Unconjugated Bilirubin Exhibits Spontaneous Diffusion through ...
Upload
ahsan-tanio-daulayCategory
view
214download
0
8/12/2019 Unconjugated Bilirubin
http://slidepdf.com/reader/full/unconjugated-bilirubin 1/9
Unconjugated hyperbilirubinemia is inversely associated withnon-alcoholic steatohepatitis (NASH)M. Hjelkrem*, A. Morales †, C. D. Williams* & S. A. Harrison ‡
*Brooke Army Medical Center,Gastroenterology Service, Fort SamHouston, TX, USA.†Brooke Army Medical Center,Internal Medicine Service, Fort SamHouston, TX, USA.‡Brooke Army Medical Center,Hepatology Service, Fort SamHouston, TX, USA.
Correspondence to:Dr S. A. Harrison, Division ofGastroenterology and Hepatology,Department of Medicine, BrookeArmy Medical Center, Fort SamHouston, TX 78234, USA.E-mails: [email protected], [email protected]
Publication dataSubmitted 12 March 2012First decision 23 March 2012Resubmitted 3 April 2012Accepted 9 April 2012EV Pub Online 29 April 2012
SUMMARY
BackgroundIt has been recognised that unconjugated bilirubin contains hepatic anti- br-ogenic and anti-in ammatory properties and is a potent physiological antiox-idant cytoprotectant. We believe that unconjugated hyperbilirubinemia may protect against development of non-alcoholic steatohepatitis (NASH).
AimThis study was conducted to assess the association of serum unconjugatedbilirubin levels and histological liver damage in non-alcoholic fatty liver dis-ease (NAFLD).
MethodsThis was a retrospective analysis involving adult patients from a tertiary medical centre undergoing liver biopsy to evaluate suspected NAFLD orNASH and a control group without NAFLD based on normal liverultrasound, labs and history. Identi cation of unconjugated hyperbilirubin-emia was based on the presence of predominantly unconjugated bilirubin
1.0 mg/dL (17.1 l mol/L) while fasting, in the absence of haemolyticdisease or other hepatic function alteration.
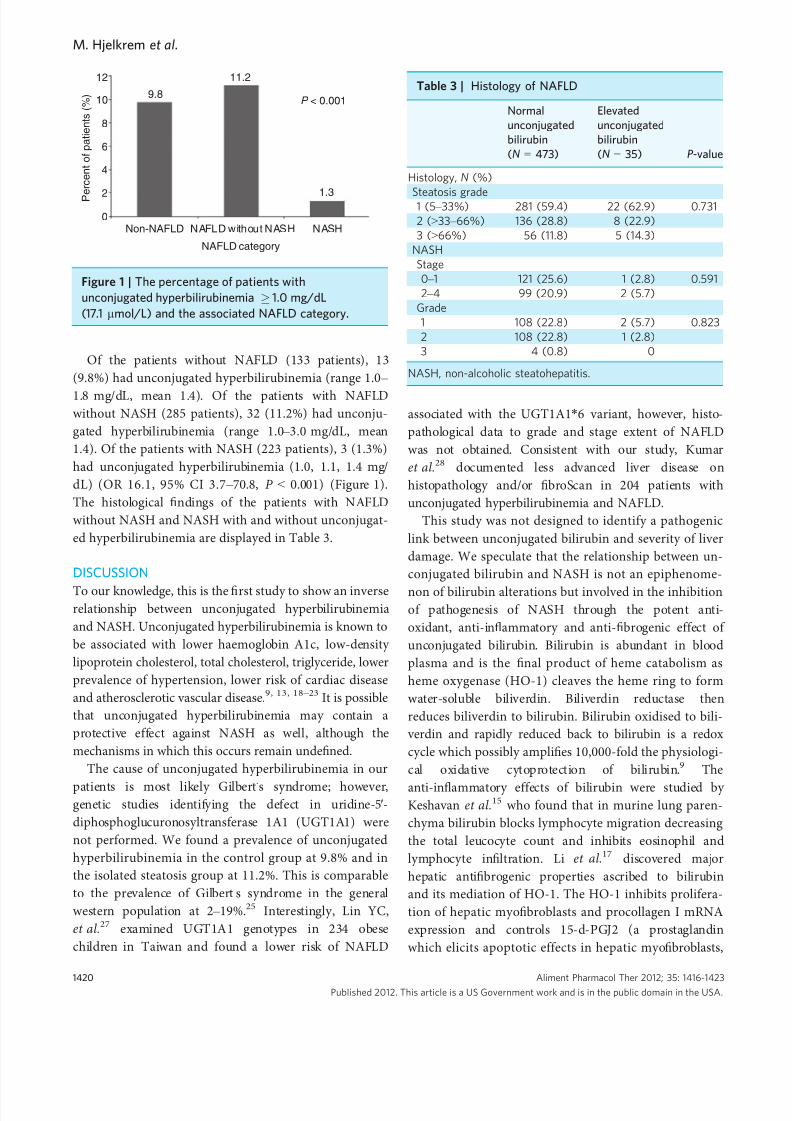
ResultsSix-hundred and forty-one patients were included. Unconjugated hyperbiliru-binemia was inversely associated with NASH (OR 16.1, 95% CI 3.7 – 70.8P < 0.001). Of the patients without NAFLD (133 patients), 13 (9.8%) had un-conjugated hyperbilirubinemia (range 1.0 – 1.8, mean 1.4). Of the patients withNAFLD without NASH (285 patients), 32 (11.2%) had unconjugated hyperbi-lirubinemia (range 1.0 – 3.0, mean 1.4). Of the patients with NASH (223patients), three (1.3%) had unconjugated hyperbilirubinemia (1.0, 1.1, 1.4).
