Uncontrolled Asthma: Burden, Patient Perceptions and Clinical Implications Paolo Tassinari MD...
29
Uncontrolled Asthma: Burden, Patient Perceptions and Clinical Implications Paolo Tassinari MD Instituto de Inmunología Hospital de Clínicas Caracas Venezuela
-
Upload
emil-melton -
Category
Documents
-
view
217 -
download
0
Transcript of Uncontrolled Asthma: Burden, Patient Perceptions and Clinical Implications Paolo Tassinari MD...

Uncontrolled Asthma: Burden, Patient Perceptions and Clinical Implications
Paolo Tassinari MDInstituto de InmunologíaHospital de Clínicas CaracasVenezuela

Outline
• Asthma control
• Guidelines: current control and future risk
• Predictors of poor asthma control
• Burden of uncontrolled asthma
• Novel Approaches to Achieve Asthma Control
• Summary

Ideal Asthma Control
• Absent/minimal symptoms• Minimal/no requirement for rescue bronchodilators• No night-time or early morning symptoms• Normal lyfestyle• Minimal airway obstruction • No mortality
National Hesart, Lung, and Blood Institute. National Heart, Lung, and Blood Institute. International consensus report on diagnosis and treatment of asthma Eur Respir J 1992; 5: 601–641

Real World
• Over 50% of all patients with severe asthma and more than 30% of patients with less severe asthma remain only partially controlled or uncontrolled
– Substantial effect on patient’s quality of life (physical,
emotional, social, professional, economic)– Significant burden on the Health Care System
Kardos P. Current Medical Research & Opinion Vol. 27, No. 9, 2011, 1835–1847Chen h. J Allergy Clin Immunol 2007; 120:396-402Weiss K. J Allergy Clin Immunol 2001; 107:3-8

International GuidelinesGoals of Asthma Treatment
• Control of patient’s current symptoms• Prevention of future adverse outcomes
– Greater emphasis on the assessment of asthma control vs. asthma severity
– Use of combination measures vs. any single measure for more consistent evaluation of asthma control
National Heart, Lung, and Blood Institute. National Asthma Education and Prevention Program. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma 2007

Asthma Control
• Asthma control:Asthma control: Extent to which the manifestations of asthma have been reduced or removed by treatment– Current clinical control: symptoms, reliever use, lung
function – Future risk: exacerbations, lung function decline
American Thoracic Society/European Respiratory Society Task ForceTaylor DR. Eur Respir J 2008; 32:545-554

7
ATS/ERS Statement: Clinical Recognition of Asthma Exacerbations
ATS = American Thoracic Society. ERS = European Respiratory Society
Reddel HK, et al. Am J Respir Crit Care Med. 2009;180:59–99
Exacerbations can be clinically identified by changes in lung function, rescue use, and/or symptoms outside the patient’s usual range of
day-to-day variation
ATS/ERS Statement
Exacerbations are episodes of asthma that: – Are troublesome to patients AND– Prompt a treatment change
Exacerbations can vary considerably in: – Speed of onset (minutes/hours/weeks)– Time to resolution– Absolute severity between and within individuals
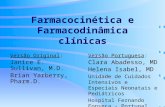
Goals of Asthma Management
Overall asthma controlOverall asthma control
CURRENT CONTROL CURRENT CONTROL FUTURE RISKFUTURE RISK
Symptoms
Activity
Reliever use
Lung functionLung function
loss
Instability/worsening
Exacerbations
MedicationAdverse effects
achieving reducing
Defined by Defined by

Asthma Control
• GINA 2006 and classification of asthma GINA 2006 and classification of asthma control: control: – ControlledControlled Symptoms frequencySymptoms frequency– Partly controlledPartly controlled Reliever useReliever use– UncontrolledUncontrolled Night wakingNight waking
Activity limitationActivity limitation
Airway obstructionAirway obstruction
ExacerbationsExacerbations
Global Initiative for Asthma. Global strategy for asthma management and prevention 2006

10
GINA Guidelines Recommend Evaluating Short- and Long-term Patient History to Assess Asthma Control To achieve and maintain long-term asthma control, GINA guidelines
recommend managing both current symptoms and potential future risk
FEV1 = forced expiratory volume in 1 secondGINA Strategy for Asthma Management and Prevention. 2009. Available at: www.ginasthma.org
Clinical goals for current impairment should be evaluated over the past 4 weeks
Current Symptoms
Symptoms/exacerbations associated with future risk should be evaluated over the past year
Future Risk
Daytime symptoms occurring twice per week or less
No nocturnal symptoms or awakenings Need for reliever/rescue treatment twice per
week or less No limitations of activities Normal lung function
Poor clinical control Frequent exacerbations Admission to critical care for asthma Low FEV1

