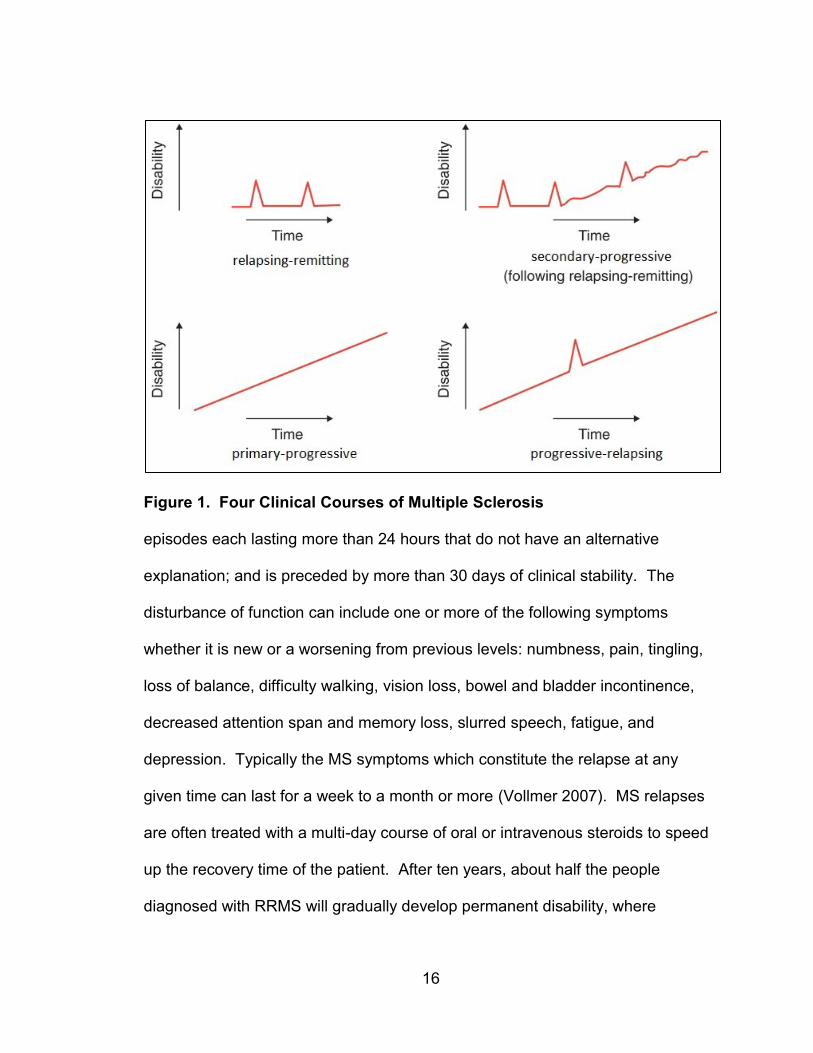
addition to slow progression (Vollmer 2007). Figure 1 shows the four different
disease patterns comparing increasing disability over time.
Although these four categories help with identifying the nature and pattern
of MS symptoms, a large proportion, approximately 85%, of MS patients initially
present with the relapsing-remitting MS form of the disease. A relapse,
particularly for use in clinical trials, has been defined by Schumacher et al. (1965)
as: a focal disturbance of function affecting a white matter5 tract; two or more
5 White matter is the part of the CNS that contains the myelinated portion of nerve cells. It appears white
in color because of the myelin coating which assists in conducting electronic nerve impulses. Grey matter is part of the CNS that contains the cell bodies of nerve cells.
16
Figure 1. Four Clinical Courses of Multiple Sclerosis episodes each lasting more than 24 hours that do not have an alternative
explanation; and is preceded by more than 30 days of clinical stability. The
disturbance of function can include one or more of the following symptoms
whether it is new or a worsening from previous levels: numbness, pain, tingling,
loss of balance, difficulty walking, vision loss, bowel and bladder incontinence,
decreased attention span and memory loss, slurred speech, fatigue, and
depression. Typically the MS symptoms which constitute the relapse at any
given time can last for a week to a month or more (Vollmer 2007). MS relapses
are often treated with a multi-day course of oral or intravenous steroids to speed
up the recovery time of the patient. After ten years, about half the people
diagnosed with RRMS will gradually develop permanent disability, where
17
relapses may still occur, but periods in between are characterized by a continued
disease progression phase (Pucci, et al. 2011).
Although the treatment of MS has come a long way from the death
sentence it used to carry only 20 years ago, there is still much to learn about
what causes it, who gets it, how patients and providers can manage it better, or
whether finding a cure is possible. Current therapies focus on how to reduce the
rate of patient relapses, which slow the progression of permanent neurologic
deficiencies, but are not a cure. Annual relapse rate has been used as an
outcome in both clinical care and medical research (Coyle and Johnson 2007)
and relapse rates currently average 1.1 per year early in the disease course
(Vollmer 2007). Despite the overall outlook of disease progression, on an
individual level, MS follows unpredictable patterns of disease accumulation and
there is still too much variability to predict an individual’s disease course (Vollmer
2007).
Multiple Sclerosis as Identity
The manifestation of MS is extremely variable due to the unpredictability
of when a patient can expect a relapse and how long and how severe a particular
relapse can be. During relapses, in addition to physical changes, cognitive
changes can occur and MS patients are often at higher risk for depression. The
anticipation and experience of relapses can create feelings of grief, anxiety,
anger, and guilt which make it difficult to accept the totality of the diagnosis (Kalb
2007). Upon first diagnosis, the patient, patient’s family, and friends may utilize

18
themes of denial in order to show support that the patient is actually well, that
other people with MS are far worse than this, that the doctor made a mistake, or
that the patient will be able to beat this. Upon experiencing subsequent relapses,
the patient is forced to acknowledge the beginning of his or her life with a chronic
illness. This requires a change in self-image, although patients, partners,
children, and family may continue to blame the manifestation of the disease on
not being strong enough to fight it (Kalb 2007).
Much of the literature on the adjustment period for an MS patient focuses
on the transition of self and identity from pre-diagnosis to diagnosis and beyond.
The resolution or redefinition of identity occurs slowly over time but is often
psychological and spiritual rather than physical. The patient must focus on being
successful at fully adapting to his or her diagnosis so that his or her rehabilitation
potential and quality of life can be fulfilled (Irvine, et al. 2009). Although fatigue
and depression are associated with MS, the correlation of neurologic impairment
to fatigue severity disappears when looking at the concept of helplessness (Van
der Werf, et al. 2003). Thus, fatigue severity, which is associated with
depression, is not directly related to MS severity, but is affected by feelings of
helplessness as patients attempt to navigate the unpredictability of MS. Because
a patient’s understanding and ability to cope with his or her disease can have a
direct effect on the physical manifestation of that disease, community groups,
even for pediatric MS populations, help foster motivation and self-competency for
improved quality of life. Group activities are often designed to help redefine the

19
assumptions of disability in order to nurture confidence (Block and Rodriguez
2008).
The preservation of self and identity in persons with a chronic illness
becomes even more complex with MS because many of the neurologic
symptoms of MS, such as fatigue, loss of vision, or numbness, are invisible to
others. Unlike those with obvious disabilities, people with MS can often choose
whether or not to keep their disabilities hidden. This can be an empowering
option, as the possibility of controlling their illness identity is well within reach.
However, this often creates a dilemma for the MS patient who may attempt to
keep his or her disability hidden from others, at the risk of others assuming that
an inability to perform job duties is due to laziness or poor work ethic rather than
accumulating physical disabilities. On the other hand, the MS patient may decide
to reveal his or her disability, at the risk of assuming the socially created stigma
of what it means to be chronically ill or disabled (Fitzgerald and Paterson 1995).
Acceptance of the diagnosis of MS is a long and difficult process that
involves redefinition of self, building confidence in identifying with a chronic
illness, and understanding how to relate to a world that does not immediately
comprehend the needs or accommodations a person with MS may require.
Much of the focus for those with MS is on how the individual can cope with the
diagnosis and rise above the difficulty in transitioning from a healthy individual to
one with chronic illness. The transition can be made psychologically or
spiritually. Support groups and counseling available to those with MS offer an

20
empowering way for each individual to control his or her own disease through
self-education, self-advocacy, and self-determination. Mastery and personal
control over the unpredictable course of MS involve, “ordering and sequencing
the myriad range of phenomena in everyday life which may or may not be
perceived as related to health and illness” (Robinson 1990: 1185). It is perhaps
this illusion of control that draws MS patients towards clinical trials as a way to
exert power and deny the feeling of powerlessness.
An Epidemiological Story
MS is considered the leading cause of neurologic disability in young
adults. Onset of the disease typically occurs between the ages of 20 to 50, with
30 the mean age of onset. However, the disease can develop in childhood and
after age 60. MS is 2.5 times more common in women than in men (Multiple
Sclerosis International Federation 2013; Noonan, et al. 2002). In 2008, the
median global prevalence of MS was 30 per 100,000 persons (World Health
Organization and Multiple Sclerosis International Federation 2008). By 2013, the
median global prevalence of MS increased to 33 per 100,000 persons (Multiple
Sclerosis International Federation 2013). It is difficult to ascertain whether this
increase was due to a true increase in the number of people who have MS
globally, or if it was due to better diagnosis and reporting. While it is clear that
MS can be found in all regions of the world, MS prevalence has great variability
across the globe. North American, European, East Asian, and Sub-Saharan
African prevalence is 140, 108, 2.2, and 2.1 per 100,000 persons, respectively. It

21
is important to note, however, that these numbers only tell part of the
epidemiological story, since MS prevalence also has variability within a particular
region. For example in Europe, the highest prevalence is in Sweden which
reports 189 per 100,000 persons while the lowest prevalence is in Albania which
reports only 22 per 100,000 persons (Multiple Sclerosis International Federation
2013).
Additional indicators of potential MS treatment progress and resource
availability may mask continued disparities between countries. From the same
period of 2008 to 2013, there was a 30% increase in the number of neurologists
in the world. A majority of these were attributed to increases in reporting in the
Americas and the West Pacific regions, in addition to a proportionally higher
increase in low-income countries than middle- and high-income countries. The
increase in the global number of neurologists from 1.01 to 1.32 per 100,000
seems like a positive improvement for patients who did not previously have
access to a neurologist. However, the comparison of neurologists between high-
income countries and low-income countries reveal the chronic inequalities that
remain for patients seeking specialized neurological medical care. High-income
countries report 3.6 neurologists per 100,000 while low-income countries report
only 0.03 per 100,000 persons, which is approximately 100 times fewer
neurologists per person than high-income countries (Multiple Sclerosis
International Federation 2013).

22
Similarly, the number of MRI machines available is indicative of a region’s
ability to diagnose MS earlier using the most recent McDonald Criteria. Although
the number of MRI machines has doubled in the same five year period, high-
income countries report 1.474 MRI machines per 100,000 persons while low-
income countries report 0.012 MRI machines per 100,000 persons. Because
low-income countries do not have the same access to MRI machines as high-
income countries, low-income countries were more likely to use older diagnostic
criteria to diagnosis MS since the older criteria do not rely on the availability of
MRI. Thus diagnosis rates in these countries may not be consistent with the
methods used in high-income countries. The availability of disease-modifying
therapies which are fully or partially funded by a country’s government also follow
the pattern of high medication availability in high-income countries, to no
availability in low-income countries (Multiple Sclerosis International Federation
2013). When looking at other pieces of the story, such as access to neurologists,
clinical technology like MRI machines, and MS treatments, global inequalities are
revealed.
In the US, recent estimates of MS prevalence by race and ethnicity
suggest a higher prevalence among Caucasian men and women as compared
with African Americans and all other racial and ethnic categories. The increased
prevalence in women versus men is consistent among all racial and ethnic
groups (Noonan, et al. 2002; Noonan, et al. 2010). Table 2 presents the
estimated prevalence rates of MS in the US by race and ethnicity. Caucasians
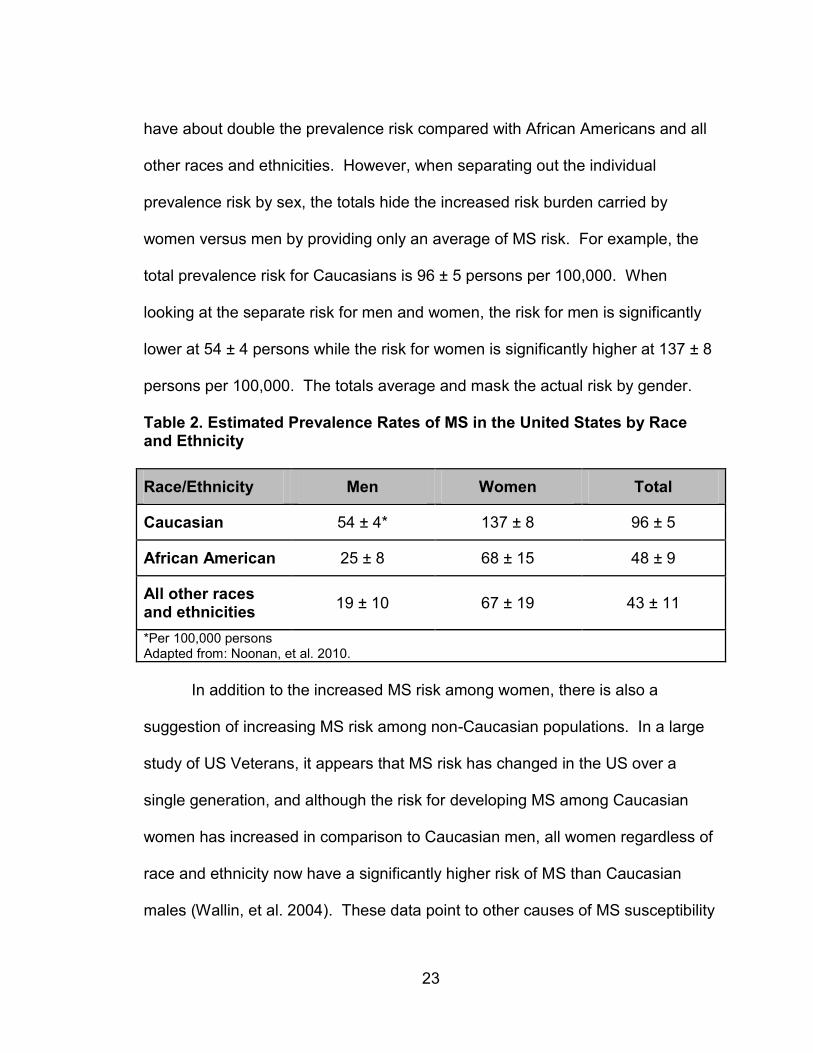
23
have about double the prevalence risk compared with African Americans and all
other races and ethnicities. However, when separating out the individual
prevalence risk by sex, the totals hide the increased risk burden carried by
women versus men by providing only an average of MS risk. For example, the
total prevalence risk for Caucasians is 96 ± 5 persons per 100,000. When
looking at the separate risk for men and women, the risk for men is significantly
lower at 54 ± 4 persons while the risk for women is significantly higher at 137 ± 8
persons per 100,000. The totals average and mask the actual risk by gender.
Table 2. Estimated Prevalence Rates of MS in the United States by Race and Ethnicity
Race/Ethnicity Men Women Total
Caucasian 54 ± 4* 137 ± 8 96 ± 5
African American 25 ± 8 68 ± 15 48 ± 9
All other races and ethnicities
19 ± 10 67 ± 19 43 ± 11
*Per 100,000 persons Adapted from: Noonan, et al. 2010.
In addition to the increased MS risk among women, there is also a
suggestion of increasing MS risk among non-Caucasian populations. In a large
study of US Veterans, it appears that MS risk has changed in the US over a
single generation, and although the risk for developing MS among Caucasian
women has increased in comparison to Caucasian men, all women regardless of
race and ethnicity now have a significantly higher risk of MS than Caucasian
males (Wallin, et al. 2004). These data point to other causes of MS susceptibility
24
besides race and ethnicity, such a migration history and environmental risk. In
addition, Langer-Gould (2013) found that the incidence of MS was actually higher
in African Americans, and lower in Latinos and Asians than Caucasians. African
American women have a higher risk of MS, while African American men had the
same risk compared to Caucasians. These studies challenge the assertion that
non-Caucasian groups have a lower risk of MS than Caucasians, and that there
may be significant and rapid effects on MS prevalence which have not been
noted previously. At the very least, these studies suggest that race and ethnicity
and geographic location may have a decreasing influence on MS prevalence,
while a yet unknown environmental factor may play an increasing role in MS
prevalence.
In addition to different MS prevalence rates in different racial and ethnic
groups, there are physical differences in the manifestation of the disease
between racial and ethnic groups. Studies have identified what is called a
“Western type” of MS versus an “Asian type” of MS, the Asian type MS being
characterized by a higher age at onset, selective involvement of the optic nerve
and/or spinal cord (versus widespread demyelination of the brain in the Western
type), a higher number of lesions on spinal cord MRI, and a lower number of
lesions seen on brain MRI (Kira, et al. 1996). Studies in other countries attempt
to compare their population’s clinical course to either the Western or Asian type
of MS. Arab (Benamer, et al. 2009; Wasay, et al. 2006), Argentinian (Melcon, et
al. 2008), and Southeast Asian studies (Wasay, et al. 2006) have identified

25
similarities between their populations and the Western type of MS rather than the
Asian type of MS. Asian type MS seems to affect mostly East Asian populations,
such as in Japan, China, Hong Kong, Taiwan, Singapore, Thailand, Korea, and
Malaysia (Chan, et al. 2011; Tsai, et al. 2004; Wasay, et al. 2006). Recent
radiographic studies on MS are revealing different disease progression profiles in
those of Indian and African descent, again highlighting the potential for divergent
clinical presentations of MS (Cree and Waubant 2010).
It is important to note that prevalence studies, like the ones discussed
above, and even a global meta-analysis of prevalence studies, can only provide
a snapshot of what MS looks like at any given time point. Weaknesses include
merging together different formats of information from prevalence studies
conducted in different areas at different times using a variety of population sizes,
ages, ethnic origins, and migratory histories. In addition, the ascertainment of
MS cases is dependent on access to medical care, local medical expertise,
number of neurologists, accessibility of diagnostic procedures like MRI, and the
degree of public awareness of MS (Rosati 2001). Further, local practices may
inflate any perceived differences in prevalence rates due to a failure to
distinguish between clinical and MRI features of MS and other recurrent
inflammatory demyelinating diseases of the CNS, inclusion of cases with MS
onset prior to arrival in the study area, and the consideration of neuromyelitis
optica as a variant of MS. Thus any differences in race or ethnicity may also be
due to variability in diagnosis. Interestingly, in a clinical questionnaire survey that

26
was sent to 108 neurologists around the world, only two thirds of the 30 cases
presented to them were diagnosed correctly, meaning that on average, the
neurologists incorrectly diagnosed one third of the patients. Experience, country
of training, and specialization in MS made no difference in the error rate (Poser
and Brinar 2007).
The Causation Hypotheses
In an attempt to make sense of the epidemiological data and combine
them into a unified theory, the following hypotheses have been proposed to
explain the observed patterns and exceptions. For example, the latitude
hypothesis seeks to explain the greater prevalence of MS in higher latitudes,
such as in the northern portions of North America and Europe and in the
southernmost areas of Australia and New Zealand, and lower rate in populations
located closer to the equator. Many studies have demonstrated the increased
incidence, prevalence, and mortalities related to MS as degree of latitude
increases on either side of the equator (Noonan, et al. 2002; Risco, et al. 2011;
Simpson, et al. 2011). However, additional evidence points to a more nuanced
explanation than the latitude hypothesis, since many studies have shown that
either the latitude gradient of MS incidence is decreasing over time or that this
pattern does not actually hold true in certain areas of the world (Alonso and
Hernan 2008; Koch-Henriksen and Sorensen 2011; Melcon, et al. 2008; Wallin,
et al. 2004). The epidemiology of MS globally seems to indicate an increase in
prevalence of MS in all areas of the world independent of latitude due to

27
increased survival times, an increase in incidence of MS in women, and an
apparent lack of a latitudinal gradient in the northern hemisphere. Interestingly,
the north-south latitude gradient in the southern hemisphere seems to be
preserved, although at similar latitudes equidistant from the equator where you
would expect to see similar prevalence rates, Latin American prevalence is 21.5
per 100,000 persons while the US prevalence is close to 100 per 100,000
persons (Risco, et al. 2011). These exceptions and caveats counter the
traditional latitude hypothesis, but may point to a still related phenomenon,
namely, Vitamin D production.
A corollary of the latitude hypothesis is that exposure to ultraviolet
radiation, which aids in the synthesis and increased absorption of Vitamin D, has
been found to have immune system supportive properties, potentially preventing
the immune system from attacking its own nerve cells as is the case in MS.
Thus, greater exposure to ultraviolet radiation has neuroprotective effects on
these individuals, making it less likely that they would develop MS (Cristiano, et
al. 2008; Simpson, et al. 2011). For example, in France MS prevalence was
correlated with the geographic distribution of ultraviolet radiation (Orton, et al.
2011). Similarly, in Bulgaria an association was found with regional annual
sunshine hours rather than latitude (Kalafatova 1987). In Norway, summer
outdoor activities in childhood were associated with reduced risk of MS even
north of the Arctic Circle (Kampman, et al. 2007). Even if the latitude hypothesis
and north-south MS gradient may not hold true, there might be some connection

28
to ultraviolet radiation exposure which may then be mediated by genetic
disposition, additional environmental factors, and migratory patterns. Scientists
are still left with the question about whether genes provide susceptibility to
particular environmental triggers for MS or whether the environment influences
gene expression or a combination of both.
The hygiene hypothesis points to epidemiological studies that find
immunological and autoimmune disorders to be less common in developing
countries and more common in developed countries. The theory is that people
living in developing countries are able to build up stronger immunity due to higher
exposure to infectious agents when compared to developed countries. This
pattern was recognized as early as the mid-19th century when chronic
inflammatory disorders like allergies, inflammatory bowel diseases, Type 1
diabetes, and multiple sclerosis were on the rise (Rook 2012). Since those in
developed countries became less and less exposed to infectious agents through
modern urban development, they also became more susceptible to being
infected by viruses thought to provoke the development of MS, such as the
Epstein-Barr virus and the John Cunningham virus among others (Rook 2012).
It seems that a wide range of explanations exist for the variety of
incidence and prevalence rates of MS around the world, while the etiology of MS
remains unknown. Immunological, environmental, infectious, and genetic factors
have all been shown to increase the risk of developing the disease in varying
degrees and combinations. Most scientists speculate that certain people are

29
born with a genetic predisposition that can react to some environmental or
infectious agent that, upon exposure, triggers an autoimmune response.
Missing Pages of the Epidemiological Story
Much of the epidemiological story of MS seems to focus on a difference in
both prevalence rates and clinical presentation between racial and ethnic groups.
The uncertainty surrounding the cause and prevalence of MS is further
complicated by the fact that most of the data collected on individuals with the
disease represent primarily Caucasians. For example, in the North American
Research Committee on Multiple Sclerosis Registry, one of the largest patient
databases specific to MS with about 35,000 registered participants, 93% are
Caucasian, 2.5% are Latinos, and 4.5% are African American (Buchanan, et al.
2010). The paucity of information about MS patients who are not of Caucasian
descent makes it difficult to narrow down the potential causes of MS and
identifying who may be more susceptible to developing MS. In addition,
registries like this may, by its design, underrepresent less disabled, rural,
southern, and lower income persons with MS (Minden, et al. 2006). Upon further
inspection, among Latinos, African Americans, and Caucasians participating in
the North American Research Committee on Multiple Sclerosis Registry,
significant differences are observed between these groups on several factors,
including demographics, disease characteristics, and treatments. Caucasians
are typically older when experiencing their first MS symptoms and diagnosis.
Latinos report more mobility and bowel and bladder issues than Caucasians.

30
Latinos and African Americans report more depression than their Caucasian
counterparts. More Latinos have never had mental health or rehabilitation care
and more African Americans have never seen an MS neurologist (Buchanan, et
al. 2010).
In addition to the lack of racial and ethnic representation, differences in
prevalence rates and clinical presentations could be due to racial and ethnic
differences, which most medical researchers equate with biological and genetic
differences, but they could also be due to health disparities between Caucasian
and non-Caucasian populations. For example, the presence of comorbidities,
which are common in the general population, is associated with worse health
outcomes. In the MS population, 37% of patients report at least one comorbidity,
with high cholesterol, high blood pressure, and arthritis being the most common.
The risk of comorbidity was higher for males, older patients (over age 60),
African Americans, and those of lower socioeconomic status. Lower
socioeconomic status is associated with decreased access to medical care,
lower quality of care, adoption of poor health behaviors, increased psychosocial
stress, lower health literacy, and lack of social support (Marrie, et al. 2008;
Shabas and Heffner 2005). Because physical and mental comorbidities can
affect disease, clinical phenotype, diagnostic delay between onset and diagnosis,
disability progression, and quality of life, comorbidities may confound the
appearance that non-Caucasians have worse MS presentation than Caucasians
(Marrie and Horwitz 2010).

31
What much of the data seems to indicate is that racial and ethnic
differences do have some kind of influence on the prevalence of MS, but that this
genetic difference does not operate in a vacuum and is most likely mediated by
exposure to the environment, which in turn, is determined by human behavior,
migratory patterns, sociocultural norms, access to modern technology, political
structure, and economic forces. Researchers should be cautioned against the
use of race and ethnic categories to predict a more or less severe disease
course or to decide on a treatment regimen since race is difficult to define, even
biologically (Cree and Waubant 2010). As seen with heart disease, cancer,
diabetes, and a host of other diseases, health disparities that exist between racial
and ethnic groups act as a confounding factor.
In addition, some anthropologists argue that attacking a problem as
complex as how MS affects the entire life of an individual using the “objective”
lens through which medicine and science view disease may be entirely missing
important insight due to the structure of rigorous scientific methodologies
(Cassell 2002). Modern epidemiology has evolved into an increasingly method-
driven science that limits research problems to those that are strictly quantifiable.
Despite continued integration of epidemiology and anthropology, epidemiology
often translates the concept of culture to a “belief,” which fits within the natural
epistemology of Western medicine. This has the detrimental effect of turning
culture into “difference” which in turn increases the gap between patients and
providers (DiGiacomo 1999).

32
All of these competing, or more likely overlapping, hypotheses of MS
cause and prevalence point to a far more complex interaction of population
genetics, geographically determined environmental factors such as ultraviolet
radiation exposure and viral agents, cultural habits and behaviors, socio-
economic demographics, and access to medical care. Given the number of
unknowns about the causes and natural history of MS, the underrepresentation
of racial and ethnic minority groups in clinical research has been detrimental to
developing a comprehensive understanding of MS treatments that respond to the
disease course variety seen in different individuals.
33
Chapter 3 – Underrepresentation in Clinical Trials
Reporting Rates of Clinical Trial Participants by Race and Ethnicity
In 1993, the National Institutes of Health (NIH) passed the Revitalization
Act in an effort to increase women and minority participation in research. It
contained Public Law 103-43, which states that women and minorities must be
included in all clinical research studies, that cost is not an acceptable reason for
their exclusion, and that the NIH will support efforts to recruit women and
minorities in clinical research studies (National Institutes of Health 2001). The
intent of this mandate was to balance the burdens and benefits of research,
thereby improving the ethical principal of justice in clinical research originally
stipulated in the 1979 Belmont Report. The Belmont Report resulted from the
unethical treatment of African American men in the Tuskegee Syphilis Study
(National Commission for the Protection of Human Subjects of Biomedical and
Behavioral Research 1979). Despite this mandate, underrepresentation of racial
and ethnic minority groups remains pervasive in medical research across all
medical specialties.
The North American Research Committee on Multiple Sclerosis Registry
for MS patients indicates that disparities exist, not only in the participation of
racial and ethnic minorities, but in the demographic and clinical characteristics of
the racial and ethnic minorities who do participate in the registry. If
underrepresentation of racial and ethnic minorities groups in MS clinical trials
exists, then the MS community is at a significant disadvantage to attempt to
34
answer all of its questions about etiology, prevalence rates, natural history, and
finding more effective treatments, perhaps even a cure.
Surprisingly, the issue of underrepresentation in MS clinical trials is not
well characterized or described in the medical literature. No studies could be
identified that looked at whether underrepresentation in MS clinical studies
exists, let alone reasons for the underrepresentation. Aside from the North
American Research Committee on Multiple Sclerosis Registry, which reported
the proportion of its registry participants by race and ethnic group, little
information is available to help understand this deficit. What was readily
available in the medical literature were studies about underrepresentation of
racial and ethnic minority groups in many other different types of clinical trials,
namely cancer, cardiac, HIV/AIDS, asthma, diabetes and pain disorder trials.
The first step in understanding the underrepresentation is to review the reporting
rates of trial participants by race and ethnicity as required by the 1993 NIH
mandate. For example, in a comprehensive review of 156 randomized controlled
cardiac trials, race and ethnicity were only reported in 35% of the industry funded
trials. NIH funded trials reported at a higher rate of 67% but a significant gap in
reporting still exists despite the NIH mandate (Berger, et al. 2009). In a similar
review of 47 panic disorder trials, less than half reported racial and ethnic data on
their participants. But for those trials that did report this data,
underrepresentation of racial and ethnic minorities were revealed. Approximately