ConclusionsUnconjugated hyperbilirubinemia is inversely associated with the histopath-ological severity of liver damage in non-alcoholic fatty liver disease.
Aliment Pharmacol Ther 2012; 35: 1416–1423
Published 2012. This article is a US Government work and is in the public domain in the USA.doi:10.1111/j.1365-2036.2012.05114.x
1416
Alimentary Pharmacology and Therapeutics

8/12/2019 Unconjugated Bilirubin
http://slidepdf.com/reader/full/unconjugated-bilirubin 2/9
INTRODUCTIONNon-alcoholic fatty liver disease (NAFLD) is the hepaticmanifestation of the metabolic syndrome and has emergedin the last two decades as a burgeoning disease, rapidly increasing in prevalence as it is closely tied to the increas-ing prevalence of obesity, diabetes and the metabolic syn-drome. 1 Patients who develop non-alcoholicsteatohepatitis (NASH) have signi cantly worse clinicaloutcomes with the potential to develop cirrhosis, end stageliver disease and hepatocellular carcinoma.2, 3
The pathogenic mechanisms that result in the develop-ment of NASH remain incomplete. Dysregulation of fatty acid metabolism, development of hepatic insulin resistanceand hyperinsulinemia lead to the development of NAFLD.4
Fortunately, the majority of patients with NAFLD do notdevelop NASH.1, 4 Among patients with NAFLD, up to 1/3 have histological lesions consistent with NASH1 andapproximately 11% of these patients progress to cirrhosisover 15 years.5 Adaptive responses to sustained lipotoxic-ity are inadequate in these patients and this may be modu-lated through environmental and/or genetic processes thatultimately lead to hepatocyte necrosis and in ammation,activation of the brogenic cascade and subsequent bro-sis. Oxidative stress and impaired antioxidant defensemechanisms are widely believed to be factors involved inthis process.4, 6 – 8 Fatty acid accumulation in the liver pro- vides a source of mitochondrial oxidative stress leading tocellular damage, in ammation and progressive brosis.6
Bilirubin, and particularly unconjugated bilirubin, isknown to be a potent physiological antioxidant cytopro-tectant. 9 Bilirubin protects against oxidative stress due toinhibitory effects on the activity of NAD(P)H oxidasewhich may be a basis for increased superoxide produc-tion.10, 11 Furthermore, bilirubin can scavenge peroxylradicals, hydroxyl radicals, singlet oxygen, reactive nitro-gen species12 – 14 and reduce the alpha-tocopheroxyl radi-cal promoting recycling of vitamin E.14 One study showed as little as 10 nmol/L bilirubin has the ability toprotect neuronal cultures against 10 000-fold higher con-centrations of H 2 O2 .9 In addition, bilirubin may have
anti-in ammatory properties 15, 16 and can act as a majoranti brogenic agent via heme oxygenase-1 (HO-1).17
There is also strong supporting clinical evidence for thebene cial cytoprotective effects of unconjugated bilirubinas observed in Gilbert’ s syndrome. It has been shownthat unconjugated hyperbilirubinemia is associated withdecreased risk of coronary and carotid stenosis,13, 18, 19
peripheral atherosclerosis, 20, 21 ischaemic heart disease,22
vascular complications in diabetics23 and even cancer. 24
Patients with unconjugated hyperbilirubinemia have a
signi cantly lower haemoglobin A1c, low-density lipo-protein cholesterol, total cholesterol, triglyceride andlower prevalence of hypertension.23
It is possible that unconjugated hyperbilirubinemiacan reduce oxidative stress, decrease in ammation andprevent brosis ultimately impacting the development of NASH. We aimed to assess the association betweenunconjugated bilirubin levels and histological liver dam-age in patients with NAFLD and NASH.
