
Understanding Dialysis Event (DE) Surveillance &...
36
1 2 Connecticut Department of Public Health Association for Professionals in Infection Control and Epidemiology Network of New England Centers for Disease Control and Prevention Understanding Dialysis Event (DE) Surveillance & Reporting in National Healthcare Safety Network (NHSN) Jenny Kitsen Executive Director Network of New England 3
Transcript of Understanding Dialysis Event (DE) Surveillance &...

1
2
Connecticut Department of Public HealthAssociation for Professionals in Infection Control and Epidemiology
Network of New EnglandCenters for Disease Control and Prevention
Understanding Dialysis Event (DE)Surveillance & Reporting in National Healthcare
Safety Network (NHSN)
Jenny Kitsen
Executive Director
Network of New England
3

4
Unique CollaborationConnecticut Department of Public Health, Emerging Infections ProgramRichard Melchreit, MD., Healthcare Associated Infections Program Coordinator has awarded Network of New England a contract to do a provider level data validation, expand the number of providers enrolled in NHSN and conduct educational activities on lessons learned in reporting dialysis events
Association for Professionals in Infection Control and Epidemiology (APIC) promoted and coordinated this webinar including the availability of CEU’s.
Network of New England has coordinated the content of this webinar and has incorporated lessons learned from site visits conducted for data validation and will share that experience in this Webinar
Centers with Disease Control and Prevention (CDC) Dr. Priti Patel and Alicia Shugart, M.A ., serve on the New England Dialysis Collaborative on Healthcare Associated Infections Regional Advisory Committee and provide technical expertise and consultation. CDC will provide an overview of reporting requirements in NHSN
MIPPA Medicare Improvements for Patients and Providers Act 2008
Section 153(c) ESRD Quality Incentive Program (QIP)
• Select Measures• Establish performance standards• Specify a one-year performance period • Develop method for assessing each facility’s total
performance on the measures relative to performance standards
• Apply an appropriate payment reduction to facilities that do not meet or exceed the established total performance score
• Publicly report results through websites and certificates posted at facilities
5
Medicare Dialysis Quality Incentive Program Overview
6
• Withholding Dialysis Payment to Providers Begins January 2012
• Provider performance for payment year 2012 has been evaluated inyear 2010
• On December 15th 2011 the provider performance score certificate was released by Centers for Medicare and Medicaid Services (CMS) forposting by dialysis provider
• Different Performance measures are used for payment formula for each year

QIP Performance Report Payment Reduction Year
Year 2010
Provider data from Medicare claims in 2010•URR > 65%•Hgb < 10g/dL•Hgb > 12g/dL
Weighted value is 50% for < 10g/dL25% each for other two measures
1/1/2012 – 12/31/2012
Max points 30Payment reduction scale starts at below 26 points to 0 points with maximum of 2% withheld.
Performance Year 2010
7
QIP Performance Report Payment Reduction Year
Year 2011
Provider data from Medicare claims in 2011
•URR > 65%•Hgb > 12 g/dL
Weight value 50% each
1/1/2013 – 12/31/2013
Maximum points 30
Payment reduction starts at 29 points to 0 points for max of 2% withheld.
Performance Year 2011
8
Performance Year 2012
QIP Performance Report Payment Reduction Year
Year 2012Provider data from Medicare claims in 2012
Clinical measures•Hgb > 12 g/dL•URR > 65%•Vascular access TypeThree reporting measures•National Health Safety Network (NHSN) Dialysis Event (DE)•Patient experience of care (ICH CAHPS)•Mineral metabolism
CMS has not determined the achievement thresholds for these measures. That will be released before 1/31/2012
1/1/2014 – 12/31/2014
Maximum points 100
•The 3 clinical measures will be equally weighted and add up to 90% of the total performance score•The 3 reporting measures will be equally weighted and add up to 10% of the total performance score
9

• Completion of enrollment in the NHSN and successful training (digital certificate from CDC), submission of a minimum of 3 consecutive months of data to the NHSN according to the Dialysis Event Protocol during the performance period: 1/1/2012 to 3/31/2013- NHSN DE reporting
• Attestation by the provider/facility at the end of the performance period that they have successfully administered the ICH CHAPS survey during the proposed performance period
• Whether the provider/facility monitored the serum phosphorus and calcium levels of patients treated by the provider/facility throughout the duration of the performance period
Details of Three Reporting Measures For Performance Year 2012
10
Importance of Early Participation in NHSN
• National priority of the government to reduce infections
• Routine surveillance establishes baseline identification of dialysis events– IV Antimicrobial start
– Positive blood cultures
– Pus, redness or increased swelling at access site
11
Early Risk Assessment and Protective Intervention will….
• Improve patient care
• Reduce hospitalization
• Reduce Antimicrobial use
• Avoid reduction in Medicare payment to provider
• Contribute to positive performance reports (public reporting at the state, federal level)
12

Dialysis Event Surveillance and Reporting in NHSN
Priti Patel, MD, MPHAlicia Shugart, MA
Division of Healthcare Quality PromotionCenters for Disease Control and Prevention
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention
Performing Surveillance
• Purpose: – Use for action; improve the health of
patients– Provide important national data, including
benchmarks
• Examples of local use– Problem detection– Prevention, evaluation of interventions
Problem Detection
• Six outpatient hemodialysis facilities in Idaho conducted prospective surveillance for vascular access infections
• Stratified rates by vascular access type• Observed an increase in vascular access
infections related to tunneled catheters• Connected it to clinical observations• Took action
Hannah EL, et al. Infect Control Hosp Epidemiol 2002;23:538-41