35
82.7% of participants were Caucasian, 4.9% were African American, 3.4% were
Latino, 1.1% were Asian, and 1.4% identified as Other (Mendoza, et al. 2012).
When looking at the reporting rates for 87 asthma trials, only 26%
reported the race and ethnicity of the participants. Of those trials that did report
race and ethnicity, none explained how the racial and ethnic group was
determined (whether by participant self-report or by researcher classification),
and none did an analysis of the race and ethnicity data (Frampton, et al. 2009).
Likewise, an even larger review of 253 diabetes, cardiac, HIV/AIDS, and cancer
trials were examined for race and ethnicity reporting, specifically targeted
because these are diseases with known racial and ethnic health disparities. This
review found that 59% of these trials reported race, but of these, 46% reported
only one or two racial categories. Surprisingly, in 43% of the trials that reported
race, the participant numbers did not add up properly. Data analysis by race and
ethnicity was reported in 2 trials out of the 253 total trials (Corbie-Smith, et al.
2003). Unfortunately, even in diseases with known health disparities, many do
not report race and ethnicity, and almost none conduct data analyses by race
and ethnicity.
Despite extensive recommendations in the literature and the 1993 NIH
mandate, reporting and analysis of demographic data is extremely inconsistent
and vague. Identifying underrepresentation and correcting this disparity is only
the first step along the path to improving clinical trial design and impact. Analysis
by demographics is the next step necessary to determine whether there are any
36
therapeutic differences by race or ethnicity to be identified and reported;
otherwise, the generalizability of the findings are thrown into question without a
truly representative sample of participants.
Are There Differences By Race and Ethnicity?
In addition to reporting the racial and ethnic breakdown of trial participants
and the participation disparities that exist, studies have looked at reasons for
these disparities and posited that underrepresentation is usually due to minority
distrust of research or the medical community in general. Much of this research
has focused on differences between Caucasians and African Americans. For
example, the effect of race and place of residence on cancer clinical trial
participation was assessed by comparing clinical trial accrual rate to cancer case
ratios. Both race and place were significant predictors of participation in both
therapeutic and non-therapeutic clinical trials alike. Caucasian, female, non-
Baltimore City catchment area persons of the wealthiest counties had the highest
participation rate. African American persons living in Baltimore City or the non-
catchment area had the lowest participation rate. Poverty level was not
significant but was retained as a confounder (Kanarek, et al. 2010).
Several phone surveys have been conducted with Caucasian and African
American individuals not associated with a medical center or particular disease to
understand if there are differences in willingness to participate in a clinical trial.
African Americans often display lower willingness to participate in trials than
Caucasians, even after adjusting for age, sex, and socioeconomic status.
37
African Americans also report higher distrust of research than Caucasians
(Braunstein, et al. 2008; Byrd, et al. 2011; Shavers, et al. 2002).
The impact that knowledge of the Tuskegee Syphilis Study6 has on clinical
trial participation has also been studied among African American and Caucasian
individuals. Using phone surveys, a significantly larger proportion of African
Americans (81%) had knowledge of Tuskegee than Caucasians (28%).
Knowledge of Tuskegee resulted in less trust of researchers for a greater
proportion of African Americans (51%) than Caucasians (17%). Approximately
46% of African Americans and 35% of Caucasian participants said this
knowledge would affect their future research decisions. Of these, 49% African
Americans versus 17% Caucasians would not be willing to participate in future
research at all (Shavers, et al. 2000).
Perhaps because distrust seems to be a recurring theme in understanding
why underrepresentation of minority groups exist, a 7-item index of distrust was
created by Corbie-Smith, et al. (2002) to measure different levels of distrust in
medical research. A phone survey revealed that African Americans are more
likely than Caucasians to not trust that their own doctor would fully explain
research participation and to say that their own doctor exposed them to
unnecessary risk. African Americans also had a significantly higher mean
6 The Tuskegee Study of Untreated Syphilis in the Negro Male was conducted by the United States
government under the Public Health Service and lasted approximately 40 years from 1932 to 1972. This study was conducted on 399 African American men from Macon County, Alabama who were deliberately denied effective treatment for syphilis in order to document the natural history of the disease, even after penicillin was discovered and proven to be an effective treatment in the 1940s (Brandon 2005).
38
distrust index score than Caucasians even after controlling for socio-
demographic variables, indicating that race and ethnicity on their own yield
differences in trust.
To further deconstruct different types of distrust, the 7-item index of
distrust was altered to differentiate between societal and interpersonal distrust
among Caucasians and African Americans. African Americans were found to
have higher societal distrust than Caucasians, but there was no difference
between the two groups on interpersonal distrust. Further analysis could not
explain the relationship between societal distrust and African Americans using
any of the following factors: trust in one’s doctor, experience of previous
discrimination, or awareness of Tuskegee (Durant, et al. 2011). A parent-report
survey on the likelihood that parents would let their children participate in
research found that minority parents reported more fear of allowing their children
to participate in research, but were just as likely as everyone else to consent their
child's participation if asked by their own doctor. All parents, regardless of race
and ethnicity, were afraid of their child being a guinea pig. Specifically, Latinos
had the highest fear score compared with Caucasian parents, while Asians were
the mostly likely group to participate in research. Low education level and public
health insurance were associated with higher likelihood of allowing their child to
participate in research (Svensson, et al. 2012).
Notably, these results seem to provide direct evidence contrary to the
previous studies’ results. While distrust seems to be a huge contributor to lower
39
clinical trial participation rates among African Americans and other racial and
ethnic minorities, there may be other contributing factors that trust may be
masking. When the notion of trust is divided into different types (societal and
interpersonal) and analyzed, the influence that distrust has on clinical trial
participation rates becomes murky. One could speculate that distrust could be
further divided into institutional distrust, governmental distrust, historical distrust,
or present distrust. The issue that causes low representation of minority groups
in clinical trials may be distrust, or it may be that the categorization of “distrust” is
a proxy for other yet unexplored issues contributing to this representation
disparity. Additionally, the connection between knowledge of Tuskegee and
lower willingness to participate does not seem consistent across studies, and
minority groups other than African Americans may have differing views on clinical
trial participation.
Several studies seem to provide more definitive evidence that the
proposed connection between minority groups and distrust is tenuous, or at least,
more nuanced than researchers previously thought. More phone surveys done
with African Americans and Caucasians did not reveal any differences by race in
knowledge of or about Tuskegee, and any knowledge of Tuskegee was not a
predictor of distrust in medical research (Brandon, et al. 2005). Additionally,
African American men of all ages were willing to participate in several different
types of studies and their decision to participate was motivated by civic duty,

40
monetary compensation, and a connection to the disease under study. Higher
participation was related to higher education level (Byrd, et al. 2011).
The willingness of racial and ethnic minorities to participate in clinical trials
could also be seen in reviews of actual participation data. A review of 20 health
research studies accounting for 70,000 patient participants found that African
Americans had a lower, non-significant consent rate than Caucasians while
Latinos had a higher, non-significant consent rate than Caucasians. For the
clinical intervention studies, African Americans had a higher, non-significant
consent rate than Caucasians and Latinos had a higher, significant consent rate
versus Caucasians. For surgical trials which reported minorities as one group,
minorities had a higher, non-significant consent rate than Caucasians (Wendler,
et al. 2006). Underrepresentation of minority groups in clinical trials is further
challenged when trial participation rates are reviewed by trial phase. There is
evidence that minority groups actually participate in Phase I clinical trials as
healthy volunteers more than Caucasians (Fisher and Kalbaugh 2011). Most of
the literature focuses exclusively on Phase III therapeutic trials, so these studies
may mask other important issues regarding minority participation in clinical trials.
Barriers to Clinical Trial Participation
While the degree of underrepresentation of racial and ethnic minorities is
yet understudied, many scholars have investigated potential barriers to minority
participation. Barriers to participation could be organized into three different
themes: patient barriers, structural barriers, and provider barriers (Calderon, et
41
al. 2006; Colon-Otero, et al. 2008; Corbie-Smith, et al. 1999; Eggly, et al. 2013;
Howerton, et al. 2007; Hussain-Gambles, et al. 2004; Joseph and Dohan 2009;
Penberthy, et al. 2012; Schmotzer 2012; Sheikh, et al. 2009; van Ryn and Burke
2000). Patient barriers often related to fear of experimentation or harm, mistrust
of medical community, transportation issues, lack of financial resources, work
and family time conflicts, lack of childcare, language, burden of number of visits
required, and when community outreach is involved, poorly developed ideas from
community leaders on research aims and characteristics (Calderon, et al. 2006;
Hussain-Gambles, et al. 2004; Schmotzer 2012; Sheikh, et al. 2009). Mistrust of
doctors, scientists and government were consistently reported and concerns of
ethical conduct of clinicians were identified, often with examples of exploitation,
like Tuskegee, although participants were misinformed about facts of study.
Many also incorrectly assumed that the informed consent form relinquished their
autonomy and gave clinicians legal protection. Despite many of these fears,
most were still in favor of medical research, but did not want to be a guinea pig
(Corbie-Smith, et al. 1999).
Structural barriers are related to clinical trial design that may inadvertently
exclude particular groups of people, such as racial and ethnic minorities. In a
unique trial design by Penberthy, et al. (2012), clinical trial eligibility and
invitations to patients were observed prospectively. Interestingly, African
Americans were more likely than Caucasians to be ineligible for the cancer
clinical trial being observed, but African Americans were more likely to be

42
ineligible due to mental status or perceived noncompliance, while Caucasians
were more likely to be ineligible due to study-specific or cancer characteristics.
However, if African Americans were eligible to participate in the trial, they were
more likely to refuse participation than their Caucasian counterparts, even after
adjusting for age, gender, study phase, and cancer type. Reasons for refusal
were slightly different between the two groups. African American refusal was
often because they were not interested in clinical trials, they experienced family
pressure, or they felt overwhelmed. Caucasians more likely refused due to the
extra burden of trial participation, concerns with randomization and toxicity, or
they have a specific treatment preference outside of the study (Penberthy, et al.
2012). Lack of insurance or underinsurance and lack of medical facility access to
trials, funding, and investigators also seem to be structural barriers to clinical trial
participation (Colon-Otero, et al. 2008).
Provider-related factors may also have a strong influence on recruitment
of underrepresented groups to clinical trials. Oftentimes, provider attitudes and
assumptions about potential trial participants can affect participation levels of
racial and ethnic minority groups. Clinicians, who are often responsible for
identifying and recruiting participants to trials, are affected by their own biases
and make judgments about how well they think a patient will be able to adhere to
a protocol, whether a patient is meticulous, proactive, compliant, a good
communicator, and embedded in strong social support networks, all for the
purpose of completing the trial in a timely and efficient manner (Howerton, et al.
43
2007; Schmotzer 2012). Clinicians have admitted to subjectively identifying such
“good study patients” to target their recruitment efforts (Joseph and Dohan 2009).
Research suggests that physician perspectives may also be influenced by
race and ethnicity and assumed socioeconomic status, even when controlling for
patient age, sex, disease status, depression, mastery, social assertiveness, and
physician characteristics. African Americans and low and middle socioeconomic
groups were perceived negatively by physicians, while Caucasians and upper
socioeconomic groups were perceived positively. Patient race was also
associated with physician assessment of patient intelligence, feelings of affiliation
toward the patient, beliefs about patient risk behavior, and medical adherence.
Patient socioeconomic status was associated with physician perception of patient
personality, abilities, behavioral tendencies, and role demands (Van Ryn and
Burke 2000).
These differences in physician perspectives may also be played out in the
actual invitations extended to potential clinical trial participants. Another study
video recorded oncology visits with 11 African Americans and 11 Caucasians
being invited to participate in a clinical trial. Analysis revealed that visits with
African Americans compared to Caucasians were shorter overall and included
fewer mentions of and less discussion of clinical trials. Also, visits with African
Americans included less discussion of the purpose and risks of trials offered, but
more discussion of voluntary participation (Eggly, et al. 2013). Additional
provider barriers include provider stereotypes and prejudices about difficulties
44
engaging with minority populations, deficient provider communication methods
(lack of compassion and respect, rushed discussion, defensive and patronizing
responses), misgivings about the scientific importance of a study questions, and
complete lack of provider awareness of clinical trials (Howerton, et al. 2007;
Sheikh, et al. 2009).
Facilitators to Clinical Trial Participation
Importantly, work has also been done to understand what motivates racial
and ethnic minorities to participate in clinical trials, what facilitators help influence
them, and what strategies have been identified to help further improve racial and
ethnic minority group participation. African Americans and Latinos shared
several motivators to trial participation including: having a disease without cure,
helping a family member who has the disease, wanting to find a cure for the
disease, staff being from same racial and ethnic group, providing childcare and
transportation, and the trial having a limited number of visits (Calderon, et al.
2006). Physician enthusiasm, good communication, clear and concise clinical
trial information, good provider-patient relationship, and caring and
understanding trial staff all seem to facilitate participation of racial and ethnic
minorities. A common motivation across racial and ethnic groups was appealing
to participants’ altruistic nature, willingness to help others, and want to contribute
to furthering medical knowledge. However, "conditional altruism” appears to be
the more accurate term since it is their willingness to help others that initially
inclines them to participate in a trial, but it is the perceived personal benefit that
45
actually informs the decision. Potential clinical trial participants would be less
likely to participate if they had willingness to help others but without the personal
benefit (Hussain-Gambles 2004; McCann, et al. 2010; Schmotzer 2012).
Suggested strategies to help increase participation of racial and ethnic
minority groups in clinical trials include solutions on a spectrum from the macro-
scale to the micro-scale. The following macro-scale solutions have been
identified: reforming the health care system for better health care access, provide
regulatory incentives for industry to enroll diverse populations, provide better
training for researchers to understand disparities and engage communities in
planning, enrollment, and dissemination stages of research, prioritize and fund
research through government agencies that address diseases affecting
underserved populations (which are less likely to be funded by industry), develop
programs to increase minority physicians, implement navigator programs to help
potential trial participants address the logistic barriers of trial participation, and
partner with nonprofits, local health departments, and private practices to
increase trial visibility (Colon-Otero, et al. 2008; Gross 2008). Providing better
education in school on the importance and purpose of research may also help
dispel any fears or misunderstandings (Corbie-Smith, et al. 1999).
Mid-level strategies might include institutional actions to try and increase
racial and ethnic minority participation. Successful strategies include
implementation of structural changes to induce and sustain minority accrual to
therapeutic cancer clinical trials via 1) leadership support, 2) center-wide policy

46
change, 3) infrastructural process control, data analysis, and reporting, and 4)
follow up with investigators (Anwuri, et al. 2013). Community-based recruitment
strategies have also been successful in recruiting more minority populations to
clinical trials by targeting faith-based institutions, health fairs, senior centers,
university employees, and physicians serving African Americans and Latinos or
other minority populations. Building a relationship with community leaders,
community advisory panels, or utilizing community-based participatory research
methods help with visibility and trust. Approaching community members as
partners and not subjects is essential (Cabral, et al. 2003; Coakley, et al. 2012;
Corbie-Smith, et al. 2007; De las Nueces, et al. 2012).
Micro-scale strategies highlight the importance of interpersonal
relationships in recruiting for clinical trials. Honest and respectful
communication, sharing full knowledge of the risks and benefits of research in
different formats, having appropriate time to consider with family and friends, and
having the study physician available for questions at any time for the duration of
the study are all vital components of building a strong provider-patient
relationship (Coakley, et al. 2012; Corbie-Smith, et al. 1999; Corbie-Smith, et al.
2007). Specific tailoring of these strategies is likely required depending on the
local context of the health care facility, local population, and regulatory
requirements. For example, African Americans and Latinos in South Carolina
were asked to assess solutions to commonly cited barriers to clinical trial
participation. Common responses between the two groups included addressing

47
trial costs to the participant, recruiting in community contexts, providing
community and individual education on trials, and sharing patient safety
information. African American specific solutions included diversification of the
research staff, recognition of past research abuses, and increasing community
trust. Latino specific solutions included provision of low-literacy materials,
provision of Spanish-speaking doctors and advocates, and clarification that
immigration status does not get documented or prevent trial participation (Ford,
et al. 2013; Symonds, et al. 2012).
Finally, issues with informed consent are often cited as barriers to
recruitment so strategies focusing on how to tailor consent forms to the local
racial and ethnic minority population should be considered, as well as
alternatives to the traditional written informed consent for those from cultures with
no previous experience with clinical research or human subject’s protection.
Written translations of informed consent forms are often of limited value if
patients have limited or no knowledge of English. Tape recorded audio consent
should be considered acceptable rather than written consent and considerations
for familial consent rather than individual consent may also be required to
accommodate differences in decision-making practices among racial and ethnic
minority groups (Adams, et al. 2007; Ryan, et al. 2008; Sankar 2004).
Precautions
The existence of underrepresentation of racial and ethnic groups in clinical
trials can be seen in a number of disease indications including cancer, cardiac,

48
HIV/AIDS, asthma, diabetes and pain disorder trials. There are indications from
the North American Research Committee on Multiple Sclerosis Registry that
underrepresentation may also exist for MS clinical trials, but there are no studies
to date that have been completed. Barriers to clinical trial participation for
minorities are plentiful, but the majority seems to center around issues of patient
distrust, provider bias, and structural obstacles including access to health care,
and transportation, financial, childcare, and time constraints. The selection of a
representative sample from the larger population to participate in a clinical trial is
critical for the results of the trial to be valid and for those results to be
generalizable to the larger population. The consequences of not having a
representative sample for a clinical trial can result in incorrect conclusions about
a drug’s safety or efficacy for the general population, or overlooked safety and
efficacy differences between particular subgroups.
For example, during a statin drug trial to reduce cardiovascular disease,
only 16.3% of trial participants were women, while women make up 45% of the
general population with statin needs. Those aged 65 and older made up two-
thirds of the statin needs population while the same group made up only one fifth
of the trial sample. Although no severe consequences have been reported,
association of side effects with socio-demographic factors was only revealed in
follow up data analysis after drug approval, and not during the clinical trials
(Bartlett, et al. 2005). Similar to sex and age underrepresentation, if race and
ethnicity are not appropriately represented in a trial, evidence can be skewed to
49
show drug effectiveness and safety when it might not exist or it could exist at a
different effectiveness and risk level for particular socio-demographic groups.
Underrepresentation can bias any effectiveness or safety estimates.
Alternatively, underrepresentation of a particular group can also prevent a helpful
medication from reaching an audience who could benefit from its use. This was
the case with an improper subgroup analysis by gender, which resulted in aspirin
treatment being withheld from women in the prevention of stroke for 20 years
until an appropriately designed trial showed that aspirin therapy is also beneficial
to women for the prevention of stroke (Kreatsoulas and Anand 2009; Ridker, et
al. 2005).
Although the risks, remedies, and consequences of underrepresentation
of racial and ethnic minorities in clinical trials have been well documented, the
numerous causes of participation disparities offer conflicting evidence of what
might be driving this phenomenon. Some studies have pointed to distrust of
research, particularly in the African American community, which leads to
unwillingness to participate, while others have found that levels of distrust, even
knowledge of Tuskegee, does not influence minority willingness to participate. In
fact, there is evidence that minority groups are just as willing as their Caucasian
counterparts to participate in medical research, but either 1) provider bias results
in inequitable trial discussions, 2) minority groups are not asked to participate in
the first place, and/or 3) minority groups are less likely than Caucasians to have

50
health insurance which often provides access to medical facilities and the clinical
trials conducted within (Fisher and Kalbaugh 2011; Hasnain-Wynia, et al. 2007).
The equitable inclusion of all racial and ethnic groups in clinical trials is a
noble and ethically necessary goal, but explicit consideration of race and
ethnicity as a prerequisite for trial participation does raise some concerns worth
exploring. What is still unclear in many studies thus far is the process by which
the low participation rates of minority groups are determined. The proportions of
racial and ethnic groups should be a reflection of a variety of contextual factors,
namely geographic variations in demographics, differences between urban and
rural populations, differences in prevalence rates depending on the disease in
question, and differences in which groups have access to the medical centers
conducting the trials. The question of underrepresentation may need to be
revisited depending on the particular context the underrepresentation is taking
place. What exactly constitutes the “right” prevalence of racial and ethnic groups
in a clinical trial? The racial and ethnic make-up of participants in a clinical trial
could be designed to match that of the general population. It could be designed
to match that of the disease under examination. If designed to match the
disease under examination, researchers could look at prevalence, incidence,
burden of disease, or outcomes. Once a proper prevalence rate is chosen,
proper analysis of racial and ethnic subgroups in clinical trials needs to be
considered. In order to assess the consistency of study findings across different
groups, oversampling of racial and ethnic minorities would be required. If the
51
real intent of clinical trials is to produce results that consider differences in safety
and efficacy by racial and ethnic group, then these considerations need to be
incorporated into the trial’s initial design. The consequences of attempting to
include racial and ethnic minorities in research without properly considering trial
design can result in inaccurate conclusions of racial variations in therapeutic
efficacy when none exists, or vice versa (Rathore and Krumholz 2003).
Another consideration for explicitly including racial and ethnic minorities in
clinical trials is determining whether or not race and ethnicity categories
constitute biological differences that have real effects on trial outcomes. There
are considerable dangers to assuming race and ethnicity are biological
constructs rather than social constructs. More likely, race and ethnicity are
proxies for a mix of genetic, disease, social, behavioral, and clinical
characteristics that vary and overlap by group. Using race and ethnicity rather
than the specific factor causing the difference, results in pseudoscientific
rationalizations of categorization. Also, the fact that race and ethnicity are
determined either by the physician based on a subjective assessment on what he
thinks the patient looks like, or by patient’s perceived or self-reported race and
ethnicity, may not capture the supposed difference between groups (Acquaviva
and Mintz 2010; Rathore and Krumholz 2003; Schwartz 2001). Thus, race and
ethnicity should not be considered equivalent to genetic or biological differences,
nor should they be considered equivalent to socioeconomic status.

52
Chapter 4 – The Anthropology of Clinical Trials
The Inclusion-and-Difference Paradigm
The 1993 NIH Revitalization Act changed the face of clinical research
through its requirement that researchers actively recruit previously
underrepresented groups such as women, children, the elderly, and minority
groups. Although underrepresentation of racial and ethnic groups is still rampant
in the medical literature, a lot of attention is being paid and resources allocated to
remedying this gap. Interestingly, the NIH mandate encompasses two seemingly
opposing goals: 1) to include members of groups who have been previously
underrepresented as subjects in clinical trials, and 2) to analyze the differences
that exist between these groups related to treatment effect, disease programs, or
other biological processes. The slow but powerful adoption of this “inclusion-
and-difference paradigm” was promoted by biomedical reformers, including
policy makers, scientists, clinical providers, and patients, who argued for greater
inclusiveness in clinical trials.
These reformers framed their arguments in five distinct ways. First and
foremost was the focus on underrepresentation of minority groups in research,
which helped make the case for inequity by focusing attention on inclusion
statistics. Secondly, well-intentioned regulations were critiqued as misguided
protectionism resulting in paternalistic systems that only served to neglect
specific populations. Not only were the risks of research being removed from
these “vulnerable populations,” so were the benefits. The AIDS activist
53
movement served as a fulcrum to push for the right of patients to choose to serve
as guinea pigs, to access experimental drugs, and to consider access to
experimental trials a social good (Epstein 2007). Third, false universalism has
extended the experience of Caucasian males, as the dominant group in society,
to represent the general population and universal experience. Finally, both
health disparities and biological differences point to the negative consequences
of inadequate inclusion of underrepresented groups in clinical research (Epstein
2007).
Although reformers rejected the idea of the universal human, they failed to
advocate for clinical research to produce individualized therapy. Instead of
focusing on the medical uniqueness of each individual, reformers proposed the
standardization of medical therapy, not for one type of person, but for specified
human groupings: women, children, and racial and ethnic groups. Even in
medicine itself, the language of individualism is used even though the policies
developed are aimed at social groups. For example, according to an article in
Science, “Since the early 1980s, the FDA has been interested in the
individualization of therapy, that is, determining whether and how treatment
should be modified for various demographic groups within the population”
(Epstein 2007: 139). Using the terms individual and group interchangeably is a
common feature of the inclusion-and-difference paradigm. This flexibility
provides the paradigm with legitimacy through the association with individualism,
an ever-present value upheld by American culture. On the other hand, the
54
grouping of individuals into demographic groups may reflect the reality that
medical science and technology is not yet able to tailor medications and
treatments to individuals, and instead merges tenuous categories of individuals
together with little evidence that significant differences actually exist between
them.
Ultimately, though, the reformers did not simply presume the biological
significance of categories; they reinforced this perception. The irony of the
inclusion-and-difference paradigm is that while health inequalities by race and
ethnicity are a very real and overwhelming social problem deserving significant
attention, the focus on race and ethnicity as a proxy for biologically based
differences is not the way to address them. The focus on biology is misplaced
because there is an assumption that the categories created to include specific
groups of people by scientific and government entities are in fact based in a
biological reality that can be clearly delineated. While seeking to reduce
inequalities between groups, the inclusion-and-difference paradigm only serves
to reshape how we think about sex, gender, race, and ethnicity in that it
encourages and reinforces these ways of differing as attributable to strictly our
biological makeup.
Biopolitical Citizenship and the Illusion of Race
Citizenship can be understood as the different ways individuals or groups
are fully or partially incorporated into the national polity which is mediated by the
notion of member rights and responsibilities. Biology has become grounds for
55
social membership in a group and the basis for staking citizenship claims
(Petryna 2002). Other forms of group classification have been created which
also provide a basis for affiliation and include all those who share a disease, a
treatment, a genetic risk factor, an exposure, gender, or racial and ethnic group
(Rabinow 1996). Because of increased attention on the effect classification has
on social actors, many concepts have been offered to understand this
phenomenon including, “biological citizenship,” “genetic citizenship,” “therapeutic
citizenship,” and “sanitary citizenship” (Briggs 2005; Briggs and Mantini-Briggs
2003; Epstein 2007). For Epstein (2007), all of these concepts can be combined
into the concept of “biopolitical citizenship” because those promoting inclusion of
underrepresented groups in clinical trials were looking for more than just
representation in a quantifiable sense; they were looking for inclusion into society
for political representation. This biopolitical citizenship points to the political
nature of making claims to these groupings and being able to control their
meaning. The ability of individuals or groups to lay claims to the full rights and
responsibilities of this citizenship is dependent on the influence that the
biomedical industry has on creating and transforming these categories into tools
of social stratification and exclusion.
It is helpful to conceptualize the clinical encounter as an interaction
between patient, as potential clinical trial participant, and provider, as gatekeeper
to the clinical trial. This singular encounter, which occurs within a particular place
at a particular time, is the result of the regulatory, political, medical, institutional,

56
social, cultural, and personal forces intersecting and influencing their actions.
When this encounter is influenced by meanings of biological difference and the
status of socially subordinated groups, new and generally accepted ways of
categorizing patients and bodies are created. These classification systems
reflect prevailing hierarchies of power (Farmer 2006) and help shape social and
moral order where benefits are distributed on the basis of categorical
membership. Briggs (Briggs 2005; Briggs and Mantini-Briggs 2003) refers to the
way that social actors seek to control the production, circulation, and reception of
public discourses about difference as the politics of “communicability.”
The idea that every citizen is shaped through the everyday acts of creating
hierarchies of communicability is powerful in explaining the evolving and dynamic
relationships that exist between medical researcher and the community.
Communicability is the central dimension of self-regulation and self-control, in
which individuals find themselves disseminators, receivers, or not in the loop at
all. In the clinical trial industry, communicability connects medicalization and
racialization to explain how theories about medical causation constitute ways of
thinking about the world and acting on it. Narratives about underrepresentation
of racial and ethnic minorities in clinical trials seem natural when explained by the
medical community as a result of minority distrust. These racialized populations
are then deprived of any agency, and become either passive victims (who lack of
knowledge and resources), or targets of blame. As a result, medical profiling of
patients can occur where clinicians assume that members of certain communities

57
are less likely to be capable and cooperative patients. Those who can
demonstrate the subjectively determined characteristics of a compliant and
proactive clinical trial participant are acknowledged as “sanitary citizens,” while
those who are deemed to be incapable of adopting these characteristics become
“unsanitary citizens” (Briggs 2005).
This medical and racial profiling is used on a large scale when attempting
to ameliorate the underrepresentation of minority groups in clinical trials. The
remedy to underrepresentation is to increase representation of minority groups,
without true consideration of what their inclusion means. Many researchers
openly defend race as a legitimate framework for analyzing genetic difference in
disease risk (Gravlee and Sweet 2008). Models in health research treat race as
a “black box” and fail to explore how race actually impacts health. As a result of
the assumption that race is a legitimate and meaningful classification, its
continued use seems rational, logical, and incontestable (Hunt, et al. 2013). In
fact, race and ethnicity are the most commonly used variables in health research
and the use of these variables is on the rise. Despite their pervasive use, the
concepts of race and ethnicity are rarely defined (Gravlee and Sweet 2008).
However, over the past two decades, more health researchers, as well as
anthropologists, have become increasingly critical of using race and ethnicity as
a biological construct.
Genetic studies actually show the recency of our common ancestry and
continuous gene flow exchange which results in less genetic variation among
58
human populations than many other non-human mammals (American
Anthropological Association 1998; Jablonski 2004; Kuzawa and Sweet 2009;
Race Ethnicity and Genetics Working Group 2005). In fact, genetic data show
that no matter how racial groups are defined, two people from the same racial
group are as different from each other as two people from two different racial
groups (American Anthropological Association 1998). In addition, skin
pigmentation, often used as a subjective determinate of race, is a recent human
adaptation and its evolution has been influenced by environmental conditions
rather than genetic differentiation. Thus light or dark skin only provides evidence
of past environments, and is not a unique marker for a particular race (Jablonski
2004).
Even if one assumes that racial and ethnic categories are a proper genetic
representation of unique human groupings, our current understanding of genetics
remains problematic. For example, Marks (2002) argues that the recent
discovery that human and chimpanzees share 98% of their DNA structure is
flawed. Depending on the techniques used and DNA segments that are
compared, the rate of similarity can be widely varied. In addition, genetic
expression of a particular DNA segment (or epigenetics) seems to vary
depending on the particular individual, which scientists speculate may be due to
environmental exposure, diet, exercise, geographic location, or a host of other
social and cultural influences. For example, given the same DNA segment
between two individuals, the one who is more likely to have a particular vitamin in
59
his diet may result in 100% gene expression while the one who does not have
that vitamin in his diet may only have partial or no gene expression. Thus, even
genes by themselves do not determine a specific gene expression. Because of
this and because there is similar genetic variation among all humans,
identification of discrete genetic groups has been impossible (Marks 2002).
Race and ethnicity are social and cultural constructs that categorize
people based on perceived differences in biology or physical appearance.
Categorization of groups of people by race has been and continues to be
controversial because of the numerous ways these invented categories have
served to rationalize mistreatment or justify exclusion. Categories of race have
historically been used to achieve political ends (such as during the Holocaust and
slavery), without true consideration of biological differences. These perceived
differences have their roots in a European taxonomy which was solidified after
Columbus sailed to the Americas. It was used as a way to determine the
absolute biological, behavioral, and cultural differences between races that not
only served to create arbitrary categories of race, but categories which served
the basis for ranking the superiority of races.
The fluidity of racial and ethnic categories is appreciated when considering
their history and change over time. For example, Irish, Italians, and Jews were
all considered to be racial groups in the early 20th century, distinct from the white
population. Today, we observe that these same groups are now considered to
be part of the majority white racial group (American Anthropological Association
60
1998). In addition, health research often relies on the racial and ethnic
categories developed by the US Census which were not created based on a
scientific, biological understanding of race, but on a mixture of criteria, including
national origin, language, minority status, and physical characteristics in an
attempt to represent true differences between groups of people (Kuzawa and
Sweet 2009). Racial and ethnic categories are also conceptualized differently
outside of the US, again showing that the construction of racial and ethnic
categories is the result of social and cultural preconceptions (American
Anthropological Association 2011). An additional incongruence exists between
these racial and ethnic categories and the way people choose to self-identify.
Individuals of the same “race” may choose to identify themselves differently.
Also, an individual’s association with a particular racial group may also be fluid
and change over time (American Anthropological Association 1998).
When attempting to identify the reasons for underrepresentation of
minorities in clinical trials, racial and ethnic minority group distrust of research
and medicine is often invoked as a reason for low participation rates. To the
contrary, there is ample evidence suggesting that regardless of feelings about
distrust, minority groups are just as willing as their Caucasian counterparts to
participate in a clinical trial. Other structural confounders may also explain low
participation rates, such as provider bias and access to care. The continuous
recycling of distrust as a reason minority groups do not participate in clinical
research only serves to “blame” the disparity of participation on a particular
61
attitude of the minority group in question. When framing these discussions in the
context of spheres of communicability, how much of the discourse currently used
to try and improve disparities in minority participation only serve to maintain the
difference, distrust, and paternalistic relationship between medical researchers
and potential clinical trial participants?
Recruitmentology
Despite the concerns raised about medical and racial profiling when
recruiting minorities for clinical trials, Epstein (2008) has identified the emergence
of a new science that he calls, “recruitmentology,” which seeks to develop an
empirical body of evidence evaluating the efficacy of particular social, cultural,
psychological, technological, and economic strategies to convince people to
participate in research studies. Practitioners attempt to generate and
disseminate knowledge about how to successfully recruit and retain participants
in clinical trials, particularly those considered to be hard to recruit populations.
Many of the current techniques borrow cues from the marketing and advertising
worlds. For example, in a new clinical trial studying a novel infusion therapy for
MS at BAMC, all study literature and patient information is tagged with the name
of the study and its slogan: “OPERA: The sound of a new research opportunity in
MS.” Similarly, a non-profit organization called The Center for Information and
Study on Clinical Research Participation (CISCRP), attempts to engage and
inform the public about clinical research. CISCRP invites those who have
participated in a clinical trial to join their “Medical Hero Community” which serves
62
as a public service campaign to assist the public in thinking differently about
clinical research (Center for Information and Study on Clinical Research
Participation 2014).
As more and more portions of clinical trial activities are being outsourced
to private companies, recruitment is often turned over to for-profit companies who
specialize in recruitment of trial participants. This specialization is transforming
the art of recruitment into an actual science through establishment of quantitative
measures of recruitment effectiveness (i.e., cost-benefit analysis of recruitment
efforts and potential subject “yield”). The science of recruitmentology, to its
credit, has recognized the need to address the collective memory of racism and
research abuses, distrust of research, fear of experimentation and perceived lack
of benefit. Additional efforts have focused on highlighting the altruistic side of
clinical trial participation. Still others have looked at research positionality and
have recognized the relative success of recruitment based on a researcher’s
embeddedness and connectedness within community networks. Others have
attempted to create a body of evidence for particular cultural groups, such as
how confidentiality issues would affect potential participants in rural areas, or
how the family orientation of Native Americans may affect researchers’ ability to
enroll Native American participants. However, caution must be applied here
since these categories are treated by practicing recruitmentologists as static and
homogenous groups that are knowable and unchanging (Epstein 2008).