METHODS
Study populationCharts were reviewed in 641 patients,18 years and olderwho were eligible for care at Brooke Army Medical Center(BAMC), San Antonio, TX, comprising three groups: 133patients without NAFLD (control group), 285 patientswith NAFLD but without meeting strict histopathologicalcriteria for NASH and 223 patients with NASH. Patientsreferred to the Hepatology Clinic to evaluate suspectedNAFLD during the time period 1 January 2003 through 1May 2010 and whose liver biopsy demonstrated NAFLD(not meeting strict criteria for NASH) or NASH wereincluded in the chart review. The control group consistedof patients from a previous study at the same institution 1
who were recruited through study handouts or posters inthe Primary Care Clinic waiting area and from patientspresenting for colon cancer screening classes in the Gas-troenterology Clinic. The control group patients had noprior history of liver disease, normal liver function tests,normal hepatic ultrasound examinations and demo-graphic data similar to the general population. No patientswere included if they had a diagnosis of liver disease fromany other cause to include viral hepatitis, alcoholic hepati-tis, haemochromatosis, alpha-1 antitrypsin de ciency,Wilson ’ s disease; or were taking any medications associ-ated with fatty liver disease (e.g. steroids, tamoxifen, ami-odorone). The study protocol was approved by theInstitutional review board of BAMC.
Data collectionThe following blood test results that were reviewedincluded: serum aspartate aminotransferase (AST),alanine aminotransferase (ALT), total bilirubin, directbilirubin, alkaline phosphatase (ALP), total cholesterol,low-density lipoprotein (LDL), high-density lipoprotein(HDL) and haemoglobin A1C. Tests to include total bili-rubin, direct bilirubin, AST, ALT, ALP, HDL, LDL andtotal cholesterol were collected. Bilirubin values weregathered when they were collected at the same time as
Aliment Pharmacol Ther 2012; 35: 1416-1423 1417Published 2012. This article is a US Government work and is in the public domain in the USA.
Unconjugated hyperbilirubinemia and NASH

8/12/2019 Unconjugated Bilirubin
http://slidepdf.com/reader/full/unconjugated-bilirubin 3/9
cholesterol lab tests thus it was presumed the values were
drawn after at least an 8 h overnight fast. Identi cationof unconjugated hyperbilirubinemia was based on thepresence of predominantly unconjugated bilirubin
1.0 mg/dL (17.1 l mol/L) in the absence of otherhepatic function alteration. 18, 22, 25 Data points closest intime to the liver biopsy were used for statistical analysis.
Histology assessmentAll liver biopsy specimens were prepared and stored atBAMC. Each biopsy was xed in formalin and embedded
in paraf n and Haematoxylin and Eosin (H&E) and Mas-
son Trichrome stains were submitted for analysis. All liverbiopsies were evaluated by a single expert hepatopatholo-gist. A diagnosis of NASH was based on the following criteria: steatosis (typically in zone three/centrilobular),necroin ammatory hepatocellular injury, hepatocellularballooning degeneration with Mallory-Denk bodies. 2, 26
Hepatic ultrasoundThe control group all had normal hepatic ultrasoundexaminations. One staff radiologist with 13 years of
Table 1 | Baseline characteristics of patients
Normal liver ( N = 133)NAFLD without NASH(N = 285) NASH ( N = 223) P -value
Age (years)Mean ± s.d. 54.5 ± 7.2 51.4 ± 9.9 51.8 ± 9.3 0.004Range 31 – 70 21 – 81 19 – 79
Male gender, N
(%) 55 (41.4) 164 (57.5) 105 (47.1) 0.004Body mass index (kg/m 2 )Mean ± s.d. 28.2 ± 5.00 32.3 ± 5.30 33.1 ± 5.72< 25, N (%) 36 (27.1) 14 (4.9) 13 (5.8) < 0.00125 – 29.9, N (%) 56 (42.1) 79 (27.7) 53 (23.8) 0.001
