
Uncertainty April Blackmon Auburn University/Auburn...
20
Running head: Uncertainty Uncertainty April Blackmon Auburn University/Auburn Montgomery
Transcript of Uncertainty April Blackmon Auburn University/Auburn...

Running head: Uncertainty
Uncertainty
April Blackmon
Auburn University/Auburn Montgomery
Uncertainty
2
Abstract
This paper explores several published articles that report how uncertainty can play a role in one’s
life. Decision-making anxiety can hinder or help the nurse that is caring for the patient suffering
from illness. Current or recurrent illness can impact a patients’ quality of life. Uncertainty is
unique in that no two people will experience the same feelings associated with that uncertainty.
Nurses also experience uncertainty in bedside practice. Fear, doubt, lack of education all
contribute to uncertainty. One goal of this concept analysis to examine how patients’ with illness
experience uncertainties. Another goal for this analysis is to look closely into how uncertainty
affects nurses and how the nurse is able to over-come self-doubt. Dealing with death and acute
events in life-threatening matters only adds to the stress of decision-making for nurses.
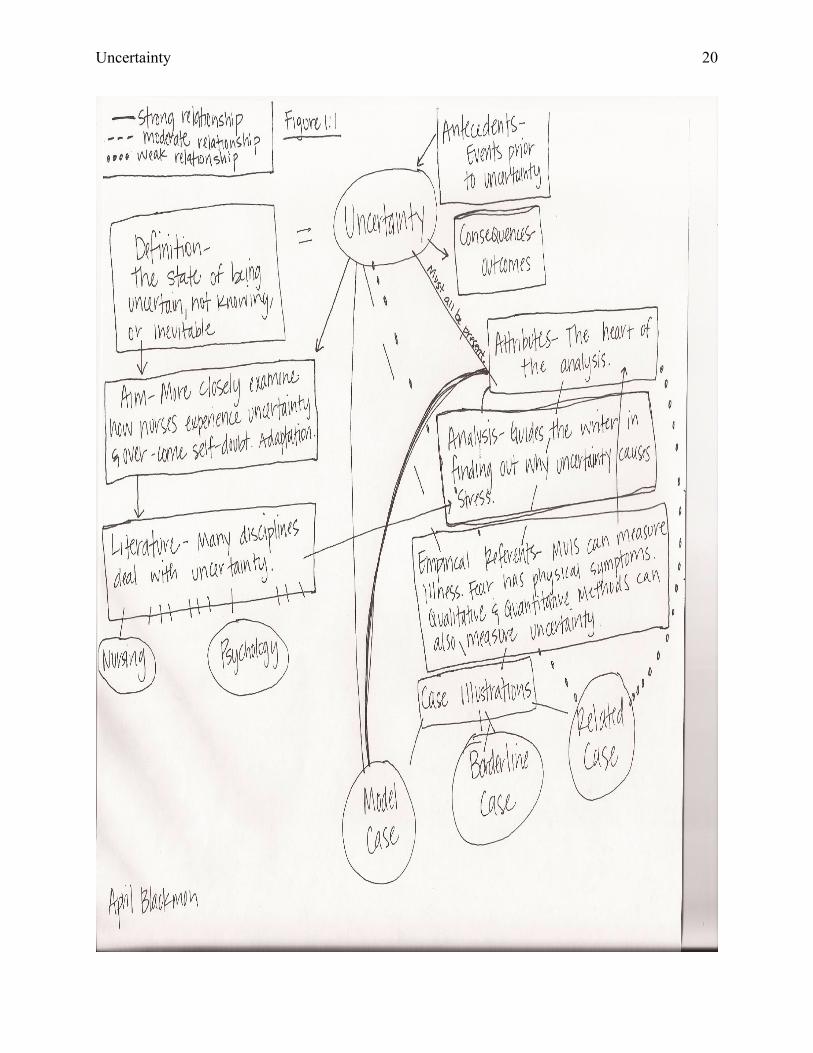
Figure 1:1 (p. 20) illustrates how the topics listed throughout this concept analysis are related and
how it helps the reader make connections between the topics.

Uncertainty
3
Uncertainty
Uncertainty can be defined as the state of being uncertain, not knowing the “for sure”
answer, lack of education or knowing that something is inevitable. Uncertainty can occur in
nursing, psychology, economics, sociology, and for the physician. Each area in which being
uncertain can occur has a different experience with the meaning of uncertainty (Ratner, 2011).
