Uncommon presentation of a giant biliary cystadenoma: Correlation between MRI and pathologic...
4
Clinical Note Uncommon Presentation of a Giant Biliary Cystadenoma: Correlation Between MRI and Pathologic Findings Christian Frahm, MD, 1 * Arthur Zimmermann, MD, 2 Martin Heller, MD, 1 and Joachim Brossmann, MD 1 An uncommon case of a giant mucinous biliary cystade- noma (BCA) of the liver is described. On T2-weighted and STIR images, a large hyperintense cystic mass revealed some septations and multiple intracystic masses of similar size and shape and uniform signal intensity, which was isointense to liver parenchyma. On T1-weighted images, intracystic bodies were obscured and the cyst was hyper- intense. The magnetic resonance (MR) appearance of in- tracystic fluid and structures was not due to mucinous or proteinous or hyperproteinous material, but corresponded to clots floating within hemorrhagic fluid. J. Magn. Reson. Imaging 2001;14:649 – 652. © 2001 Wiley-Liss, Inc. Index terms: liver; cystadenoma; MRI; hemorrhage; bile duct tumor BILIARY CYSTADENOMA (BCA; SYNONYM: hepatobili- ary cystadenoma; WHO: intrahepatic bile duct cystade- noma) is a rare benign cystic tumor that usually arises in the liver or occasionally in the extrahepatic bile ducts (4,7,8,11). In general, the tumor is multilocular and, at gross examination, well defined by a fibrous capsule. BCAs are lined by a cuboidal to columnar epithelium that typically shows papillary infoldings. The cavities of BCA contain a thin, opalescent or glairy fluid, or a mucinous viscous material. Two histological variants are recognized: the more common mucinous type and the rare serous type (3,11). Mucinous BCAs usually occur in middle-aged women (1,4,11). BCAs may cause massive enlargement, hemorrhage, rupture, secondary infection, jaundice, or vena caval obstruction (2,4,6 – 8). Occasionally, the patient is asymptomatic, and the le- sion is discovered incidentally (1). We reported a case of hepatobiliary cystadenoma showing unusual magnetic resonance (MR) findings due to intracystic hemorrhage. CASE REPORT A 75-year-old woman was admitted to the hospital be- cause of a large cystic mass in the right hepatic lobe. The tumor had been discovered incidentally by an ab- dominal ultrasound examination, which had been per- formed because of an episode of fever, hematuresis, and left abdominal pain 3 months before admission. Sero- logic tests for echinococcosis were negative. A contrast- enhanced CT showed an 18-cm hypodense mass with- out calcifications and without enhancement. MR examination on a 1.0-T imager (Magnetom Harmony, Siemens AG, Erlangen, Germany) demonstrated an 18- to 25-cm cystic mass with some internal septations in the upper pole. The cyst contained multiple small masses of similar size (3–5 cm) and shape, which re- vealed uniform signal characteristics (Fig. 1a and b). The shape of these masses was more or less spherical with markedly lobulated contours. After administration of Gd-DTPA, only mild enhancement of the capsule was noted. On T2-weighted images (HASTE with and without frequency-selective fat saturation, TR 5 1000 msec, TE 5 65 msec) and Turbo-STIR images (TR 5 4000 msec, TE 5 66 msec, TI 5 150 msec), the internal septations and multiple small intracystic masses were nearly isointense, when compared to liver parenchyma (Fig. 1a and b). On T1-weighted images (FLASH with and without frequency-selective fat saturation, flip an- gle 5 70°, TR 5 119 –140 msec, TE 5 6 msec), the whole cystic mass was homogeneously hyperintense, and the septations and multiple small intracystic masses were not visible (Fig. 1c and d). At surgery, a large cystic mass was found arising from the right hepatic lobe, which compressed and displaced the right kidney. A total resection of the mass was performed. On gross examination, the tumor consisted of two large cysts and one small cyst (2.5 cm). Because two cysts were completely collapsed, only one large cyst had been recog- nized on preoperative imaging. This cyst weighed 5700 g and was covered by a tough fibrous capsule (Fig. 2a). Upon incision of the capsule, 2100 g of a hemorrhagic fluid discharged. Furthermore, numerous, more-or-less- 1 Department of Diagnostic Radiology, University Hospital Kiel, Kiel, Germany. 2 Department of Pathology, University of Bern, Bern, Switzerland. *Address reprint requests to: C.F., Department of Diagnostic Radiology, University Hospital Kiel, Arnold-Heller-Strasse 9, D–24105 Kiel, Ger- many. E-mail: [email protected] Received December 6, 2000; Accepted July 10, 2001. JOURNAL OF MAGNETIC RESONANCE IMAGING 14:649 – 652 (2001) © 2001 Wiley-Liss, Inc. 649
-
Upload
christian-frahm -
Category
Documents
-
view
218 -
download
0
Transcript of Uncommon presentation of a giant biliary cystadenoma: Correlation between MRI and pathologic...