30, N (%) 41 (30.8) 192 (67.4) 157 (70.4) < 0.001Diabetes, N (%) 14 (10.5) 76 (26.7) 101 (45.3) < 0.001Average A1C 5.9 ± 0.7 6.1 ± 1.2 6.4 ± 1.2 0.003A1C > 6, N (%) 19 (29.7) 100 (39.1) 99 (46.5) 0.040
Hypertension, N (%) 54 (40.6) 183 (64.2) 158 (70.9) < 0.001Race, N (%)White 80 (60.2) 137 (48.1) 108 (48.4) 0.050Hispanic 25 (18.8) 64 (22.5) 50 (22.4) 0.662African American 20 (15.0) 23 (8.1) 12 (5.4) 0.007Other 8 (6.0) 61 (21.4) 53 (23.8) < 0.001
Unconjugated bilirubin (mean ± s.d.) 0.6 ± 0.3 0.6 ± 0.3 0.4 ± 0.2 < 0.001Liver enzymes (mean ± s.d.)Alanine aminotransferase (IU) 24.5 ± 9.1 56.3 ± 44.7 62.1 ± 49.5 < 0.001Aspartate aminotransferase (IU) 25.4 ± 7.2 39.3 ± 21.7 46.4 ± 29.0 < 0.001Alkaline phosphatase 75.2 ± 26.3 89.4 ± 41.1 90.7 ± 36.7 < 0.001
Cholesterol (mean ± s.d.)Total cholesterol 186.8 ± 43.9 197.6 ± 42.2 190.4 ± 42.6 0.027LDL cholesterol 107.9 ± 35.3 117.3 ± 36.0 109.9 ± 33.4 0.009HDL cholesterol 57.2 ± 17.3 47.6 ± 14.0 46.9 ± 14.3 < 0.001
Histology, N (%)Steatosis1 (5 – 33%) 207 (72.6) 96 (43.0) < 0.0012 ( > 33 – 66%) 60 (21.1) 84 (37.7)3 (> 66%) 18 (6.3) 43 (19.3)
Stage, N (%)0 – 1 122 (54.7)2 – 4 101 (45.3)
Grade, N (%)1 110 (49.3)2 109 (48.9)3 4 (1.8)
LDL, low-density lipoprotein; HDL, high-density lipoprotein; s.d., standard deviation.
1418 Aliment Pharmacol Ther 2012; 35: 1416-1423Published 2012. This article is a US Government work and is in the public domain in the USA.
M. Hjelkrem et al.

8/12/2019 Unconjugated Bilirubin
http://slidepdf.com/reader/full/unconjugated-bilirubin 4/9
experience in sonography interpreted all the images for
the presence or absence of steatosis. A hepatic ultrasoundwas considered normal if it had homogeneous echotex-ture with no acoustic attenuation, the diaphragm andportal veins were well visualised, and the echogenicity was either similar or slightly higher than that of renalparenchyma. The ultrasound was considered positive forfatty liver if there was increased echogenicity comparedwith renal parenchyma, there was attenuation of theultrasound beam with the diaphragm indistinct and/orthe portal vein walls were less visible.
Statistical analysesContinuous variables were calculated as mean ± s.d. Thestudent ’ s t or Mann – Whitney test was used to evaluateany differences between two groups and the ANOVA orKruskal – Wallis was used to evaluate differences betweengroups of three or more. A Fisher exact test was used forassessment of potential differences between descriptivestatistics calculated for all groups. SPSS 16.0 statisticalsoftware (SPSS Inc., Chicago, IL, USA) was used for allcalculations.
RESULTS
A total of 641 patients were assessed. Demographic datafor the three groups are shown in Table 1. The meanage was 52.2 ± 9.3 (range 19 – 81) and 49.5% werewomen. Not surprisingly, patients with NAFLD andNASH had a signi cantly higher body mass index andhigher prevalence of diabetes, hypertension, AST, ALT,ALP, LDL cholesterol and HDL cholesterol than con-trols. Only 533 patients (83%) had haemoglobin A1c lev-els and higher levels were associated with NAFLD andNASH. Overall, NASH was associated with a lower meanunconjugated bilirubin then the control group and the
NAFLD without NASH group (P < 0.001).The univariate and multivariate comparison of patient
variables with and without elevated unconjugated biliru-bin are reported in Table 2. Unconjugated hyperbiliru-binemia was an independent factor inversely associatedwith NASH among patients with fatty liver when con-trolled for other variables. Multivariate logistic regressionanalysis showed that there were no variables indepen-dently linked to unconjugated bilirubinemia which couldexplain the inverse association with NASH.
