Understanding household attitudes to polio vaccination and routine immunisation in Northern Nigeria...
35
Understanding household attitudes to polio vaccination and routine immunisation in Northern Nigeria BBC Media Action 16 March, 2015
-
Upload
lorena-owens -
Category
Documents
-
view
221 -
download
0
Transcript of Understanding household attitudes to polio vaccination and routine immunisation in Northern Nigeria...

Understanding household attitudes to polio vaccination and routine immunisation in
Northern Nigeria
BBC Media Action16 March, 2015
Context and research ‘problem’

Nigeria, Polio: 2004-14…2015?
• During the mid-2000s, Nigeria constituted one of the primary engines of global poliovirus transmission
• By 2014, circulating wild virus was driven to a historical low– In February 2015, there have been no new cases for 8 months [last WPV1 24th July
2014]
• But Nigeria should not consider itself ‘nearly there’ (IMB, October 2014)
• Significant vulnerabilities remain: – Uneven SIA quality and coverage – Small residual clusters of incidental and/or chronically missed children

‘Missed children’: intentional or incidental
• Improved programme and independent data on ‘missed children’
• But continuing uncertainty about nature and causes of missed children (demand-side)– Refusal, ‘covert refusal’; ‘child absent/out of household’; caregiver hesitancy (‘too much
OPV’, ‘no felt need’, ‘other priorities’)– Need to distinguish between intentional and incidental missed children (Pakistan TAG,
2015; IMB, 2014, 2012), and between ‘intrinsic’ and ‘instrumental’ vaccine rejection– Need to understand what shapes underlying household and community-level
social/political attitudes that, themselves, shape polio-related attitudes and behaviour

Research in the endgame: going beyond averages
• Residual nature of ‘problem’ suggests advantages of purposive sampling rather than (or complementary to) population-sampling
• Purposive sampling enables comparison of ‘high-’ and ‘low-performing’ areas
• Complex causation and localised combinations of factors influencing rate of missed children suggests research approaches which test a relatively broad set of contributory variables
• In particular integrating and testing quantitative and qualitative factors

Original research hypotheses
• That household attitudes to polio vaccination (and wider immunisation) are likely to be shaped, to an important extent, by knowledge, ideas, experiences and perceptions unconnected to the specific disease and vaccine
• That material socioeconomic and demographic conditions shaping households’ vaccine behaviour are themselves likely to be influenced by structural experiences of interaction with – reliance on or trust in – external actors within the health sector, but also perceived to be important in wider development and governance processes
• That future programmes relying on mass compliance (not least in public health) need to develop research and analysis modes which can differentiate non-compliance based on lack of information and consequential misunderstanding, on intrinsic doctrinal objection, and on instrumental expression of other socioeconomic and political issues
Household experiences of health and healthcare access/provision
Household socioeconomic and cultural characteristics
Polio missed children, RI attitude etc
Household experiences and perceptions of wider development,
governance and participation
Research in practice

