Understanding Acupuncture
43
CHAPTER CONTENTS The Asian revival 46 The pre-Second World War decline 47 The post-Second World War recovery 51 Westward transmission 60 Acupuncture in the USA 60 Acupuncture in the UK 68 Acupuncture in the Commonwealth countries 69 Acupuncture in European nations 70 Acupuncture in the former USSR nations 71 A summary of westward transmissions 73 Modern Western intellectual trends 73 The numbers game 77 China 77 Taiwan 78 Japan 78 The USA 78 The UK 79 France 79 Germany 79 Utilization worldwide 79 The acculturation and re-acculturation of acupuncture Considering the history of traditional Chinese medicines, finding a diversity of techniques and ideas in modern practice should be unsurprising. The scope of the tradition is so great in age and extent that scholars have concluded that clinical techniques cannot be accurately applied, or even translated, without considering their historical context. The reputation of a medicinal in a Tang source, or a Ming theoretical notion, cannot be unquestionably applied without considering their generative context. For example, merely knowing the acupoints used to treat a particular pattern is insufficient because we must also know the qualitative criteria by which the pat- tern was recognized and the stimulus sought in treatment. Although this does mean that some Western notions need re-thinking, knowledge of this diversity helps us understand acupuncture. Viable human skills evolve, change, and adapt to circumstance. Knowing that acupuncture has often successfully met the challenge of adap- tation is a far stronger demand on our attention than are fanciful histories and faith-like notions of purity. Consider, for example, the often- expressed idea that the holism of Asian med- icines derives from a lack of anatomical explo- ration. Not only does this obscure Chinese history, but it also prejudicially assumes that the Chinese were a a uniquely rigid and uncurious people. Although acupuncture’s history is com- plex and often indistinct, it does reveal a vibrant system of practice that has served vast popu- lations for nearly 2000 years. That which we 2 43
Transcript of Understanding Acupuncture

CHAPTER CONTENTS
The Asian revival 46
The pre-Second World War decline 47
The post-Second World War recovery 51
Westward transmission 60Acupuncture in the USA 60Acupuncture in the UK 68Acupuncture in the Commonwealth countries 69Acupuncture in European nations 70Acupuncture in the former USSR nations 71A summary of westward transmissions 73
Modern Western intellectual trends 73
The numbers game 77China 77Taiwan 78Japan 78The USA 78The UK 79France 79Germany 79Utilization worldwide 79
The acculturation andre-acculturation ofacupuncture
Considering the history of traditional Chinesemedicines, finding a diversity of techniques andideas in modern practice should be unsurprising.The scope of the tradition is so great in age andextent that scholars have concluded that clinicaltechniques cannot be accurately applied, or eventranslated, without considering their historicalcontext. The reputation of a medicinal in a Tangsource, or a Ming theoretical notion, cannot beunquestionably applied without consideringtheir generative context. For example, merelyknowing the acupoints used to treat a particularpattern is insufficient because we must alsoknow the qualitative criteria by which the pat-tern was recognized and the stimulus sought intreatment.
Although this does mean that some Westernnotions need re-thinking, knowledge of thisdiversity helps us understand acupuncture.Viable human skills evolve, change, and adaptto circumstance. Knowing that acupuncture hasoften successfully met the challenge of adap-tation is a far stronger demand on our attentionthan are fanciful histories and faith-like notionsof purity. Consider, for example, the often-expressed idea that the holism of Asian med-icines derives from a lack of anatomical explo-ration. Not only does this obscure Chinesehistory, but it also prejudicially assumes that theChinese were a a uniquely rigid and uncuriouspeople. Although acupuncture’s history is com-plex and often indistinct, it does reveal a vibrantsystem of practice that has served vast popu-lations for nearly 2000 years. That which we
2
43
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 43 (Black plate)

44 WHAT ACUPUNCTURE IS
can learn from it, including holistic techniques,is rooted in the practical experience of thathistory, not in Chinese peculiarities.
We also must re-think Western impressionsthat are based on assumptions which historydoes not confirm. For example, if we were toimagine that all the known medical collegesand all the centers of literate learning hadgraduated scholar-practitioners at unimaginablecapacity, it would still be impossible to thinkthat the Chinese people were primarily treatedby ru yi, scholar-doctors. There were neverenough classically trained doctors to serveentire populations. Medicine was not a high-status profession in China, indeed even now-famous physicians like Sun Si-miao were oncedisdained for following a medical career. Thevast majority of treatments were performed bypeople who trained as apprentices, like trades-men. Many, if not most, were illiterate. Becauseapprentices are trained to replicate exactly theirteacher’s skills, this led to teacher–student linesof specialized practice. Thus there were perhapsthousands of lineal specializations of greater orlesser import.
Again, diversity; again, ways of thinking andlearning different from our own. Even today,Chinese physicians who have learned theexpectations of Western students will warn:‘Never ask, “What is a slippery pulse?” Insteadask: “What do you call a slippery pulse andwhat do you do when you find one?” Only thenwill you learn what your teacher actually does.’In essence then there is no more a single, uni-versal ‘traditional Chinese acupuncture’ thanthere is a single, universal ‘traditional Europeanart.’ Tradition is not a synonym for unchangingtruth, lack of innovation, or a dogmatic fixity ofideas. It is a vast source of experience, opinion,and information that must be understood incontext. One of Yoshio Manaka’s many storiesclearly illustrates these issues:
Let us imagine that it is nearly four hundred yearsago in China and I am a good friend of Yang Ji-Zhou,the author of the Zhen Jiu Da Cheng. Because of this,he might have included these [(e.g. Manaka’s)]treatments in his text of 1601 [The Great Compendium],despite the limited experience of my two cases.
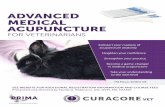
Figure 2.1 Qing Dynasty Acupuncture Chart, front view.(200 × 530 cm; ink on paper, courtesy of ParadigmPublications.)
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 44 (Black plate)

THE ACCULTURATION AND RE-ACCULTURATION OF ACUPUNCTURE 45
Today, almost four hundred years later, practitionersand students reading his text will place great trust inmy results because they were included in this greatand revered text, and because my friend’s reputationin later centuries is excellent. Is this a sufficientcriteria for making general proclamations about thetreatment of asthma and trigeminal neuralgia?
What if these treatments were to go through themill of heuristic adaptations and later authorstransmitted my results by saying only that CV-22 isgood for asthma, or TB-5 is good for trigeminalneuralgia, without including the method I used(moxa) or the theory of the extraordinary vessels?What if translators then simplified the terms withwhich I diagnosed these conditions? Would thesepoints reliably produce the desired results or wouldthere be only a statistical percentage of patients whowere helped?1
Methodology is lacking in traditional literaturebecause books were used in a different way.They supplemented hands-on, naked-senseteaching. Once understood, once set in context,once the assumptions of the compilers andtranslators are known, Chinese literature can beof tremendous value. Unavoidably, the story ofacupuncture’s westward flow has too oftenbeen a tale of partial information taken as thewhole. Because acupuncture was simultaneouslyre-acculturating in every Asian nation, risingfrom the ashes of traditional cultures foreverchanged by war and other vast political andcultural events, it has been difficult for Westernresearchers to examine the generative contextof many ideas.
This was true from the first. News ofacupuncture and Chinese traditional medicalpractices arrived in Europe early in the Qingdynasty (Box 2.1). There were already referencesto, and descriptions of, pulse diagnosis,acupuncture, and moxibustion in Germany,Holland, and England by 1700. But by 1718 itwas described as a remedy that had gone outof fashion. In 1755 the Dutch physicianGerhard van Swieten anticipated modern devel-opments in acupuncture by nearly 2 centurieswhen he speculated that acupuncture andmoxibustion were neurological phenomena.This idea was to appear again in 1798 — whenRougement would label acumoxa treatment as
Figure 2.2 Qing Dynasty Acupuncture Chart, back view.(200 × 530 cm, ink on paper, courtesy of ParadigmPublications.)
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 45 (Black plate)

‘counter irritation therapy’ – an idea that wouldresurface in Japan a century later.
Acupuncture was primarily used in thetreatment of pain through methods that werevoid of traditional theories (Box 2.2). The firstand most common Western adaptation wasneedling pressure-sensitive points near a patient-reported pain. As we saw in Chapter 1, thismethod was first described in the 6th centuryby Sun Si-miao, who referred to these as a-shi(‘it’s there’ or ‘ouch’) points. Nineteenth centuryuses were neither fully traditional nor verybroadly based. More importantly though, theyclearly reflected the biases of the Western physi-cians who adopted acupuncture.
THE ASIAN REVIVAL
If Western physicians took too much for granted,the Chinese lost too much to circumstance. By1912, acupuncture and moxibustion were inprecipitous decline, barely able to counter thegrowth of biomedicine in Japan and China. Inother East Asian countries, for example Vietnam,the same decline was also evident. In Europeand North America, acupuncture and moxibus-tion had gained a finger-hold, but were farfrom accepted. A simplified form of acupunc-ture had been adopted by a few physicians, butSoulie de Morant spent another decade in Chinabefore he returned with a vision of acupunc-ture that would take hold in Europe. Of course,acupuncture and moxibustion were practicedby Asians living in Europe, especially ethnicChinese and Vietnamese in their own commu-nities. Islands of traditional practice remainedin Asia; the blind practitioners of Japan neverceased to preserve and innovate. But, as theworld stood at the brink of the First WorldWar, the traditional arts of acupuncture andmoxibustion were close to cultural extinction.
In China the supports of traditional medicinehad shattered. The failure of the traditionalbureaucracy, the indifference of Europeanpowers, the abject poverty and misery of thepopulation, and the rapidly increasing influenceof Western medicine, all contributed to itsdecimation. It met the 20th century as isolated
46 WHAT ACUPUNCTURE IS
Figure 2.3 Qing Dynasty Acupuncture Chart, side view.(200 × 530 cm, ink on paper, courtesy of ParadigmPublications.)
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 46 (Black plate)

and competing forms. In Japan, acupuncturewas held hostage. With each successful mod-ernization and industrialization, and with thegrowing therapeutic repertoire of biomedicine,it was restricted further. In Europe, acupuncturewas also in decline. It had a few strongsupporters, and would resurge significantlyonly after George Soulie de Morant had spent20 years tirelessly working against indifferenceand hostility. In North America acupuncturebegan this era as a footnote. A simplified formof acupuncture was recommended for low-backpain in Osler’s Principles and Practice of Medicine,but this endorsement apparently influencedfew physicians. Although fascinating storieshave undoubtedly been lost by historicalinattention to the lives of Chinese immigrantsto western USA, among European Americans,acupuncture was barely practiced at all.
Despite these unimpressive beginnings, themodern story of acupuncture is nonetheless itsrise from impotence at the beginning of the20th century, hiatus and persecution throughthe Second World War, to resurgence in EastAsia and expansion throughout the West. Yet,from this loss of place, this lack of social orpolitical influence, it gained its freedom.
Unfettered by now-defunct traditional formsand prejudices, and thought to be of littleeconomic value, acupuncture was carriedforward only by those whose attachment waseither to the art itself or to one of its practicalapplications. Orphaned by the old establishment,it was adopted and put to work. Because it didwell, today, at the turn of the 20th century, itenjoys what may be its greatest popularity todate. An estimated 1–1.5 million people practiceacupuncture somewhere on the planet, and asmany as a quarter of the Earth’s population hasready access to an acupuncturist.
THE PRE-SECOND WORLD WARDECLINE
We are presenting this part of acupuncture’sstory in two major sections: its radical declineeverywhere before the Second World War andits recovery since. Again, this is a convenientway to tell the story, but the country-by-countryexposition understates the many complex inter-actions. Because there are so few formal histo-ries concerning acupuncture in the West, ourrecounting is often, of necessity, based oninterviews. We have thus surely understated the
THE ACCULTURATION AND RE-ACCULTURATION OF ACUPUNCTURE 47
Box 2.1 Cross-fertilization
1658 Jacob de Bondt published the first reference to Chinese pulse diagnosis1682 The German Andreas Cleyer wrote a treatise on Chinese pulse diagnosis1683 The Dutch physician Willem ten Rhinje published an essay on acupuncture, including the first
illustrations of the acupuncture channel system1693 The English physician William Temple wrote about the use of moxibustion1712 The German physician Englebert Kaempfer wrote essays on acupuncture and moxibustion1718 Acupuncture was mentioned in a surgical text as a remedy that had gone out of fashion1755 The Dutch physician Gerhard van Swieten speculated on the possible neurological basis of
acupuncture and moxibustion1798 C. J. Rougement wrote of acupuncture and moxibustion as a form of ‘counter-irritant’ therapy1774 Sugita Gempaku translated a Dutch anatomical text into Japanese, signaling the beginning of a strong
Western influence on Japanese traditional medicine1805 The Jennerian smallpox vaccine was introduced to China1835 The first medical missionary–surgeon arrived in China, with techniques that fascinated the Chinese
at that time1851–1858 The first six Western medical texts appeared in China1880 Gray’s Anatomy first appeared in China1886 The first missionary medical school was established in China1894 In Japan, Tesai Okubo declared acupuncture and moxibustion to be ‘stimulation therapies’Late 1890s The European germ theories of Koch, List, and Pasteur start to arrive in China. By the 19th century,
acupuncture and moxibustion were more widely used in Europe and their use spread to the USA.For example, in 1892, acupuncture was described in Osler’s landmark medical textbook
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 47 (Black plate)

contributions of many, to whom we apologize.Although modern Asian medical history hasbeen professionally explored, and those worksare cited herein, there are very few scrutinizablesources for the Western acculturation ofacupuncture. Thus the following presentation ispreliminary. Nonetheless, we think it reasonableto assert that, after the Second World War, andparticularly after 1970, the explosive acceptanceof acupuncture in the West has made it a trulyinternational field, and that this is the centraltrend of the period. Thus, because what mostmodern acupuncturists do took shape in thesecond half of the 20th century, acupuncturetoday encompasses an enormous diversity ofpractices, with roots in several countries.Although many of these practices can fairlyidentify earlier texts and traditions as theirsource, acupuncture has effectively become amodern art that can be understood in themodern social, political, and economic context.
Again, it is China that has been the leadingplayer. The story of medicine in China in the20th century is the story of a new social andpolitical order in which both Eastern andWestern medicine were applied. China’s viewof its own medicine must be seen in the contextof its new faith in ways of thinking that wereclose enough to the Chinese mindset to encour-age adoption but different enough to allowhope for a better future. China, like the rest ofAsia in the early 20th century, was floodedwith European and American influence. How-ever, what Europeans first brought to Chinawas not medicine or culture; it was a narcoticdrug. China had been ‘opened’ largely throughan imposed trade in opium. European andAmerican merchants promoted the demand foropium to acquire previously unavailable Chineseproducts for resale in the West. Between 1821and 1854, opium deliveries to China wouldincrease by 1600%.2 It was a trade in agony andhuman suffering, twisted to typify the Chineseand not the Westerners who organized it fortheir own profit. Still indistinct in Westernhistories, the opium trade was a social horrorthat very aptly reflects the subhuman status inwhich many Westerners held the Chinese. This
48 WHAT ACUPUNCTURE IS
Figure 2.4 Qing Dynasty Acupuncture Chart, Zang Fu.(200 × 530 cm; ink on paper, courtesy of ParadigmPublications.)
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 48 (Black plate)

chauvinism, naturally, biased Western opinionsof the creations of Chinese culture, includingacupuncture.
In the political arena, China fared no better.Between 1853 and 1865, during what is knownas the ‘Taiping Rebellion,’ a rebel leader occu-pied Nanjing for 12 years. He was displacedonly when British troops resolved the conflict.The Qing government’s impotence in the faceof this rebellion — during which as many as 20million Chinese may have died — is an effectivesymbol for the end of the governmental systemthat had served China for nearly 2000 years.Although French and British forces did occupyBeijing, and treaty ports or concessions wereoccupied by colonial powers, China was neveractually colonized. Governmental efficacy wasnonetheless lost. In 1877–1878 there was afamine that left 9 million people in horrifyingcondition. Parents sold or killed their children,people maimed themselves because begging,other than suicide, seemed the only escapefrom starvation.3 There was no public sanitation;open sewers and refuse-strewn streets were thestandard urban vista. In this atmosphere ofdecline and loss of self-determination, theRepublic of China was formed in 1911. The lastdynastic ruler’s abdication was the prelude to astruggle for power among those who differed
in their views of how China should be rebuiltin the image of the West.4
When the Qing dynasty ended, general XuanShi Kai, friend of the well-known Westernmedical doctor Sun Yat Sen, became the firstpresident of the Chinese Republic. However,democracy had no root in Chinese culture anddid not survive. It was not until 1926 that JiangJieshi (Chiang Kai-shek), by force of arms andnot politics, united the country. Meanwhile,another Western import, Communism, hadalready taken hold. The Chinese CommunistParty (CCP) was formed in 1921. Althoughbriefly allied with the Nationalist Guomindang(GMD) until 1927, violence rooted in politicaldiscord would set it on a solitary course. TheCCP established itself in guerrilla bases afterthe invasion by Japan. The period beginning in1937 with that invasion and the Second WorldWar, and ending in 1949 with successful revo-lution, left China in ruins.
For China, the first half of the 20th centurywas a period of nearly unimaginable humansuffering. A horrifying drama of starvation andacts of human desperation played against theterror of the Japanese invasion. The Japanesebrought nothing of their own earlier and morerapid scientization except weapons of total waraimed at a population only barely prepared to
THE ACCULTURATION AND RE-ACCULTURATION OF ACUPUNCTURE 49
Box 2.2 Nineteenth-century uses of acupuncture in the West
1802 England W. Coley wrote about the uses of acupuncture1816 France L. Berlioz wrote a book on acupuncture1820 Italy S. Bozetti wrote a book on acupuncture1821 England J. M. Churchill wrote on the use of acupuncture for rheumatalgia1822 USA First favorable comments on acupuncture in a US medical journal1825 France J. B. Sarlandiere first wrote on the uses of electro acupuncture1825 Italy A. Carraro wrote on the uses of acupuncture1825 USA F. Bache started using acupuncture for pain relief1826 England D. Wandsworth wrote on the uses of acupuncture for pain relief1826 Germany G. E. Woost reviewed the status of acupuncture1827 England J. Elliotson wrote on the uses of acupuncture for rheumatalgia1828 Germany J. Bernstein wrote on acupuncture for rheumatic pain1828 Germany L. H. A. Lohmayer wrote on acupuncture for rheumatic pain1828 France J. Cloquet and T. M. Dantu wrote a book on acupuncture1833 USA W. M. Lee wrote on the use of acupuncture for rheumatism1834 Italy F. S. da Camin reproduced Sarlandiere’s electroacupuncture ideas1871 England T. P. Teale wrote on acupuncture for pain relief1880 England S. Snell wrote on acupuncture for pain relief1892 Canada W. Osler described the use of acupuncture for lumbago in his influential Principles and Practice of
Medicine
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 49 (Black plate)

