Understanding Options to Reduce Disparities in Cardiovascular ...
54
Understanding Options to Reduce Disparities in Cardiovascular Disease through Comparative Effectiveness Research Landscape Review Prepared for PCORI by LaShawn Glasgow, Mahima Ashok, Deborah Porterfield, Lindsay Morris, and Zhi-Jie Zheng December 2013
Transcript of Understanding Options to Reduce Disparities in Cardiovascular ...

Understanding Options to Reduce Disparities in Cardiovascular Disease through Comparative
Effectiveness Research
Landscape Review
Prepared for PCORI by LaShawn Glasgow, Mahima Ashok, Deborah Porterfield, Lindsay
Morris, and Zhi-Jie Zheng
December 2013
This report was prepared under PCORI RFQ # PCO-CVDLDSR2013 for the Addressing Disparities Program
Acknowledgments The authors would like to thank PCORI colleagues, Romana Hasnain-Wynia, Ayodola Anise, and Katie Lewis for their guidance and input throughout the landscape review process. Additionally, we acknowledge RTI Library and Information Services staff Mark Howell Elizabeth Bedini for providing literature search support.
DISCLAIMER All statements, findings, and conclusions in this publication are solely those of the authors and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute (PCORI) or its Board of Governors. This publication was developed through a contract to support PCORI’s work and is being made available free of charge for the information of the scientific community and general public as part of PCORI’s ongoing research programs. Questions or comments may be sent to PCORI at [email protected] or by mail to Suite 900, 1828 L Street, NW, Washington, DC 20036.

Overview
The Addressing Disparities Program at the Patient-Centered Outcomes Research Institute (PCORI) commissioned this landscape review to assess gaps in evidence for addressing cardiovascular disease (CVD) in populations at risk for experiencing disparities. This landscape review also identifies opportunities for PCORI to grow the evidence base for interventions designed to reduce or eliminate CVD disparities by conducting comparative effectiveness research (CER) in this area. Consistent with PCORI’s focus on CER and the Addressing Disparities Program’s focus on linking clinical care and the community, this task was limited to a review of secondary and tertiary prevention approaches implemented in a clinical setting or as a joint clinical–community-based effort. Reviewed studies must also have tested either a disparities intervention or a targeted intervention, which are defined as follows for the purposes of this review:
Disparities interventions explicitly aim to address disparities (i.e., differences between segments of the population) in CVD-related patient-centered or patient-level outcomes.
Targeted interventions explicitly aim to address CVD in a single population group that experiences disparate health outcomes.
Applying these criteria and other basic search parameters described in Appendix A, we identified 37 articles describing 36 CVD interventions (7 disparities and 29 targeted). From a social-ecological perspective, interventions targeted 3 levels: systems (n=3), patient-provider (n=2), and patient (n=31). As summarized in Appendix A, we also reviewed selected websites to identify additional interventions meeting the inclusion criteria and research gaps related to addressing CVD disparities.
Through our targeted literature and website review, we identified several opportunities for future research. In general, there is a need for more research directed to developing, testing, and assessing the comparative effectiveness of disparities interventions designed to narrow differences in health outcomes between two groups, as opposed to targeted interventions that focus on improving health outcomes for a single group. There is also an opportunity to better integrate health disparities and patient-centered outcomes research.
Beyond these broader gaps in the evidence for addressing health disparities in general, there are several research gaps specific to identifying effective strategies for reducing and eliminating CVD disparities. For example, future studies are needed to help answer the following research questions:
i

Are health system quality improvement (QI) interventions effective at reducing or eliminating CVD disparities? If so, which QI interventions are most effective?
Are interventions that deliver provider and patient education to improve quality of care and adherence to disease management guidelines effective at reducing or eliminating CVD disparities? If so, are these patient and provider level interventions more effective than those that include only a patient education component?
Do self-management support interventions effectively address CVD disparities? If so, what levels of intervention intensity and duration are necessary to achieve intended outcomes? What is the comparative effectiveness of different self-management support interventions on CVD disparities (e.g., interventions with different delivery modes)?
ii

Acronyms
Acronym Full Term AHRQ Agency for Healthcare Research and Quality CDC Centers for Disease Control and Prevention CER Comparative Effectiveness Research CFIR Consolidated Framework for Implementation Research CVD Cardiovascular Disease CVH Cardiovascular Health FOA Funding Opportunity Announcement IOM Institute of Medicine LDL Low-Density Lipoprotein LGBT Lesbian, Gay, Bisexual, and Transgender NCCAM National Center for Complementary and Alternative Medicine NHLBI National Heart, Lung and Blood Institute NIH National Institutes of Health QI Quality Improvement SEM Social-Ecological Model SES Socioeconomic Status
iii

Contents Overview .......................................................................................................................... i Acronyms ........................................................................................................................ iii Introduction ..................................................................................................................... 1
Burden on Society ........................................................................................................... 3
Options for Addressing the Issue .................................................................................... 5
Description of interventions ......................................................................................... 5
Relative Benefits ........................................................................................................ 11
Relative Harms .......................................................................................................... 12
Opportunities for New Research ................................................................................ 12
Recent Innovations .................................................................................................... 15
Pace of Research ...................................................................................................... 16
Potential for New Information to Rapidly Improve Care and Patient-Centered Outcomes ...................................................................................................................... 17
Summary of the Factors that Would Affect the Translation of New Research Findings to Practice ................................................................................................... 17
Discussion of Likelihood of New Research Findings Being Immediately Implemented in Practice ............................................................................................ 18
Durability of Information ................................................................................................ 21
Conclusion .................................................................................................................... 22
References .................................................................................................................... 23
Appendix A: Methods Highlights ..................................................................................... 1
Appendix B: At-a-Glance Summary of Interventions ....................................................... 1
Appendix C: Glossary ...................................................................................................... 1
iv

Introduction Cardiovascular disease (CVD) is a leading cause of death and disability in the U.S. (CDC 2011), and CVD-related health disparities are well documented. However, evidence for approaches to effectively address CVD disparities is limited. In their national action plan, the National Prevention Council highlighted the need to develop, monitor, and evaluate community-based interventions to reduce health disparities (National Prevention Council 2012). A systematic review of health care systems interventions concluded that “virtually no literature specifically addressed disparity reduction” (Davis et al. 2008,1). Notably, since 2007 the National Institutes of Health (NIH) has issued consecutive funding opportunities for research to understand the causes of health disparities (in a number of areas, including CVD) and to test interventions to reduce or eliminate disparities (NIH 2007).
Addressing health disparities is one of PCORI’s five national research priorities (PCORI 2012). PCORI’s Addressing Disparities Program aims to identify “potential differences in prevention, diagnosis or treatment effectiveness, or preferred clinical outcomes across patient populations and the health care required to achieve best outcomes in each population” (PCORI 2012, 8). In April 2013, the Advisory Panel on Addressing Disparities selected hypertension and cardiovascular disease as priority areas for future research (PCORI 2013). Developed to support the work of the Addressing Disparities Program and the Advisory Panel, this landscape review describes current evidence for CVD disparities interventions, illuminates the evidence gaps, and identifies opportunities for PCORI-funded comparative effectiveness research (CER).
Although this landscape review examines evidence for interventions that target a very inclusive list of potentially disparate populations, it is restricted to a subset of intervention types and settings consistent with PCORI’s central focus on CER. This landscape review summarizes evidence, and gaps in evidence, for a subset of interventions as follows:
We focused the review on CVD secondary prevention (e.g., screening and diagnosis) and tertiary prevention (e.g., tobacco use cessation or hypertension control in persons with diagnosed CVD).
We focused the review on interventions that took place in a clinical setting; those that were based in a clinical setting but extended into a community setting (e.g., a senior center, the patient’s home); and those that involved organizational linkages or partnerships between clinical and community organizations.
We excluded studies that focused on home blood pressure monitoring as this was the subject of a recent AHRQ review (Uhlig et al., 2012).
Reduce Disparities in Cardiovascular Disease 1
Finally, this review was limited to disparities and targeted interventions, which are defined as follows for the purposes of this review:
Disparities interventions explicitly aim to address disparities (i.e., differences between segments of the population) in CVD-related patient-centered or patient-level outcomes.
Targeted interventions explicitly aim to address CVD in a single population group experiencing disparate health outcomes.
Further details on landscape review methods are provided in Appendix A.
Within this scope, this document provides an overview of types of interventions addressing CVD disparities and reported patient-centered and patient-level outcomes. The interventions identified through this landscape review can be characterized, from the social-ecological model (SEM) perspective, by intervention level. We adopted this approach to typifying interventions because addressing health disparities in CVD and other conditions requires comprehensive, interdisciplinary approaches that operate at multiple levels of the SEM (Mensah 2005; CDC n.d.; NIH 2012). Studies meeting the criteria for this landscape review tested interventions at the systems level, patient-provider level, and patient level. This landscape review highlights evidence gaps for these disparities interventions. Furthermore, this review proposes the potential role of PCORI in further developing the evidence base through CER and supporting research translation in order to both improve health outcomes for populations experiencing CVD disparities and reduce and eliminate CVD disparities.
Reduce Disparities in Cardiovascular Disease 2

Burden on Society The term CVD, also called heart disease, refers to pathological conditions involving the heart and blood vessels, such as coronary heart disease, hypertension, and stroke. CVD is a leading cause of death and disability in the U.S. (CDC 2011), and high rates of hypertension, high cholesterol, and smoking—preventable CVD risk factors—contribute to the CVD burden. Approximately one in three U.S. adults have one or more types of CVD (Go et al. 2013). Exhibit 1 lists prevalence estimates by population group and CVD condition. Each year, approximately 610,000 U.S. adults will have a new coronary attack, which is defined by Go et al. (2013) as first hospitalized myocardial infarction or coronary heart disease death.
Exhibit 1. Age-adjusted Prevalence Estimates for Diagnosed CVD Conditions
Population group (adults ≥ 18 years of
age) Heart Disease Coronary Heart
Disease Hypertension Stroke
African Americans 10.7% 6.9% 33.4% 4.5%
American Indians or Alaska Natives 12.7% 7.2% 25.8% 4.6%
Asians 7.4% 4.3% 18.7% 2.7%
Hispanics or Latinos 8.6% 5.9% 22.2% 2.8%
Native Hawaiians or other Pacific Islanders … … 21.8% …
Whites 11.1% 6.3% 23.3% 2.3% Source: Go et al. 2013 Note: Data are not available for empty cells.
CVD poses a significant burden on public health, the health care system, and the economy. By 2030, total direct medical costs of CVD are expected to top $800 billion (Heidenreich et al. 2011). Heart disease, stroke, and hypertension are among the top 15 conditions that cause functional disabilities among Americans, which include challenges with daily living, inability to do housework, and inability to work at a job or business (Go et al., 2013). Stroke is a leading cause of long-term disability among U.S. adults, and post-stroke depression is experienced by nearly one-third of stroke survivors (Go et al., 2013).
During the period from 1999-2009, the rate of death attributable to CVD declined by approximately 33%. However, despite advances in addressing this leading cause of death in the U.S., CVD-related disparities persist among populations defined by race/ethnicity; socioeconomic status (SES), including income and education; health insurance status; geographic location; disability status; gender; and sexual orientation.
Reduce Disparities in Cardiovascular Disease 3

Heart disease and stroke incidence and mortality rates continue to be higher among African Americans and Hispanics, adults with low SES, and those living in the southeastern part of the country (Go et al. 2013)
The prevalence rate of hypertension in African American adults is the highest in the world (Go et al. 2013).
During the period from 1995 to 2002, Puerto Rican Americans had a higher hypertension-related mortality rate than non-Hispanic whites and all other Hispanic subgroups (Go et al., 2013).
In all years of National Health and Nutrition Examination Survey administration starting in 1988 (1988–1994, 1999–2002, 2003–2006, 2007–2010), Mexican Americans were less likely than whites to have their blood pressure under control (AHRQ 2012a).
In 2007, African American men were 30% more likely to die from heart disease compared to non- Hispanic white men (CDC 2013).
CVD has been the leading cause of death among U.S. women since 1984, resulting in more CVD-related deaths compared to men (Beth Israel Deaconess Medical Center 2003).
During most of the period 2001–2009, residents of the lowest area income quartile had significantly higher inpatient heart attack mortality rates than residents of the highest area income quartile (AHRQ 2012a). Women had higher rates of inpatient heart attack deaths compared to men, and uninsured patients’ rates of inpatient heart attack deaths were higher than privately insured patients.
Adults living in rural environments in the U.S. are more likely to be diagnosed with coronary heart disease compared to adults living in urban areas (O’Connor & Wellenius 2012).
With regard to lesbian, gay, bisexual, and transgender (LGBT) health, it is important to note that research on CVD in this population has focused primarily on increased risk among LGBT persons infected with HIV and among transgender persons taking masculinizing hormones (Institute of Medicine [IOM] 2011). However, IOM concluded that there was insufficient research supporting these risks. IOM recommends additional research on CVD among all LGBT adults. Reducing and eliminating health disparities is a critical component of addressing the CVD burden. However, more evidence is needed to determine the best approaches for intervening on CVD disparities. As a key step in growing the evidence base in this area, and, in turn, informing health care decisions related to addressing CVD disparities or improving CVD outcomes among population groups that experience disparate outcomes, this landscape review will illuminate evidence gaps and identify opportunities for PCORI-funded CER.
Reduce Disparities in Cardiovascular Disease 4