Rates of Vascular Access Infection, Six Facilities, Jan 1998 – Mar 2001
Pre-Outbreak Jan 1998 – Jun
1999
OutbreakJul 1999 – Jan
2000
Post-Outbreak Feb 2000 – Mar
2001
All vascular access types
4.1 5.8
Tunneled catheters only
8.9 18.1
Rates expressed per 1,000 dialysis sessions
Hannah EL, et al. Infect Control Hosp Epidemiol 2002;23:538-41
Rates of Vascular Access Infection, Six Facilities, Jan 1998 – Mar 2001
Pre-Outbreak Jan 1998 – Jun
1999
OutbreakJul 1999 – Jan
2000
Post-Outbreak Feb 2000 – Mar
2001
All vascular access types
4.1 5.8 3.3
Tunneled catheters only
8.9 18.1 10.8
Rates expressed per 1,000 dialysis sessions
Hannah EL, et al. Infect Control Hosp Epidemiol 2002;23:538-41
Outbreak of Bloodstream Infections (BSIs)
• Hospital-based outpatient hemodialysis facility in Illinois
• Outbreak occurred after ownership changed from hospital to private medical group– Biweekly infection control monitoring provided by the
hospital stopped
• “Fortunately” the unit continued to send blood cultures to the hospital microbiology laboratory�outbreak discovered
Price CS, et al. Infect Control Hosp Epidemiol 2002;23:725-9

BSI Rates Relative to Change in OwnershipJan 1999 - Jan 2000Rate = 0.7 per 100 pt-months
Feb 2000 - Apr 2001Rate = 4.2 per 100 pt-months
Price CS, et al. Infect Control Hosp Epidemiol 2002;23:725-9
Findings & Actions
• Under hospital ownership, hospital infection preventionist – Performed surveillance, monitored positive blood
culture results, observed aseptic technique
• Intervention included staff education, changes in catheter care practice
Price CS, et al. Infect Control Hosp Epidemiol 2002;23:725-9
Surveillance as an Intervention
• Dialysis unit in London implemented CDC dialysis surveillance; described their experience over 18 months
• Tracking rates and feeding back data to staff resulted in reductions in – Access-related BSI– Antibiotic usage
George A, Tokars JI, Clutterbuck EJ, et al. BMJ 2006; 332:1435-1439

Access-Related Bacteremia
George A, Tokars JI, Clutterbuck EJ, et al. BMJ 2006; 332:1435-1439
Observations
• “Surveillance raised awareness and provided a cornerstone for improved infection control and line care involving all staff of the dialysis unit.”
• “The data feedback generated unit led programs of risk reduction and infection control.”
George A, Tokars JI, Clutterbuck EJ, et al. BMJ 2006; 332:1435-1439
Importance of…
• Conducting prospective surveillance– Utilizing consistent approach to
measurement– Systematically analyzing the data– Utilizing the data in the unit
• Correlate findings with what is happening in the unit, including relevant practices
• To prompt interventions and assess their effectiveness
• Give staff feedback

Learning Objectives
� Describe the Dialysis Event Protocol
� Review instructions for completing forms
� Explain NHSN definitions and key terms
� Provide examples of reporting methodology
� Address Frequently Asked Questions (FAQs) about Dialysis Event surveillance
Key Term - Surveillance
� Public health surveillance is the ongoing, systemat ic collection, analysis, interpretation, and dissemination of data regarding health-related events for use in public health action to reduce morbidity and mortality and improve health
DIALYSIS EVENT PROTOCOL
What is the Dialysis Event Protocol?
� The Dialysis Event Protocol is a document that provides instructions for reporting
� Includes� Surveillance population
� Definitions of key terms
� Required data reporting elements and reporting frequency
Reporting Requirements
� All users are required to read the Dialysis Event Protocol to become familiar with instructions, definitions and procedures
� Data are collected on forms according to the protoc ol� Report Monthly Patient Census (denominator data) within 30 days
of the end of the month
� Report Dialysis Events (numerator data) if they occur, within 30days of the end of the month
� Collecting data uniformly is essential to meaningfu l surveillance
Data Reporting Requirements
1. Outpatient Dialysis Center Practices Survey� Completed upon enrollment and annually thereafter
2. Monthly Reporting Plan� Indicate what NHSN surveillance your facility will do each month
3. Denominators for Outpatient Dialysis form� Completed once monthly
4. Dialysis Event form� Completed monthly, one for each dialysis event that occurs

Data Collection
� All resources are available on the public NHSN website: www.cdc.gov/nhsn/� Protocol & forms
� NHSN is accessed through a secure website: https://sdn.cdc.gov� Data entry/reporting
Data Reporting
INSTRUCTIONS FOR FORMS
Outpatient Dialysis Center Practices Survey
� Completed during enrollment in NHSN and annually thereafter
� Includes questions about staff and patients during the first week of January� It is recommended to complete the survey in January each year
� Available on the Dialysis Event homepage� http://www.cdc.gov/nhsn/forms/57.104_PSOutptDialysisSurv_BL
ANK.pdf