63
Significant attention is paid to the issue of distrust in recruitmentology.
Trust is described in the context of historical abuses of patients by researchers,
of which Tuskegee is not the only event to contribute to the collective memory of
research abuses and unequal power relations. Additional historical examples
cited include the use of slaves for medical experimentation in the pre-Civil War
South, the use of black cadavers for dissection in the 19th century, legends about
“night doctors” in the post-Civil War period who were hired to kidnap blacks in the
South to use in medical experiments, the Tuskegee syphilis patients who were
denied treatment even though treatment was available for nearly three decades,
the HIV/AIDS epidemic, and the presence of drugs in black neighborhoods which
is related to a claim that the CIA deliberately pushed the sale of crack cocaine in
black neighborhoods (Epstein 2008). Although Tuskegee is often used and
mentioned as a placeholder of the source of mistrust, it only serves to mask a
real consideration of the broader set of historical and political issues affecting
minority groups and their willingness to participate in clinical research.
Trust-building can be directly related to transforming the imbalance of
power that exists in the provider-patient relationship (Grimen 2009). Epstein
(2008) recommends that building trust can be accomplished using a variety of
methods such as participatory action research and community-based
participatory research. These methods involve a reciprocal relationship with a
mutually beneficial exchange of knowledge and resources. “Drive-by” research
is discarded for a true, long-term commitment and relationship to the community.

64
While the inclusion-and-difference paradigm attempts to remedy the
underrepresentation of minority groups by promoting the use of race and
ethnicity as distinct biological groups, the science of recruitmentology seeks to
solve deep, historical issues of trust by scientifically engineering strategies to
induce cooperation and participation of these underrepresented groups.
Unfortunately, the use of race as a biological construct may undermine the larger
goal of eliminating health disparities which are mostly due to sociopolitical
causes rather than biological. In addition, the attempt to better recruit minority
groups to clinical research by scientifically engineering recruitment efforts does
not serve to change the power dynamic in the provider-patient relationship. In
this sense, the problem of minority recruitment remains a problem to be solved or
socially engineered by the researcher, rather than a problem of social
relationships governed by positionality and embeddedness in arenas of power.
Risk
Remarkably, little attention is paid to the concept of risk in the debate over
underrepresentation of racial and ethnic minorities in clinical trials. Much effort is
spent trying to understand the causes of underrepresentation by attributing the
existing participation disparities to an intrinsic cultural factor, distrust, with
variable results. Then potential strategies for correcting this underrepresentation
are elucidated. Although this is not a frivolous exercise, a discussion of the
causes and solutions to underrepresentation cannot be comprehensive without
thorough consideration of risk and risk perception. Perhaps the lack of

65
discussion is due to the fact that participation in clinical trials carries inherent
risks that both researchers and patients are aware of and assume no further
attention is required. However, risk may be the most salient issue to consider
when trying to understand minority underrepresentation in clinical trials. The use
of distrust in minority populations to explain underrepresentation has not yielded
consistent findings and this could be because participation is mediated by a
related but separate concept, risk perception.
Risk is not an unknown concept to many MS patients. Current MS
treatment options carry significant side effects, and oftentimes the choice
between treatments is a choice, not of fewer side effects, but acceptable side
effects. Much time is spent by the MS medical community to evaluate, monitor,
and quantify therapeutic risk. The MS field is at a unique point in its history since
there has been an explosion of treatment options in the past decade. This is
remarkable considering that the first MS medication was available in 1993, a little
over 20 years ago. Since then, different types of therapeutics have been
developed, each with their own treatment benefits, modes of administration, and
risk profiles. Attempts to generate a general risk algorithm for all MS treatments
have been difficult considering this ever-changing therapeutic landscape (Clanet,
et al. 2014). Risks related to specific MS medications have also been difficult to
understand because comparison of “actual” risk (quantified, statistical risk of a
particular side effect) often does not match patient perceived risk. MS patients
treated with natalizumab and mixantrone were often willing to accept a higher
66
risk of side effects than their neurologists (Heesen, et al. 2010; Hofmann, et al.
2013). There may also be a difference between risk perception and risk
acceptance. Risk perception is when patients perceive and interpret risk
differently from others; risk acceptance is when patients may perceive a risk to
be high but determine that it is an acceptable risk to take (Tur, et al. 2013).
This approach to understanding risk, through use of calculated
probabilities and epidemiologic statistics, dominates research in the health
sciences. In epidemiology, risk is calculated as the probability that something will
occur given a specific population and risk factor relative to a reference population
(Frankenberg 1993; Launiala and Honkasalo 2010). This approach is often used
to assist clinicians and patients make “objective” decisions about a medical
intervention. However, it is often the case that even if individuals perceive
themselves to be at significant health risk, they do not take the identified
measures to reduce that risk. The conception of an “objective” and calculable
risk is at odds with local experience and perceptions of identity. Given the same
danger, people do not consider themselves equally at risk of harm (Nichter
2001). Risk perceptions are influenced by a process of cultural interpretation,
disease identity, and personal meanings of vulnerability, agency, and perhaps
trust (Goldade and Nichter 2010).
Anthropologists critique the epidemiological approach to risk as failing to
account for the complex sociocultural context within which risk is situated
(Frankenberg 1993; Launiala and Honkasalo 2010; Lupton 1999; Trostle 2005).

67
This critique was first cited in the work of Mary Douglas (1992) on risk and
blame, in which she identified the disadvantages to risk analysts’ assumptions.
In an effort to avoid bias and politicization, risk researchers purposefully chose to
omit considerations of culture, politics, and morals in search of objectivity
(Douglas 1992). Because of these shortcomings, social scientists have
attempted to move beyond the medicalization of risk and the individualistic risk
paradigm into risk behaviors that are understood within their respective social
and cultural contexts (Frankenberg 1993; Sommerfeld, et al. 2002). Medical
anthropologists have taken this approach to risk further by pushing for an
examination of the structural forces that exist, such as poverty, inequality, access
to health care, and health economics, which contribute to risk perception
(Farmer, et al. 2006; Sommerfeld, et al. 2002). Taking these macro level factors
into consideration makes it clear that individual risk behavior and perceptions of
risk are severely limited and mediated by intersecting agencies of power.
68
Chapter 5 – Research Design
Research Questions
The intent of this project is to better understand the complexities
surrounding MS clinical trial participation, in the context of underrepresentation of
minority racial and ethnic groups in clinical trials, the unknowns that exist about
MS etiology and prognosis, and the conflicting evidence on whether reasons for
participation are related to distrust as the medical literature seems to suggest, or
some other unknown factor. In order to explore these issues in more detail, I set
out to answer three main research questions:
1. Is there underrepresentation of racial and ethnic minority groups in MS
clinical trials? If so, why?
2. In what ways do preconceptions about medical research, altruistic
motivations, and daily experience with disease contribute to MS
patients’ participation in clinical trials?
3. What are the salient MS patient attitudes towards clinical trials?
Research Methods
A mixed-methods approach was utilized to answer the three research
questions. First, archival data were reviewed for all MS patients being seen at
BAMC to identify whether the racial and ethnic group proportions matched the
racial and ethnic group proportions of the general MS population. The racial and
ethnic makeup of MS patients who had participated or were currently
participating in clinical trials at BAMC were compared to the findings from this
69
review to determine whether there is underrepresentation of minority groups in
BAMC clinical trials. Second, an electronic survey was administered to capture
opinions from MS patients regardless of their exposure to or knowledge of clinical
trials. Third, semi-structured interviews were conducted with MS patients who
have experience participating in a clinical trial to provide depth to the topic and
rich context for thematic analysis.
Archival Data
In the original study design, I wanted to understand the proportion of MS
patients who had been invited to participate in a clinical trial, the number of that
group who had accepted or declined, and whether there were any differences by
racial and ethnic group. To do this, a search of BAMC's electronic medical
record database was conducted. In theory, the database could be used to
search and extract from clinic notes whether or not patients with an MS diagnosis
with reported gender, race, and ethnicity were invited to participate in research,
whether they accepted or declined, and any other reasons noted for the
acceptance or decline. Unfortunately, this database review of MS patients
revealed that I would not be able to ascertain which patients had been invited to
participate in a clinical trial, nor whether a patient had declined or agreed. There
was no formal section of the electronic medical record where a clinician could
document that a patient was participating in a clinical trial. In lieu of this, I
attempted a key word search in the text of every clinic note to see if I could find
mention of clinical trial invitations during clinical encounters. In an attempt to be
70
as inclusive as possible, general search terms such as “trial,” “research,” and
“study” were used but did not reveal any documented clinical trial discussion.
Often these words were used interchangeably in documenting a patient’s regular
medical care (i.e., try a different medication for a “trial” period). Thus, it appeared
that information about clinical trial invitation, acceptance, or decline was not
documented in any official or unofficial way in the patient’s medical chart. Given
this constraint, the database review was then used to learn the number of total
MS patients served by BAMC’s MS Clinic. Additionally, the racial and ethnic
make up of the MS patient population was obtained to reveal if BAMC’s MS
patient population matches that of the US and whether underrepresentation of
minority groups in clinical trials exists at BAMC.
Because there are no studies to date documenting whether
underrepresentation exists in MS clinical trials (except for the North American
Research Committee on Multiple Sclerosis Registry), the government website,
ClinicalTrials.gov was reviewed to determine participation rates of minority
groups in MS clinical trials across the US. ClinicalTrials.gov is a web-based
database that is maintained by the National Library of Medicine and the NIH.
This website was created as the result of the Food and Drug Administration
Modernization Act of 1997. The FDA Modernization Act required the NIH to
develop a registry of clinical trials for both federally and privately funded trials
conducted under investigational new drug applications. The website was made
available for public use in February 2000. Additional requirements were
71
expanded in the FDA Amendments Act of 2007. The FDA Amendments Act
required that more types of trials be registered and additional trial information be
submitted. In addition, the law required submission of results for certain trials,
which can now be found in the ClinicalTrials.gov results database which contains
information about study participants, such as total number of participants,
participants by sex, race, ethnicity, and disease status (National Library of
Medicine and National Insitutes of Health 2014). The demographic data
gathered from Clinicaltrials.gov provided information about MS clinical trial
participants across the country by race and ethnicity and serves as a comparison
to BAMC’s MS population.
Electronic Survey
An electronic survey was developed using REDCap, which is a secure,
HIPAA7 compliant, web application for building and managing online surveys.
Because the database search did not reveal any documentation of actual clinical
trial invitations or trial acceptance or declines, the survey was created to
understand whether MS patients had ever been invited to participate in a clinical
trial, what their primary reason would be for accepting or declining participation in
a trial, and their general knowledge of and views towards clinical trial
participation. Potential reasons for acceptance and declination were adopted
from common reasons for trial participation identified in the medical literature.
7 HIPAA is the Health Information Portability and Accountability Act which provides federal protection for
individually identifiable health information.
72
The survey had a total of 34 questions including demographic questions at the
end.
All BAMC MS patients were eligible to participate. MS patients were
chosen from the total list of 1,439 MS patients being seen at BAMC. In May,
June, and July 2014, surveys were administered to MS patients in four waves.
The first wave of invitations was emailed to 102 MS patients with an email
address listed in their electronic medical record regardless of race and ethnicity.
The second wave of invitations was emailed to 24 MS patients with an email
address listed in their medical chart, specifically targeting non-Caucasian
patients. A significantly lower proportion of non-Caucasian patients had an email
listed in their medical chart (26%) than Caucasian patients (68%). Because of
this, it was exceedingly difficult to target non-Caucasian patients by presence of
an email address alone in the electronic medical record. Thus, a third wave of
invitations was sent by mail to 68 non-Caucasian MS patients at their listed
address, which instructed them to go online and take the electronic survey.
Finally, a fourth wave of invitations was emailed to 60 Caucasian patients in an
attempt to increase participant numbers. Out of 254 invitations to participate in
the survey, only 48 patients responded (19% response rate). Of these, 37 were
Caucasian and 11 non-Caucasian (seven Hispanic/Latino, three Asian, and one
African American patient). The survey served as a validity check against data
gathered during the archival data review and semi-structured interviews. Survey
data were analyzed using SPSS (Version 21.0).

73
A major limitation of the survey is the fact that it was created only as an
electronic survey to be administered online. Even when I attempted to remedy
the oversampling over Caucasian MS patients by sending the survey invitations
in the mail rather than by email, patients were still required to have access to a
computer with an internet connection to complete it. Because I designed the
survey to be anonymous to protect the confidentiality of MS patients, no link was
available for me between survey responses and patient to determine which
patient from which invitation wave decided to complete the survey. Thus, I was
unable to discern how successful each wave of invitation was at reaching MS
patients for survey participation.
Semi-Structured Interviews
The initial intent for the semi-structured interviews was to interview two
groups of patients: those who had accepted participation in a clinical trial and
those who had declined participation in a clinical trial. The purpose was to do a
comparison of willingness or unwillingness to participate in a trial and see if there
were any differences based on race and ethnicity or any other factor. However,
upon conducting the archival research and completing the BAMC electronic
medical record review, documentation by clinicians of their invitations to patients
for clinical trials and their subsequent acceptance or rejection were nonexistent in
the medical charts. Therefore, it was nearly impossible to identify a patient who
had been previously invited to a trial and declined participation in order to
interview. In addition, MS trials at BAMC were not currently enrolling, so there

74
were no prospective declinations available either. Instead of having two groups,
the study was altered to interview only MS patients who had been invited to
participate in clinical trials and had accepted. Thus, only currently active MS
clinical trial patients were available for invitation to the interview. There were 22
MS clinical trial patients in this category, 6 of whom were non-Caucasian. An
attempt was made to over sample non-Caucasian patients to explore any
potential differences in attitudes toward clinical trials by race and ethnicity.
Sixteen patients were invited to participate in the semi-structured interview, 10
Caucasian and 6 non-Caucasian. Only 11 MS patients agreed to participate, 7
Caucasian and 4 non-Caucasian (one African American and three
Hispanic/Latino patients).
An interview guide was created for the semi-structured interview to direct
the conversations through a natural, but logical progression using open-ended
questions (Bernard 2011). Some questions were added and others removed as
the utility and relevance of certain topics became clear after conducting the first
few interviews.
Interviews were conducted in May, June, and July of 2014 in a location
that was most convenient and comfortable for the patient. The first offer for an
interview location could be outside of BAMC so that any potential influence from
being in the medical center during the interview would be allayed. Despite the
offer, two patients preferred to come to BAMC to complete the interview while
they were already at BAMC for another medical appointment, six patients
75
preferred to meet in public locations (coffee shop, café) for the interview, and
three preferred to conduct the interview in the comfort of their own homes. The
interviews lasted from one to one and a half hours and all were consented in-
person and agreed to audio-recording.
The audio recordings of the interviews were transcribed using manual
transcription software (oTranscribe.com open source software) and input into
Atlas.ti for coding and analysis. A codebook was made based on a review of
themes from the first several interviews, and was refined as additional interviews
were transcribed and coded. A total of 47 codes were created to capture the
themes from all 11 interviews. These codes were analyzed further for relevant
sub-themes to identify significant patterns across all interview participants.
Institutional Approvals
Because participants for this project were recruited from BAMC’s MS
Clinic, institutional approvals from both BAMC and San Jose State University’s
IRBs were obtained. Approval for the BAMC clinical database, the electronic
survey, and the semi-structured interviews were first submitted and approved
under the BAMC IRB on March 7, 2014; then these approval documents were
submitted to SJSU IRB and approved on April 9, 2014. The SJSU IRB accepted
the consent format from BAMC because study participants were being recruited
through BAMC which has its own consent requirements for human subjects.
76
Chapter 6 – Results
Archival Data
To understand whether underrepresentation of racial and ethnic groups
exists in MS clinical trials, a review of the national clinical trial database,
ClinicalTrials.gov, was completed on all MS trials being currently conducted in
the US. In addition, a search of BAMC’s patient database was completed to
reveal rates of MS clinical trial participation by race and ethnic group compared
to the overall population of BAMC MS patients.
National Reporting
Using the ClinicalTrials.gov database, a search was done for all MS
clinical trials registered on the website. A total of 1,334 clinical trials for MS
patients were registered. Of those, 475 were completed trials (the remaining 859
trials were either newly registered trials still recruiting patients or still actively
conducting the trial). A total of 134 MS clinical trials had actually reported
results. Some of this low reporting percentage (28%) could be due to the
different reporting requirements based on clinical trial type, or for the simple
reason that these completed trials failed to report their results. Of the 134 MS
clinical trials reporting results, only 22 trials (16.4%) reported on participants’
race and ethnicity. The remaining 112 trials only reported participants based on
sex and disease status, along with trial results and adverse events, but failed to
report participant race and ethnicity data.

77
As discussed earlier, the MS prevalence rate for females is approximately
2.5 times the prevalence rate for males in the US (Multiple Sclerosis International
Federation 2013; Noonan, et al. 2002). Comparing this prevalence rate with the
participation rates of males and females in MS clinical trials in Table 3, the
proportion of male and female participants in MS clinical trials roughly mirrors the
prevalence of MS. In this case the participation rate for females is 2.2 times the
participation rate for males (1,241 males and 2,734 females) perhaps indicating a
slightly heavier participation of males relative to the general MS population.
Table 3. MS Clinical Trial Participants in the US by Sex
Trial Male Female Total 1 185 332 517
2 159 322 481
3 60 179 239
4 154 248 402
5 129 300 429
6 13 11 24
7 11 20 31
8 100 308 408
9 8 12 20
10 66 111 177
11 16 22 38
12 9 51 60
13 70 144 214
14 1 9 10
15 3 36 39
16 87 182 269
17 46 132 178
18 22 91 113
19 22 126 148
20 2 9 11
21 24 23 47
22 54 66 120
Total 1241 2734 3975
Percent 31.2% 68.8% Data from systematic review of ClinicalTrials.gov as of December 2014.
78
When looking at the prevalence breakdown of racial and ethnic groups in
the US, the prevalence of Caucasians (96 per 100,000 persons) is approximately
2.0 times the prevalence rate of African Americans (48 per 100,000 persons) and
2.0 times the prevalence rate of all other racial and ethnic groups (43 per
100,000 persons) (Noonan 2010). Rates of participation by race (Table 4) and
ethnicity (Table 5) show that the proportion of Caucasian MS patients
participating in clinical trials far exceeds the proportion of Caucasian MS patients
in the general population. For example, the participation rate of Caucasian MS
patients is approximately 36 times the participation rate of African American MS
patients (Table 4). Similarly, when combining all other racial categories, the
participation rate of Caucasian MS patients is almost 57 times the participation of
MS patients from all other racial categories (Table 4). Similarly, the participation
rate of Non-Hispanic/Latino patients is significantly higher than the participation
rate of Hispanic/Latino patients (Table 5).
Of significance, the reporting of race and ethnicity was not consistent
across trials. Most trials used the most recent 2010 US Census race categories,
but without reporting ethnicity categories. Some trials reported both race and
ethnicity categories while other trials only reported ethnicity categories. Some
trials added their own racial category of “Hispanic” rather than separating it out
as an ethnicity category. One trial even created its own race and ethnicity
categories of “White” and “Non-White.”
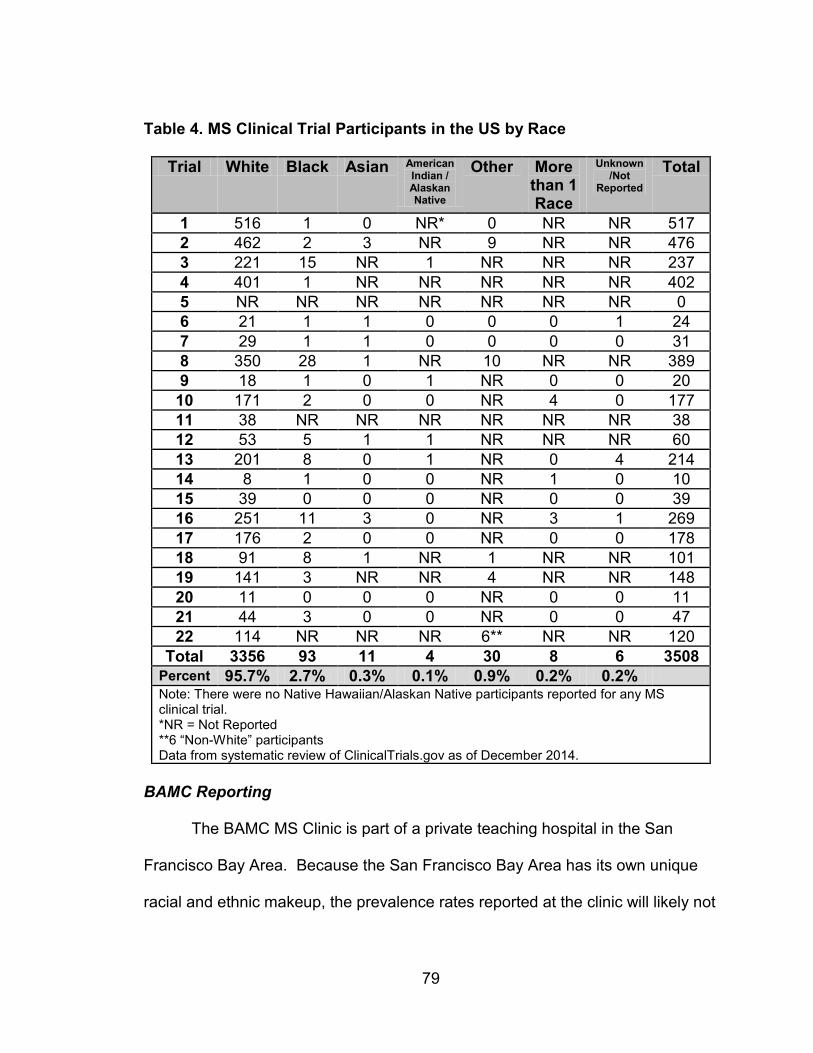
79
Table 4. MS Clinical Trial Participants in the US by Race
Trial White Black Asian American Indian / Alaskan Native
Other More than 1 Race
Unknown /Not
Reported
Total
1 516 1 0 NR* 0 NR NR 517
2 462 2 3 NR 9 NR NR 476
3 221 15 NR 1 NR NR NR 237
4 401 1 NR NR NR NR NR 402
5 NR NR NR NR NR NR NR 0
6 21 1 1 0 0 0 1 24
7 29 1 1 0 0 0 0 31
8 350 28 1 NR 10 NR NR 389
9 18 1 0 1 NR 0 0 20
10 171 2 0 0 NR 4 0 177
11 38 NR NR NR NR NR NR 38
12 53 5 1 1 NR NR NR 60
13 201 8 0 1 NR 0 4 214
14 8 1 0 0 NR 1 0 10
15 39 0 0 0 NR 0 0 39
16 251 11 3 0 NR 3 1 269
17 176 2 0 0 NR 0 0 178
18 91 8 1 NR 1 NR NR 101
19 141 3 NR NR 4 NR NR 148
20 11 0 0 0 NR 0 0 11
21 44 3 0 0 NR 0 0 47
22 114 NR NR NR 6** NR NR 120
Total 3356 93 11 4 30 8 6 3508
Percent 95.7% 2.7% 0.3% 0.1% 0.9% 0.2% 0.2% Note: There were no Native Hawaiian/Alaskan Native participants reported for any MS clinical trial. *NR = Not Reported **6 “Non-White” participants Data from systematic review of ClinicalTrials.gov as of December 2014.
BAMC Reporting
The BAMC MS Clinic is part of a private teaching hospital in the San
Francisco Bay Area. Because the San Francisco Bay Area has its own unique
racial and ethnic makeup, the prevalence rates reported at the clinic will likely not
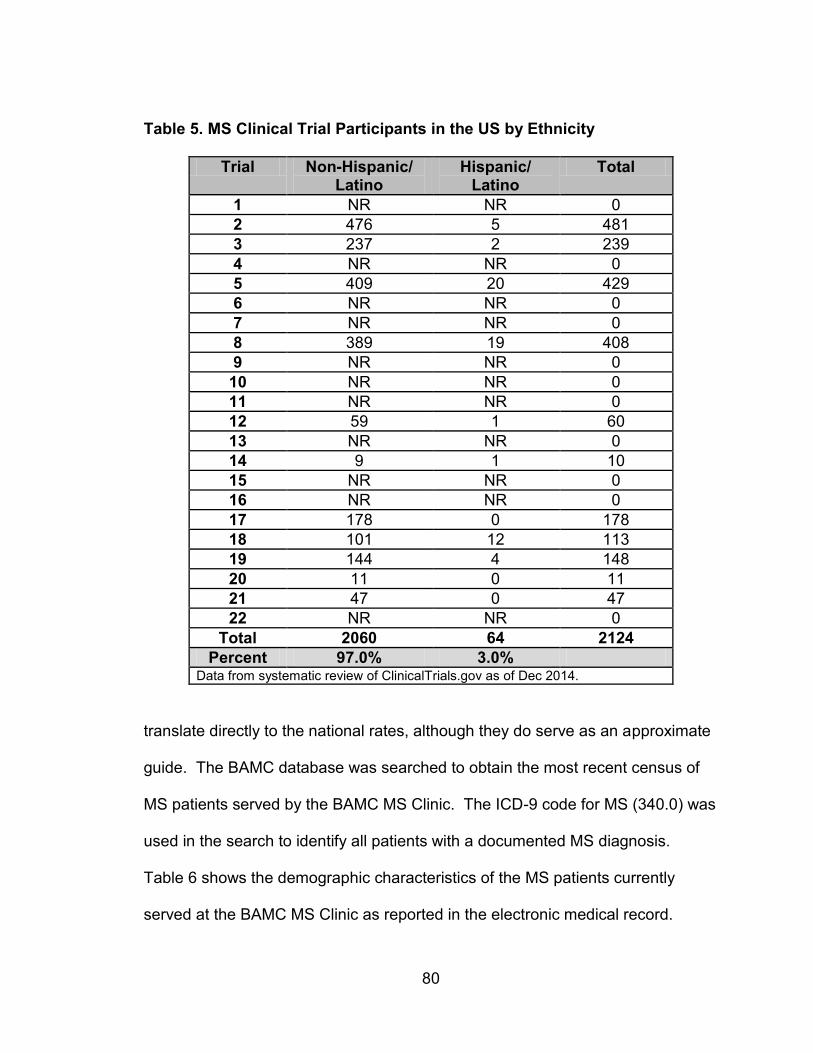
80
Table 5. MS Clinical Trial Participants in the US by Ethnicity
Trial Non-Hispanic/ Latino
Hispanic/ Latino
Total
1 NR NR 0
2 476 5 481
3 237 2 239
4 NR NR 0
5 409 20 429
6 NR NR 0
7 NR NR 0
8 389 19 408
9 NR NR 0
10 NR NR 0
11 NR NR 0
12 59 1 60
13 NR NR 0
14 9 1 10
15 NR NR 0
16 NR NR 0
17 178 0 178
18 101 12 113
19 144 4 148
20 11 0 11
21 47 0 47
22 NR NR 0
Total 2060 64 2124
Percent 97.0% 3.0% Data from systematic review of ClinicalTrials.gov as of Dec 2014.
translate directly to the national rates, although they do serve as an approximate
guide. The BAMC database was searched to obtain the most recent census of
MS patients served by the BAMC MS Clinic. The ICD-9 code for MS (340.0) was
used in the search to identify all patients with a documented MS diagnosis.
Table 6 shows the demographic characteristics of the MS patients currently
served at the BAMC MS Clinic as reported in the electronic medical record.