Options for Addressing the Issue
Description of interventions
As noted in the Introduction, disparities and targeted interventions were included in this landscape review, and interventions identified through this landscape review targeted one of three SEM levels: systems, patient-provider, or patient. In this section, which is organized by intervention level, we provide brief descriptions of the studies, including intervention aim (i.e., disparities or targeted), followed by a high-level summary of reported results. Appendix B provides an at-a-glance summary of the interventions included in this landscape review.
Systems-level interventions: study descriptions. Three pre-post studies tested health care quality improvement (QI) interventions: (1) a statewide ST-segment-elevation myocardial infarction (STEMI) regionalization program designed to reduce treatment times among women, minorities, and the elderly (Glickman et al. 2010); (2) a registry and performance-improvement program intended to improve quality of care and outcomes for African Americans hospitalized with heart failure (Yancy et al. 2008); and (3) a heart failure disease management program, which provided a standardized algorithm of care to eliminate disparities in hypertension care for African American and Hispanic patients in an urban and a rural safety net hospital (Hebert et al. 2011). All three interventions were disparities interventions (i.e., explicitly aimed to address differences between segments of the population on CVD outcomes) and were implemented in the clinical setting. It is important to note that Herbert et al. (2011) did not provide a detailed description of the disease management intervention, but statements included in the paper imply that the primary components of the intervention involved systems-level changes to “ensure that the best practices known to medical science are incorporated with minimal variation over the entire continuum of care”(Hebert et al. 2011, 567).
Systems-level interventions: study results. Glickman et al. (2010) reported a significant decrease in baseline care differences of door-to-treatment times in women versus men. However, with the exception of this indicator, the intervention did not improve disparities in STEMI treatment times. Yancy et al. (2008) concluded that African American heart failure patients exposed to the performance-improvement program had better-than-previously observed treatment with evidence-based therapies. Additionally, African American heart failure patients had similar or better outcomes compared with non–African American patients. However, the researchers acknowledge that further research is needed to assess the effect of a performance-improvement intervention on health care disparities among African Americans with CVD. Herbert et al. (2011) reported significant reductions in mean systolic and diastolic blood pressure, but also reported a “persistent” health disparity for blood pressure control: whites were
Reduce Disparities in Cardiovascular Disease 5

more likely to reach blood pressure control goals than African Americans or Hispanics (2011, 571).Study objectives did not include assessment of rural versus urban safety net disparities.
Patient-provider level interventions: study descriptions. Two randomized trials tested interventions that included patient and provider education: (1) a study to compare the effectiveness of physician communication skills training and patient coaching on hypertension among underserved primary care patients (Cooper et al. 2011); and (2) a study to compare the effectiveness of physician education, patient education, and both on improving blood pressure control in African American patients (Johnson et al. 2011). Both interventions were targeted interventions (i.e., explicitly aimed to address CVD in a single population group experiencing disparate health outcomes) and both were implemented in the clinical setting but included some community linkage. For example, community health workers provided patient coaching in Cooper et al.’s trial, and American Society of Hypertension certified hypertension specialists provided lectures to physicians in Johnson et al.’s trial.
Patient-provider level interventions: study results. In Johnson et al.’s study, the patient and physician education group achieved a significantly better decrease in systolic blood pressure compared with the usual care group. Cooper et al. (2011) found no improvements in patient adherence to medication; however, they reported suggestive (i.e., not statistically significant but potentially practically important) improvements in systolic blood pressure among patients with uncontrolled hypertension in the patient and physician education intervention group.
Patient-level interventions. The remaining 32 papers reported on 31 patient-level interventions designed to support patients in managing their blood pressure and CVD. These interventions varied widely by content or types of services provided, mode of service delivery, and service provider; descriptions are grouped by similar intervention approach.
Integrative medicine interventions: study descriptions. Two randomized trials tested integrative medicine interventions; that is, they incorporated non-mainstream health care approaches (National Center for Complementary and Alternative Medicine [NCCAM] 2013): (1) a study to determine the comparative effectiveness of patient education versus patient education with positive-affect induction and self-affirmation among hypertensive African American patients from two primary care practices (Ogedegbe et al. 2012); and (2) a study of a secondary CVD prevention intervention for African Americans that involved transcendental meditation versus health education (Schneider et al. 2012). Both interventions were targeted interventions and included support or services provided beyond the clinical setting. For example, in Ogedegbe et al.’s study, research assistants provided regular telephone-based support, which
Reduce Disparities in Cardiovascular Disease 6
allowed patients to receive services outside of the clinical setting. The transcendental meditation technique was taught by an external instructor certified by Maharishi Foundation USA.
Integrative medicine interventions: study results. Ogedegbe et al. (2012) reported that the integrative medicine intervention had a significant impact on medication adherence, but not on blood pressure reduction. Schneider et al. (2012) reported a significant reduction in systolic blood pressure as well as significant reductions in anger expression and a 48% risk reduction in the composite of all-cause mortality, myocardial infarction, or stroke.
Enhanced lifestyle interventions: study descriptions. We classified four patient-level interventions as “enhanced lifestyle” interventions because they provided in-person self-management support paired with supervised exercise sessions and/or interactive sessions related to healthy eating/cooking. These pre-post studies were designed to (1) examine the relative effectiveness of a multisite cardiac lifestyle intervention program (MCLIP) for male and female coronary heart disease (CHD) patients of lower SES compared to patients with higher SES (Govil et al. 2009) (MCLIP included in-person education, nurse case management, and supervised exercise); (2) assess the effectiveness of a 12-week community-based education and physical activity intervention on blood pressure control among African American adults (Rigsby 2011); (3) assess the feasibility of a culturally tailored behavioral intervention to lower blood pressure in Latino adults (Rocha-Goldberg Mdel et al. 2010); and (4) evaluate a community-based, culturally tailored nutrition and physical activity program designed to improve the CVH of African American women (Rodriguez et al. 2012). One of the four interventions was a disparities intervention (Govil et al. 2009); the remaining three were targeted interventions,
Enhanced lifestyle interventions: study results. Govil et al. (2009) found improvements in patient-reported well-being across all SES levels. Patient-reported improvements in diet, stress management, and physical activity were also documented, and exercise capacity improved to more than 10 metabolic equivalents, across all educational and income levels. Rocha-Goldberg Mdel et al. (2010) reported clinically significant decreases in systolic blood pressure among participants. Rigsby found improvements in participants’ knowledge and blood pressure control, but significance of results was not reported. Rodriguez et al. (2012) reported a significant reduction systolic blood pressure from baseline to the end of the intervention period.
Traditional self-management interventions: study descriptions and results. Studies of 14 patient-level interventions (9 randomized trials, 1 nonrandomized trial, 2 pre-post studies, 1 observational study, and 1 study involving post-hoc analysis of data from a randomized trial) involved the provision of in-person education and/or counseling,
Reduce Disparities in Cardiovascular Disease 7

services by phone, or through a mix of both methods by clinical staff (e.g., nurses), non-clinical health workers (e.g., promotoras, community health workers, and health educators), or research staff. All of these self-management interventions were clinical-community linkage interventions in that they extended the services provided by a clinical setting and/or were implemented through considerable partnering with community-based health workers and organizations.
Two of the self-management interventions were disparities interventions. (Jackson et al. 2012, Noureldin et al. 2012). Jackson et al. (2012) conducted a randomized trial to compare the effect of a telephone-based, nurse-delivered medication management and behavioral self-management support intervention on change in blood pressure among African American and non-Hispanic white U.S. Department of Veterans Affairs primary care patients. This intervention included services that extended beyond the clinical setting, including home blood pressure monitoring and telephone-based self-management support. Jackson et al. (2012) reported significant improvement in mean systolic blood pressure at 12 and 18 months among African American patients receiving the combined medication management and behavioral self-management support intervention compared to African American patients receiving usual care. No comparable changes in blood pressure were found for non-Hispanic white patients. In post-hoc analysis of data from a randomized trial, Noureldin et al. (2012) compared the effect of a pharmacist intervention, including patient education, therapeutic monitoring, and communication with primary care providers, on medication adherence among heart failure patients with limited versus adequate health literacy. Researchers reported that, in general, the intervention improved medication adherence, and in patients with limited health literacy, adherence was increased to levels similar to baseline adherence among patients with adequate health literacy.
The remaining 12 traditional self-management interventions were targeted interventions (Anderson et al. 2010, Balcazar et al. 2009, Cene et al. 2008, Cook et al. 2010, DeWalt et al. 2012, Evans-Hudnall et al. 2012, Han et al. 2010, Gross et al. 2013, Kim et al. 2011, Mosca et al. 2010, Pezzin et al. 2011, Shaya et al. 2013, Zarate-Abbott et al. 2008). The evidence is mixed as to the effectiveness of traditional self-management interventions for addressing CVD in subgroups experiencing disparities.
Anderson et al. (2010) found no significant benefit on key clinical and behavioral outcomes for a randomized trial of a telephone-based disease management intervention designed to improve CVD outcomes for community health center patients with diabetes. In a randomized trial to test an in-person and phone-based intervention delivered by promotoras to improve hypertension control among Mexican Americans, Balcazar et al. (2009) reported significant differences in diet-related heart-healthy behaviors between the intervention and control groups. Cene et al. (2008) reported no group differences in
Reduce Disparities in Cardiovascular Disease 8

mean risk factor levels at 5 years for their randomized trial to compare the effectiveness of community-based care provided by a nurse practitioner/community health worker team versus enhanced usual care on CVD risk among high-risk African American families. Based on results of their randomized trial to compare the effectiveness of a single session literacy sensitive training to improve self-care among patients with heart failure versus the single session plus ongoing telephone-based support provided by a health educator, DeWalt et al. (2012) concluded that patients with low health literacy may benefit more from interventions that involve multiple sessions compared to those with higher health literacy. However, DeWalt et al. found no differences between intervention groups on clinical outcomes, including all cause hospitalization and all cause death. Evans-Hudnall et al. (2012) reported significant increases in stroke knowledge and decreased secondary stroke risk factors among underserved racial/ethnic minorities for their randomized clinical trial of a secondary stroke self-care pilot program. Mosca et al. (2010) conducted a randomized trial of an education and counseling intervention provided by a prevention facilitator/educator during hospitalization and by phone following discharge to improve adherence to secondary CHD prevention guidelines among women. The researchers reported no difference between the intervention and usual care groups on a summary score of prevention goals met, but found that minority women in the intervention group were about twice as likely to reach blood pressure goals at 6 months compared to minority women receiving usual care. In a randomized clinical trial of the effect of a nurse and health educator counseling intervention on blood pressure control among high-risk African American home care adults, Pezzin et al. (2011) found significant improvements in blood pressure control. Kim et al. (2011) and Han et al. (2010), whose publications are based on a randomized trial of the same intervention, compared the effectiveness of more-intensive versus less-intensive nurse-provided telephone counseling on hypertension management among Korean American patients with high blood pressure. Improvements in medication adherence and blood pressure were found in both intervention groups with no significant group differences.
Results from Cook et al.’s (2010) observational study of a nurse-delivered educational intervention designed to address health care disparities among Native Hawaiians include improvements in adverse events following percutaneous coronary interventions for Native Hawaiian patients and a decrease in readmissions that occur within 30 days among patients admitted with myocardial infarction and heart failure. Study limitations notwithstanding, Gross et al. (2013) reported that the 10 African American community clinic patients who participated in a culturally sensitive education program to support lifestyle changes and medication adherence demonstrated diet, exercise, and medication adherence improvements. Shaya et al. (2013) conducted a non-randomized trial to assess the effectiveness of nurse-led group education sessions on hypertension
Reduce Disparities in Cardiovascular Disease 9