50 WHAT ACUPUNCTURE IS
deal with the previous century. Some of thecrimes of the Japanese occupation are onlytoday being revealed. The industrialized citieswere places of awful working and livingconditions. The countryside was an ocean ofimpoverished peasants. Infectious diseaseswere endemic and epidemic.5
Traditional medicine was not in a position toexercise its abilities. Could acupuncture, whichhad long offered vermifugal treatments, havecured these millions? Perhaps, but no empiresurvived to organize the effort, and manyChinese probably knew nothing of the possibil-ity. Those who did might have searched in vainfor capable acupuncturists, as many Chinesetraditional practitioners were lost in the plaguesthat raged through China.6 The Chinese werelooking to modernize as much as possible andwere turning to Western medicine. Thus thebeginning of the 20th century was theoretically,as well as practically, devastating for acupunc-ture and traditional Chinese pharmaceutics.
Although the history of the conflict betweenChina’s old and new philosophies would bewritten by the CCP and the eventual communistgovernment of China, that conflict was not essen-tially created by communism. Both communismand biomedicine were being acculturated in ashift from the now-repudiated traditional valuesto newly adopted concepts that had found favorin the West. The Marxist theory of dialecticalmaterialism was seen by many as a scientificexpression. No less an authority than Maohimself would proclaim that communist culturewas based in science.7 Thus it interested many,not just those politically active as Communists.8In effect, Western ideas that seemed rooted inscience were replacing the Three Pillars as thefoundations of Chinese medicine:
Modern science assumed the role of the doctrine ofsystematic correspondence, whose magic-derivedconcepts of yin-yang and the five phases were nowspurned as fully inadequate for the solution of newtechnological problems.
Marxism, which appeared in China claiming to bea scientific social theory, replaced Confucianism,whose socio-theoretical concepts and view of historyhad been closely associated with the old ‘naturalscience’ of systematic correspondence.9
Thus from the Republic’s first days theintellectual elite were prepared to abandontraditional culture. Everywhere, the qi paradigmwas rebuked. When traditional practitionerssought registration from the Minister ofEducation, they were informed that he hadalready decided to prohibit their practice. Asearly as September 1915 an order was issueddemanding that medical, pharmacy, andveterinary students meet the qualificationsestablished by Western nations.10 In 1922, theMinister of the Interior licensed both Westernand traditional practitioners. Then, in 1929, theMinistry of Health finally ceased registration oftraditional doctors, and announced an explicitproposal to abolish traditional medicine. Chinarepudiated its own medicine, taking faith in itsWestern rival.
However, faith in the new medicine and itsencompassing science were not sufficient tocreate a working medical system. Althoughboth the national government and the Europeanconcessions made constructive attempts, thesewere so small, so poorly funded, and so late asto have no effect. When the Japanese invadedin 1937, there were only 77 health centers and144 rural care stations in a nation that consistedof 2000 cities and 100 000 villages.11
Chinese medicine was not without its heroes.The zhong yi movement proposed innovationsthat would later be incorporated into what isnow called Traditional Chinese Medicine (TCM).During the 1920s a number of traditional prac-titioners — among them Qin Bowei, who wouldlater contribute to the modern technical des-cription of TCM12 — sought to salvage traditionalmedicine. They attempted to reconcile manytraditions under a single banner, zhong yi, creat-ing a solid front that could resist the encroach-ment of xi yi, Western medicine.13 Although notthen successful, this movement laid the founda-tion of the modern development of traditionalmedicine after the Second World War.
In Japan, scientific validation of acupunctureand moxibustion was also everywhere encour-aged. Technically, 120 koketsu, discrete acupunc-ture points, were defined by underlying, usuallyneurological, structures. The only acupuncture
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 50 (Black plate)

THE ACCULTURATION AND RE-ACCULTURATION OF ACUPUNCTURE 51
points now considered valid were those thathad empirically observed clinical effects.Traditional concepts, qi, yin-yang, and channelswere entirely discarded. Acupuncture was seenas a practice based on the stimulation ofdiscrete anatomically-defined points withscientifically-demonstrated effects. Providedthis was the model taught and practiced,acupuncture and moxibustion were allowed tosurvive. The movement that was started bySugita Gempaku and was promoted by theRampo school achieved dominance. In theseveral decades after 1868, the basis ofacupuncture practice shifted from the coexistenceof modern and traditional explanatory modelsto a purely scientific rationale.
Traditional medical practices in all of Asiafollowed the trends in China and Japan. InKorea during the first half of this century therewas little innovation or development. Acupunc-ture, moxibustion, and traditional pharmaceuticslost ground to biomedicine, and suffered appre-ciably in the violent political upheavals of thetime. The Japanese invasion of Korea devastatedKorean culture, including traditional medicine.Acupuncture and moxibustion in Vietnam werealso slow to develop, compared with the post-war years. Not much information is available.Under French colonial rule biomedicine wasactively promoted and traditional medicinessuffered except in areas that could not affordWestern-style clinics.
Little can be found about acupuncture inEurope and North America during this period.Probably the most significant events were thereturn of Soulie de Morant to France in 1917and his subsequent publications. But thesedid not find a receptive audience until afterthe Second World War. It is probable thatacupuncture was practiced in the Asiancommunities of Europe and North America, butlittle information survives.
THE POST-SECOND WORLD WARRECOVERY
After the Second World War, there was adramatic resurgence of acupuncture around the
world, particularly in China. In the periodbefore the Japanese invasion of China, therehad been many debates about the future oftraditional medicine; but it was the war expe-rience of Mao Ze-dong that gave traditionalmedicine a firm commitment. The communistofficial Ma Hai-de stated this clearly:
The witch doctors are banned, they are dangerous.We got rid of them by introducing them in the‘yangko’ plays so that the people laughed at themand we got them better jobs – gave them farms –anything, as long as they would stop harming thepeople. The herb doctors, the acupuncturists and themidwives we kept but we gave them training in theessentials of Western medicine. Chinese herb-doctorshave done an enormous lot of good.14
Thus, as the communists under Mao promotedtraditional medicine, they set about changing itto make it more acceptable, more scientific.
In the first days of the People’s Republic,among the first orders of business was healthcare for a huge society, the already threadbarefabric of which had been reduced to anunraveled mass of disconnected threads. Thesocial structures that had supported traditionalmedicine were in ruins. The Three Pillars couldnot support their own weight, much less amodel of medical reality under constant attack.The islands of traditional skill that Soulie deMorant had known, the last physician scholars,the current generation of lineal apprentices – somany had drowned beneath violent waves ofwar, social collapse, epidemic, and famine.
China’s political leaders were faced with theseemingly insurmountable problems of servinga half billion population with less than 40 000Western physicians and upwards of 500 000disorganized and discursively trained tradi-tional practitioners. This is the health-care crisisthat the United Nations Relief Organizationcalled ‘the greatest and most intractable publichealth problem of any nation in the world.’15
Here was the clear, pragmatic reason for theCCP to promote traditional medicine; there wasno other choice.
Although the experience of war and pro-viding health care to a vast nation would makeMao Ze-dong the most reliable political advocate
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 51 (Black plate)

for traditional medicine, even admired mem-bers of the CCP would continue to oppose it.Mao would need to purge party leaders andstate officials in defense of TCM.16 However, inthe CCP generally there was a strong feelingfor preserving the essence of Chinese cultureagainst the onslaught of Western creations.These feelings helped save traditional medicinefrom outright abandonment or prohibition. Butin the CCP’s political environment traditionalmedicine could not survive without beingscientized. This was the political compromisethat evolved between conservatives who saw itas an aspect of Chinese culture to preserve andmodernists who saw it as, at best, a collection ofempirical tricks, some of which might be useful.
Starting in the 1950s traditional medicalschools with standardized curricula wereestablished to teach basic biomedical sciences,traditional pharmacotherapy, and acupuncture.To accomplish this the theoretical basis ofacupuncture and herbal medicine had to bestandardized and adapted to classroom training.For the first time in history a united medicinewas abstracted from the materials of tradition.The zhong yi movement, which had begun todescribe a coherent mode of practice in the1920s, triumphantly re-emerged. Their work isthe foundation of treatments used today. In theprocess, however, political compromise wouldguarantee the exclusion of many traditionalideas that did not fit party doctrine. Ashistorians Hillier and Jewell state it:
The Communist Party sought to achieve theobjectives the Guomindang government had failedto reach in 1935; to unify and regulate traditionalpractitioners and incorporate them with doctors ofWestern medicine into a single federation understate control. Such unification was necessary toutilize in the most efficient way every availablemedical resource to combat the huge burden ofinfectious and parasitic disease in China, to build upthe ramshackle health care system, and to exertideological control over both the ‘bourgeois’tendencies of modern doctors and the ‘feudalsuperstitions’ of the traditional ones.17
Traditional medical practice was saved, butthe qi paradigm was its ransom. As PaulUnschuld notes, it was now the branches of a
tree, the philosophical roots of which had beensevered.18 Nonetheless, for the first time in the20th century, Chinese medicine had a firmcultural position, a clear economic role, and apowerful political patron.
Meanwhile, many Western medical schoolswere established. Creating a Western medicalsystem was such a priority that today only 30%of China’s medical colleges are traditionallyoriented,19 and Western physicians outnumbertraditional practitioners two to one.20 Thesepressures changed acupuncture and traditionalherbal medicine profoundly, because it was theincreasing demand for medical services, not thepreservation of traditional methods, thatoccupied the nation’s resources. Better training,the supervision of apprentice programs, prose-cution of medical drug smuggling, and thepolicing of ineffective herbal remedies were thepriority undertakings. By providing doctors ofTCM with an opportunity to research andpublish, the government gave them status.However, the state exercised control, and bio-medical doctors earned five to ten times greatersalaries, a policy which continues to directChina’s best students away from TCM.21
There have been a number of importantdevelopments since. In the Great Leap Forward(1958–1959), besides a number of generalpolitical changes, some of which were econom-ically catastrophic, Mao pursued the integrationof traditional and Western medicine evenfurther. In 1958, Mao made the famous state-ment: ‘Chinese medicine is a great treasure-house! We must make all efforts to uncover itand raise its standards.’22 In the 1950s a monthof traditional medical study was required of allWestern medical students. This created a largepopulation with an exceedingly cursory trainingin acupuncture. The impact of this policywould be felt 2 decades later when Westernscientists would turn to these medical-schoolgraduates, and the English-language derivativesof the Chinese literature created to train them,to develop their clinical trials of acupuncture.Thus, these studies were often inadequate.
During the Great Leap Forward, in an envi-ronment of prominence for rural public health
52 WHAT ACUPUNCTURE IS
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 52 (Black plate)

issues, the integration of traditional and modernmedicine was to become an even more signif-icant priority. In politics, the CCP was walkinga tightrope between the preservation of a low-cost, available, and native expedient, andsupport for practices that were far too obviouslyrooted in China’s feudal history. TCM tooclearly rested on a non-materialist philosophy —correspondence rather than material logic. Thetechniques were useful, but the qi paradigmwas a political liability. This quandary calledfor a political resolution; it would be called the‘Three Combinations:’
• medical education and productive labor,mass campaigns and traditional medicine
• leading functionaries, teachers, and studentsunder Party leadership
• teaching, scientific research, and treatmentwith prevention.
In the end, economic need and political expe-dience, not theory or science, determined theoutcome. That outcome was not that traditionalmedicine was honored as an intellectual trea-sure to be preserved. Instead, it was Mao’s‘treasure-house’ from which the useful was tobe culled, sorted, scrubbed, and polished byscience in service of the state.
Yet, by the end of the Great Leap Forwardthis unification of traditional and Western med-icine was pleasing none. Traditional practi-tioners feared eventual elimination as they hadneither money nor prestige. Furthermore, theywere not themselves united. To make mattersworse, popularization and expansion hadfurther diluted what had never been a homoge-nous system. Despite this, CCP pressure for
integration continued, and the system expandedlike a tidal wave.
From the viewpoint of many Western scien-tists, one of the most important developmentsbegan in this period. This was the utilization ofacupuncture as an anesthetic and analgesicduring surgery. During this time aggressiveacupuncture techniques were developed andbecame a routine part of TCM. When Westernersstarted flooding China after Nixon’s visit, itwas these techniques they were shown. Theybrought these back to the West, where theywere popularized and became a primary focusfor research. Even today, Western books derivedfrom Chinese writings of this period evidencedeeper insertions, stronger needle stimulus,and a greater use of minor surgical techniques(Tables 2.1 and 2.2).23
Once again, everything in China wouldchange as the political unrest resulted in the‘Great Proletarian Cultural Revolution.’ AlthoughTCM did not inspire the Cultural Revolution,its roots in the qi paradigm, which was stillconsidered feudal superstition, would be apolitical focus. Traditionalists outside the statesystem would be labeled as ‘witch doctors.’Some who are today ‘living treasures’ in China,were then banned. For example, Cheng Tan An,whose treatments are now widely recognized,was persecuted.24 However, TCM would con-tinue to be popularized, because acupuncture,moxibustion, and natural drugs were stillinexpensive and useful.25
Indirectly, however, the Cultural Revolutionhad significant consequences for all medicine.Among the millions of its victims were physi-cians, scientists, and many of the intellectuals
THE ACCULTURATION AND RE-ACCULTURATION OF ACUPUNCTURE 53
Table 2.1 Depth of insertion (in cun, or ‘body inches’) and number of points at each needle depth given in historicalacupuncture textbooks
Book Mean (median) No. of pointsdepth
0.1–0.3 0.35–0.6 0.65–1.0 1.1–1.5 1.6–3.0
Zhen Jiu Jia Yi Jing (282) 0.49 (0.4) 171 113 51 5 9Tong Ren Shu Xue Zhen Jiu To Jing (1027) 0.42 (0.3) 182 94 47 1 1Zhen Jiu Ji Sheng Jing (1220) 0.41 (0.3) 196 89 50 0 1Zhen Jiu Ju Ying (1529) 0.41 (0.3) 186 99 45 1 2Zhen Jiu Da Cheng (1601) 0.41 (0.3) 191 96 48 1 1
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 53 (Black plate)

on whom both the modern and traditionalhealth-care systems depended. Training stoppedand students continued to graduate, althoughtheir colleges had not held classes for years.Political ideology ruled where modern sciencehad once held sway. Politically incorrect tradi-tionalists were forced to hide and could notteach. Some fled to the periphery of China,some to America or Europe, where they beganto impart their views and clinical systems toWestern students.26
Order was restored after the initial unrest ofthe revolution. The party began to rebuild, andby 1969 Mao had regained control of all Chinese
health care policy. Under his direction, bothrural and urban populations saw improvementsin the availability of care, but by far the mostrecognized phenomenon of the era, perhapseven to an extent greater than it may objectivelydeserve, was the Barefoot Doctor movement.Just as it appealed to the people-to-people ethicof the Red Guards, it also appealed to populistsensibilities in Western democracies and gener-ated a powerfully positive reputation in theWest.
In theory, Barefoot Doctors were worker-doctors. Their salary, education, and repertoireof medicines and equipment were financed
54 WHAT ACUPUNCTURE IS
Table 2.2 Depth of insertion (in cun, or ‘body inches’) and number of points at each needle depth given in modernacupuncture textbooks
Book Mean (median) No. of pointsdepth
0.1–0.3 0.35–0.6 0.65–1.0 1.1–1.5 1.6–3.0
Essentials of Chinese Acupuncture (1980) 0.57 (0.5) 58 151 136 12 1Chinese Acupuncture and Moxibustion (1987) 0.60 (0.6) 25 165 158 8 2Acupuncture A Comprehensive Text (1981) 1.03 (0.85) 18 41 138 121 41Fundamentals of Chinese Acupuncture (1988) 0.54 (0.45) 74 156 117 8 1
Figure 2.5 Pages from a Barefoot Doctor-era Manual (the manual was equippedwith a single filliform needle inserted through the last page). (Courtesy of ParadigmPublications.)
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 54 (Black plate)

THE ACCULTURATION AND RE-ACCULTURATION OF ACUPUNCTURE 55
through the local work units that each BarefootDoctor served. These units, called ‘brigades,’were thus freed of the bourgeois burden of fee-based medicine and the state was freed of theneed to pay for its rural medical operations. Intheory, the utilization of acupuncture and tradi-tional herbal medicines would reduce expensesto a level that rural populations could afford.Practice did not prove the theory. Acupuncturerequires physical and sensory skills that are notquickly or easily achieved. Quality control inthe selection and preparation of herbal drugshas always taken time to acquire. These facts,coupled with the popular bias expressed inlabeling biomedicine ‘modern medicine,’ meantthat the Barefoot Doctors had a tendency tomostly use biomedical drugs, disrupting thedelicate finances of the brigade.
From a Western perspective, events of thisperiod are bizarre — unskilled hospital stafftreated patients, peasants worked in scientificlaboratories, nurses operated while physicianscleaned toilets and floors, and Barefoot Doctorsprescribed scientific medicines. However, thesemore dramatic excesses should not overwhelmthe successes. By 1975 the Barefoot Doctorscould be credited with the treatment of 70–80%of all illnesses, and an increased reliance ontraditional medicinals did allow both areduction of costs and an expansion of services.
Simultaneously, TCM was changing. In theperiod between 1970 and 1976, CCP leadersdecided that, because TCM theory was merelymedieval superstition, research in TCM neededto be no more than repeated practice. Yet,despite any commitment to fund what the Westmight recognize as valid research, the statedgoal of this period was to raise TCM ‘to theplane of modern science.’27 Although the devel-opment of TCM and its subsidiary branch TCMacupuncture were on the whole very successful,the enormous political forces behind thosechanges so undermined research that acupunc-ture became more vulnerable than ever toWestern skeptics.
Following the Cultural Revolution, tradi-tional medicine stabilized. In the 1970s, underprograms sponsored by the World Health
Organization (WHO), physicians from manycountries came to China to study in one- tothree-month acupuncture programs. Since theearly 1980s many two- to three-month programshave been established for non-physicianacupuncturists from around the world. Today,many Western acupuncture schools have ties totraditional medical schools in China, and theirstudents go there to study in pre- or post-graduation programs. Since the ‘three roads’policy of the 1980s, whereby traditional med-icine, biomedicine, and their combination,‘integrated medicine,’ were permitted to developon their own, more than 2000 Chinese physicianshave graduated with a thorough training inboth traditional and modern medicine. TheWHO programs considerably contributed toacupuncture’s westward migration.
The situation for the scientific study of tradi-tional medicine has also improved, although itis still under political controls. Although muchof the newer work is better by Western stan-dards, the bulk of Chinese studies still fail toconvince Western scientists. Because the studiesare so often poorly designed and controlled,entirely absent of biostatistical technique,researchers in the West take little Chinese workseriously, some believing it to be politicallydoctrinaire.28
In Japan the same nearly instantaneousWesternization had different effects, becausethe social structure was more quickly restored.The Meiji restrictions had already caused abacklash in favor of more traditional approaches,and by the 1920s traditional approaches hadfound effective cultural supports. In 1926,Tadanao Nakayama, a journalist friend of thefamous moxibustionist Takeshi Sawada, pub-lished an influential book promoting traditionalmedicine. Other prominent practitioners suchas Sorei Yanagiya and, later, Shinichiro Takeyamabecame effective critics of the restrictiveapproach. The essence of their protest was thatthe grain had been discarded with the chaff.Although they admitted that there wereproblems with blindly following the classics,they argued that there was nonetheless valuableinformation in those texts. Yanagiya, for
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 55 (Black plate)