81
Table 6. Demographics of MS Patients Served by BAMC MS Clinic
Demographic Count Percent
Sex Male Female
379
1,060
26.3 73.7
Total 1,439 100.0
Race/Ethnicity Caucasian African American Asian Other Native American Unknown Hispanic
1,149
83 73 5 4 1
124
79.8 5.8 5.1 0.3 0.3 0.1 8.6
Total 1,439 100.0 Data from systematic review of BAMC database as of May 2014.
The BAMC MS Clinic serves a slightly higher proportion of women than
men compared to the national average of 2.5 women to every one man (Table 6).
Women are served by BAMC MS Clinic approximately 2.8 times the rate of men
(1,060 females to 379 males). Almost 80% of the BAMC MS Clinic patients are
Caucasian, while the remainder of the racial and ethnic categories total to
approximately 20% of the BAMC MS patient population (Table 6). While this is
still a far cry from the nationally reported proportions of race and ethnicity, this
may be a reflection of the local region, as well as the ability of patients to access
the medical care offered by the BAMC MS clinic. When exploring these numbers
to determine whether there is underrepresentation of minority groups in MS
clinical trials, it is important to note that the participation rates by race and
ethnicity in BAMC MS clinical trials should be compared to the makeup of the
BAMC MS patient population since these actual numbers reflect the reality and

82
constraints of local demographics, socioeconomics, and health care access
issues.
As discussed previously, initial attempts to pull clinical trial participation
rates from past patients were unsuccessful because the BAMC database did not
contain any documentation of clinical trial participation, clinical trial invitations,
nor subsequent acceptance or declination of the clinical trial. In addition, an
attempt was made to access participation rates from the BAMC IRB since they
are required by federal regulation to collect information about participants’ race
and ethnicity. However, the IRB was unable to disclose this information, as it is
only collected to monitor equitable access of clinical trials to all patients. Thus,
only information on current MS patients participating in clinical trials was
collected. Table 7 shows demographic information about MS patients currently
participating in clinical trials at the BAMC MS Clinic. The proportion of males and
females participating in clinic trials at BAMC roughly approximates the proportion
seen in the larger BAMC MS patient population, with only a slight increase in
male representation in clinical trials (total male BAMC MS patient population
26.3% versus male BAMC MS clinical trial population 29.5%). Interestingly, the
proportion of non-Caucasian clinical trial participants is higher than in the total
BAMC MS patient population (approximately 40% non-Caucasian BAMC clinical
trial participants versus 20% in the total BAMC MS patient population). Although
this is also significantly higher than the proportions of non-Caucasian patients
participating in clinical trials nationally, this rate still does not match the national

83
prevalence rates by race and ethnicity. For example, the prevalence rate
reported by Noonan et al (2010) for Caucasians, African Americans, and the
remaining racial and ethnic categories is a 2 to 1 to 1 ratio. For BAMC that ratio
is approximately 13 to 1 to 7.
Table 7. Demographics of MS Patients Participating in Clinical Trials at BAMC MS Clinic
Demographic Count Percent
Sex Male Female
13 31
29.5 70.5
Total 44 100.0
Race/Ethnicity Caucasian African American Asian Other Native American Unknown Hispanic
27 2 2 6 0 2 5
61.4 4.5 4.5
13.6 0.0 4.5
11.4
Total 44 100.0 Data from systematic review of currently active and recently completed BAMC MS clinical trial participants as of July 2014
Electronic Survey
An electronic survey was created in order to capture the opinions of the
larger BAMC MS patient population regarding participation in clinical trials. Since
participation of patients in the in-depth semi-structured interviews would be
limited, an electronic survey would be able to reach more patients, require
significantly less time for the patient, and could be completed in a convenient
location and time. Although 254 email and letter invitations were sent to BAMC

84
MS patients, only 48 responded. Table 8 shows demographic information
reported by the survey respondents.
Table 8. Demographics of Electronic Survey Respondents
Demographic Count Percent
Sex Male Female
9
38
19.1 80.9
Age Minimum Maximum Mean
21 yo 69 yo 48 yo
N/A N/A N/A
Race/Ethnicity Caucasian African American Asian Other Native American Unknown Hispanic
37 1 3 0 0 0 7
77.1 2.1 6.3 0.0 0.0 0.0
14.6
Annual Income* $49,999 or less $50,000-$99,999 $100,000-$149,999 $150,000 or more
8
11 8
20
17.0 23.4 17.0 42.6
Education Less than Bachelor’s Bachelor’s Master’s Professional or Doctorate
18 11 10 9
37.5 22.9 20.8 18.8
Insurance Private Medicare Other
38 8 2
79.2 16.7 4.2
Total 48 100.0 *Total Annual Household Income
As shown in Table 8, the population of MS patients surveyed for this study
includes individuals from a wide variety of backgrounds. However, the
85
population’s demographic characteristics are skewed and do not meet the
requirements for a normally distributed population. In fact skewedness and
kurtosis were extremely variable for all demographic variables and the only
potentially normally distributed variable is age (Kolmogorov-Smirnov = 0.089, df
= 48, p = 0.200). All other demographic variables failed this test of normality.
Thus for this analysis, non-parametric statistics were used to account for the
underlying population distribution, the small sample size, and measurement of
categorical variables. Chi-square tests for independence were used for
categorical responses, while Mann-Whitney U tests were also done to test for
differences between two independent groups on a continuous variable (e.g., four-
point scale from “No Influence” to “Strongly Influence”). Kruskal-Wallis tests
were used to compare scores on a continuous variable for three or more groups.
Follow up Mann-Whitney U tests were also done when a statistically significant
result was identified from the Kruskal-Wallis test to determine which responses
were significantly different from one another.
Patients were asked about their familiarity with and opinion about clinical
trials, which were defined in the survey as “research studies that involve patients
receiving an experimental drug, treatment, or device to evaluate its safety and
efficacy.” Patients were also asked whether they would participate in a clinical
trial and to rank the reasons why they would or would not choose to participate in
a trial. Overall, most respondents (42 out of 48 respondents) said they were
either “Very Familiar” or “Fairly Familiar” with the term “clinical trial.” However,

86
fewer respondents had ever seen a print advertisement (18 out of 48
respondents) or a digital advertisement (13 out of 48 respondents) inviting them
to participate in a clinical trial. No significant differences were found between
racial and ethnic categories.
Exactly half of respondents (24 out of 48 respondents) had discussed
participation in a clinical trial with their doctor, nurse, or research personnel.
However, a chi square test for independence (with Yates Continuity Correction)
indicated a significant association between being Caucasian or non-Caucasian
and discussing participation in a clinical trial (χ2 [1, n = 48] = 4.24, p = 0.039, phi
= -0.347). Caucasian MS patients were more likely to have discussed
participation in a clinical trial than their non-Caucasian counterparts (Figure 2).
Respondents were also asked whether they had ever been invited to participate
in a trial, if they have ever agreed to participate in a trial, or if they have ever
declined participation in a trial, but chi square tests did not reveal additional
significant differences between the responses and racial or ethnic category.
Comparisons between proportions of Caucasian and non-Caucasian
patients' stated exposure to clinical trials revealed some interesting differences.
Regarding whether a patient had discussed a clinical trial with their doctor, nurse,
or research personnel, Caucasian patients were significantly more likely to have
discussed a trial than non-Caucasian patients (Z = 2.4039, p = 0.0164).
Additionally, although a chi square test did not reveal a significant difference in
responses between racial and ethnic groups on invitations to participate in a trial,

87
Z tests indicated that a significant difference exists in the proportion of Caucasian
patients who are invited to participate in clinical trials versus non-Caucasian
patients (Z = 2.0794, p = 0.03752). In other words, Caucasian patients are more
likely to be invited to participate in a trial while non-Caucasian patients are less
likely to be invited to participate in a trial. These results may point to structural
factors (e.g., clinician bias) that influence whether a doctor discusses a clinical
trial with a patient or whether a patient is invited to participate in a clinical trial.
Figure 2. Percentage of Caucasian and Non-Caucasian Respondents who have Discussed Clinical Trial Participation with their Doctor, Nurse, or Research Personnel Respondents were also asked to choose their primary reason for both
participating in a clinical trial and declining participation in a clinical trial. The list
of reasons for agreeing to participate and declining to participate was compiled
from other studies looking at patients’ willingness to participate in clinical trials.
Tables 9 and 10 show the frequencies of responses, with “To advance science
0% 20% 40% 60% 80% 100%
No
Yes
Percent of Survey Respondents by Caucasian and Non-Caucasian Categories
Hav
e y
ou
eve
r D
ISC
USS
ED M
S cl
inic
al
tria
ls w
ith
yo
ur
do
cto
r, n
urs
e, o
r re
ear
ch p
ers
on
ne
l?
Caucasian
Non-Caucasian
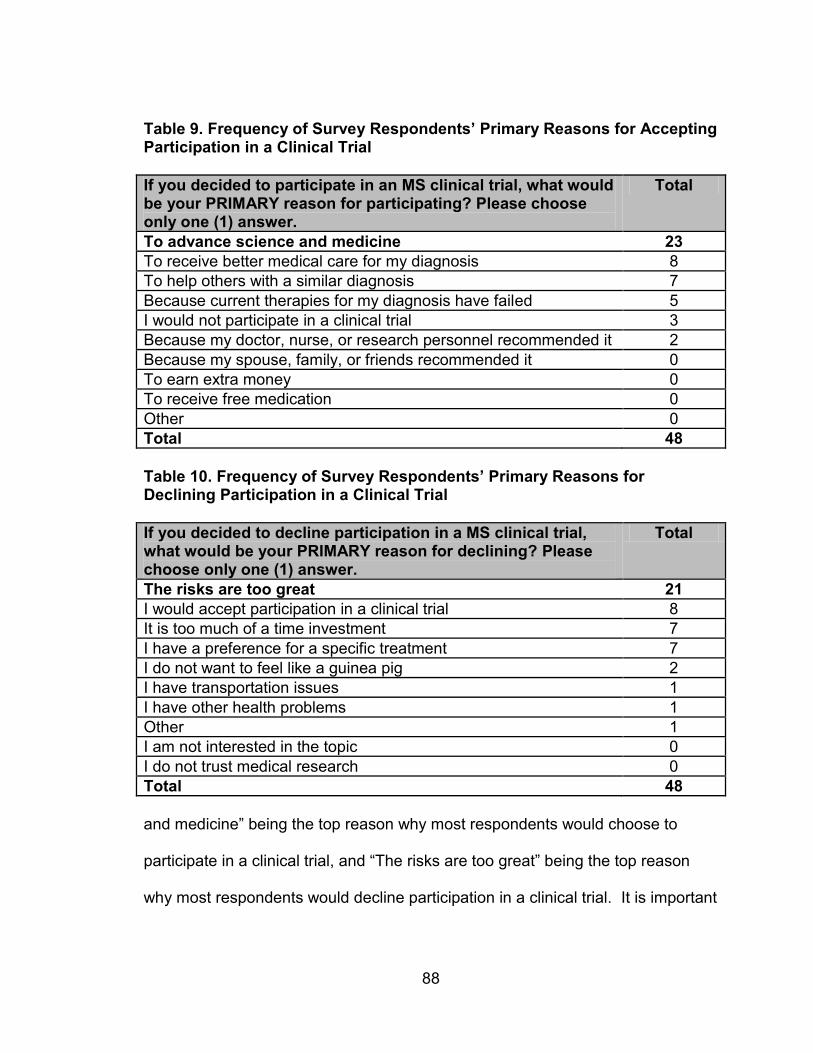
88
Table 9. Frequency of Survey Respondents’ Primary Reasons for Accepting Participation in a Clinical Trial
If you decided to participate in an MS clinical trial, what would be your PRIMARY reason for participating? Please choose only one (1) answer.
Total
To advance science and medicine 23
To receive better medical care for my diagnosis 8
To help others with a similar diagnosis 7
Because current therapies for my diagnosis have failed 5
I would not participate in a clinical trial 3
Because my doctor, nurse, or research personnel recommended it 2
Because my spouse, family, or friends recommended it 0
To earn extra money 0
To receive free medication 0
Other 0
Total 48
Table 10. Frequency of Survey Respondents’ Primary Reasons for Declining Participation in a Clinical Trial
If you decided to decline participation in a MS clinical trial, what would be your PRIMARY reason for declining? Please choose only one (1) answer.
Total
The risks are too great 21
I would accept participation in a clinical trial 8
It is too much of a time investment 7
I have a preference for a specific treatment 7
I do not want to feel like a guinea pig 2
I have transportation issues 1
I have other health problems 1
Other 1
I am not interested in the topic 0
I do not trust medical research 0
Total 48
and medicine” being the top reason why most respondents would choose to
participate in a clinical trial, and “The risks are too great” being the top reason
why most respondents would decline participation in a clinical trial. It is important
89
to note that there were no significant differences found between responses by
race or ethnicity, or by sex, education level, income level or insurance type.
To further tease out how much influence some of these reasons might
have on a patient’s decision to participation in a clinical trial, respondents were
asked to rank the degree of influence each of these reasons for accepting and
declining participation would have on their decision-making process.
Respondents ranked the reasons in both Tables 9 and 10 as either “Strongly
Influence (Level 4)”,” Moderately Influence (Level 3)”, “Little Influence (Level 2)”,
or “No Influence (Level 1).” For all of these reasons, no significant differences
were found between the degree of influence for each reason by race or ethnicity
(Table 11), sex (Table 12), or income level (Table 13). However, there were a
few significant differences found between the degree of influence of particular
participation reasons and education level and insurance type which are
discussed in more detail below.
For most influences that would affect participation in a clinical trial, there
were no significant differences found by education level except for the following
two reasons patients said they would accept participation in a clinical trial: “To
receive free medication” and “Because current therapies for my diagnosis have
failed.” A Kruskal-Wallis test revealed a statistically significant difference in the
influence of receiving free medication on participation in a clinical trial across four
different education levels (Less than Bachelor’s Degree, n = 18; Bachelor’s
Degree, n = 11; Master’s Degree, n = 10, Professional or Doctorate Degree, n =
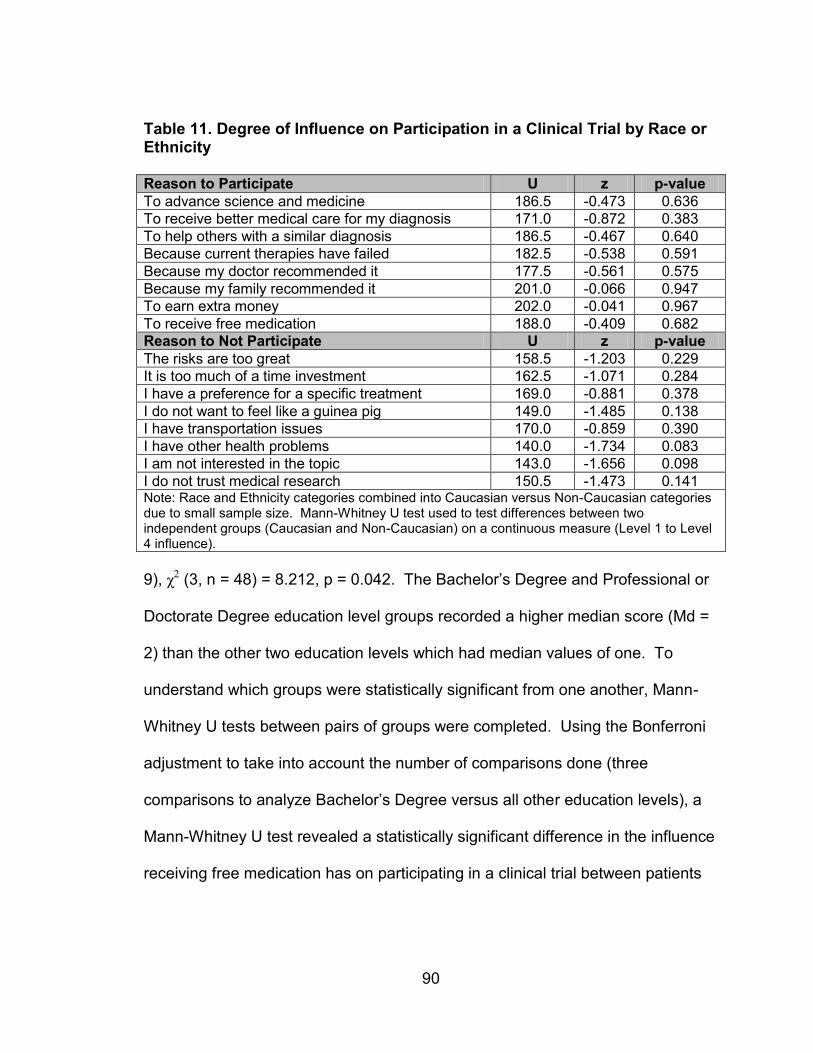
90
Table 11. Degree of Influence on Participation in a Clinical Trial by Race or Ethnicity Reason to Participate U z p-value
To advance science and medicine 186.5 -0.473 0.636
To receive better medical care for my diagnosis 171.0 -0.872 0.383
To help others with a similar diagnosis 186.5 -0.467 0.640
Because current therapies have failed 182.5 -0.538 0.591
Because my doctor recommended it 177.5 -0.561 0.575
Because my family recommended it 201.0 -0.066 0.947
To earn extra money 202.0 -0.041 0.967
To receive free medication 188.0 -0.409 0.682
Reason to Not Participate U z p-value
The risks are too great 158.5 -1.203 0.229
It is too much of a time investment 162.5 -1.071 0.284
I have a preference for a specific treatment 169.0 -0.881 0.378
I do not want to feel like a guinea pig 149.0 -1.485 0.138
I have transportation issues 170.0 -0.859 0.390
I have other health problems 140.0 -1.734 0.083
I am not interested in the topic 143.0 -1.656 0.098
I do not trust medical research 150.5 -1.473 0.141 Note: Race and Ethnicity categories combined into Caucasian versus Non-Caucasian categories due to small sample size. Mann-Whitney U test used to test differences between two independent groups (Caucasian and Non-Caucasian) on a continuous measure (Level 1 to Level 4 influence).
9), χ2 (3, n = 48) = 8.212, p = 0.042. The Bachelor’s Degree and Professional or
Doctorate Degree education level groups recorded a higher median score (Md =
2) than the other two education levels which had median values of one. To
understand which groups were statistically significant from one another, Mann-
Whitney U tests between pairs of groups were completed. Using the Bonferroni
adjustment to take into account the number of comparisons done (three
comparisons to analyze Bachelor’s Degree versus all other education levels), a
Mann-Whitney U test revealed a statistically significant difference in the influence
receiving free medication has on participating in a clinical trial between patients
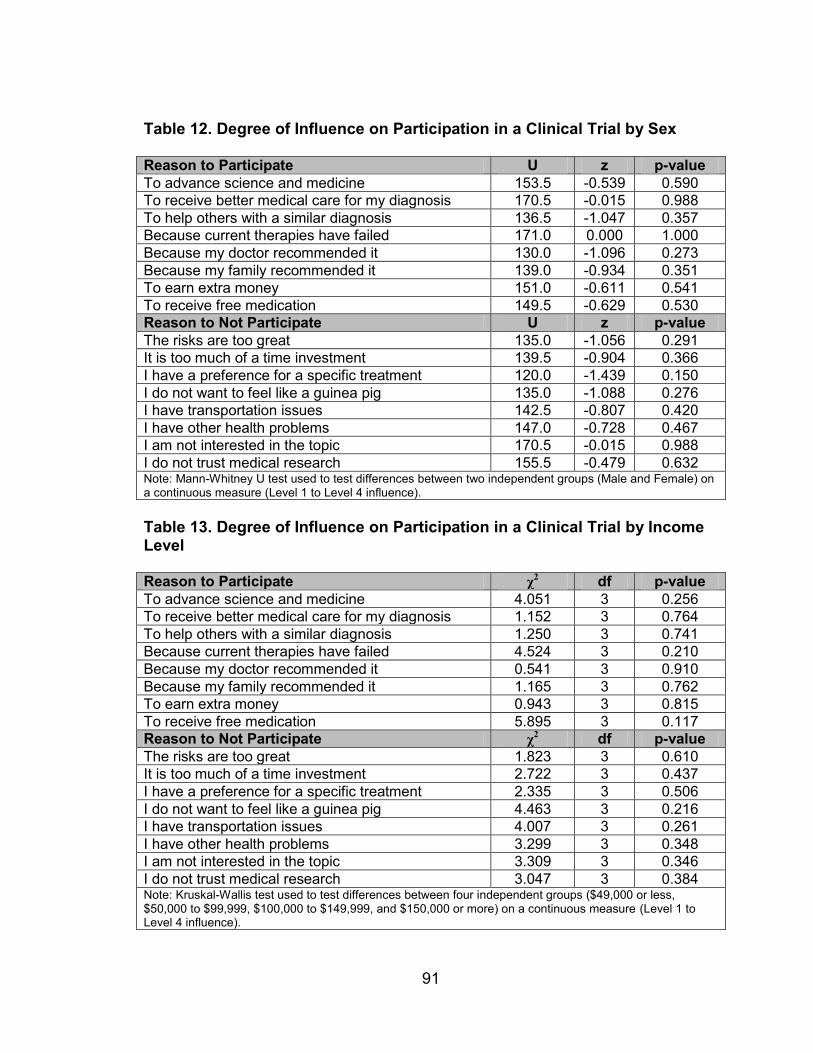
91
Table 12. Degree of Influence on Participation in a Clinical Trial by Sex Reason to Participate U z p-value
To advance science and medicine 153.5 -0.539 0.590
To receive better medical care for my diagnosis 170.5 -0.015 0.988
To help others with a similar diagnosis 136.5 -1.047 0.357
Because current therapies have failed 171.0 0.000 1.000
Because my doctor recommended it 130.0 -1.096 0.273
Because my family recommended it 139.0 -0.934 0.351
To earn extra money 151.0 -0.611 0.541
To receive free medication 149.5 -0.629 0.530
Reason to Not Participate U z p-value
The risks are too great 135.0 -1.056 0.291
It is too much of a time investment 139.5 -0.904 0.366
I have a preference for a specific treatment 120.0 -1.439 0.150
I do not want to feel like a guinea pig 135.0 -1.088 0.276
I have transportation issues 142.5 -0.807 0.420
I have other health problems 147.0 -0.728 0.467
I am not interested in the topic 170.5 -0.015 0.988
I do not trust medical research 155.5 -0.479 0.632 Note: Mann-Whitney U test used to test differences between two independent groups (Male and Female) on a continuous measure (Level 1 to Level 4 influence).
Table 13. Degree of Influence on Participation in a Clinical Trial by Income Level Reason to Participate χ
2 df p-value
To advance science and medicine 4.051 3 0.256
To receive better medical care for my diagnosis 1.152 3 0.764
To help others with a similar diagnosis 1.250 3 0.741
Because current therapies have failed 4.524 3 0.210
Because my doctor recommended it 0.541 3 0.910
Because my family recommended it 1.165 3 0.762
To earn extra money 0.943 3 0.815
To receive free medication 5.895 3 0.117
Reason to Not Participate χ2 df p-value
The risks are too great 1.823 3 0.610
It is too much of a time investment 2.722 3 0.437
I have a preference for a specific treatment 2.335 3 0.506
I do not want to feel like a guinea pig 4.463 3 0.216
I have transportation issues 4.007 3 0.261
I have other health problems 3.299 3 0.348
I am not interested in the topic 3.309 3 0.346
I do not trust medical research 3.047 3 0.384 Note: Kruskal-Wallis test used to test differences between four independent groups ($49,000 or less, $50,000 to $99,999, $100,000 to $149,999, and $150,000 or more) on a continuous measure (Level 1 to Level 4 influence).
92
having a Bachelor’s Degree (Md = 2, n = 48) and a Master’s Degree (Md = 1, n =
48), U = 20.0, z = -2.621, p = 0.009, r = 0.38.8
A Kruskal-Wallis test revealed a statistically significant difference in the
influence of failing current therapies on participation in a clinical trial across four
different education levels (Less than Bachelor’s Degree, n = 18; Bachelor’s
Degree, n = 11; Master’s Degree, n = 10, Professional or Doctorate Degree, n =
9), χ2 (3, n = 48) = 8.876, p = 0.031. The Master’s Degree education level group
recorded a higher median score (Md = 4) than the Bachelor’s Degree and
Professional or Doctorate Degree education levels which both recorded median
values of 2, and the Less than Bachelor’s Degree education level which recorded
a median value of one. To understand which groups were statistically significant
from each other, Mann-Whitney U tests between pairs of groups were completed.
Using the Bonferroni adjustment to take into account the number of comparisons
done (three comparisons to analyze Master’s Degree versus all other education
levels), a Mann-Whitney U test revealed a statistically significant difference in the
influence failing current therapies has on participating in a clinical trial between
patients having a Master’s Degree (Md = 4, n = 48) and Less than a Bacherlor’s
Degree (Md = 1, n = 48), U = 32.5, z = -2.892, p = 0.004, r = 0.42.9
For most influences that would affect participation in a clinical trial, there
were also no significant differences found by insurance type, except for one
8 The guidelines proposed by (Cohen 1988) for interpreting effect size classifies 0.01 as a small effect, 0.06
as a medium effect, and 0.14 as a large effect. 9 The guidelines proposed by Cohen (1988) for interpreting effect size classifies 0.01 as a small effect, 0.06
as a medium effect, and 0.14 as a large effect.

93
reason patients said they would decline participation in a clinical trial: “I do not
want to feel like a guinea pig.” A Kruskal-Wallis test revealed a statistically
significant difference in the influence of feeling like a guinea pig on participation
in a clinical trial across three different insurance types (Private, n = 38; Medicare,
n = 8; Other, n = 2), χ2 (2, n = 48) = 6.859, p = 0.032. The Other insurance type
group recorded a higher median score (Md = 4) than the Private and Medicare
insurance type groups which both recorded median values of one. To
understand which groups were statistically significant from each other, follow up
Mann-Whitney U tests between pairs of groups were completed. Using the
Bonferroni adjustment to take into account the number of comparisons done (two
comparisons to analyze Other insurance versus Private and Medicare), a Mann-
Whitney U test revealed a statistically significant difference in the influence
feeling like a guinea pig has on participating in a clinical trial between patients
with Other insurance (Md = 4, n = 48) and patients with Medicare (Md = 1, n =
48), U = 0.000, z = -2.372, p = 0.018, r = 0.42.10
Semi-Structured Interviews
Compared with the electronic surveys, the semi-structured interviews
allowed for a more open, unstructured and nuanced exploration of each patient’s
opinion of clinical trials. A total of 11 patients from the BAMC MS Clinic who
were currently participating or had recently participated in a clinical trial were
interviewed for this study. These patients represent a variety of clinical trials
10
The guidelines proposed by Cohen (1988) for interpreting effect size classifies 0.01 as a small effect, 0.06 as a medium effect, and 0.14 as a large effect.

94
being conducted at BAMC, and also represent a wide, demographic spectrum.
Table 14 shows the demographic information for the 11 interview participants.
Most interview participants were female which does match the higher proportion
of females who are diagnosed with MS. In addition, most interview participants
were Caucasian, although attempts were made at over sampling non-Caucasian
patients in order to understand if there are any differences in attitudes towards
clinical trials by race and ethnicity. Age of interview participants ranged from 20s
to 50s, while length of MS diagnosis ranged from a new diagnosis within the past
year to a diagnosis over 11 years ago. Most of these patients have their own
private insurance, but the ones who have either Medicare or no insurance at all
were all patients who had been referred from the local community hospital, and
specifically came to BAMC to participate in a clinical trial in lieu of having medical
coverage.
Although it is difficult to quantify the degree of MS disability, these patients
ranged from have very mild MS symptoms such that an outside observer would
not be able to tell the patient had MS, to severe MS symptoms which require that
patients are in a wheelchair with constant caregiver attention. In addition, 4 out
of the 11 patients receive California State Disability Insurance. These 11
patients also represent a number of different trials being conducted at the BAMC
MS Clinic ranging from a Phase I to a Phase III trial. These trials also range in
study duration, experimental treatment type, and the presence or absence of a
placebo arm.

95
Table 14. Demographics of Interview Participants
Demographic Count Percent
Sex Male Female
4 7
36% 64%
Race/Ethnicity White Black Hispanic
7 1 3
64% 9% 27%
Age 20-29 30-39 40-49 50-59
3 4 1 3
27% 36% 9% 27%
Length of Diagnosis 1 year 2 years 5 years 6 years 7 years 11 years
1 2 2 2 2 2
9% 18% 18% 18% 18% 18%
Insurance* Private Medicare None
9 1 2
82% 9% 18%
Disability Yes No
4 7
36% 64%
Study** Acorda (Phase I) Actelion (Phase II) Biogen (Phase II) Genzyme (Phase III) Opera (Phase II) Vitamin D
2 3 1 1 2 3
18% 27% 9% 9% 18% 27%
*One patient had two types of insurance **One patient participated in two trials

96
Primary Reasons to Participate in a Clinical Trial
Of key interest to this study was to elucidate the reason or reasons that
patients decided to participate in the clinical trial they were currently participating
in or had just finished participating in. Patients provided a spectrum of answers
that ranged in influence level and that often weaved together with their journey
exploring and experiencing their MS Identity. Before diving into specific reasons
for participation in a trial and examining the context and details, patients were
first asked to come up with a primary reason for participating in a trial before
being able to add ancillary reasons. Most patients’ primary reasons centered
around two major themes, namely for “selfish” reasons and for the bigger picture
contribution to science and medicine and other fellow MS patients. Each theme
is explored in more detail below.
For “Selfish” Reasons
Interestingly, when asked as an open-ended question, the primary reason
for participation in a clinical trial often centered on the admission that the patient
participated for a “selfish” reason. Oftentimes the patient would explicitly state
that it was a selfish reason, but helping science and medicine and other MS
patients were beneficial side effects. For example, to advance science and
medicine “…would never be my first reason because I’m entirely too selfish for
that…So I really like that reason. It’s just that I think most of us who
actually…have a condition, it invents this sort of selfishness in you” (Christine
Rogers). The “selfish” reason often met an immediate need that the patient had

97
depending on his or her particular situation. Those selfish reasons were related
to the following topics: negative side effects of current MS medications, the
desire to receive better medical care, the desire to receive free medication, future
health prospects, and finally, pure survival.
A couple of patients decided to participate in their clinical trial because
currently approved MS medications had negative side effects which they could
no longer tolerate. One patient, Jaime, was on Avonex for almost one year and
experienced severe flu-like symptoms every week which were often bad enough
to leave him in bed for the 24 hours immediately following the injection. After
enduring this medication for a year, his doctor finally recommended switching to
a different medication, Rebif, but it too was an injection that could also cause flu-
like symptoms and the frequency of the injection would have to increase from
once per week to three times per week. The difference was that Rebif was
supposed to be a more potent medication to help better prevent the increasing
MS symptoms that Jaime was experiencing at the time. This alternative was not
ideal to Jaime so there was hesitation to make the switch. His doctor, who was
at the local community hospital, then recommended a clinical trial at BAMC to
Jaime in case he wanted to consider it. However the risk of the trial was that he
could be randomized to one of two groups: 1) taking Rebif, like he was originally
considering outside of the study, or 2) the experimental medication which was an
IV infusion for a 5-day cycle during Year 1, and a 3-day cycle during Year 2.
98
Ultimately, Jaime decided to participate in the trial as an alternative to his options
outside of trial participation.
Another patient, Christine, was on Copaxone for one year but every
injection was extremely painful and left necrotic areas of skin at her injection sites
on her legs and stomach. Christine was seeing a neurologist at BAMC for her
regular MS medical care at the time, and at the end of the year, her neurologist
said she had given the Copaxone a good trial run and agreed that it was not
working for her. Similar to Jaime, Christine’s only other alternatives were other
self-injections which she refused to endure ever again. It was at this point that
her neurologist introduced a clinical trial to her that was testing a new oral
medication for MS (there were no currently approved oral medications for MS at
the time). For her, it was an easy decision to go into the clinical trial because
when comparing the approved MS injections to the oral pills, “It’s like one was
hellacious and seriously impacting my life and the other is like nothing” (Christine
Rogers). For both Jaime and Christine, neither the currently approved MS
medications that they were on, nor the other medications that were available,
were a preferable alternative. After being introduced to their respective clinical
trials, both decided that being in the trial provided them with a medication, or in
Jaime’s case a chance at a medication, that they could better tolerate both
physically and mentally.
Another “selfish” reason that some patients claimed was their primary
reason for participation in a trial was related to the desire to receive better

99
medical care for their condition. This was true for Carol who admittedly did not
take very good care of her health once she was diagnosed with MS in 2009. At
the time, she herself was a caregiver to both her grandmother and her mother, so
she did not go on any MS medication for almost two and half years. When MS
symptoms bothered her, she would get a several day course of IV steroids to
help speed her recovery time, but the frequency and severity of the attacks
increased. Finally her neurologist at the local community hospital said she could
no longer go without an MS medication because her MRIs showed many new
lesions in the brain and spinal cord. “I remember after he had said that to me, it
was just the way he looked at me, but I went down to the beach that night by
myself and I just lost it. And it was like, okay, the realization that I've been putting
it off for so long and now I really need to do something about it and take care of
my health” (Carol Heuser). The same neurologist then suggested that she might
consider a clinical trial that did not have a placebo arm, and would guarantee her
an MS treatment, independent of which treatment arm she might be randomized
to. Consequently, she chose to participate in the clinical trial. “I think the first
motivator was the fact that I would have a treatment team…I would have
protocols to stick to…and just the fact that I wasn't having to be one hundred
percent in charge of my own treatment” (Carol Heuser). Because of her past
disregard for her own medical care early in her diagnosis, Carol primarily wanted
structured care for her MS. The trial provided a treatment team that she felt was
watching multiple aspects of her disease and was vigilant for any drug adverse