Outpatient Dialysis Center Practices Survey
Monthly Reporting Plan
� Indicates what Patient Safety Component surveillance modules your facility intends to do:� Device-Associated Module >> Dialysis Event “DE”
� If not doing surveillance for a specific month, sel ect ‘No NHSN Patient Safety Modules Followed this Month’ on the Monthly Reporting Plan
� You can submit up to one year of Monthly Reporting Plans in advance
Choose only if your facility is NOT doing any surveillance this month

Indicating “DE” on your reporting plan each month helps you to
report correctly.
Vascular Access Definitions
� Fistula: A surgically created connection between an artery and a vein
� Graft: A surgically created connection between an artery a nd a vein created with implanted synthetic tubing
� Tunneled Central Line: Central venous catheter that travels a distance under the skin from the point of insertion before terminating at or close to the heart or one of the great vessels
� Nontunneled Central Line: Central venous catheter fixed in place at the point of insertion and travels directl y from the skin entry site to a vein and terminates close to t he heart or one of the great vessels
� Other Access Device: Includes hybrid access devices (e.g., HeROTM vascular access device), ports, and any other acces s devices not meeting above definitions
Use of trade names and commercial sources is for identification only and does not imply endorsement.
Infection Risk by Vascular Access
� Risk of infection varies by vascular access type:
Arteriovenous fistulasArteriovenous graftsOther access devices (e.g., hybrids)Tunneled central linesNontunneled central lines
� NHSN data are stratified by vascular access type
LOW RISK
HIGH RISK

Denominators for Outpatient Dialysis form
� Report all maintenance hemodialysis outpatients treated at your facility on the first 2 working day s of the month, stratified by 5 vascular access types
� Count each patient only once� If they have more than 1 vascular access, count that patient
under their highest infection risk access only
� Consider ALL vascular accesses present, not just those being used for dialysis
� If a patient is present on both working days (e.g., for a make-up appointment) do not count them twice
� Complete this form once per month
Dialysis Events
� Dialysis events reported to NHSN by users� IV antimicrobial starts
� Positive blood cultures
� Pus, redness or increased swelling at the vascular access site
� Dialysis events calculated in NHSN from reported data� Local access site infection
� Access-related bloodstream infection
� Vascular access infection

Dialysis Event Form
� Monitor all maintenance hemodialysis outpatients who are treated at your facility at any time during the month for dialysis events:� IV antimicrobial start
� Positive blood culture
� Pus, redness, or increased swelling at the vascular access site
� Complete a Dialysis Event form for each patient tha t has a dialysis event
Dialysis Event Form
� Any patient who receives maintenance hemodialysis treatment at your facility is included in dialysis event reporting� Even if they were not counted on the denominator form
� Include transient patients who have a dialysis event while receiving hemodialysis treatment at your facility
Dialysis Event Form
� Patient demographics
� Risk Factors
� Dialysis Event type(s) & details
� Problems/ symptoms
� Outcomes

Dialysis Event Date
Dialysis Event Date Criteria
IV antimicrobial start Date of first outpatient administration
Positive blood culture Date specimen was collected
Pus, redness, or increased swelling at vascular access site
Sign/symptom onset date
Combination Earliest date of the three types
Reporting Zero Dialysis Events
� If no dialysis events occurred during a month, sele ct “Report No Events” on the Denominators for Outpatient Dialysis form in NHSN� No IV antimicrobial starts
� No positive blood cultures
� No pus, redness, or swelling at the vascular access site
� This indicates that the numerator (dialysis events) is equal to zero for this month/year
� The denominator (patient census information) is sti ll reported
Select“Report No Events”
to report zero dialysis events for the month
DEFINITIONS AND KEY TERMS
Dialysis Event Type: IV Antimicrobial Start
� Report all outpatient IV antimicrobial starts� Include all IV antibiotics and antifungals, not just vancomycin
� Include starts that occur for any reason and duration, not just vascular access problems
� Exclude antivirals
� IV antimicrobials must be stopped for more than 21 days and then restarted to be considered a new event� If IV antimicrobials are stopped for ≤ 21 days it is still the same
event
Dialysis Event Type: Positive Blood Culture
� Include all positive blood cultures from specimens taken as an outpatient or within one (1) day after a hospital admission� Even if the patient does not receive treatment
� Even if the infection is not related to dialysis treatment
� If you have > 1 positive blood culture, they must b e more than 21 days apart to be considered separate dialysis events

Suspected Source of Positive Blood Culture
� “Vascular access ” if there is objective evidence of vascular access infection and it is thought to be t he source
� “A source other than the vascular access ” if another source is thought to be the source and either:� culture from another site has the same organism as the blood � clinical evidence of infection at the site, but site is not cultured
� “Contamination ” if organism is thought by the physician, Infection Preventionist, or head RN to b e a contaminant
� “Uncertain ” only if there is insufficient evidence to decide among the 3 previous categories
Positive Blood Culture Microorganisms
� On the back of the Dialysis Event form, report the microorganisms for positive blood cultures� Suggestion: attach microbiology lab report to paper form
� List up to 3 microorganisms (in order of importance )� Usually order of importance is indicated on the laboratory report
� For each microorganism, include antimicrobial susceptibility information� i.e., susceptible, resistant, intermediate, or not tested
� Only certain bug/drug combinations are required
Dialysis Event Type: Pus, Redness or Increased Swelling at the Vascular Access Site
� Report all episodes of one or more symptoms of pus, redness or increased swelling at a vascular access site� Even if the patient does not receive treatment
� Always report pus
� Report redness or swelling if they are more than expected and suspicious for infection at the time of onset
� There must be 21 or more days between the onset of a first and second episode of pus, redness, or increased swelling at a vascular access site to be considered separate dialysis events