This concept analysis will discuss uncertainty and how it can affect many aspects of one’s life.
Concept
Uncertainty is a dynamic state in which there is a perception of being unable to assign
probabilities for outcomes that prompts a discomforting, uneasy sensation that may be affected
through cognitive, emotive or behavioral reactions (Penrod, 2007). Uncertainty as it relates to
illness is the inability to determine the illness, how to measure the value of events and how to
assess outcomes (Padilla, Mishel, Grant, 1992). This uncertainty in illness can occur not only to
the patient but to the nurse and other healthcare providers as well. Uncertainty is a phenomenon
that is difficult for people to deal with since there is an inherent desire to always know the
answer. Uncertainty as a concept is unique for every person in that learning it is not experienced
the same by each person.
Review of the Literature
This concept analysis is about uncertainty. Walker and Avant (2011) suggest using
dictionaries, thesauruses, colleagues and all available literature to support the topic. The concept
of uncertainty in nursing links making hard decisions with having added stress and anxiety
placed upon the nurses shoulders. In psychology, uncertainty is dealing with the daily struggles
of properly caring for people with mental illness. There are a vast variety of uncertainties in
many disciplines. For this paper’s purposes, two disciplines will be focused on, nursing and
psychology.
Uncertainty
4
Definitions
Uncertainty is the state of not knowing, being uncertain on any one topic, uneducated on
a topic, or having doubt. Patients facing uncertainty may either have an illness with an uncertain
trajectory or may live with the constant possibility that a previous illness could reoccur. Padilla
et al. (1992) found that the longer chronically ill persons lived with continual uncertainty, the
more positively they evaluated the uncertainty. These patients had better critical thinking which,
in turn, opens new doors to new alternatives in adjusting and changing with the nature of their
illness (Padilla et al., 1992).
Uncertainty in nursing.
The nursing definition for uncertainty is the inability to determine the meaning of illness
related events, assign definite values to objects and events, and/or accurately predict outcomes
(Padilla et al., 1992).Uncertainty in nursing is an unavoidable task. Nurses, along with other
healthcare providers must make decisions on the patient’s behalf under pressure. This decision-
making process causes a great deal of anxiety with uncertainty if one is making the right
decision. The nurse is left with the feeling of “what if,” “what if” I had done something
differently or made a different decision, would the outcomes have been better? Unfortunately,
even when right decisions are made, the patient does not always survive. According to Fawcett
(2000), when adult nurses are learning one will enter a dwelling with uncertainty phase. The
dwelling on the uncertainty phase in nursing is spent learning information that seems obscure
and irrelevant (Fawcett, 2000). Only after this phase in nursing can the nurse then understand
unity of thought and think more critically. Uncertainty can create worry for many nurses;
however, nurses are able to develop strategies to manage these concerns (Alaszawski & Coxon,
2009).
Uncertainty
5
The existence of uncertainty in one area of illness often feeds back on itself and can
generate more uncertainty towards other illness-related events (Walker & Avant, 2011). The
patient facing illness can lose their stability in other aspects of his or her life when this occurs.
Patient’s quality of life will be affected in the physical and psychological limitations of their
ability to cope successfully. Padilla et al. (1992) found a significant relationship between social
support and uncertainty; indicating that as social support increases the uncertainty decreases.
Both uncertainty in illness and problems with coping skills will lead to added distress for the
patient and their families (Padilla et al., 1992).Families must find a way to create the appropriate
amount of uncertainty and certainty to maintain coping skills and minimize stress.
Uncertainty in psychology.
Psychology explains uncertainty as the condition of being uncertain, having doubt or
actually existing. Uncertainty in mental health practices can create anxiety and is guarded against
because it can be seen as an inevitable outcome to poor practice (Franks, 2004). The feeling of
uncertainty for many healthcare professionals is a reality; struggling to understand, make sense
of and care for patients with complex behavioral and emotional problems. Current trends in the
mental health field are related to promoting certainty in the form of standardizing and regulating
practices (Franks, 2004). According to Taylor (1983), cognitive adaptation can occur when
threatening events arise. Cognitive adaptation is the means by which human beings bounce back
from threatening or stressful events. Emotions and the pyschophysiological correlates are
thought to play an important role in decision-making under pressure (Studer & Clark, 2011).