example, promoted the idea of a critical re-evaluation of the classics in order to determinewhat was clinically valid.29
Although this re-evaluation was not basedon scientific testing methods that would meet allthe requirements of a modern research institution,it did come very close for the era and theextent of the attempt to recognize traditionalconcepts. It was in many ways similar to theempirical testing of acumoxa therapies andherbal medicines performed in China since the1950s. It concluded successfully. By 1930Yanagiya had become the center of a group oflike-minded people such as as Sodo Okabe andKeiri Inoue. From this center he sounded hisnow-famous call for a ‘return to the classics,’ atheme that echoes the centuries-earlier rallyingcry of the Koho school in Japan and the HanXue school in China.
Often it seems that, when scientific thinkinggains the upper hand in Japan or China, thereis a conservative backlash that re-invigoratestraditional medicine. But, importantly, as themodern era progressed, each of these re-invigorations has been increasingly temperedby a critical view of tradition, each has beencentered on a more carefully structuredapproach. Regardless of whether that structureis a direct Western influence, the reassertion ofa longevous strand of indigenous logic, or acombination of those trends, it is clearly atwork. The works of both Xu Da-chun and SoreiYanagiya exemplify this profoundly, despitetheir separation in time and location.
Yanagiya published many books and isregarded by most as the leader of the Japaneseclassicist movement. By the 1930s other conser-vative movements would arise. Takeshi Sawada,for example, was central to the development ofanother group. Many associations and trendsthat have survived into modern practiceemerged. Of particular import is the movementcalled keiraku chiryo, after its concentration on‘meridian (channel) therapy.’
The keiraku chiryo movement grew throughoutthe 1930s, culminating in the creation of aformal association in 1940. The movement, aswith everything traditional in Japan, was
interrupted in 1943. The association resurfacedin 1946 during the American occupation.30 Thiscarefully structured return to the traditionalmethods of practice was distinguished by twofeatures. First, the leaders of the keiraku chiryomovement were famous clinicians who sub-jected their classical interpretations to scrutinyin clinical practice. Secondly, the classic of choicewas the Nan Jing. For developing palpationmethods and for refining delicate needle tech-niques, the Nan Jing was the richest source.Keiri Inoue, for example, was well known for‘needling’ points without actually inserting a needle.
The keiraku chiryo movement also became afocal point for blind practitioners such as KodoFukushima. In the early 1930s Fukushima hadbeen an anti-war activist, opposing the Japanesegovernment’s aggressive foreign adventures.For this he was punitively conscripted and sentto the Manchurian front line. There, in 1932, hereceived a head wound. But, known as an anti-war activist, he was denied proper treatmentand allowed to go blind. Discharged, blinded,and judged ineligible for veteran assistancebecause of his anti-war protests, he studiedacupuncture, graduating from acupunctureschool in 1938. Dissatisfied with what he learnedin school, he approached Yanagiya and hisgroup in 1940. At first he was rejected, but hewas then encouraged to begin his own studygroup for other blind practitioners. This even-tually led to the establishment in 1959 of theassociation known as Toyohari, ‘East Asianneedle therapy group.’31
At the end of the war, Japan was in shambles.The American occupation forces under USGeneral Douglas MacArthur were overseeingthe reconstruction of Japan. Everywhere thecountry pieced itself together. Acupuncturistswho had survived the conflict began to regroupand, despite desperate shortages, in October1945 Soichiro Tobe, the long-standing senioreditor of the Ido no Nippon magazine, was ableto publish an issue of this important acupunc-ture journal.32 Survivors of the Hiroshima andNagasaki atomic bombings would provide afurther impetus to traditional medicine, as
56 WHAT ACUPUNCTURE IS
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 56 (Black plate)

Japanese traditional medicines were employedto counter the effects of radiation.33 Amongthese were practitioners such as YoshiharuShibata, a physician whose lifetime research inacupuncture, herbal, and diet therapies forradiation-related problems would eventually beapplied to improving cancer therapies. In 1947,in a political move not unlike those launchedby Western physicians in China, Japanesephysicians who opposed traditional medicineconvinced MacArthur’s headquarters to elim-inate traditional practices completely. Thisbecame a rallying point for the acupuncturecommunity. A group of prominent acupunc-turists, including Soichiro Tobe, encampedMacArthur, becoming a regular feature at hisheadquarters in protest of this decision. Otherprominent acupuncturists and physicians alsopleaded the case for acupuncture.34 Probablythe most influential event was a mass rally ofblind acupuncturists in Tokyo. Organizingquickly to preserve the profession, they becamethe catalyst of acupuncture’s salvation.35
There was already a growing sympathy fortraditional medicines at the American head-quarters, but this protest was the ‘last straw.’ Itwould have been politically devastating forMacArthur to eliminate a traditional socialinstitution for Japan’s blind. Thus, as a directconsequence of these protests, MacArthurwithdrew the original announcement and issueda notice of his intention to allow the continuedpractice of traditional medicine. However, thiscontinuance would require the establishment ofthose institutions thought necessary for med-icine in a modern Western society. There wouldbe centralized and standardized curricula andlicensure laws.36 As in China, a political leaderdecided the future of acupuncture. Ironically, itwould be the American general who was everybit as dramatic as Mao.
In 1948 the licensure laws for acupuncture,moxibustion, and massage were passed, andcommittees were formed to structure the corecurricula of schools.37 There would be significanttraining in biomedical sciences, at that timeapproximately 35% of the classroom hours. Asthere had been separate traditions of practice in
acupuncture, moxibustion, and massage, eachof these practices was provided with a separatelicense, but individuals who earned more thanone license were allowed to combine theirpractice. This policy continues today in Japaneseacupuncture education. Students can learn inone of four tracks: only acupuncture; onlymoxibustion; acupuncture and moxibustion; oracupuncture, moxibustion, anma, and shiatsumassage.38 The law restricting the practice ofKampo to Western-trained physicians andpharmacists has been retained.
This approach had the advantage of allowingspecialization in a socioeconomic environ-ment that encouraged adaptation, research,and development. By, perhaps inadvertently,recognizing the diversity of approaches andpreferences that have always characterizedthe practice of traditional medicines throughoutAsia, the new laws gave acupuncture a chanceto adapt to a new era. Acupuncture could meetnew needs in the diffuse and organic way thathad characterized its many historical adapta-tions. In essence this approach preserved plu-ralism by forcing economic competition.Instead of politically eliminating practices byexcising them from curricula and examinations,every idea had to survive the marketplace.This, particularly as the dominance of biomed-icine grew stronger, demanded specialization,research, and competition. Thus, in Japan,acupuncture and herbal medicine grew inde-pendently within an increasingly sophisticatedWestern medical economy, acquiring consid-erable technical specialization.
Progression has been consistent. In the late1940s there were about 60 acupuncture andmoxibustion schools for the blind and a fewschools for the sighted. The new regulationsencouraged an influx of sighted practitioners;thus there are today about 40 schools forsighted students and 20 for blind students.39
With the licenses established encouragingdiversity and specialization, the blossoming ofideas, methods, and techniques that began inthe 1950s has continued to the present. Oncefree of active government suppression and ableto compete in an economy dominated by
THE ACCULTURATION AND RE-ACCULTURATION OF ACUPUNCTURE 57
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 57 (Black plate)

biomedicine, acupuncturists and moxibustion-ists proved studious and inventive. Those whowere not failed.
Because the population became more andmore accepting of Western medicine and scien-tific methods, and because physicians couldalso practice acupuncture without any specialtraining, acupuncture and moxibustion adaptedto the needs of the entire population, rich andpoor, laborer and intellectual, as practitionersspecialized in the resulting competition forpatients. These and other historical pressuresfostered one of the most significant periods ofgrowth and development for acupuncture andmoxibustion in all of Japanese history.
The traditionally oriented trend that hadcoalesced into the keiraku chiryo movement ofthe early 1940s became a number of differentschools based on slight variances in the inter-pretation of classical passages as well as spe-cializations of technique. These allied schoolstoday represent about 20% of the acupunc-turists in Japan. The scientifically orientedtrends derived from the earlier Rampo schoolcontinued to receive government support.Today, scientific approaches represent another20% of Japanese acupuncturists. The remaining60% do not stand beneath any one banner, bututilize a variety of approaches and explanatorymodels.40
In general, the post-war period was one ofconsiderable fecundity for acupuncture inJapan. In the 1950s Kobei Akabane invented thechannel-balancing method of practice as well asthe hinaishin, or ‘intradermal needle.’ Boththese creations, but especially the latter, arepopular in Japan today. Yoshio Nakatani, withthe assistance of his friend Yoshio Manaka,invented the Ryodoraku electrodermal measure-ment method to objectify diagnosis. Manakainvented the ‘ion pumping cords’ and performedsurgical analgesia for appendectomies in hishospital in Odawara as early as the mid-1950s.Manaka’s reputation among Chinese politicalleaders resulted in a personally mediated inter-national exchange, even when diplomatic rela-tions were closed.41 Japanese publishers providedJapanese editions of Chinese texts.
In this period many practitioners started toapply electro acupuncture methods. All theschools of thought flourished, and a significantdialogue between Japanese practitioners andinterested Westerners began. For example, thearrival in Japan of the German physicianHerbert Schmidt was much heralded because itwas seen as increasing the prestige of acupunc-ture in both Japan and Europe.42 There was anexchange of ideas between European physi-cians and Japanese practitioners that providedthe foundation of several European andAmerican systems of practice. Some of theseare still active today. At this time China wasclosed to the West, open only to its Soviet allies.Thus Japan was the center of acupuncture’sdissemination because information from Chinaflowed only through those who had fled therevolution, many of whom practiced pre-TCMforms of acupuncture.
In the 1960s, while these various schoolscontinued to flourish, the newly developedstatistical clinical research methods knownas ‘biostatistics’ arrived in Japan. This led tothe first controlled clinical trials of acupunctureby Haruto Kinoshita and Sodo Okabe.43 Thearrival of these powerful research methodsalso armed scientifically oriented practitionerswith a new method for challenging traditionalapproaches. Although some good research wasdone, some tried to put traditional methods to‘do or die’ tests that heated the debate, breddistrust, and nonetheless failed. Some of thistension remains today.
In the 1970s acupuncture and moxibustionunderwent the same boom in Japan as it didelsewhere around the world following thereopening of relations between the USA andChina in 1971. Significant growth in the num-bers of practitioners and approaches cameduring the 1970s, but the work of Japanesepractitioners was eclipsed by the world’sattention to newly innovated TCM. The Japaneseexpansion continued almost unnoticed in the1980s and 1990s, as did individual Japaneseacupuncturists’ influence around the world.Today acupuncture in Japan can be reimbursedunder the National Health Insurance plan for
58 WHAT ACUPUNCTURE IS
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 58 (Black plate)

the following six conditions: whiplash, low-backpain, neuralgia, rheumatism, cervico-brachialsyndrome, and periarthritis of the shoulder,only after failed biomedical treatment. However,not all acupuncturists routinely make claimsagainst this coverage.44
After the Second World War, traditionalmedicines regained ground in Korea (at least inthe South, as little is known about the North).In 1948, traditional herbal medicine wasrecognized and absorbed by the Ministry ofHealth and Social Affairs. Regulations passedin 1952 legitimized the practice,45 but actuallicensure was never achieved. This remains as aproblem for Korea’s current generation oftraditional practitioners. In Korea the trendtowards the unified practice of traditionalpharmaceutics, acupuncture, and moxibustionwas institutionalized by the ‘Doctor of OrientalMedicine’ degree.46 This degree was officiallyrecognized and Oriental medical schools wereestablished. Generally the trend in Korea hadbeen similar to that in China — pharmaceuticalmedicine was the dominant traditional system.Thus, when acumoxa therapy was integratedwith Oriental medical curricula, acupuncturebecame an adjunct to pharmaceutics. Acupunc-ture and moxibustion are becoming increasinglypopular, especially in the treatment of strokepatients. However, Korean methods are as yetless well known in the West than are Japaneseand Chinese approaches.
The teaching of Oriental medicine in Koreaincludes basic biomedical science as well astraditional theories and techniques. Among thelatter are the Korean-founded four acupointcombinations of Sa-Am of the 16th century andthe four constitutional patterns of Lee Che-maof the late 19th century. Although there appearsto be a diversity of ideas expressed in theclinical practice of acupuncture, a system ofpractice not dissimilar to Chinese TCM isstandard.47 As in China, validation of practiceand theory through scientific research is animportant goal. One of the important figures inthis research was Kim Bong Han. He announcedthe discovery of an anatomical basis for thechannels and acupoints in a correlated corpus-
cular system.48 However, because others wereunable to reproduce his findings, they are nolonger considered valid.
Another interesting development occurred inKorea during the 1970s. This was Tae WooYoo’s discovery of Koryo Sooji Chim. Known inthe West as ‘Korean Hand Acupuncture,’ thissystem is similar to the auricular acupuncturesystems of the French doctor Paul Nogier, inthat it maps all parts of the body to a corre-sponding region — in Tae Woo Yoo’s case,regions of the hands. In his system the handsare exclusively treated.
After North Vietnam entered the Chinesesphere of influence, its leader Ho Chi Minhadopted Chinese health policy, probably inresponse to the same political and public healthpressures operative in post-liberation China. In1955, he proposed that ‘medical cadres shouldbuild on our own medicine, harmonizingEastern and Western medicine,’ a clear reflectionof contemporary Chinese policy. By 1960 theNational Congress of the Vietnamese Com-munist Party advocated the combination oftraditional and modern medicines in all fields.Supportive policy revisions were added in1961, 1966, and 1967.49
In 1973, John Levinson glimpsed traditionalmedicine in North Vietnam and found that, likeChina and Korea, traditional pharmaceuticswas the dominant practice. Trends in educationwere similar to those in China. There wereshort courses of study available, all medicalstudents were taught some traditional medicine,and more extensive training was available forthose who wished it.50 Today, Vietnamesevariations of acupuncture and moxibustionreach the West primarily through Vietnamese-born French nationals. Nguyen Van Nghi ofFrance, for example, has written several bookson acupuncture that reflect Vietnamese influ-ences. He has also interpreted Vietnameseeditions of famous Chinese texts.
After the exodus to Taiwan following theGuomindang’s defeat in 1949, medicine in theRepublic of China was dominated by biomed-icine. As the country modernized, establishingitself as a powerful economy, the popularity of
THE ACCULTURATION AND RE-ACCULTURATION OF ACUPUNCTURE 59
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 59 (Black plate)

biomedicine increased. However, the Republicof China also managed to retain much of therichness and plurality of traditional medicalpractice. Today, traditional pharmaceutics isused more than any other traditional medicine,but acupuncture and moxibustion remain rela-tively popular. Wu Huiping, a personal friendof Jiang Jieshi (Chiang Kai-shek), advocated foracupuncture, and thus it was never suppressed.As in the People’s Republic, physicians inTaiwan can practice acupuncture and moxi-bustion with less training than traditionalpractitioners. However, unlike the People’sRepublic, practices such as shamanism andgeomancy are not forbidden, and adherents inthe general population practice openly.51
Economically, Taiwan is more like Japan thanChina. Acupuncture and moxibustion mustsurvive as discretionary services in a medicaleconomy dominated by biomedicine. There arean estimated 7500 Chinese medical doctorspracticing in Taiwan. Of these, an estimated10% routinely practice acupuncture and moxi-bustion. These traditional physicians are licensedby one of two means. They can graduate froman established program such as that of ChinaMedical College, or they may study lessformally and pass both a basic and a specificexamination.52 Graduates of the China MedicalCollege learn both Chinese medicine and bio-medicine. Around 38% of the 7-year program isdevoted to the study of traditional medicine, asmall portion of which is acupuncture training.After completing the program, graduates areadmitted to licensing examinations in bothWestern and Chinese medicine, but manygraduates do not choose to sit for the Chinesemedical examination. Even those who focusalmost exclusively on Chinese medicine mustalso learn biomedicine, much as do students ofacupuncture in Japan.
The system in Taiwan provides public andprivate insurance coverage of acupuncture andmoxibustion. Labor Insurance (what is usuallytermed ‘Worker’s Compensation’ in the USA)has reimbursed acupuncture providers since1983, and government employee insurancesince 1988. In all, acupuncture and moxibustion
are relatively popular in Taiwan, but are dwarfedby both biomedicine and traditional pharma-cotherapy. The ‘leading edge’ of acupunctureand moxibustion in Taiwan, as in mainlandChina, is research. Many physicians who practiceacupuncture and moxibustion are involved inresearch. Institutions like the China MedicalCollege are famous for their research. Indeed,some of the best research published in the Westhas been done at this college.
WESTWARD TRANSMISSION
With what must now be a familiar caveatregarding the arbitrariness of chronologicalnarrative, we propose that acupuncture jour-neyed westward in rough parallel to its re-acculturation in East Asia. For this reasoncurrent Western understandings are often partial,and are often keyed to a particular person,place, or time of transmission. As acupuncturerecovered social status, economic utility, andpolitical sponsorship in China, Japan, and theother Asian nations where it had traditionallybeen practiced, it became more apparent totravelers and more worthy of mention. Its firstmodern transmissions thus came from Japan,where the American occupation, a growingpolitical and social amnity with Western nations,and rapid economic development increased thepoints of contact. At first, Chinese influencewas sporadic, as it was carried by Chinese ofvarying skills who were escaping China forpolitical or economic reasons. However, as soonas Chinese interchange with the West was re-established and a political resolution foracupuncture evolved within the CCP, it wouldagain be Chinese ideas and innovations thatdominated Western attentions.
Acupuncture in the USA
Prior to 1971, with Nixon’s opening of Chinaand James Reston’s New York Times articledetailing his experience with acupuncture forpost-surgical pain control, there was littleacupuncture available in the USA. People inAsian communities, especially the Chinatowns
60 WHAT ACUPUNCTURE IS
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 60 (Black plate)