21 Day Rule
� There must be 21 or more days between dialysis events of the same type
� Purpose of the rule is prevent over-reporting of wh at is likely the same patient problem
21 Day Rule Example
� A patient has two positive blood cultures within 21 days as a result of a bloodstream infection on January 1 st and January 9 th
� Report 1 dialysis event
� Event date is January 1st
� The patient has a third positive blood culture on February 20 th
� Report a second dialysis event
� Because event date of this new positive blood culture is 21 or more days after the last reported positive blood culture
Dialysis Event Problems & Outcomes
� Specify problems associated with the dialysis event� Fever, chills or rigors, drop in blood pressure
� Wound (not related to the vascular access) with pus or increasedredness
� Cellulitis
� Pneumonia or respiratory infection
� Other problem
� Specify outcomes associated with either the dialysi s event or problems� Hospitalization
� Death
Dialysis Event Combinations
� 1 Dialysis Event report may have multiple parts, combining:� IV antimicrobial start
� Positive blood culture
� Pus, redness or increased swelling at vascular access site
� For example, if a positive blood culture is the rea son that a patient is treated with IV antimicrobials, t his is part of the same group of events and they are reported together
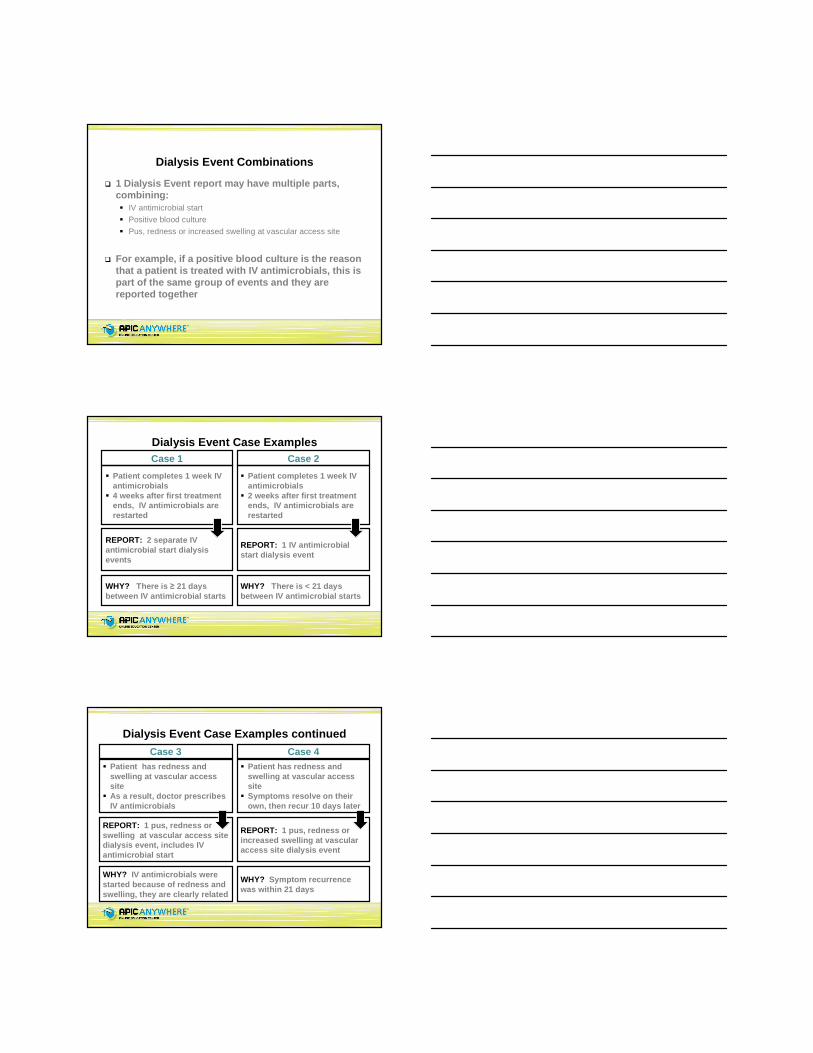
Dialysis Event Case Examples
WHY? There is ≥ 21 days between IV antimicrobial starts
� Patient completes 1 week IV antimicrobials
� 4 weeks after first treatment ends, IV antimicrobials are restarted
Case 1
REPORT: 2 separate IV antimicrobial start dialysis events
WHY? There is < 21 days between IV antimicrobial starts
� Patient completes 1 week IV antimicrobials
� 2 weeks after first treatment ends, IV antimicrobials are restarted
Case 2
REPORT: 1 IV antimicrobial start dialysis event
Dialysis Event Case Examples continued
REPORT: 1 pus, redness or swelling at vascular access site dialysis event, includes IV antimicrobial start
WHY? IV antimicrobials were started because of redness and swelling, they are clearly related
REPORT: 1 pus, redness or increased swelling at vascular access site dialysis event
WHY? Symptom recurrence was within 21 days
� Patient has redness and swelling at vascular access site
� As a result, doctor prescribes IV antimicrobials
Case 3� Patient has redness and
swelling at vascular access site
� Symptoms resolve on their own, then recur 10 days later
Case 4