100
effects. It also provided a schedule to follow according to the trial protocol so it
was clear to her and through continuous staff communication, where she needed
to be and when.
Another primary reason some patients cited as their reason for
participation was the benefit of receiving free medication through the trial. For
Lydia, this was her primary reason, even though she had private insurance that
would cover a large portion of the drug costs. Because the trial was two years,
that was two years she didn’t have to fight with her insurance company about
covering the costs, or paying whatever the monthly copay would be. MS
medications are a significant financial burden to many MS patients, and even the
coverage of insurance plans does little to lessen the financial burden. In
addition, the burden of proof for starting a medication is often on the patient and
his or her neurologist as many of the MS medications have restrictions on
availability. Most MS medications are only approved for the RRMS form of MS,
and even if you are a patient with RRMS, you might also need to prove that you
failed your previous MS medication before the insurance company can approve
you for another MS medication. Oftentimes this “proof” involves months of
waiting while MS attacks occur and increased disability progression develops.
So for Lydia, when asked what her primary reason for participating in her clinical
trial, she replied, “Honestly? The free, not having to pay for my medication. That's
the big, that was the selling point pretty much is, okay I'm going to be helping
101
somebody else, but I don't have to pay for my medication because I don't know if
my insurance was going to cover it completely” (Lydia Ochoa).
Still other patients expressed their primary “selfish” reason for participating
in a clinical trial being related to their future health prospects. Bruce explained
that his primary reason for participating in a clinical trial was to help secure his
future with his wife and a family. “I want to have as normal of a life as possible
with kids. So I don't want to be the dad in the wheelchair on the sidelines of the
soccer game or the ballet recital. I just want to have a normal life. I don't want
my wife to have to take care of me” (Bruce Eldridge). So if a positive result can
come out of the trial he is currently participating in, that would help contribute to
improving the prospects for his health in the future and his participation would be
worth the effort. Similarly, Edward participated in his clinical trial because if he is
going to deal with MS for the next 50-60 years, then anything he can do now to
help in the next 50-60 years will directly benefit him. “It’s a little selfish to be that
way. But I find it pragmatic and proactive” (Edward Foster). If his participation in
the trial can help make an impact on the way treatment is provided for MS
patients, then it will have a direct impact to him. Even though both Bruce and
Edward have such mild forms of MS that an outside observer would not be able
to tell they had MS, both were fully aware of the unpredictable nature of the
disease and saw the clinical trial as a way to help improve their future health
projections.
102
Finally, in some of the MS patients who have more severe MS symptoms
and disability progression, the main “selfish” reason for participating in a clinical
trial was for immediate MS symptom relief and survival. For Faye, who was the
most severely affected patient that was interviewed, was in a wheelchair, and
required a caregiver, participating in a clinical trial was a potential way for her to
try to actually see improvements in her current disease state. When Faye was
first referred to BAMC by her neurologist at the local community hospital to
participate in a clinical trial, she did not qualify for the trial because there were
specific requirements patients had to meet in order to be included. Specifically,
she needed to walk unassisted (without a cane, crutch, or human assistance) for
a length of 100 feet and she was unable to meet this requirement. Faye kept in
touch with me for over a year checking in to see if there were any new clinical
trials she could qualify for. Finally, she was able to enroll in a clinical trial and
even enrolled in a second clinical trial immediately after the first one ended.
When asked if she could identify what her primary reason was for participating in
these clinical trials, she said,
The main reason is for me to be able to play with my grandbaby. And be able to take her to the park and be able to help her ride her first bike. I mean, she is what I'm fighting for because that's my baby. And all she's known Nana as being in the [wheel] chair. I want to be able to have my independence back because I have a caregiver now and I just don't like anybody taking care of me. I want to be able to do everything by myself. I've always been an independent lady, always. And right now is just hard to be independent. This is not me at all. [Faye Smith]
103
Faye has a continued interested in clinical trials because her regular
medical care cannot offer her anything except maintenance of her condition. In
her opinion, she doesn’t see the need to go to a regular doctor anyways. They
just bring her in every six months and tell her to keep taking her injections. The
clinical trials offered her a way to actually do something about her diagnosis. “I
don't want to say I'm to the point where I'm desperate but kinda. Because I just
don't like living like this. It's just tough. It's tough. I can't drive anymore. I can't
do anything. It's terrible. I have to do something so that's what I did right? I
signed up” (Faye Smith).
As we learned in the introduction of this paper, Isabelle expressed her
reason for participation in a clinical trial as pure survival. Since her diagnosis in
2008, despite being on Rebif, Isabelle continued to have MS attacks and
accumulated more disability at a faster and faster rate. She tried going to
occupational therapy to re-train herself to do activities of daily living with
appropriate modifications, and tried physical therapy to learn how to use crutches
when she was having difficulty walking on her own. Through this physical
decline, she was no longer able to work and lost her medical insurance. She
also went through a divorce and found herself extremely depressed with no
hope. Her physical health continued to decline and she was finally given a
prescription by her neurologist to get a wheelchair. She remembers the moment
when she wanted to consider a clinical trial. “I had a prescription in my hands to
get a wheelchair. But I refused it. I was just too stubborn and that was the
104
crossing point for me saying okay I’m going to get on some kind of study”
(Isabelle Carbajal). She explained that somehow she pulled herself out of the
despair and wanted to fight for her survival. She was even willing to risk her life
for the clinical trial because she didn’t feel like there was anything to live for
anymore. Isabelle thought at least the clinical trial was a way for her to try
something since she did not have any insurance.
For Science and Medicine and “Fellow MS Sufferers”
Another group of patients stated that their primary reasons for participating
in a clinical trial were to advance science and medicine and help others with MS.
Some explained that if you have a condition like MS, you have an obligation to try
to make a contribution to understanding the disease, making progress in
treatment, and finding a cure. Patients also talked about an almost higher-order
connection to other MS patients and the need to reduce suffering, lessen the
confusion around MS diagnosis, lessen the confusion about medication choices,
and diminish the guilt they had about patients with greater disability than
themselves. According to the patients, all of this could be accomplished through
participation in clinical trials.
Several MS patients talked about the idea of participating in a clinical trial
to be somewhat obligatory considering the nature of the disease and the need for
better treatments and a cure. Carol discussed her feeling of obligation as being
part of a larger community with a responsibility to help where she can. “I think
that's really important, especially if you're somebody without any medical

105
conditions, then you have a different view on things. If you have medical
conditions that bug you, you're like, what can we do about it, especially if you're
running out of treatment options” (Carol Heuser). Similarly, Bruce saw his role
participating in a clinical trial as an obligation to help contribute to pushing the
research forward.
I think one of the big factors was, I'm a big believer in data, so if I'm going to be selfish and say no. Like, oh it's too much hassle for me to go every 3 months or whatever, if there's 100 other people like me or just 20 other people like me that also say no and have the same thought process, there's going to be no progress in the industry. So it's like, well, I have to do my part and contribute to the, even if I'm not, even if I'm just a blip out of 100 people, I have to do, I have to do what I think's right. [Bruce Eldridge]
Other MS patients recognized that they had the ability to help fellow MS
patients, just like past MS patients had done to help them. If MS patients had not
participated in the clinical trials of the past, then the explosion of MS medication
options would have never happened and diagnosis would still be extremely slow
with high misdiagnosis rates. Mary admitted that previous research and past MS
patients helped get her an extremely fast MS diagnosis. Before this
breakthrough, doctors would have dismissed her symptoms of tingling fingers for
months, perhaps even years, depending on how quickly her MS symptoms
developed without treatment. If she could provide someone with the same
assistance, then she was willing to participate. Jaime also wanted to provide
better medication options for fellow MS patients through his participation in a
clinical trial, although at first his motivation was to help get better treatment
options for himself. His painful experience with Avonex injections inspired him to

106
want to help others to not go through what he had to go through. He also spoke
of his participation in a trial as a kind of obligation. “It [to advance science and
medicine] was basically one of the main reasons because you have to be able to
find the cure you know? Regardless you have to be able to help out to find the
cure” (Jaime Alarcon).
These sentiments were echoed by all of the MS clinical trial patients.
Many wanted to contribute to something bigger than themselves. When asked
why she wanted to participate in a clinical trial, Sarah Tomas explained, “Just to
do something good. Something good for the cause. Something bigger than
myself, you know?” Edward Foster relayed a similar thought:
I think this is probably one of the other really big parts of the reason why I decided, was that it gives me some sort of impact on MS. Like I'm having an impact on it. I don't know how huge or wonderful or great it is. But the decision to participate, I think, the biggest motivator was the feeling that I was having an impact on something that's part of me. [Edward Foster]
For Lydia Ochoa, “You know, if it's going to help somebody else that's
even better so they don't have to go through the same thing I went through. And
you know, maybe it will help to get them diagnosed a little sooner. Anything.
Okay, you know, do it. Yes, you're going to find a better cure? Okay, let's go.”
For Faye Smith, “You know…I also want to help others that are suffering, the MS
sufferers. If I could do something in research that's going to really work for me
that could also help somebody else, then I'm down for that.”
When describing additional reasons for participating in a clinical trial,
including advance science and medicine and help others with a similar diagnosis,
107
oftentimes the explanation bordered on guilt the patient felt for other MS patients
who might have more severe symptoms or a lack of opportunities for treatment.
Bruce felt that helping others through participating in a clinical trial was
necessary considering how many MS patients have more difficult MS symptoms
and disability.
That can be a good reason [to help others]. You know especially when you start googling and researching and see how many people have it worse than you. Or you see people in the 1990s when treatment was a lot less prevalent and people didn't know. They don't find out they have MS until they're 75 and by then it's too late you know. They've already had their disability. So yeah, I think if you can be involved to prevent the same type of thing from happening to other folks [Bruce Eldridge]
Likewise, Carol Heuser expressed her concern for other MS patients who
have it worse than her: “But since I have the disease and I think it's the people
who are very debilitated by it that sort of get me in the gut, in the heart more.
Because it, especially if you haven't done something and you've gotten a
disease, it's like, kind of unfair.”
Jaime also expressed concern about his fellow MS patients experiencing
worse MS symptoms and drug side effects than he experienced on Avonex.
I know what it is to go through every week taking a shot and it's really stressful. And then from what I heard, there's people who get even worse symptoms than what I got. So if that was really hard for me to take, just the headache, I could just imagine other people having worse symptoms than that you know? [Jaime Alarcon]
Finally, Isabelle specifically shared her feelings of guilt with me regarding
those MS patients who have not been able to experience the kind of turn around
she has had participating in her clinical trial.

108
I can never forget how far along I've come even in some of the hardest days, it's like, you know, the people that I know of who do have MS, I feel guilty when I see them, like the person I was going to refer to you, cuz I know that there is much better stuff out there now that I've been on the study and just thinking about where I've been. [Isabelle Carbajal]
Additional Reasons to Participate in a Clinical Trial
After patients were asked identify their primary reason for participating in a
clinical trial, they were asked to discuss any additional reasons that might
influence their participation in a trial based on a similar list of reasons offered in
the electronic survey (see Table 9). As shown in Table 15, more interview
participants said “To help others with a similar diagnosis” would influence them
more often when deciding to participate in a clinical trial. For survey participants,
“To advance science and medicine” was the most frequent response chosen.
Although there seems to be a contradiction in reasons for participating in a trial
between survey and interview respondents, the interview participants often spoke
about advancing science and medicine and helping others with a similar
diagnosis interchangeably. So it could be that these two reasons are two sides
of the same coin. All four of the non-Caucasian interview participants said “To
receive better medical care for my diagnosis” would not influence their
participation in a clinical trial. For the remainder of the reasons below, there
were no discernable patterns seen in the responses by race or ethnicity of the
patient.
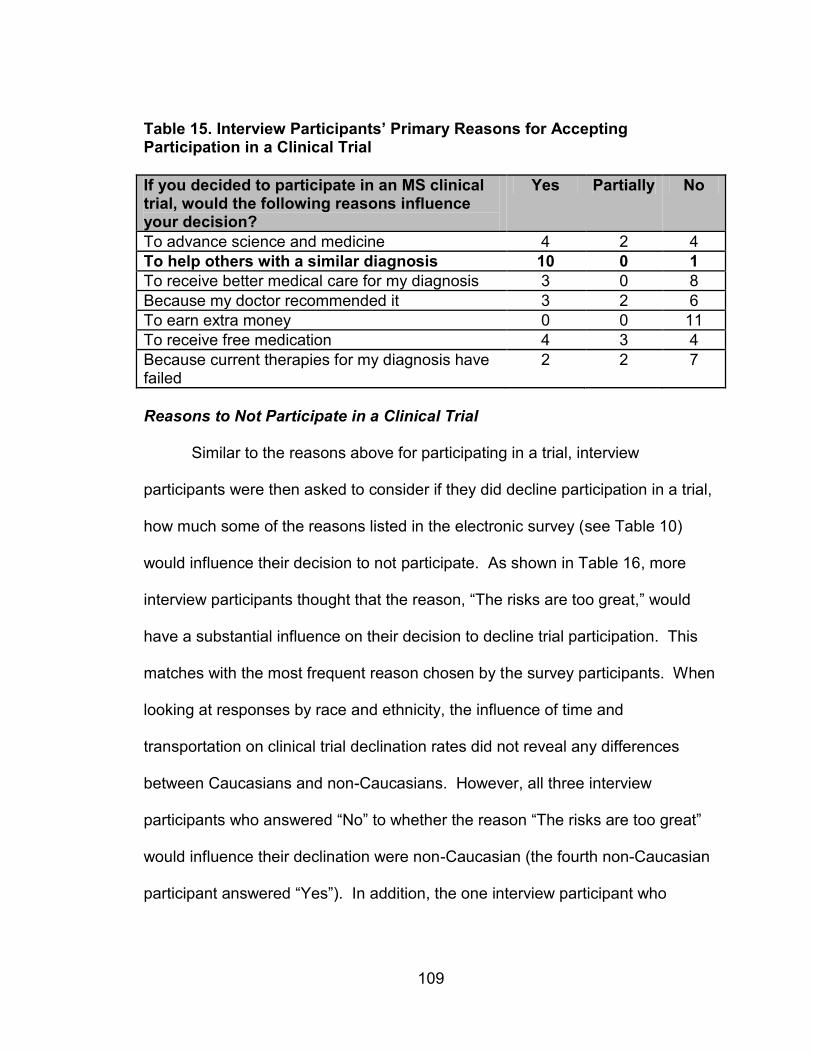
109
Table 15. Interview Participants’ Primary Reasons for Accepting Participation in a Clinical Trial
If you decided to participate in an MS clinical trial, would the following reasons influence your decision?
Yes Partially No
To advance science and medicine 4 2 4
To help others with a similar diagnosis 10 0 1
To receive better medical care for my diagnosis 3 0 8
Because my doctor recommended it 3 2 6
To earn extra money 0 0 11
To receive free medication 4 3 4
Because current therapies for my diagnosis have failed
2 2 7
Reasons to Not Participate in a Clinical Trial
Similar to the reasons above for participating in a trial, interview
participants were then asked to consider if they did decline participation in a trial,
how much some of the reasons listed in the electronic survey (see Table 10)
would influence their decision to not participate. As shown in Table 16, more
interview participants thought that the reason, “The risks are too great,” would
have a substantial influence on their decision to decline trial participation. This
matches with the most frequent reason chosen by the survey participants. When
looking at responses by race and ethnicity, the influence of time and
transportation on clinical trial declination rates did not reveal any differences
between Caucasians and non-Caucasians. However, all three interview
participants who answered “No” to whether the reason “The risks are too great”
would influence their declination were non-Caucasian (the fourth non-Caucasian
participant answered “Yes”). In addition, the one interview participant who
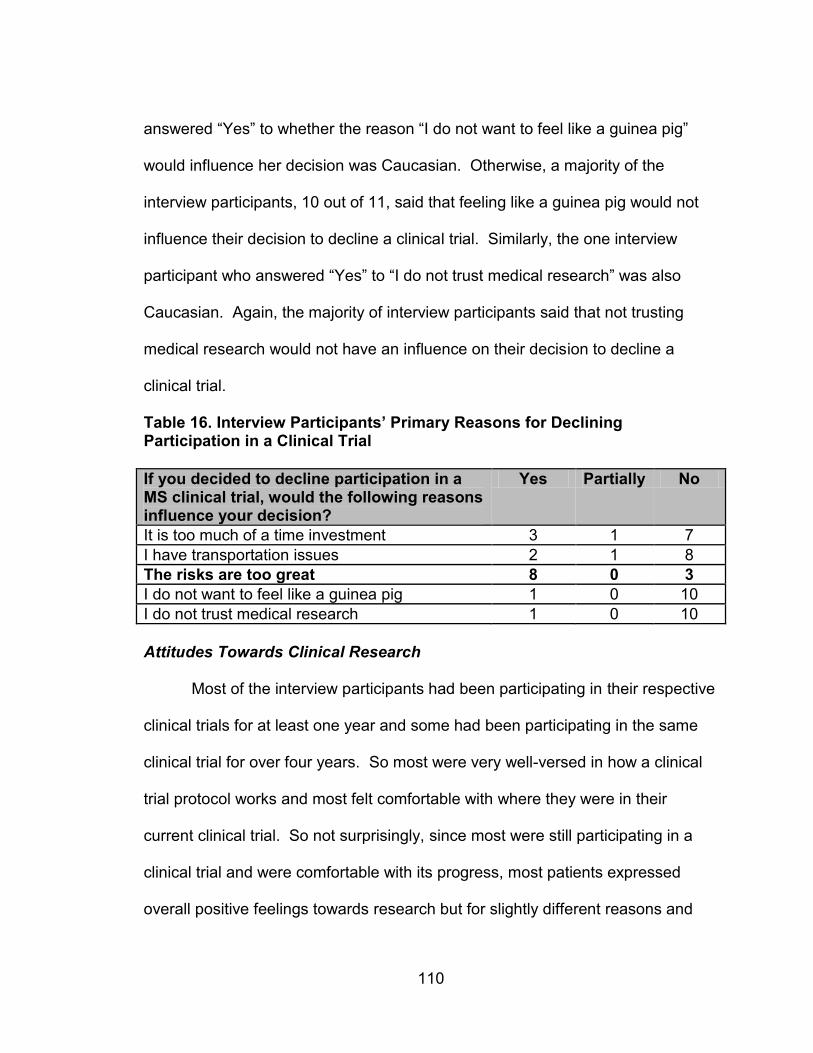
110
answered “Yes” to whether the reason “I do not want to feel like a guinea pig”
would influence her decision was Caucasian. Otherwise, a majority of the
interview participants, 10 out of 11, said that feeling like a guinea pig would not
influence their decision to decline a clinical trial. Similarly, the one interview
participant who answered “Yes” to “I do not trust medical research” was also
Caucasian. Again, the majority of interview participants said that not trusting
medical research would not have an influence on their decision to decline a
clinical trial.
Table 16. Interview Participants’ Primary Reasons for Declining Participation in a Clinical Trial
If you decided to decline participation in a MS clinical trial, would the following reasons influence your decision?
Yes Partially No
It is too much of a time investment 3 1 7
I have transportation issues 2 1 8
The risks are too great 8 0 3
I do not want to feel like a guinea pig 1 0 10
I do not trust medical research 1 0 10
Attitudes Towards Clinical Research
Most of the interview participants had been participating in their respective
clinical trials for at least one year and some had been participating in the same
clinical trial for over four years. So most were very well-versed in how a clinical
trial protocol works and most felt comfortable with where they were in their
current clinical trial. So not surprisingly, since most were still participating in a
clinical trial and were comfortable with its progress, most patients expressed
overall positive feelings towards research but for slightly different reasons and

111
their personal experience colored their particular opinions. Many of the patients
had actually seen improvements in their health which could have contributed to
the positive attitudes. Still others, even when experiencing significant side
effects, had a positive opinion about research because the study still offered
them a superior treatment to what was currently approved.
For example, Isabelle, who had a prescription for a wheelchair in her hand
before she signed up for a clinical trial and can now walk moderate distances
without a cane or crutches, is ecstatic about clinical research. She described her
experience with a clinical trial to be a life-changer, not only medically speaking,
but as a whole person. Because she regained her ability to walk again, her
whole life turned around. Before, her confidence was low and she was
depressed about her condition. When she had to use her crutches in public
places, everyone would ignore her and bump into her. She attributes her
improvement to the experimental drug in the clinical trial. Being in the trial
allowed her to walk which, in turn, allowed her to do things she hadn’t been able
to do in years. Over four years into her clinical trial, she is now happily remarried
with a supportive husband who comes with her to all of her clinical trial visits, and
she runs her own graphic design business which is so successful that she has to
turn down work. Regarding her participation in her trial and her positive
outcome, “It’s like winning the lottery. The difference is night and day. It’s not a
one hundred percent cure, but oh my God, you get your life back” (Isabelle
Carbajal).
112
For the patient currently in a wheelchair, Faye, participating in both of her
clinical trials has given her hope that she hasn’t had in a long time. Most people
take things for granted like being able to shower by yourself, being able to drive a
car, or just being able to walk in a park or through a mall. But she has seen little
improvements here and there since her clinical trial participation. She also
appreciates when her family and friends notice the improvements. She joked
that she didn’t know if it was the first clinical trial or her current clinical trial that is
making her better, but either way she is extremely happy about it. Her
participation in the trials and the small improvements have also helped to
improve her mood.
Jaime looked to his clinical trial as a chance to stop his self-injections with
horrible flu-like symptoms if he could just get randomized to the experimental
study drug. He was extremely excited when he was, in fact, randomized to
receive the experimental study drug. This meant that he no longer had to take
any self-injections, but did have to endure a 5-day infusion cycle followed by a 3-
day infusion cycle one year later. Unfortunately for Jaime, his very first infusion
turned out to be very difficult because he had an allergic reaction to one of the
pre-medications (which, ironically, is given to the patient prior to the experimental
study drug to prevent reactions) with a large body rash. It made him extremely
uncomfortable for the first day but it was easily treated with Benadryl. Within two
days of starting the infusion cycle, his MS symptoms of vision loss, body
numbness, and difficulty walking went away completely. Jaime has since

113
completed his first 5-day infusion cycle and the 3-day infusion cycle and has not
had to take any MS medications since the 3-day infusion cycle, which was
approximately three years ago. Jaime has also not experienced any MS attacks
since before starting on the experimental study drug. So he is also very
impressed with clinical research and has an extremely positive attitude towards
it, despite the initial allergic reaction.
Another patient, Christine, has positive feelings towards research despite
experiencing a moderate adverse effect from taking the experimental medication.
The main mechanism of action of the experimental oral medication she is on,
which is similar to most FDA-approved medications for MS, decreases the body’s
ability to fight infections because it reduces the number of white blood cells
available to defend from bacterial or viral intruders. The theory is that by
reducing the number of white blood cells, the body is less likely to attack its own
nerve cells in the CNS which in turn, reduces the number of MS attacks and CNS
lesions a patient might otherwise accumulate. However, it has the added side
effect of an increased risk for many infections. Two years into taking her
experimental medication, Christine developed vaginal herpes simplex virus-1
(HSV-1). HSV-1 is typically the virus responsible for cold sores but it has been
shown to also cause genital herpes. Unfortunately this is something that
Christine will have to manage for the rest of her life, in addition to her MS, and it
requires her to take another daily medication to prevent outbreaks. Despite this,
the study is still worth participating in. For her, being in the trial is bigger than
114
anything money can provide. “It’s beyond worth it to me. My life changed taking
one little pill instead of all those shots” (Christine Rogers).
Other patients had a change in opinion after deciding to participate in their
clinical trials. For Sarah, her initial opinion of clinical trials was that they were
dangerous and pharmaceutical companies do not have a patient’s best interests
in mind. She had also received a negative message about clinical research from
media sources. However, now that she has been participating in her clinical trial
for over four years, her opinion has changed to a more positive view of research
since her personal experience in her clinical trial has been positive. She also
feels that the study isn’t as risky or dangerous as she first thought when
considering participation. For Edward, he went into his clinical trial with negative
connotations from the public feeding his perceptions, although at the same time
he didn’t think he was going to be guinea pig. But his experience in his clinical
trial for a year and a half has been extremely positive and he did not expect the
level of care that he received under the trial. “I’m not saying that I expected it to
be bad, I just wasn't expecting it to be as phenomenal as it's been to be honest…
I did not expect the level of humanity to be involved in the research process”
(Edward Foster). He was immediately impressed with the clinical trial team’s
concern for him as a person and patient rather than a subject. Everyone started
conversations with him almost like they were catching up with a friend and
wanted to know what was new in his life and how he was doing instead of going
straight to the clinical testing or obtaining data from him.

115
Other positive attitudes towards research included the benefit of having
the clinical research staff stay on top of the scheduling the appointments,
sending reminders, and checking that patients remember to take their study drug.
The goal of advancing science and helping others with MS also contributed to
positive patient outlooks on clinical trials. One patient, Ronald, even expressed
his opinion of research as being fun. He said he would participate in clinical trials
anytime, all the time.
One out of the 11 interview participants, Mary, expressed an uneasy
feeling towards clinical research despite participating in a clinical trial because
she was very uncomfortable with the idea of being randomized to a placebo
instead of an actual medication. The clinical trial she is participating in provides
her with an FDA-approved medication while being randomized to a high or low-
dose of Vitamin D. Thus, she was very comfortable participating in her clinical
trial since there was no placebo arm. Even so, research in general still made her
comfortable because of the uncertainty that comes with potentially being
randomized to a placebo arm. She would resent the fact that she participated in
a placebo-controlled study if something happened to her while she was on
placebo. The unknown element of other trials served to maintain her uneasy
attitude towards research even though she admits she has had a positive
experience participating in her current clinical trial for the past year and a half.
116
Comparing Medical Care with Research Care
All interview participants were also asked to compare the medical care
they received for their MS with the research care they were experiencing in their
respective clinical trials. Only one patient, Sarah, found research care to be
more difficult than medical care, mostly because of how many appointments
were required of her for the clinical trial she is participating in. Although her visits
are once every three months, her visits are two-day ordeals which require a
minimum of 10 appointments to be made for her at many different departments
throughout the hospital. Sarah walks with a cane so mobility is difficult and
oftentimes walking between different departments on different floors or on the
opposite side of the building can be a significant challenge. Hospital parking is
also a major obstacle. Some of the appointments she has to make are at a
satellite campus about 20 minutes away from the main hospital. Even though
she knows what to expect from the clinical trial since she has been participating
in it for over four years, it is still a pain. When asked whether the all of the
inconvenience was worth being in the trial, there was a long pause before she
answered, “I think so” (Sarah Tomas). When she first started the trial she would
have said yes right away, but now the trial is not new and exciting anymore.
In spite of Sarah’s response, a majority of the participants, 10 out of 11,
agreed that there were significant differences between their medical care and
research care, and most of them attributed those differences to a similar
observation. Medical care was described as generally decent, but that there

117
were limits to what current medical care could offer for an MS patient. The
medical care focuses on trying to figure out what the underlying problem is at
first, so much of the initial time spent with a neurologist is trying to confirm the
diagnosis of MS while ruling out other neurological conditions. Once the
diagnosis is confirmed, however, there is not much current medical care can offer
except the FDA-approved medications and monitoring of MS symptoms every
few months and doing an MRI of the brain and spinal cord every year. For
Christine, medical care is like “using already established practices to treat
already established diseases, illnesses. Whereas with research there's the
promise that it's going to be eradicated all together” (Christine Rogers). So
despite the fact that with research there is no guarantee of successful outcomes
and a chance of unknown side effects, it is that very fact that research is figuring
it out as it goes along, so there is more promise that a new breakthrough could
be made.
Medical care seemed to do well with providing a diagnosis, deciding which
medication to take, and making patients comfortable for the long road of chronic
disease maintenance. Research care seemed to offer another level of care that
medical care could not provide. By participating in their respective clinical trials,
the patients came to see research as being more interested in figuring out
exactly what MS is, how a patient gets it, why certain medicines work better with
some patients and not others, or trying to find better medications and ways to
treat MS. With research there are more eyes watching an individual patient and
118
the research staff pays more attention and asks more questions to understand
how the patient is doing. For Bruce, in medical care no one is watching or
double-checking that he takes his medications properly or closely watching all of
his minor MS symptoms. With research care, the staff takes care of all the
details for the patient so there is little to worry about. Additionally, as a medical
patient, you might be one out of hundreds of other patients, whereas as a
research patient, you are often only one out of four patients in that clinical trial at
that site.
Jaime much preferred his research care to his previous medical care. He
often felt that with his medical care, they saw him every three to six months just
to check in but they didn’t really worry about him until he walked in the clinic door
again. With his research care, even though his visits were every three months,
he was required to do blood tests and phone calls every month, so he felt that
the research staff were keeping a much closer watch over him and his MS
symptoms. He also liked that fact that when his research doctor told him he was
doing well, he actually believed it since it was based on all of the data they were
collecting on him. This is in opposition to his medical care where he felt that his
medical doctor didn’t have as much data to be able to say how he was doing with
any certainty.
Although Edward didn’t have much medical care experience for MS
outside of his clinical trial, with other specialists he has seen, the focus is more
on trying to figure out what the problem is, but not how to solve that problem
119
once it is identified. In his research experience, Edward felt like the focus was
more on him as a person rather than a patient. For him, being in research “feels
very self-determinate. I feel like I'm very much in control of my health or my path
even though I'm in a clinical trial” (Edward Foster). He explained that despite all
of the circumscribed procedures and protocols of the trial, ultimately it was his
decision to choose to participate in order to help improve his health and possibly
the health of other MS patients. He feels that all of his decisions about his health
are his and are completely within his control. Edward explained that he feels like
he is planting some seeds and working on a garden, the effects of which cannot
be seen right now, but at some point in the future it will be extremely rewarding.
Although most patients had a very positive view of research care and an
average opinion of medical care, a couple patients had a positive view of
research care combined with a negative view of medical care. For Isabelle, her
experience at the local community hospital made her feel like just a number. She
also had to meet with so many different doctors, so there was no consistency in
her care. “When the doctor would see me for the first time they would show up
with this thing [her medical chart] and I knew they didn't read it and didn't know
what I was seeing them for” (Isabelle Carbajal). She admitted that her
experience was probably due to the fact that it was a large, regional community
hospital that was overwhelmed with patients like her. But it still made her feel
like a lost number in a sea of thousands of other patients. She felt like her
medical care for her MS was not satisfactory, so when she was given the

120
prescription for her wheelchair, she refused to fill it and wanted to look to clinical
trials instead. That’s when she told her neurologist that she was going to take
things into her own hands and raise money to do an MS stem cell trial abroad.
“You have to be your own advocate one hundred percent because you won't get
the care you need” (Isabelle Carbajal). It wasn’t until she mentioned her intention
to her neurologist that he told her about the clinical trial at BAMC, a mere 30
minutes from her house rather than a plane ride away. Isabelle much preferred
the research care because she wanted more than just maintenance for her MS
diagnosis; she wanted to get better.
Ronald also had a more negative view of medical research. For him,
medical research represented the unknown because every time he went in for an
appointment, his care or treatment might change, or his neurologist might inform
him of a new affliction. He remembers leaving many of his medical care visits in
tears because of the adjustments he had to make to accept his disease. The
uncertainty, especially immediately after his MS diagnosis was scary. With
research care, he always knew what to expect and it was very clearly laid out for
him. There were absolutely no surprises and all trial activities were set. Nothing
about his research experience was ever upsetting like his medical care visits
sometimes were.
Guinea Pig
It is difficult to talk about medical research and clinical trials without talking
about the concept of guinea pigs. The idea of being a guinea pig in a clinical trial
121
is an image that looms large in the public consciousness when it comes to
medical research. Oftentimes the term has a negative connotation implying
experimentation on unknowing people without their knowledge or consent of
what the true risks and consequences of their participation really are.
Interestingly, 5 out of the 11 interview participants independently mentioned the
term “guinea pig” before being officially asked about it as part of the semi-
structured interview. One additional patient independently referred to a test
monkey and used the term in a similar vein as the guinea pig users. Thus, at
least half of the interview participants were familiar with and freely associated the
term “guinea pig” with their participation in a clinical trial without being prompted.
When all interview participants were asked how much the idea of being a guinea
pig would influence them to decline participation in a clinical trial, 10 out of 11
patients vehemently responded “No.” Despite most agreeing that this would not
influence them in declining a clinical trial, the respondents were split on whether
they thought they were guinea pigs or not. About half of the patients said they
were not guinea pigs and would not decline a trial, while the other half said they
were guinea pigs and still would not decline a trial.
For patients who did not feel like they were guinea pigs, there were a
variety of explanations and caveats provided. Patients do not feel like a guinea
pig:
Because you always feel like a person and patient, not a test subject
Because you do not feel demeaned or dehumanized

122
If you chose this and know what your reasons are for participating
Because study risks are so low
Even though you are a guinea pig
But would be if you were in a placebo study
Many interview participants repeated the idea that they did not feel like a
guinea pig because they never felt like they were a test subject where the
research staff was just collecting data in a standardized, sterile fashion. It always
seemed that the research staff genuinely cared about them and their wellbeing
as a person. Even when a hand dexterity test or an audio cognitive test needed
to be administered, patients never felt dehumanized or demeaned and
understood that this data was necessary in order to determine whether the study
drug was making any significant clinical improvements for MS patients. “I think
the whole term guinea pig or lab rat…is to feel dehumanized, to feel like you're
not a person… I've never once not felt like a patient in any aspect” (Edward
Foster).
One patient, Carol, explained why she didn’t feel like a guinea pig and, in
fact, embraces the title in jest when she explains to friends that her treatment for
MS involves being a guinea pig at BAMC. The main reason she doesn’t feel like
a guinea pig is because she chose to participate in the trial and she knows
exactly what her reasons are for agreeing to participate in the trial. In a sense,
she is taking ownership of her decision to be in the trial and it is that agency that
helps her rise above the status of guinea pig. “I feel like it's not a guinea pig kind