of the east and west coasts, were certainlypracticing acupuncture, mostly for their fellowAsians. Little was known, and only a verysmall group of Americans was studyingacupuncture in California by 1969.53 The samewas true on the east coast, where only a fewpeople, largely members of the Boston mac-robiotic movement, had begun to study withlocal Chinese and Japanese teachers. FollowingJapanese management techniques, a young edu-cator, Dr Nakamura, who is today Presidentof Meiji Acupuncture College in Japan, wassent to Boston to teach and become acquaintedwith American ways. Hiroshi Hayashi, amaster of the O Zen Dai, a lineal Japanesemedicinal cooking tradition, operated a trainingprogram (Box 2.3) in which dozens ofAmericans and Europeans became apprenticed.Graduates of these programs often figured inthe westward transmission of the Japanesetraditional health professions. Toshi Hasegawa,a young Japanese surgeon, encouragedJapanese–American communications throughJapanese-language articles on the American
holistic health movement in the mainstreamJapanese press.54
In retrospect, however, these activities pro-duced a distinct cycle of interest and acceptancein the USA. In the first half of the 1970sacupuncture was a darling of the Americanmedia, but in the second half of the decade therewas a sharp decline in popularity. This wasfollowed by another slow but steady increase inthe early 1980s. Why this cycle? There areprobably several reasons. Among these is the factthat the 1970s was the decade in which 1960sstudent activists came of age. Many were com-pleting graduate and undergraduate degrees.Others were looking for nontraditional ways tosupport their young families. As the strongfeelings of the protest era were still very muchalive in Europe and America, many of itsveterans were effectively unemployable, either bychoice or due to employer bias. Thus there was aready audience for new ideas and new careers,and there were literally thousands of activiststrained in the demanding schools of grass-rootspolitical protest. The bridge between student
THE ACCULTURATION AND RE-ACCULTURATION OF ACUPUNCTURE 61
At three in the morning, a young American is sittingwith the Master, his teacher’s teacher, the ‘Emperorof a Thousand Chefs.’ One thousand being symbolicfor all, the title describes a Dai Sensei, GreatTeacher. His own teacher, himself a sensei, is theGrand Master’s principal deshi, a word that impliesnot merely the condition of being a student, but alsothat of owing an unpardonable debt, a responsibilitythat involves life-long submission to a somethinggreater than oneself. He is in the presence of twomen, one who now leads, and one who will nextlead, a lineal tradition that has lasted generations.
The meal his teacher has prepared was morethan merely delicious, it was beautiful, art for amoment, a work of skills earned by long practiceand tireless discipline. Even well-picked its remainsshow a delicate mastery. But, despite an emptybottle of Napolean Brandy, an offering to the GreatMaster bought at the expense of 3 weeks’ pay, theyoung deshi is still on edge, afraid to embarrass histeacher with some faux pas of language or custom.
He is profoundly aware that he is an imposter. Ittakes years of disciplined life and demonstrations ofrigorous skill for a Japanese to earn a place at thistable. He is here because he is a novelty, aninteresting diversion. Strongly constitutioned and
only a few years from athletic training, he can learnby example and make sensory distinctions that hisfellow American and European students seem not toperceive. He can survive this initiation of excessivedrink, sleep on the floor, live through a ritual coldshower, and be at work on time, more or lesscapable. Hardly the stuff of a full-fledged adept, butgood enough for a gaijin, a ‘foreigner.’
As Sensei teases sensei about the deficiencies ofhis copy book, notes copied character by character,teacher to student, for unimaginable years, theforeign deshi’s curiosity gets the best of his caution.He asks to learn something from this treasure,something found nowhere in his own own culture.They laugh and play act a story in English:Deshi: Sensei, I must prepare a meal for our Lordand the Chinese Ambassador. They come to speakof war and peace. What should I prepare?Sensei: ‘What do you want, war or peace?’
Maybe it is truth, maybe it is not, maybe it is astory older than any of them. But who cares, it is agood night to talk of how mind is qi, of how qi arisesfrom food, and how food is transformed by fire andthe qi of the chef, of the difference between men’sfood and women’s food, of how food is the foundationof health and the highest expression of medicine.
Box 2.3 The nervous deshi
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 61 (Black plate)

leader and organizer, war resister and entre-preneur, was short, broad, and well traveled.
Professional politics probably also played arole. Paul Root Wolpe of Yale University hasargued that the decreased interest in acupunc-ture during the latter half of the 1970s was dueto a systematic effort by the biomedical com-munity to reestablish professional authority orcultural dominance over acupuncture.55 In1973, the US Food and Drug Administration(FDA) classified the acupuncture needle, andthus acupuncture, as experimental. In 1974, theAmerican Medical Association asserted that, asacupuncture was experimental, it should onlybe practiced in the context of establishedresearch protocols by physicians and not at allby so-called ‘lay practitioners,’ including theexpert Asians of the time. Wolpe argues thatthe singular successes of acupuncture in theearly 1970s were perceived by many physiciansas a threat to their authority, just as Westernmedicine was seen as a threat when it firstarrived in China and Japan. He proposes that,by placing acupuncture in the ‘holding cell’ ofexperimental status, that threat was eliminated.
For those who participated in acupuncturelicensure efforts, it is clear that both physicianopposition and internal conflict among acupunc-ture’s philosophical and ethnic divisions retardedthose efforts. However, the extent of any physi-cian-funded opposition is unclear. And, regard-less of what future in-depth research will revealregarding the political role of physicians, thecontribution of individual physicians shouldnot go unmentioned. It was they who providedthe medical supervision without which earlyacupuncturists could not have practiced legally.Thus there are many individual physicians whohave made important contributions to acupunc-ture’s development. For example, it is certainthat the first US acupuncture school would nothave survived without the pioneering support ofJames Doyle, a Massachusetts osteopath.
Contests concerning who could or could notpractice acupuncture under the restrictions ofthe experimental label did not always go theway of physicians. In 1980 a Texas judge ruledon a restriction allowing only physicians topractice acupuncture by saying that acupunc-ture ‘is no more experimental as a mode of
62 WHAT ACUPUNCTURE IS
Licensure in Massachusetts came relatively lateconsidering that some of the first classes, nativeacupuncturists, and the nation’s first school werenear the capitol city of Boston. Delays came frominternal struggles, conflicts between Asian andAmerican supporters over a proposed Englishlanguage requirement, and a variety of politicalproblems. But, thanks to the steady efforts ofvolunteers from the New England School ofAcupuncture, the Massachusetts AcupunctureSociety, the Chinese community, practitioners, andpatients, acupuncture finally got its ‘day in court,’ apublic hearing before the appropriate legislativecommittee.
This meeting came to its defining moment when ahandsome, grey-haired, physician, the seniorneurologist at one of Boston’s prestigious medicalcenters, stepped forward to testify. Speaking directlyto the legislators, the fingers of his hands tappinglightly together as if to contact the gods of medicinein prayer, he urged them to save the residents ofMassachusetts from this impending curse. He was illinformed, the bulk of his factual information being anoverstatement of a 1977 study by George Ulett. Yet,the power of his bearing, the tone with which he
delivered words like ‘protoscience,’ his rhetoricalskill, had force. He smiled at the committeemembers as he left, thanking each personally, nodoubt just as he did when they were guests at hishospital’s fund-raising dinners.
As he left, a slender man passed him comingforward. Unannounced and uninvited, slowly limpingon his cane, he worked his way through thecrowded aisles until he stood directly before thecommittee’s table. He raised the cane, notthreateningly, but deliberatly and rapped the table asif it were he who held the chairman’s gavel – rap!rap! rap! There was silence. rap! rap! rap! ‘Don’tlisten to that man’ rap! rap! ‘These arrogant doctors’rap! ‘They said I would never drive.’ rap! ‘They said Iwould never walk.’ rap! ‘They said the only thing formy pain was their expensive drugs.’ rap! ‘I drovehere today.’ rap! ‘I walked here to tell you, don’tlisten to that man, acupuncture saved my life, andyou’re not going to take it away from me.’
He lowered his cane, and walked back to hischair. The meeting slowly returned to more mundanetestimony. But, for many there, this was the momentthat acupuncture came to Massachusetts.
Box 2.4 The grateful patient
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 62 (Black plate)

medical treatment than is the Chinese languageas a mode of communication. What is experi-mental is not acupuncture, but Westerners’understanding of it and their ability to utilize itproperly.’56 Turf wars between physicians and,specifically, trained acupuncturists have comeand gone, but today they are transforming tocollaborative efforts based on common goals.Pennsylvania is a model state in this regard.There, with the careful work of the physicianPat LaRiccia, considerable cooperation has beenachieved. In New York, the Mercy CollegeAcupuncture Program operates with the co-operation of the medical staff in the hospitalwhere its clinical training occurs.57
Although it is true that the ‘experimental’label imposed a stigma of quackery that wasexploited in anti-acupuncture lobbying, it isdifficult to find any evidence that supports thecommonly held idea that an inimicable FDAdeliberately created that barrier. At the April1994 FDA Workshop on Acupuncture, FDAofficials revealed that acupuncture was classifiedas experimental only after noone steppedforward with positive evidence. After the FDArealized that it was required to do somethingabout acupuncture because there was no evi-dence of safety and efficacy, the periods setaside for public and professional commentexpired without anyone offering evidence.Although this was clearly an opportunity thatthe acupuncture community failed to recognize,there were very few practitioners and verylittle research available in 1973. An organizeddefense of acupuncture would have beendifficult, even had the existing organizationsundertaken the effort. However, classifying theacupuncture needle as a class III (experimental)device hardly retarded the grass-roots move-ments that had already begun.
Perhaps unknown to those physicians whotried to assert their authority over acupuncturein the early 1970s, acupuncture had alreadytaken hold. By the mid-1970s it had started toestablish itself through home-grown teachingprograms, books, and increasingly formalschools. By 1974, the few acupuncture booksavailable were selling in quantities that would
not be matched until new schools would beginin the 1980s. Classes based on Soulie de Morant’swork were being taught in the USA andCanada, and acupuncture training had alreadybegun to move from teachers’ living rooms tothe storefronts and storerooms from which thefirst professional schools would begin.
Bill Prensky, an acupuncturist and now Deanof Mercy College’s acupuncture program, helpedpioneer acupuncture’s move from informal toprofessional training. In 1969 Bill and hiscolleagues Steven Rosenblatt and David Breslerfounded the Institute of Taoist Studies in LosAngeles, where they studied acupuncture withJu Gim Shek. In 1973 they brought the well-known acupuncturist James Tin Yau So fromHong Kong, where he was not only a famousclinician but also a sought-after teacher. Theyarranged for Dr So to be teacher and senioracupuncturist at the Acupuncture ResearchProject of the UCLA School of Medicine, whichthey had begun that year. After working on theproject for a year, they all moved to Boston in1974. This core group founded the two seminalUS acupuncture schools: The New EnglandSchool of Acupuncture in Boston, and TheCalifornia Acupuncture College in San Francisco.Following the founding of these two schools,both of which obtained state approval, otherstate-approved education programs beganaround the USA. Acupuncture training becamefirmly established. These developments laid thefoundation for the rapid growth of acupuncturein the 1980s.58
Another factor that contributed to the resur-gence of acupuncture was the return of youngWesterners who had gone to Asia to studyacupuncture. Among the first to become wellknown were Ted Kaptchuk, John O’Connor, andDan Bensky. After studying together in Macaoin the mid-1970s, with Bensky studying furtherin Taiwan, they produced influential books.Largely for the first time, Westerners werehearing from students who had studied inChinese settings. Kaptchuk’s 1983 book, The WebThat Has No Weaver, is still a popular presen-tation of traditional medicine practiced in modernChina. Dan Bensky and John O’Connor’s
THE ACCULTURATION AND RE-ACCULTURATION OF ACUPUNCTURE 63
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 63 (Black plate)

Acupuncture: A Comprehensive Text (1981) wasthe first publicly available translation of amodern Chinese acupuncture textbook. Thesebooks provided not only the substance of manyearly acupuncture courses, but also the data onwhich license examinations would be based.
Although it was Chinese TCM that wouldeventually dominate acupuncture in the English-speaking world, those who were finishing adecade of education and apprenticeship inJapan would also contribute. Miles Roberts, DanKenner, Peter Thompson, and others graduatedfrom the Meiji Oriental Medicine Institute inKyoto, completing not only the 3-year programbut also the demanding Japanese nationallicensure examination entirely in Japanese.Returning after 7- to 10-year apprenticeshipswith experienced teachers, they continue topromote and support the technical developmentof acupuncture with their practices, writing,and research.
The most recent estimates are that some 50acupuncture or Oriental medical schools operatein the USA, with smaller but proportionalnumbers in Europe and the Commonwealthnations. There are also several programs fortraining physicians. The early acupunctureschools formed a national council, now calledthe Council of Colleges of Acupuncture andOriental Medicine, (CCAOM), which in 1982formed the National Accreditation Commissionfor Schools and Colleges of Acupuncture andOriental Medicine, (NACSCAOM), now knownas the Accreditation Commission for Acupunc-ture and Oriental Medicine, (ACAOM). TheACAOM produced an accreditation process.The Department of Education accepted thatprogram to the professional master’s degreelevel in 1988. At present, 24 schools have beenaccredited and 10 are candidates.59 This accred-itation gives eligible students access to USstudent-loan programs, a benefit that hasresulted in a continual increase in the numberof students. The length of training in theseprograms is 3–4 years.
Training for physicians is available throughprograms such as those at the New YorkUniversity School of Medicine and Dentistry,
and the American Academy of MedicalAcupuncturists, (AAMA), originally throughUCLA. These programs have trained some 3000physicians, osteopaths, and dentists in MedicalAcupuncture, which by the mid-1980s hadbecome distinct from what is taught in ACAOMschools. Joseph Helms, founding president ofthe AAMA, was instrumental in establishing atraining program for physicians that parallelsthat for acupuncturists in extent. He adapted amodel of practice developed by France’s MauriceMussat. This differs in several seminal technicaldetails and clinical strategies from the TCMmodel. The AAMA training program satisfiesthe minimum educational standards establishedby the World Federation of Acupuncture andMoxibustion Societies, an international acupunc-ture organization.
Most schools and colleges followed the cur-riculum used in China in the 1960s, 1970s, andearly 1980s, combining acupuncture with tradi-tional pharmaceutics. Although this approachhas been replaced in China by specializedtraining in either acupuncture or traditionalpharmaceutics, many US schools prefer theintegrated curriculum, hence the designation ofschools as teaching ‘Acupuncture’ or ‘OrientalMedicine.’ Among US acupuncture educatorsthere is some friction between those promotingthe integrated approach and those promotingspecialized training. This, as well as otherfactors, led to the 1994 separation of a NationalAcupuncture and Oriental Medicine Alliance(NAOMA) from the original US practitionerorganization, the American Association ofAcupuncture and Oriental Medicine, (AAAOM)— now the American Association of OrientalMedicine (AAOM). As seen in our review ofhistory, factionalization is nothing new. Acupunc-ture, moxibustion, traditional pharmaceutics,and their several permutations of combinationhave long been matters where individualchoice and political and social constraints havemixed. Professional structures in Asian nationswere equally fragmented until their currentstructures were politically determined.
Although the establishment of formal train-ing programs helped spawn a revival of
64 WHAT ACUPUNCTURE IS
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 64 (Black plate)

acupuncture from the early 1980s onward, theissues of who can do what, and who makeswhich practice-governing decisions, are farfrom settled. There are significant discrepanciesin laws determining the scope of practice, theinclusion of traditional pharmaceutics, and theextent of training and practice independence.There are also significant differences in thedegree of physician supervision required andthe training demanded of physicians who wishto practice acupuncture. However, this issue ismostly confined to the USA. Most countries usenational regulations. With federal as well as50 state regulatory bodies, it is possible to haveup to 51 different rules on any practice issue.
This makes US acupuncture laws uniquelyconfusing and sometimes simply strange.California, which was so liberal as to requirestate insurance reimbursements in advance ofmost published efficacy research, nonethelessbans a number of non-Chinese techniques forwhich the research is good. States such asConnecticut and New York refuse to recognizeindividuals who were trained prior to theACAOM era. For example, for an establishedpractitioner like Birch to be licensed in thesestates he would need to regraduate from theschool he helped develop, where his formerstudents would train him to pass examinations
that are partly based on the textbooks he haswritten. Although humorous and moot in Birch’scase, such circumstance are not laughing matters.For example, one of the health-care organiza-tions that has most aggressively pursued com-plementary approaches in the eastern USA,Oxford Health Plans, Inc., must legally excludefrom service providers those who have themost experience.
Although US acupuncture has seen bothgrowth and decline during the last 20 years, itis currently surging, as ever more schools openup and more jurisdictions legitimize its practice.The jurisdictions that regulate or licenseacupuncture and the year in which the lawtook effect are shown in Box 2.5.60 Althougheach state has its own educational and licenserequirements, a majority have adopted anexamination promulgated nationally as thegeneric standard of minimum competence. Thisexamination was devised by the NationalCommission for the Certification of Acupunc-turists (NCCA) — now the National Com-mission for the Certification of Acupunctureand Oriental Medicine (NCCAOM), which wasformed and funded by US acupuncture schoolsin 1985.
One estimate sets the number of acupuncturelicenses issued in the USA by July 1993 at
THE ACCULTURATION AND RE-ACCULTURATION OF ACUPUNCTURE 65
Box 2.5 Acupuncture licensure approved state-by-state in the USA
1973 Nevada, Oregon1974 Hawaii, Montana1975 Louisiana1976 California1978 New Mexico, Rhode Island1981 Florida1982 Maryland1983 New Jersey, South Carolina, Utah1985 Vermont, Washington1986 Massachusetts, Pennsylvania1987 Maine1989 Colorado, Washington DC, Wisconsin1990 Alaska1991 New York1993 Iowa, North Carolina, Texas, Virginia1994 Minnesota1995 Connecticut
In 1996 and 1997, five more states have achieved licensure: Arizona, Illinois, New Hampshire, Tennessee, and WestVirginia
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 65 (Black plate)

6476.61 An FDA report of the same year byDavid Lytle estimated that there are probablyaround 9000 acupuncturists in the USA, ofwhich physicians are thought to comprisebetween 2000–3000 and while a comprehensivesurvey has yet to be conducted, recent con-servative estimates suggest that there are nowsome 10 000 practitioners in the USA, one forevery 25 000 people.62 The same FDA reportestimates that 9–12 million treatments areadministered every year, a 0.5 billion dollarmicro-economy.63 Although Eisenberg andcolleagues’ recent studies of ‘unconventional’medical practices shows that only a smallpercentage of Americans currently use acupunc-ture, the 1993 study indicated that visits toacupuncturists per patient are more frequentthan for any other complementary therapy, andthat there are signs of significant growth.64
To understand these trends, it is useful tolook at the diversity of methods and approachesfound in the USA, and some specialized usesthat are having a profound impact on US healthcare. Although most acupuncture schools focuson the TCM acupuncture that evolved between1950 and 1970 in China, a diversity ofapproaches is actually practiced. The USA haslong been known as a ‘melting pot’ of culturesand ideas, and as regards acupuncture this isstill certainly true. European acupuncture,having begun with the heritage of Soulie deMorant, now evidences a similar diversitywithin a growing TCM plurality.65
Besides the dominant TCM approach, otherChinese systems are also practiced. Theseinclude methods taught by James Tin Yau So,Tung family-style acupuncture, and otherfamilial or lineal forms imported from Taiwan,Hong Kong, or pre-liberation China. There arealso a variety of Japanese approaches, such asyin–yang balancing, keiraku chiryo, and toyohari,currently taught in the USA. Birch, his wifeJunko Ida, and their associates began the firstAmerican branches of the Toyohari Associationin 1992. Other forms of keiraku chiryo includethe yin–yang channel-balancing therapy of YoshioManaka and modern forms, such as thosetaught by Miki Shima. Nakatani’s Ryodoraku
system is practiced worldwide, often amongphysicians. The traditional acupuncture begunin the UK by Jack Worsley is also taught in USschools. A number of modern approaches fromFrance and Germany, in particular Paul Nogier’sauriculotherapy, and Rheinhold Voll’s EAV(electro acupuncture according to Voll) aretransmitted through programs for workingacupuncturists. Yves Requena’s Terrain systemis taught through seminars at the largestacupuncture school in the USA, the PacificCollege. Korean and Vietnamese systems, forexample, Korean constitutional acupuncture orTae Woo Yoo’s hand acupuncture, are also taughtand practiced.
The fastest growing acupuncture programin the USA was pioneered by Michael Smithat the Lincoln Hospital in Bronx, New York. Itapplies acupuncture as part of a comprehensivedrug rehabilitation program. First used byH. L. Wen of Hong Kong in 1972, this treat-ment has proven to be a valuable part of acomprehensive therapy for drug addiction. Justas the systematized use of acupuncture inChina served a necessity for which Westernmedicine was unprepared, acupuncture is nowplaying a growing role in this critical problem.
Drug abuse is one of the largest public healthproblems in the West, especially the USA. Thereare an estimated 18 million people who abuseor are addicted to alcohol, 12 million whoabuse prescription drugs, and approximately1 million heroin addicts in the USA alone.An estimated 2 million people use cocaineevery week.66 Drugs that cost pennies toproduce have huge street values, so the largestproportion of crimes are committed in orderto be able to afford illicit drugs. A recent studyof 573 hard drug abusers in Miami found thatin 1 year their crimes were as follows:67
• 6000 robberies and assaults• 6700 burglaries• 900 automobile thefts• 25 000 acts of shoplifting• 46 000 other larcenies or frauds.
This is a total of 84 600 crimes, an average of148 crimes per addict per year. Clearly, sub-
66 WHAT ACUPUNCTURE IS
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 66 (Black plate)