Research purpose
- To assess the attitude of male and female heads of household towards polio vaccination in particular and child immunization in general
- To investigate what factors are associated with reported attitude– Inc. religion/sect, ethnicity, educational status, economic status, health history,
perceived community development, community participation, perceptions of/trust in external government and non-government actors
Research oversight and consultationSupporting, Advisory and Guiding Actors and Agencies
Dr J Muhammed Ado, Dr MJ Abdullahi & Prof. Okey Akpala Executive Director, Director (PRS) and
Senior Advisor, NPHCDA (GoN)Dr Pascal Mkanda WHO
Ms Melissa Corkum Unicef
Kano/Sokoto EOC Incident Managers, Bauchi SPHCDA GoN
Ms Marit van Strien, Dr Nancy Lowenthal USAID
Frank Mahoney, John Vertefeuille and team CDC
Mizan Siddiqi Executive Director, PHSS, local PI
Prof. Mahmud Khan University of South Carolina
Chris Morry, Hassan Jibiya & Barbara Rawlins Communication Initiative/JSI/JHU(PI)
Dr Sebastian Taylor Principal Investigator
LGA Chairs, Ward Focal Points, Primary Health Coordinators, Education Coordinators, Ward Heads, Settlement Heads, LGA, Ward and Settlement Imams and traditional leaders, health facility staff, participating households
Kano, Sokoto & Bauchi States
Research design process
• Originally designed as a small-n study (est. 200 households)• Sample significantly enlarged following programme partner consultations
– Learning: operationally-oriented research has to be responsive to programme partner perceived research needs
• Original design focus was polio-specific• Knowledge of and attitudes to routine immunisation included to reflect
both PEI end-game and host institution emphases– Learning: research design has to be responsive to long-run programme and post-
programme utility
• Purposive rather than randomised sampling – enhancing case comparison, but limiting generalisablity– Learning: there may be an operational preference for either population-level or area-
specific research, but less so for mid-range purposive sampling
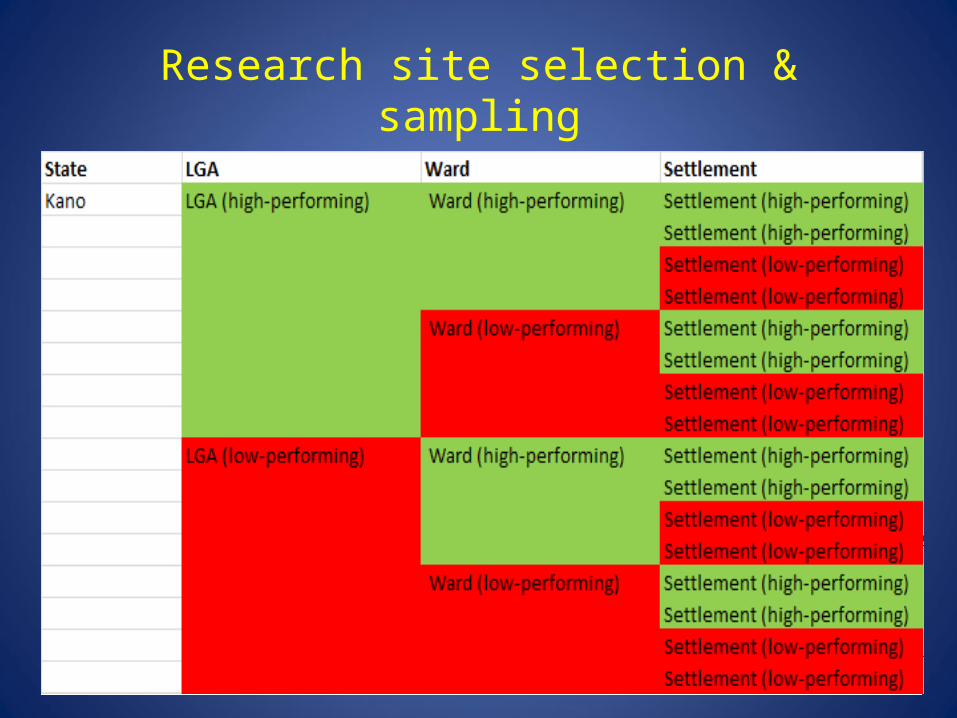
Research site selection & sampling
• We chose 3 of the 11 high-risk states (as defined by the national programme), to reflect a spread of geographic and socio-cultural characteristics– Kano (pop. 11m), Sokoto (pop. 4.2m), Bauchi (4.6m)
• Sample size was calculated for state populations of 5-10m (CI 95% with a design effect of 2), giving 480 households per state (1,440 households, by 2 respondents (male/female) = 2,880 observations; final sample after exclusions and substitutions: 1,653 households; 3,306 observations)2
– Paired LGAs and Wards were selected (‘high-performing’ (HP) and ‘low-performing’ (LP) using the national polio programme’s risk classification)
– Pairs of settlements (2 per Ward, HP/LP) were selected using programme data on rates of missed children (as available) supplemented by expert guidance by programme field staff
– In each settlement, 30 households were randomly selected– Learning: the absence or paucity of data on SIA coverage and incidence of missed
children below Ward level is – or should be - alarming

Research site selection and sampling
• We wanted to include rural, semi-urban and urban settlements in the survey (using Nigerian Government definitional criteria)
• Logistical and security considerations placed some constraint on selection of sites
• In the end, we were able to survey rural and urban settlements in Sokoto, rural and semi-urban settlements in Kano, and rural settlements in Bauchi
• Whilst this places constraints on cross-state comparison by sector, it allows for 3-state rural analysis as well as state-specific analysis of rural-urban and rural-semi-urban households and settlementsSokoto urban (283)
Sokoto rural (293)
Kano semi-urban (259)
Kano rural (276) Bauchi rural (542)