Dialysis Event Case Examples continued
REPORT: 1 Dialysis Event, with positive blood culture and includes IV antimicrobial start
WHY? Blood was drawn before antimicrobials started, both relate to same infection
� Blood is drawn on Monday� Tuesday: IV antimicrobial
start � Wednesday: blood culture
results are positive
Case 5
� Patient has symptoms of a bloodstream infection:
REPORT: 1 positive blood culture Dialysis Event, with hospitalization outcome
WHY? PBC sample was drawn within a day of admission. Both relate to same infection.
� Patient is hospitalized� 4 hours after admission,
blood is drawn, culture results are positive next day
Case 6
REPORT: Pus, redness, or increased swelling at the vascular access site Dialysis Event with positive blood cult ure
PBC suspected source: vascular access
WHY? There is objective evidence of infection at vascula r access site
� Patient’s vascular access site has pus, redness and swelling� Blood culture grows Staphylococcus aureus
Case 7
Dialysis Event Case Examples continued
Dialysis Event Case Examples continued
REPORT: Pus, redness, or increased swelling at vascular access site Dialysis Event with positive blood cult ure
PBC suspected source: vascular access
WHY? Objective evidence of infection at vascular access site exists. Different organisms in blood & wound: canno t attribute positive blood culture to a ‘source other than vasc ular access’
� Patient’s vascular access site has pus, redness and swelling� Blood culture grows Staphylococcus aureus� Visibly infected leg wound grows Enterococcus
Case 8

Dialysis Event Case Examples continued
REPORT: Positive blood culture
Suspected source: A source other than vascular access site
WHY? Evidence of infection at wound site, no evidence at VA site. Both wound and blood grow same organism.
� Patient’s leg wound has pus, redness and swelling� Vascular access looks normal� Wound culture: Staphylococcus aureus� Blood culture: Staphylococcus aureus
Case 9
Dialysis Event Case Examples continued
REPORT: Positive blood culture
Suspected source: contamination
WHY? Only 1 of 2 blood draws was positive & it was a com mon skin organism. Doctor was asked for interpretation and indicated the positive was the result of contaminat ion.
� Patient reports chills, but no fever� Patient has 2 blood draws � 1 draw grows coagulase-negative staphylococci � Patient’s symptoms resolve and doctor does not trea t patient
Case 10
Reporting Difficult Dialysis Events
� Refer to the Protocol and Tables of Instructions fo r reference
� If you are unsure how to report a Dialysis Event, g et the opinion of the physician, infection preventioni st, or nurse manager
� Additional assistance is available through the NHSN Helpdesk at [email protected]

FREQUENTLY ASKED QUESTIONS ABOUT DIALYSIS EVENT REPORTING
FAQs – Who is Monitored Each Month
Q: Does the dialysis event surveillance population include pediatric patients?� Yes, include all hemodialysis outpatients in dialysis event
surveillance, including pediatric patients. Date of birth is a required event field, so age is captured for each dialysis event.
Q: Does the dialysis event surveillance population include peritoneal dialysis patients?� No, the dialysis event surveillance population includes only
maintenance hemodialysis outpatients.
FAQs – Who is Monitored Each Month
Q: A patient was scheduled for hemodialysis on one of the first two working days of the month, but missed the appointment. Is he or she still counted on the Denominators for Outpatient Dialysis form?� No, only count patients who actually received hemodialysis
treatment at your facility during the first two working days of the month on the Denominators for Outpatient Dialysis form
� Patients who were not dialyzed on these days are not counted, regardless of the reason they missed the treatment

FAQs – Who is Monitored Each Month
Q: A patient missed treatment on the first two wor king days of the month and so was not counted on the Denominators for Outpatient Dialysis form. If he ha s a dialysis event that month, is it reported?� Yes, all outpatients that receive maintenance hemodialysis at
your facility any time during the month should be monitored for dialysis events
� These dialysis events are reported regardless of whether or not the patient was counted in the denominator for that month
FAQs – Vascular Accesses
Q: Are vascular accesses that are not being used f or hemodialysis still included for Dialysis Event reporting (e.g., a port for chemotherapy)?� Yes, vascular accesses that are not being used for hemodialysis
are included in Dialysis Event surveillance
� Dialysis Event form: indicate all of the patient’s vascular accesses
� Denominators for Outpatient Dialysis form: count the patient under the highest infection risk vascular access type that he has
FAQs – Antimicrobials
Q: If the type of IV antimicrobial being used is switched with another type to treat the same infection, is this a new IV antimicrobial start? � No, a change in the type of IV antimicrobial being used to treat
the same infection does not constitute a new dialysis event.
FAQs – Positive blood cultures
Q: The patient lives in a long-term care facility. Do blood cultures drawn there meet the criteria of ‘specimen collected as an outpatient’?� Any specimen collected outside of an acute care setting
(hospital) is reported if positive
� A long-term care facility, skilled nursing facility, or nursing home is considered an outpatient facility so any positive blood cultures collected in this setting are reportable.
� Note: a long-term care facility is different from a long-term acutecare facility, which is an inpatient setting
FAQs – Wounds
Q: Are wound cultures reported?� No, wound cultures are not reportable for dialysis event
surveillance� Some wound information is collected, but not culture information
Necessary Preparation for Reporting
� Familiarity with the Dialysis Event Protocol, especially definitions, as well as the reporting instructions, and data collection forms
� Determine what processes might need to be implemented in order to collect the data consistent ly and completely, according to the Dialysis Event Protocol
� Enroll in NHSN� Step by step instructions, specific to dialysis facilities, are online
� http://www.cdc.gov/nhsn/dialysis/cms-dialysis-enroll-steps.html

