An attempt to enhance solubility of metoclopramide base by ...

Postgraduate Medical Journal (March 1981) 57, 185-188
Uncontrolled diabetes mellitus due to gastroparesis diabeticorum:treatment with metoclopramide
ERIK E. MULSM.D.
GERARD F. LAMBERIGTSM.D.
Department of Internal Medicine, Endocrine Unit, A.Z. St Jan, Ruddershove,B-8000 Brugge, Belgium
SummaryA case is reported of uncontrolled diabetes mellitusdue to gastroparesis diabeticorum in which treatmentwith metoclopramide restored diabetic control. Diag-nostic, pathological and therapeutic aspects of dia-betic gastroparesis, which is thought to reflectautonomic neuropathy involving the gastrointestinaltract, are discussed.
IntroductionUncontrolled diabetes mellitus may be caused by
diabetic gastroparesis, i.e. gastric atony and delayedemptying. This can occur without obvious ali-mentary symptoms. A patient is described in whommetoclopramide treatment improved gastric empty-ing and restored diabetic control.
Case reportA 78-year-old woman with a maturity-onset
diabetes of 21 years' duration was admitted to thehospital after a fortnight of severe daily hypo-glycaemic episodes. She had lost 30 kg in one year.Gastrointestinal complaints were absent except forone episode of watery diarrhoea on the day beforeadmission. On examination the abdomen wasnormal. She had postural hypotension and restingtachycardia (100 beats/min). Signs of peripheralsensorimotor neuropathy were present. She had noretinopathy, nephropathy, sweating abnormalities,ar urinary bladder dysfunction. The insulin dosagewas reduced from 36 to 22 units daily, but herdiabetes was still poorly controlled and hypo-glycaemic episodes recurred.A radiological examination of the gastrointestinal
tract showed diminished oesophageal peristalticwaves, gastric food residues, dilatation of thestomach with decreased peristalsis and with bariumretention for more than 24 hr (Fig. 1). The transittime of the contrast medium through the smallintestine was prolonged. Gastroduodenoscopy re-vealed no pyloro-duodenal obstruction. Electro-
myography showed the presence of peripheralneuropathy. The postural hypotension and theresting tachycardia had suggested autonomic neuro-pathy involving the cardiovascular system. This wasconfirmed by measuring the immediate heart rateresponse to standing as described by Ewing et al.(1978): the electrocardiographic R-R interval ratioat beat 30 v. beat 15 after standing was 0.95 in thepatient, whereas diabetics without autonomicneuropathy have a 30: 15 R-R interval ratio of>1.03.These data led to the diagnosis of gastroparesis
diabeticorum causing the worsening of diabeticcontrol in a patient with peripheral and autonomicneuropathy. Treatment was instituted with oralmetoclopramide in a dosage of 10 mg, 30 min beforeeach meal. The insulin regimen of 22 units daily wasnot changed. Diabetic control improved and nofurther hypoglycaemic episode occurred during thefollowing months.
X-ray control (Fig. 2) during the fifth week ofmetoclopramide therapy showed considerable im-provement, although complete gastric emptying ofthe barium still required 7 hr (compared with morethan 24 hr before treatment).
DiscussionUncontrolled diabetes mellitus may be due to
irregular food absorption caused by gastric atonyand delayed emptying of the stomach (gastroparesisdiabeticorum). This worsening of diabetic controlcan occur in the absence of gastrointestinal com-plaints. The usual clinical manifestations are nausea,vomiting, vague abdominal complaints or anorexia.Bezoar formation can occur. Gastroparesis shouldalso be suspected in the diabetic with unexplainedweight loss, particularly if neuropathy involvingother systems exists.
Radiological investigation is a readily availablebut relatively insensitive diagnostic method. Solidresidue in the stomach at the beginning of the
0032-5473/81/0300-0185 $02.00 ©Q 1981 The Fellowship of Postgraduate Medicine
by copyright. on S
eptember 5, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.57.665.185 on 1 March 1981. D
ownloaded from

186 Case reports
r~~~~~~~~~~~~~~~~~~........ $,11ikf~~~i t ;.F.
_- _ _-;-_~~~~~~~~~~~~~~~~~~~~fT
jft_
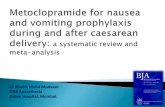
FIG. 1. Before the administration of metoclopramide, gastrointestinal radiological examination shows markedbarium retention after 5 hr (a) and after 24 hr (b).
examination, decreased peristalsis with delayedgastric emptying and duodenal bulb atony are theprincipal radiological signs (Gramm, Reuter andCostello, 1978). Endoscopy should be done toexclude pyloro-duodenal obstruction. Gastric scinti-scanning is a more accurate way to study gastricemptying. Using a double isotope scintiscanningtechnique, which differentiates between solid andliquid emptying, Campbell et al. (1977) showedgastric stasis to be present in all 3 patients withdiabetic autonomic neuropathy and symptoms ofgastroparesis although impaired gastric emptyingwas recognized radiologically in only one patient.The delay in gastric emptying has been attributed
to vagal damage occurring as part of a moregeneralized autonomic neuropathy (Wooten andMeriwether, 1961). Diabetics with symptoms ofautonomic neuropathy have an impaired vagally-mediated acid secretion in response to insulin-induced hypoglycaemia but they have normalparietal cell function (Hosking et al., 1975). Surgicalvagotomy, however, has no effect on the pattern ofgastric emptying in non-diabetics when measured
with the scintiscanning technique (Heading et al.,1975).
Pathological data concerning diabetics with gas-troparesis are scarce. Duchen et al. (1980) recentlyreported post-mortem studies of the autonomicnervous system in 5 insulin-dependent diabeticswith peripheral and autonomic neuropathy involvingthe gastrointestinal tract. There was a severe loss ofmyelinated axons and a marked excess of collagen inthe vagus nerve of all patients studied. This confirmsthe earlier observation of myelin degeneration in thevagal nerves as well as in the peripheral nerves ofdiabetics by Kristensson et al. (1971). However,several other pathological lesions were found inthese patients such as distension and vacuolizationof neurones in coeliac and other sympathetic ganglia,inflammatory changes in the autonomic ganglia andin or around unmyelinated nerve fibres, and focalhyaline degeneration in the visceral smooth muscle.These findings suggested to Duchen et al. thatseveral different pathogenetic mechanisms may beinvolved in the development of autonomic neuro-pathy in diabetes. The ultrastructural analysis of
by copyright. on S
eptember 5, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.57.665.185 on 1 March 1981. D
ownloaded from