control among African American adults in urban communities. Researchers reported a significant decrease in blood pressure among the intervention group at 18-month follow-up. Zarate-Abbott et al. (2008) conducted a pre-post study to determine the effects of a nurse-led workplace education program for low-income, immigrant Hispanic women on blood pressure control and heart-healthy behaviors. Study findings showed a significant reduction in blood pressure over the 17-month intervention.
Alternative modes of service delivery: study descriptions and results. Nine of the 31 patient-level interventions (5 randomized trials, 3 nonrandomized trial, and 1 pre-post study) used alternative modes of service delivery, including self-management provided by DVD (Eckman et al. 2012, Houston et al. 2011), text message (Nundy et al. 2013), telehealth kiosk (Resnick et al. 2012), website/computer (Bove et al. 2011, Martin et al. 2011, Migneault et al. 2012), illustrated medication schedules (Kripalani, Schmotzer, and Jacobson 2012), and a mix of visual, written, aural and kinesthetic strategies based on patients learning styles (Giuse et al. 2012). All of these interventions were targeted interventions.
Eckman et al. (2012) conducted a randomized trial to compare the effectiveness of a VHS/DVD plus printed booklet educational intervention versus only the printed booklet on coronary artery disease knowledge among patients with low health literacy. The researchers concluded that results trended towards increased improvement on knowledge scores among patients in the VHS/DVD plus printed booklet group, but found no significant differences in knowledge score improvements or clinical outcomes between patients with low health literacy and those with higher health literacy. Houston et al.’s (2011) randomized trial to test the impact of an interactive storytelling intervention, delivered via DVD, on blood pressure improvement among African American adults found significant improvements in blood pressure among patients with baseline uncontrolled hypertension in the intervention group. Nundy et al. (2013) conducted a pre-post study to assess the feasibility of a text message-based intervention on heart failure self-management among African American adults following hospital discharge. Researchers reported clinically significant improvements in self-care maintenance and management. Resnick et al.’s (2012) pilot study, a non-randomized trial on the effect of nurse-monitored telehealth kiosks placed in community-based senior centers on blood pressure, reported lower blood pressure levels and improved blood pressure control among the telemonitoring group. However, the pilot was not powered or designed for hypothesis testing, so no inferential statistics were provided.
With regard to website/computer interventions, no intervention effects were observed in a randomized trial to test the effectiveness of a culturally tailored, automated telephone system on adherence to medication and other self-management guidelines among hypertensive African American adults (Migneault et al. 2012). Similarly, Martin et al.’s
Reduce Disparities in Cardiovascular Disease 10

(2011) randomized trial of a multimedia computer-based program designed to improve medication adherence among low-income hypertensive African American adults found no intervention-control group differences. Bove et al. (2011) observed significant CVD risk reduction among medically underserved urban and rural patients in both the telemedicine and comparison office-based nurse management and education interventions, which were tested in a randomized trial.
Kripalani et al.’s (2012) randomized trial to evaluate the effect of illustrated medication schedule and refill reminder postcards on medication adherence among patients with low health literacy reported no significant improvements in medication adherence. However, results of post-hoc analyses suggest that illustrated medication schedules may improve medication adherence among patients with low medication self-efficacy, those with polypharmacy, or those with non-adherence at baseline. Guise et al. (2012) conducted a randomized trial to compare the effectiveness of educational materials tailored to health literacy level versus those tailored to health literacy level and learning style (e.g., education provided via audio recording for aural learners) on hypertension knowledge among emergency department patients with high blood pressure. Participants in both intervention groups demonstrated improvements in post-test scores for hypertension knowledge with increased improvements among those receiving materials tailored to health literacy level and learning style.
Unique providers: study descriptions and results. Two patient-level interventions, both tested in randomized trials, involved non-traditional providers of self-management support services. Turner et al. (2012) evaluated the effectiveness of phone-based counseling provided by peer patients with well-controlled hypertension paired with office-based counseling provided by trained practice staff on CHD risk among African American patients with uncontrolled hypertension. Researchers concluded that risk reduction favored the intervention group; however, results were not statistically significant. Victor et al. (2011) conducted a randomized cluster trial to determine whether a blood pressure monitoring and referral program administered by barbers in community barber shops led to improved blood pressure control among patrons with high blood pressure. Results indicate that the hypertension control rate increased more in intervention barbershops than in comparison barbershops.
Relative Benefits
As detailed in the previous section, this landscape review found that studies of interventions that explicitly addressed disparities in CVD health outcomes and those that addressed CVD in populations experiencing disparate health outcomes reported statistically significant and suggestive improvements in patient-level and patient-centered outcomes (see Appendix C for definitions adopted for the purposes of this
Reduce Disparities in Cardiovascular Disease 11

landscape review). Patient-level outcomes commonly reported across all reviewed studies include improvements in
patient knowledge, attitudes, and behaviors related to CVD management;
physiological measures (e.g., blood pressure); and
medication adherence.
Quality of care improvements were also reported in two systems-level intervention studies (Glickman et al. 2010; Yancy et al. 2008) and in one patient and provider-level intervention (Cooper et al. 2011).
Patient-centered outcomes were less commonly reported than patient-level outcomes. Two studies reported health-related quality of life benefits, including improvements in depression scores, following patient-level self-management support interventions (Govil et al. 2009; Kim et al. 2011). Reduction in risk for CVD (Bove et al. 2011), inpatient mortality (Yancy et al. 2008) and composite morbidity and mortality (Schneider et al. 2012) were also reported. Based on results from an observational study, Cook et al. (2010) reported improvements in 30-day hospital readmissions for myocardial infarction and heart failure patients.
Relative Harms
None of the papers reviewed included information about the relative harms of the interventions. However, the recent NIH funding opportunity announcement (FOA) identified through the web scan, Behavioral and Social Science Research on Understanding and Reducing Health Disparities, notes that interventions focused on improving the absolute level of a single group’s health may not improve the group’s relative health and instead could result in maintaining or exacerbating disparities (NIH 2013a).
Opportunities for New Research
In general, PCORI can advance health disparities research by increasing the inclusion and reporting of patient-centered outcomes and by funding intervention studies that focus on reducing disparities (i.e., differences in health outcomes between two groups), in addition to studies of targeted interventions:
Enhance the inclusion and reporting of patient-centered outcomes. About one-quarter of the papers included in full-text review covered chief patient-centered outcomes. A recent AHRQ funding opportunity identified through the web scan, Closing the Gap in Healthcare Disparities through the Dissemination and Implementation of Patient Centered Outcomes Research, reflects the importance of integrating health disparities and patient-centered outcomes research (NIH 2013b). However, the cooperative agreement focuses on health
Reduce Disparities in Cardiovascular Disease 12

care disparities in racial and ethnic minority populations in under-resourced health care settings. PCORI research could complement AHRQ research by broadening an integrated approach to health disparities and patient-centered outcomes research to other groups experiencing disparities (i.e., beyond racial and ethnic populations) and by focusing on CVD disparities.
Focus on measurement of disparities between or among two or more groups. In general, there is a need for more research aimed at developing interventions, and assessing the comparative effective of interventions, designed to reduce or eliminate disparities in CVD health outcomes, as opposed to research that aims to improve CVD-related outcomes in a single population experiencing disparities. This research gap is reflected in the small number of disparities studies found through this landscape review (Glickman et al. 2010; Govil et al. 2009; Eckman et al. 2012; Hebert et al. 2011; Jackson et al. 2012; Yancy et al. 2008; Noureldin et al. 2012). And the recently released NIH Funding Opportunity Announcement (FOA) for research on understanding and reducing disparities, which stresses that “applied research under the FOA should be aimed at narrowing the differential between groups,” underscores the importance of addressing this research gap (NIH 2013a, 4).
There is an opportunity for PCORI to complement NIH disparities research by funding studies that compare the effectiveness of various disparities interventions developed and tested under the NIH R01. A patient-level self-management support intervention determined to be effective at reducing disparities versus usual care can be further examined in comparative effectiveness studies to determine, for example, which intervention components are critical for achieving intended outcomes. It is worth noting that the NIH FOA is “restricted health disparities among populations defined by race/ethnicity, SES, and/or rural-urban residence” NIH 2013a, 3), and the National, Heart, Lung and Blood Institute “will only support research project (R01) that test interventions, not observational studies, [rather]…projects…employing randomized designs” (NIH 2013a,11). Therefore PCORI can also complement NIH research by funding studies that compare the effectiveness of interventions designed to reduce health disparities between groups not covered under the R01 and/or studies that employ non-randomized, yet rigorous designs (e.g., regression discontinuity).
In addition to these broader gaps in evidence for addressing health disparities, there are several gaps in research specific to CVD disparities. To help address these evidence gaps, this landscape review suggests three types of studies that PCORI could fund: those that assess the effectiveness of QI interventions; those that explore the added value of provider education; and those that compare the effectiveness of various self-management support intervention models, including within model studies that compare effectiveness at different levels of intervention intensity and duration.
Studies that assess the effectiveness of QI interventions. PCORI can help address gaps in CVD disparities research by funding studies that compare the
Reduce Disparities in Cardiovascular Disease 13

effectiveness of QI interventions on reducing disparities and improving patient-centered outcomes. In following with AHRQ’s definition (AHRQ 2012b), QI interventions would include any multidisciplinary, systems-focused, data-driven methods applied to improve the efficiency, effectiveness, and reliability of health processes and outcomes of care. As described in the previous section, we found only three studies of QI interventions designed to address disparities between two or more groups (Glickman et al. 2010; Yancy et al. 2008; Hebert et al. 2011). As a recent AHRQ report identified through the web scan notes, although QI interventions have proven effective for improving health and health care, it is unclear whether they are effective at reducing disparities (AHRQ 2012b). The Community Preventive Services Task Force recommendations for CVD prevention and control align with the AHRQ findings. The Task Force recommends clinical decision-support systems (CDSS) for prevention of CVD and team-based care to improve blood pressure control (Community Preventive Services Task Force 2013). However, evidence gap summaries highlight the need for more evidence around the impact of CDSS on reducing health disparities and more assessment of the effectiveness of team-based care for groups experiencing health disparities, including patients from low-SES groups and racial and ethnic minorities other than African Americans. The Task Force also concludes that more information is needed about the patient-centered outcomes of these QI interventions.
Studies that explore the added value of provider education. PCORI can expand the evidence for CVD disparities interventions by funding studies that compare the relative impact of (a) provider education, (b) patient education, and (c) provider and patient education on patient-centered and patient-level CVD outcomes, including quality of care. As summarized in the previous section, this landscape review identified only two studies that compared the relative effectiveness of provider education, patient education, and provider and patient education interventions to address disparities in hypertension control (Cooper et al. 2011; Johnson et al. 2011). One of the studies found that the dual provider and patient education intervention yielded significantly better reduction in blood pressure compared to the usual care group (Johnson et al. 2011). Both studies suggest that more research is needed to identify the intervention components and levels of intensity required to improve patient outcomes. Research to identify the subgroups of clinicians and patients who are most likely to benefit from education interventions was also recommended (Johnson et al. 2011).
Studies that compare the effectiveness of various self-management support intervention models. PCORI can help develop the evidence base for CVD disparities interventions by funding studies that compare the effectiveness of various self-management support models, including studies designed to identify which intervention components are critical for achieving intended outcomes. As described in the previous section, most (31 of 37) of the studies reviewed tested patient-level interventions designed to support patients in managing their blood pressure and CVD. Interventions varied widely by the provider of services, types of services provided, service delivery mode, and
Reduce Disparities in Cardiovascular Disease 14

setting. The diversity of self-management support interventions offers many options for CER within and between intervention models. Indeed, most papers included a recommendation to compare the intervention’s effectiveness at different levels of intensity and duration. Researchers suggested that this within-intervention CER is necessary to identify essential elements of the intervention, which could, in turn, facilitate translation of research findings into real world practice.
Two patient-level interventions were integrative medicine interventions (Ogedegbe et al. 2012; Schneider et al. 2012). Under the NIH FOA, the National Center for Complementary and Alternative Medicine identifies “comparative effectiveness studies of combined pharmacological/non-pharmacological integrative health interventions” as an example research area (NIH 2013a,9). However, CVD is not listed as a specific area of focus, and this is a research gap that PCORI can address.
We classified three patient-level interventions as enhanced lifestyle interventions because they provide in-person self-management support paired with supervised exercise sessions and/or interactive sessions related to healthy eating/cooking (Govil et al. 2009; Rigsby 2011; Rodriguez et al. 2012). Future research should compare the effectiveness of enhanced lifestyle interventions to more basic patient education and counseling services on patient-centered and patient-level outcomes and assess whether effectiveness varies across different groups experiencing CVD disparities.
Recent Innovations
Current innovations and contextual events are important for PCORI to consider as it plans its portfolio of CVD disparities research. Electronic health records and health information exchange are the key innovations that may facilitate CER related to addressing CVD disparities and/or improving patient-centered and patient-level outcomes in groups experiencing disparities. For example, health information technology may minimize or altogether remove the burden of abstracting patient data from registries or paper medical charts, making it easier for researchers to gather data on health indicators and outcomes of interest at baseline, during the intervention, and at follow-up. The Office of the National Coordinator (ONC) for Health Information Technology has concluded that “health IT has potential to impact the health of populations experiencing health disparities” (ONC 2013, 2).ONC’s future work in this area may present additional opportunities for PCORI research.
Reduce Disparities in Cardiovascular Disease 15