Questions?
NHSN [email protected]
Priscilla Laliberty, RD
HAI Project Coordinator
ESRD Network of New England
Validation of Your Information is Important!
Prevent Over And / Or Under Reporting
77
Correct Way To Collect And Report Denominator (Census)
Patients must be physically present for their maintenance Hemodialysis treatment on the first two working days of the month to be counted in the Denominator “Census”:
• Include transient patients
• Include pediatric patients
• Exclude hospitalized patients
• Exclude peritoneal dialysis patients
• Exclude acute dialysis patients
• Exclude patients that skip or otherwise miss their treatment
• Excludehome hemodialysis patients
78
Denominator Count (con’t): This is different from Your “Fistula First Count”
More Rules:• Count each patient only once: If a patient is present on both working
days (e.g., for a make-up appointment) do not count them twice
• If they have more than 1 vascular access, count that patient under their highest infection risk access only, (whether or not in use at the time of the count); stratified by 5 vascular access types.
[HIGHEST RISK] Non tunneled Central Line > Tunneled Central Line > Other Access Device > Graft > Fistula [LOWEST RISK]
Report your denominator once per month, regardless of whether or not any dialysis events occurred.
79
Basic Principles to Prevent Over and/or Under Reporting – Use your Resources!
• Clarifying knowledge of criteria – Check the Dialysis Event Protocol for criteria details if you are not sure the situation is a Dialysis Event or not.
• Discussion of situations and definitions – with the details in hand, talk to the Medical Director as a clinical consult only. To determine whether it is an Event or Not, talk to surveillance experts in NHSN!
• And, When in doubt• Go to “Frequently Asked Questions” on NHSN website Dialysis Reporting FAQs
• Send email to NHSN [email protected] will help you decide
80
Things I have learned! Nothing that looks simple is!
• When dealing with people, “interpretation” means there are many ways of understanding what is said. More communication clarifies the situation. Statements should be “simple,” then ask what people heard you say. When everyone hears the same thing… it may be a clear concept!
• “Frequently asked questions” from the NHSN homepage can help in keeping the “interpretations” the same from unit to unit!
81

A Very Important RULE! For “Numerators”
21 Day RULE
• Applies to all 3 events reported in NHSN
• “One event ends”if 21 days have passed from the end of the first event to start of the second event
If the difference is not 21 days between the end of the first event to start of the second event, it is the same event
82
• IV antimicrobial start (Anti-bacterial and Anti-fungal)
• Positive blood culture (All positive blood cultures)
• Pus, redness, or increased swelling at the vascular access site
Pay attention to the 21 day rule to determine if it is a new event or the same event!
“Numerators” are Dialysis Events as per NHSN criteria
83
IV Antimicrobial Therapy
• If ORAL antimicrobials are used, IGNOREthem. Only IV antimicrobials for NHSN surveillance
• Pay attention to start and end dates; look at previous antimicrobial. If 21 days are not there between end of one antimicrobial event and beginning of another, it is nota NEW event
• If started on IV antimicrobial in the hospital, your start date of an Event is when they came to you and you continued the antimicrobial prescribed in hospital (outpatient) –and these have to be reported
84
Positive Blood Cultures
• The draw date of a blood culture, if positive, is the “Dialysis Event date”(unless other criteria happened first.)
• If the Blood Culture is drawn within 1 calendar day of a hospitalization admission, report it. If you hear about this later, “edit” it into the Dialysis Event
• If the result of the Blood Culture is negative/no growth DO NOT REPORT IT
• If it is “contaminated” you must report. (See the Dialysis Event Protocol for instructions from NHSN). Follow your laboratory procedure for blood draws. Good technique will reduce result of “contamination”. This will improve your rates!!
85
Pus, Redness, or Increased Swelling at the Vascular Access Site
• Try to make this as objective as possible
• “Red” counts… “Pink” no… unless continued documentation implies possible infection
– Try to have the staff agree upon “red” or “pink”– Slightly red – yes; very pink – no. Consistency is best
• If what you see is “expected,” it is not an event. Example: access work done 2 days ago, thus, some swelling and redness at stitches as healing; same scenario 10 days after , probably not “as expected”so is an event!
86
Pus, Redness, or Increased Swelling at the Vascular Access Site (con’t..)
• If Pus is present at the Catheter site and a wound culture is taken it is an event… because pus was documented. If a blood culture is done and IS POSITIVE check the draw date and use whichever of these came first. Wound culture is not part of theevent, however would be noted under “problems”
• If pus is noted at a leg wound it is not an event (unless blood cultures are done and they are positive)
• If a hand is swollen on the AVF arm, it is not an event… only if at the access site – unless other criteria are present
87