11
GINA Guidelines: Asthma Control Classification and Treatment Approach
Classification
Symptoms Controlled(all of the following)
Partially Controlled(any measure present in any week)
Uncontrolled
Daytime Symptoms ≤2 times per week ≥3 times per week ≥3 features of partly controlled asthma present in any weeka
Limitations of Activities None Any
Nocturnal Symptoms/Awakening
None Any
Need for Reliever Treatment ≤2 times per week ≥3 times per week
Lung Function (PEF or FEV1) Normal <80% of previous lung function test
GINA = Global Initiative for Asthma; PEF = peak expiratory flow; FEV1 = forced expiratory volume in 1 secondAdapted from GINA Strategy for Asthma Management and Prevention. 2009. Available at: www.ginasthma.org
Treatment Action
Assessment of Future Risk Risk of exacerbations, instability, rapid decline in lung function, side effectsaAny exacerbation should prompt review of maintenance treatment to ensure that it is adequate

12
Consistently Very Poorly Controlled (VPC) Asthma Increased the Risk of Future Asthma Exacerbations
Haselkorn T, et al. J Allergy Clin Immunol. 2009;124:895–902.e4
Risk of Asthma Exacerbations Associated With Consistently VPC
Asthma in TENOR
Level of asthma control based on the impairment domain of the NHLBI EPR-3 guidelines
Adolescents/Adults (≥12 years)
Hospitalization Hospitalization/ED Visit/Corticosteroid Burst Composite
Corticosteroid Burst
Hospitalization/ED Visit Composite
ED Visit
Increased Risk →Odds Ratio and 95% Confidence Intervals
0.5 1 2 5 10 100
OR P Value (95% CI)
4.9 0.13(0.64, 37.2)
3.2 <0.001(1.91, 5.33)
2.8 <0.001(1.71, 4.75)
2.2 0.12(0.81, 5.97) 2.0 0.187(0.72, 5.43)
TENOR(The Epidemiology and Natural
history of asthma: Outcomes and treatment Regimens)
Objective
To evaluate whether current level of control predicts risk for future hospitalizations, emergency department (ED) visits, or corticosteroid bursts
Conclusion
Patients with consistently VPC asthma were more likely to have a corticosteroid burst or hospitalization, ED visit, or corticosteroid burst (composite)

Asthma Severity
• Asthma severity:Asthma severity: Intensity of treatment required to achieve good asthma control– Underlying disease activity– Patient’s phenotype
American Thoracic Society/European Respiratory Society Task ForceTaylor DR. Eur Respir J 2008; 32: 545-554

Asthma Severity
• Mild asthma – Good control with very low-intensity treatment
• Severe asthma– Need for high-intensity treatment
American Thoracic Society/European Respiratory Society Task ForceTaylor DR. Eur Respir J 2008; 32:545-554

Asthma controlCurrent clinical control Future risk
Asthma severity(based on intensity of
treatment required)
Disease Activity
Asthma phenotypes
Eur Respir J 2008; 32:545
Treatment Genetic and environmental
factors

Poor Asthma Control Predictors
• Underlying severe disease or resistance to therapy• Poor compliance• Poor inhaler technique• Under-prescribing• Environmental factors (allergen exposure,
smoking)• Incorrect diagnosis/significant comorbidities
American Thoracic Society. Proceedings of the ATS workshop on refractory asthma: current understanding, recommendations, and unanswered questions. Am J Respir Crit Care Med 2000; 162:2341–2351

Poor Asthma Control Predictors
Armour C, et al. Using the community pharmacy to identify patients at risk of poor asthma control and factors which contribute to this poor control. J Asthma 2011; 48:914-22
• 96 pharmacies in Australia• 570 patients >18 years with doctor-diagnosed
asthma and at risk of poor asthma control• Comprehensive asthma assessment: asthma
control was classified using a symptom and activity tool based on self-reported frequency of symptoms during the previous month

Poor Asthma Control Predictors
Armour C, et al. Using the community pharmacy to identify patients at risk of poor asthma control and factors which contribute to this poor control. J Asthma 2011; 48:914-22
• Results:– 77% patients had poor asthma control– 21% smoked– 19% had asthma action plan– 69% used combination of ICS/LABA– 17-28% used their inhaler device correctly
• Adherence:– 90% had their ICS or ICS/LABA dispensed <6
times in the previous 6 months

Poor Asthma Control Impact
Wertz D. Impact of asthma control on sleep, attendance at work, normal activities and disease burden. Ann Allergy Asthma Immunol 2010; 105:118-23
• In the real world, asthmatic patients have substantially lower levels of asthma control despite the availability of effective treatments
• Lower levels of asthma control are positively correlated with measures of morbidity, productivity and medical resources