Successful adaptation depends, in a large part, on the ability to withstand and modify illusions
that shield not only the present threats but also against further threats (Taylor, 1983). If the
uncertainty remains, it can dismantle the existing cognitive structures that can give meaning to

Uncertainty
6
everyday events (Walker & Avant, 2011). This loss of meaning can throw the person with a
mental illness into a state of confusion and disorganization (Walker & Avant, 2011).
Aim of the Analysis
Uncertainty plays a significant role in explaining various outcomes for the chronically
ill. When individuals are faced with illness it can be devastating to comprehend all the changes
and decisions that go along with disease. This writer is interested in Mishel’s Uncertainty in
Illness Theory to see how individuals adapt to illness and how this affects their quality of life.
Uncertainty is an important topic due to the simple fact that it can cause so much anxiety in one’s
life. Nursing is also a career in which one faces uncertainty. This writer would like to more
closely examine how nurses experience uncertainty when making decisions for others and how
he or she overcomes self-doubt. Dealing with death and acute life-threatening events only adds
to the stress of decision-making.
Analysis of the Concept
Uncertainty has many different meanings and ideas that can be relevant in several
different professions and in life itself. Uncertainty can occur to anyone at any time throughout
the lifespan. It can occur when illness strikes or when faced with the anxiety of making tough
decisions.
Process of Analysis
Walker and Avant (2011) suggest that when choosing a topic for analysis to follow these
eight steps: “1. Select a topic. 2. Determine the aims or purposes of the analysis. 3. Identify all
uses of the concept that one can discover. 4. Determine the defining attributes. 5. Identify a
model case. 6. Identify borderline, related, contrary, invented and illegitimate cases. 7. Identify
antecedents and consequences. 8. Define empirical referents”. This writer will use these eight
Uncertainty
7
steps to help guide the analysis of uncertainty and all results found. Uncertainty is an important
concept; it can include uncertainty in nursing, illness, psychology, economics, and sociology.
The “aims or purposes of the analysis helps center concentration on exactly what the writer
intends to make of the results” (Walker & Avant, 2011). This writer is interested in finding out
why uncertainty causes so much stress on an individual.
The defining attributes of the concept are the “guts” of the analysis (Walker & Avant,
2011). It is not uncommon for the attributes to appear numerous times in different topics related
to the concept (Walker & Avant, 2011). Model cases can be from real life experiences, found in
research or made up by the writer. Borderline cases are examples that include most defining
attributes but not all of them. Related cases are comparable to the concept but differ from them
when examined more closely (Walker & Avant, 2011). Contrary, invented and illegitimate cases
are all examples of what the concept is not and they do not contain all attributes.
Antecedents are events that occur prior to the event or concept. If uncertainty in illness is
the concept then an antecedent would be life prior to the illness. Consequences are the events
that happen as a result of the concept, or the outcomes (Walker & Avant, 2011). The outcomes of
uncertainty in illness would be overcoming of the illness or progression of the illness. Lastly,
defining empirical referents is the final step. The empirical referents are not a measurement tool;
they are simply the means by which one can distinguish the defining attributes of the concept
(Walker & Avant, 2011). After all steps are taken, the final result will yield a proper concept
analysis.
Critical/Defining Attributes
Determining what constitutes as defining attributes of uncertainty are the “guts” of
concept analysis (Walker & Avant, 2011). If faced with a tough decision, one must understand

Uncertainty
8
and measure all attributes of uncertainty. Attributes of uncertainty are: not knowing, doubt, fear,
lack of education or something that is inevitable. Fear, an attribute of uncertainty can cause
physical measures to become elevated. Blood pressure rises, heart rate increases, diaphoresis sets
in and this causes more distress in the person making decisions. Alaszewski & Coxon (2009)
suggest that uncertainty is growing in contemporary society; this writer would like to examine
how that threatens individual well-being. If faced with this anxiety, it could cause a person to
become more uncertain about whether or not he or she is making the right decisions. If attributes
of uncertainty continues in nurses, this could eventually lead to disparities within the nursing
field (Potter & Perry, 2006). Uncertainty has been the focus of a great deal of research over the
past decade and has consistently predicted illness-related outcomes (Wallace, 2005).