Pace of Research
Based on publication trends and recent FOAs, we expect a steady pace of research related to addressing CVD disparities. Our assessment of publication trends is limited to those papers that met the inclusion criteria for this landscape review. The number of articles for 2013 includes projections based on seven published study protocols that have not yet published results, but abstracts suggest that planned studies and those in progress align with the focus of this landscape review (Cabassa et al. 2011; LeBlanc et al. 2012; Lee et al. 2012; Ogedegbe et al. 2013; Schoenthaler et al. 2011; Warner et al. 2013; Willard-Grace et al. 2013).
The NIH and AHRQ FOAs posted in summer 2013 will support new behavioral and social science research on reducing health disparities. Because these FOAs are not specific to CVD and do not cover all groups experiencing disparities—the NIH FOA is restricted to racial/ethnic, socioeconomic status, and rural-urban health disparities and the AHRQ FOA focuses on racial/ethnic disparities in under-resourced settings—there is an opportunity for PCORI to complement and expand on research projects funded through the NIH and AHRQ FOAs and ensure that patient-centered outcomes research is integrated with health disparities research.
Exhibit 2. Number of Articles Meeting Landscape Review Inclusion Criteria by Publication Year
Note: 2013 includes actual (n = 3) and expected number of articles (n = 7) based on published study protocols identifed through this landscape review.
02468
101214
2008 2009 2010 2011 2012 2013
Num
ber o
f Pub
licat
ions
Publication Year
Reduce Disparities in Cardiovascular Disease 16

Potential for New Information to Rapidly Improve Care and Patient-Centered Outcomes Summary of the Factors that Would Affect the Translation of New Research Findings to Practice
Interventions that have been shown to be effective in the research setting have often failed when translated to practice (Damshroder et al. 2009). Adoption rates for innovations vary considerably; some are adopted and spread rapidly, while others fail to gain traction (Greenhalgh et al. 2004). To understand which research findings are likely to be quickly adopted and effectively implemented, researchers and organizations seeking to fund new research opportunities should examine the potential for successful translation. In this section, we discuss factors that impact the potential of interventions to be effectively translated into practice. We then examine the research opportunities identified in this landscape review, and described in the previous section, through the lens of these factors.
The implementation science literature offers multiple translation-related theories but with a significant amount of overlap. To overcome the issue of redundancy between various existing theories, and to develop a practical, usable, and comprehensive meta-framework that can assist in identifying which interventions may work in practice, Damshroder et al. (2009) developed the Consolidated Framework for Implementation Research (CFIR). The CFIR consists of a set of 37 total constructs, or factors, grouped by domains. We have selected and adapted five constructs that we believe provide PCORI with the answer to the question at hand: What factors affect translation of new research findings to practice?
Exhibit 3 presents selected CFIR domains, or major areas that impact implementation of interventions, as well as brief descriptions of five factors that are useful in evaluating the potential of interventions to be effectively translated into practice.
Reduce Disparities in Cardiovascular Disease 17

Exhibit 3. Factors that Impact Translation of Research Findings into Practice
Domain Factors
Intervention Characteristics: Characteristics of the intervention being implemented in practice
Adaptability: the extent to which the intervention can be modified to suit local needs
Trialability: whether the intervention can be tested on a small scale before large-scale implementation and whether course can be reversed easily if desired
Complexity: the difficulty of implementation, including the extent to which it disrupts current operations and systems, number of stages in implementation, scope, and duration of implementation
Outer Setting: The environmental factors that may affect implementation.
External policies: incentives, mandates, and insurance-related issues that may affect effective translation
Inner Setting: Features of the organization, system, or community in which in the intervention is being implemented in practice
Readiness for implementation: commitment of staff, involvement of staff, level of resources dedicated to implementation, accessibility of information for staff regarding implementation and sustainability
Source: Adapted and modified from Damshroder et al. 2009.
The domains and factors described in Exhibit 3 provide a structure to evaluate the potential of interventions identified in this landscape review to be effectively translated and adopted. This potential varies based on the interventions themselves and the contexts in which they are implemented (Damshroder et al. 2009). In the following section, we provide a brief discussion of the likelihood of the research findings identified in this landscape review being implemented in practice, using the factors listed in Exhibit 3 as a guide.
Discussion of Likelihood of New Research Findings Being Immediately Implemented in Practice
In previous sections, we identified opportunities for PCORI to help address research gaps around interventions to reduce or eliminate CVD disparities. In this section, we examine these research opportunities with a focus on factors that impact likelihood of translation (Exhibit 4). We designated the likelihood of translation as being low, intermediate, or high based on our expertise and on qualitative examination of the each of the constructs described in Exhibit 4. In addition, we considered each intervention’s characteristics across the translation constructs relative to the others. A description of our qualitative assessment follows.
Reduce Disparities in Cardiovascular Disease 18

Assess effectiveness of QI interventions. Overall, we rate QI interventions as having an intermediate likelihood for immediate implementation based on the following considerations outlined in Exhibits 3 and 4:
The adaptability and complexity of QI interventions will vary with the context and scope of the intervention itself. For example, if clinics in a health system are all part of a QI initiative, they will all have common goals, but the Plan-Do-Study-Act (PDSA) cycles in each clinic should be tailored appropriately. QI interventions typically do well on the trialability factor because starting on a small scale and expanding is an essential feature of QI initiatives, making it easier to reverse course or correct errors in implementation. Complexity depends on context, but QI interventions can be very complex, particularly when interfacing with electronic health records.
External policies depend on contextual factors, but generally speaking, insurance coverage for QI initiatives is not common, although health systems themselves may sponsor these initiatives based on the promise of increased future efficiencies.
Internal to the organization, leadership support for QI interventions that improve quality of care and efficiency of services can generally be expected to be strong. However, for effective implementation, resources need to be guaranteed prior to beginning the process of operationalization. Similarly, staff support within organizations for these initiatives is typically broad as long as the initiatives do not impact negatively on staffing or compensation.
Explore the added value of provider education. We suggest that effective patient and provider education interventions designed to improve quality of care and self-management of CVD have a high likelihood for immediate implementation based on the following considerations:
We assess dual patient-provider education interventions as being adaptable to contextual needs (e.g., physician training requirements and patient language barriers) and less complex (e.g., compared to the QI interventions described above). Additionally, these interventions do well on the trialability factor because they generally do not require commitment of large-scale resources for implementation.
Provider education is required and encouraged by licensing boards and health systems. However, provider education components are more likely to be adopted by providers if the education program aligns with these external forces.
Readiness of implementation can be expected to be high for these interventions. For example, staff can be trained and prepared using online trainings, webinars etc.
Reduce Disparities in Cardiovascular Disease 19

Exhibit 4. Translatability Considerations for Opportunities to Address CVD Disparities through CER
CER Opportunities
Translatability Considerations Intervention
Characteristics (Adaptability)
Intervention Characteristics
(Trialability)
Intervention Characteristics
(Complexity) Outer Setting (External
Policies) Inner Setting (Readiness of
Interventions) QI Depends on
context Yes Depends on context Unlikely that insurance will
cover staff time on QI in the future, but it is possible that health systems themselves will self-fund QI
Generally, strong leadership support can be expected, but commitment of resources prior to implementation is required; staff require training on QI
Patient and Provider Education
Adaptable to contextual needs
Yes Less complex Alignment with institutional and board requirements will influence provider adoption
Readiness may be easily achieved with webinars and other online training
Self-Management
Adaptable to contextual needs
Yes, but less so than other interventions described above
Complexity varies Most likely to be covered by insurance in the future
Staff availability may be a concern
Reduce Disparities in Cardiovascular Disease 20

Compare the effectiveness of various self-management support intervention models. We rate patient self-management interventions as having an intermediate likelihood for immediate implementation based on the following considerations:
Adaptability to patient needs is a primary requirement for self-management models and is usually built into the design. The complexity of the interventions varies significantly. For example, technology that interfaces with electronic health records tends to be more complex. Increased complexity also contributes to greater difficulty in implementing the intervention and reversing course if needed.
Of the three kinds of research areas discussed here, patient self-management interventions are most likely to be covered by insurance in the future.
Availability of staff to train patients on using the self-management model may be a concern for these interventions.
Durability of Information The interventions identified in this literature review, and in particular, those identified as having a high likelihood of being implemented in practice, are relatively durable. Concerns regarding durability are pressing in interventions where medical devices or other technological innovations are a major component because these technologies are replaced with improved versions, often on a continual basis (PCORI 2012). Medical devices and other technological solutions are not primary components of the interventions identified in this landscape review. However, QI interventions that have a major technological innovation component may be less durable than other interventions identified here. Although provider and patient education as well as patient-directed self-management programs may include software-components (such as interactive education applications), the core of these interventions is the education and self-management content, which is highly durable.
Reduce Disparities in Cardiovascular Disease 21

Conclusion This landscape review revealed several opportunities for new research designed to identify effective strategies for addressing CVD disparities and improving CVD outcomes among populations experiencing disparities. Generally, there is a need for more research directed at developing, testing, and assessing the comparative effectiveness of disparities interventions (i.e., interventions explicitly aimed at eliminating differences in CVD outcomes between segments of the population). In addition, there is an opportunity to better integrate health disparities and patient-centered outcomes research (few studies included in this review incorporated patient-centered outcomes of high importance to PCORI).
Specifically, within the context of interventions to address CVD disparities, studies are needed to (1) assess the effectiveness of health systems quality improvement interventions on reducing disparities and improving patient-centered outcomes, (2) compare the relative impact of provider education versus patient education versus provider and patient education on patient-level and patient-centered outcomes, and (3) compare the effectiveness of various self-management support intervention models. Based on our expertise and qualitative examination of key translatability constructs for these recommended studies, we conclude that findings from new research have an intermediate to high likelihood of swift translation into practice. Considering recent publication trends and AHRQ and NIH FOAs, we expect a steady pace of research related to addressing CVD disparities. However, because these FOAs are not specific to CVD and do not cover all groups experiencing disparities, there is an opportunity for PCORI to complement and expand on research projects funded through the NIH and AHRQ FOAs and ensure that patient-centered outcomes research is integrated with health disparities research. We also expect that electronic health records and health information exchange will facilitate new research on reducing disparities in CVD.
Reduce Disparities in Cardiovascular Disease 22

References Agency for Healthcare Research and Quality (AHRQ). 2012a. National Healthcare Disparities
Report. Available at http://www.ahrq.gov/research/findings/nhqrdr/nhdr12/nhdr12_prov.pdf. Accessed November 11, 2013.
Agency for Healthcare Research and Quality (AHRQ). 2012b. Closing the Quality Gap: Revisiting the State of the Science Series: Quality Improvement Interventions to Address Health Disparities. Available at http://www.ahrq.gov/legacy/clinic/tp/gapdisptp.htm. Accessed November 11, 2013.
Anderson, Daren R., Joan Christison-Lagay, Victor Villagra, Haibei Liu, and James Dziura. 2010. "Managing the Space Between Visits: A Randomized Trial of Disease Management for Diabetes in a Community Health Center." Journal of General Internal Medicine 25 (10): 1116–22.
Balcazar, Hector G, Theresa L Byrd, Melchor Ortiz, Sumanth R. Tondapu, and Monica Chavez. 2009. "A Randomized Community Intervention to improve Hypertension Control Among Mexican Americans: Using the Promotoras De Salud Community Outreach Model." Journal of Health Care for the Poor and Underserved 20 (4): 1079–94.
Beth Israel Deaconess Medical Center. 2003. Heart Disease: Differences Between Men and Women. Available at http://www.bidmc.org/CentersandDepartments/Departments/Medicine/Divisions/CardiovascularMedicine/YourHeartHealth/TipsforHeartHealth/HeartDiseaseDifferencesBetweenMenandWomen.aspx. Accessed November 11, 2013.
Bove, Alfred A., William P. Santamore, Carol Homko, Abul Kashem, Robert Cross, Timothy R. McConnell, Gail Shirk, and Francis Menapace. 2011. "Reducing Cardiovascular Disease Risk in Medically Underserved Urban and Rural Communities." American Heart Journal 161 (2): 351–9.
Cabassa, Leopoldo J., Benjamin Druss, Yuanjia Wang, and Roberto Lewis-Fernandez. 2011. "Collaborative Planning Approach to Inform the Implementation of a Healthcare Manager Intervention for Hispanics with Serious Mental Illness: A Study Protocol." Implementation Science 6: 80.
Cene, Crystal W., Lisa R. Yanek, Taryn F. Moy, David M. Levine, Lewis C. Becker, and Diane M. Becker. 2008. "Sustainability of a Multiple Risk Factor Intervention on Cardiovascular Disease in High-Risk African American Families." Ethnicity & Disease 18 (2): 169–75.
Centers for Disease Control and Prevention (CDC). 2011. “Million Hearts: Strategies to Reduce the Prevalence of Leading Cardiovascular Disease Risk Factors.” Morbidity and Mortality Weekly Report, 60 (36): 1248–51.
Centers for Disease Control and Prevention (CDC). 2013. Million Hearts: Risk Factors: About Heart Disease & Stroke. Available at http://millionhearts.hhs.gov/abouthds/risk-factors.html#hdRace. Accessed November 11, 2013.
Reduce Disparities in Cardiovascular Disease 23