Poor Asthma Control Impact
Wertz D. Impact of asthma control on sleep, attendance at work, normal activities and disease burden. Ann Allergy Asthma Immunol 2010; 105:118-23
• Patients aged 18-64 years enrolled in commercially insured health plans, with at least one medical claim for asthma and one pharmacy claim of asthma controller medication in the last year (Aug 2006)
• Survey of 56 items:– 21 → for control status (Asthma Therapy Assessment
Questionnaire (ATAQ),– 9 → extent of disease impact on work and regular activities (Work
Productivity and Activity Impairment-Asthma Questionnaire),– 15 → Quality of life (Mini Asthma Quality of life Questionnaire)

Poor Asthma Control Impact
Wertz D. Ann Allergy Asthma Immunol 2010;105:118-23
Well-controlled patients
(ATAQ=0) (12%)
Not well-controlled patients
(ATAQ=1-2) (77%)
Very poorly controlled patients
(ATAQ=3-4) (11%)
Comorbid conditions (%)
Insomnia 10.3 8.0 16.2
Depression 17.1 16.7 28.5
Coronary heart disease
2.1 3.1 6.2
Allergies 82.9 86.9 83.8
Baseline Characteristics of the 1,199 Survey Patients
ATAQ: Asthma Therapy Assessment Questionnaire

Poor Asthma Control Impact
Wertz D. Ann Allergy Asthma Immunol 2010;105:118-23
Well-controlled patients
(ATAQ=0) (12%)
Not well-controlled patients
(ATAQ=1-2) (77%)
Very poorly controlled patients
(ATAQ=3-4) (11%)
Asthma severity (%)
Mild 77.4 63.3 23.1
Moderate 20.5 33.2 60.8
Severe 2.1 3.6 16.2
Patient-Reported Asthma Severity
ATAQ: Asthma Therapy Assessment Questionnaire

Poor Asthma Control Impact
Wertz D. Ann Allergy Asthma Immunol 2010;105:118-23
Well-controlled patients
(ATAQ=0) (12%)
Not well-controlled patients
(ATAQ=1-2) (77%)
Very poorly controlled patients
(ATAQ=3-4) (11%)
WPAI-Asthma metric: professional (%)
Work time missed 0.70 3.07 11.92
Impairment while working
10.65 13.62 26.48
Overall work impairment
10.74 14.11 27.55
Work Productivity and Activity Impairment-Asthma (WPAI-Asthma) Questionnaire
ATAQ: Asthma Therapy Assessment Questionnaire

Poor Asthma Control Impact
Neffen H. Asthma control in Latin America: The Asthma Insights and Reality in Latrin America (AIRLA) survey. Rev Panam Salud Publica/Pan Am J Health 17;191-7
• 2.184 adults or parents of children with asthma in 11 Latin American countries in 2003
• Daytime asthma symptoms were reported by 56% of respondents
• Night wakening by 51% of respondents• >50% had been hospitalized, attended hospital
emergency service or made unscheduled emergency visit to healthcare facilities during the previous year

Poor Asthma Control Impact
Neffen H. Asthma control in Latin America: The Asthma Insights and Reality in Latrin America (AIRLA) survey. Rev Panam Salud Publica/Pan Am J Health 17;191-7
• Patients with severe persistent asthma regarded their disease as being well or completely controlled (44.7%)
• Only 2.4% of patients met all criteria for asthma control
• Most adults (79%) and children (68%) reported that asthma symptoms limited their activities
• Absence from school and work was reported by 58% of the children and 31% of adults respectively

Novel Approaches to Achieve Asthma Control
• Patient-oriented vs. Disease-oriented management strategies
• Combination of pharmacological and nonpharmacological treatment modalities
Sarver N. J Am Academy of Nurse Practitioners 2008; 21:54-65

Novel Approaches to Achieve Asthma Control• Solid partnerships between healthcare providers and
patients• Comprehensive patient and caregiver education• Personalized written asthma action plans• Patient reported evaluation of symptoms control• Appropriate drug therapy• Strategies for improving compliance with asthma
medication regimens• Treatment algorithm that outlines the facets of asthma
management
Sarver N. J Am Academy of Nurse Practitioners 2008; 21:54-65
Novel Approaches to Achieve Asthma Control
• Solid partnerships between healthcare providers and patients:– Establishing open communications
– Identifying patient and family concerns regarding asthma control and treatment
– Identifying patient and family treatment preferences regarding options and barriers to its implementation
– Developing treatment goals together with patients and family
– Encouraging active self-assessment and self-management of asthma
National Heart Lung and Blood Institute & National Asthma Education andPrevention Program 2007

Summary• Although the goal of asthma management is to
achieve and maintain overall disease control while minimizing adverse events, many patients’ symptoms are not well controlled despite the availability of effective, well-tolerated therapies and evidence-based guidelines containing treatment recommendations
• More effective oversight and modification of asthma treatment needs to be targeted to asthmatic patients to improve asthma control and decrease impairment of patients’ quality of life and functional capacity


