stance abuse is an immense burden on publichealth and safety.
Standard treatments for substance abusehave clearly proven inadequate. Among thosereceiving standard treatment for drug addictionthere is at least a 60% recidivism – 60% returnto use driven by their addiction. For example,one of the standard therapies for heroin addic-tion is the daily administration of methadone.Recent studies have found that upwards of60% of these so-called ‘maintained addicts’were abusing cocaine and other drugs, despitemethadone treatment. There is essentially nostandard treatment for cocaine or crack-cocaineabuse, the worst of inner-city problems.
It is here that the pioneering work ofpractitioners such as psychiatrist Mike Smith inthe Bronx, Pat Culliton in Minneapolis, AnaOlivera in New York, Janet Konefal in Miami,David Eisen in Oregon, Lianne Audette in LosAngeles, Joe Kay in Boston, and their col-leagues in more than 600 centers have had asignificant impact. In fact, what is sometimescalled ‘acupuncture detoxification’ has been sosuccessful that various state authorities haveadopted acupuncture as a rehabilitation tool.
The US Attorney General Janet Reno andFirst Lady Hillary Clinton’s brother HughRodham were involved in establishing the drugdiversionary program in Metro-Dade County,Florida, together with judges Herbert Klein andStanley Goldstein. In Metro-Dade County, as inmany places, courts and prisons are over-whelmed with repeat drug offenders. In 1988the failure of the system inspired the ChiefJustice of the Florida Supreme Court to sendAssociate Chief Judge Herbert Klein to tour theUSA looking for answers to the crack-cocaineproblem. He found Mike Smith and theprogram at the Lincoln Hospital in the Bronx.Agreeing that it would be more useful torehabilitate rather than punish drug offenders,Klein and his associates set up an experimentaldrug diversion and treatment program withJudge Goldstein on the bench.68
Starting in 1989, drug offenders were offeredthe choice of prison or rehabilitation. Rehabili-tation involves four phases: I, detoxification
(featuring acupuncture); II, counseling (withfollow-up acupuncture); III, education or voca-tional assessment and training; and IV, gradua-tion. Successful completion of the program,‘graduation,’ requires ‘clean urines’ (no chem-ical signs of drug use) and no re-arrest for anyreason for 1 year. The program coordinator TimMurray estimates that, between June 1989 andMarch 1993, 4500 entered the program and that60% graduated or are still in the program. Ofthose who have graduated, only 11% have beenre-arrested on any criminal charge. With normalrecidivism rates six times higher, this is anunqualified success.69
This is not the only accomplishment. AnInstitute of Justice study found that the Metro-Dade County program (between June 1989 andMarch 1993) had to drop fewer cases, had lowerincarceration and re-arrest rates, and had a sig-nificant increase in time before re-arrest. Thosenot re-arrested increased from the standard45% to 52–67%. Time before re-arrest rose from75–88 days to 235 days.70 This implies that halfof those who entered the program refrainedfrom all criminal activity. In simple terms thisis a reduction of 330 000 crimes per year justamong the 4500 persons in the Miami diversionprogram. Whether or not this estimate isaccurate, it is clear that no other program hascome near to these results and that the socialbenefits are immense. Tim Murray estimatesthat the program costs about $800 per clientper year, the cost of 9 days in jail.71
An innovative pilot study at the SantaBarbara County Jail explored the role ofacupuncture in preventing ‘post-acute with-drawal syndrome,’ which is thought to con-tribute to re-arrests following release from jail.Alex Brumbaugh and his colleagues treatedinmates during the 30-day period prior to theirparole. They treated 51 inmate volunteers, 85%of whom had a history of abusing alcohol oranother drug. Inmates who received 24 or moretreatments during their last 30 days ofincarceration were two-thirds less likely to bere-arrested in the 2 months following releasethan were those who received six treatments orless.72 Although this is a pilot study from which
THE ACCULTURATION AND RE-ACCULTURATION OF ACUPUNCTURE 67
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 67 (Black plate)

sweeping conclusions should not be drawn, thepotential it indicates is clearly important.
Currently, both state and federal prisonofficials, courts, and judges are interested inacupuncture rehabilitation programs. In mid-1994 there were 30 documentable programs,operating in, for example, California, Minnesota,Alabama, Oregon, Texas, Missouri, Nevada,New York, Arkansas, and Washington, DC, withplans for many more in process. Although acrime bill submitted by the Clinton adminis-tration contained substantial funding for theseprograms, these funds would never reach thosein need. That bill became the center of a nationalpartisan conflict in which it was defeated.
Despite political failures, several major devel-opments have occurred in the USA. Theseinvolved major government acceptance ofacupuncture at a level unprecedented in theWest. Since 1973 the US FDA has classified theacupuncture needle as an experimental device.73
This meant that acupuncture needles couldonly be used in experimental studies. This hasbeen a major impediment to mainstream accep-tance of acupuncture. Pressure to change thisclassification began in the early 1990s, andresulted in a major Workshop on Acupuncturein April 1994. The workshop was jointlysponsored by the FDA and the Office ofAlternative Medicine at the National Institutesof Health. Leading US and internationalresearchers assembled to present the best evid-ence of acupuncture’s efficacy. FDA researchersthen scrutinized the data in preparation for acitizens’ petition to classify the acupunctureneedle as safe and effective.
Five major areas of effectiveness wereidentified for which reasonable data fromclinical trials existed: pain, respiratory disease,substance abuse, rehabilitation from centralnervous system damage, and emesis. After wait-ing for more than a year, the FDA reclassifiedthe acupuncture needle as safe and effective.However, this approval was not based on theweight of evidence, as none of the indicationsof effectiveness was approved. Rather it was‘grandfathered’ by long-term use74 (see Ch. 5).Birch, who was the principal author of the
‘pain’ submission and helped compile the otherfour submissions, suggests that the workshopwas successful despite its less than idealconclusion, in part because it was needed forthe next step of approval.
In November 1997, a Consensus DevelopmentConference on Acupuncture was convened atthe National Institutes of Health. This con-ference also involved evidence on the nature,practice, and effectiveness of acupuncture for avariety of conditions. A panel of independentexperts reviewed and weighed the evidence.They issued a finding very favorable toacupuncture, simultaneously calling for moreand better research.75 The full implications ofthis conclusion and the FDA approval are toorecent to be fully understood. However, it isclear that a door has opened to the wideracceptance and practice of acupuncture, a topicwe will revisit later in this text.
Acupuncture in the UK
Acupuncture began to emerge in the UK in the1960s. There were two major movements. Thefirst focused on physicians, the second on thosespecifically educated as acupuncturists.76 Physi-cian practitioner Felix Mann had begun towrite about acupuncture. This helped found amedical acupuncture movement that is stillpresent in the UK today. Mann described tradi-tional theories, concepts, and practices, helpingto popularize acupuncture for English-speakingreaders. But he eventually rejected traditionalexplanatory models in favor of scientific expla-nations that he proposed. His books have beeninfluential; they were arguably the most com-prehensive English-language works until theearly 1980s.
The acupuncture movement in the UK prim-arily centered around three individuals whoinitially studied and formed a school together,but then, after disagreements, each started theirown schools. These were Messrs Worsley, VanBuren, and Rose-Neil. Worsley began the move-ment called ‘traditional acupuncture,’ which isstill popular today in both the UK and theUSA. It is estimated that most of the acupunc-
68 WHAT ACUPUNCTURE IS
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 68 (Black plate)

turists in the UK were trained at Worsley’sschool at Leamington Spa.77 Van Buren andRose-Neil’s schools have perhaps been lessinfluential, except within the UK. Since theearly 1980s when practitioners and studentsstarted going to China to study, a number ofTCM-based schools have also begun.78 Theseschools sponsor a seminar circuit for popularauthors that is making ideas about acupuncturerelatively more homogeneous in the English-speaking nations.
The various UK schools, although initially inconflict with each other, have begun the sameprocess that the US schools began — that ofaccreditation, as well as a movement towardscertification and licensure.79 Currently there isno license for acupuncture in the UK; itspractice is allowed by common law. Thus thelegal pressures operative in Asia and the USAhave played a lesser homogenizing role. Thereare practitioners who are not graduates of anyschool, graduates of correspondence courses,and practitioners with various amounts ofapprentice training. Today, UK schools aregenerally following the non-academic accredita-tion strategy used in the USA. However, someschools are academically accredited and offeracademic bachelor’s or master’s degree.80
In an effort to organize as better educatedpractitioners, and to unite in the face of possi-ble European Economic Union rules that couldpotentially restrict the practice of acupuncture,graduates of these acupuncture schools haveformed an umbrella register. Today there are anestimated 1500 members.81 Yet, there is no clearestimate of the total number of UK practi-tioners. Assuming that UK and US attitudes arebroadly similar, we can guess that the practi-tioner ratio in the UK is similar to that in theUSA (i.e. about one practitioner per 25 000population).
Acupuncture is partially covered by theBritish National Health Service (NHS). Practi-tioners who work within an NHS clinic, forexample physicians working in a hospital,receive NHS reimbursement for acupuncture.However, since the early 1990s restructuring ofthe NHS, acupuncturists receive NHS funds
only if they work through a general practi-tioner’s clinic.82 A recent survey of members onthe National Register found that as many as18% of respondents were working in NHS-based practices; 55% receive referrals fromphysicians working within the NHS.83
There are also organized efforts towards moreand improved research in the UK. George Lewithand Julian Kenyon’s Center for the Study ofComplementary Medicine in Southampton, theacademic center at the University of Exeter, theCentre for Complementary Health Studies,started by Simon Mills and Roger Hill, andrecently joined by Edzard Ernst, and the London-based Research Council for ComplementaryMedicine are actively pursuing this goal. Someof the best research on acupuncture has comefrom these centers, notably the work done byGeorge Lewith and Charles Vincent. The Princeof Wales, Prince Charles, initiated an explo-ration of how complementary medicines, includ-ing acupuncture, can be moved towards furtherintegration with biomedicine. The group hecommenced recently published a report thatdiscusses research strategies to assist thatintegration.84
Generally, acupuncture is relatively popularin the UK, with significant cultural and politi-cal support. The Queen has a personal acupunc-turist, Prince Charles and the late PrincessDiana have used acupuncture. Rumors aboundthat even the Conservative Party ex-leaderMargaret Thatcher uses acupuncture. Today,acupuncture is a slowly growing but firmlyrooted system in the UK, with levels ofutilization similar to those in the USA and nopowerful political or economic disincentives.
Acupuncture in the Commonwealthcountries
In Commonwealth countries such as Canada,Australia, and New Zealand the situation issomewhat similar. There are both physicianand acupuncture groups in each country thatare to some extent competitive. Recent socio-logical research from Australia traces a historyof acupuncture, particularly acupuncture schools,
THE ACCULTURATION AND RE-ACCULTURATION OF ACUPUNCTURE 69
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 69 (Black plate)

that is very similar to that in the USA.85 InAustralia three acupuncture schools operatewithin university programs and provide theirgraduates with a formal degree. There areplans for more university programs. Over 4500practitioners have been identified in Australia,86
which, with a population of less than 20 million,gives an approximate ratio of one practitionerfor every 3800 persons, a higher use of com-plementary medicines than Eisenberg reportsfor the USA. MacLennan et al87 estimate thathalf the Australian population (as compared toover one-third of the US population88) haveused an alternative medicine. Thus, there areseveral evidences of a greater utilization ofacupuncture in Australia than in other English-speaking nations.89 The physician acupuncturegroups such as the Australian and the NewZealand Medical Acupuncture Societies havegrowing memberships with well organizedtraining programs. In Quebec, where there is alarge French-speaking population, French influ-ence is, of course, strong. Yet, at present it isChinese TCM that appears to be the mostinfluential trend. French writers such as Nogier,Soulie de Morant, Chamfrault, and Requena,and Quebequois such as Oscar and MarioWexu remain influential.
Acupuncture in European nations
The situation for acupuncture in the rest ofEurope is somewhat different than in theEnglish-speaking countries. Each country inEurope generally has both a different set ofrules and a different level of extra-legaltolerance. Many countries only allow physiciansto practice acupuncture, for example, France,Belgium, Denmark, the Scandinavian countries,and Italy. However, acupuncturists are toleratedthrough unambitious enforcement of theseexclusionary laws.
The oldest and most established school in theNetherlands, the Anglo-Dutch Institute forOriental Medicine, was established in 1972.This school has primarily trained physiciansand physical therapists in acupuncture. Thisemphasis arose not only because the founders
thought it more practical to train people whoalready possessed a medical training, but alsobecause until recently the practice of acupunc-ture was legally restricted to physicians andphysical therapists. However, when the Dutchgovernment realized that there were thousandspracticing who were neither physicians norphysical therapists, and that more than 20schools existed to train them, laws governingthe practice of acupuncture were liberalized.90
With a population of 16 million and anestimated 5000 practitioners or more, there isabout one practitioner to every 3200 people inthe Netherlands. Birch currently practices inHolland, teaching throughout Europe.
Not all European nations have tried torestrict acupuncture practice to physicians. Forexample, in Germany there are estimated tobe 20 000 to 30 000 physicians who practiceacupuncture (somewhere between 10% and 20%of practicing physicians),91 and possibly asmany as 2000 who trained as heil-praktikers ornatural therapists (Heil-praktik, ‘health practice,’is a movement that began in the 1930s andallows a broad choice of healing disciplines).The practice of acupuncture in Germany wasinfluenced by acupuncture in Japan, just asJapanese medicine was influenced by Germanmedicine before the Second World War. In the1950s, Sorei Yanagiya taught there, paving theway for the introduction of a variety ofJapanese approaches, particularly Keiraku chiryo.In fact, one of his students, Herbert Schmidt,who also studied in Japan with Yoshio Manaka,was one of Worsley’s teachers. This lineageresulted in a significant Japanese influence inthe traditional acupuncture movement thatWorsley began, a fact that has only recentlybeen made public through Peter Eckman’sresearch.92 Europe’s colonial history also con-tributed to acupuncture’s European accultura-tion. As a French colony, Vietnam influencedEuropean acupuncture both through Vietnamesepractitioners who lived in France and theFrench who lived in Vietnam.
The opening of relations with China in theearly 1970s attracted the same attention inEurope that it attracted in the USA and UK.
70 WHAT ACUPUNCTURE IS
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 70 (Black plate)

However, because acupuncture was alreadyestablished in Europe, a more rapid assimila-tion was accomplished within the establishedmedical systems. With a larger percentage ofphysicians practicing acupuncture, some as amedical specialty, acupuncture appears to bemore widely used in Europe than in the USAand UK. In France, where physicians have beenable to study acupuncture as a medical subspe-cialty for about 4 decades, there are now anestimated 10 000 physicians practicing acupunc-ture. Over 20% of the population of France hasused or continues to use acupuncture.93 This ismuch greater than the approximately 1%utilization in the USA and the UK.94 Taken as awhole, the situation in Europe is comparable tothat in the USA, where each state has its ownset of rules and regulations, sometimes incontradiction. Part of the reason for the widerEuropean acceptance is that more literature hasexisted for a longer time, and East Asian infor-mation has thus been more directly available.Many of the most noted sinologists andacupuncture experts have been European. Wehave noted George Soulie de Morant’s instru-mental work in several instances. However,writers such as Marcel Granet, the author of LaPense Chinoise (Chinese Thought) also contributedto the acculturation of acupuncture in Europeby making Asian philosophies more available.
However, it is important to note that Euro-pean acupuncturists did not simply copy; ratherthey innovated, fully participating in theongoing adaptation of acupuncture. Investi-gating the healing effects resulting from cauter-izing a region of a patient’s ear led Paul Nogierto discover a system of ear acupuncture.95 Thissystem was adapted by the Chinese who thencreated their own elaboration. During the 1950s,while Yoshio Nakatani was making electricalmeasurements of the channel and acupointsystems in Japan, developing the system nowknown as Ryodoraku, Rheinhold Voll wasconducting similar experiments in Germany.Voll’s system differs from Nakatani’s (whichwill be discussed later in the text) and isknown now as EAV (electro acupunctureaccording to Voll).96 Just as Manaka and others
such as Tsugio Nagatomo were researching theeffects of two-metal contact in Japan, similarwork was performed in Germany by GerhardBachmann.97 At the same time that the heavierneedling techniques that are typical of TCMacupuncture were being developed in China,much lighter needling techniques were beingdeveloped and utilized in Europe, simulta-neous with similar developments in Japan.
Although often unnoted outside of Europe,considerable basic and clinical research has alsobeen conducted. When it became acceptable forphysicians to practice acupuncture in France(the first regulations were formulated in 1952),physicians and researchers also began to inves-tigate acupuncture. Researcher-practitioners,such as Niboyet and de la Fuye in Franceand Bischko and Kellner in Austria, have madesignificant contributions. European centersof sinological research have long been active,for example Joseph Needham’s institute atCambridge. Paul Unschuld has established aproject for the collation, philological study, andtranslation of the Nei Jing at the Institute forthe Study of the History of Medicine at theUniversity of Munich Medical School. There,working with Asian and European scholars andthe generation of PhD candidates for whomhe is an inspiration and advisor, ProfessorUnschuld has helped advance the standards ofChinese medical collection, translation, andstudy throughout the world.
Acupuncture in the former USSRnations
Acupuncture arrived in the USSR in the mid-1950s. After the 1949 revolution, the isolatedChinese could only turn to their communistneighbors for assistance. Political ties with theSoviet Union began in 1953, and not longthereafter medical methods and techniqueswere exchanged.98 The Soviets had alreadyestablished a three-tier system of medical train-ing. This system influenced the Chinese, whoadopted versions of it for both modern andtraditional medicine. In China there were 4- to5-year programs for physicians or traditional
THE ACCULTURATION AND RE-ACCULTURATION OF ACUPUNCTURE 71
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 71 (Black plate)