Antecedents
Antecedents are events that occur prior to the uncertainty (Walker & Avant, 2011). If
uncertainty in illness is occurring in ones’ life, then an antecedent for that person would be:
quality of life before the illness occurred. Decision-making before an acute illness may have
seemed trivial. In illness, another antecedent is the stimuli frame. This frame consists of
symptom patterns and event familiarity (Mishel & Braden, 1987). The symptom pattern relates
to the disease that the patient is experiencing. In event familiarity, the degree to which a situation
is habitual, repetitive or contains recognizable cues is fostered by time and experience in the
health care environment (Mishel & Braden, 1987).
In the nursing field, the antecedent for decision-making would be to understand all
knowledge related to that person’s specialty and how to react in acute events (Fawcett, 2000).
Another antecedent would be cognitive capacity. This is the information-processing ability of a
Uncertainty
9
person and any physiological malfunction that may impair ability (Wallace, 2005). An
individual’s physical illness symptoms and perceived dangers have been largely shown to
decrease cognitive capacity.
Empirical Referents
Mishel developed the Mishel Uncertainty in Illness Scale (MUIS) which is used to
determine levels of adaptation in relation to an illness. With this scale one can measure how the
patient perceives the illness and how they are coping with said illness. The two main processes
of this scale are inference and illusion. With the inference and illusion processes patients are
evaluating situations related to their own illness. The inference and illusion can be viewed as
positive or negative; positive meaning an opportunity and negative suggesting danger. If two
patients have the same illness and patient “A” receives treatment and recovers from the illness
then that would be viewed as an opportunity. Patient “B” could gather information on the illness
and relate it to his or her own situation. This opportunity helps the patient to gather the
information needed, have a relatable situation and make the decision to resolve the illness. This
process of inference and illusion may help the patient increase quality of life. If in the same
scenario patient “A” had not recovered from the illness that would be viewed as a threat or
danger using the inference and illusion process. Patient “B” would continue with uncertainty by
not gathering information, not having a relatable situation and not adapting or coping with the
illness. This would inflict a decrease in the patient’s quality of life. The negative inference and
illusion of not recovering from the illness would create lower quality of life and decreases coping
skills (Potter& Perry, 2006).
Uncertainty
10
Fear, when dealing with uncertainty can be measured with physical symptoms. The
person experiencing fear will exhibit fright, increased cardiac excitation, and responses of flight
or fight for adaptive purposes. Measurement indices of fear include: enhanced startle response,
increased sweating from the skin, MRI scan displays of amygdala activation, and changes in the
autonomic nervous system (Bay & Algase, 1999). Doubt, although different from uncertainty
and fear can be experienced in the same measures. Doubt is being uncertain about something or
hesitating to believe in something. If one is undergoing hesitation, his or her speech pattern will
become guarded. The person will experience excessive breaks in the flow of normal speech.
Qualitative and quantitative methods can be used to measure these referents. Using
qualitative methods the information collected would be subjective, describe the problem an
individual is facing and contain more in-depth material (Timmerman, 1999). An opinion of how
the person is experiencing the uncertainty whether in illness or life is an excellent example of
qualitative measurements. Quantitative methods are more objective, less in depth and more
generalizable. The experiences individuals have with uncertainty would be based more on
diagnostic tests, such as, MRI or PET scan to accurately use quantitative methods for
measurement. Both of the methods can however, measure uncertainty and how it is perceived in
each individual.
Nurses must always be aware and understanding of uncertainty (Potter & Perry 2006).
Decision-making is a large part of a nurses’ duty. Making decisions under extreme pressure
when uncertain medical issues arise is a large concern for nurses and other healthcare providers.
The practical way general practitioners deal with uncertainty remains unclear (Scheider et al.
2010). One’s sense of confidence and sense of control are primary factors that can determine the
nature of the experience with uncertainty (Penrod, 2007). Each nurse or healthcare provider will
Uncertainty
11
experience and handle uncertainties differently. The consequences of these experiences are
discussed in the next section.
Consequences
“Consequences are those events or incidents that occur as a result of the occurrence of the
concept” (Walker & Avant, 2011). A consequence of uncertainty in illness would be that the
patient is able to adapt to the disease. If one views the illness as a positive the outcome for that
person is coping abilities, adaptation and increases in quality of life. On the other hand, if one
views the illness as a negative his or her outcome will be viewed as a threat or danger, the coping
skills are lacking or absent, adaptation does not take place and this will result in decreased
quality of life.