Case reports 187
- R- -IrI,
t x t -~~~
FIG. 2. Following metoclopramide therapy gastric emptying improved considerably, as shown 3 hr after thebarium ingestion.
Auerbach's myenteric plexuses of the small intestinein ketonuric diabetic Chinese hamsters with radio-logical abnormalities comparable to those found inhuman gastroparesis diabeticorum showed degenera-tion of the distal unmyelinated axons (Diani et al.,1979).Treatment of diabetic gastroparesis with pyloro-
plasty or partial gastrectomy, cholinergic agents orcholinesterase inhibitors has been disappointing(Wooten and Meriwether, 1961; Zitom-r, Grammand Kozak, 1968). More recently, however, a limitednumber of reports about metoclopramide therapyfor diabetic gastroparesis have suggested an improve-ment in gastric emptying and diabetic control asevidenced in the present patient (Berkowitz, Metzgerand Sturdevant, 1976; Campbell et al., 1977;Longstreth, Malagelada and Kelly, 1977; Braverman
and Bogoch, 1978). The dopamine antagonistmetoclopramide increases the frequency of type IIgastric peristaltic contractions, speeding up the rateof gastric emptying (Longstreth et al., 1977). Meto-clopramide may act by increasing the amount ofacetylcholine released at the postganglionic nerveendings (Hay, 1977).The authors conclude that gastroparesis diabeti-
corum should be considered in the patient withuncontrolled diabetes mellitus, even in the absenceof abdominal symptoms, and that metoclopramidecan be helpful in its treatment.
ReferencesBERKOWITZ, D.M., METZGER, W.H. & STURDEVANT, R.A.
(1976) Effect of metoclopramide in diabetic gastroparesis.Clinical Research, 24, 103A.
by copyright. on S
eptember 5, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.57.665.185 on 1 March 1981. D
ownloaded from

188 Case reports
BRAVERMAN, D. & BOGOCH, A. (1978) Metoclopramide forgastroparesis diabeticorum. Diabetes Care, 1, 356.
CAMPBELL, I.W., HEADING, R.C., TOTHILL, P., BUIST, T.A.,EWING, D.J. & CLARKE, B.F. (1977) Gastric emptying indiabetic autonomic neuropathy. Gut, 18, 462.
DIANI, A.R., GROGAN, D.M., YATES, M.E., RISINGER, D.L.& GERRITSEN, G.C. (1979) Radiologic abnormalities andautonomic neuropathology in the digestive tract of theketonuric diabetic Chinese hamster. Diabetologia, 17, 33.
DUCHEN, L.W., ANJORIN, A., WATKINS, P.J. & MACKAY,J.D. (1980) Pathology of autonomic neuropathy indiabetes mellitus. Annals of Internal Medicine, 92, 301.
EWING, D.J., CAMPBELL, I.W., MURRAY, A., NEILSON, J.M.& CLARKE, B.F. (1978) Immediate heart-rate response tostanding: simple test for autonomic neuropathy in dia-betes. British Medical Journal, 1, 145.
GRAMM, H.F., REUTER, K. & COSTELLO, P. (1978) Theradiologic manifestations of diabetic gastric neuropathyand its differential diagnosis. Gastrointestinal Radiology, 3,151.
HAY, A.M. (1977) Pharmacological analysis of the effects of
metoclopramide on the guinea-pig isolated stomach.Gastroenterology, 72, 864.
HEADING, R.C., TOTHILL, P., MCLOUGHIN, G.P. & SHEAR-MAN, D.J. (1975) Effects of gastric surgery in differentialemptying of solid and liquid components of the gastriccontents. British Journal of Surgery, 62, 659.
HOSKING, D.J., MOODY, F., STEWART, I.M. & ATKINSON, M.(1975) Vagal impairment of gastric secretion in diabeticautonomic neuropathy. British Medical Journal, 2, 588.
KRISTENSSON, Y., NORDBORG, C., OLSSON, Y. & SOURANDER,P. (1971) Changes in the vagus nerve in diabetes mellitus.Acta pathologica et microbiologica scandinavica, 79A, 684.
LONGSTRETH, G.F., MALAGELADA, J.R. & KELLY, K.A.(1977) Metoclopramide stimulation of gastric motility andemptying in diabetic gastroparesis. Annals of InternalMedicine, 86, 195.
WOOTEN, R.L. & MERIWETHER, T.W. (1961) Diabetic gastricatony: a clinical study. Journal of the American MedicalAssociation, 176, 1082.
ZITOMER, B.R., GRAMM, H.F. & KOZAK, G.P. (1968) Gastric,neuropathy in diabetes mellitus: clinical and radiologicobservations. Metabolism, 17, 199.
by copyright. on S
eptember 5, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.57.665.185 on 1 March 1981. D
ownloaded from