72 WHAT ACUPUNCTURE IS
doctors, 2-year programs for assistant doctorsand assistant traditional doctors, and 3- to6-month programs for paramedics. Later therewere somewhat longer programs for BarefootDoctors (in the USSR these rural health workerswere called feldshers).
What the Soviets imported was a ‘scientifi-cally scrubbed’ acupuncture that became knownas ‘reflexotherapy.’99 It was and is practiced byphysicians. Although acupuncture is practicedby those specifically trained as acupuncturists itis not officially recognized; rather it is tolerated.‘Reflexotherapy’ became the neutral term chosento label the wide variety of acupunctureapproaches imported from China, Japan, andEurope. Generally, however, it incorporatesthose systems of practice that have been judged‘scientifically validated,’ and is thus essentiallyvoid of traditional explanations. It is generallytaught to physicians in postgraduate medicalcolleges, but is only partially centrally controlledor researched. It is used for a reasonably broadrange of conditions. For example, it was report-edly used in military front-line medical centersduring the Soviet army’s tenure in Afghanistan.
Acupuncture is also practiced in Russia aspart of what is called ‘Traditional Medicine,’and is one of the many traditional methods oftherapy that are practiced there.100 Currentlythere are over 30 centers in Russia that teachspecialized courses in Traditional Medicine tomedical students and postgraduate physicians.There are more than 30 large research institutionsinvestigating these therapies. Eugene Bragin ofthe Institute of Traditional Methods of Therapyin Moscow is a leading Russian proponent ofacupuncture. He reports that acupuncture andother traditional methods are being increas-ingly selected by both physicians and patients.Most hospitals and medical centers havedepartments of Traditional Medicine for both inpatients and outpatients.101 Viktor Praznikov ofthe same institute notes that this increasedutilization is largely the result of problems inthe distribution of biomedical care in Russia.102
From the USSR, acupuncture was also quicklydisseminated to East European countries. Theretoo it has typically been practiced by physi-
cians. It is used in Romania, East Germany,Hungary, Czechoslovakia, Poland, and virtuallyall the former Soviet bloc. It was officiallyacknowledged as a medical treatment inRomania in 1958 under the leadership of DrBratu. It is now taught in 3-year postgraduatetraining programs as a medical specialty, and isthought to be practiced by as many as 1000physicians, with approximately 5% of physicianspracticing acupuncture alone.103 In December1996 the Polish News Agency estimated thatover 1000 physicians have ‘learned to cureillnesses using traditional Chinese acupunctureand moxibustion.’
With the lifting of the iron curtain, acupunc-ture has also been adopted into public healthprograms. Substance abuse is a significant prob-lem in Eastern Europe and Russia, just as it isin the West. After practitioners in Eastern Europe,especially in Hungary, heard of the NationalAcupuncture Detox Association (NADA) move-ment in the USA, senior acupuncturist PaulZmiewski, who had already helped found aUS school,104 moved to Hungary to establishsubstance abuse programs. Before his untimelydeath in 1993, the program Paul began inBudapest was adopted by the Hungariangovernment as a national model.
The trends of medical practice in the formerSoviet bloc mirror the broader trends of recenthistory. Acupuncture was assimilated only whenit was labeled as ‘scientifically validated.’ Thiswas true regardless of the level or system inwhich acupuncture was eventually settled. Thiswas determined by economic factors. In theSoviet bloc there were already sufficient numbersof mid-level health workers and paramedics.Thus acupuncture was assimilated as a phy-sician’s specialty. In China and North Vietnam,where poverty, insufficient resources, and mas-sive pre-existing health problems demandedgovernment attention, acupuncture was adopt-ed to different extents at each level of practice.In Japan, where biomedical dominance of themedical system was more complete, bothpolitically and practically, acupuncture was notso much assimilated as given a chance tocompete at something of a disadvantage.
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 72 (Black plate)

A summary of westwardtransmissions
The principal events that occurred in theacupuncture field after the end of the SecondWorld War are summarized in Box 2.6.
MODERN WESTERN INTELLECTUALTRENDS
If any modern Western history of acupunctureis preliminary, the intellectual history of itsWestern transmission is at best an outline.
THE ACCULTURATION AND RE-ACCULTURATION OF ACUPUNCTURE 73
Box 2.6 The principal events in the field of acupuncture since the end of the Second World War
1947 Following Douglas MacArthur’s attempt to eliminate acupuncture and moxibustion in Japan,effective personal and public protest resulted in proposals for testing and licensing procedures
1948 Licensing procedures were enacted in Japan1948 Traditional medicine including acupuncture and moxibustion, was promoted in KoreaEarly 1950s Chinese traditional medicines received support from Mao and others sympathetic to Chinese
cultural demands. Political committees were formed to scientize and standardize traditionalmedicine, so that it could contribute to the country’s vast primary-care needs. The major traditionalmedical schools were established. Soulie de Morant’s publications become available in French
1950s Acupuncture and moxibustion developed in France, Germany, Austria, and other European countries1952 The first official ruling on acupuncture and moxibustion in France limited the practice of
acupuncture to physiciansMid-1950s Acupuncture and moxibustion were exported to the USSR and from there to other Eastern bloc
countries. For example, Romania officially adopted the practice in 19581957 The treatment repertoire of Soulie de Morant’s influential text L’Acuponcture Chinoise was
published posthumously.1958 Mao declared ‘Chinese medicine is a great treasure-house! We must make all efforts to uncover
it and raise its standards’1958–1959 The ‘Great Leap Forward’ in China; traditional and modern medicine began to be integrated1960 Acupuncture and moxibustion were integrated into the health-care system in Vietnam1960s Acupuncture and moxibustion started to be promulgated in the UK through the works of Mann,
Worsley, and othersLate 1960s Proponents of traditional and scientific schools of thought concerning acupuncture and
moxibustion competed in Japan1965–1966 The first controlled clinical trials of acupuncture were conducted by Kinoshita and Okabe in Japan1969 The Barefoot Doctor program in China began1971 James Reston wrote about his postsurgical acupuncture experiences; acupuncture made headlines
in the West1972 American President Richard Nixon visited China. Starting in this year acupuncture and moxibustion
were either introduced to, or strongly developed in, many countries: the USA, the UK, Australia,France, Germany, Austria, Italy, Finland, Norway, Denmark, Sweden, Spain, Eire, Portugal,Greece, Belgium, the Netherlands, Canada, New Zealand, South Africa, Ghana, Nigeria,Pakistan, to name but a few
1972 onward Acupuncture and moxibustion grew on all continents, either as a newly introduced therapy orfrom indigenous ethnic Chinese and Asian communities
Post-1972 Many clinical trials of acupuncture began to be conducted around the world, especially in theUSA and Europe
1972 Dr Wen of Hong Kong described the first use of ear acupuncture as a drug detoxification therapy1977 The WHO adopted the ‘health for all by the year 2000’ policy1978 The WHO began advocating the use of traditional medical practitioners to aid in the
dissemination of health care to all, ‘including the promotion of acupuncture/moxibustion, providedthat the therapies are adequately tested and shown to be safe and effective, and so long as theskills and knowledge of the traditional practitioners are upgraded’
1980 The Chinese Government put forward the principle that ‘traditional medicine, Western medicineand the combination of the two are three parallel forces,’ and that therefore attention should begiven to ensuring their coexistence and development
Early 1980s The first authentic texts on acupuncture, based on the work of influential practitioners who wentto China to study the medicine, were published in English. TCM was introduced into the USAand UK. These texts spawned significant developments for acupuncture in the USA and elsewhere
Mid- to late 1980s Increasing numbers of texts on acupuncture were published, including the first of recentJapanese acupuncture texts. As TCM continued to expand in the USA, other systems such asJapanese and Korean acupuncture methods established a firm foothold
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 73 (Black plate)

Foremost, it is far from complete. It is alsolargely unexamined. However, acupuncturecannot be understood until we recognize theintellectual trends of its acculturation. Thewestward transmission of acupuncture has mostoften been the work of enthusiasts and entre-preneurs whose only interest was clinicalapplication. With notable exceptions, academicsinology has played a lesser role. Acupuncturewould never have become as broadly andsuccessfully introduced without this narrowlyfocused transmission. However, what is todaycommonly believed has only rarely been subjectto academic methods or open critique.
In Western acupuncture communities the factthat acupuncture is adapting to the West, justas it has adapted in East Asian cultures, has yetto be incorporated into acupuncture education.As we have seen, acupuncture theory wasreformulated in China to assure politicalsurvival. In Meiji and post-Meiji Japan it wasscientized; in the USA and other Westernnations it is also subject to the modifying forceof political, economic, and cultural demands.Yet this is rarely noted in the training of eitherspecifically trained or physician acupuncturists.
There are also important transmission issuesthat have only begun to be scrutinized. Westernstudents are trying to understand traditionalpractices that are transmitted with Asianterminologies that are so old and specializedthat even native Chinese speakers requiretranslations into modern characters and idioms.So too, the philosophical orientations thatWesterners identify as inherent to beingChinese are in reality as specialized in China asin the West:
Each new generation in China finds the ancientphilosophies increasingly alien. The doctrines of yinand yang and the five phases have lost their rank asthe obvious way of understanding reality; they areno longer part of school or family education, and haveto be painstakingly learned. The medicine thesedoctrines serve is today cognitively isolated. Incontrast, the modern sciences and technology, physicsand mathematics, are part of the education of everyChinese child. They have made their imprint over thewhole of private and professional life, making modernmedicine automatically, as it were, appear to be true.105
Thus, without discipline in selection and trans-lation, and without secure means of judgingthe clinical efficacy of adapted ideas, somemistransmission is highly likely.
During the early years when acupuncturepioneers defied law and convention to giveacupuncture force in numbers and thecredibility of success, little attention could bepaid to technical issues, understanding alienconcepts, or the need for developing appropriatesystems for insuring clinical validity. Becausemany hoped that acupuncture would providewhat they found lacking in modern medicine,acupuncture’s development concentrated on theelements that most encouraged those hopes. Thephilosophical unity of traditional concepts wasoften seen as a solution to the fragmentationand alienation of modern society; thus acupunc-ture’s traditional and sometimes mundane rolein day-to-day symptom resolution is stilllargely ignored by writers, who concentrate onits holistic features. In the same way, loosetranslations of Asian literature make it easier topropose loose parallels to modern science,sometimes at the expense of traditional ideas.
In the simplest sense there are two mainissues: authenticity and clinical validity. Deter-mining whether an idea is authentic, when andwhere it fits into the massive literate and oraltraditions, is no simple feat. It requires a spe-cialized knowledge of language and literature,a broad understanding of cultural and philo-sophical developments, as well as a familiaritywith history, politics, and economics. As wewill discuss in much greater detail later in thistext, ideas of how to determine what is clini-cally valid are only beginning to mutuallyserve the needs of both scientists and acupunc-turists. Importantly, both of these issues are solarge that their resolution is neither individualnor field-specific. Rather, it depends upon thedevelopment of multidisciplinary methods andcooperation.
Because the largest transmission of modernWestern ideas about acupuncture occurredwithout either scrutiny by Western academicsystems or the master–apprentice safeguards ofthe East, anomalies in how acupuncture is
74 WHAT ACUPUNCTURE IS
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 74 (Black plate)

understood were certain. For example, thosewriting on acupuncture rarely note that there isa difference between cultural continuity andtechnical equivalence when discussing the med-icine of ancient dynasties. Although such issuesmay seem mere academic niceties, scholarlymethod is in fact of considerable importance toworking acupuncturists. A good example ofhow mistransmission has affected both theconception and practice of acupuncture is arecently promulgated model of the qi jing bamai, or eight ‘extraordinary vessels’ (which arediscussed briefly in Chs 3, 6, and 7). Althoughtechnical in detail, you need not know muchabout the extraordinary vessels to understandthis transmission problem. Furthermore, thisexample is interesting because it results not ina single clinical error, but in the loss of theclinical variety and adaptability that has con-tributed to acupuncture’s success. In effect, iteliminates or waters down an entire set ofclinical tools.
Some English-language authors propose thatthe extraordinary vessels store and circulate thejing (essence)106 and yuan qi (original qi),107 orboth.108 We will discuss these concepts later ingreater detail; they are qualities essential tohuman life. Many of these authors propose aclose connection between all the extraordinaryvessels and the shen, or kidneys,109 and throughthe kidneys to the jing qi and/or the yuan qi.These too are entities with critical importancefor human health. Each describes a quality thatis easily lost and hard to regain. Simply put,this particular set of channels is said to play asignificant role in the distribution of energiesthat is critical to human health. Because Westernwriters think of all these entities as energy, andenergy is a straight-line phenomenon, theyassume that needling the extraordinary vesselsmust deplete these essential energies. Putsimply, the extraordinary vessels are concep-tualized as a circuit that can drain the batteryof human life without regard to the metaphoricquality of the traditional concepts.
As we will discuss in Chapter 3, this material-ization of qi-related phenomena is itself aproblematic trend. However, what is important
here is that this concept is novel. The traditionalliterature concerning the extraordinary vesselsis very diverse and often contradictory.110 Thislikely indicates that these theories and theirclinical applications developed after those ofthe regular channels, the jing mai.111 However,even within this considerable variety, there areno primary sources that support this description,nor is there an obvious literature of contraindica-tion and restorative treatments for the iatrogenicdamage this idea implies.112
A review of passages concerning the extra-ordinary vessels in the principal texts thatdiscuss them, the Huang Di Nei Jing Su Wen,Huang Di Nei Jing Ling Shu, Nan Jing, Shi Si JingFa Hui, Zhen Jiu Da Quan, Zhen Jiu Ju Ying,Zhen Jiu Da Cheng, and Qi Jing Ba Mai Kao,113
reveals no explicit mention of any associationbetween the extraordinary vessels and jing qi oryuan qi. Only one of the extraordinary vesselswas traditionally described in relation to thekidneys, although two, in some descriptionsthree, intersect the kidney channel. Interestingly,two authors who claim to be transmitting themodern TCM system also claim these associ-ations,114 despite the lack of such claims inChinese-language TCM texts.115
When naive students and other authorsuncritically accept these associations,116 and usethem to extrapolate clinical principles, theimplications become profound. In this case,clinicians are told that needling the extra-ordinary vessels expends and damages jing.117
Logically then, treatment of the extraordinaryvessels with any regularity would be harmfulto human health. What well-meaning clinicianwould consider their use or study the meansand methods of treatments that employ them?
Ironically, a clinical alternative that has a pos-itive reputation in a broad selection of authen-tic traditional East Asian literature has begunto acquire a negative reputation in the West.Thus, the work of many practitioners, in manyeras, will not be consulted because of assump-tions that stand upon no firm traditional ground.Because of this misunderstanding, studentsignore, practitioners fail to learn, and patientsare denied potentially effective treatments.
THE ACCULTURATION AND RE-ACCULTURATION OF ACUPUNCTURE 75
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 75 (Black plate)

Where did these misconceptions come from?The likely origin is earlier European ‘translations’of acupuncture texts.118 This idea appears tooriginate with the French authors AlbertChamfrault and Nguyen Van Nghi, whosewritings during the 1960s were among the fewbooks available in a Western language.119 Theseauthors appear to have promoted a novelmodel whereby yuan qi is associated with theextraordinary vessels.120 Chamfrault and VanNghi cite Chapter 62 of the Ling Shu asjustification,121 although none of the versionsof the Ling Shu we consulted had any suchreference.122 Neither does Soulie de Morant’simmense, and then-available, French-languagecompilation of Chinese acupuncture literature.123
This supports Peter Eckman’s conclusion thatthis idea may originally be of Vietnameseorigin.124 Put simply, an idea that is at best anAsian or European variant has come to standfor the entire tradition because there are toofew scholarly safeguards protecting the trans-mission of that tradition.
What is most important here is that facts inTraditional East Asian Medicine (TEAM) do notexist outside of context and, if transmittedwithout that context, they are easily altered byreaders’ expectations. Because the force of thoseexpectations has not been routinely restrainedby referencing and translation disciplines, ideasin acupuncture have become more idiosyncraticthan they actually are. For example, the extra-ordinary vessel model just discussed wasassimilated by many clinicians and writers whoused Chamfrault and Van Nghi as sources –clearly evidencing the danger of one-and-onlytextbooks and secondary sources. Only one ofthe authors cited who assert an associationbetween the extraordinary vessels and the jing qi,yuan qi, and/or kidneys claims to have trans-lated Chinese, and he cites no sources for thosestatements.125 Thus, an understanding of theextraordinary vessels that is less founded in thesource literature than the ideas it has replacedbecomes ‘standard.’
Again, the most important issue is, why? Thisidiosyncratic understanding has influencedpractitioners, because its authors became popu-
lar in the West and the education system hasyet to provide a sufficient means of peerreview. For example, there has never been anysinological review of the facts demanded ofstudents on licensing examinations. Further-more, there is literally no way to challengethose ideas. This is very important because, asPaul Unschuld has noted, there is a strongtendency among Westerners to accept whatevernotion best fits Western needs.126 Because thisidea fits best the behavior of energy in Westernthought — linear, point-to-point, circuit-likerelations — it appears natural, and thus true toWestern minds. Because it satisfies the Westerncraving for integrated knowledge, it is easilyaccepted. Because theories of qi are assumed todescribe the universe as Western theories do,the metaphoric nature of qi is forgotten. BecauseWestern thought assumes singular truths, anidea that East Asian clinicians might take as aschool of thought, or a model appropriate to aparticular treatment system, becomes a ‘truth,’variance from which is ‘wrong.’ As we will seein Chapter 3, Eastern minds are not soexclusionary.
Fortunately, a new generation of scholars andresearchers has begun to address these prob-lems by making more Asian-centered viewsavailable. Kevin and Marnae Ergil, VolkerScheid, Nigel Wiseman, and others have estab-lished well-founded doctoral level investiga-tions that give us greater access to the Asianroots of tradition. Marnae Ergil’s research allowsWesterners to see TCM in its native Chinesecontext — for example, how students are selectedand trained in China — information that iscritical not only to the successful Westernadaptation of Chinese approaches, but also tounderstanding the role of the written materialsthat Westerners decide to translate and teach.Kevin Ergil is exploring the challenge tomedical hegemony that acupuncture is said tomake. Many claim that acupuncture is a fullydeveloped model, ‘an alternative medicine.’Yet, the way in which Westerners practiceacupuncture actually undermines that claim.Ergil cites examples of how the biomedicalmodel dominates traditional ideas. He quotes
76 WHAT ACUPUNCTURE IS
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 76 (Black plate)