Centers for Disease Control and Prevention (CDC). n.d. Health Equity Resource Toolkit for State Practitioners Addressing Obesity Disparities. Available at http://www.cdc.gov/obesity/downloads/CDCHealthEquityObesityToolkit508.pdf. Accessed November 11, 2013.
Community Preventive Services Task Force. 2013. Guide to Community Preventive Services. Cardiovascular Disease Prevention and Control: Clinical Decision-Support Systems (CDSS). Available at www.thecommunityguide.org/cvd/CDSS.html. Accessed November 11, 2013.
Cook, Ann, Coraleen T. Grothaus, Carol E. Gutierrez, Kimberly A. Kehoe, and Mona R. Valentin. 2010. "Closing the gap: Disparity in Native Hawaiian Cardiac Care." Hawaii Medical Journal 69 (5 Suppl 2): 7–10.
Cooper, Lisa A., Debra L. Roter, Kathryn A. Carson, Lee R. Bone, Susan M. Larson, Edgar R. Miller, 3rd, M. S. Barr, and D. M. Levine. 2011. "A Randomized Trial to Improve Patient-Centered Care and Hypertension Control in Underserved Primary Care Patients." Journal of General Internal Medicine 26 (11): 1297–304.
Damschroder, Laura J., David C. Aron, Rosalind E. Keith, Susan R. Kirsh, Jeffery A. Alexander, and Julie C. Lowery. 2009. "Fostering Implementation of Health Services Research Findings into Practice: A Consolidated Framework for Advancing Implementation Science." Implementation Science 4 (1): 50.
Davis, Andrew M., Vinci, Lisa M., Okwuosa, Tochi M., Chase, Ayana R., & Huang, Elbert S. (2008). “Cardiovascular Health Disparities: A Systematic Review of Health Care Interventions.” Medical Care Research and Review, 64: 29S–100S. Available at: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2367222/
DeWalt, Dean A., Dean Schillinger, Bernice Ruo, Kirsten Bibbins-Domingo, David W. Baker, George M. Holmes, Morris Weinberger, Aurelia Macabasco-O’Connell, Kimberly Broucksou, Victoria Hawk, Kathleen L. Grady, Brian Erman, Carla A. Sueta, Patricia P. Chang, Crystal Wiley Cene, Jia-Rong Wu, Christine D. Jones, and Michael Pignone. 2012. "Multisite randomized trial of a single-session versus multisession literacy-sensitive self-care intervention for patients with heart failure." Circulation 125 (23):2854-62.
Eckman, Mark H., Ruth Wise, Anthony C. Leonard, Estrelita Dixon, Christine Burrows, Faisal Khan, and Eric Warma. 2012. "Impact of health literacy on outcomes and effectiveness of an educational intervention in patients with chronic diseases." Patient Educ Couns 87 (2):143-51.
Evans-Hudnall, Gina L., Melinda A. Stanley, Allison N. Clark, Amber L. Bush, Ken Resnicow, Yu Kass Liu, Joseph S. Kass, and Angelle M. Sander. 2012. "Improving Secondary Stroke Self-Care Among Underserved Ethnic Minority Individuals: A Randomized Clinical Trial of a Pilot Intervention." Journal of Behavioral Medicine. [Epub ahead of publication]
Reduce Disparities in Cardiovascular Disease 24

Glickman, Seth W., Christopher B. Granger, Fang-Shu Ou, Sean O'Brien, Barbara L. Lytle, Charles B. Cairns, Greg Mears, James W. Hoekstra, J. Lee Garvey, Eric D. Peterson, and James G. Jollis. 2010. "Impact of a Statewide ST-Segment-Elevation Myocardial Infarction Regionalization Program on Treatment Times for Women, Minorities, and the Elderly." Circulation: Cardiovascular Quality Outcomes (5): 514–21.
Go, Alan S., Mozaffarian, Dariush, Roger, Veronique L., Benjamin, Emelia J., Berry, Jarett D., Borden, William B., Bravata, Dawn M., Dai, Shifan, Ford, Earl S., Fox, Caroline S., Franco, Sheila, Fullerton, Heather J., Gillespie, Cathleen, Hailpern, Susan M., Heit, John A., Howard, Virginia J., Huffman, Mark D., Kissela, Brett M., Kittner, Steven J., Lackland, Daniel T., Lichtman, Judith H., Lisabeth, Lynda D., Magid, David, Marcus, Gregory M., Marelli, Ariane, Matchar, David B., McGuire, Darren K., Mohler, Emile R., Moy, Claudia S., Mussolino, Michael E., Nichol, Graham, Paynter, Nina P., Schreiner, Pamela J., Sorlie, Paul D., Stein, Joel, Turan, Tanya N., Virani, Salim S., Wong, Nathan D., Woo, Daniel, & Turner, Melanie B.; on behalf of the American Heart Association Statistics Committee and Stroke Statistics Subcommittee (2013). “Heart Disease and Stroke Statistics—2013 Update: A Report from the American Heart Association.” Circulation, 127, e6–e245.
Govil, Sarah R., Gerdi Weidner, Terri Merritt-Worden, and Dean Ornish. 2009. "Socioeconomic Status and Improvements in Lifestyle, Coronary Risk Factors, and Quality of Life: The Multisite Cardiac Lifestyle Intervention Program." American Journal of Public Health 99 (7): 1263–70.
Greenhalgh, Trisha, Glenn Robert, Fraser Macfarlane, Paul Bate, and Olivia Kyriakidou. 2004, "Diffusion of Innovations in Service Organizations: Systematic Review and Recommendations." Milbank Quarterly 82, (4): 581–629.
Gross, Barbara, E. Faye Anderson, Steven Busby, Karen H. Frith, and Christine E. Panco. 2013. "Using Culturally Sensitive Education To Improve Adherence With Anti-Hypertension Regimen." Journal of Cultural Diversity 20 (2): 75–79.
Giuse, Nunzia B., Taneya Y. Koonce , Alan B. Storrow , Sheila V. Kusnoor & Fei Ye. 2012. “Using Health Literacy and Learning Style Preferences to Optimize the Delivery of Health Information.” Journal of Health Communication 17 (3): 122–140.
Han, Hae- Ra, Jiyun Kim, Kim B. Kim, Seonghee Jeong, David Levine, Chunyu Li, Heejung Song, and Miyong T. Kim. 2010. "Implementation and Success of Nurse Telephone Counseling in Linguistically Isolated Korean American Patients with High Blood Pressure." Patient Education and Counselling 80 (1): 130–4.
Hebert, Kathy, Elyse Julian, Jorge Alvarez, Andre Dias, Leonardo Tamariz, Lee Arcement, and Henry C. Quevedo. 2011. "Eliminating Disparities in Hypertension Care for Hispanics and Blacks Using a Heart Failure Disease Management Program." Southern Medical Journal 104 (8): 567–73.
Heidenreich, Paul A., Trogdon, Justin G., Khavjou, Olga A., Butler, Javed, Dracup, Kathleen, Ezekowitz, Michael D., et al. (2011). “Forecasting the Future of Cardiovascular Disease in the United States.” Circulation, 123 (8): 933–44.
Reduce Disparities in Cardiovascular Disease 25

Houston, Thomas K., Jeroan J. Allison, Marc Sussman, Wendy Horn, Cheryl L. Holt, John Trobaugh, Maribel Salas, Maria Pisu, Yendelela L. Cuffee, Damien Larkin, Sharina D. Person, Bruce Barton, Catarina I. Kiefe, and Sandral Hullett. 2011. "Culturally Appropriate Storytelling to Improve Blood Pressure: A Randomized Trial." Annals of Internal Medicine 154 (2): 77–84.
Institute of Medicine (IOM). 2011. The Health of Lesbian, Gay, Bisexual, and Transgender People: Building a Foundation for Better Understanding. Washington, DC: The National Academies Press.
Jackson, George L., Eugene Z. Oddone, Maren K. Olsen, Benjamin J. Powers, Janet M. Grubber, Felicia McCant, and Hayden B. Bosworth. 2012. "Racial Differences in the Effect of a Telephone-Delivered Hypertension Disease Management Program." Journal of General Internal Medicine 27 (12): 1682–9.
Johnson, Wallace, Fadia T. Shaya, Niharika Khanna, Verlyn O. Warrington, Vivienne A. Rose, Xia Yan, Bessie Bailey-Weaver, C. Daniel Mullins, and Elijah Saunders. 2011. "The Baltimore Partnership to Educate and Achieve Control of Hypertension (The BPTEACH Trial): A Randomized Trial of the Effect of Education on Improving Blood Pressure Control in a Largely African American Population." Journal of Clinical Hypertension (Greenwich) 13 (8): 563–70.
Kim, Miyong T., Hea-Ra Han, Haley Hedlin, Jiyun Kim, Hee J. Song, Kim B. Kim, and Martha N. Hill. 2011. "Teletransmitted Monitoring of Blood Pressure and Bilingual Nurse Counseling-Sustained Improvements in Blood Pressure Control During 12 Months in Hypertensive Korean Americans." Journal of Clinical Hypertension (Greenwich, Conn.) no. 13 (8): 605–12.
Kripalani, Sunil, Brian Schmotzer, and Terry A. Jacobson. 2012. "Improving Medication Adherence through Graphically Enhanced Interventions in Coronary Heart Disease (IMAGE-CHD): A Randomized Controlled Trial." Journal of General Internal Medicine 27 (12): 1609–17.
LeBlanc, Annie, Kari L. Ruud, Megan E. Branda, Kristina Tiedje, Kasey R. Boehmer, Laurie J. Pencille, Holly Van Houten, Marc Matthews, Nilay D. Shah, Carl R. May, Barbara P. Yawn, and Victor M. Montori. 2012. "The Impact of Decision Aids to Enhance Shared Decision Making for Diabetes (The DAD Study): Protocol of a Cluster Randomized Trial." BMC Health Services Research 12: 130.
Lee, Elisa T., Jared B. Jobe, Jeunliang Yeh, Tauqeer Ali, Everett R. Rhoades, Allen W. Knehans, Diane J. Willis, Melanie R. Johnson, Ying Zhang, Bryce Poolaw, and Billy Rogers. 2012. "A Cardiovascular Risk Reduction Program for American Indians with Metabolic Syndrome: The Balance Study." Journal of Primary Prevention 33 (4): 187-96.
Martin, Michelle Y., Young-il Kim, Polly Kratt, Mark S. Litaker, Connie L. Kohler, Yu-Mei Schoenberger, Stephen J. Clarke, Heather Prayor-Patterson, Tung-Sung Tseng, Maria Pisu, and O. Dale Williams. 2011. "Medication Adherence Among Rural, Low-Income Hypertensive Adults: A Randomized Trial of a Multimedia Community-Based Intervention." American Journal of Health Promotion 25 (6):372-8.
Reduce Disparities in Cardiovascular Disease 26