YOU ARE NOT ALONE FIGURING THIS OUT! USE YOUR RESOURCES… DO IT RIGHT!
send an email to NHSN. Write “Dialysis Event” and the scenario. They will help you figure it out!
88
If in doubt……
You can EDIT!• If more information comes to you after you began a Dialysis Event in
NHSN… you can EDIT it!
• If you learn about a positive blood culture from the hospital admission, you can fix it by using that date!
• Fixing an Event date can impact on the next Event if there is one… (21 day rule)
• If you reviewed denominator information and needed to fix your entry…”Edit it” …
Save it when you edit it! Save button is at the very bottom.
Right is good!
89
It is Important to Check the Validity of Your Data as You Go From Month to Month!
• To prevent over and under reporting it is important to follow all of the criteria
• Look at beginning and end of each event in terms of dates. This will help with the 21 day rule
90
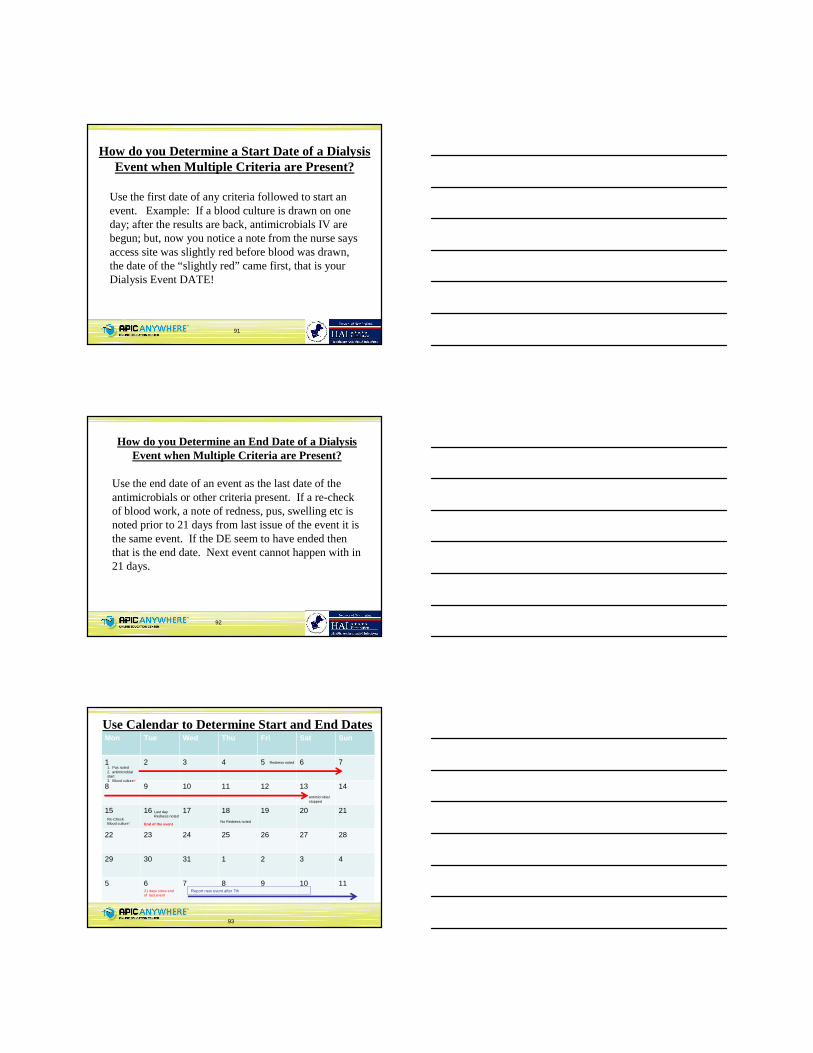
Use the first date of any criteria followed to start an event. Example: If a blood culture is drawn on one day; after the results are back, antimicrobials IV are begun; but, now you notice a note from the nurse says access site was slightly red before blood was drawn, the date of the “slightly red” came first, that is your Dialysis Event DATE!
How do you Determine a Start Date of a Dialysis Event when Multiple Criteria are Present?
91
How do you Determine an End Date of a Dialysis Event when Multiple Criteria are Present?
Use the end date of an event as the last date of the antimicrobials or other criteria present. If a re-check of blood work, a note of redness, pus, swelling etc is noted prior to 21 days from last issue of the event it is the same event. If the DE seem to have ended then that is the end date. Next event cannot happen with in 21 days.
92
93
Mon Tue Wed Thu Fri Sat Sun
1 2 3 4 5 6 7
8 9 10 11 12 13 14
15 16 17 18 19 20 21
22 23 24 25 26 27 28
29 30 31 1 2 3 4
5 6 7 8 9 10 11
1. Pus noted 2. antimicrobial start3. Blood culture+
Re-Check Blood culture-
Redness noted
Last day Redness noted
No Redness noted
antimicrobial stopped
End of the event
21 days since end of last event
Report new event after 7th
Use Calendar to Determine Start and End Dates