the example of a patient whose TCM diagnosisis ‘blood stasis and uterine fibroids.’ The latteris a purely biomedical diagnosis that hasentirely replaced long-standing traditionalconcepts.127 Similarly, Manfred Porkert studied2000 case histories at the Beijing College ofTraditional Chinese Medicine, and found thatevery diagnosis was of biomedical origin.128
In both East and West, the dominant cultureof biomedicine often completely overridestraditional interpretations. Simplification oftranslation methodology further encourages thereplacement of Asian ideas by biomedicalterms. This is particularly true of those trad-itional ideas that do not fit Western expecta-tions.129 Thus diagnostic competence subtlyshifts from acupuncturists to physicians, a shiftthat is anything but trivial, because it reinforcesthe dominant cultural bias, and thus deeplychallenges acupuncturists’ claims of indepen-dence.
Kevin Ergil is also exploring the strategicrepresentations acupuncturists make when tryingto clinically validate traditional practices. Theseefforts rely heavily on labels that are meant toimpart authenticity by implying a coherentbody of knowledge with a long, continuouspractice.130 Effective iteration over millennia isoffered as proof of clinical validity (the ‘test oftime’) and is assumed to be an effectivesubstitute for conventional Western validitytesting. However, as we have seen throughoutthe history of Chinese medicine, there has neverbeen one right way of practice or a static con-tinuity. It would be more accurate, but perhapsoverly dramatic, to say that no system of practicehas ever been older than its most longevousmaster–apprentice line. The means of reportingand validating claims of clinical success arethus far from firmly established, something wewill explore in detail later in the text.
Paul Unschuld’s research shows us howWesterners have chosen acupuncture and phar-macotherapeutics from the variety of traditionaltechniques to represent all of Chinese medicinebecause it is these ideas that most closelyresemble our own. Nigel Wiseman shows howthe words popularly chosen to translate Chinese
medicine hide qualities of the Chinese art thatdo not fit the expectations of readers. Writerssuch as Dan Benksy, Charles Chace, and AndyEllis are giving voice to Chinese clinicians,historic and modern, through reliably translatedtexts and accounts of traditional medicine.Marnae Ergil and Bob Flaws have pioneeredChinese-language training for future cliniciansand educators.
It is fair to say that there is progress on manyfronts, and that the integration of acupuncturein the West would never have occurred withoutthe enthusiastic pursuit of its original propo-nents. However, until there is a workable wayto label ideas attributed to tradition and personalexperience, students and clinicians will have nomeans to judge the source of purported facts.Until disinterested scholars have a reasonablechance of affecting curricula and licensingexaminations, the predominance of popularinterpretation will burden the development ofacupuncture. Without an effective peer system,there is no possible check on commercialtrends. Early, simplistic, and sometimes mis-leading attempts to authenticate acupuncturetoday leave it vulnerable not only to the attackof skeptics, but also the internal conflictsfueled by competing interpretations and personalrivalry, despite its vast gains in public andprofessional acceptance. Until the more secureand workable methods of transmission, edu-cation, and clinical validation are achieved, thecontinued acculturation of acupuncture cannotbe assumed.
THE NUMBERS GAME
China131
Western medicine is dominant in the People’sRepublic of China. Recent estimates put thenumber of health-care workers trained inacupuncture at more than a million. Althoughthe number who currently practice acupunctureis unclear, we do know that most are trained intraditional medicine, zhong yi, typically herbalpharmaceutics and acupuncture. How manypractice acupuncture or herbal medicine alone
THE ACCULTURATION AND RE-ACCULTURATION OF ACUPUNCTURE 77
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 77 (Black plate)

or in combination is unknown but more than300 000 traditional doctors have graduatedfrom China’s 24 medical colleges, where theyreceived 5 years of training in basic biomedicalsciences, acupuncture, and herbal medicine.More than 30 000 assistant traditional doctorshave graduated from 3-year programs thatoffer the same subjects in less detail. There aremany Chinese biomedical physicians who haveattended abbreviated acupuncture courses, andmore than 2000 physicians have graduatedfrom both a traditional and a Western medicalprogram. By the early 1980s over 1 millionBarefoot Doctors had been trained in 6-monthto 2-year programs. Today, these famousworker-practitioners are paramedics who learnessential herbal medicine, Western medicine,and acupuncture techniques in Western-styleprograms. An unknown number of peoplehave begun private acupuncture practice sinceit was again permitted during recent economicliberalizations. The training of these practi-tioners is unknown.
Herbal medicine is far more popular inChina than is acupuncture, which retains itstraditional lesser prestige. Thus the number ofpracticing acupuncturists is probably lowerthan the training statistics suggest. Acupunc-ture services are part of China’s socializedmedical system, but increasing numbers ofpatients now pay out-of-pocket as China’sprivate sector grows. It thus is unclear whatpercentage of the population receives acupunc-ture treatment.
Taiwan132
Biomedicine is also the dominant medicinein Taiwan; however, traditional medicinessurvive and flourish. There are an estimated7500 Chinese medical doctors, about 10% ofwhom practice acupuncture extensively. Thereare some 2000 biomedical physicians trained inacupuncture and actually practicing. Althoughinsurance coverage for acupuncture is common,the percentage of the population that usesacupuncture is unknown.
Japan133
Although Western medicine is by far the dom-inant medicine, Japan’s variation of herbalmedicine (Kampo) and acupuncture are compar-atively popular and thriving. Current estimatesare that over 60 000 national licensees use somecombination of acupuncture, moxibustion, andmassage, each of which is separately licensedafter completion of 3-to-4-year training pro-grams. About 40% of these acupuncturists areblind. In the early 1980s there were about 6000physicians practicing acupuncture. There areprobably more today. The training of thesephysicians is variable and unknown. Acupunc-turists do not prescribe herbal medicine, onlyphysicians or pharmacists are so permitted bylaw. Health insurance only pays for acupunc-ture when it is performed at the referral of aphysician from an independent clinic, or is fortreatment of one of the six approved indications.Thus most acupuncture is a discretionary expense.Recent estimates suggest that at least 2% of theJapanese population uses acupuncture, this usebeing concentrated in the larger cities.
The USA134
Like most Western countries, biomedicine is byfar the most popular medicine. However, recentstudies suggest that over one-third of the USpopulation is using an ‘unconventional med-icine.’ These same studies estimate that the pro-portion of the population using acupuncture is1% or less. There are an estimated 11 000acupuncturists in the USA, approximately 3000of whom are biomedical physicians. Currentestimates are that the numbers will increase to21 000 by 2005 and 40 000 by 2015. Specificallytrained graduates complete 2- to 3-year pro-grams, in which acupuncture may be taught incombination with Chinese herbal medicine. Thescope of acupuncture education in the USAvaries, with some schools integrating herbalmedicine, massage, homeopathy, or other naturaltherapies. Current estimates are that by the year2001 these schools will be graduating 2000students per year. Physicians’ interest is increasing
78 WHAT ACUPUNCTURE IS
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 78 (Black plate)

and physicians can practice in many stateswithout formal training; however, more andmore physicians are training in postgraduatenonresidential programs. Over half the stateshave some form of licensure, with variabledegrees of autonomy, scopes of practice andrequirements for practice. There are also anunknown number of drug detox specialistswho are trained in an acupuncture protocol,and who, working under trained acupuncturists,administer acupuncture as part of drug treat-ment in centers throughout the USA. There arealso an unknown number of dentists, veterinar-ians, and chiropractors who practice acupunc-ture, after training programs of variable contentand length. Some states have extensive insurancereimbursement available for acupuncture; mostdo not. Most acupuncture is paid for bypatients. Recent estimates put the number oftreatments per year at at least 12 million.
The UK135
The numbers of practitioners and the extent oftheir training is unclear, largely because of whatis called Common Law. This allows therapieslike acupuncture to be practiced without anyspecific training. However, it is estimated thatthere are over 2000 practitioners in the UK. Anunknown number of these are physicians.Recently, the British government has allowedacupuncture to be covered by the NationalHealth Service, if it is supervised by a generalpractitioner as part of their practice. It isthought, however, that most acupuncture ispaid for out-of-pocket. As in the USA, manyacupuncturists combine acupuncture with othertherapies such as Chinese herbal medicine,massage, and homeopathy. Recent estimatesput the proportion of the population usingacupuncture at around 1%, although it isthought to be increasing.
France136
Generally the practice of acupuncture is asubspecialty of biomedicine. Only physiciansare legally permitted to practice acupuncture.
Although there are over 10 000 physicians trainedin acupuncture, there is a considerable butunknown number of nonphysician practitioners,many of whom are Vietnamese. Many physi-cians combine other therapies with acupunc-ture and biomedicine. Recent estimates placethe proportion of the population using acupunc-ture at over 20%, probably because it is aninsurance-reimbursable medical specialty.
Germany137
An estimated 20 000 to 30 000 physicians and2000 heil-praktikers, or natural therapists, practiceacupuncture. Natural or traditional therapiesare very popular in Germany, with more herbsconsumed by Germans than most of Europecombined. It seems that acupuncture is relativelypopular among the general population. Certainlyit is more widely used in Germany than in theUSA and UK, and probably as much as inFrance. Many acupuncturists combine acupunc-ture with other therapies, especially home-opathy and phytotherapy (an herbal medicinebased on higher potency extractions).
Utilization worldwide
In a recent Canadian survey it was estimatedthat less than 1% of Canadians use acupunc-ture.138 In European countries, especially thosewhere laws restrict acupuncture practice tophysicians, the percentage of use is routinelyhigher. Recent estimates suggest 3% in Denmark,6% in Belgium, and 2% in the Netherlands.139
The Netherlands is an interesting and perhapsrepresentative case. Although only physiciansand physiotherapists were allowed to practiceacupuncture legally (there were 2000 suchpractitioners) they were actually a minority.Recent studies estimated that there were over5000 nonphysician, nonphysiotherapist acupunc-turists working in the Netherlands.140 These‘underground’ practitioners were not onlytolerated, but their numbers were great enoughto force legislative change. It is possible thatthe same phenomenon may be found in otherEuropean countries.
THE ACCULTURATION AND RE-ACCULTURATION OF ACUPUNCTURE 79
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 79 (Black plate)

Alfio Bangrazi of the Istituto Paracelso inItaly compiled a list of 109 organizationsthroughout 24 European and Middle Easterncountries that promote or are involved inacupuncture. Although not a formal survey andnow slightly dated, this compilation suggestswidespread use of acupuncture in Western andEastern Europe.141 Table 2.3 shows the numberof organizations in these 24 countries. Althoughthis cannot be assumed to be authoritative, it isnonetheless usefully indicative.
It makes sense that the number of acupunc-ture treatments is greatest in less industrialcountries, where it is has been used historically,where it is inexpensive, and where it benefitsfrom political and economic support. However,among industrialized countries it is relativelymore popular where its practice is dominatedby Western physicians, making it part ofnations’ mainstream health-delivery andmedical-payment systems. In industrializedcountries like the USA and the UK, and even
Japan where acupuncture has a long history, itis largely excluded from mainstream medicalfinance, and is thus less widely used.
Acupuncture has significantly increased inpopularity throughout the world since the1970s, particularly since Richard Nixon’s trip toChina and James Reston’s post-appendectomyarticles. Western interest has increased theamount of attention that acupuncture receivesin East Asia. The WHO reports that it hashelped develop Chinese acupuncture programsthat have already trained people from over 100countries.142 Practitioners can now be found inKorea, Vietnam, Malaysia, Sri Lanka, Pakistan,India, Russia, Romania, Hungary, Austria, Italy,Switzerland, Finland, Sweden, Norway, Eire,Spain, Portugal, Greece, Australia, New Zealand,South Africa, Nigeria, Ghana, Israel, SaudiArabia, Ecuador, Brazil, Mexico, and on andon. With most of the national boundaries that ithas crossed, it has changed and adapted to suitthe needs of the peoples to whom it waspresented.
Nineteen-hundred years from its firstthorough elaboration, acupuncture is effec-tively a modern art. It is no longer anywhereprimarily supported by the philosophicaltenets from which it arose, even in its ownlands. Although philosophical loyalties anddivergent views still divide its practitioners, itsmost powerful political opponents and pro-ponents are almost universally moved byeconomic and social demands. The world-view of its foundations, the principles on whichits practices are derived, must now do serviceto the cultural demands of the 21st century.It is these aspects that we will explore inChapter 3.
80 WHAT ACUPUNCTURE IS
Table 2.1 Pan-European utilization of acupuncture
No. oforganizations Countries
1 Egypt, Hungary, Iceland, Poland, Sweden,Switzerland, Turkey
2 Austria, Denmark, Netherlands, Portugal,Slovenia
3 Czech Republic, Norway4 France, Greece5 Belgium, Bulgaria, Spain8 Ireland9 Finland
10 Germany17 Italy19 UK
NOTES
1 Manaka Y, Itaya K, Birch S 1995 Chasing the dragon’stail. Paradigm Publications, Brookline, MA, p 11
2 Hillier SM, Jewell JA 1983 Health care and traditionalChinese medicine in China 1800–1982; Routledge &Kegan Paul, London, p 13.
3 Ibid. p 15
4 Unschuld PU 1985 Medicine in China: a history ofideas. University of California Press, Berkeley p 229
5 (a) See note 2, p 29 (b) For a very compelling andmoving account of the period through the eyes of onefamily, see Chang J, 1992, Wild Swans, Flamingo, London
6 Ibid. p 39
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 80 (Black plate)

7 See note 4, p 2468 Ibid. p 2459 Ibid.
10 See note 2, p 30911 Ibid. p 5612 Chace C, Zhang TL (trans) 1997 A Qin Bowei
anthology, Paradigm Publications, Brookline, MA, p 413 See note 4, p 25014 See note 2, p 6015 Ibid. p 6616 Ibid. p 8317 Ibid. p 31318 Unschuld, PU 1998 Chinese Medicine. Paradigm
Publications, Brookline, MA, p 8319 Rosenthal MM 1987 Health care in the People’s
Republic of China: moving toward modernization.Westview Press, Boulder, CO, p 172
20 Evans JR 1988 Medical education in China. In BowersJZ, Hess JW, Sivin N (eds) Science and medicine intwentieth century China: research and education. AnnArbor, Center for Chinese studies, University ofMichigan, p 244
21 See note 2, p 31522 See note 3, p 25123 One of the most influential books in the transmission
of the TCM system of acupuncture was: O’Connor J,Bensky D 1981 Acupuncture: a comprehensive text.Eastland Press, Seattle. This book is a translation of textswritten in 1962 and 1974 by the Shanghai College ofTCM (p. xv). It reflects the pioneering work of the Collegein the 1950s and 1960s. One of the more striking featuresof the acupuncture described in this text is a considerableincrease in the recommended depth of needle insertion atthe acupuncture points. To explore this issue systematically,Birch examined historical and modern acupuncturetextbooks, including Acupuncture: A Comprehensive Text, totabulate the depths of insertion in cun, or ‘body inches.’Major acupuncture points in the following importanthistorical acupuncture texts were noted: Zhen Jiu Jia YiJing, by Huang Fu-mi (282), Tong Ren Shu Xue Zhen Jiu TuJing, by Wang Wei-yi (1027), Zhen Jiu Ji Sheng Jing, by WangZhi-zhong (1220), Zhen Jiu Ju Ying, by Gao Wu (1529),and the Zhen Jiu Da Cheng by Yang Ji-zhou (1601). Basedon the number of points recommended at each needledepth, Birch calculated the mean depth of insertion andmedian depth of insertion as indicators of relative depth.Table 2.1 lists the numbers of points at each recommendeddepth range given, the overall mean depth of insertion,and the median depth of insertion for these five historicalsources (for points that were given a range of depth ofinsertion, the midpoint of that range is given in the table).
Birch then tabulated the recommended depths ofinsertion for all the major acupuncture points in fourmodern Chinese textbooks on acupuncture: Essentials ofChinese Acupuncture, Anon. (1981), Chinese Acupunctureand Moxibustion, by Cheng (1987), Acupuncture: AComprehensive Text, by O’Connor & Bensky (1981), andFundamentals of Chinese Acupuncture, by Ellis, Wiseman &Boss (1988). In addition, he calculated the overall meandepths of insertion, and the median depths of insertion.Table 2.2 lists the numbers of points recommended ineach text in the depth ranges given, the overall meandepths of insertion and the median depths of insertionfor these four modern sources (for points that were given
a range of depth of insertion, the midpoint of that rangeis given in the table).
All the modern texts recommend deeper needleinsertions than the historical texts. Looking at the meandepth of insertion and median depth of insertion asgeneral indicators, Acupuncture: A Comprehensive Textrecommends needling more than twice as deeply as thehistorical texts. Clearly, the practice of acupuncturechanged in China during the 1950s and 1960s, when thework that preceded the publication of these modern textswas done. Although any absolute measure of the cun willvary because it is a relative measure that varies betweenindividuals and areas of the body, changes in the cunconcept cannot account for these increases in insertiondepth. A modern Chinese researcher has estimated thatthe cun is approximately 2.23 cm (Chen et al 1979), whileclassical scholars estimate that the cun was about 2.31 cmin antiquity (Harper 1982).
24 Felt. Interview of Tin Yao So. So, who was named the‘father of acupuncture in America,’ has played a historicrole in the acculturation of acupuncture in the USA. Bothof the present authors studied with Tin Yao So, Birchformally. We also have access to written and videomaterials from which we can make statements from So’sperspective. Thus, references to acupuncture before theSecond World War and Chinese apprentice training arefrequently referenced to Dr So.
25 See note 2, pp 320–32126 (a) Felt. Interview of Ping Chang (b) For a disturbing
but compelling account of the major events and theirbizarre events and consequences of the CulturalRevolution see note 5(b)
27 See note 2, p 32228 This is a complex issue. Although there is probably
some degree of chauvinism on the part of Westerners,there is evidence that this is the case. See, for example:Unschuld PU 1985 The evaluation of acupunctureanesthesia must seek truth from facts (see note 4, p 160)
29 This development is discussed in: Shudo D 1990Japanese classical acupuncture: introduction to meridiantherapy. Eastland Press, Seattle, 5 ff
30 Soichiro Tobe. Personal communication31 Kodo Fukushima. Personal communication32 Anon 1986 Shukan Bunshun, Bunshun library June 26,
128 (in Japanese)33 Felt. Interview of Yoshiharu Shibata, MD34 Anon 1947 Serious news. Ido no Nippon 6(7): 4435 Anon 1947 Demonstration by the blind. Asahi Shinbun,
October (in Japanese)36 Anon 1947 (in Japanese) Compensation for our efforts:
status law is passed. Ido no Nippon 6(9): 46 (in Japanese)37 Yanagiya S 1948 The future of acupuncture. Ido no
Nippon 7(1): 50 (in Japanese)38 Birch S 1989–1991 Acupuncture in Japan;
an introductory survey. Review: Part 1, 6: 12–13, 1989;Part 2 7:16–20, 1990; Part 3, 8:21–26; Part 4, 9:28–31,39–42, 1991
39 See note 3840 These are the personal estimates of Yoshio Manaka and
Kodo Fukushima41 Yoshio Manaka. Personal communication42 Soichiro Tobe. Personal communication43 (a) Tsutani K, Shichido T, Sakuma K 1990. When
acupuncture met biostatistics. Paper presented at the
THE ACCULTURATION AND RE-ACCULTURATION OF ACUPUNCTURE 81
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 81 (Black plate)