Table 2 | Univariate and multivariate analysis of unconjugated hyperbilirubinemia
Normalunconjugatedbilirubin(N = 593)
Elevatedunconjugatedbilirubin(N = 48)
UnivariateanalysisP -value
Multivariate analysisOR (95% CI) P -value
Body mass index (kg/m 2 )
Mean ±
s.d. 31.8 ±
5.8 30.4 ±
3.9 0.030< 25, N (%) 61 (10.3) 2 (4.2) 0.17125 – 29.9, N (%) 168 (28.3) 20 (41.7) 0.051 3.563 (0.741 – 17.138) 0.113
30, N (%) 364 (61.4) 26 (54.2) 0.325 2.976 (0.595 – 14.872) 0.184Diabetes, N (%) 179 (30.2) 12 (25.0) 0.450 1.275 (0.568 – 2.864) 0.556Average A1C 6.2 ± 1.2 6.0 ± 1.3 0.011A1C > 6, N (%) 207 (41.9) 11 (28.2) 0.094
Hypertension, N (%) 371 (62.6) 24 (50.0) 0.085 0.795 (0.383 – 1.651) 0.538Race, N (%)White 299 (50.4) 26 (54.2) 0.618Hispanic 126 (21.2) 13 (27.1) 0.345 1.028 (0.473 – 2.234) 0.944African American 53 (8.9) 2 (4.2) 0.256 0.280 (0.057 – 1.365) 0.115Others 115 (19.4) 7 (14.6) 0.414 0.681 (0.262 – 1.774) 0.432
Liver enzymes (mean ± s.d.)Alanine aminotransferase 50.7 ± 41.7 65.0 ± 67.7 0.247 0.996 (0.985 – 1.008) 0.529Aspartate aminotransferase 38.4 ± 23.1 45.6 ± 30.9 0.147 1.019 (0.995 – 1.044) 0.118Alkaline phosphatase 86.7 ± 37.6 89.2 ± 34.3 0.524 1.006 (0.998 – 1.013) 0.142
Cholesterol (mean ± s.d.)Total cholesterol 193.0 ± 43.5 192.6 ± 33.8 0.950 0.997 (0.982 – 1.012) 0.658LDL cholesterol 112.6 ± 35.5 116.7 ± 29.4 0.432 1.006 (0.988 – 1.024) 0.541HDL cholesterol 49.6 ± 15.6 46.6 ± 11.8 0.201 1.002 (0.975 – 1.029) 0.912
HDL, high-density lipoprotein; LDL, low-density lipoprotein; NASH, non-alcoholic steatohepatitis; s.d., standard deviation.
Aliment Pharmacol Ther 2012; 35: 1416-1423 1419Published 2012. This article is a US Government work and is in the public domain in the USA.
Unconjugated hyperbilirubinemia and NASH
8/12/2019 Unconjugated Bilirubin
http://slidepdf.com/reader/full/unconjugated-bilirubin 5/9

8/12/2019 Unconjugated Bilirubin
http://slidepdf.com/reader/full/unconjugated-bilirubin 6/9
inhibits collagen and proin ammatory chemokine syn-thesis and displays growth inhibitory effects).17
A strategy has been proposed for treating or preventing atherosclerotic vascular disease by inducing an ‘ iatrogenicGilbert ’ s syndrome ’ with therapies that decrease hepaticglucuronidation activity. 13, 29 If a protective association isidenti ed between unconjugated bilirubin and NASH,inducing an ‘ iatrogenic Gilbert ’ s syndrome ’ may be a con-sideration for individuals at high risk for NASH. Probene-cid, a uricosuric medication, inhibits UDP-glucuronic acidtransport from the cytoplasm into the endoplasmic reticu-lum and is listed as a possible cause of unconjugated hyp-erbilirubinemia. 30 Interestingly, studies have shown a link between higher uric acid serum levels and NAFLD inde-pendent of other metabolic risk factors.31 – 33 A recentstudy found hyperuricemia to be associated with the sever-ity of liver damage in NAFLD independent of other meta-bolic syndrome factors.34 This may implicate uric acid as afactor in pathogenesis of metabolic disorders35 and pro-gressive liver damage in NAFLD34 and could act as apotential therapeutic target. 29, 34 Other medications whichraise serum bilirubin include rifampin 36 which inhibits amembrane transport protein OAP1B1 and valproate 37
which inhibits binding of bilirubin to albumin andincreases free unconjugated bilirubin in tissue. Side-effectpro les of rifampin and valproate would likely excludethese medications for use in a large population and valproate has been linked to NAFLD due to increasedbody weight and insulin resistance.38 Other proposedtherapeutic avenues for utilising the oxidative propertiesof bilirubin include phycobilins and algal biliver-din.13, 29, 39, 40 However, the association between uncon- jugated bilirubin and NASH would need to be validatedand a causative effect would need veri cation withprospective randomised controlled studies prior to use of these proposed therapies. Furthermore, therapies thatdecrease hepatic glucuronidation would need safety evalu-ations due to the possible adverse impact on conjugationand clearance of drugs and toxins.