Survey household questionnaire
• The survey questionnaire was designed, in consultation with Nigerian programme partners, to gather data on household conditions and experiences in four domains of explanatory variable:– Demographic, socioeconomic and cultural characteristics of households– Perceptions of development conditions; participation in community development processes; quality of governance and ‘trust’
in external actors– Health experiences and health-seeking practices– Knowledge, experience of and attitudes to RI and PEI
• The survey incorporated four outcome variables:– Missed children in past SIAs & ‘propensity to refuse’ OPV in future– Approval/disapproval of PEI and RI
• The survey process was designed to avoid immediate association with polio and PEI

Household perceptions of the external world
• We included a number of questions to test respondents’ perceptions of ‘external actors’ (government, local traditional/religious leadership, NGO)
• Using a range of scenarios, including health and healthcare seeking, we asked respondents whom they would turn to, or expect help from, for:
a) Informationb) Problem-solving advice c) Support in the provision of key services
• The intention was to generate information on how, in relative terms, households view the legitimacy and/or reliability of external actors in a range of health and non-health contexts

Multi-variable indices
• During data analysis, we composed several indices incorporating multiple variables within a thematic area
• These included:– Index of gender agreement– Index of household ‘trust in government’– Index of household ‘religiosity’– Index of household ‘community participation’– Household health experience index &– Vaccine knowledge index
• Some of these have produced interesting results – but the composition of variables and interpretation of composite effect require further work

Research process and teams
• The final survey questionnaire– Included 60 questions (approx. 50-80 mins to administer)– Translated and back-translated for key terms (English-Hausa), pre-tested in Kano– Had ethical clearance (IRB) obtained from the Nigerian Health Research Ethics Committee (NHREC),
Johns Hopkins University, and University of East Anglia
• The survey targeted– 1 male respondent (HoH) and 1 female respondent (senior wife) per household– Through paired male/female survey teams (recruited from states to which subsequently deployed)– With 2-day training (1 desk-based, 1 field-based)– Data recorded on tablet (with completion requirement per page) reviewed by supervisors and uploaded
daily3
• Household survey complemented by a smaller ‘key informant’ survey at Settlement, Ward & LGA levels

Data-set completion and analysis
• Frequency, validity and coding checks were conducted on the data-set
• A second phase of household surveys was instituted to substitute for ineligible households excluded from the original data-set
• Data were uploaded to STATA for bivariate and multivariate logistic regression analysis (Prof. Mahmud Khan, University of South Carolina)
• Initial analysis incorporated data from all three states
• At preliminary findings presentation in Abuja (December 11-12, 2014), partners requested additional breakdown of analysis by state (for operational purposes), and by urban/rural