Nurses, deal with uncertainty on an almost daily basis. Nurses also experience guilt or
fault when death occurs, even if the right decisions were made and all life saving measures was
taken. The outcomes of these situations result in added stress and anxiety for the nurse. Decision-
making skills can become tainted in the nurse with high stress and anxiety over uncertainties
when caring for others. The consequence of confusion is replacing anxiety with feelings of
freedom to critically examine old ways and explore new ways in nursing (Fawcett, 2000). This
helps the nurse to think more critically in an acute event. The concept of guided clinical learning
under supervision of a more experienced nurse is by no means a new trend (Charleston &
Happell, 2005). The responsibility of teaching a new nurse adds stress and anxiety on the
decision maker. An outcome for this event creates more uncertainty for the senior nurse in
charge of the new hire. This process becomes a vicious cycle, the new nurse then learns the
concept of uncertainty in the beginning of his or her career.
Uncertainty
12
Case Illustrations
“A model case is an example of the use of the concept that demonstrates all the defining
attributes of the concept” (Walker & Avant, 2011). The model case should be one that is absolute
in the concept chosen. “The model case can be made up from life experiences, found in literature
or constructed by the writer” (Walker & Avant, 2011).
Model Case
Uncertainty in nursing is the example chosen for the model case. As a nurse, one faces
uncertainty in almost every instance of an acute event. The patient is crashing, what should one
do next? Did one check the electrolytes, does the patient have an airway, is there an ambu bag in
the room, where are the emergency drugs. Defining attributes for uncertainty in nursing are: not
knowing, doubt, fear, or lack of education. Not knowing in nursing can be the result of being
unfamiliar with the surroundings or simply not knowing why the event is occurring. Working in
a large hospital, the utilization of a pool staff is common. The nurse may have never worked on
the unit before and does not know where emergency drugs are kept or how to follow the chain
for emergency help. This increases stress and uncertainty in the nurse.
Having doubts about the event are also common. Doubt for why this is happening, and
how to correct it quickly. Doubt is being uncertain related to an event and this is a sure example
of uncertainty. Fear is activation of flight or fight, hormones are kicking in and the nurse will
show signs of increased heart rate, blood pressure and sweat gland activity. The nurse will begin
to question his or her day; did the patient complain of chest pain, what did the chest x-ray look
like, what were the lab values. Uncertainty is at full force in the period. Lack of education can
Uncertainty
13
affect nurses. Perhaps, this is a new nurse with a seemingly stable patient whom just crashed; the
nurse does not yet have the skills to think quick and acutely for decision-making.
Antecedents for this case would be the nurse knowing everything about this patient and
this unit before the acute event. Knowing how to think critically and through a sequence of prior
events to determine causes of acute events are also antecedents of this case. Consequences for
this case would be dealing with guilt or fault in the event this situation ends badly. Another
consequence would be if the patient stabilizes, the nurse can think of how he or she reacted and
how to better prepare for similar events in the future.
Attributes for the model case are not knowing, fear, doubt and uncertainty. The nurse
experiences all attributes when dealing in an acute event. The knowledge is measured by how the
nurse reacts to the situation. Fear is seen in physical symptoms, sweat, elevated heart rate and
blood pressure. Doubt is measured by how the nurse is speaking throughout the event; talking
rapidly, or stuttering in thoughts. These are all attributes of uncertainty and as Walker & Avant
(2011) state, demonstrate the concept.
Borderline Case
“Borderline cases are examples that contain most of the defining attributes of the concept
but not all of them” (Walker & Avant, 2011). These types of cases help the reader see why the
model case is so important. An example of a borderline case for uncertainty is new nurses
making decisions for patients. Caring for others is a hard enough task, but making decisions for
others regarding care can be a daunting assignment. Upon starting work at the University of
Alabama at Birmingham hospital one must endure a lengthy orientation period. This phase
consists of learning how to effectively care for others and promotes confidence in the new nurse.

Uncertainty
14
The hospital offers a professional environment to help nurses establish caring relationships with
staff, patients and their families. The nurse-to-patient ratios give the new nurse opportunities for
a beneficial and rewarding care of experiences. Nurses share the governance model that
recognizes the important contributions and leadership of nursing staff, and encourages nursing
staff involvement of decision making (UAB, 2011). This model will help ease some added
anxiety the nurse faces when making decisions for patients. This case helps clarify thinking
about the defining attributes of the concept of interest (Walker & Avant, 2011).