Mensah George A. 2005. Eliminating Disparities in Cardiovascular Health: Six Strategic Imperatives and a Framework for Action. Circulation. 15; 111(10): 1332–6
Migneault, Jeffrey P., Julien J. Dedier, Julie A. Wright, Timothy Heeren, Marci K. Campbell, Donald E. Morisky, Peter Rudd, and Robert H. Friedman. 2012. "A Culturally Adapted Telecommunication Aystem to Improve Physical Activity, Diet Quality, and Medication Adherence Among Hypertensive African-Americans: A Randomized Controlled Trial." Annals of Behavioral Medicine 43 (1): 62–73.
Mosca, Lori, Allison H. Christian, Heidi Mochari-Greenberger, Paul Kligfield, and Sidney C. Smith, Jr. 2010. "A Randomized Clinical Trial of Secondary Prevention Among Women Hospitalized with Coronary Heart Disease." Journal of Women’s Health (Larchmt) 19 (2): 195-202.
National Center for Complementary and Alternative Medicine. 2013. Complementary, Alternative, or Integrative Health: What’s In a Name? Available at http://nccam.nih.gov/health/whatiscam. Accessed November 20, 2013.
National Institutes of Health. 2012. Theory at a Glance: A Guide for Health Promotion Practice. Available at http://www.cancer.gov/cancertopics/cancerlibrary/theory.pdf. Accessed November 20, 2013.
National Institutes of Health. 2013a. Behavioral and Social Science Research on Understanding and Reducing Health Disparities (R01). PA-13-292. Available at http://grants.nih.gov/grants/guide/pa-files/PA-13-292.html. Accessed November 11, 2013.
National Institutes of Health. 2013b. Closing the Gap in Healthcare Disparities through the Dissemination and Implementation of Patient Centered Outcomes Research. RFA-HS-13-010. Available at http://grants.nih.gov/grants/guide/rfa-files/RFA-HS-13-010.html. Accessed November 11, 2013.
National Prevention Council (2102). National Prevention Council Action Plan: Implementing the National Prevention Strategy. Available at: http://www.surgeongeneral.gov/initiatives/prevention/2012-npc-action-plan.pdf
Noureldin, Marwa, Kimberly S. Plake, Daniel G. Morrow, Wanzhu Tu, Jingwei Wu, and Michael D. Murray. 2012. "Effect of Health Literacy on Drug Adherence in Patients with Heart Failure." Pharmacotherapy 32 (9): 819-26.
Nundy, Shantanu, Rabia R. Razi, Jonathan J. Dick, Bryan Smith, Ainoa Mayo, Anne O'Connor, and David O. Meltzer. 2013. "A Text Messaging Intervention to Improve Heart Failure Self-Management after Hospital Discharge in a Largely African-American Population: Before-After Study." Journal of Medical Internet Research 15 (3): e53.
O'Connor, Alane, and Gregory A. Wellenius. 2012. “Rural–Urban Disparities in the Prevalence of Diabetes and Coronary Heart Disease.” Public Health 126, (10): 813-20.
Office of the National Coordinator (ONC). 2013. Understanding the Impact of Health IT in Underserved Communities and Those with Health Disparities. Available at http://www.healthit.gov/sites/default/files/hit_disparities_report_050713.pdf
Reduce Disparities in Cardiovascular Disease 27

Ogedegbe, Gbenga, Senaida Fernandez, Leanne Fournier, Stephanie A. Silver, Jian Kong, Sara Gallagher, Franze de la Calle, Jordan Plumhoff, Sheba Sethi, Evelyn Choudhury, and Jeanne A. Teresi. 2013. "The Counseling Older Adults to Control Hypertension (COACH) Trial: Design and Methodology of a Group-Based Lifestyle Intervention for Hypertensive Minority Older Adults." Contemporary Clinical Trials 35 (1), 70–9.
Ogedegbe, Gbenga O., Carla Boutin-Foster, Martin T. Wells, John P. Allegrante, Alice M. Isen, Jared B. Jobe, and Mary E. Charlson. 2012. "A Randomized Controlled Trial of Positive-Affect Intervention and Medication Adherence in Hypertensive African Americans." Archives of Internal Medicine 172 (4): 322–6.
PCORI. 2007. PCORI’s National Priorities for Research and Research Agenda. Adopted by the PCORI Board of Governors on May 21, 2012 http://www.pcori.org/research-we-support/priorities-agenda/ Accessed November 11, 2013.
PCORI. 2012. From Questions to Funding: About Our Topic Generation and Research Prioritization Process. Available at: http://www.pcori.org/funding-opportunities/funding-announcements/from-research-questions-to-research-funding-about-our-topic-generation-and-research-prioritization-process/. Accessed November 20, 2013.
PCORI. 2013. Advisory Panel on Addressing Disparities. September 11, 2013 Meeting Summary. Available at: http://www.pcori.org/get-involved/pcori-advisory-panels/advisory-panel-on-addressing-disparities/ Accessed November 7, 2013.
Pezzin, Liliana E., Penny H. Feldman, Jennifer M. Mongoven, Margaret V. McDonald, Linda M. Gerber, and Timothy R. Peng. 2011. "Improving Blood Pressure Control: Results of Home-Based Post-Acute Care Interventions." Journal of General Internal Medicine 26 (3):280–6.
Resnick, Helaine E., Perla R. Ilagan, Mary Beth Kaylor, Diane Mehling, and Majd Alwan. 2012. "TEAhM-Technologies for Enhancing Access to Health Management: A Pilot Study of Community-Based Telehealth." Telemedicine Journal and E-Health 18 (3)166-74.
Rigsby, Brenda D. 2011. "Hypertension Improvement Through Healthy Lifestyle Modifications." ABNF Journal 22 (2): 41–3.
Rocha-Goldberg Maria del, Pilar., Leonor Corsino, Bryan Batch, Corrine I. Voils, Carolyn T. Thorpe, Hayden B. Bosworth, and Laura P. Svetkey. 2010. "Hypertension Improvement Project (HIP) Latino: Results of a Pilot Study of lifestyle Intervention for Lowering Blood Pressure in Latino Adults." Ethnicity & Health 15 (3):269–82.
Rodriguez, Fatima, Lula Christopher, Caitlin E. Johnson, Yun Wang, and JoAnne M. Foody. 2012. "Love Your Heart: A Pilot Community-Based Intervention to Improve the Cardiovascular Health of African American Women." Ethnicity & Disease 22 (4): 416–21.
Schneider, Robert H., Clarence E. Grim, Maxwell V. Rainforth, Theodore Kotchen, Sanford I. Nidich, Carolyn Gaylord-King, John W. Salerno, Jane M. Kotchen, and Charles N. Alexander. 2012. "Stress Reduction in the Secondary Prevention of Cardiovascular Disease: Randomized, Controlled Trial of Transcendental Meditation and Health Education in Blacks." Circulation: Cardiovascular Quality Outcomes 5 (6):750–8.
Reduce Disparities in Cardiovascular Disease 28

Schoenthaler, Antoinette, Leanne Luerassi, Jeanne A. Teresi, Stephanie Silver, Jian Kong, Taiye Odedosu, Samantha Trilling, Anna Errico, Oshevire Uvwo, Kimberly Sebek, Adetutu Adekoya, and Gbenga Ogedegbe. 2011. "A Practice-Based Trial of Blood Pressure Control in African Americans (TLC-Clinic): Study Protocol for a Randomized Controlled Trial." Trials 12: 265.
Shaya, Fadia T., Viktor V. Chirikov, C. Daniel Mullins, Jon Shematek, Deleonardo Howard, Clyde Foster, and Elijah Saunders. 2013. "Social Networks Help Control Hypertension." Journal of Clinical Hypertension (Greenwich) 15 (1): 34–40.
Turner, Barbara J., Christopher S. Hollenbeak, Yuanyuan Liang, Kavita Pandit, Shelly Joseph, and Mark G. Weiner. 2012. "A Randomized Trial of Peer Coach and Office Staff Support to Reduce Coronary Heart Disease Risk in African-Americans with Uncontrolled Hypertension." Journal of General Internal Medicine 27 (10): 1258–64.
Uhlig Katrin, Balk Ethan M., Patel Kamal, Ip Stanley, Kitsios Georgios D., Obadan Ndidiamaka O., Haynes Shana M., Stefan Mihaela, Rao Madhumathi, Kong Win Chang Lina, Gaylor Jim, Iovin Ramon C. 2012. “Self-Measured Blood Pressure Monitoring: Comparative Effectiveness.” Comparative Effectiveness Review 45. Rockville, MD: Agency for Healthcare Research and Quality.
Victor, Ronald G., Joseph E. Ravenell, Anne Freeman, David Leonard, Deepa G. Bhat, Moiz Shafiq, Patricia Knowles, Joy S. Storm, Emily Adhikari, Kirsten Bibbins-Domingo, Pamela G. Coxson, Mark J. Pletcher, Peter Hannan, and Robert W. Haley. 2011. "Effectiveness of a Barber-Based Intervention for Improving Hypertension Control In Black Men: The BARBER-1 Study: A Cluster Randomized Trial." Archives of Internal Medicine 171 (4): 342–50.
Warner, Erica T., Russell E. Glasgow, Karen M. Emmons, Gary G. Bennett, Sandy Askew, Bernard Rosner, and Graham A. Colditz. 2013. "Recruitment and Retention of Participants in a Pragmatic Randomized Intervention Trial at Three Community Health Clinics: Results and Lessons Learned." BMC Public Health 13: 192.
Willard-Grace, Rachel, Denise DeVore, Ellen H. Chen, Danielle Hessler, Thomas Bodenheimer, and David H. Thom. 2013. "The Effectiveness of Medical Assistant Health Coaching for Low-Income Patients with uncontrolled Diabetes, Hypertension, and Hyperlipidemia: Protocol for a Randomized Controlled Trial and Baseline Characteristics of the Study Population." BMC Family Practice 14: 27.
Yancy, Clyde W., William T. Abraham, Nancy M. Albert, Robert Clare, Wendy Gattis Stough, Mihai Gheorghiade, Barry H. Greenberg, Christopher M. O'Connor, Lilin She, Jie Lena Sun, James B. Young, and Gregg C. Fonarow. 2008. "Quality of Care of and Outcomes for African Americans Hospitalized with Heart Failure: Findings from the OPTIMIZE-HF (Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients With Heart Failure) registry." Journal of the American College of Cardiology 51 (17): 1675–84.
Zarate-Abbott, Perla, Annette Etnyre, Irene Gilliland, Marveen Mahon, David Allwein, Jennifer Cook, Vanessa Mikan, Maureen Rauschhuber, Renee Sethness, Larua Munoz, Jolynn Lowry, and Mary Elaine Jones. 2008. "Workplace Health Promotion: Strategies for low-Income Hispanic Immigrant Women." AAOHN Journal 56 (5): 217–22.
Reduce Disparities in Cardiovascular Disease 29

Appendix A: Methods Highlights
We conducted a non-systematic literature review as well as a grey literature search (scan of websites of relevant organizations) to identify interventions to address CVD disparities and related research gaps. Our goal was to identify interventions of the following two broad types:
clinical and clinical-community linkage interventions aimed at addressing disparities in health outcomes associated with cardiovascular disease (CVD), including hypertension; and
clinical and clinical-community linkage interventions aimed at addressing CVD in populations experiencing disparate health outcomes.
Literature Review
To identify relevant articles, we conducted a literature search using three databases: PubMed, CINAHL, and the Cochrane Library. To guide our search in these databases, we identified medical subject heading (MeSH) terms and keywords related to CVD, health disparities or disparate populations, and types of interventions. The search had the following limits:
time period: 2008 to present;
publication language: English;
population: U.S. adults; and
abstract available.
We did not limit the abstract literature search based study design. Based on the PCORI-RTI team’s expertise in this area, we did not expect to find many randomized controlled trials on this topic and agreed that insights regarding research gaps could be gained through studies that span the spectrum from observational to experimental. A team of four persons conducted single-reviewer review of the abstracts using the inclusion and exclusion criteria detailed in Exhibit 5. Prior to abstract review, a training and pilot review of 10 abstracts was conducted to standardize reviews.
Reduce Disparities in Cardiovascular Disease A-1