Clinical Note
Uncommon Presentation of a Giant BiliaryCystadenoma: Correlation Between MRIand Pathologic Findings
Christian Frahm, MD,1* Arthur Zimmermann, MD,2 Martin Heller, MD,1
and Joachim Brossmann, MD1
An uncommon case of a giant mucinous biliary cystade-noma (BCA) of the liver is described. On T2-weighted andSTIR images, a large hyperintense cystic mass revealedsome septations and multiple intracystic masses of similarsize and shape and uniform signal intensity, which wasisointense to liver parenchyma. On T1-weighted images,intracystic bodies were obscured and the cyst was hyper-intense. The magnetic resonance (MR) appearance of in-tracystic fluid and structures was not due to mucinous orproteinous or hyperproteinous material, but correspondedto clots floating within hemorrhagic fluid. J. Magn. Reson.Imaging 2001;14:649–652. © 2001 Wiley-Liss, Inc.
Index terms: liver; cystadenoma; MRI; hemorrhage; bile ducttumor
BILIARY CYSTADENOMA (BCA; SYNONYM: hepatobili-ary cystadenoma; WHO: intrahepatic bile duct cystade-noma) is a rare benign cystic tumor that usually arisesin the liver or occasionally in the extrahepatic bile ducts(4,7,8,11). In general, the tumor is multilocular and, atgross examination, well defined by a fibrous capsule.BCAs are lined by a cuboidal to columnar epitheliumthat typically shows papillary infoldings. The cavities ofBCA contain a thin, opalescent or glairy fluid, or amucinous viscous material. Two histological variantsare recognized: the more common mucinous type andthe rare serous type (3,11). Mucinous BCAs usuallyoccur in middle-aged women (1,4,11). BCAs may causemassive enlargement, hemorrhage, rupture, secondaryinfection, jaundice, or vena caval obstruction (2,4,6–8).Occasionally, the patient is asymptomatic, and the le-sion is discovered incidentally (1).
We reported a case of hepatobiliary cystadenomashowing unusual magnetic resonance (MR) findingsdue to intracystic hemorrhage.
CASE REPORT
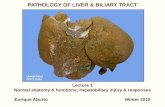
A 75-year-old woman was admitted to the hospital be-cause of a large cystic mass in the right hepatic lobe.The tumor had been discovered incidentally by an ab-dominal ultrasound examination, which had been per-formed because of an episode of fever, hematuresis, andleft abdominal pain 3 months before admission. Sero-logic tests for echinococcosis were negative. A contrast-enhanced CT showed an 18-cm hypodense mass with-out calcifications and without enhancement. MRexamination on a 1.0-T imager (Magnetom Harmony,Siemens AG, Erlangen, Germany) demonstrated an 18-to 25-cm cystic mass with some internal septations inthe upper pole. The cyst contained multiple smallmasses of similar size (3–5 cm) and shape, which re-vealed uniform signal characteristics (Fig. 1a and b).The shape of these masses was more or less sphericalwith markedly lobulated contours. After administrationof Gd-DTPA, only mild enhancement of the capsule wasnoted.
On T2-weighted images (HASTE with and withoutfrequency-selective fat saturation, TR 5 1000 msec,TE 5 65 msec) and Turbo-STIR images (TR 5 4000msec, TE 5 66 msec, TI 5 150 msec), the internalseptations and multiple small intracystic masses werenearly isointense, when compared to liver parenchyma(Fig. 1a and b). On T1-weighted images (FLASH withand without frequency-selective fat saturation, flip an-gle 5 70°, TR 5 119–140 msec, TE 5 6 msec), the wholecystic mass was homogeneously hyperintense, and theseptations and multiple small intracystic masses werenot visible (Fig. 1c and d).