Preliminary findings

DemographicsVariable Rural (%) Semiurban (%) Urban (%)
HH with at least one child <1yr 54.5 51.3 44.2
Years in settlement: <10yrs 15.5 19.7 26.5
10-25yrs 36.4 46.3 42.8
25-50yrs 45 30.9 22.9
>25yrs 3.1 3.1 7.8
Knows where the nearest health facility is: 99.55 100 100
Time needed to go to the nearest health facility: <15mins 16-30 mins 31-60 mins >1 hour
32.820.138.29
49.835.113.51.5
64.730.44.60
Time needed to go to the nearest market: <15mins 16-30 mins 31-60 mins >1 hour
27.728.931.112.2
42.516.629.311.6
63.632.22.51.8
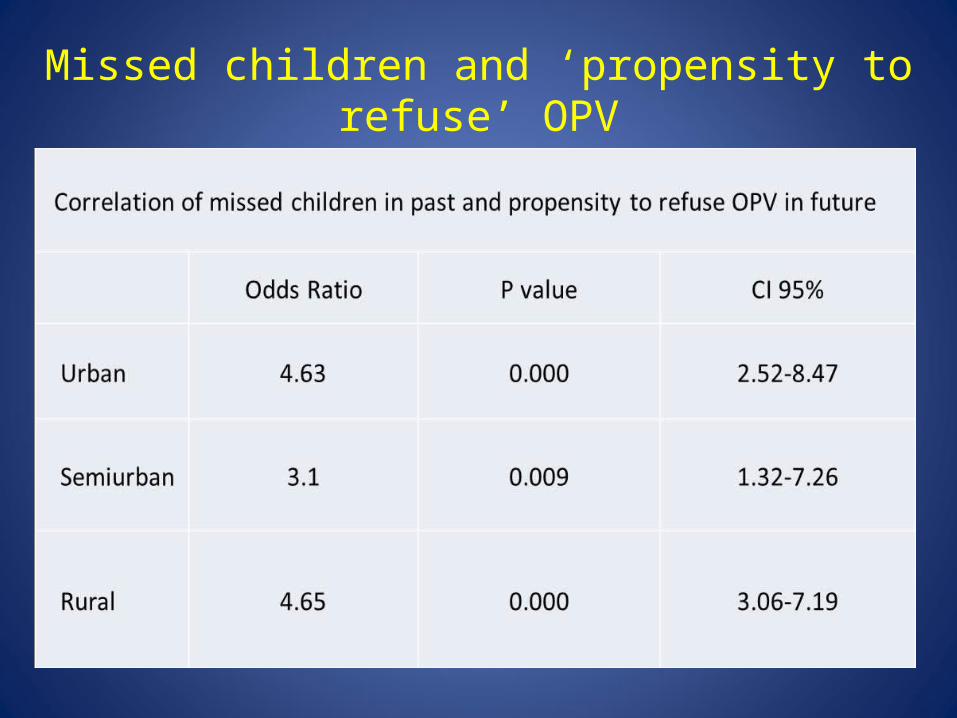
Missed children and ‘propensity to refuse’ OPV
• We found significant minorities of households reporting both missed children in past SIAs and propensity to refuse OPV in future
• We further found that households reporting missed children in past SIAs showed a systematic increase in risk of OPV refusal in the future
• This may indicate that a significant proportion of missed children are the result of continuous and by implication intentional household behaviour

Focusing on ‘propensity to refuse’
• Given the correlation between missed children and future risk of refusal, we focused analysis on understanding the characteristics of households manifesting propensity to refuse OPV

Clustering of OPV refusal risk
• We found that propensity to refuse OPV was unevenly distributed
• A fifth of the sample (13/60 settlements) accounted for 73.7% of households reporting risk of OPV refusal, and 53% of households reporting missed children
• Comparing this against our original selection of high-/low-performing settlements, we find substantial discrepancy
• Identifying ‘very high-refusal’ (VHR) settlements allowed us to complement household analysis with analysis of community-level factors

Urban as OPV refusal risk
• Propensity to refuse was highest in Sokoto (OR 1.84, p=0.000, CI 1.39-2.49), followed by Kano (OR 1.42, p=0.017, CI 1.06-1.9)– This is consistent with recent independent analysis of state and sub-state SIA coverage
and risk of ‘missingness’ by state and LGA (EMOD, 2013)
• Propensity to refuse OPV was higher among households in urban settlements (OR 3.17, p=0.000, CI 2.37-4.24)– Being in a semiurban settlement appears to reduce risk of refusal (OR 0.43, p=0.000, CI
0.29-0.64)