Exhibit 5. Inclusion and Exclusion Criteria for Literature Review Component of the Landscape Review
Category Include Exclusion Population Adults aged 18 and older
U.S. population Populations experiencing disparate
health outcomes associated with CVD • Racial/ethnic minorities • Low socioeconomic status • Uninsured or underinsured • Limited English proficiency, low
literacy, and/or low numeracy • Rural • Living in the southeastern part of
the country • Medically underserved • Living with disabilities • Women • LGBT
Study populations where even a portion of the population is less than 18 years of age
Intervention Intervention is present AND Intervention explicitly aimed at
addressing disparities in CVD health outcomes OR addressing CVD in populations experiencing disparate health outcomes
AND Clinical (e.g., health care
setting/system) OR clinical-community linkage (e.g., community health workers, community pharmacists, chronic disease self-management programs) interventions
AND CVD secondary prevention (e.g.,
screening and diagnosis) OR tertiary prevention (e.g., tobacco use cessation in persons with diagnosed CVD; treatment/management interventions)
No intervention implemented (e.g., description of CVD burden and/or disparities; study protocol or other description of planned intervention)
CVD not identified as a primary focus of the intervention (e.g., HIV intervention that includes blood pressure monitoring)
Addressing disparities OR CVD in disparate populations not an explicit intervention aim
Purely community-based interventions (e.g., media campaigns, built or food environment initiatives)
Interventions that focus only on primary prevention
Drug or device studies Papers describing trial design but
not including outcome data
Reduce Disparities in Cardiovascular Disease A-2
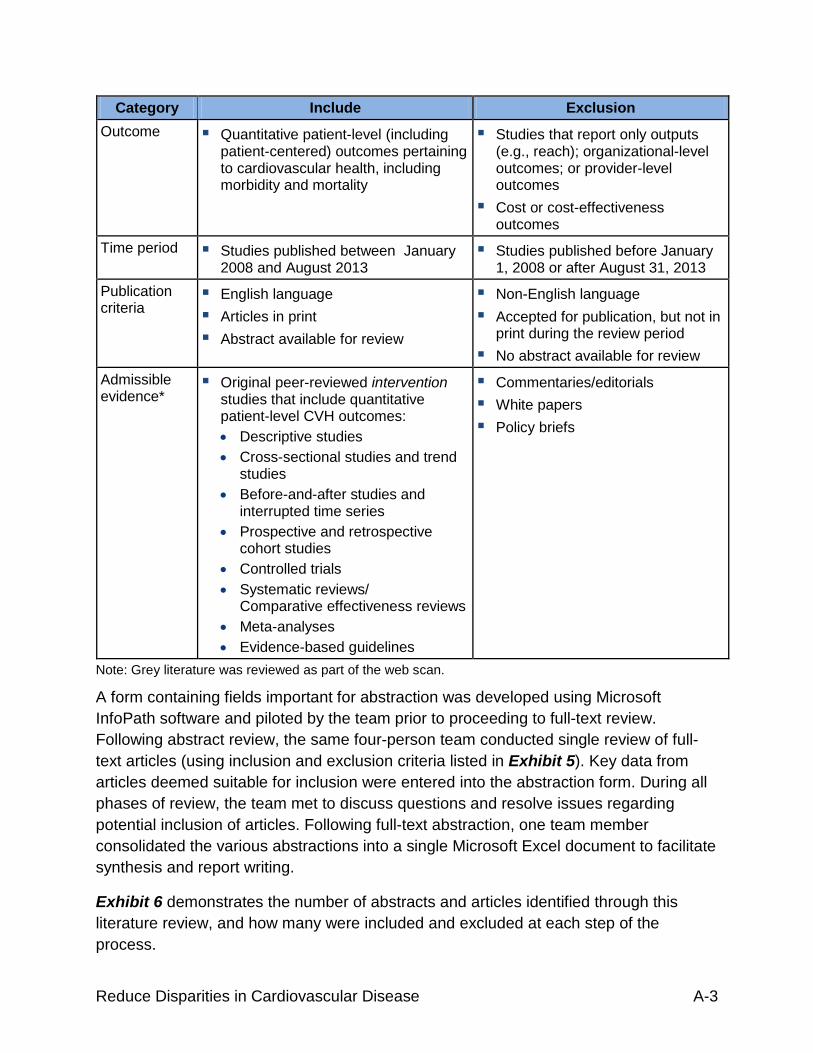
Category Include Exclusion Outcome Quantitative patient-level (including
patient-centered) outcomes pertaining to cardiovascular health, including morbidity and mortality
Studies that report only outputs (e.g., reach); organizational-level outcomes; or provider-level outcomes
Cost or cost-effectiveness outcomes
Time period Studies published between January 2008 and August 2013
Studies published before January 1, 2008 or after August 31, 2013
Publication criteria
English language Articles in print Abstract available for review
Non-English language Accepted for publication, but not in
print during the review period No abstract available for review
Admissible evidence*
Original peer-reviewed intervention studies that include quantitative patient-level CVH outcomes: • Descriptive studies • Cross-sectional studies and trend
studies • Before-and-after studies and
interrupted time series • Prospective and retrospective
cohort studies • Controlled trials • Systematic reviews/
Comparative effectiveness reviews • Meta-analyses • Evidence-based guidelines
Commentaries/editorials White papers Policy briefs
Note: Grey literature was reviewed as part of the web scan.
A form containing fields important for abstraction was developed using Microsoft InfoPath software and piloted by the team prior to proceeding to full-text review. Following abstract review, the same four-person team conducted single review of full-text articles (using inclusion and exclusion criteria listed in Exhibit 5). Key data from articles deemed suitable for inclusion were entered into the abstraction form. During all phases of review, the team met to discuss questions and resolve issues regarding potential inclusion of articles. Following full-text abstraction, one team member consolidated the various abstractions into a single Microsoft Excel document to facilitate synthesis and report writing.
Exhibit 6 demonstrates the number of abstracts and articles identified through this literature review, and how many were included and excluded at each step of the process.
Reduce Disparities in Cardiovascular Disease A-3

Exhibit 6. Summary of Literature Search and Selection
Reduce Disparities in Cardiovascular Disease A-4

Grey Literature Scan (Website Review)
We conducted a review of a targeted list of websites to identify additional interventions meeting our inclusion criteria and/or research gaps related to addressing CVD disparities. We reviewed the following websites:
AHRQ
CDC
Million Hearts
AHA
NHLBI
The Community Guide
AHRQ and NIH FOAs, Community Guide recommendations, CVD burden data, and CVD health disparities statistics were identified through the web scan and cited throughout this landscape review as appropriate.
Reduce Disparities in Cardiovascular Disease A-5

Appendix B: At-a-Glance Summary of Interventions SYSTEMS-LEVEL INTERVENTIONS
Citation Intervention Description Length of
Intervention* Study
Design Length of
Study* Sample
Size Summary of Reported Results Glickman et al. 2010
Statewide ST-segment-elevation myocardial infarction (STEMI) regionalization program designed to reduce treatment times among women, minorities, and the elderly
-- Pre-post 1.5 years
N=2,063 Patient Level: Women, minorities, and the elderly received comparable benefits relative to their counterparts from improved systems of care that were implemented. The intervention was also associated with a significant reduction in baseline care differences in door-to-electrocardiogram times in women versus men.
Hebert et al. 2011
Heart failure disease management program that provided a standardized algorithm of care to eliminate disparities in hypertension care for African American and Hispanic patients in an urban and a rural safety net hospital
-- Pre-post 10 years N=898 Patient Level: Whites were more likely than African Americans or Hispanics to achieve a lower final blood pressure (BP) reading as well as reaching either the standard or more intensive BP goal, despite all groups having similar absolute changes in BP per patient from baseline.
Yancy et al. 2008
Registry and performance-improvement program intended to improve quality of care and outcomes for African Americans hospitalized with heart failure
-- Pre-post 2 years N=5,791 Patient Centered: African American patients had a lower risk-adjusted inpatient mortality due to heart failure, but a similar adjusted 60- to 90-day post-discharge morbidity and mortality risk due to heart failure. Patient Level: Among participating hospitals, the provision of most but not all quality measures were similar between African American patients and patients of other races.
* Estimated value based on information provided in cited paper -- Unable to determine based on information provided in cited paper
Reduce Disparities in Cardiovascular Disease B-1

PATIENT-PROVIDER LEVEL INTERVENTIONS
Citation Intervention Description Length of
Intervention* Study
Design Length of
Study* Sample
Size Summary of Reported Results Cooper et al. 2011
Physician communication skills training and patient coaching interventions designed to address hypertension among underserved primary care patients
-- Randomized trial
3 years Physicians: N=41 Patients: N=279
Patient Level: No improvements in patient adherence to medication were reported. Positive intervention effects reported include patient satisfaction with physicians’ decision-making styles, facilitation, and information exchange, and the clinically significant, though not statistically significant, reductions in systolic BP among uncontrolled hypertensive patients. The greatest improvements in BP were seen among patients who received coaching by a community health worker and whose physicians also received patient-centered communication skills training.
Johnson et al. 2011
Physician education, patient education, and physician and patient education interventions designed to improve blood pressure control in African American patients
Physicians: 12 education sessions over 24 months Patients: --
Randomized trial
2.5 years Physicians: N=10 Patients: N=552
Patient Level: The physician and patient education intervention group achieved a significantly better reduction in systolic BP compared with the usual care group.
* Estimated value based on information provided in cited paper -- Unable to determine based on information provided in cited paper
Reduce Disparities in Cardiovascular Disease B-2

PATIENT-LEVEL INTERVENTIONS
Citation Intervention Description Length of
Intervention* Study
Design Length of
Study* Sample
Size Summary of Reported Results Anderson et al. 2010
Telephone-based disease management intervention designed to improve CVD and other health outcomes for community health center patients with diabetes
12 months Randomized trial
-- N=295 Patient Centered: Perceived health status did not vary between treatment and control groups. Patient Level: Results indicated no significant benefit on a wide variety of primary and secondary clinical and behavioral outcomes, including self-reported rates of physical activity. Interval estimates for a primary outcome variable, glycemic control, excluded a clinically significant difference in HbA1c.
Balcazar et al. 2009
In-person and phone-based promotora intervention designed to improve hypertension control among Mexican Americans
2 months Randomized trial
3 years N=98 Patient Level: Results indicated statistically significant differences between the intervention and control groups on perceived benefits of healthy behaviors and two behavioral outcomes (reduce intake of salt and sodium, reduce cholesterol and fat).
Reduce Disparities in Cardiovascular Disease B-3

PATIENT-LEVEL INTERVENTIONS
Citation Intervention Description Length of
Intervention* Study
Design Length of
Study* Sample
Size Summary of Reported Results Bove et al. 2011
Nurse management (NM) CVD risk reduction program and NM system augmented with telemedicine communication interventions
12 months Randomized trial
1 year N=388 Patient Centered: In both groups, risk score was reduced, driven by a reduction in hypertension and hyperlipidemia prevalence, early in the study and was sustained throughout the 1-year study. Patient Level: Total cholesterol decreased significantly in both groups. There were no significant differences between groups on BP response Medication adherence was similar in both high- and intermediate-risk subjects.
Cene et al. 2008
Community-based self-management care provided by a nurse practitioner/community health worker team and enhanced usual care interventions to reduce CVD risk among high-risk African American families
12 months Randomized trial
3 years N=363 Patient Level: No significant differences were detected between groups in mean low-density lipoprotein cholesterol, systolic and diastolic blood pressure, or in the overall percentages achieving goal cholesterol, blood pressure, or smoking status.
Cook et al. 2010
Nurse-delivered educational intervention designed to address health care disparities among Native Hawaiian patients admitted with myocardial infarction and heart failure
-- Observational study
2 years N=137* Patient Centered: All quality indicators for patients improved; readmissions that occurred in less than 30 days for patients admitted with myocardial infarctions and heart failure decreased to match those for all other patient populations. There was a reduction in adverse events following percutaneous coronary interventions among the target population.
Reduce Disparities in Cardiovascular Disease B-4

PATIENT-LEVEL INTERVENTIONS
Citation Intervention Description Length of
Intervention* Study
Design Length of
Study* Sample
Size Summary of Reported Results DeWalt et al. 2012
Single session literacy sensitive self-care training for clinic patients with heart failure and single session plus ongoing telephone-based support
Single session: 40 minutes Telephone-based support: 1 month
Randomized trial
2 years N=605 Patient Centered: There was no difference between single session and multiple session intervention groups on all cause hospitalization or death. Patient Level: Emergency department visits not resulting in hospitalization did not differ between groups.
Eckman et al. 2012
Single occurrence VHS/DVD plus printed booklet intervention and printed booklet only intervention designed to improve coronary artery disease knowledge among patients with low health literacy
40 minutes Randomized trial
4 years N=187 Patient Level: Coronary artery disease knowledge scores increased significantly in all groups, and health behaviors improved for both intervention groups. There were no significant differences in improvements on coronary artery disease knowledge scores between patients with lower and higher health literacy.
Evans-Hudnall et al. 2012
STOP (secondary stroke prevention program) consisted of three culturally tailored information sessions and goal-setting activities that were delivered in person by a research assistant
-- Randomized trial
2 years N=52 Patient Level: Secondary stroke risk factors decreased among underserved racial/ethnic minorities.
Reduce Disparities in Cardiovascular Disease B-5