The attributes in the borderline case are doubt and uncertainty. This case experiences
some of the defining attributes but not all that are correlated with uncertainty. New nurses
experience doubt in if he or she have made the right decision for a lifelong career and are
uncertain in starting a new job. The measurements of these attributes are observing the new
nurse. He or she will be hesitant in their actions with patients. The new nurse will also
experience uncertainty in any interventions that he or she may provide in patient care.
Antecedents for this case are graduating from an accredited nursing school and completion of
state board exams. Consequences for this case include: outcomes of the nursing orientation
period and preceptorship.
Related Case
“Related cases are instances of concepts that can be related to the concept but does not
contain all the defining attributes” (Walker & Avant, 2011). The related case will be associated
in some way to the concept. An example of a related case for uncertainty is having doubt when
making decisions. Doubt and uncertainty are synonyms but can be thought of differently when
making decisions. Each one of us is blasted with many decision-making opportunities each and
Uncertainty
15
every day. Many factors become involved in the decision-making process; those factors can
include self-doubt. Self-doubt is the fear of making a mistake.
Information about decision making comes from the environment and from those involved
in the decision. Some information may be supportive and encouraging and some may not. This is
where self-doubt of making mistakes arises, other’s expectations of the decision and even
criticism of past mistakes. Responses, from others help to shape and develop one’s self-
perception, part of which involves decision-making abilities. If allowed, fear can interfere with a
decision, self-doubt sets in and the decision becomes that much harder to make. A self-doubting
mindset can set one up to fail. According to Walker & Avant (2011), related cases should have
names of their own; this case would be named “Self-Doubt.” This case can help the reader see
how self-doubt is related to uncertainty but does not contain the defining attributes of
uncertainty.
Attributes of the related case are experiencing doubt when making decisions. This is the
only attribute in this case. Doubt is measured in this case by how the nurse values self. Self-
doubt comes from how the nurse values him or herself and the expectations in place from others.
The nurse will be hesitant in patient care and most likely seek others’ opinions for help in
decision-making. Hesitation can be seen in speech as slow, stuttering or rapid. Antecedents of
this case are having knowledge of what the decision is regarding and how to properly proceed.
Consequences in the related case are overcoming the self-doubt or continuing with the doubt. If
the new nurse is able to overcome the self-doubt an outcome would be confidence in decision-
making skills. If the nurse is unable to overcome the self-doubt, he or she will continue to suffer
when making decisions.

Uncertainty
16
Analysis Summary
Walker & Avant (2011) suggest using eight steps to guide the analysis process. These
steps are listed above and used throughout this analysis. Uncertainty can occur in nursing,
psychology, economics, sociology, statistics and for the physician. Each area in which
uncertainty occurs has different experiences and meanings with the concept. Uncertainty is a
dynamic state in which there is a perception of being unable to assign probabilities for outcomes
that prompts a discomforting, uneasy sensation that is affected through cognitive, emotive or
behavioral reactions (Penrod, 2007). Uncertainty affects patients, nurses and other healthcare
providers. In nursing, one is responsible for making decisions on the patients’ behalf. This leaves
the nurse with the “what if” feeling, “what if” a different decision could have been made or
another outcome could have been better? Uncertainty can create added worry for many nurses;
however, nurses are able to develop strategies to help manage these concerns (Alaszawski &
Coxon, 2009).
Psychologists are faced with struggling to understand, make sense of and care for patients
with complex behavioral and emotional problems. According to Taylor, cognitive adaptation can
occur when threatening events arise (Taylor, 1983). If this uncertainty remains, it can dismantle
the existing cognitive structures that give meaning to everyday events (Walker & Avant, 2011).
When individuals are faced with illness it can be devastating to comprehend all the
changes and decisions that go along with the disease. The disease can be comprehended as a
positive or as a threat. Positive meaning that the event is viewed as an opportunity and the patient
will make the necessary changes to increase quality of life, cope appropriately and adaptation
occurs. If the event is viewed as a negative or as a threat the patient does not develop any coping
skills, adaptation does not occur and quality of life decreases.