Bilirubin may have a physiological role in modulating
tumorigenesis.41 – 43 In fact, some epidemiological analysesdemonstrate an inverse correlation between serum bilirubinlevels and risk of cancer.23, 44 Elevated serum bilirubin andHO-1 has been shown to be associated with reduced risk for breast cancer45 and squamous oral cancer. 46 An analysisusing data from the Third National Health and Nutrition
Examination Survey found that each increase in serum bili-rubin of 1 mg/dL was associated with a substantial decreasein prevalence of colorectal cancer (OR = 0.257, 95% CI0.245 – 0.260).24 However, an earlier study found no suchassociation between bilirubin and colon cancer risk 47 and asubsequent study found no association between baselineserum bilirubin and incidence of colorectal cancer. 48
The main limitation of this study is the retrospectivedesign and further prospective studies are needed. Fur-thermore, genetic analysis de ning elevated unconjugatedbilirubin as Gilbert’ s disease was not done. For futurestudies this may be important to help de ne if the asso-ciation is due to UGT1A1 expression and its contribu-tion to NASH. Also, the differences in metaboliccharacteristics between the three groups likely representcharacteristic mediating factors associated with NAFLDbut could raise the possibility of selection bias. The con-trol group consisted of 30% obese patients for whichhepatic ultrasound determination of NAFLD is less sen-sitive and it is possible that some of the patient’ s withnormal ultrasounds may have NASH. Another limitationis the possible narrow external validity of our resultsapplied to different populations and settings. Our study cohort consisted of patients enrolled at a tertiary carecentre with government and military health insuranceand may not be applicable to the general population.
In conclusion, we found a signi cantly lower prevalenceof unconjugated hyperbilirubinemia in patients with histo-pathological evidence of steatohepatitis (NASH) comparedto NAFLD without NASH and absence of NAFLD. Addi-tional study is needed to con rm this association as ther-apy that results in higher unconjugated bilirubin may beconsidered in the future to confer a histopathological ben-e t in patients at risk for NASH.
ACKNOWLEDGEMENTSThe opinion or assertions contained herein are the private views of the authors and are not to be construed as of cialor re ecting the view of the US Department of the Army or the US Department of Defense. Declaration of personal
interests: Stephen A. Harrison has served as an ad hoc advisory board member for Amylin Pharmaceuticals andhas received research funding from Rottapharm andMochida Pharmaceuticals. Declaration of funding interests: None.
Aliment Pharmacol Ther 2012; 35: 1416-1423 1421Published 2012. This article is a US Government work and is in the public domain in the USA.
Unconjugated hyperbilirubinemia and NASH

8/12/2019 Unconjugated Bilirubin
http://slidepdf.com/reader/full/unconjugated-bilirubin 7/9
REFERENCES1. Williams CD, Stengel J, Asike MI,
et al. Prevalence of nonalcoholic fatty liver disease and nonalcoholicsteatohepatitis among a largely middle-aged population utilizing ultrasound and liver biopsy: aprospective study. Gastroenterology 2011; 140 : 124 – 31.
2. Kleiner DE. Design and validation of ahistological scoring system fornonalcoholic fatty liver disease.Hepatology 2005; 41 : 1313 – 21.
3. Brunt EM. Histopathology of non-alcoholic fatty liver disease. Clin Liver Dis 2009; 13 : 533 – 44.
4. Pinzani M. Pathophysiology of non-alcoholic steatohepatitis and basisfor treatment. Dig Dis 2011; 29 : 243 – 8.
5. Angulo P. Diagnosing steatohepatitis
and predicting liver-related mortality in patients with NAFLD: twodistinct concepts. Hepatology 2011; 53 :1792 – 4.
6. Koruk M, Taysi S, Savas MC, et al.Oxidative stress and enzymaticantioxidant status in patients withnonalcoholic steatohepatitis. Ann ClinLab Sci 2004; 34 : 57 – 62.
7. Marchesini G, Forlani G. NASH: fromliver diseases to metabolic disorders andback to clinical hepatology. Hepatology 2002; 35 : 497 – 9.
8. McCullough AJ. Pathophysiology of non-alcoholic steatohepatitis. J Clin
Gastroenterol 2006; 40
(Suppl. 1): S17 –
29.9. Baranano DE, Rao M, Ferris CD, et al.
Biliverdin reductase: a majorphysiologic cytoprotectant. Proc Natl Acad Sci USA 2002; 99 :16093 – 8.