Factors

Health knowledge
• Knowledge of vaccines is strongly associated with reduced risk of OPV refusal, although it is knowledge of vaccines more widely (rather than specific knowledge of OPV) that appears to drive this effect
• For both households and settlements, a higher score on the ‘Vaccine Knowledge Index’ (e.g. women’s knowledge of vaccines, approval of immunisation practice, positive vaccine effects, and where to get vaccinated) is associated with reduced risk of OPV refusal
• But VKI operates differently in urban and rural contexts– In urban and semiurban settlements, wealth is the strongest correlate of VKI (urban: OR 9.8,
p=0.000, CI7.3-12.6; semiurban: OR 4.2, p=0.004, CI 1.35-7.05)– In rural settlements, wealth is replaced by female literacy (OR 6.8, p=0.000, CI 4.27-9.37) and
female participation in community-level meetings (OR 12.21, p=0.000, CI 9.79-14.62) as a determinant of VKI
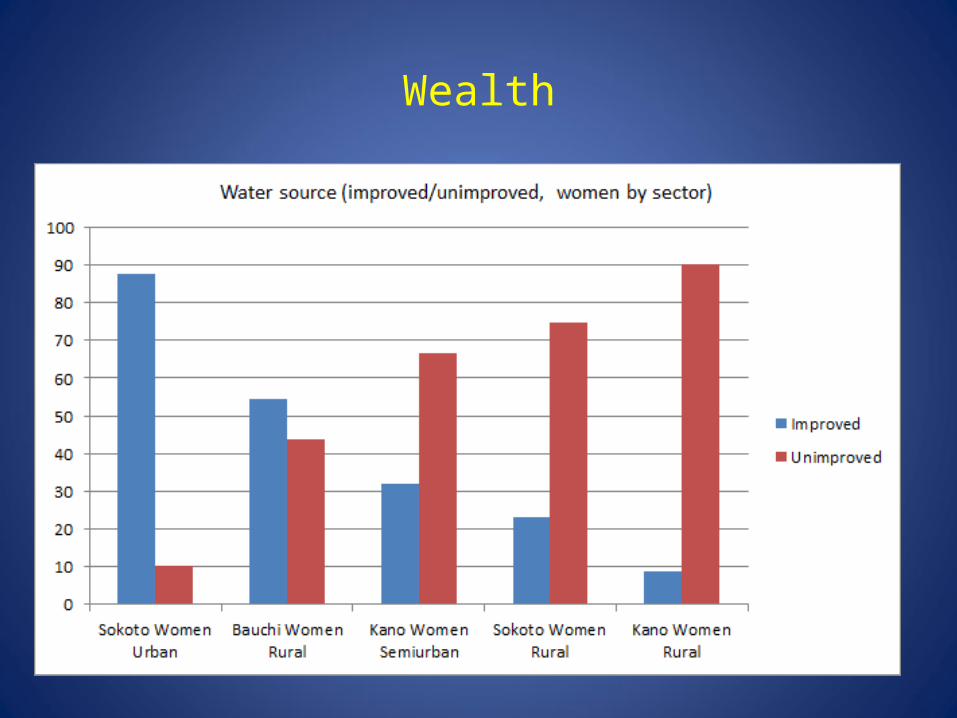
Wealth
• Wealth appears to be ambiguously associated with propensity to refuse OPV
• In a comparison of rural and urban/semiurban households, wealth reduces risk of OPV refusal in rural areas (OR 0.67, p=0.022, CI 0.47-0.94)
• But relative wealth appears to raise the risk of OPV refusal in very high-refusal (VHR) settlements – VHR households have greater asset holdings (e.g. fridge/freezer (t-stat 10.8), TV (t-stat
10.2)), better water and sanitation, are closer to market centres (<15mins t-stat 6.03) and to health facilities (<15 mins t-stat 7.8)
• This may be an effect of urban Sokoto• But it may also suggest that, in this sample, relative poverty is not, on its
own, a strong driver of OPV refusal risk

Education
• Neither ‘years of education’ nor ‘educational level’ shows significant relation to propensity to refuse OPV– The educational profile of households with missed children mirrors that of the general
sample in the same area
• Although female literacy reduces the risk of rural households refusing OPV (OR 0.59, p=0.015, CI 0.39-0.9), it marginally increases risk in very high-risk settlements (t-stat 2.9)
• VHR settlements are characterised by a range of educational attitudes which may express an underlying social conservatism (women’s preference for boys education (t-stat 2.23), men reporting madrassa education of eldest child (t-stat 6.7), men and women reporting own madrassa education (t-stats 9.49 & 4.83)

Religious identity
• We found no significant correlation between household religious or ethnic identity and propensity to refuse OPV– In indices of trust in (or reliance on) external actors, households consistently scored
‘traditional and religious leaders’ significantly lower than other options (e.g. ‘family’, ‘local leadership’, ‘government’)
– A preference for religious advice from religious authorities was associated with a reduced risk of OPV refusal comparing VHR and VLR settlements (OR 0.4, p=0.000, CI 0.26-0.6)
• Respondents – equally in VHR and VLR settlements – appear to demarcate, quite clearly, the role of religious leaders in providing religious information, with a distinctly lesser role in other areas including health
Radio
TV
Mob/IT
Print/crier
Family
Neighbour
Rel Leader
Ward/LGA
State/Nat.
Int. Orgs