Uncertainty
17
Implications/Application to Nursing Practice
Several uses of the results of this concept analysis have been discussed. Implications for
uncertainty in illness are inference and illusion; this is when patients are evaluating situations
related to their own illness. The process of inference and illusion may help or hinder quality of
life.
Problem-solving and decision-making are important skills for nursing and in life. One
implication for nursing practice would be better decision-making skills. Some nurses may have
moderate decision-making skills but should still focus more on improving the quality of their
decisions (Studer & Clark, 2011). Nurses that are less natural in decision-making, especially
under pressure, may be able to handle a quality assessment of an acute event but need to practice
being more decisive in acting upon that assessment (Struder & Clark, 2009).
Controlling fear is another implication for nursing. There are many factors that can create
fear in nursing. Fear is a product of subconscious reactions to certain stimuli that is internal to
oneself (UAB, 2011). When the fear level is increased, the ability to think rationally tends to
spiral downward to the point where one’s actions can become inappropriate for the situation. To
begin controlling fear, one must examine the mechanisms that cause fear. Often preparing for an
event that is fearful can help one master control over the situation. Train the mind to
acknowledge the fear and accept if for what it is, simply the mind telling the body that it is
distressed about something (UAB, 2011).

Uncertainty
18
References
Alaszewski, A., & Coxon, K. (2009). Uncertainty in everyday life: risk, worry and
trust. Health Risk and Society 11(3), 201-207
Bay, E. J., & Algase, D. L. (1999). Fear and anxiety: a simultaneous concept. Nursing
Diagnosis 7, 99-111
Bonis, S. A. (2009). Knowing in nursing: a concept analysis. Journal of Advacned
Nursing 65(6), 1328-1341.
Franks, V. (2004). Journal of Psychiatric and Mental Health Nursing 11, 99-105
Mishel, M.H. & Braden, C. J., (1987). Uncertainty a mediator between support and
adjustment. Western Journal of Nursing Research 9(1), 43-57.
Mamner, T. A., & Ralie, A. M. Nursing theorists and their work. The Health Promotion
Model. St. Louis: Mosby: 2005
Padilla, G.V., Mishel, M. H., & Grant, M.M. (1992). Uncertainty, appraisal, and quality of
life. Quality of Life Research 1, 155-165.
Penrod, J. (2007). Living with uncertainty: concept advancement. Journal of Advanced
Nursing 57(6), 658-667.
doi: 10.1111/j.1365-2648.2006.04008.x
Polit, D., F., & Beck, C., T. Nursing research: Principles and Methods. 7th Ed.
Philadelphia: Lippincott, Williams, & Wilkins; 2007.
Potter, P. A., & Perry, A. G. Fundamentals of nursing. 6th Ed. St. Louis: Elsevier Mosby;
2006
Ratner, N., B. (2011). Some pragmatic tips for dealing with clinical uncertainty.
American Speech-Language Hearing Association 42, 77-80

Uncertainty
19
Schneider, A., Lowe, B., Barie, S., Joos, S., Engeser, E., & Szecsenyi, J. (2010). How do
primary care doctors deal with uncertainty in diagnostic decisions? Journal of
Evaluation in Clinical Practice 16 (2010), 431-437
Studer, B., & Clark, L. (2011). Place your bets: psychophysiological correlates of
decision-making under risk. Cognitive, Afecctive & Behavioral Neuroscience
11(2), 144-158.
Taylor, S. (1983). Adjustment to threatening events: a theory of cognitive adaptation.
American Pyschologist 38 (11), 1161-1173
Timmerman, G., B. (1999). Using a women’s health perspective to guide decisions made
in quantitative research. Journal of Advanced Nursing 30(3), 640-645.
University of Alabama at Birmingham Nursing Personal Development. (n.d.). Retrieved on
July 29, 2011, from http://www.uab.edu
University of Alabama at Birmingham Nursing Recruitment Page. (n.d.). Retrieved on
July 14, 2011, from http://www.uab.edu
Walker, L. O., & Avant, K. C. (2011). Strategies for Theory Construction in Nursing. 5th
Ed. Upper Saddle River, NJ: Pearson Prentice Hall.
Wallace, M. (2005). Finding more meaning: the antecedents of uncertainty revisited.
Journal of Clinical Nursing 14, 863-868
Uncertainty
20


