Quick Validation
When you review your “dialysis events”from month to month, look at these pieces of information to make sure you are not over reporting
– Patient name. If the same patient had an event last and this month… perhaps the IV antimicrobials continued into the next event… so it wouldn’t be a new event
– If last month a patient was in the hospital and came back on antimicrobials but the patient was on antimicrobials prior to this hospital stay and <21 days - Not a new event
94
Quick Validation (con’t)
95
Confusion in Communication?
• Regarding Infections and IV antimicrobial – Discuss dose, frequency and when one or more are selected and given, with your team. Why is one antimicrobial vs. another used? What does the nurse say to the doctor which produces an order—are we talking the same language? Did the doctor understand what the nurse was saying? (Reporting symptoms? Orconcern regarding possible infection?)
• Blood culture draws – how they are drawn and when they are done, are they ordered enough of the time? If no, why not? What prevents that from happening? Should they be drawn?
Is there a possibility of events started due to lack of clear communication?
96

Clarity in Communication …
Has there been a team meeting with the doctors about communication of signs and symptoms? What do the words mean to the doctor… are you saying what you mean and is the doctor
hearing the same thing?
97
When information is put in following the criteria, the data is reported back under different categories by NHSN
Reports coming to your unit will use the following terms. You will use these terms when comparing your unit to National or Network data
“Bloodstream infection”(BSI) is a positive blood culture you put in to NHSN (including contamination)
“ Vascular access infection”is either “local access site infection” or “access-related bloodstream infection”:
“Local access site infection”is “Pus, redness, or swelling of the vascular access site”and negative blood culture (s) or the absence of blood culture (s)“Access-related bloodstream infection”is positive blood culture with suspected sourceidentified as the “vascular access site” or “uncertain”
You may wonder…What happens to Information you put in to NHSN?
98
Dialysis Event (DE) Rates in NHSN per 100 Patient’s at Risk Based on data entered by 22 Providers from 01/2011 to 08/2011
99
You may see information sent to you that looks like this..
IV onlyAny positive blood
cultures
Access related bloodstream infections
In the Network of New England collaborative, there were 2.39 antimicrobial starts, called events, per 100 patient months among those patients with fistulas for the months January to August 2011. What does this mean? It’s the same as saying that an average of 2.39% of patients with fistulas had an event during the months January to August 2011.

• If your facility has 25 patients with a fistula each monththat means that each patient with a fistula has a month of exposure (risk for a dialysis event) in the first month for a total of 25 patient months. If there are another 25 patients at risk of a dialysis event in the second, third and fourth month, it takes 4 months for your facility to have 100 patient months of exposure. If there is 1antimicrobial start in your facility every 2 months, your rate is similar to the Network rate - about 2 events per 100 patient months.
• If your facility has 50 patients with a fistula per month, 100 patient months of exposure are achieved in 2 months. Therefore, if your facility has 1 antimicrobial start every 1 month your rate is similar to the Network rate - about 2 events per 100 patient months.
• If your facility has 100 patients with fistula each month, 100 patient months of exposure are achieved in one month and 2 antimicrobial starts in that month means your rate is similar to the Network rate - about 2 events per 100 patient months.
Notice that the IV antimicrobial start rate for all fistula patients is 2.39 (about 2 events) per 100 patient months.
How to Calculate and Compare Your Facility Rate?
100
• Add the number of “antimicrobial starts” for your patients during the months January to August 2011. This is your numerator.
•Example: 2 in January + 3 in February + 2 in March + 5 in April + 3 in May + 6 in June + 2 in July + 3 in August = 26 “antimicrobial starts” events
• Add the number of patients you had with fistulas in each of the months January through August 2011. This is the number of patient months at risk for an event, called simply the number of patient months. This is your denominator.
•Example: 50 patients in January + 45 in February + 55 in March + 56 in April + 60 in May + 60 in June + 50 in July + 55 in August = 431 patient months (patients at risk)
• Divide the numerator by the denominator and multiply by 100.•Example: (26/431)*100 = 6.03%. This means that an average of 6.03% of patients with fistulas in your facility had an event. Stated another way, it also means that there were 6.03 events per 100 patient months among patients with fistulas.
Comparing your average events among fistula patients to that of the Network, you see that you have a higher average monthly rate: 6.03% versus 2.39% or, stated another way, 6.03 events per 100 patient months versus 2.39 events per 100 patient months.
Check your data and make sure all the criteria are followed including the 21-day rule
How does the Network average compare to your average?
101
(This is an example only)
Total
26
Rate = Dialysis Events (numerator)
Patient Census (denominator)X 100
102
Rate = X 100
Jan Feb Mar Apr May Jun Jul Aug
IV antimicrobial starts in fistula patients
2 3 2 5 3 6 2 3
Number of fistula patients
50 45 55 56 60 60 50 55
26
= 0.0603 X 100
= 6.03%
On average, from January through August, there were 6.03 IV antimicrobial starts
for every 100 fistula patients each month.
431
431
+ + + + + + + =
+ + + + + + + =
Rate Calculation

Rate Calculations
Rate = Dialysis Events(numerator)
Patient Census (denominator)
103
100
Monthly Rate =
Dialysis Events(numerator)
Patient Census (denominator) 100 12
A Note About Rate Calculations
� Yearly rate is more important
� Monthly rate will help to know where the problem is
� Keep in mind Zero is our goal, Network rate is a benchmark for NOW
104
105
Last thoughts…..
• Make sure none of the positive cultures are wound cultures (if other criteria are noted, then it will be an event)
• Make sure if redness, pus or increased swelling is seen it is at the vascular access site (if a wound, it should not be an event)
• Once data are validated, work with your team for possible reasons for the events that occurred in your setting. See what you can do to reduce them.

106


