123
of thing. I'm choosing to do this and I know what my reasons are for doing it too.
It's not like I'm just going out there and saying, hey go ahead and stick me [draw
blood] for the fun of it. There's reasons and objectives behind it” (Carol Heuser).
Some of the patients did not feel like guinea pigs because their risk
perception of the clinical trial they were participating in was low. For Bruce, his
trial involved taking a currently approved MS medication, Copaxone, which has
already been on the market for almost 20 years. In addition to taking the
Copaxone, he is being randomized to a high or low-dose of Vitamin D. Although
he doesn’t know which dose he has been randomized to, Bruce was already
taking Vitamin D as a supplement before the trial so this was something that he
wanted to continue taking and the chance of having an adverse reaction to
Vitamin D is extremely low. Although he didn’t speculate, it does raise the
question about whether he would feel like a guinea pig if he considered the risk
of a clinical trial to be higher than his current experience. This sentiment was
explicitly expressed by one of the patients who did feel like a guinea and is
described in more detail below.
Echoing Bruce’s response, Lydia agreed that she didn’t feel like a guinea
pig in the clinical trial she was participating in which is the same one as Bruce
with the Vitamin D. But she would feel differently if she were participating in a
trial where there was a chance that she might get randomized to placebo. It is
that unknown factor that would make her a guinea pig in that case. So because
she feels that there are fewer unknowns with the Vitamin D trial, she does not

124
currently feel like a guinea pig. She did admit though that being a guinea pig is a
good thing because there is no other way to figure out whether a new medication
works before giving it to the general public. So even though it does have a
negative connotation, it serves a positive purpose and will benefit someone one
day.
Another patient made a distinction between feeling like a guinea pig and
being a guinea pig. “I never thought I was a guinea pig although I am. But I
never felt like a guinea pig… If I felt like a guinea pig, I probably wouldn't have
done it” (Sarah Tomas). Sarah explained that she never felt like a guinea pig
because she was always treated humanely and has had a very positive
experience throughout the four years she has been on her clinical trial. Although
for her, the fact remains that she is a guinea pig since she is helping test out an
experimental medication. So there is a component of her participation that
requires that she submit herself, like a guinea pig, to testing of a new drug.
For patients who did feel like they were guinea pigs, there were also a
variety of explanations provided. Surprisingly, even though these patients did
feel like they were guinea pigs, this feeling had zero influence on their
hypothetical declination of a clinical. Patients do feel like a guinea pig:
But it is worth it to help with MS
But that’s what it takes to do research
But you benefit from being in the study
But you have a good handler and a deluxe wheel

125
This group of patients did not have any hesitation in admitting and
acknowledging that they were, in fact, guinea pigs for participating in their
respective clinical trials. Faye admitted, “I feel like a guinea pig but…It doesn't
bother me. I don't care about that. I want to be a guinea pig in order to help
somebody else deal with this illness because if I can be a guinea pig and help
others with this, then I've done my job” (Faye Smith). She spoke of her role
almost as if she were doing her duty to help someone else deal with the illness
like she has to. She also approaches this role with no fear. “I'm not scared to be
a guinea pig. I'm not scared to be a test dummy” (Faye Smith). In a sense, her
sacrifice playing the role of guinea pig is worth it to her if it can help someone
else in the future dealing with MS.
Jaime also freely admitted his guinea pig status and explained that it was
the literal truth. People participating in clinical trials are literally guinea pigs
because experimental drugs are being tested on human beings. However, doing
testing on humans is what it takes to make progress in medical research to find
better treatments, and hopefully a cure from MS. Research cannot test new
drugs in animals forever. At some point if humans need to take the medication,
the medication needs to be tested in humans. In a way, Jaime sees his guinea
pig status as a logical outcome of the process new pharmaceutical agents are
required to go through to gain FDA approval. Being a guinea pig is what it takes
to do research.
126
Another patient who fully embraces her status as a guinea pig also freely
posts that status on her Facebook page. There is no escaping being a guinea
pig when signing up for a clinical trial. However, according to Isabelle, her
guinea pig status does not go uncompensated. She feels that despite being a
guinea pig, she reaps the benefits of participating in the clinical trial. Submitting
herself to a clinical trial as a guinea pig is a minor effort compared with the many
positive outcomes she experienced as a result of her participation. From
Isabelle’s perspective, in return for her service to science, she was able to go
from wheelchair to walking without assistance. This would be a significant
benefit from being a guinea pig, but a benefit that can never be expected or
guaranteed.
Christine seemed to have the ability to be more calculating about
becoming a guinea pig. She doesn’t entirely like the fact that she is a guinea pig,
but she weighed many factors that ultimately resulted in her participating in a
clinical trial. One factor was that her clinical trial was a Phase II trial, so she
already knew that this was not the first time the study medication was being
looked at in humans and there was safety data available from the Phase I trial
that put her more at ease. Additionally, she saw the level of care and extreme
precautions required as part of the trial to monitor and prepare for any possible
side effects in patients. There was also a level of expertise that was apparent in
the research staff that was taking care of her throughout the trial. All of these
factors combined to help solidify her decision to be part of the clinical trial, but
127
she felt secure in the fact that she would be well taken care of and watched over
by expert staff. “Of course I'm a guinea pig, but I'm a guinea pig in pretty good
hands so I'm alright. It's a nice cage. It's got the deluxe wheel from the deluxe
pet store. I’m good” (Christine Rogers).
BAMC Mystique
Interview participants were asked whether recommendations from their
doctor would make them more likely to participate in a clinical trial or if opinions
from friends and family members would sway them to make one decision over
another. Generally, most participants revealed that neither recommendations
from their doctor nor opinions from their family and friends would significantly
influence their decision to participate in a trial. Most patients appreciated the fact
that when the clinical trial was first introduced to them by their neurologist, it was
not recommended per se. Instead, patients described it as a free offering,
explained in detail, but with no pressure to choose it. It was explained in a
matter-of-fact way and left for the patient to decide whether or not they felt it was
a good fit. Additionally, most participants admitted that any dissent from family
and friends about participating in a trial would not be tolerated or influence them
to choose differently. Those who did experience resistance from family and
friends said it was merely their choice to make and their family would ultimately
learn to accept it, which all of them did.
Surprisingly, these two reasons for participating in a trial did not seem to
be significant factors when these MS patients were making their decisions about

128
entering a trial. However, an additional factor, which was not explicitly asked
about in the semi-structured interview, did come up independently in 8 out of the
11 interviews. This factor was related to the perception that patients had of the
hospital the trial was being conducted at, BAMC. Patients often expressed their
fascination with and respect for BAMC’s name, reputation, and high status
compared with other regional hospitals. BAMC’s mystique came up so often in
the interviews that it is likely a bigger influence on patients deciding to participate
in a clinical trial than originally accounted for. The status of BAMC is a factor that
may play a role in potential clinical trial participants’ decision-making process.
For Jaime, he came to BAMC specifically to start his clinical trial since he
was being seen at the local community hospital for his regular medical care.
What helped him feel more comfortable moving to BAMC and participating in a
clinical trial was the fact that BAMC had a good reputation. So even though he
was personally unfamiliar with the doctors that were going to take care of him, he
knew he at least could trust the BAMC name.
The place makes a lot of difference because people can trust this place you know, trust the hospital itself just by the name, the reputation that it has. That can make a lot of difference. It does make a lot of difference. Especially because you can't trust the doctors at the beginning, you don't know what you're getting yourself into so you have to be secure about something. [Jaime Alarcon]
Regarding the unknown risks inherent to participating in a clinical trial,
Jaime felt secure in the fact that even if something bad happened to him as the
result of the trial, BAMC would be able to take care of him. Jaime had complete
129
trust in the BAMC name. “You can't really distrust BAMC. You know, it's a well-
known hospital. You can't really say, Oh they're going to mess up my health and
stuff. And if they do, they'll find something to be able to get you back on your
feet” (Jaime Alarcon).
Similar to Jaime, Edward felt that BAMC’s name and reputation for
conducting medical research and being a teaching hospital put him at ease when
he decided to participate in his clinical trial. “BAMC does a lot of research in
general, but you know, medically, BAMC is well known to be a great place for
medical research, a teaching hospital, things like that so I feel like any concerns
they might have are very much allayed by the name of the institution” (Edward
Foster).
In Isabelle’s descriptions of BAMC, her language was much more extreme
and seemed to have a significant influence on her decision to participate in a
clinical trial. Keeping in mind that Isabelle had an amazing recovery of her
walking ability that she attributes to the experimental medication she was taking
in her clinical trial, she compares the care she received at her local community
hospital with the care she received at BAMC on the clinical trial. “I mean I went
through a lot of stuff that was very helpful at [the local community hospital] but it
was almost like I graduated and now I'm in the BAMC program. I kind of see
regular care as down here and the study and BAMC up here and if I was to back
here [down] it would be like eating my vomit” (Isabelle Carbajal). Isabelle also
remembers that when she was a child, her brother had gone to BAMC to get care
130
for a mysterious skin disease that they were able to treat and cure. She
speculates that from that initial encounter, even though it was a long time ago,
she must have formulated an opinion about the kind of hospital BAMC was. “I
must have identified BAMC as being this great hospital with doctors in the sky or
something” (Isabelle Carbajal).
Other patients seem to proclaim BAMC’s status as a foregone conclusion.
Oftentimes patients, like Mary Conners, would just use the phrase, “Oh, well it’s
BAMC,” as if the phrase itself was self-explanatory. When pressed to further
explain what this statement meant, most had difficulty articulating the reason that
BAMC had this status in their minds. For Carol Heuser, “This is BAMC that I'm
going into, so it wasn't like some little Podunk medical center in the middle of
nowhere. It's BAMC.” Christine Rogers explained that “BAMC is more deluxe.”
Independent of each patient’s explanation, the commonality between all patients
was that BAMC was held in high regard because of its reputation as a good
medical hospital, a good research hospital, and a good teaching hospital which
imbues an almost mystical quality to it, such that patients were put at ease when
deciding to participate in a clinical trial conducted by BAMC. BAMC was perhaps
even given collective biomedical authority by these MS patients, as well as the
general public, who had heard of and accepted the reputation of the medical
center as an additional guarantee of safety and security.
131
Trust and Distrust
As discussed previously, there are many studies that show minority
groups distrust clinical research and the medical industry in general. This was
definitely a theme that was worth exploring in more detail with the interview
participants. Unfortunately, because patients who had declined a clinical trial
were not easily accessible, the perspectives on trust in research from those that
did participate in a clinical trial may be skewed toward a lack of distrust. By not
interviewing those who declined participation in a trial, this study may be missing
perspectives from those people who would agree that they distrust medical
research and that it heavily influenced them to decline to participate. However,
even though all of the interview participants had agreed to participate in a clinical
trial, the patients may have a sense of whether or not there was a feeling of
distrust that they were familiar with from their family or community.
With this limitation in mind, all 11 interview participants were asked about
whether or not distrust in medical research would influence them to decline a
clinical trial. Only 1 out of 11 said that distrust would influence him to decline a
clinical trial. Interestingly, that one patient was Bruce who is Caucasian, not non-
Caucasian as the medical literature would suggest. Bruce’s reasons for
distrusting research had to do with distrusting pharmaceutical companies and
their motives. Ultimately, pharmaceutical companies are for-profit companies
that have an obligation to their stakeholders. They have to report to Wall Street
and send out their quarterly earnings reports. Bruce admits that they are trying
132
to make the world a better place, and he is all for a capitalistic society where the
free market is the judge of success and failure, but inherently this design means
that studies results will be biased. For example, even for the clinical trial he is
participating in, if the study doesn’t show a positive result for using Copaxone
and Vitamin D to reduce MS relapse rates, the pharmaceutical company is not
likely to report the negative findings to the public. Pharmaceutical companies will
strategize ways to increase profit, perhaps by pushing sales which sometimes
cause physicians to overprescribe medications unnecessarily, or they might be
doing a clinical trial on a new drug because their patent on another drug is
running out and they need to identify another revenue source.
This distrust in pharmaceutical companies described by Bruce was the
only form of distrust that was uncovered during the interviews with all
participants. Like Bruce, three additional patients brought up the distrust in
pharmaceutical companies independently: Christine, Sarah, and Faye. Unlike
Bruce, this distrust would not influence their decision to participate in a clinical
trial. For Christine, she is extremely suspicious of the profit motive of
pharmaceutical companies and how those without insurance are unable to
benefit from great medical discoveries because the medications are so
expensive and out of reach. Despite her distrust, she does differentiate between
distrust for the pharmaceutical company itself and distrust for research.
According to her, it is understandable to distrust the pharmaceutical companies,
but not to distrust the research. In fact, it is good to have a healthy distrust for
133
the system into which the research is placed, but not the research itself and the
positive intent behind it which is to find better treatments and a cure for MS.
Christine feels that being in a needful situation, like having a disease like MS and
needing to find a better treatment for it through a clinical trial, would significantly
increase someone’s ability to trust research. Someone might consider that
coercion, but the trial is also offering help to a patient who needs it.
A patient who fell into the category of her needful situation increasing her
ability to trust research was Sarah. Sarah does not trust pharmaceutical
companies because all they care about is money. These companies just want to
keep patients sick because that is how they make their money. If they find a
cure, then their profit stream disappears. She believes that pharmaceutical
companies are not really trying to cure anything. Given this extreme distrust,
Sarah had to struggle with her decision to participate in her clinical trial. Her
sister and family were against her participating in the trial at first too since they all
had the same opinion about pharmaceutical companies as Sarah. Although
Sarah Tomas felt like she was “…going to fall right into their web,” she also
needed an MS treatment that didn’t have as many side effects as the FDA-
approved medications currently available. Ultimately she came to the decision
that she needed to participate in the clinical trial for herself and for the greater
good of all the MS patients who would come behind her.
Like Sarah, Faye thinks that pharmaceutical companies are trying to figure
out what causes MS and how people get it and how to treat it. However, she is
134
very negative about the prospect of pharmaceutical companies finding a cure,
because if they do, they will go out of business. Why would they find a cure if
they will lose money and jobs? Politics is a powerful force that works behind the
scenes, so although she doesn’t think that pharmaceutical companies will find a
cure, she does think that they will continue to find different treatments for MS.
Even if the pharmaceutical company doesn’t cure her, at least they can keep her
going. Given this less ambitious motive of finding better treatments instead of a
cure, Faye does trust that they’re doing it for the right reasons and that they are
not going to harm you intentionally. So Faye trusts pharmaceutical companies in
this regard. She also finds it incomprehensible when other MS patients have told
her that they were scared to get their blood drawn, even as part of regular
medical care, because they feared that their blood was being sold and distributed
without their knowledge and that some researcher might be using their DNA to
make a clone. Compared with Bruce, Christine, and Sarah, Faye seems to have
a more tempered distrust of pharmaceutical companies that ends at their motives
for finding a cure. Otherwise, they are trying to at least find better treatments and
right now, that is good enough for Faye.
Out of the four patients who expressed distrust for pharmaceutical
companies, three were Caucasian, Bruce, Christine, and Sarah, and one was
African American, Faye. Although this is a small sample of interview participants,
this result does not mirror studies suggesting that it should be non-Caucasian
populations who have a higher distrust for medical research. For the four non-
135
Caucasian patients who did participate in the interviews, it could have been a
quirk of their individuality that three out of four had no issues of trust with medical
research. In a way, they were self-selected for by the nature of participating in a
clinical trial. Non-Caucasian patients who did distrust research would likely not
have participated in a clinical trial in the first place. In order to fully explore this
idea at the end of the interview, all patients, both Caucasian and non-Caucasian,
were specifically asked if they were familiar with the idea of medical distrust in
minority populations and if they agreed or not based on their own experience and
knowledge. They were also asked to share their thoughts about
underrepresentation of minority groups in clinical trials.
Out of the four non-Caucasian interview participants, two were not familiar
with the idea that there is medical distrust among minority populations and had
never heard anyone mention it before. For Isabelle who identifies as Latina, she
was surprised to hear that there were many studies showing that minorities were
more likely to distrust medical research than Caucasians. In her experience, her
family did not know much about clinical trials but they have been amazed to see
the progress that she has made since starting her trial. In fact they are extremely
happy for her because she has come so far in the past four years. She doesn’t
remember any resistance or negativity when she was first considering the trial.
Ultimately, her family was supportive of her decision. Unfortunately, lack of
knowledge about clinical trials may be one factor influencing trial participation
rates that the family experienced personally. For Isabelle, it was only after she
136
educated herself about clinical trials and demanded to participate in one, that her
neurologist gave her information about how to access a local clinical trial. If she
had never made this demand, she might still be unaware that clinical trials are an
option. Prior to her experience, Isabelle says her mother would have participated
in a clinical trial for dementia if they had just known about it at the time. Although
distrust was not an issue for Isabelle, her experience may point to how a lack of
knowledge and access to clinical trials and provider bias might affect participation
rates.
Faye, who identifies as African American, is the second non-Caucasian
participant who had never heard that minorities are more likely to distrust
research than Caucasians. Like Isabelle, Faye was also surprised by this
statistic and she attempted to postulate reasons why this might be the case. She
wondered if the individuals who didn’t trust research might not trust anyone in
general, so it might be less about a distrust of research specifically and more
about having a distrusting disposition. She also wondered if lower minority
participation rates in clinical trials might be related to logistical reasons, like
transportation issues, instead of trust issues. These factors, she reasoned,
should not be restricted to a particular race or ethnicity. Ultimately, Faye did not
think that more distrust in non-Caucasian patients made any sense because if
anyone, regardless of race or ethnicity, was in her situation, they would make the
same decision to participate in a clinical trial.

137
The remaining two non-Caucasian interview participants, Jaime and Lydia
who both identify as Latino, had heard of minority distrust of medical research,
although it did not personally affect their decision to participate in a clinical trial.
Jaime’s explanation for the distrust and subsequent underrepresentation in
clinical trials was that many minority groups do not like to go to the doctor and
are extremely conservative. His sense was that people will go to the doctor
when necessary, but will not do more than is necessary for their care, which
would likely include participating in a clinical trial. Despite these characteristics,
Jaime admitted that the problem of underrepresentation of minorities in clinical
trials probably has less to do with being a minority and more to do with individual
preference. In his view, even a high proportion of those in the majority
(Caucasians) do not take the opportunity to participate in clinical trials.
Lydia has also heard of distrust of medical research in minority
communities and has also had personal experience dealing with the
consequences of this distrust. Many years ago, her grandmother was diagnosed
with breast cancer but it had gone into remission twice. The third time,
unfortunately, it came back and had spread to her liver. During her treatment,
Lydia’s grandfather already had a difficult time dealing with the fact that his wife
had breast cancer. So when Lydia’s grandmother was offered a chance to
participate in a clinical trial for breast cancer, Lydia’s grandfather would not allow
her to participate. According to Lydia Ochoa, “he was a very old school Mexican
man” who was having trouble accepting his wife’s illness, so the idea of

138
participating in a clinical trial that might help other people he didn’t know or care
about was not first on his list. He was stubborn and if he didn’t directly know who
it was going to help, then it wasn’t his problem. At the time, her grandmother
was okay with not participating, but later expressed regret because she missed
an opportunity to potentially help others. During the recruitment for the breast
cancer trial, Lydia remembers her mother making a comment that there were
more Caucasians than minorities being recruited into the trial and that they
needed to make more of an effort to recruit Latinos since they are the minor
majority. Lydia’s explanation was that this distrust, at least from the Mexican
community, might be due to a lack of information about medical research.
Information that is provided needs to be translated carefully because it could
have a negative effect on their decision to participate in a clinical trial. She
suggests not focusing so much on the risks and presenting the benefits first.
For the remaining seven Caucasian interview participants, most (six out of
seven) were not familiar with the idea that minority groups were more likely to
distrust medical research and were under represented in clinical trials. Several
of them offered up some potential reasons why this might be the case and most
of the posited reasons had to do with logistical barriers that would create an
illusion of distrust and measurable underrepresentation in clinical trial. Sarah
wondered if the restrictive inclusion criteria listed in clinical trial protocols makes
it difficult for many patients to qualify to participate. The protocols themselves
could be inadvertently excluding particular populations of patients. Edward

139
suggested that decreased minority access to health care might contribute to the
lower representation of minority groups in clinical trials. Time restraints and lack
of knowledge about trials could also be factors. Carol speculated that location
and proximity to a large medical center would limit access to studies and care.
Bruce wondered if the lower rates of minority participation were only a reflection
of the lower incidence rates of MS in minority populations.
The one Caucasian interview participant who was familiar with the idea
that minorities are more likely to distrust medical research was Christine.
Christine explains that minorities, but African Americans in particular, have every
reason to distrust the medical system. It is a system that has excluded them,
and when it does include them, provides them with improper medical care. They
have a higher rate of mortality, a high rate of disease, and a lower rate of care.
They often get lower care from the same doctor as their Caucasian counterpart.
For Christine, the motive behind the distrust is completely understandable.
Christine admits that it was a privilege for her to even have the choice to
participate in a clinical trial.
Risk
As seen in both the electronic survey and interview responses, the
concept of risk plays an important role in determining whether someone will
decide to participate in a clinical trial. As discussed earlier, the interview
participants were asked whether or not the following reason would influence their
declination of clinical trial participation: “The risks are too great.” A majority of

140
interview participants, 8 out of 11, said that this reason would definitely influence
their decision to decline a trial if they determined that the risks were too great.
Although there was only one planned question about risk in the semi-structured
interview, the concept of risk was a theme thread woven throughout all interviews
in some way.
Placebo Risk
When patients say that they think the risks are too great to participate, the
assumption is that the risks of the experimental drug, which is not FDA-approved
and has only been tested in a small number of other humans, are the risks that
patients are referring to. Although the risks of the experimental drug are not
negligible, in these interviews it became clear that the most important risk a
patient could take was the risk of NOT getting the experimental drug. Many MS
clinical trial designs involve the possibility of being randomized to a placebo arm
where a patient would not be receiving the experimental drug. It is this scenario,
where a patient is randomized to receive placebo instead of the experimental
drug, which is considered to be the ultimate risk. The 11 interview participants
represent six different clinical trials being conducted at BAMC. Those six clinical
trials are listed in Table 17 below.
The design of each trial is unique because some, like the Acorda Phase I
trial, involve randomization to four different doses of the study drug or a placebo;
thus, there was an 80% chance that a patient could be randomized to one of the
study drug doses. This trial, which is rare for MS clinical trials, allowed patients

141
Table 17. Current MS Clinical Trials Being Conducted at BAMC
Trial Phase Drug Study Design Primary Side Effects
Trial Length
Acorda I Single IV infusion
Randomized to study drug or placebo (80% chance of study drug)
Allergic reaction, anaphylaxis
90 days
Actelion II Daily oral pill
Randomized to study drug or placebo for 6 months; then all pts on study drug (75% chance of study drug)
Cardiac issues, macular edema, increased risk of infection, liver problems, shortness of breath
4 years+
Biogen II IV infusion Q4W + Avonex
Randomized to study drug or placebo + Avonex (80% chance of study drug)
Allergic reaction, anaphylaxis
2 years + extension
Genzyme III IV infusion, yearly for 2 years or Rebif
Randomized to study drug or Rebif (50% chance of study drug)
Allergic reaction, anaphylaxis, immune thrombocytopenia, kidney disease, thyroid disorders, increased cancer risk
4 years+
Opera III IV infusion Q6M + Rebif
Randomized to either study drug or Rebif (50% chance of study drug)
Allergic reaction, anaphylaxis
2 years + extension
Vitamin D N/A Daily oral pill + Copaxone
Randomized to low or high dose study drug + Copaxone (50% chance high dose study drug)
Hypercalcemia 2 years
Adapted from: National Multiple Sclerosis Society, 2014, Treating MS: Medications, http://www.nationalmssociety.org/Treating-MS/Medications, accessed December 16, 2014.
142
to be on their current, FDA-approved MS medication in addition to being
randomized to either the study drug or placebo. Thus, the risk of being
randomized to the placebo arm in this trial may be minimized since MS patients
do not need to go without their normal MS treatment for the duration of the trial.
In the Actelion Phase II study, patients could be randomized to one of
three different doses of the study drug or a placebo for a 6-month period. After
this period, all trial patients, no matter what arm they were initially randomized to,
would be assigned to take the study drug for the remainder of the trial. With this
trial, there is a potential that a patient could be completely off of all MS
medications for a six-month period if they were randomized to the placebo arm.
The Biogen Phase II trial required all patients to take the FDA-approved MS
medication, Avonex, in addition to being randomized to the study drug or
placebo. Even if a patient was randomized to placebo, they were still guaranteed
to be taking Avonex. The Genzyme Phase III trial required that patients be
randomized to either the study drug or Rebif, an FDA-approved MS medication.
There was a chance for patients who were randomized to receive only Rebif to
switch over to receive the study drug after spending a minimum of two years in
the trial. The Opera Phase III trial was designed to randomize patients to either
the study drug or Rebif. The Vitamin D trial is in a slightly different category
since the study drug, Vitamin D, is not considered an experimental drug, but the
study design still involved randomizing patients to receive either low or high-dose
143
Vitamin D with the added requirement of taking Avonex, another FDA-approved
MS medication.
Understanding the risk that a placebo poses requires consideration of
what might cause harm to an MS patient. The biggest harm would be an
increase in MS symptoms, having an MS attack, and/or experiencing disability
progression. Having an MS attack while in a clinical trial can be difficult to deal
with because there are many different factors at play and potential causes. One
potential cause is the fact that the patient may have been randomized to the
placebo arm, so if they are not taking any MS medications, they may be more
likely to experience an MS attack. Another cause could be that the patient was
randomized to receive the study drug, but it turns out that it is not as effective as
other FDA-approved medications at reducing the relapse rate in MS patients.
Another potential cause could be related to the nature of MS itself. For example,
the patient may have been randomized to the study drug treatment arm, and the
study drug could be just as effective as other FDA-approved medications, if not
more effective, but the patient could still have an MS attack.
Remember that MS is extremely unpredictable in the frequency, duration,
and severity of attacks. Even for FDA-approved MS medications, none of them
are a cure, and all of them only reduce the rate of MS attacks in patients. Given
that each individual MS patient will experience MS symptoms and attacks
differently from the next, it can be almost impossible to determine whether a
particular MS attack would have been due to the natural course of disease, the

144
ineffectiveness of a particular medication, or because the patient is actually on
placebo. This is why MS clinical trials are so important because the only way to
understand if an experimental medication has any effect on lowering the relapse
rate is by gathering aggregate data and seeing if there are any differences in the
actual relapse rate of MS patients in the study drug group compared with the
placebo group (or currently approved MS medications). Unfortunately, parsing
out the individual causation of MS attacks is impossible given our current
understanding of the disease.
Despite this unknown, the risk of receiving placebo instead of an actual
MS medication, whether it is approved by the FDA or not, still seems to be a very
real concern for MS patients. It seems that the unpredictable nature of MS
symptoms and attacks makes patients extremely wary of not being on any MS
medication. Mary explains that she would not participate in a research study if
she did not know whether she was on placebo or the study drug. First, she
would blame herself and resent the fact that she chose to participate in a study if
something happened to her, like an MS attack. Then, she might even blame the
trial even though she is fully aware of the concept of randomization in clinical
trials and the risk she incurred. If Mary experienced a relapse or other side effect
while in the trial, it would be hard for her to justify participating in the trial at the
expense of her own health. Even if she had the “good luck” to be randomized to
the study drug, she wouldn’t know and neither would the research team or her
doctors. “That would freak me out” (Mary Conners). Mary felt secure

145
participating in the Vitamin D clinical trial since she was only being randomized to
a low or high-dose vitamin in addition to taking an FDA-approved MS medication.
Although most of the interview participants agreed that medical research
and clinical trials are necessary in order to make advances in science and the
treatment of MS, it is difficult to weigh that necessity with the potential of going
without treatment for a certain amount of time. Similar to Mary, Carol speculated
that if the clinical trial she was participating in, the Opera trial, had a placebo arm,
she would have been less likely to participate. If there was a chance that she
could get randomized to be on placebo, that would definitely be a risk to her
since her neurologist had told her she needed to be on some type of MS
medication. For her, not being on an MS medication would not be worth
participating in a trial, even with the noble goal of trying to help MS patients find
better treatments. The Opera trial offered Carol a way to participate in a clinical
trial without the risk of being randomized to a placebo arm. Although she doesn’t
know which medication she is taking, Carol can be assured that she is actually
on an MS medication, either Rebif or the study drug. Edward, who is also
participating in the Opera trial, agreed that if there was a chance that he would
be on placebo and he would have to go untreated for a certain amount of time, it
would make him reconsider participation in the trial. Lydia even relates the risk
of being on placebo as equivalent to being a guinea pig.
146
Risk of FDA-Approved MS Medications
Another surprising discovery that came out of the interviews was how
some patients considered the risk of current FDA-approved MS medications to
be the same if not worse than the experimental medications being tested in a
clinical trial. The risk of current FDA-approved medications was often related to
the number of side effects associated with taking these drugs. Oftentimes, even
for patients who never participate in the medical research world, treating their MS
is a choice between enduring different side effects. Although there are now 12
FDA-approved MS medications, all of which only slow the progression of MS
(there is currently no cure for MS), most have a significant side effect profile that
individual patients need to weigh against their tolerance for risk of MS disease
progression. Table 18 lists the current FDA-approved MS medications and a
brief side effect profile for each.
Patients who are risk-adverse tend to gravitate towards the MS
medications that have been approved the longest. These medications have the
longest track record, so in theory, more should be known about these drugs and
their side effects than the most recently approved medications. Betaseron,
Avonex, Copaxone, and Rebif are often referred to as platform MS therapy, or
first-line MS therapy, because they have been around the longest, and are the
most conservative MS medications available in terms of side effects. These
medications are often used on patients in whom MS was diagnosed quickly (so
they have little existing disease burden) and have little disease activity. If
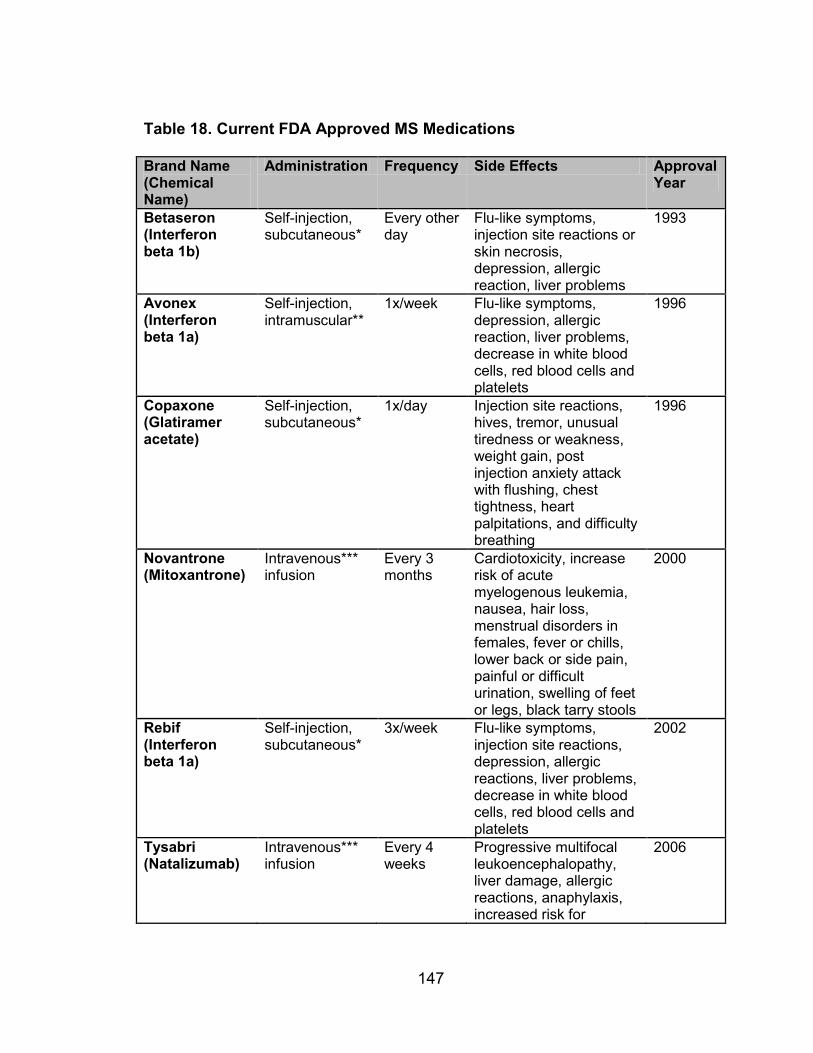
147
Table 18. Current FDA Approved MS Medications
Brand Name (Chemical Name)
Administration Frequency Side Effects Approval Year
Betaseron (Interferon beta 1b)
Self-injection, subcutaneous*
Every other day
Flu-like symptoms, injection site reactions or skin necrosis, depression, allergic reaction, liver problems
1993
Avonex (Interferon beta 1a)
Self-injection, intramuscular**
1x/week Flu-like symptoms, depression, allergic reaction, liver problems, decrease in white blood cells, red blood cells and platelets
1996
Copaxone (Glatiramer acetate)
Self-injection, subcutaneous*
1x/day Injection site reactions, hives, tremor, unusual tiredness or weakness, weight gain, post injection anxiety attack with flushing, chest tightness, heart palpitations, and difficulty breathing
1996
Novantrone (Mitoxantrone)
Intravenous*** infusion
Every 3 months
Cardiotoxicity, increase risk of acute myelogenous leukemia, nausea, hair loss, menstrual disorders in females, fever or chills, lower back or side pain, painful or difficult urination, swelling of feet or legs, black tarry stools
2000
Rebif (Interferon beta 1a)
Self-injection, subcutaneous*
3x/week Flu-like symptoms, injection site reactions, depression, allergic reactions, liver problems, decrease in white blood cells, red blood cells and platelets
2002
Tysabri (Natalizumab)
Intravenous*** infusion
Every 4 weeks
Progressive multifocal leukoencephalopathy, liver damage, allergic reactions, anaphylaxis, increased risk for
2006