At surgery, a large cystic mass was found arising fromthe right hepatic lobe, which compressed and displacedthe right kidney. A total resection of the mass wasperformed.
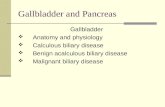
On gross examination, the tumor consisted of two largecysts and one small cyst (2.5 cm). Because two cysts werecompletely collapsed, only one large cyst had been recog-nized on preoperative imaging. This cyst weighed 5700 gand was covered by a tough fibrous capsule (Fig. 2a).Upon incision of the capsule, 2100 g of a hemorrhagicfluid discharged. Furthermore, numerous, more-or-less-
1Department of Diagnostic Radiology, University Hospital Kiel, Kiel,Germany.2Department of Pathology, University of Bern, Bern, Switzerland.*Address reprint requests to: C.F., Department of Diagnostic Radiology,University Hospital Kiel, Arnold-Heller-Strasse 9, D–24105 Kiel, Ger-many. E-mail: [email protected] December 6, 2000; Accepted July 10, 2001.
JOURNAL OF MAGNETIC RESONANCE IMAGING 14:649–652 (2001)
© 2001 Wiley-Liss, Inc. 649

spherical clots of 3–5 cm in size were found within the cyst(Fig. 2a and b).
Histologically, the wall of the large cyst consisted ofan inner layer of necrotic tissue and old blood, partlyorganized by granulation tissue, and an outer layer ofcollagen-rich connective tissue. No intact epithelial lin-ing was found. The walls of the two collapsed cystsconsisted of fibrous, pseudocapsule-like tissue with ad-jacent, markedly atrophic liver parenchyma. Part of theinner surface was covered by an atypical epithelial lin-ing with medium-sized cuboid cells forming a singlelayer (Fig. 3). These cells revealed periodic acid sulphur(PAS)-positive mucin in the cytoplasm. No subepitheliallayer of ovarian-like stroma was found.
DISCUSSION
In general, the mucinous fluid within a BCA appearedhypointense on T1-weighted images and markedly hy-perintense on T2-weighted images (9). However, de-pending on protein concentration, signal intensity ofmucinous fluid may vary. On T1-weighted images, thesignal intensity may change from hypointense to hyper-intense as protein concentration increases. On T2-weighted images, signal intensity of mucinous fluidmay decrease from markedly hyperintense to markedlyhypointense as protein concentration and viscosity in-creases (3). Similar changes may be provoked by inter-nal hemorrhage; however, fluid-fluid levels are usuallyfound in these cases (6,10).
In our particular case, the cystic mass found on MRimaging (MRI) corresponded to an old part of a BCA.This large cyst revealed no intact epithelial lining ormucinous contents and was completely filled with hem-orrhagic material exhibiting a very peculiar, quite uni-form pattern of the clotted blood with no fluid-fluidlevel. Probably, the epithelial lining was lost owing tocellular damage induced by the pressure of the massivehemorrhage. Histological diagnosis of mucinous BCAwas made from the walls of adjacent, completely col-lapsed cysts that were not depicted on MRI or otherimaging modalities.
Figure 1. MR appearance of the large cystic liver mass oc-cupying the whole upper right abdomen in a 75-year-oldwoman. a and b: Within the hyperintense fluid, multipleintracystic masses of similar, more-or-less-spherical shapeare seen on T2-weighted images (a: HASTE with fat satura-tion, TR 5 1000 msec, TE5 65 msec, coronal plane), as wellas on STIR images (b: Turbo-STIR, TR 5 4000 msec, TE 5 66msec, TI 5 150 msec). Some septations were seen adjacentto the capsule. Note the caudal displacement of the rightkidney and a small ovarian cyst (a). c: On T1-weightedimages (c: FLASH, flip angle 5 70°, TR 5 119 msec, TE 5 6msec), the whole contents of the cyst are hyperintense, andtherefore, no intracystic masses and septations are seen.After i.v. Gd-DTPA administration, only slight capsular en-hancement was found (not shown). (Note: The general signalinhomogeneity in anterior-posterior direction is due to theuse of a phased-array coil).