10. Inoguchi T, Li P, Umeda F, et al. Highglucose level and free fatty acidstimulate reactive oxygen speciesproduction through protein kinase C-dependent activation of NAD(P)Hoxidase in cultured vascular cells.Diabetes 2000; 49 : 1939 – 45.
11. Lanone S, Bloc S, Foresti R, et al.
Bilirubin decreases NOS2 expression viainhibition of NAD(P)H oxidase:implication for protection againstendotoxic shock in rats. FASEB J 2005;19 : 1890 – 2.
12. Stocker R, Yamamoto Y, McDonaghAF, et al. Bilirubin is an antioxidant of possible physiological importance.Science 1987; 235 : 1043 – 6.
13. Schwertner HA, Vatek L. Gilbertsyndrome, UGT1A1* 28 allele, andcardiovascular disease risk: possibleprotective effects and therapeutic
applications of bilirubin. Atherosclerosis2008; 198 : 1 – 11.
14. Stocker R. Antioxidant activities of bilepigments. Antioxid Redox Signal 2004;6 : 841 – 9.
15. Keshavan P, Deem TL, SchwembergerSJ, et al. Unconjugated bilirubininhibits VCAM-1-mediatedtransendothelial leukocyte migration. J Immunol 2005; 174 : 3709 – 18.
16. Willis D, Moore AR, Frederik R, et al.Heme oxygenase: a novel target for themodulation of the in ammatory response. Nat Med 1996; 2 : 87 – 90.
17. Li L, Grenard P, Van Nhieu J, et al.Heme oxygenase-1 is an anti brogenicprotein in human hepaticmyo broblasts. Gastroenterology 2003;125 : 460 – 8.
18. Vitek L, Novotny L, Sperl M, et al. Theinverse association of elevated serumbilirubin levels with subclinical carotidatherosclerosis. Cerebrovasc Dis 2006;21 : 408 – 14.
19. Ishizaka N, Ishizaka Y, Takahashi E,et al. High serum bilirubin level isinversely associated with the presenceof carotid plaque. Stroke 2001; 32 : 580 –
3.20. Novotny L, Vitek L. Inverse
relationship between serum bilirubinand atherosclerosis in men: a meta-analysis of published studies. Exp Biol Med 2003; 228 : 568 – 71.
21. Krijgsman B, Papadakis JA, GanotakisES, et al. The effect of peripheral vascular disease on the serum levels of natural anti-oxidants: bilirubin andalbumin. Int Angiol 2002; 21 : 44 – 52.
22. Vitek L, Jirsa M, Brodanova M, et al.Gilbert syndrome and ischemic heartdisease: a protective effect of elevatedbilirubin levels. Atherosclerosis 2002;160 : 449 – 56.
23. Inoguchi T, Sasaki S, Kobayashi K,et al. Relationship between Gilbertsyndrome and prevalence of vascularcomplications in patients with diabetes. JAMA 2007; 298 : 1398 – 400.
24. Zucker SD, Horn PS, Sherman KE,et al. Serum bilirubin levels in the U.S.population: gender effect and inversecorrelation with colorectal cancer.Hepatology 2004; 40 : 827 – 35.
25. Clarke DJ, Moghrabi N, Monaghan G,et al. Genetic defects of the UDP-glucuronosyltransferase-1 (UGTII) genethat cause familial non-haemolyticunconjugated hyperbilirubinaemias.Clin Chim Acta 1997; 266 : 63 – 74.
26. Brunt EM, Janney CG, Di BisceglieAM, Neuschwander-Tetri BA, Bacon
BR. Nonalcoholic steatohepatitis: aproposal for grading and staging thehistological lesion. Am J Gastroenterol 1999; 94 : 2467 – 74.
27. Lin YC, Chang PF, Hu FC, et al.Variants in the UGT1A1 gene and therisk of pediatric nonalcoholic fatty liver disease. Pediatrics 2009; 124 :e1221 – 7.
28. Kumar R, Rastogi A, Maras JS, et al.Unconjugated hyperbilirubinemia inpatients with non-alcoholic fatty liverdisease: a favorable endogenousresponse. Clin Biochem 2012; 45 :272 – 4.
29. McCarty M. “ Iatrogenic gilbertsyndrome ” – a strategy for reducing vascular and cancer risk by increasing plasma unconjugated bilirubin. Med
Hypotheses 2007; 69
: 974 –
94.30. Mukherjee S, katz J. Gilbert’ s syndrome.E-medicine website; 2011. Available at:http://emedicine.medscape.com/article/176822-overview.
31. Afzali A, Weiss NS, Boyko EJ, et al.Association between serum uric acidlevel and chronic liver disease in theUnited States. Hepatology 2010; 52 : 578 – 89.