148
Brand Name (Chemical Name)
Administration Frequency Side Effects Approval Year
infections
Extavia (Interferon beta 1b)
Self-injection, subcutaneous*
Every other day
Flu-like symptoms, injection site reactions and skin necrosis, depression, liver problems, allergic reactions, thyroid problems, decrease in white blood cells, red blood cells and platelets
2009
Gilenya (Fingolimod)
Oral 1x/day Cardiac issues, macular edema, increased risk of infection, liver problems, shortness of breath
2010
Aubagio (Teriflunomide)
Oral 1x/day Liver damage, significant birth defects if used during pregnancy, peripheral neuropathy, acute kidney failure, high levels of potassium, severe skin reactions, hair thinning
2012
Tecfidera (Dimethyl fumarate)
Oral 2x/day Allergic reactions, anaphylaxis, angioedema (swelling under skin usually in throat and tongue), low white blood cell count, flushing, diarrhea, nausea, upper abdominal pain (one case of PML)
2013
Plegridy (Peginterferon beta-1a)
Self-injection, subcutaneous*
Every 2 weeks
Flu-like symptoms, allergic reactions, injection site reactions, cardiac problems, anemia, low white blood cell count, thyroid problems, seizures
2014
Lemtrada (Alemtuzumab)
Intravenous*** infusion
5-day cycle, Year 1 3-day cycle, Year 2
Allergic reaction, anaphylaxis, immune thrombocytopenia, kidney disease, thyroid disorders, increased cancer risk
2014

149
Brand Name (Chemical Name)
Administration Frequency Side Effects Approval Year
*Subcutaneous = injected just under the skin **Intramuscular = injected directly into the muscle ***Intravenous = infused directly into the vein Flu-like symptoms = fatigue, chills, fever, muscle aches, and sweating Injection site reactions = swelling, redness, discoloration, and pain Depression = sadness, anxiety, loss of interest in daily activities, irritability, low self-esteem, guilt, poor concentration, indecisiveness, confusion, and eating and sleep disturbances Adapted from: National Multiple Sclerosis Society 2014.
patients experience an increase in the frequency of MS attacks or they have
accumulated a greater disease burden over time, usually they need to consider
moving to different MS medications that might be more effective. Some of the
more recently approved MS medications, like Gilenya and Tysabri, fall into that
category of second-line MS therapy. These medications might be more
aggressive in treating MS, but they usually also come with more dangerous side
effects, some of which were not realized until after FDA approval.
Gilenya, for example, was approved by the FDA for public use in 2010. It
was approved with the understanding that it caused patients to experience a
slowed heart rate immediately after taking the first dose. Thus, prescribing
instructions required that neurologists observe all patients for at least six hours
after receiving their first dose of Gilenya. Unfortunately, in December 2011, an
MS patient who received Gilenya died within 24 hours of receiving the first dose
(Food and Drug Administration 2011). A review of all reported safety data that
year revealed that ten more deaths had been reported in the European Union
from apparent cardiovascular or unknown origin. Ultimately, it was determined
that Gilenya’s contribution to all of these deaths was unclear, but the potential
150
relationship between Gilenya and the patient deaths could not be ruled out. As a
result, the FDA issued new prescribing guidance for Gilenya which requires six
hour observation with continuous electrocardiogram, blood pressure, and heart
rate monitoring, and extended cardiac monitoring for up to 24 hours in patients
who have pre-existing cardiac conditions (Food and Drug Administration 2012).
Tysabri, originally approved by the FDA in November 2004, is another
example. In February 2005, the drug was pulled off the market because three
patients developed progressive multifocal leukoenchephalopathy (PML), a rare
but serious brain infection fatal in about 20% of cases (Kappos, et al. 2011). It
wasn’t until June 2006 that Tysabri was re-approved by the FDA for use in MS
but only through a risk minimization plan that all patients receiving Tysabri are
required to register in. The plan provides close monitoring for the occurrence of
PML and other opportunistic infections. Tysabri continues to be used today
despite the risk of PML. Over time, the risk of developing PML while on Tysabri
has been better understood. A patient’s risk of developing PML increases the
longer they have been on Tysabri, especially after 2 years, if the patient tests
positive for the John Cunningham (JC) virus, and if the patient has previously
been on any immunosuppressant medication (Food and Drug Administration
2010).
It may not be such a surprise that MS patients might consider FDA-
approved MS medications to be risky, if not riskier than some of the medications
being tested in clinical trials. Even just making decisions about normal medical
151
care for MS can be a difficult choice for patients because their choice depends
on how much risk they are willing to shoulder, how tolerable the method of
administration is (can they do self-injections three times a week?), how severe
their MS symptoms are, and, of course, what their insurance companies are
willing to cover. Despite not being approved by the FDA, MS experimental
medications being studied in clinical trials usually have some kind of information
about the safety of the medication and its efficacy to date. This information is
built upon numerous animal studies required to better understand how the drug
works and how safe it is before administration to human subjects. Phase I
clinical trials provide the first safety information about the experimental drug in
humans, while Phase II and III studies further refine data about both safety and
efficacy. The most current safety and efficacy data is made available to potential
clinical trial participants so they can make informed decisions.
Given the current treatment options available to MS patients, it was
intriguing to discover that experimental medications in clinical trials were given
just as much consideration as FDA-approved medications by many of the
interview participants. In fact for Mary, who seems to be the most risk-adverse
patient out of the 11 interview participants, she would not even consider taking
some of the FDA-approved MS medications. It is too much of a risk because
they have only been on the market for a few years. “Even my mom was like,
‘They have all these pills now.’ But even those are almost too new for my
comfort...they've already gone through the trials and they've already been tested

152
and they're approved but for me I'm like, it's only been out two years. I don't
know if I'm comfortable” (Mary Conners). One of the reasons she likes her
clinical trial so much is that she is on an FDA-approved medication, Copaxone,
that was approved almost 20 years ago, and she has to take a low or high-dose
Vitamin D pill. For her, this is as low risk as she can get for a clinical trial and for
her regular MS treatment.
Sarah was all too familiar with Tysabri being pulled off of the market in
2005. She was just about to start her Tysabri infusions as recommended by her
neurologist, but the day after her insurance approved the medication, it was
taken off the market due to PML risk. So Sarah decided to go on Rebif and
remained on it for four years and endured flu-like symptoms three times a week.
The side effects were awful for her, but she was stable on Rebif and had no MS
attacks. She remained on Rebif until her body started developing antibodies to it
in 2009, so she needed to find a different drug that her body would not reject. At
this point she had moved her medical care to BAMC and they suggested Tysabri.
She went through the process of getting insurance approval, but something
stopped her from getting that first infusion. Sarah remembers keeping track of
the number of PML cases which seemed to grow by the day. It was at that point
that her neurologist recommended the Actelion clinical trial to her and she was
immediately intrigued. At the time there were no FDA-approved oral medications
for MS, so this seemed like a great alternative to the Rebif injections her body
was rejecting and the high risk Tysabri carried which Sarah was not quite willing
153
to accept. When asked about her current tolerance of MS medications now,
Sarah explained that she would not try any of the currently approved oral MS
medications but might reconsider taking Tysabri. However, if she tested positive
for the JC virus which increases your risk of developing PML, she would not start
Tysabri. It is important to note that JC virus is a common infection that is found
in approximately 50-90% of healthy adults but there are often no associated
symptoms (Bellizzi, et al. 2013).
The JC virus factor is a common concern for MS patients considering
Tysabri for treatment. Most MS patients, even if they are not taking Tysabri, are
aware of the PML risk associated with it and how testing positive for JC virus
increases that risk. Faye admitted that she was considering going on Tysabri
before she was able to qualify for participation in a clinical trial. She had even
had the blood test and found out that she did have the JC virus. Her neurologist
was trying to explain the risk statistics to her, but she wasn’t convinced even
though she apparently had a greater chance of dying in a car accident then dying
from PML. Ultimately, she remained on Avonex for almost 9 years and then
switched to Rebif a few months before entering her clinical trial in 2013.
Understanding how MS patients conceptualize risk requires taking a
comprehensive look at the treatment options available to them for regular
medical treatment and then comparing them to the risk profiles of experimental
MS medications. Many times, patients chose to enter clinical trials rather than
deal with the FDA-approved medications available to them. As discussed

154
previously, both Jaime and Christine had experienced unbearable side effects
related to their FDA-approved medications. Jaime had to endure severe flu-like
symptoms every week that left him bed ridden for 24 hours after each injection,
while Christine found her injections to be extremely painful and sometimes
caused skin necrosis at the injections sites. One thing is clear: comparing the
side effect profiles of the current FDA-approved medications with those from the
experimental medications in clinical trials requires significant effort and
deliberation no matter how risk-averse or risk-seeking a patient is. It seems that
many patients considered FDA-approved medications to be risky, if not riskier
than some of the clinical trial options.
Risk Perception of Current Clinical Trial
When asked to rank the risk level of their clinical trial, all 11 interview
participants rated their clinical trial as low risk. Even though it would be difficult
to objectively rank which of the trials was more risky than the others, it is obvious
that all the clinical trials listed in Table 14 do not have the same risk level. The
Vitamin D trial for example is the lowest risk because it involves the
administration of an FDA-approved MS medication combined with low or high
dose Vitamin D. Some participants gave a general risk level (low) while others
placed the risk level on a scale of one to ten, with one being the least risk and ten
being the highest risk they could think of. When using this scale, none of the
patients ranked their clinical trial over a score of three.
155
For the three patients interviewed participating in the Vitamin D trial, Mary,
Lydia, and Bruce, all considered this trial to be extremely low risk because the
experimental drug was Vitamin D combined with a first-line MS medication,
Copaxone, approved by the FDA almost 20 years ago. Mary always thought of
the Vitamin D study as the least intrusive way to conduct a trial since she was
going to go on Copaxone regardless of her participation in the trial, and she was
going to take Vitamin D supplements which are often recommended to MS
patients by neurologists in normal medical care. The trial mirrored what she was
going to do during her medical care anyway, so she reasoned that a researcher
might as well collect data during this process in order to try and get information
out of it that could help future MS patients. For Bruce, the only risk he mentioned
for this trial was related to confidentiality. His biggest concern was someone
finding out at work that 1) he has MS, and 2) he is participating in a clinical trial.
He is very aware of the potential for workplace discrimination if coworkers or
supervisors were made aware of either situation. As a CRC, I was always
careful to try and schedule Bruce’s trial appointments as early in the morning or
late in the afternoon as possible to minimize the amount of time he had to ask off
of work without raising any suspicions.
Both Ronald and Faye participated in the Acorda trial, which was a Phase
I, first in human trial looking at a new medication that has the potential to actually
repair damaged nerve cells in the CNS. The repair of nerve cells in MS is
something that none of the currently FDA-approved medications do and is
156
considered the “holy grail” of new MS medications. Despite this experimental
drug only being tested in animals previously, both patients ranked this trial as low
risk. Ronald did not consider it to be risky after discussing the trial with the lead
neurologist who put him at ease. He did admit that he thought about the
unknown risks, but did not dwell on this. However, he specifically omitted this
information when discussing it with his wife so she didn’t dwell or stress over the
risks. When asked if anything about the Acorda trial concerned her, Faye Smith
said, “No. Nothing. I’m a ride or die chick. I'm gonna do whatever I've gotta do.”
After the Acorda trial, Faye also participated in the Biogen trial, a Phase II
trial, also looking at a potential nerve repair medication combined with an FDA-
approved medication, Avonex. She ranked this study a two or three out of ten
and thought it was not a very dangerous study and in fact hoped that she was
getting the study drug. When prompted, it did not concern her that the study
drug was not yet approved and was experimental. She reasoned that all drugs
had to be experimental drugs at one point, and there would be no way for them
to get approved if they weren’t being studied first.
The three participants in the Actelion study, Isabelle, Christine, and Sarah,
all rated this study as low risk. Isabelle explained that she was so intent on
qualifying for this study and receiving the experimental drug that she could not
remember any specific risk concerns when she first entered the trial; however,
she understood enough about clinical trials and unknown risk to be willing to die
over her participation if there were any unpredictable side effects. She does

157
remember that BAMC did do a good job at informing her about the study phases
and her rights as a clinical trial participant, so she felt confident that she was
going to be taken care of in the trial. This was a theme that both Christine and
Sarah echoed. Christine took comfort in the study because of how meticulous
the protocol was for monitoring side effects and collecting data. For example,
her blood pressure had to be taken from a blood pressure machine that required
annual calibration (to be reported to the pharmaceutical company), on her left
arm, after the she was supine for a minimum of five minutes. Similarly, Sarah
was comforted by the detailed monitoring required during her participation. “So
they didn't just give me a pill and send me home” (Sarah Tomas).
Christine ranked the Actelion study a three out of ten explaining that it was
definitely below a five but as high as a three because the study drug was
affecting her white blood cell count. Still she described the study as very low risk
with high benefit. Although she elaborates that her risk perception has remained
the same level over her four year participation, at first that level was dominated
by fear of the unknown. Now that she’s been in it for four years, the concern is
for long-term side effects, although those do not keep her up at night. Her
biggest fear right now, more than the long-term side effects, is getting kicked off
of the study or not being let back on the study if she decided to have a baby.
Sarah ranked the Actelion study three out of ten when she initially started. She
knew that “horrible” things could happen to her because there are unknown risks,
but she still felt pretty comfortable that it wasn’t really that dangerous. Since she
158
has also been participating in this trial for over four years and nothing has
happened, she no longer thinks that anything can happen and ranked the
Actelion study a one out of ten.
For the Phase III Genzyme trial, Jaime did not consider this trial a risk at
all. Although the study drug, which was recently FDA-approved in 2014, does
have a significant side effect profile with a high percentage of patients (33%)
developing thyroid disorders, Jaime included. It was difficult to get him to
elaborate and perhaps remember since he had been on his trial for almost five
years. When prompted, he said that he didn’t consider the possibility of being
randomized to Rebif a risk, because if he wasn’t in the study, that’s what he was
going to have to take anyways. If he was randomized to Rebif, that would be
fine, but if he was randomized to the study drug (which he was), that would be
even better.
The Phase II Opera trial was an interesting case in risk perception
because the two participants, Carol and Edward, had been participating in the
trial for about three to six months when two deaths were reported and all trial
participants had to be informed and re-consented. For Edward, he ranked the
Opera trial as low risk because he felt satisfied with the way the trial was first
explained to him, both the positives and the negatives, so this alleviated any
concerns he had about potential study drug side effects. When he was informed
about the two deaths of patients who were participating in the same study, he
also felt that the situation was explained to him extremely thoroughly and

159
ultimately he decided it was not a big risk because there were mitigating factors.
Edward feels that he made a rational decision considering all of the facts
available to him at the time. He even compared the risk of death in this study,
two out of one thousand, to another study he was familiar with where the risk of
death was one in five.
Carol also saw the risk of this study as low. She did not see it as a risk to
get randomized to either Rebif or the study drug because both were thought to
treat MS and reduce MS relapse rates. Although, she admitted that she did
prefer to be randomized to the study drug. When asked if she saw an
experimental drug not yet approved by the FDA as a risk, she replied, “Do you
know how much stuff I put in my body that probably isn't approved by the FDA?”
(Carol Heuser). Carol clearly did not have any concern about the study drug in
her clinical trial. Regarding the two deaths, similar to Edward, she considered
the circumstances surrounding the deaths and made a calculation that the
number of people who died on the study out of the total was a small percentage,
so she continued to consider the drug to be low risk.
Although all interview participants ranked their clinical trial risk as low, they
also understood that participating in clinical trials was not without risk.
Submitting oneself to a clinical trial means accepting the unknown risks of the
study drug and most of the interview participants admitted that the unknown was
a real risk of research. However, this risk seemed to be outweighed by different
factors for each patient, most related to the benefit they feel that they received
160
from their trial. As discussed earlier, some actually saw the risk of the unknown
study drug as comparable to the risk of FDA-approved medications, as well as
other non-MS medications. Faye explained that she doesn’t see the risks of
research because there are risks with taking Tylenol or other over-the-counter
medications. During her study, Lydia was taking an FDA-approved medication
for toe fungus and she ended up having abnormal liver function and had to stop
taking it. Lydia sees the risk of a clinical trial in the context of the risks of life.
There’s a risk that you will get hit by a car. There’s a risk that the stove will
explode when you turn it on. There is risk in everything that we do every day.
Looking back at Table 14, it is apparent that different trials carry different
levels of risk, but attempting to draw conclusions about which of the MS trials is
the least or most risky from an objective standpoint is problematic because some
patients are more concerned about method of administration, some are
concerned about side effects, and some about the study design. What can be
said is that Phase I trials have the least amount of data on human safety and
efficacy available and Phase III trials have the most amount of data available.
Experimental drugs must progress through these phases, with FDA approval
required between each phase. If a trial does not have favorable data at any point
along this path, it is not allowed to move to the next trial phase. Despite this
regulatory requirement, patients did not seem overly concerned with the phase
their trial was in, except that they knew it was more likely to have more
information available about the drug the farther the drug was in the process.

161
Chapter 7 – Discussion
Underrepresentation Exists
Conducting a systematic review of the ClinicalTrials.gov website revealed
that there are significant reporting deficits of MS clinical trial participants by race
and ethnicity. Of the 475 completed MS trials, only 134 (28%) reported results.
Of these, even fewer, 22 trials (16.4%) reported their results by race and
ethnicity. Additionally, of those 22 clinical trials that did report participants by
race and ethnicity, significant underrepresentation of racial and minority groups
was revealed. Across the US, clinical trials favor Caucasian participation,
significantly making up 95.7% of reported trial participants, African Americans
making up 2.7%, and all other racial groups combined making up 1.7% of trial
participants. In other words, the participation rate of Caucasian MS patients is
approximately 36 times the participation rate of African American MS patients
and almost 57 times the participation of MS patients from all other racial
categories. When comparing the ethnicity categories of Latinos to Non-Latinos,
Non-Latinos dominate clinical trial participation at 97.0% versus 3.0%
participation. Although the prevalence rate reported by Noonan et al (2010) for
Caucasians, African Americans, and the remaining racial and ethnic categories is
a 2:1:1 ratio, actual clinical trial participation is far from matching this racial and
ethnic proportion.
These results disprove the assertion that is often offered by clinicians,
researchers, and patients (even some of the patients interviewed for this project),
162
to explain underrepresentation of minority groups in MS clinical trials.
Specifically, because racial and ethnic minority groups are less likely to develop
MS, they are also less likely to participate in clinical trials. While this logic is
generally accurate, the proportion of racial and ethnic group participation is vastly
different from actual prevalence rates. Racial and ethnic minorities would require
significant increases in participation rates in order to match the prevalence rates
reported by Noonan et al (2010).
BAMC does a better job at representing racial and ethnic minority groups
in its MS clinical trials, but disparities still remain. For example, approximately
38.4% of BAMC MS trial participants are non-Caucasian. Although this is also
significantly higher than the proportion of non-Caucasian patients participating in
clinical trials nationally, this rate still does not match the national prevalence rates
by race and ethnicity. Again, if comparing the racial and ethnic the prevalence
rates reported by Noonan et al (2010) for Caucasians, African Americans, and
the remaining racial and ethnic categories which is a 2:1:1 ratio, for BAMC that
ratio is approximately 13:1:7. Interestingly, this ratio seems to indicate that the
representation of all other racial and ethnic categories combined, excluding
African Americans, may approximate the MS prevalence rates observed
nationally. Unfortunately, this also means that African Americans are severely
underrepresented in BAMC MS clinical trials.
For clinical trials nationally and at BAMC, participation rates for males and
females seemed to reflect the MS gender prevalence rates observed nationally.

163
In the US, women are 2.5 times more likely than men to develop MS, while
women were 2.2 times more likely than men to participate in a clinical trial
nationally. At BAMC, women were 2.4 times more likely than men to participate
in a clinical trial. Although these rates approximate the national gender
prevalence, the small differences may indicate a slightly heavier participation of
males in clinical trials relative to the general MS population.
Despite the 1993 NIH Revitalization Act mandate to increase women and
minority participation in research and the 2007 FDA Amendments Act which
required submission of clinical trial results by race and ethnic categories, under-
reporting and underrepresentation seem to persist in MS clinical trials.
Apparently not unique to MS, since much of the literature indicates this is also
the case for cancer, cardiac, HIV/AIDS, asthma, diabetes and pain disorder
clinical trials, the question still remains whether tracking trial participation by race
and ethnicity are appropriate proxies for including and measuring the range of
biological difference. The inclusion-and-difference paradigm seems to forge
ahead without much thought to the consequences of this “black box”
categorization. On the one hand, medical researchers want to remedy any
underrepresentation of minority groups in clinical trials in order to generate
results that are more generalizable to the public. On the other hand, the way
they conceive of making trial results generalizable is by grouping individuals into
racial and ethnic categories that may not actually represent biological difference.
In fact, much of the research shows that race and ethnicity are not accurate

164
representations of biological categories and instead, are constructed by social,
cultural, and historical forces (American Anthropological Association 1998;
Jablonski 2004; Kuzawa and Sweet 2009; Race Ethnicity and Genetics Working
Group 2005).
This racial and medical profiling of potential clinical trial participants
creates more difference in its attempt at inclusion. Clinicians, medical
institutions, pharmaceutical companies, and regulatory bodies remain the
gatekeepers to clinical trial participation through their ability to pass binding
research regulations, design clinical trial protocols, allow access to medical care,
and offer invitations to potential study participants. This ability to shape the
context of clinical trial participation gives these entities significant power over
social actors who may or may not seek clinical trial participation on their own
accord. The politics of communicability requires that particular individuals
become enveloped in particular categories, for purposes prescribed by those in
power. In this case, racial and ethnic minorities become passive victims of
underrepresentation, who require assistance by gatekeepers who can grant
access to the desired clinical trials. However, access can only be granted to
“sanitary citizens” who are demonstrably compliant, proactive, and
communicative patients. In contrast, “unsanitary subjects” are those patients
incapable of adopting these characteristics and are thus deemed unfit for clinical
trial participation (Briggs 2005). A successful patient is an individual who
successfully learns how to be a “good trial patient” and is rewarded with clinical

165
trial access. Inherent in this acceptance of terms is the patient’s categorization
into the appropriate racial and ethnic category in an attempt to alleviate minority
underrepresentation and lack of generalizability of trial results.
Foucault’s (1975) conception of “docile bodies” may also help to describe
how particular clinical trial patients are shaped by the needs of the clinical
research industry. Docile bodies are those that “may be subjected, used,
transformed, and improved…and can only be achieved through strict regiment of
disciplinary acts” (Foucault 1975: 136). Importantly, clinical trial patients are not
forced or coerced into proper trial behavior, but are shaped by increments of
discipline. In fact, this discipline creates a new form of individuality for bodies
that enable them to perform their duty within the confines of those disciplinary
intuitions. Unfortunately, this arrangement is not something that an individual
can choose to enter, but this control is exerted upon an individual absolutely
through technology and power. “Docile bodies” in the research world translate to
clinical trial patients who are agreeable, punctual, responsible, communicative,
and proactive in order to maintain the rigorous requirements of a clinical trial
protocol. Those who do not fall into this category are not fit for participation and
lose their utility to the clinical research industry.
In an attempt to better recruit minority groups to clinical trials,
recruitmentology endeavors to scientifically engineer recruitment efforts for “hard
to recruit” populations. Unfortunately, this engineering does not serve to change
the power dynamic inherent in the provider-patient relationship. Ultimately, the

166
problem of minority recruitment in clinical trials is a problem to be solved and
engineered by the researcher, rather than a problem of power and positionality of
all social actors involved in shaping the context of trial participation. Further, the
use of race as a biological construct may undermine the larger goal of eliminating
health disparities which are mostly due to sociopolitical causes rather than
biological. Although the goal of inclusion is a worthy cause, the current discourse
surrounding improvement of minority participation may only serve to maintain the
paternalistic relationship between researchers and potential clinical trial
participants. This is particularly true when much of the medical literature focuses
on distrust as a reason for minority underrepresentation. As discussed
previously, distrust is a nuanced concept, and there is conflicting evidence
regarding the role distrust plays in preventing minority groups from participating
in clinical trials.
Distrust is Real but Not Absolute
It would be wrong to discount the influence of distrust on participation
rates of racial and ethnic minority groups in clinical research. Real and tragic
abuses in research have transpired (e.g., Tuskegee) and should not be ignored.
However, the medical community may not be considering the entire picture,
when focusing on minority distrust as a reason for low clinical trial participation
rates. There is significant evidence questioning the absolute contribution of
distrust to influencing clinical trial participation. For example, Wendler, et al.
(2006) found that minorities are just as willing to participate in trials but they are
167
asked to participate less often. Specific studies have looked at the influence of
Tuskegee on willingness to participate, and many have found that knowledge of
Tuskegee does not influence minority participation rates and, in fact, they were
just as willing to participate as their Caucasian counterparts (Brandon, et al.
2005; Durant, et al. 2011; Katz, et al. 2009). When specifying particular types of
distrust among the African American community, such as societal and
interpersonal distrust, it becomes less clear that distrust is a singular notion that
has absolute influence on participation rates (Durant, et al. 2011). Conflicting
evidence even suggests that minority groups are actually overrepresented in
Phase I clinical trials versus Phase III clinical trials, pointing to increased burden
of risk for those participating in Phase I trials (Fisher and Kalbaugh 2011).
As previously discussed, there are many other potential reasons for low
participation rates relating to structural barriers, such as provider bias and access
to care. The continuous recycling of distrust as a reason minority groups do not
participate in clinical research only serves to “blame” the disparity of participation
on a particular attitude of the minority group in question. Again, this is not to
discount the contribution of distrust in influencing minority participation rates, but
to question the identification by research of a singular concept that contributes to
low participation. In a sense, laying the blame on the group in question frees
researchers from this responsibility, and prevents them from having to endure
significant reflection to remedy the causes of low participation. Even the
discourse surrounding strategies for minority recruitment revolve around

168
overcoming this minority distrust by providers and researchers becoming more
trustworthy. Again, while strategies to improve relationships between
researchers and potential patients are not fruitless, the strategy may ignore the
inherent positionality of each party and how the unchanging and perpetual power
positions of social actors will continue to create this distrust, rather than eliminate
it. Importantly, Epstein (2008) suggests that building trust can be accomplished
by using a variety of methods that involve a reciprocal relationship with a
mutually beneficial exchange of knowledge and resources. The community is
treated as a true partner in research rather than research subjects that passively
accept the agenda of the researchers.
Distrust of research was not found to influence any of the electronic
survey respondents when making a decision about clinical trial participation. In
addition, no patterns were identified relating to the influence of distrust between
racial and ethnic groups. For the interview participants, only one out of 11 said
that distrust in research would influence his participation in a clinical trial.
Contrary to what the literature might predict, that one patient was Caucasian and
his reason for distrusting research had to do with distrusting pharmaceutical
companies and their profit motives. Three additional interview participants, two
Caucasian and one non-Caucasian, admitted that they also had a distrust of
pharmaceutical companies, but said it would not influence their decision to
participate in a trial. Their biggest fear was that these companies did not have

169
patients’ best interests in mind as they strategized how to minimize losses and
maximize revenue through the provision of experimental medications.
Independent of their distrust of pharmaceutical companies, only three of
the 11 interview participants, two non-Caucasian and one Caucasian, were
familiar with the notion that minority groups had more distrust of research than
Caucasians. The two non-Caucasian interview participants who had heard of
distrust also had personal experience of distrust in their families; however, one
participant suggested that it was more likely that individual differences rather
than race or ethnicity would dictate how trusting someone would be toward
research. The other participant’s grandfather had a distrust of research, while
her grandmother, mother, and she were far more amenable to trial participation
based on the concept of altruism. The Caucasian interview participant who was
familiar with minority distrust admitted that her ability to decide to participate in
her clinical trial was a privilege that few were offered, indicating a parallel cause
of underrepresentation related to structural barriers.
Although trust of individual doctors did not seem to matter for the 11
interview participants, trust in BAMC as a medical institution did. Although this
would require further examination, if these participants did not have the same
trust in a medical institution as they do in BAMC, they may have been less likely
to participate in a clinical trial, but the degree of this influence is yet unexplored.
The role of distrust in explaining low participation rates of minority groups does
seem to be present in some form, but the exact influence it has on minority

170
participation rates is uncertain. It may be that distrust is a convenient way to
blame low participation rates on minority populations rather than consider the
structural violence that exists and contributes to the participation disparities
experienced by potential trial participants as biopolitical citizens. This research
points to another factor that may help mediate participation in clinical trials: risk
perception.
Risk Perception
The most frequent reason that survey and interview participants alike said
would influence them to decline participation in a clinical trial was that the risks of
the trial were too great. Risk and risk perception is not a well explored topic in
explanations for low minority group participation in clinical trials. However, risk is
well known to epidemiologists looking to quantify risks and calculate probabilities
in search of an “objective” and knowable risk profile. Many risk calculations have
been made in an attempt to understand risk of current FDA-approved MS
medications, but oftentimes, the calculated risks by the experts, does not match
the risk perception of MS patients, nor their acceptance of risk (Clanet, et al.
2014; Heesen, et al. 2010; Hofmann, et al. 2013; Tur, et al. 2013).
Risk was a significant topic for the interview participants and it was
explored at length during the majority of interviews. Risk seemed to be the most
prominent consideration for MS trial participants, above trust or any other
influence. Risk, like distrust, is also a nuanced concept and several surprising
findings were made during the interviews with MS clinical trial patients. First was
171
the idea that the risk of being randomized to a placebo treatment arm was
considered worse than the unknown risks of the study drug. I had made the
assumption that the risk of an unknown, unapproved experimental medication
being tested in humans would be the primary consideration for MS patients. To
the contrary, fear of being off any kind of medication, whether it was FDA
approved or not, far outweighed the fear of potential study drug side effects.
Second, considerations of the current MS medication landscape was required to
understand how MS patients also believed that currently FDA-approved MS
medications were sometimes just as, if not more risky, than an experimental
medication. Third, MS clinical trial patients all considered their own clinical trial
to be low risk, despite the fact that they represented six different clinical trials
with significant variability in trial design, study drug characteristics, and risk.
The influence of risk perception was a surprising finding since most of the
literature focuses on the influence of distrust in clinical trial participation. Risk
perception also seems to play an important but separate role from risk
acceptance since a patient can perceive a high risk to be low, or can perceive a
high risk to be high, yet accept the potential consequences of the high risk
scenario. This may have been the case with Isabelle since she admits that she
was willing to die by participating in her clinical trial, just for the chance to find
something that would help improve her dire situation. In order to make that
statement, she must have thought the clinical trial risks were high enough to
potentially cause her lethal harm. So even though her risk perception of the