Second World Conference of Acupuncture andMoxibustion, Paris.(b) Shichido T 1996 Clinical evaluation of acupunctureand moxibustion. Ido no Nippon 623(8,7):94–102
44 Hiroshi Watanabe, Kiichiro Tsutani. Personalcommunication
45 World Health Organization 1980 Use of acupuncture inmodern health care. WHO Chronicle 34:294–301
46 Song Jang-Heon 1985 The role of Korean orientalmedicine. Korean Oriental Medical Association, Seoul
47 See note 4648 Tiller WA 1972 Some physical network characteristics
of acupuncture points and meridians. Proceedings of theAcademy of Parapsychology and Medicine Symposium.Stanford University, Stanford, CT
49 See note 4550 Levinson JM 1974 Traditional medicine in the
Democratic Republic of North Vietnam. American Journalof Chinese Medicine 2(2):159–162
51 Kleinman A 1980 Patients and healers in the context ofculture. University of California Press, Berkeley, p 12
52 Wiseman N. Personal communication53 Felt RL Interviews with Bill Prensky54 Felt RL Personal account55 Wolpe PR 1985 The maintenance of professional
authority: acupuncture and the American physician.Social Problems 32(5):409–424
56 See note 5557 Felt RL. Interviews with Mercy College faculty58 Felt RL. Interviews with Bill Prensky59 Accreditation Commission for Acupuncture and
Oriental Medicine 1997 Accredited and candidateprograms (as of May 4, 1997), Acupuncture and orientalmedicine accreditation. ACAOM, Washington DC
60 Based on presentations at the Workshop onAcupuncture, co-sponsored by the Office of AlternativeMedicine and the FDA, April 1994, (see the special issueof Journal of Alternative and Complementary Medicine2(1), 1996, and presentations at the ConsensusDevelopment Conference on Acupuncture at the NationalInstitutes of Health, November 3–5, 1997
61 Mitchell B 1996 Educational and licensing requirementsfor acupuncturists. Journal of Alternative andComplementary Medicine 2(2):33–35
62 (a) Lytle CD 1993 An overview of acupuncture. USDepartment of Health and Human Services, PublicHealth Service, Food and Drug Administration, Centerfor Devices and Radiological Health.(b) Helms JM 1993 Physicians and acupuncture in the1990s: a report. The AAMA Review 5(1):1–6(c) Cooper RA, Land P, Dietrich CL 1998. Current andprojected workforce of nonphysician clinicians. JAMA280(9):788–794
63 See note 62(a)64 (a) Eisenberg DM, Kessler RC, Foster C, Norlock FE,
Calkins DR, Delbanco TL 1993 Unconventional medicinein the United States; prevalence, costs, and patterns ofuse. New England Journal of Medicine 328(4):246–252(b) Eisenberg DM, Davis RB, Ettner SL, Appel S, Wilkey S,von Rompay M, Kessler RC. Trends in alternativemedicine use in the United States 1990–1997: results of afollow-up national survey. JAMA 280(18):1569–1575
65 There are no central sources of treatment data fromwhich solid conclusions can be drawn. These are
assumptions based on commercial evidence. Forexample, the bulk of both USA and European advertisingdirected to practitioners via their periodicals is TCM-centric, as are new book releases and the productsoffered. Sales of Japanese acupuncture equipment, suchas disposable needles are proportionally high but,because of trends in Western populations, TCMpractitioners routinely purchase these devices.
66 Califano JA, Kleber HD 1992 Center on addiction andsubstance abuse. Annual report. Columbia University
67 Goldkamp JS, Weiland D 1993 Assessing the impact ofDade County’s Felony Drug Court. National Institute ofJustice, US Department of Justice, NCJ 145302
68 Finn P, Newlyn AK 1993 Miami’s ‘Drug Court’, adifferent approach. National Institute of Justice, USDepartment of Justice, NCJ 142412
69 See note 6770 See note 6771 Presentation, Washington, DC, May 199472 Brumbaugh AG, 1993 Acupuncture: new perspectives
in chemical dependency treatment. Journal of SubstanceAbuse Treatment 10:35–43
73 See note 62(a)74 Alpert S. In: Birch S, Hammerschlag R (eds),
Acupuncture efficacy. National Academy of Acupunctureand Oriental Medicine, New York
75 Anon 1998 Acupuncture: NIH consensus developmentpanel on acupuncture. JAMA 280(17):1518–1524
76 Because of the unsettled economic and political statusof acupuncture in the West, labels are often claims of‘belonging’ to a particular view. Thus there is acrimoniusdebate concerning the use of ‘lay’ and ‘non-physician’ aslabels for acupuncturists who do not have a physician’straining, or the use of the title ‘Doctor’ to labelacupuncturists or traditional Chinese herbalists with orwithout degress like the Oriental Medical Doctor (OMD)or Doctor of Oriental Medicine (DOM). We are using‘specifically trained’ to label acupuncturists who do nothold standard Western academic or medical credentialsbecause this label reflects patients’ concern for theirpractitioners’ relevant experience and training. This furtherdirects attention to the long-term issue of acupunctureeducation rather than transient intra- and interprofessionaltensions. We recognize that some physicians have a didacticand/or clinical training just as specific as specificallytrained acupuncturists, and that this could justify referingto them in parallel as ‘multiply trained.’ However, that isnot the case for all, and thus the label is inappropriateexcept for specific individuals. From the patient’sperspective, what counts is experience in the systempracticed. Thus, where a physician may be advantagedin the practice of a system with a biomedical basis, theywould be disadvantaged relative to a specifically trainedacupuncturist with greater experience with traditional skills.
77 Hill S. Personal communication78 Kaptchuk TJ 1997 Foreword. In: Maciocia G 1997
Obstetrics and gynecology in Chinese medicine. ChurchillLivingstone, Edinburgh
79 Shifrin K 1993 Setting standards for acupuncturetraining – a model for complementary medicine;Complementary Therapies in Medicine 1(2):91–95
80 The difference between a professional master’s degreeand an academic master’s degree is one of accreditationstandards and agencies. Typically, issues such as credits
82 WHAT ACUPUNCTURE IS
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 82 (Black plate)

for courses taken, transfer, and admission standards aredetermined within accrediting systems. For example, aperson with a professional master’s degree inacupuncture might receive ‘life experience’ credits fromsome academic institution, but probably would not beadmitted to a doctoral program based on theirprofessional degree.
81 Hill S. Personal communication82 Stephen Dorrell clarifies the position on alternative and
complementary therapies; Press Release, December 3, 199183 Anglo Dutch Institute for Oriental Medicine Magazine,
Spring: 11 199784 Anon 1997 Integrated healthcare. A way forward for
the next five years? The Foundation for IntegratedHealthcare, London
85 O’Neill A 1994 Enemies within and without. LaTrobeUniversity Press, Bundoora, Victoria
86 Bensoussan A, Myers S 1997 Towards a safer choice.University of Western Sydney, Macarthur, 23
87 MacLennan A, Wilson D, Taylor A 1996 Prevalence andcost of alternative medicine in Australia. Lancet347:569–573
88 See note 6489 See note 86, p 2290 Hemken A, 1995 The Anglo-Dutch Institute for Oriental
Medicine and the situation on alternative medicine in theNetherlands. European Journal of Oriental Medicine 1,6:30–31
91 Stux G. Personal communication92 Eckman P 1996 In the footsteps of the yellow emperor.Cypress Book Company, San Francisco
93 Bossy J 1993 History and present status ofacupuncture in France. In: Abstracts of the Third Worldconference on acupuncture. World Federation ofAcupuncture and Moxibustion Societies, Kyoto
94(a) See note 64(b) Thomas KJ, Carr J, Westlake L et al 1991 Use of non-
orthodox and conventional health care in Great Britain.British Medical Journal 302:207–210
95 Nogier PFM 1983 From auriculotherapy toauriculomedicine. Maisonneuve, Saint-Ruffine
96 For discussions of the differences, see:(a) Kenyon JN 1983 Modern techniques of acupuncture,vols 1 and 2. Thorsons, Wellingborough.(b) Tiller WA 1989 On the evolution and futuredevelopment of electrodermal diagnostic instruments. In:Energy fields in medicine: a study of device technologybased on acupuncture meridians and chi energy.Proceedings of a symposium sponsored by the John. E.Fetzer Foundation, pp 257–328
97 See examples in: Matsumoto K, Birch S 1986Extraordinary Vessels. Paradigm Publications, Brookline, MA
98(a) Bragin E 1993 Present and future of traditionalmedicine in Russia. In: Abstracts of the Third Worldconference on acupuncture. World Federation ofAcupuncture and Moxibustion Societies, Kyoto(b) Praznikov VP 1993. The role of acupuncture inmodern medicine. In: Abstracts of the Third Worldconference on acupuncture. World Federation ofAcupuncture and Moxibustion Societies, Kyoto(c) Rudenko M, Kabaruchin B 1993 The system of educationin traditional Chinese medicine in Russia. Abstracts ofthe Third World conference on acupuncture. WorldFederation of Acupuncture and Moxibustion Societies, Kyoto
99 Stoyunovsky D 1981 Acupuncture reflexotherapy:handbook–atlas. Cartya Moldovenyaske, Kishinev (inRussian)
100 See note 98(b)101 See note 98(a)102 See note 98(b)103 Ionescu-Tirgoviste C 1991 Acupuncture in Romania.
Complementary Medicine Research 5(2):89–92104 Paul helped found the Midwest Center of Oriental
Medicine in Chicago, IL, and contributed to thedevelopment of programs at the New England School ofAcupuncture in Boston, MA.
105 Unschuld PU 1998 Chinese medicine. ParadigmPublications, Brookline, MA p 87
106 The following are representative examples:(a) ‘The extraordinary vessels all derive their energyfrom the Kidneys and all contain the Essence which isstored in the Kidneys. They circulate the Essence aroundthe body.’ Maciocia G 1989 Foundations of Chinesemedicine. Churchill Livingstone, Edinburgh, p 355(b) ‘[Four of the extraordinary vessels] are interlinked forthe production, circulation, discharge and regeneration ofthe Essence.’ Maciocia G. 1997 Obstetrics and gynecologyin Chinese medicine. Churchill Livingstone, Edinburgh p 24(c) ‘Jing circulates in the Jing Luo system, and inparticular in the network of the eight ExtraordinaryChannels.’ Ross J 1985 Zang Fu, 2nd edn. ChurchillLivingstone, Edinburgh, p 67Other references to this concept are:(d) Pirog JE 1996 The practical application of meridianstyle acupuncture. Pacific View Press, Berkeley, p 158.(e) Seem M 1992 American acupuncture comes of age:perspectives from the front lines. American Academy ofMedical Acupuncture Review, 4(2):16–23(f) Seem M 1993 A new American acupuncture. BluePoppy Press, Boulder, CO, p 52
107(a) ‘Yuan qi is most concentrated in the curiousmeridians [extraordinary vessels].’ Helms JM 1995Acupuncture Energetics. Medical AcupuncturePublishers, Berkeley, CA, pp 523–524(b) ‘The irregular vessels [extraordinary vessels] functionon a deep, fundamental level, and this is in perfect accordwith the traditional statement that they are the carriers ofthe yuan ch’i(sic) or ancestral energy.’ Low R 1983Secondary vessels. Thorsons, Wellingborough, pp 70,147–164(c) ‘In addition, all the extraordinary vessels are in someway connected to the kidneys or to the kidney meridian,and by extension to the original qi.’ See note 106(a), p 156
108 See note 106(b), pp 22–24, and note 106(d), pp 156–158109 See: note 107(b), pp 70, 147; note 106(a), p 355; note
106(b) p 22: note 106(d) p 156110 One of the clearest discussions of the diverse
descriptions of the qi jing ba mai can be found in:Matsumoto K, Birch S 1986 Extraordinary vessels.Paradigm Publications, Brookline, MA, pp 4–137
111 See discussions in note 110, pp 4–6112 When empirical observation and experience indicate
that acupoints or naturally occurring medicines haveunwelcome effects in particular circumstances orcombinations these contraindications appear in theliterature. Although there are variances in thesecontraindications over time, had treating the extraordinaryvessels created a significant history of iatrogenic effects,
THE ACCULTURATION AND RE-ACCULTURATION OF ACUPUNCTURE 83
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 83 (Black plate)

there would be obvious contraindications in booksdescribing the use of their acupoints.
113 These texts are all discussed in Chapter 1 and inAppendix 2. They all made significant contributions tothe theories and uses of the extraordinary vessels. Thesalient passages are translated by Matsumoto & Birch(see note 110)
114 See: note 106(a), p 355; note 106(b), pp 22–24; note106(c), p67.
115 Direct translations of modern TCM textbooks fromChina make no mention of these associations. Therelationships described are to the liver, kidney, andminor organs, and there is specific mention that theextraordinary vessels are so named because, unlike theregular channels, ‘they have neither a continuousinterlinking pattern of circulation, nor are they eachassociated with a specific organ.’
See: Wiseman N, Ellis A 1994 Fundamentals of Chinesemedicine. Paradigm Publications, Brookline, MA, pp 40–43.
Yuan qi, original qi, is defined by Chinese sources as‘right qi,’ which stands in opposition to any entity thatmay harm the body, and ‘source qi,’ which is the basic qiof the body. It is specifically noted as not appearingin the Inner Canon. Yuan qi is not uniquely associatedwith the kidney, but with a combination of the essentialqi of the kidney, the qi of food via the spleen, and the qiof air through the lung. It is specifically stated as accessedvia the source points of the regular channels.
See: Wiseman N, Feng Y 1998 A practical dictionaryof Chinese medicine. Paradigm Publications, Brookline,MA, pp 421, 507, 548
116 See: note 106(d), p 158; note 106(e), p 52; note 107(a),pp 523–524; note 107(b), pp 147–164
117 Zand J 1997 Presentation at the Pacific Symposium,San Diego, November 6
118 Use of the term ‘translation’ typically asserts a moreor less word-for-word version of a foreign-languagesource. However, in English-language acupunctureliterature the label is freely applied to works that areloosely referenced and which contain undifferentiatedquotation, paraphrasing, and original writing. Theantiquity of Chinese medicine’s generative literature alsocontributes to discrepancies in interpretation. Becausethese ancient documents were recorded on perishablematerials, they exist as archaeological fragments,references in other archaeological fragments, andquotations or attributions in later editions of those texts.Thus translations of these works require an assembly andverification process known as ‘collation.’ Because thecontents have been assembled in different eras andreflect the assumptions of those that produced,commented upon, and sometimes edited those editions,the content of these texts is a complex issue. This israrely noted, nor are the commentaries that accompanyAsian editions typically available.
119 See note 92, p 163.120 Chamfrault A 1969 Van Nghi N 1969 L’energetique
humaine en medicine Chinoise. Imprimerie de laCharente, Angouleme, p 241
An English-language exposition of this model appearsin Yves Requena’s work. Requena is a direct student ofVan Nghi and played an important role in the early yearsof the transmission of acupuncture. He references themodel directly to Chamfrualt. See: Requena Y 1986
Terrains and pathology in acupuncture, vol 1, Correlationswith diathetic medicine. Paradigm Publications, Brookline,MA, p 14
121 See note 120122 We looked at:
(a) Kitasato kenkyujo huzoku toyoigaku sogokenkyujorinsho koten kenkyuhan: 1982 Reisu Rinsho Sakuinshu, theLingshu Clinical Index. Kokusho Kankokai, Tokyo,(b) Anon 1988 Ling Shu Jing. Chung Hwa BookCompany, Taipei(c) Huang Di Nei Jing Ling Shu Yi Jie. 2nd edn. ChineseRepublic Publishing Company, Taipei, 1978
Note, however, that because Chinese literature is soextensive (the vast majority of the literature has neverbeen translated into any Western language), there is nophysical evidence for much of what is reputed to be inthese early, seminal texts, only fragments of whichsurvive. Thus it is impossible to make definitivestatements. It is the continual presence of an idea in abroad range of the surrounding and followingcommentary and related literature that is the mostreliable evidence of authenticity. Although the referenceshere are necessary, the best evidence for theidiosyncrasity of this idea is its isolation in the writingsof European and European-influenced American authors.
123 Soulie de Morant notes that yuan qi is ‘mostly used inthe sense of vitality, strength and resistance,’ a definitionthat accords with Chinese sources. Soulie de Morant G1994 Chinese acupuncture. Paradigm Publications,Brookline, MA, p 46
124 See note 92, p 163125 See: note 106(a), p 355; note 106(b), pp 22–24126 Unschuld PU 1992 Epistemological issues and changing
legitimation: traditional Chinese medicine in the twentiethcentury. In: Leslie C, Young A (eds). Paths to Asian medicalKnowledge, University of California Press, Berkeley
127 Ergil KV 1990 A challenge to medical hegemony?Epistemological issues informing the practice of TCM inthe United States. Paper presented at the Third InternationalCongress on Traditional Asian Medicine, Bombay.
128 Porkert M, The difficult task of blending Chinese andWestern science: the case of modern interpretations oftraditional Chinese medicine. Quoted in Sivin N 1987Traditional medicine in contemporary China. Center forChinese Studies, University of Michigan, Ann Arbor, MI,p 28
129 See: Wiseman N 1990 Introduction. In: Wiseman N,Boss K A glossary of Chinese medicine and acupuncturepoints. Paradigm Publications, Brookline, MA
130 Ergil KV 1992 Strategic representations: ‘oriental’medicine at large. Paper presented at AmericanAnthropological Association Annual Meeting
131 This section is based on: (a) Evans JR 1988 In: BowersJE, Hess JW, Sivin N (eds) Science and medicine intwentieth-century China: research and education. TheCenter for Chinese Studies, University of Michigan, AnnArbor, MI.(b) Hillier SM, Jewell JA 1983 Health care and traditionalChinese medicine in China 1800–1982. Routledge &Kegan Paul, London(c) Rosenthal MM 1987 Health care in the People’sRepublic of China: moving toward modernization.Westview Press, Boulder, CO
84 WHAT ACUPUNCTURE IS
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 84 (Black plate)

132 This section is based on Nigel Wiseman’s interviewswith his colleagues at the Journal of Chinese Medicineand the China Medical College (Taichung, ROC)
133 This section is based on:(a) Birch, Acupuncture in Japan (see note 38),(b) Sonoda K 1988 Health and illness in changingJapanese society. University of Tokyo Press, Tokyo
134 This section is based on presentations at theWorkshop on Acupuncture sponsored by the Office ofAlternative Medicine and the FDA (see the special issueof Journal of Alternative and Complementary Medicine2(1), 1996 and presentations at the ConsensusDevelopment Conference on Acupuncture at the NationalInstitutes of Health, November 3–5, 1997
135 Based on: (a) Birch, Acupuncture in Japan (see note 38)(b) Fulder SJ, Munro RE 1985 Complementary medicinein the United Kingdom: patients, practitioners, andconsultations. Lancet 542–545(c) Thomas KJ et al (see note 94(b))(d) note 62(c)(e) note 64(a and b)(f) Cooper RA, Henderson T, Dietrich CL 1998 Roles ofnonphysician clinicians as autonomous providers ofhealth care. JAMA 280(9):795–802(g) Wetzel MS, Eisenberg DM, Kaptchuk TJ 1998 Coursesinvolving complementary and alternative medicine at USmedical schools. JAMA 280(9):784–787
136 Based on:(a) Bossy J 1993 History and present status of acupuncturein France. Abstracts of the Third World Conference on
Acupuncture. World Federation of Acupuncture andMoxibustion Societies, Kyoto(b) Bouchayer F 1990 Alternative medicines: a generalapproach to the French situation. ComplementaryMedicine Research 4(2):4–8
137 Based on:(a) Aldridge D 1990 Pluralism of medical practicein West Germany. Complementary Medicine Research4(2): 14–15(b) Heise TE 1986 Historical development of traditionalChinese medicine in West Germany. Journal ofTraditional Chinese Medicine 6(3):227–230(c) Stux G. Personal communication
138 Anon 1991 One in five Canadians is using alternativetherapies, survey finds. Canadian Medical AssociationJournal 144(4):469
139(a) Rasmussen NK, Morgall JM 1990 The use of alternativetreatment in the Danish adult population. ComplementaryMedicine Research 4(2):16–22(b) Sermeus G 1990 Alternative health care in Belgium.Complementary Medicine Research 4(2):9–13(c) Uddin J 1993 Acupuncture, Europe and the law.European Journal of Oriental Medicine 1(1):53–55
140 Hemken A, Personal communication.141 Bangrazi A, Tsutani K 1998 Global communication on
acupuncture (10) Directory of Societies in the field ofAcupuncture. Journal of the Japan Society ofAcupuncture 48(2): 176–185
142 World Health Organization 1985 The role oftraditional medicine in primary health care. WHO, Geneva WPR/RC36/Technical Discussions/s
THE ACCULTURATION AND RE-ACCULTURATION OF ACUPUNCTURE 85
02 acculturation&re-… 2/12/98 01/07/2000 11:39 AM Page 85 (Black plate)