32. Yamada T, Suzuki S, Fukatsu M, et al.Elevated serum uric acid is anindependent risk factor fornonalcoholic fatty liver disease inJapanese undergoing a health checkup.
Acta Gastroenterol Belg 2010; 73
: 12 –
7.33. Lonardo A, Loria P, Leonardi F, et al.POLI.ST.E.N.A. Study Group. Fasting insulin and uric acid levels but notindices of iron metabolism areindependent predictors of non-alcoholicfatty liver disease. A case-control study.Dig Liver Dis 2002; 34 : 204 – 11.
34. Petta S, Camma C, Cabibi D, et al.Hyperuricemia is associated withhistological liver damage in patientswith non-alcoholic fatty liver disease. Aliment Pharmacol Ther 2011; 34 : 757 –
66.35. Yamada T, Fukatsu M, Suzuki S, et al.
Elevated serum uric acid predictsimpaired fasting glucose and type 2diabetes only among Japanese womenundergoing health checkups. Diabetes Metab 2011; 37 : 252 – 8.
36. Murthy GD, Byron D, Shoemaker D,et al. The utility of rifampin indiagnosing Gilbert’ s syndrome. Am J Gastroenterol 2001; 96 : 1150 – 4.
37. Yu HY, Shen YZ. Displacement effectof valproate on bilirubin-albuminbinding in human plasma. J Formos Med Assoc 1999; 98 : 201 – 4.
1422 Aliment Pharmacol Ther 2012; 35: 1416-1423Published 2012. This article is a US Government work and is in the public domain in the USA.
M. Hjelkrem et al.

8/12/2019 Unconjugated Bilirubin
http://slidepdf.com/reader/full/unconjugated-bilirubin 8/9
38. Verotti A, Di Marco G, La torre R,et al. Nonalcoholic fatty liver diseaseduring valproate therapy. Eur J Pediatr 2009; 168 : 1391 – 4.
39. Yamashita K, McDaid J, Ollinger R,et al. Biliverdin, a natural product of heme catabolism, induces tolerance tocardiac allografts. FASEB J 2004; 18 :765 – 7.
40. Brown SB, Houghton JD, Vernon DI,et al. Biosynthesis of phycobilins.Formation of the chromophore of phytochrome, phycocyanin, andphycoerythrin. J Photochem Photobiol,B 1990; 5 : 3 – 23.
41. Keshavan P, Schwemberger SJ, SmithDL, et al. Unconjugated bilirubininduces apoptosis in colon cancer cellsby triggering mitochondrial
depolarization. Int J Cancer 2004; 112 :433 – 5.
42. Rao P, Suzuki R, Mizobuchi S, et al.Bilirubin exhibits a novel anti-cancereffect on human adenocarcinoma.Biochem Biophys Res Commun 2006;342 : 1279 – 83.
43. Ollinger R, Kogler P, Troppmair J,et al. Bilirubin inhibits tumor cell
growth via activation of ERK. Cell Cycle2007; 6 : 3078 – 85.44. Temme EH, Zhang J, Schouten EG,
et al. Serum bilirubin and 10-yearmortality risk in a Belgian population.Cancer Causes Control 2001; 12 : 887 – 94.
45. Ching S, Ingram D, hahnel R, et al.Serum levels of micronutrients,antioxidants and total antioxidantstatus predict risk of breast cancer in a
case control study. J Nutr 2002; 132 :303 – 6.
46. Chang KW, Lee TC, Yeh WI, et al.Polymorphism in heme oxygenase-1(HO-1) promoter is related to the risk of oral squamous cell carcinomaoccurring on male areca chewers. Br J Cancer 2004; 91 : 1551 – 5.
47. Ko WF, Helzlsouer KJ, Comstock GW.
Serum albumin, bilirubin, and uric acidand the anatomic site-speci c incidenceof colon cancer. J Natl Cancer Inst 1994;86 : 1874 – 5.
48. Ioannou GN, Liou IW, Weiss NS.Serum bilirubin and colorectal cancerrisk: a population-based cohort study. Aliment Pharmacol Ther 2006; 23 : 1637 – 42.
Aliment Pharmacol Ther 2012; 35: 1416-1423 1423Published 2012. This article is a US Government work and is in the public domain in the USA.
Unconjugated hyperbilirubinemia and NASH

8/12/2019 Unconjugated Bilirubin
http://slidepdf.com/reader/full/unconjugated-bilirubin 9/9
Copyright of Alimentary Pharmacology & Therapeutics is the property of Wiley-Blackwell and its content may
not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written
permission. However, users may print, download, or email articles for individual use.