PATIENT-LEVEL INTERVENTIONS
Citation Intervention Description Length of
Intervention* Study
Design Length of
Study* Sample
Size Summary of Reported Results Govil et al. 2009
Multisite cardiac lifestyle intervention program (MCLIP) for male and female coronary heart disease (CHD) patients of lower SES
3 months Pre-post 6 months N=863 Patient Centered: Participants at all SES levels reported improvements in wellbeing (e.g., depression, hostility, quality of life). Patient Level: Participants across all education and income levels reported reduced dietary fat, improved stress management, and increased physical activity. Improvements in exercise capacity were also reported.
Gross et al. 2013
Culturally sensitive education program to support lifestyle changes and medication adherence among African American adults
2 months Pre-post -- N=10 Patient Level: Participants demonstrated improved adherence to their treatment routine, including life style changes, diet, exercise, and medication adherence.
Giuse et al. 2012
Educational material tailored to health literacy level and educational material tailored to health literacy level and learning style designed to improve hypertension knowledge among emergency department patients with high blood pressure
-- Randomized trial
5 months N=172 Patient Level: Participants in both intervention groups demonstrated improvements in post-test scores for hypertension knowledge with increased improvements among those receiving materials tailored to health literacy level and learning style.
Han et al. 2010
More-intensive and less-intensive nurse-provided telephone counseling to improve hypertension management among Korean American patients
24 months Randomized trial
5 years N=360 Patient Level: Over the 12-month counseling period, both groups demonstrated improved medication-taking, reduced alcohol consumption, and increased exercise; there were no significant group differences.
Reduce Disparities in Cardiovascular Disease B-6

PATIENT-LEVEL INTERVENTIONS
Citation Intervention Description Length of
Intervention* Study
Design Length of
Study* Sample
Size Summary of Reported Results Houston et al. 2011
Interactive storytelling intervention delivered via DVD designed to improve blood pressure among African American adults
6 months Randomized trial
1 year N=299 Patient Level: Patients with uncontrolled hypertension who were assigned to the intervention group experienced an 11–mm Hg greater reduction in systolic blood pressure than the comparison group. Following the intervention, blood pressure subsequently increased in both groups; however, the relative advantage for the intervention group was sustained until the end of follow-up.
Jackson et al. 2012
Three telephone-based interventions (nurse-administered and physician directed medication management that included use of a validated clinical decision support system; nurse-administered behavioral management intervention; and combined behavioral management and medication management intervention) for African American and white U.S. Department of Veterans Affairs primary care patients
18 months Randomized trial
3 years N=591 Patient Level: Results indicated significant improvement in mean systolic blood pressure at 12 and 18 months among African American patients receiving the combined medication management and behavioral self-management support intervention compared to African American patients receiving usual care. No comparable changes in blood pressure were found for non-Hispanic white patients.
Reduce Disparities in Cardiovascular Disease B-7

PATIENT-LEVEL INTERVENTIONS
Citation Intervention Description Length of
Intervention* Study
Design Length of
Study* Sample
Size Summary of Reported Results Kim et al. 2011
More-intensive and less-intensive nurse-provided telephone counseling to improve hypertension management among Korean American patients
24 months Randomized trial
~5 years N=360 Patient Centered: Depression scores for both groups decreased over time with no statistically significant differences between the groups. Patient Level: Both groups demonstrated slight increases in high blood pressure knowledge questionnaire scores. Perceived self-efficacy was slightly increased over time for participants in the more-intensive counseling group and slightly decreased in the less-intensive counseling group. Participants in both groups demonstrated improvements in adherence to HBP treatment recommendations.
Kripalani, Schmotzer, and Jacobson 2012
Randomized trial to evaluate the effect of illustrated medication schedule and refill reminder postcards on medication adherence among patients with low health literacy reported no significant improvements in medication adherence
12 months Randomized trial
1 year N=435 Patient Level: Neither mailed refill reminders nor illustrated medication schedules improved adherence overall. Post hoc subgroup analyses indicated that illustrated medication schedules may improve adherence among patients with low medication self-efficacy, polypharmacy, or baseline non-adherence.
Martin et al. 2011
Multimedia computer-based program designed to improve medication adherence among low-income hypertensive African American adults
6 months Randomized trial
-- N=434 Patient Level: Participants receiving the intervention did not differ from individuals in the control group on medication adherence.
Reduce Disparities in Cardiovascular Disease B-8

PATIENT-LEVEL INTERVENTIONS
Citation Intervention Description Length of
Intervention* Study
Design Length of
Study* Sample
Size Summary of Reported Results Migneault et al. 2012
Culturally tailored, automated telephone system designed to improve adherence to medication and other self-management guidelines among hypertensive African American adults
8 months Randomized trial
4 years N=337 Patient Level: No significant intervention effects were observed at the 4- and 12-month assessments. Based on post-hoc analysis, the intervention was associated with greater absolute improvements in most primary and secondary outcomes among diabetics, but results were not statistically significant given the small subgroup size (n=127).
Mosca et al. 2010
Education and counseling intervention provided by a prevention facilitator/educator during hospitalization and by phone following discharge to improve adherence to secondary CHD prevention guidelines among women
-- Randomized trial
2.5 years N=304 Patient Level: Minority women assigned to the intervention were two times as likely to achieve the blood pressure goal compared with minority women who received usual care.
Noureldin et al. 2012
Pharmacist intervention, including patient education, therapeutic monitoring, and communication with primary care providers designed to improve medication adherence among heart failure patients with limited versus adequate health literacy
9 month intervention with 3 month follow-up period
Post hoc analysis of randomized trial data
3 years N=314 Patient Level: The intervention generally increased medication taking and scheduling adherence. In patients with inadequate health literacy, the intervention increased adherence levels similar to baseline of those with adequate health literacy.
Reduce Disparities in Cardiovascular Disease B-9

PATIENT-LEVEL INTERVENTIONS
Citation Intervention Description Length of
Intervention* Study
Design Length of
Study* Sample
Size Summary of Reported Results Nundy et al. 2013
Text message–based intervention designed to improve heart failure self-management following hospital discharge among African American adults
1 month Pre-post 3 months N=15 Patient Level: The text messaging intervention was associated with clinically significant improvements in self-care maintenance and management.
Ogedegbe et al. 2012
Patient education and patient education with positive-affect induction and self-affirmation interventions for hypertensive African American patients in two primary care practices
12 months Randomized trial
-- N=256 Patient Level: The positive-affect intervention had a significantly greater impact on medication adherence compared to the patient education intervention. The positive-affect intervention had no significant effect on BP reduction.
Pezzin et al. 2011
Nurse and health educator counseling intervention to improve blood pressure control among high-risk African American home care adults
3 months Randomized trial
3 years N=845 Patient Level: The nurse-led intervention significantly improved BP control among patients with stage 2 hypertension as defined in the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure.
Resnick et al. 2012
Nurse-monitored telehealth kiosks placed in community-based senior centers to lower blood pressure levels and improve blood pressure control among older adults
3 months Non-randomized trial
10 months N=112 Patient Level: Relative to baseline, mean blood pressure at 10 months post-intervention were lower and the percentage of participants with controlled BP was higher in the intervention group. Note that inferential statistics were not provided because the pilot study was not powered or designed for hypothesis testing.
Reduce Disparities in Cardiovascular Disease B-10

PATIENT-LEVEL INTERVENTIONS
Citation Intervention Description Length of
Intervention* Study
Design Length of
Study* Sample
Size Summary of Reported Results Rigsby 2011 Community-based education
and physical activity intervention designed to improve blood pressure control among African American adults
3 months Pre-post -- N=36 Patient Level: Patients experienced an improvement in both knowledge and BP control, but significance tests were not conducted.
Rocha-Goldberg Mdel et al. 2010
Culturally tailored behavioral intervention to lower blood pressure in Latino adults
1.5 months Pre-post study
1.5 months N=17 Patient Level: The intervention yielded clinically significant decreases in systolic blood pressure among participants.
Rodriguez et al. 2012
Community-based, culturally tailored nutrition and physical activity program designed to improve the cardiovascular health of African American women
3 months Pre-post study
4 months N=34 Patient Level: Intervention participants had a significant reduction in systolic BP, as well as clinically important reduction in systolic BPs.
Schneider et al. 2012
Transcendental meditation and health educations interventions focused on secondary CVD prevention for African Americans
-- Randomized trial
8 years N=201 Patient Centered: Based on follow-up data (average follow-up of 5.4 years), there was a significant reduction of risk for mortality, myocardial infarction, and stroke in coronary heart disease patients in the transcendental meditation intervention group. Patient Level: There were significant reductions of systolic blood pressure and anger expression among transcendental meditation intervention participants.
Reduce Disparities in Cardiovascular Disease B-11

PATIENT-LEVEL INTERVENTIONS
Citation Intervention Description Length of
Intervention* Study
Design Length of
Study* Sample
Size Summary of Reported Results Shaya et al. 2013
Nurse-led group education sessions designed to improve hypertension control among African American adults in urban communities
-- Non-randomized trial
3 years N=530 Patient Level: At the 18-month follow up, the intervention group had a statistically significant larger decrease in systolic and diastolic BP and compared with the control group.
Turner et al. 2012
Phone-based counseling provided by peer patients with well-controlled hypertension paired and office-based counseling provided by trained practice staff designed to reduce CHD risk among African American patients with uncontrolled hypertension
6 months Randomized trial
2.5 years N=280 Patient Level: Compared to the control group, more patients in the intervention group achieved target BP reductions. CHD risk reduction favored the intervention, but this result was not statistically significant.
Victor et al. 2011
Blood pressure monitoring and referral program administered by barbers in community barber shops designed to improve blood pressure control among patrons with high blood pressure
10 months Randomized cluster trial
13 months N=1,022 Patient Level: The hypertension control rate increased more in intervention group than in control group, but a marginal effect was found for systolic BP change in the intervention group.
Zarate-Abbott et al. 2008
Conducted a pre-post study to determine the effects of a nurse-led workplace education program for low-income, immigrant Hispanic women on blood pressure control and heart-healthy behaviors
1.5 years Pre-post study
1.5 years N=39 Patient Level: Intervention participants demonstrated a significant reduction in both systolic and diastolic BP over the course of the intervention.
* Estimated value based on information provided in cited paper -- Unable to determine based on information provided in cited paper
Reduce Disparities in Cardiovascular Disease B-12

Appendix C: Glossary Definitions of Key Terms as Developed for the Purposes of this Landscape Review
Cardiovascular disease (CVD): pathological conditions involving the cardiovascular system, including the heart, the blood vessels, or the pericardium (hypertension included)
Cardiovascular health (CVH): The American Heart Association defines cardiovascular health as the absence of disease and the presence of seven key health factors and behaviors: blood pressure, physical activity, cholesterol, healthy diet, healthy weight, smoking status, and blood glucose.
Interventions: includes diagnosis, secondary (e.g., screening) and tertiary (e.g., tobacco cessation in persons with diagnosed CVD) prevention approaches, and treatment; interventions may be implemented in clinical or community settings, or be a joint community-clinical effort
Health disparities: differences in health outcomes and their determinants between segments of the population, as defined by social, demographic, environmental, and geographic attributes
Populations at risk for experiencing CVD disparities:
racial/ethnic minorities
low socioeconomic status
uninsured or underinsured
limited English proficiency, low literacy, and/or low numeracy
rural populations
adults living in the southeastern part of the country
medically underserved
living with disabilities
women
lesbian/gay/bisexual/transgender
Patient-centered outcomes: outcomes that are important to patients, including
Reduce Disparities in Cardiovascular Disease C-1
new diagnosis, incident disease
disease-specific morbidity (e.g., amputations, hospitalizations, getting a stent for CVD)
disease-specific or all-cause mortality
health-related quality of life as measured by generally accepted generic health-related quality-of-life measures (e.g., short-form questionnaires, EuroQOL) or disease-specific measures
symptoms, patient-reported
activities of daily living as measured by generally accepted standardized measures of basic and/or instrumental activities of daily living (e.g., Katz, Lawton, or Bristol instruments) or with instruments that have demonstrated validity and reliability
patient satisfaction with care
work or school absenteeism
patient and caregiver participation in medical care and decision making
Patient-level outcomes: outcomes patients experience, or that are measured from the patients’ perspective, including
quality of care
patient knowledge, attitudes, and behaviors
adherence to medications and self-management behaviors
physiological measures (blood pressure level, HbA1c)
goals of therapy met
health care utilization (doctor visits)
Harms: unintended patient-centered, patient-level, or systems level outcomes, including
patient fatigue
patient distress
breach of patient confidentiality
stigmatization
perpetuation of disparities in patient-centered or patient-level outcomes
Reduce Disparities in Cardiovascular Disease C-2