650 Frahm et al.

In general, for cystic hepatic masses containing ma-terial appearing hyperintense on T1-weighted imagesand hypointense on T2-weighted images, the differen-tial diagnoses include cystic masses with mucinousand/or hemorrhagic content: simple hemorrhagic cyst,mucinous BCA and cystadenocarcinoma with or with-
out secondary hemorrhage, hepatic foregut cyst (5),and benign or malignant primary liver tumors or livermetastases with cystic or necrotic components contain-ing secondary hemorrhage. This case describes an un-usual MR appearance of a hemorrhagic cystic mass ofthe liver in general and of a BCA in particular.
Figure 2. Gross pathologic specimen of the hemorrhagic cyst corresponding to the cystic mass depicted on preoperative MRI.a: Large cystic mass after exposure of the capsule. Upon incision, approximately 2 L of hemorrhagic fluid discharged. The cystis filled with numerous clots exhibiting a lobulated, coral-like surface structure, corresponding to the more-or-less-sphericalmasses seen on MRI. b: Four of the spherical clots isolated from the cyst. Most of these clots had a diameter ranging from 3–5cm. [Color figure can be viewed in the online issue, which is available at www.interscience.wiley.com]
Figure 3. Histological ex-amination demonstrates theepithelial lining of a cystade-noma. Tumor cells are ar-ranged in one layer, reveal-ing vacuoles and mucinouscytoplasmic contents (he-matoxylin and eosin stain).The diagnosis was madefrom the walls of twocompletely collapsed cysts,which were found adjacentto the large hemorrhagiccyst on gross examina-tion. These collapsed cystswere not depicted on MRIor other imaging modali-ties. [Color figure can beviewed in the online issuewhich is available at www.interscience.wiley.com]
Uncommon Presentation of a Giant BCA 651

REFERENCES
1. Adam YG, Nonas CJ. Hepatobiliary cystadenoma. South Med J1995;88:1140–1143.
2. Catto JWF, Madan M, Alexander DJ. Hepatobiliary cystadenomapresenting with intermittent inferior vena caval obstruction.J Hepatobiliary Pancreat Surg 1999;6:324–326.
3. Gabata T, Kadoya M, Matsui O, et al. Biliary cystadenoma withmesenchymal stroma of the liver: correlation between unusual MRappearance and pathologic findings. J Magn Reson Imaging 1998;8:503–504.
4. Gadzijew EM, Pleskovic A, Stanisavljevic D, et al. Hepatobiliarycystadenoma can protrude and grow into the bile ducts. Hepato-gastroenterology 1998;45:1446–1451.
5. Kadoya M, Matsui O, Nakanuma Y, et al. Ciliated hepatic foregutcyst: radiologic feature. Radiology 1990;175:475–477.
6. Kawashima A, Fishman EK, Hruban RH, et al. Biliary cystadenomawith intratumoral bleeding: radiologic-pathologic correlation.J Comput Assist Tomogr 1991;15:1035–1038.
7. Lewis WD, Jenkins RL, Rossi RL. Surgical treatment of biliarycystadenoma: a report of 15 cases. Arch Surg 1988;123:563–568.
8. Lind S, Adolph V, Parker GA. Mucinous biliary cystadenoma: a casereport and review of the literature. J Surg Oncol 1992;51:207–210.
9. Palacios E, Shannon M, Solomon C, et al. Biliary cystadenoma:ultrasound, CT, and MRI. Gastrointest Radiol 1990;15:313–316.
10. Soyer P, Bluemke DA, Fishman EK et al. Fluid-fluid levels withinfocal hepatic lesions: imaging appearance and etiology. AbdomImaging 1998;23:161–165.
11. Zimmermann A. Tumours of the bile duct—pathological aspects.In: Blumgart LH, editor. Surgery of the liver and biliarytract, volume 2. Edinburgh: Churchill Livingstone; 1994. p 925–940.
652 Frahm et al.

![Biliary cystadenoma – A rare cystic neoplasm of livercystic lesions of liver with majority of the cases being intrahepatic (80-85%) [5,6]. These lesions constitute less than 5 %](https://static.fdocuments.in/doc/165x107/5f10af037e708231d44a5012/biliary-cystadenoma-a-a-rare-cystic-neoplasm-of-liver-cystic-lesions-of-liver.jpg)