172
clinical trial was high, she also had a high tolerance for that level or risk because
of her particular situation. This may point to another common denominator, in
addition to risk, that may significantly influence trial participation rates. It seems
that risks would not be worth taking without perceiving or hoping for a potential,
direct benefit for the patient.
Why Participate in Clinical Trials?
When the 11 interview participants were asked what their primary reason
was for participating in their clinical trial, all of them related their primary
response to a “selfish” reason. Although advancing science and medicine and
helping fellow MS patients were noble, bonus reasons for participation, the main
reason for participation was contingent on a perceived benefit. Some patients
saw their clinical trial as offering them a superior MS medication compared to the
FDA-approved MS medications currently available, better medical care, receipt of
free medication, improvement upon future health prospects, hope, and survival.
It may be that for whatever potential benefit a clinical trial can offer a patient, it
mediates the perception of risk and/or the acceptance of risk. In addition, there
were no differences discovered in the survey or the interviews in reasons to
participate in a clinical trial by race and ethnicity. There were several significant
findings in the survey highlighting different reasons to accept and decline
participation in a clinical trial, but these were not significant by race and ethnicity.
Instead, they were significant based on education level and insurance type,

173
pointing again to structural barriers to participation in clinical trials rather than
something inherent and strictly categorized by racial and ethnic group.
The most frequent response for survey participants on why they would
participate in a clinical trial was “to advance science and medicine.” Although
this may be the case for the general MS population, it could also be that the
survey respondents were more inclined to produce responses that would be seen
more favorably by the researcher conducting the survey. This provides evidence
that trying to understand a topic as complex as clinical trial participation cannot
be completed based on survey administration alone, like many of the research
studies exploring distrust seemed to do. The semi-structured interviews allowed
for a more honest discussion about true motivations for MS patients beyond what
makes them look good. Of course, this is not to say that participating in a clinical
trial for selfish reasons is bad. But a true understanding of the motivations of MS
patients is required to fix any problems with underrepresentation of minority
groups in clinical trials. Reducing the problem to one of minority groups
categorized as distinct and absolute biological and even cultural divisions ignores
the larger and more complex forces at play influencing clinical trial participation.
It seems that the decision to participate in a clinical trial is mediated, not by
arbitrary categories of race and ethnicity, but by a complicated interaction
between distrust, risk perception and acceptance, and perceived benefits in
combination with the many structural barriers that may prevent clinical trial
participation (access to health care and clinician bias). Critical medical

174
anthropology reminds us of the “importance of political and economic forces,
including the exercise of power, in shaping health, disease, illness experience,
and health care” (Singer and Baer 1995) including the clinical trial experience, or
lack thereof, of potential clinical trial participants.
175
References Cited
Acquaviva, K. D., and M. Mintz 2010 Perspective: are we teaching racial profiling? The dangers of
subjective determinations of race and ethnicity in case presentations. Acad Med 85(4):702-5.
Adams, V., S. Miller, S. Craig, Sonam, Nyima, Droyoung, P. V. Le, and M. Varner 2007 Informed Consent in cross-cultural perspective: clinical research in
the Tibetan Autonomous Region, PRC. Cult Med Psychiatry 31(4):445-72. Alonso, A., and M. A. Hernan 2008 Temporal trends in the incidence of multiple sclerosis: a systematic
review. Neurology 71(2):129-35. American Anthropological Association 1998 American Anthropological Association Statement on "Race".
http://www.aaanet.org/stmts/racepp.htm, accessed December 17, 2014. — 2011 RACE - Are we so different? A Project of the American
Anthropological Assocation. http://www.understandingrace.org/lived/global_census.html, accessed February 22, 2015.
Anwuri, V. V., L. E. Hall, K. Mathews, B. C. Springer, J. R. Tappenden, D. M. Farria, S. Jackson, M. S. Goodman, T. J. Eberlein, and G. A. Colditz 2013 An institutional strategy to increase minority recruitment to
therapeutic trials. Cancer Causes Control 24(10):1797-809. Azevedo, Kathryn, and Christopher Payne 2006 Scrutinizing the Clinical Trials Process for Improved Patient
Protection—A New Role for Applied Anthropologists? Practicing Anthropology 28(1):35-39.
Barnett, Clifford R. 1985 Anthropological Research in Clinical Settings: Role Requirements
and Adapations. Medical Anthropology Quarterly 16(3):59-61. Bartlett, C., L. Doyal, S. Ebrahim, P. Davey, M. Bachmann, M. Egger, and P. Dieppe 2005 The causes and effects of socio-demographic exclusions from
clinical trials. Health Technol Assess 9(38):iii-iv, ix-x, 1-152.
176
Bellizzi, A., E. Anzivino, D. M. Rodio, A. T. Palamara, L. Nencioni, and V. Pietropaolo 2013 New insights on human polyomavirus JC and pathogenesis of
progressive multifocal leukoencephalopathy. Clin Dev Immunol 2013:839719.
Benamer, H. T., E. S. Ahmed, A. S. Al-Din, and D. G. Grosset 2009 Frequency and clinical patterns of multiple sclerosis in Arab
countries: a systematic review. J Neurol Sci 278(1-2):1-4. Berger, J. S., C. Melloni, T. Y. Wang, R. J. Dolor, C. G. Frazier, Z. Samad, E. D. Peterson, D. B. Mark, and L. K. Newby 2009 Reporting and representation of race/ethnicity in published
randomized trials. Am Heart J 158(5):742-7. Bernard, H. Russell 2011 Research Methods in Anthropology: Qualitative and Quantitative
Approaches. Lanham, MD: AltaMira Press. Block, Pamela, and Eva Rodriguez 2008 Team Building: An Anthropologist, An Occupational Therapist, and
the Story of a Pediatric Multiple Sclerosis Community. Practicing Anthropology 30(3):6-9.
Brandon, D. T., L. A. Isaac, and T. A. LaVeist 2005 The legacy of Tuskegee and trust in medical care: is Tuskegee
responsible for race differences in mistrust of medical care? J Natl Med Assoc 97(7):951-6.
Braunstein, J. B., N. S. Sherber, S. P. Schulman, E. L. Ding, and N. R. Powe 2008 Race, medical researcher distrust, perceived harm, and willingness
to participate in cardiovascular prevention trials. Medicine (Baltimore) 87(1):1-9.
Briggs, Charles L. 2005 Communicability, Racial Discourse, and Disease. Annual Review of
Anthropology 34(1):269-291. Briggs, Charles L., and Clara Mantini-Briggs 2003 Stories in the Time of Cholera: Racial Profiling During a Medical
Nightmare. Berkeley, CA: University of California Press.
177
Buchanan, R. J., M. A. Zuniga, G. Carrillo-Zuniga, B. J. Chakravorty, T. Tyry, R. L. Moreau, C. Huang, and T. Vollmer 2010 Comparisons of Latinos, African Americans, and Caucasians with
multiple sclerosis. Ethn Dis 20(4):451-7. Byrd, G. S., C. L. Edwards, V. A. Kelkar, R. G. Phillips, J. R. Byrd, D. S. Pim-Pong, T. D. Starks, A. L. Taylor, R. E. McKinley, Y. J. Li, and M. Pericak-Vance 2011 Recruiting intergenerational African American males for biomedical
research Studies: a major research challenge. J Natl Med Assoc 103(6):480-7.
Cabral, D. N., A. M. Napoles-Springer, R. Miike, A. McMillan, J. D. Sison, M. R. Wrensch, E. J. Perez-Stable, and J. K. Wiencke 2003 Population- and community-based recruitment of African Americans
and Latinos: the San Francisco Bay Area Lung Cancer Study. Am J Epidemiol 158(3):272-9.
Calderon, J. L., R. S. Baker, H. Fabrega, J. G. Conde, R. D. Hays, E. Fleming, and K. Norris 2006 An ethno-medical perspective on research participation: a
qualitative pilot study. MedGenMed 8(2):23. Cassell, Joan 2002 Perturbing the System: "Hard Science," "Soft Science," and Social
Science, The Anxiety and Madness of Method. Human Organization 61(2):177-185.
Center for Information and Study on Clinical Research Participation 2014 Who We Are. https://www.ciscrp.org/, accessed December 14,
2014. Chan, K. H., K. L. Tsang, P. W. Ho, C. T. Tse, J. S. Kwan, J. W. Ho, A. C. Chu, R. S. Chang, and S. L. Ho 2011 Clinical outcome of relapsing remitting multiple sclerosis among
Hong Kong Chinese. Clin Neurol Neurosurg 113(8):617-22. Clanet, M. C., J. S. Wolinsky, R. J. Ashton, H. P. Hartung, and S. C. Reingold 2014 Risk evaluation and monitoring in multiple sclerosis therapeutics.
Mult Scler 20(10):1306-11. Coakley, M., E. O. Fadiran, L. J. Parrish, R. A. Griffith, E. Weiss, and C. Carter 2012 Dialogues on diversifying clinical trials: successful strategies for
engaging women and minorities in clinical trials. J Womens Health (Larchmt) 21(7):713-6.
178
Cohen, J.W. 1988 Statistical Power Analysis for the Behavioral Sciences. Hillsdale,
NJ: Lawrence Erlbaum Associates. Colon-Otero, G., R. C. Smallridge, L. A. Solberg, Jr., T. D. Keith, T. A. Woodward, F. B. Willis, and A. N. Dunn 2008 Disparities in participation in cancer clinical trials in the United
States : a symptom of a healthcare system in crisis. Cancer 112(3):447-54.
Corbie-Smith, G., D. M. St George, S. Moody-Ayers, and D. F. Ransohoff 2003 Adequacy of reporting race/ethnicity in clinical trials in areas of
health disparities. J Clin Epidemiol 56(5):416-20. Corbie-Smith, G., S. B. Thomas, and D. M. St George 2002 Distrust, race, and research. Arch Intern Med 162(21):2458-63. Corbie-Smith, G., S. B. Thomas, M. V. Williams, and S. Moody-Ayers 1999 Attitudes and beliefs of African Americans toward participation in
medical research. J Gen Intern Med 14(9):537-46. Corbie-Smith, G., I. C. Williams, C. Blumenthal, J. Dorrance, S. E. Estroff, and G. Henderson 2007 Relationships and communication in minority participation in
research: multidimensional and multidirectional. J Natl Med Assoc 99(5):489-98.
Coyle, P. K., and K. P. Johnson 2007 Relapses matter: the costs & consequences of multiple sclerosis
relapses. J Neurol Sci 256 Suppl 1:S1-4. Cree, B., and E. Waubant 2010 Does race matter for multiple sclerosis? Neurology 74(7):532-3. Cristiano, E., L. Patrucco, and J. I. Rojas 2008 A systematic review of the epidemiology of multiple sclerosis in
South America. Eur J Neurol 15(12):1273-8. De las Nueces, D., K. Hacker, A. DiGirolamo, and L. S. Hicks 2012 A systematic review of community-based participatory research to
enhance clinical trials in racial and ethnic minority groups. Health Serv Res 47(3 Pt 2):1363-86.
179
DiGiacomo, Susan M. 1999 Can there be a cultural epidemiology? Medical Anthropology
Quarterly 13(4):436-457. Douglas, Mary 1992 Risk and Blame: Essays in Cultural Theory. London: Routledge. Durant, R. W., A. T. Legedza, E. R. Marcantonio, M. B. Freeman, and B. E. Landon 2011 Different types of distrust in clinical research among whites and
African Americans. J Natl Med Assoc 103(2):123-30. Eggly, S., E. Barton, A. Winckles, L. A. Penner, and T. L. Albrecht 2013 A disparity of words: racial differences in oncologist-patient
communication about clinical trials. Health Expect. Epstein, Steven 2007 Inclusion: The Politcs of Difference in Clinical Research. Chicago,
IL: The University of Chicago Press. — 2008 The rise of 'recruitmentology': clinical research, racial knowledge,
and the politics of inclusion and difference. Soc Stud Sci 38(5):801-32. Farmer, P. E., B. Nizeye, S. Stulac, and S. Keshavjee 2006 Structural violence and clinical medicine. PLoS Med 3(10):e449. Fisher, J. A., and C. A. Kalbaugh 2011 Challenging assumptions about minority participation in US clinical
research. Am J Public Health 101(12):2217-22. Fitzgerald, Maureen H., and Kathryn A. Paterson 1995 The hidden disability dilemma for the preservation of self. Journal of
Occupational Science 2(1):13-21. Food and Drug Administration 2010 FDA Drug Safety Communication: Risk of Progressive Multifocal
Leukoencephalopathy (PML) with the use of Tysabri (natalizumab). http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm199872.htm, accessed December 17, 2014.
— 2011 FDA Drug Safety Communication: Safety review of a reported
death after the first dose of Multiple Sclerosis drug Gilenya (fingolimod).

180
http://www.fda.gov/Drugs/DrugSafety/ucm284240.htm, accessed December 16, 2014.
— 2012 FDA Drug Safety Communication: Revised recommendations for
cardiovascular monitoring and use of multiple sclerosis drug Gilenya (fingolimod). http://www.fda.gov/Drugs/DrugSafety/ucm303192.htm, accessed December 17, 2014.
— 2014 Code of Federal Regulations Title 21.
http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?CFRPart=56, accessed January 2, 2015.
Ford, M. E., L. A. Siminoff, E. Pickelsimer, A. G. Mainous, D. W. Smith, V. A. Diaz, L. H. Soderstrom, M. S. Jefferson, and B. C. Tilley 2013 Unequal burden of disease, unequal participation in clinical trials:
solutions from African American and Latino community members. Health Soc Work 38(1):29-38.
Foucault, Michael 1975 Discipline and Punish: the Birth of the Prison. New York: Random
House. Frampton, G. K., J. Shepherd, and J. L. Dorne 2009 Demographic data in asthma clinical trials: a systematic review with
implications for generalizing trial findings and tackling health disparities. Soc Sci Med 69(8):1147-54.
Frankenberg, Ronald 1993 Risk: Anthropological and Epidemiological Narratives of Prevention.
In Knowledge, Power, and Practice: The Anthropology of Medicine and Everyday Life. S. Lindenbaum and M. Lock, eds. Berkeley, CA: University of California Press.
Goldade, Kate, and Mark A. Nichter 2010 Risk Perceptions and Knowledge of Sexually Transmitted Infections
(STIs) and HIV Among Undocumented Nicaraguan Migrant Women in Costa Rica. NAPA Bulletin 34(1):195-212.
Gravlee, C. C., and E. Sweet 2008 Race, ethnicity, and racism in medical anthropology, 1977-2002.
Med Anthropol Q 22(1):27-51.
181
Grimen, H. 2009 Power, trust, and risk: some reflections on an absent issue. Med
Anthropol Q 23(1):16-33. Gross, C. P. 2008 Racial disparities in clinical trial enrolment. Lancet 372(9651):1713-
4. Hasnain-Wynia, R., D. W. Baker, D. Nerenz, J. Feinglass, A. C. Beal, M. B. Landrum, R. Behal, and J. S. Weissman 2007 Disparities in health care are driven by where minority patients seek
care: examination of the hospital quality alliance measures. Arch Intern Med 167(12):1233-9.
Heesen, C., I. Kleiter, F. Nguyen, N. Schaffler, J. Kasper, S. Kopke, and W. Gaissmaier 2010 Risk perception in natalizumab-treated multiple sclerosis patients
and their neurologists. Mult Scler 16(12):1507-12. Hofmann, A., J. P. Stellmann, J. Kasper, F. Ufer, W. G. Elias, I. Pauly, J. Repenthin, T. Rosenkranz, T. Weber, S. Kopke, and C. Heesen 2013 Long-term treatment risks in multiple sclerosis: risk knowledge and
risk perception in a large cohort of mitoxantrone-treated patients. Mult Scler 19(7):920-5.
Holland, NJ, TJ Murray, and SC Reingold 2007 Multiple Sclerosis: A Guide for the Newly Diagnosed. New York,
NY: Demos Medical Publishing. Howerton, M. W., M. C. Gibbons, C. R. Baffi, T. L. Gary, G. Y. Lai, S. Bolen, J. Tilburt, T. P. Tanpitukpongse, R. F. Wilson, N. R. Powe, E. B. Bass, and J. G. Ford 2007 Provider roles in the recruitment of underrepresented populations to
cancer clinical trials. Cancer 109(3):465-76. Hunt, L. M., N. D. Truesdell, and M. J. Kreiner 2013 Genes, race, and culture in clinical care: racial profiling in the
management of chronic illness. Med Anthropol Q 27(2):253-71. Hussain-Gambles, M. 2004 South Asian patients' views and experiences of clinical trial
participation. Fam Pract 21(6):636-42.
182
Hussain-Gambles, M., K. Atkin, and B. Leese 2004 Why ethnic minority groups are under-represented in clinical trials:
a review of the literature. Health Soc Care Community 12(5):382-8. Irvine, H., C. Davidson, K. Hoy, and A. Lowe-Strong 2009 Psychosocial adjustment to multiple sclerosis: exploration of
identity redefinition. Disabil Rehabil 31(8):599-606. Jablonski, Nina G. 2004 The Evolution of Human Skin and Skin Color. Annual Review of
Anthropology 33:585-623. Joseph, G., and D. Dohan 2009 Diversity of participants in clinical trials in an academic medical
center: the role of the 'Good Study Patient?'. Cancer 115(3):608-15. Kalafatova, O. 1987 Geographic and climatic factors and multiple sclerosis in some
districts of Bulgaria. Neuroepidemiology 6(3):116-9. Kalb, R. 2007 The emotional and psychological impact of multiple sclerosis
relapses. J Neurol Sci 256 Suppl 1:S29-33. Kampman, M. T., T. Wilsgaard, and S. I. Mellgren 2007 Outdoor activities and diet in childhood and adolescence relate to
MS risk above the Arctic Circle. Journal of Neurology 254(4):471-477. Kanarek, N. F., H. L. Tsai, S. Metzger-Gaud, D. Damron, A. Guseynova, J. F. Klamerus, and C. M. Rudin 2010 Geographic proximity and racial disparities in cancer clinical trial
participation. J Natl Compr Canc Netw 8(12):1343-51. Kappos, L., D. Bates, G. Edan, M. Eraksoy, A. Garcia-Merino, N. Grigoriadis, H. P. Hartung, E. Havrdova, J. Hillert, R. Hohlfeld, M. Kremenchutzky, O. Lyon-Caen, A. Miller, C. Pozzilli, M. Ravnborg, T. Saida, C. Sindic, K. Vass, D. B. Clifford, S. Hauser, E. O. Major, P. W. O'Connor, H. L. Weiner, M. Clanet, R. Gold, H. H. Hirsch, E. W. Radu, P. S. Sorensen, and J. King 2011 Natalizumab treatment for multiple sclerosis: updated
recommendations for patient selection and monitoring. Lancet Neurol 10(8):745-58.
183
Katz, R. V., B. L. Green, N. R. Kressin, S. A. James, M. Q. Wang, C. Claudio, and S. L. Russell 2009 Exploring the "legacy" of the Tuskegee Syphilis Study: a follow-up
study from the Tuskegee Legacy Project. J Natl Med Assoc 101(2):179-83.
Kira, J., T. Kanai, Y. Nishimura, K. Yamasaki, S. Matsushita, Y. Kawano, K. Hasuo, S. Tobimatsu, and T. Kobayashi 1996 Western versus Asian types of multiple sclerosis:
immunogenetically and clinically distinct disorders. Ann Neurol 40(4):569-74.
Koch-Henriksen, N., and P. S. Sorensen 2011 Why does the north-south gradient of incidence of multiple sclerosis
seem to have disappeared on the northern hemisphere? J Neurol Sci 311(1-2):58-63.
Kreatsoulas, C., and S. Anand 2009 Considering race/ethnicity and socio-economic status in
randomized controlled trials. A commentary on Frampton et al.'s systematic review generalizing trial findings and tackling health disparities in asthma research. Soc Sci Med 69(8):1155-6.
Kuzawa, C. W., and E. Sweet 2009 Epigenetics and the embodiment of race: developmental origins of
US racial disparities in cardiovascular health. Am J Hum Biol 21(1):2-15. Langer-Gould, A., S. M. Brara, B. E. Beaber, and J. L. Zhang 2013 Incidence of multiple sclerosis in multiple racial and ethnic groups.
Neurology 80(19):1734-9. Launiala, A., and M. L. Honkasalo 2010 Malaria, danger, and risk perceptions among the Yao in rural
Malawi. Med Anthropol Q 24(3):399-420. Lupton, Deborah 1999 Risk. London: Routledge. Marks, Jonathan 2002 What it means to be 98% Chimpanzee: Apes, People, and Their
Genes. Berkeley, CA: University of California Press.

184
Marrie, R. A., and R. I. Horwitz 2010 Emerging effects of comorbidities on multiple sclerosis. Lancet
Neurol 9(8):820-8. Marrie, R., R. Horwitz, G. Cutter, T. Tyry, D. Campagnolo, and T. Vollmer 2008 Comorbidity, socioeconomic status and multiple sclerosis. Mult
Scler 14(8):1091-8. McCann, S. K., M. K. Campbell, and V. A. Entwistle 2010 Reasons for participating in randomised controlled trials: conditional
altruism and considerations for self. Trials 11:31. Melcon, M. O., L. Gold, A. Carra, F. Caceres, J. Correale, E. Cristiano, N. Fernandez Liguori, O. Garcea, G. Luetic, and M. Kremenchutzky 2008 Argentine Patagonia: prevalence and clinical features of multiple
sclerosis. Mult Scler 14(5):656-62. Mendoza, D. B., M. T. Williams, L. K. Chapman, and M. Powers 2012 Minority inclusion in randomized clinical trials of panic disorder. J
Anxiety Disord 26(5):574-82. Milo, R., and A. Miller 2014 Revised diagnostic criteria of multiple sclerosis. Autoimmun Rev
13(4-5):518-24. Minden, S. L., D. Frankel, L. Hadden, J. Perloffp, K. P. Srinath, and D. C. Hoaglin 2006 The Sonya Slifka Longitudinal Multiple Sclerosis Study: methods
and sample characteristics. Mult Scler 12(1):24-38. Multiple Sclerosis International Federation 2013 Atlas of MS 2013 - Mapping Multiple Sclerosis Around the World. National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research 1979 The Belmont Report: Ethical Principals and Guidelines for the
Protection of Human Subjects of Research. National Institutes of Health 2001 NIH Policy and Guidelines on the Inclusion of Women and
Minorities as Subjects in Clinical Research - Amended October 2001. http://grants.nih.gov/grants/funding/women_min/guidelines_amended_10_2001.htm.

185
— 2014a ClinicalTrials.gov: Learn About Clinical Trials.
https://clinicaltrials.gov/ct2/about-studies/learn, accessed January 2, 2015. — 2014b NIH Clinical Research Trials and You.
http://www.nih.gov/health/clinicaltrials/basics.htm, accessed January 2, 2015.
National Library of Medicine and National Insitutes of Health 2014 ClinicalTrials.gov Background. https://clinicaltrials.gov/ct2/about-
site/background, accessed December 31, 2014. National Multiple Sclerosis Society 2014 Treating MS: Medications.
http://www.nationalmssociety.org/Treating-MS/Medications, accessed December 16, 2014.
Nichter, Mark 2001 Risk, Vulnerability and Harm Reduction: Preventing STIs in
Southeast Asia by Antibiotic Prophylaxis, a Misguided Practice. In Cultural Perspectives on Reproductive Health. C.M. Obermeyer, ed. Oxford: Oxford University Press.
Noonan, C. W., S. J. Kathman, and M. C. White 2002 Prevalence estimates for MS in the United States and evidence of
an increasing trend for women. Neurology 58(1):136-8. Noonan, C. W., D. M. Williamson, J. P. Henry, R. Indian, S. G. Lynch, J. S. Neuberger, R. Schiffer, J. Trottier, L. Wagner, and R. A. Marrie 2010 The prevalence of multiple sclerosis in 3 US communities. Prev
Chronic Dis 7(1):A12. Orton, S. M., L. Wald, C. Confavreux, S. Vukusic, J. P. Krohn, S. V. Ramagopalan, B. M. Herrera, A. D. Sadovnick, and G. C. Ebers 2011 Association of UV radiation with multiple sclerosis prevalence and
sex ratio in France. Neurology 76(5):425-31. Penberthy, L., R. Brown, M. Wilson-Genderson, B. Dahman, G. Ginder, and L. A. Siminoff 2012 Barriers to therapeutic clinical trials enrollment: differences between
African-American and white cancer patients identified at the time of eligibility assessment. Clin Trials 9(6):788-97.
186
Petryna, Adriana 2002 Life Exposed: Biological Citizens after Chernobyl. Princeton, NJ:
Princeton University Press. — 2005 Ethical variability: Drug development and globalizing clinical trials.
American Ethnologist 32(2):183-197. — 2007 Experimentality: On the Global Mobility and Regulation of Human
Subjects Research. Political and Legal Anthropology Review 30(2):288-304.
Poser, C. M., and V. V. Brinar 2007 The accuracy of prevalence rates of multiple sclerosis: a critical
review. Neuroepidemiology 29(3-4):150-5. Pucci, E., G. Giuliani, A. Solari, S. Simi, S. Minozzi, C. Di Pietrantonj, and I. Galea 2011 Natalizumab for relapsing remitting multiple sclerosis. Cochrane
Database Syst Rev (10):Cd007621. Rabinow, Paul 1996 Essays on the Anthropology of Reason. Princeton, NJ: Princeton
University Press. Race Ethnicity and Genetics Working Group 2005 The use of racial, ethnic, and ancestral categories in human
genetics research. Am J Hum Genet 77(4):519-32. Rathore, S. S., and H. M. Krumholz 2003 Race, ethnic group, and clinical research. BMJ 327(7418):763-4. Ridker, P. M., N. R. Cook, I. M. Lee, D. Gordon, J. M. Gaziano, J. E. Manson, C. H. Hennekens, and J. E. Buring 2005 A randomized trial of low-dose aspirin in the primary prevention of
cardiovascular disease in women. N Engl J Med 352(13):1293-304. Risco, J., H. Maldonado, L. Luna, J. Osada, P. Ruiz, A. Juarez, and D. Vizcarra 2011 Latitudinal prevalence gradient of multiple sclerosis in Latin
America. Mult Scler 17(9):1055-9.
187
Robinson, I. 1990 Personal narratives, social careers and medical courses: analysing
life trajectories in autobiographies of people with multiple sclerosis. Soc Sci Med 30(11):1173-86.
Rook, G. A. 2012 Hygiene hypothesis and autoimmune diseases. Clin Rev Allergy
Immunol 42(1):5-15. Rosati, G. 2001 The prevalence of multiple sclerosis in the world: an update. Neurol
Sci 22(2):117-39. Ryan, R. E., M. J. Prictor, K. J. McLaughlin, and S. J. Hill 2008 Audio-visual presentation of information for informed consent for
participation in clinical trials. Cochrane Database Syst Rev (1):Cd003717. Sankar, P. 2004 Communication and miscommunication in informed consent to
research. Medical Anthropology Quarterly 18(4):429-46. Schmotzer, G. L. 2012 Barriers and facilitators to participation of minorities in clinical trials.
Ethn Dis 22(2):226-30. Schumacher, George A., Gilbert Beebe, Robert F. Kibler, Leonard T. Kurland, John F. Kurtzke, Fletcher McDowell, Benedict Nagler, William A. Sibley, Wallace W. Tourtellotte, and Thomas L. Willmon 1965 Problems of Experiemental Trials of Therapy in Multiple Sclerosis:
Report by the Panel on the Evaluation of Experimental Trials of Therapy in Multiple Sclerosis. Annals of the New York Academy of Sciences 122(1):552-568.
Schwartz, R. S. 2001 Racial profiling in medical research. N Engl J Med 344(18):1392-3. Shabas, D., and M. Heffner 2005 Multiple sclerosis management for low-income minorities. Mult
Scler 11(6):635-40. Shavers, V. L., C. F. Lynch, and L. F. Burmeister 2000 Knowledge of the Tuskegee study and its impact on the willingness
to participate in medical research studies. J Natl Med Assoc 92(12):563-72.
188
— 2002 Racial differences in factors that influence the willingness to
participate in medical research studies. Ann Epidemiol 12(4):248-56. Sheikh, A., L. Halani, R. Bhopal, G. Netuveli, M. R. Partridge, J. Car, C. Griffiths, and M. Levy 2009 Facilitating the recruitment of minority ethnic people into research:
qualitative case study of South Asians and asthma. PLoS Med 6(10):e1000148.
Simpson, S., Jr., L. Blizzard, P. Otahal, I. Van der Mei, and B. Taylor 2011 Latitude is significantly associated with the prevalence of multiple
sclerosis: a meta-analysis. J Neurol Neurosurg Psychiatry 82(10):1132-41. Singer, Merrill, and Hans Baer 1995 Critical Medical Anthropology. Amityville, NY: Baywood Publishing
Co., Inc. Sommerfeld, Johannes, Mamadou Sanon, Bocar A. Kouyate, and Rainer Sauerborn 2002 Perceptions of Risk, Vulnerability, and Disease Prevention in Rural
Burkina Faso: Implications for Community-Based Health Care and Insurance. Human Organization 61(2):139-146.
Svensson, K., O. F. Ramirez, F. Peres, M. Barnett, and L. Claudio 2012 Socioeconomic determinants associated with willingness to
participate in medical research among a diverse population. Contemp Clin Trials 33(6):1197-205.
Symonds, R. P., K. Lord, A. J. Mitchell, and D. Raghavan 2012 Recruitment of ethnic minorities into cancer clinical trials:
experience from the front lines. Br J Cancer 107(7):1017-21. Trostle, James A. 2005 Epidemiology and Culture. New York: Cambridge University Press. Tsai, Ching-Piao, Chih-Lun Yuan, Hsiang-Yu Yu, Chien Chen, Yuh-Cherng Guo, and Din-E Shan 2004 Multiple Sclerosis in Taiwan. Journal of the Chinese Medical
Association 67(10):500-505. Tur, C., M. Tintore, A. Vidal-Jordana, D. Bichuetti, P. Nieto Gonzalez, M. J. Arevalo, G. Arrambide, E. Anglada, I. Galan, J. Castillo, C. Nos, J. Rio, M. I. Martin, M. Comabella, J. Sastre-Garriga, and X. Montalban
189
2013 Risk acceptance in multiple sclerosis patients on natalizumab treatment. PLoS One 8(12):e82796.
Van der Geest, Sjaak , Susan Reynolds-Whyte, and Anita Hardon 1996 The Anthropology of Pharmaceuticals: A Biographical Approach.
Annual Review of Anthropology 25:153-178. Van der Werf, S. P., A. Evers, P. J. Jongen, and G. Bleijenberg 2003 The role of helplessness as mediator between neurological
disability, emotional instability, experienced fatigue and depression in patients with multiple sclerosis. Mult Scler 9(1):89-94.
Van Ryn, M., and J. Burke 2000 The effect of patient race and socio-economic status on physicians'
perceptions of patients. Soc Sci Med 50(6):813-28. Vollmer, Timothy 2007 The natural history of relapses in multiple sclerosis. Journal of the
Neurological Sciences 256:S5-S13. Wallin, M. T., W. F. Page, and J. F. Kurtzke 2004 Multiple sclerosis in US veterans of the Vietnam era and later
military service: race, sex, and geography. Ann Neurol 55(1):65-71. Wasay, M., I. A. Khatri, B. Khealani, and M. Sheerani 2006 MS in Asian countries. Int MS J 13(2):58-65. Wendler, D., R. Kington, J. Madans, G. Van Wye, H. Christ-Schmidt, L. A. Pratt, O. W. Brawley, C. P. Gross, and E. Emanuel 2006 Are racial and ethnic minorities less willing to participate in health
research? PLoS Med 3(2):e19. World Health Organization and Multiple Sclerosis International Federation 2008 Atlas - Multiple Sclerosis Resources in the World.


