Perceptions of government legitimacy
• We hypothesised that household perceptions of (trust in) government may be an important influence on attitude to polio vaccination – Perception of government as ‘most effective provider’ of wat/san, health and security
services was systematically associated with increased risk of OPV refusal among VHR settlements
• This may indicate that disappointed expectations of government as wider service provider to some degree drive antagonistic views of PEI
• But when asked whom they would turn to for advice in common household problems, respondents appear to differentiate between some areas (mainly disputed material assets) in which government is preferred, and others (mainly matters of internal domestic management) in which it is not
• Health is an area in which family self-reliance almost entirely eclipses a role for government
• This pattern is amplified in VHR settlements
Family itself
Settlement
Rel/trad
Ward
LGA
State
Federal
International
Family itself
Settlement
Rel/trad
Ward
LGA
State
Federal
International
Family itself
Settlement
Rel/trad
Ward
LGA
State
Federal
International

Community engagement
• Comparing VHR and VLR settlements, community participation by women is one of the strongest factors mitigating risk of OPV refusal
• Strengthening opportunities for women’s community participation may be an important strategy for programmes such as polio
• In particular in areas (like health) where government intervention may be viewed as inadequate or inappropriate at household level

Conclusions
• Out data suggest a systematic relationship between households with missed children and risk of future OPV refusal – chronic and intentional
• Refusal appears clustered within rural and urban settlements, but with a concentration in urban Sokoto
• Health knowledge is important to reduce risk (though not limited to polio), but it appears to depend on different mechanisms in rural and urban areas
• For our sample, OPV refusal is not characterised by rural poverty and illiteracy – but more by relatively well-off, educated urban households
• Conservative attitudes (to education; to the role of government, including in health; to women’s participation in public/community activity) may be important drivers of urban household OPV refusal risk
• Working with, rather than attempting to ‘convert’, such attitudes – e.g. through alternative modes of vaccine provision that work around a conservative tendency to protect the domestic space – may be advantageous in areas such as urban Sokoto

Thanks

Annexes

Reference annex
1 See, e.g., Schneidera & Wagemann (2010); Berg-Schlosser, De Meur, Rihoux & Ragin, 2009; Hellstrom & Seura, 2001; Ragin, 19944 Ado, Etsano, Shuaib et al., 2014; Mohammed, Sabitu, Nguku et al., 2014; Ayoola Fatiregun A & Emmanuel Etukiren E, 2014; Maharani A & Tampubolon G, 2014; Larson H, Jarrett C, Eckersberger E et al., 2014; Canavan M, Sipsma H, Kassie G et al., 2014; Okafor IP, Dolapo DC, Onigbogi MO & Iloabuchi IG, 2014; Funmilayo A (nd); Bisiriyu L & Ojewumi T, 2014; Calhoun L, van Eijk A, Lindblade K et al., 2014; Hu Y, Shen LZ, Guo J & Xie SY, 2014; Gram L, Soremekun S, ten Asbroek A et al., 2014; Ibuka Y, Li M, Vietri J et al., 2014; Yaqub O, Castle-Clarke S, Sevdalis N & Chataway J, 2014; Bbaale E, 2013; Abidoye A & Odeyemi K, 2013; Siddiqui NT, Owais A, Agha A et al., 2013; Wiysonge C, Uthman O, Ndumbe P & Hussey G, 2013; Sann Chan Soeung, Grundy J, Duncan R et al., 2013; Merten S, Schaetti C, Manianga C et al., 2013; Abebaw D, 2013; Sadique MZ, Devlin N, Edmunds WJ, Parkin D, 2013; Osazuwu-Peters, 2011; Olofuwote, 2011; Renne, 2010; Yahya, 2007; Chaturvedi et al., 2011; Cockcroft A, Andersson N, Omer K et al., 2009; Jheeta M & Newell J, 2008; Nath B, Singh J V, Awasthi S et al., 2007; Anand S & Bärnighausen T, 2007; Munthali A, 2007; Gauri & Khaleghian, 2002; Streefland, 2002.
Technical annex
• 2 The formula used to calculate the sample size for large population (population >10,000): n0 = {p(1-p)z2/e2}f where p=0.33, z=1.96 (5% level of significance), e=0.05, f=1.
• 3 The software for data collection Ii an android application developed using Android SDK and Basic4andrioid. The application data base is in SQL Lite in tablet and online web data base data is in MySQL. The data base exported and backed up in CSV format. The web interface is made using PHP/Java Script/jQuery language, for chart High Chart and for mapping Google Map API. The Specification of the tablet is Android OS 4.1 with 10.1" screen.